˘ˇˆ˙˝ 1 - marianna uigakukai.marianna-u.ac.jp/idaishi/www/366/06-36-4hiromitu sekizuka.pdf ·...
TRANSCRIPT

���� ����������Vol. 36, pp. 537�544, 2008
���������� ���������������� 1�
������
�����
1 ����
��
��2 �
��
������
1 � �
��
������
1
����
��������
1 �����
�����
1 ���
�
���
1 ��� !
�
�"�1
!"����
��
#�
$#1 �
��
��
%$
��3 �
�
��
&��
� 3 '
%&
��
�
� 3
��� ! �
��'��#
1
�(� :�) 20� 11* 29��
� �+�, 45-�.( 2007� 10* 12�/0 1012345��6789:4;<=4>) ��?@=AB( C�?(DA) E 12!"F#GHF$I� �AF�?J�KBBK%�?LM(DAB( 10* 15�N�&O.F$I�6'P�Q(RF#GST)UV*WXYZ[��
����#\]^_) ���`+?abAB( `+ab�4cd06��?@=ABBKWXYZ[�HefF#G?S,A)UAB( - 30.4��4>) +g,hiABBK) j4kk/0AB( )UF#GS,lm) ��4n4F#G,Fo1& �VT��pqr�2s QRS3414&OHtuB( vw&O4xy,zluB9 �789:4;<=� 4'{? VT�|}) ~�56HF�#��+6�� �EPS�?����/��AB( 10* 25� EPSH,7e4��.Fo1498�6!&�rB( 10 * 30 � dual chamber R��JR�I���ICD�?�����( �419H AF� VT�4�:,,u��AzluB( ;�>) VT&O6'P�7ef4 ICD��O�?<K) F=F#GS,N� VT4o$)"1>9�*6��P���9�<�rB( ?1�6S,�rBWXYZ[�6N�) @��.Fo144>6 AF4&�9�<H�B( VT4o$)"9�1>6zuB��) j4F$�1>��6N� AF9!&�r���9�A�rB(
��Fo14) Q( )UF#¡) F$I�
�� �
��DB4�H) ¢£9¤ml4+g?<¥B��6F#G4S,9H��¦§,¨K©ªz;) j
4«9&O.4C¬DDE?F6A©}�( ®f¯*,) j4N�zGH?°±P�²I�A©JKzQ(RF#GST)UV*WXYZ[�� ����#\]^_) ���4S,�) ��JR�I���implantable cardioveter defibrillator; ICD� S,N�) F$I� �³´ AF �LP�4'{9Fo14�³´VT�LP�4�1>o$)"6N���9�A�rB+�?µ¶AB4HM·P�(
1 ���������N� =� �¸¹�=��2 ��������� O+3 "º»P¼QN� =� �¸¹�=��
537
25

� �
� �: 45�� ���� �: �����: ���� �amlodipine 5mg� losartan 50
mg�day ������� �atrovastatin 5mg�day ���
�: � �������� ������� : 2007 � 10 ����� 10 ��� !"#$%&' ()* +� ��,-*�.� /0,12�� �3 12�45678 AF,9:;..;<=,>?12�.� 2�+#@AB�5�C�8<=,12�.&DEF@G�H� �I2�aprindine 100mg� J2� pilsicainide 100mg� KL+ 24�MN#OP�QD.� R �STUVWXYZ[�,\]�.��������: ^_ 172 cm� `a 92 kg� BMI31.1� �� 149�103mmHg� �b 135�� ��H�� c 5de� feghiE� jk�l����� X� �Fig. 1�: 5cmn 53�� �op�5qrst��� uvw�� cxy�,z{i|}~��� j�t�������T��� 12����� �Fig. 1�: HR95-150� 5�C��� !��"#$��� �Fig. 2�: ������ PQM��� �PQ 80msec��%&'(: ����WBC 8.3�103�ml� RBC 5.3�106�ml� Hgb 15.7g�dl� Hct 46.9�� Plt20.2�104�ml ��
��� T. P 6.8g�dl� T. bil 0.4mg�dl� GOT 75IU�l�GPT 119IU�l� LDH 215IU�l� ALP 303IU�l� g-
GTP 274IU�l� BUN 16.2mg�dl� Cr 0.79mg�dl�U. A 5.7mg�dl� Na 141mEq�l� K 3.7mEq�l� Cl108mEq�l� Mg 2.0mg�dl� Glu 105mg�dl ������ CRP 0.03 mg � dl ����TSH 1.39 mU �ml�0.436�3.78�� T3 3.9 pg�ml �2.1�4.1�� T4 1.3 ng�dl�1.0�1.7�� BNP 58.3 pg�ml��)*+,'( �Fig. 3�: ��s������������54�40mm� 5������+��12�14mm� ����� �EF�51�� E�A0.82� DcT196 msec� ���� ��s����� E[8�����5�t� ��s���, ;.� �op����¡�pw.��-./01'(: �3 12�4567: PQM��� �80 msec��I�II�III�aVF �V4�6 �48 ST ¢j�A-H�M: 50 msec� H-V �M: 43 msec� Wencke-bach rate: 180 ppm� jump-up£¤��� Fast path-way ¥4¡¦§¥4��,¨�.�3 �5���©ª � J£�,«wQ¬� VT®S¯5�C� �Nj Vf:���&�A°F.� ±�6²³C� 200J 8OP�Adenosine 10 mg iv 8 ATP )1� �| fast
pathway ¥4¡´F� A-H�M: 125 msec� H-V�M: 29 msec: A-H �M¡����.� µ � PQ M� 127 msec 8�w.�UVWXYZ8 °F.!¶ QRS "b �wide
Figure 1. Chest X-ray films and electrocardiograms at the first medical examination.
·¸¹º »#±¼ o538
26
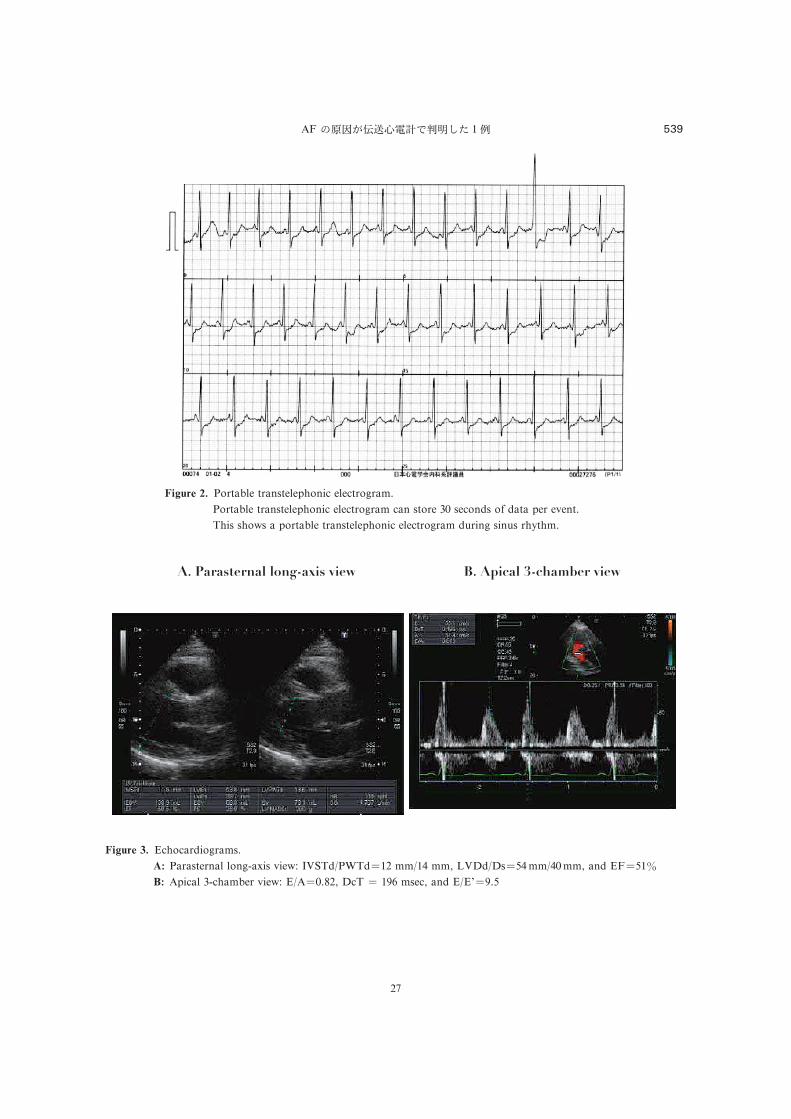
Figure 2. Portable transtelephonic electrogram.
Portable transtelephonic electrogram can store 30 seconds of data per event.
This shows a portable transtelephonic electrogram during sinus rhythm.
Figure 3. Echocardiograms.
A: Parasternal long-axis view: IVSTd�PWTd�12 mm�14 mm, LVDd�Ds�54mm�40mm, and EF�51�B: Apical 3-chamber view: E�A�0.82, DcT � 196 msec, and E�E[�9.5
AF ���������� � 1� 539
27
QRS tachycardia� �������������: �� ���� �Fig. 4� �������������� !�� ��"#$%& '( �Fig. 5�� ���) 30*+,-./0�����12 !� 3�4456 � '(789%&�:� ���;�789�7<=>?@A�.BC QRSD�=>EF"G�� H:��IJKL����MIJ�NO�KLP��?QR-. wide QRS tachycardia �%& S?�:VT P Vf MET-.UVWMG�� S�!XYZ["7\8]T�^[_Y�EPS��`a_Y5b? � cd�: 2efg� EPS"��� 3h�7<ijkl�mnop�qMrst�#uv�7<=>MwE��� 7<x�/yz�wE���4� ��o{�|+"}.+,W7<=> �sus-tained VT� P~+,W7<=> �nonsutaiend VT;NSVT� �wE������ ��7�kl �burst kl� �mn AF� 7���� 3����<W=>�wE������ -�A�� �� ��"%&��=�EF������� 3�d�? AFET�������t"}���� � � op�q�rst�#uv� VTM��[yz���W�/��wE��S??� ��M���?/ 1$���M���NO��� ��.S??� wide
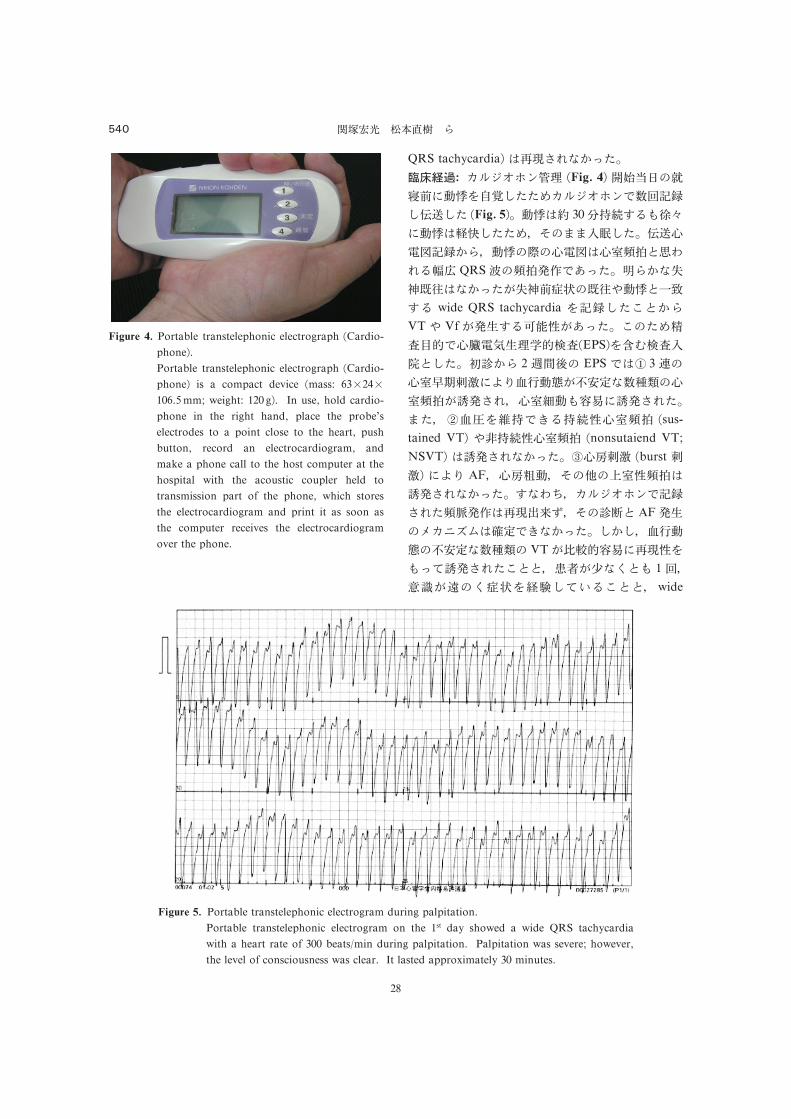
Figure 4. Portable transtelephonic electrograph �Cardio-phone�.Portable transtelephonic electrograph �Cardio-phone� is a compact device �mass: 63�24�106.5mm; weight: 120 g�. In use, hold cardio-phone in the right hand, place the probe’s
electrodes to a point close to the heart, push
button, record an electrocardiogram, and
make a phone call to the host computer at the
hospital with the acoustic coupler held to
transmission part of the phone, which stores
the electrocardiogram and print it as soon as
the computer receives the electrocardiogram
over the phone.
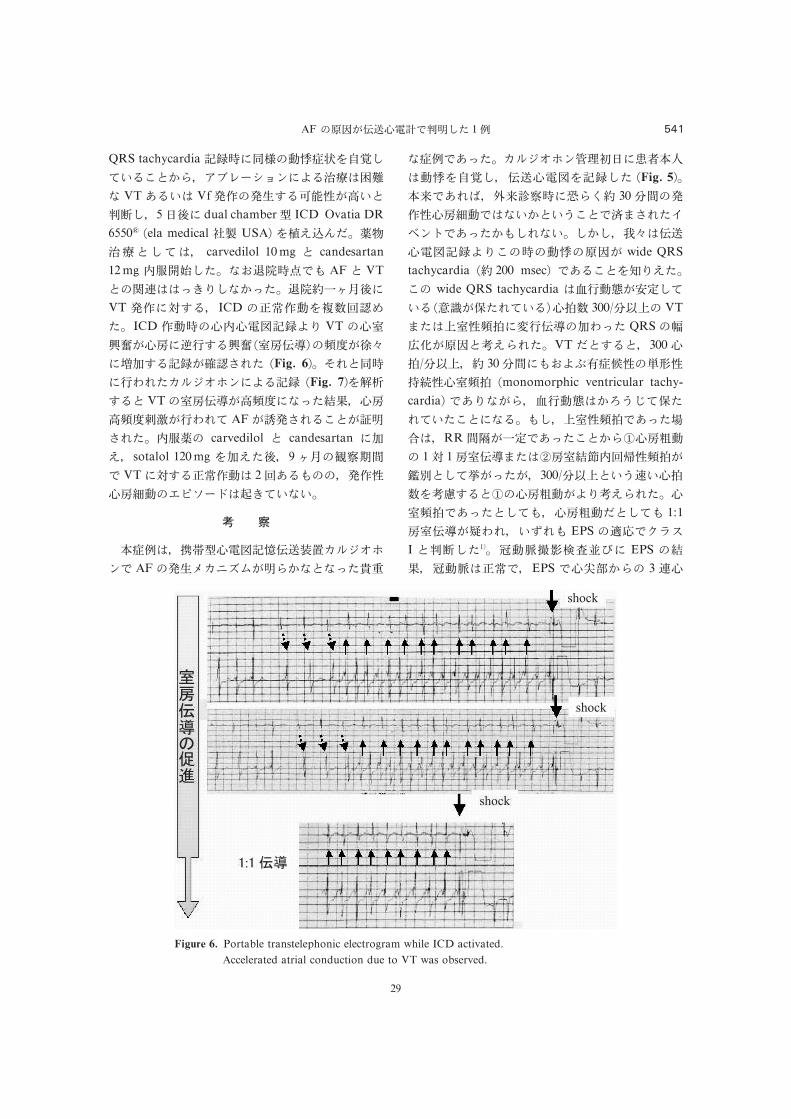
Figure 5. Portable transtelephonic electrogram during palpitation.
Portable transtelephonic electrogram on the 1st day showed a wide QRS tachycardia
with a heart rate of 300 beats�min during palpitation. Palpitation was severe; however,the level of consciousness was clear. It lasted approximately 30 minutes.
���� � ¡¢ :540
28
QRS tachycardia ������������� ������� ��������������� VT!��� Vf�"��#$�%�&'(���)�� 5�*� dual chamber+ ICD Ovatia DR6550� �ela medical ,- USA� ./012� ���� �� carvedilol 10mg � candesartan
12mg 3�45�6� 789�:;< AF� VT��=���>?@� �>6� 89 ABC*�VT �"�D$�� ICD �EF"��GH�I6� ICD "���J3JKL���@ VT �JMN�'J��OP$�N� �M�QR���S'T��UV$���'W�XY6 �Fig. 6�� ZY����P[Y6\]^_`������ �Fig. 7�ab$�� VT�M�QR'(�S� >6cd� J�(�Sef'P[Y AF'��XY���'g�XY6� 3�� carvedilol � candesartan �V/� sotalol 120mg V/6*� 9BC�hijk; VT�D$�EF"�� 2H!�<��� �"&J�l��mno�p�q? � ��
� �
����� rs+JKL�tQuvw\]^_`�; AF��#x\yz{'��� � >6|}
��;!>6� \]^_`�~�������������� QuJKL���6 �Fig. 5����;!Y�� ���i����� 30�k��"&J�l�;� �������;��XY6����;!>6�<�Y �� ���� ���QuJKL���@���������' wide QRStachycardia � 200 msec� ;!����@/6��� wide QRS tachycardia ��P��'��� �� ���'�6Y ���J�G 300����� VT�6��M&����PQR�V[>6 QRS����'����/�Y6� VT2�$��� 300J������ 30�k�<7�����&�� &¡¢&JM�� �monomorphic ventricular tachy-cardia� ;!@ '�� �P����£�¤ �6Y �6��� �� <�� �M&��;!>6¥¦�� RRk§'A�;!>6������J�¨�� 1D 1�MQR�6����Mc©3Hª&��'«��� ¬'>6'� 300��������J�G� $�����J�¨�'�@�/�Y6� JM��;!>6�� <� J�¨�2�� < 1:1�MQR'®[Y� �¯Y< EPS �°±;²³´I ��)�61�� µ�!¶·¸¹"º� EPS �cd� µ�!�EF;� EPS ;J»#��� 3 �J
Figure 6. Portable transtelephonic electrogram while ICD activated.
Accelerated atrial conduction due to VT was observed.
AF ���'QuJK¼;���6 1� 541
29
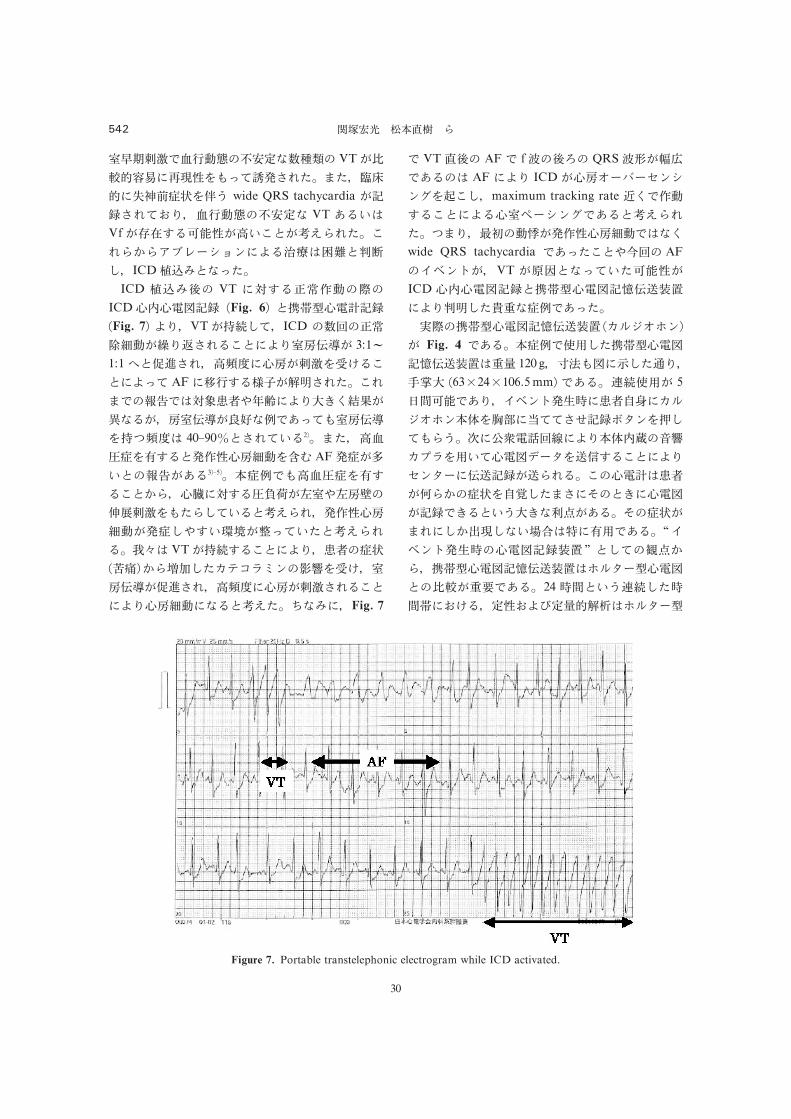
�������������� � VT������������������ ��� ������ !"��# wide QRS tachycardia �$ ���%&� ������� VT '()*Vf ��+,(-���.)/0�123��� /�34356789:;�<(=�*>�0��?� ICD@AB0����ICD @ABC VT ��,(DEF�GICDH�H�I$ �Fig. 6� 0J�KH�L$ �Fig. 7� <&� VT�M�?�� ICD �NDEOP��Q&���(/0�<&����� 3:1�1:1R0ST��� .���H�����UV(/0�<�� AF�W�,(�X�Y ���� /���!Z�*�[\]^"#�<&$_`ab�c�(�� �����%d�&�'��������Me��* 40�90�0���)(2�� ��� .�f!�',(0F�H�P��gh AF!�()0!Z�'(3��5�� )!&��.�f!�',(/043� Hi��,(f*j�k�^k�+l,�����3?�)(0123�� F�H�P��!?^,)mn�o��)�0123�(� p�* VT�M�,(/0�<&� \]!"�q-�43rs?�tuvwx;yz�UV� �����ST��� .���H������(/0�<&H�P���(012�� {�B�� Fig. 7
� VT.C AF� f/C| QRS/}�0~�'(* AF�<& ICD�H��8�8�;9;���/?� maximum tracking rate �`�F�,(/0�<(H��89;��'(0123��� e�&� ���1�F�H�P��*�`wide QRS tachycardia �'��/0^�N AF��;��� VT ���0���)�-���ICD H�H�I$ 0J�KH�I$����2�<&� ?����!&�'����GJ�KH�I$����2 �t����;�
� Fig. 4 �'(� )!&��3?�J�KH�I$����2*�4 120 g� �5�I��?�6&���$ �63�24�106.5mm� �'(� 7��3� 58�-��'&� ��;����\]� �t����;)9�¡:�;���¢$ £¤;�¥?��3#� ¦�§¨�<N©�<&)9�ª«zt¬w�3)�H�I8¤��®,(/0�<&�;¤8���$ ��3�(� /H�L*\]�¯34!"��°?����±0_�H�I�$ �_(0)#$_�=>�'(� ±!"����?4²�?�)³´*?�'3�'(� “��;���H�I$ �2” 0?�µ>43� J�KH�I$����2*��¤8KH�I0����@�'(� 24 ��0)#7�?�����%V(� ��%<¶�4�Y·*��¤8K
Figure 7. Portable transtelephonic electrogram while ICD activated.
¸A¹º »).¼ 3542
30
�������������� �� ����������������� ����� �ST-T ���������� ����������������� !�"��� #����$%��&'���()*+� ,������-./�0�1��2���"��.��23�� 45� 6�' �789�()*+� �6 ��:��,�����;<'=�()�>�� ,����$�?!"#$@AB#��:�'C%D) 56 �&� 'E 2.3 F��� �����GHC%D�IJ)"�� 36�J)6�� K)� (��>7��,����$�?!"#$'#)LM)NO 147F�)*PQR9@�(/� 45@������L!)��� 62F����'EG�+� 42.2�J)� S!@�(/� DiMarcoJP and Philbrick JT8� @A!T)*� .KU�VW"X.)YZ6�@����� ������[\����G�+�'E 22���>(/U�� ��]^���_U��"��� ,����$�?!"#$�PQR9������G�+�`U2��,I��K)� ab-�cd� .@#����$���e/C%���f0g-h�6",����$�?!"#$�1��i�2��23L!)�1�j�4*I klT� mn�5o(�Up
q�rstu� m6;v@wUwx7� 89�yz{��:|�*}��~j�8U��l !)��;� <�=>�U�? �� !�U2��!"��$�%��C%I �6@��K�@���J/U�U2�� �p9�8A�{���'B�(��CD��� %��OD��8��L!/U�� (I(� S!��@�EFG��H�L!/U��I@�U/����b�PQR9�J�K�@A�i��L�2���6 "��L!)�
����
�F���� ,����$�?!"#$� VT�AF�C%�&� ��6;��/@A���2�'�()M��@����6 '��(�
�@S�6 ��E� �N¡�@&/"� OF¢P!Q@AJ/ AF��(��£'��()¤¥�6 J)��>()�2�,����$�?!"#$�� �cd����M��&� �� 2Rm¡�SI "A��B� ���T¦�§UL!�#$�2��V�()�
����
1� ��¨©ª¡z �M��E� �NGH@v��«P¬tPR� 2004�2005W +X®Y�>� Circ J 2006; 70 �Suppl. VI�; 1391�1462.
2� Josephson ME. Clinical Cardiac Electrophysi-ology, 2nd ed. Philadelphia � London, Lea &Febiger, 1993.
3� Kannel WB, Abbott RD, Savarge DD andMcNamara PM. Epidemiologic features of
chronic atrial fibrillation: The Framingham
Study. N Engl J Med 1982; 306: 1018�1022.4� Wolf PA, Benjmin EJ, Belanger AJ, KannelWB, Levy D and D[Agostino RB. Secular
trends in the prevalence of atrial fibrillation,
the Framingham Study. Am Heart J 1996; 131:
790�795.5� ��¨©ª¡z ��P¯)�6 �Z[�«P¬tPR� 2005W +X®Y�>� Circ J 2006.
6� Shimada M, Akaishi M, Asakura K, Baba A,Iwanaga S, Asakura Y, Miyazaki T, Mitamura
H and Ogawa S. Usefulness of the newly
developed transtelephonic electrocardiogram
and computer-supported response system. J
Cardiol 1996; 27: 211�217.7� °±A\� ²]^{� ²]_�`� &abc�]d³� e]´µ� ¶·f� ·¸g¹: )*'ºh���6 @�»�#�Y¼�������=���� M��®� 2003; 80: 1945�1949.
8� DiMarco JP and Philbrick JT. Use of ambula-tory electrocardiographic �Holter� monitoring.Ann Intern Med 1990; 113: 53�68.
AF �[\�!"���V�() 1 543
31

Abstract
Portable Transtelephonic Electrograph Identified
the Underlying Cause of Atrial Fibrillation
Hiromitsu Sekizuka1, Naoki Matsumoto2, Yukako Ishikawa1, Kihei Yoneyama1,
Satoshi Nishio1, Yoshiyuki Watanabe1, Shounosuke Ryu1, Keizou Osada1,
Ryouji Kishi1, Emi Nakano3, Hisao Matsuda3, Tomoo Harada3,
and Fumihiko Miyake1
A 45-year-old male felt faint while driving around 10:00 o[clock on October 12; after that, he su#ered
from palpitation. He was diagnosed as having atrial fibrillation �AF� from the results of 12-lead electrocar-diography performed at the clinic near his house. He was referred to our hospital. From October 15, the
patient started to use portable transtelephonic electrograph �PTE�. On the same day, PTE recorded andtransmitted the electrocardiograms several times due to palpitation occurring before sleep. After he was
relieved from approximately 30-minute palpitation, he went to sleep. PTE showed prolonged QRS duration
during palpitation. He had no history of syncope. However, he felt faint while driving. Accordingly, he was
suspected as having ventricular tachycardia �VT� and was admitted to our hospital for electrophysiologicalstudy �EPS�. On October 25, EPS induced sustained VT. On October 30, the dual chamber implantablecardioverter defibrillator �ICD� was implanted. At this point, the relationship between AF and VT was notfully clarified. After admission, ICD was frequently used due to VT. The intracardiac electrocardiograms
showed greater intraventricular conduction shortening with increased pacing output. PTE, which was
recorded at the same time, demonstrated the onset of AF after nonsustained VT. We concluded that a
shorter intraventricular conduction time with increased pacing output triggered AF.
1 Division of Cardiology, St. Marianna University School of Medicine2 Division of Pharmacology, St. Marianna University School of Medicine3 Division of Cardiology, Kawasaki Municipal Tama Hospital
���� ���� 544
32