7/100,000 30% of all lymphomas male predominance heterogeneous group of tumors consisting of...
TRANSCRIPT

DLBCL

DLBCL
7/100,00030% of all lymphomas male predominanceheterogeneous group of tumors
consisting of large, transformed B-cells with prominent nucleoli and basophilic cytoplasm, a diffuse growth pattern and a high (>40 percent) proliferation fraction
60% advanced at presentationBM in 30%; EN 40%


DLBCL
tumor cells in DLBCL generally express pan B-cell antigens (CD19, CD20, CD22, CD79a), as well as CD45, along with monoclonal surface membrane IgM; occasionally other heavy chain isotypes are present.
Ki 67: > 40%70% BCL-625-80% BCL-2T(14;18) 30%; cmyc translocation 5-
15%

Large cell lymphoma: distinct clinical pathologic subtypes
T cell rich large B cell lymphomaPrimary diffuse large B-cell
lymphoma of the mediastinum, also called primary mediastinal large B-cell lymphoma
Intravascular lymphomaLymphomatoid granulomatosis, an
Epstein-Barr virus (EBV) positive large B-cell lymphoma

Primary Mediastinal DLBCL
7% of large B cellThymic B cell originCo-express weakly CD30Female predominance 4th decadePresents with massive mediastinal
disease, sometimes with SVC syndrome
Good prognosisGEP similar to HD

Case
59 y.o lawyer referred for 20 lb weight loss over 3 months, night sweats and new axillary adenopathy. Previously healthy. Grew up on a farm. Non smoker. No family history. Married with 2 kids in university
On exam: looks unwell. Palpable 2-3 cm nodes in axillae, supraclavicular and inguinal regions
Labs: Hgb 120 g/L, LDH 400 CT scans and excisional biopsy ensue

Diffuse Large B cell Lymphoma (Aggressive)
John


John gets staged…..
CT scans of abdomen and pelvis: retroperitoneal nodes and mesenteric nodes
Bone marrow aspirate and biopsy: negative
Gallium scan: gallium avid disease above and below the diaphragm in sites of nodal enlargement
HIV negativeStage IIIA

He has many questions….
How common is this cancer?What does his sub-type mean?What causes it? Are his kids at risk?What is his prognosis?What treatments are available?Can we predict if he will relapse?What if he does relapse?

Current Incidence and Mortality
Table 1Estimated New Cases and Deaths for Cancer Sites by Sex,Canada - 2005

He has many questions….
What causes it? Are his kids at risk?
What is his prognosis?What treatments are available?Can we predict if he will relapse?What if he does relapse?

Etiology Familial/Genetic (RR=2-3)
Cancer susceptibility genes Immunosuppression
acquired▪ AIDS (100x), post transplant (30-50x)
congenital▪ SCID, CVI, Wiskott Aldrich, AT
Viral: HIV, HTLV-1(5%), EBV, HHV8, Hepatitis C
Bacterial: H Pylori (6X)
Etiology Continued
Occupational Phenoxyacetic acid herbicides Farmers: organophosphate insecticides Fertilizers solvents
Social Increased diet of animal protein, fat and
meat Hair dyes

He has many questions….
What causes it? Are his kids at risk?
What is his prognosis?What treatments are available?Can we predict if he will relapse?What if he does relapse?

International Prognostic Factor Index (IPI)

Factors Included Patients of all ages
Age >=60 LDH > normal Performance status
2-4 Ann Arbor stage III-
IV Extra-nodal
involvement (>1 site)
Age adjusted Stage LDH Performance status

DLBCL: Survival by IPI
Armitage and Weisenburger, 1998

The International Non-Hodgkin's Lymphoma Prognostic Factors Project, N Engl J Med 1993;329:987-994
Outcome According to Risk Group Defined by the International Index and the Age-Adjusted International Index

Biologic Factors
BadKi-67P53CD5+LDHB-2-
microglobulinC-reactive
proteinBCL-2C-mycSurvivinCyclin D2
GoodCD10BCL-6CD40

5 yr OS
CD10 negative positive
44%74%
Bcl-6negativepositive
30%69%
Cyclin D2Negativepositive
58%11%
MUM 1negativepostive
66%36%
TMAGCB
Non-GCB76%34%
Hans, C. P. et al. Blood
2004;103:275-282

Rosenwald, A. et al. N Engl J Med 2002;346:1937-1947
Subgroups of Diffuse Large-B-Cell Lymphoma According to cDNA Gene-Expression Profiles

Copyright ©2004 American Society of Hematology. Copyright restrictions may apply.
Hans, C. P. et al. Blood 2004;103:275-282
Figure 2. Results of immunoperoxidase staining
They found that the GCB and non-GCB subtypes of DLBCL could be accurately predicted using a panel of only 3 immunostains

Copyright ©2004 American Society of Hematology. Copyright restrictions may apply.
Hans, C. P. et al. Blood 2004;103:275-282
Figure 1. Decision tree for immunoperoxidase TMA classification of DLBCL

Lymph node IHC
CD20+ BCL2+ BCL6+ CD10+ Ki67+ 50% CD5- CD23- Cyclin D1-
John Has GCB-type DLBCL

He has many questions….
What is his prognosis?What treatments are available?Can we predict if he will relapse?What if he does relapse?

CHOP or CHOP-like chemotherapy is the mainstay chemotherapy treatment for large cell lymphomas
Q 3 week cycles6-8 cyclesCyclophosphamide 750 mg/m2 Adriamycin: 50 mg/m2 day 1Vincristine 1.4 mg/m2 IV day 1Prednisone 100 mg po daily x 5
days

Fisher, R. I. et al. N Engl J Med 1993;328:1002-1006
Overall Survival in the Treatment Groups

Copyright © American Society of Clinical Oncology
Coiffier, B. J Clin Oncol; 23:6387-6393 2005
Fig 1. (A) Event-free survival, (B) progression-free survival, and (C) overall survival with a median follow-up of 5 years in CHOP (cyclophosphamide,
doxorubicin, vincristine, prednisone) and R-CHOP (rituximab-CHOP) -treated patients in the LNH-98.5 study
28%
50%

Copyright © American Society of Clinical Oncology
Coiffier, B. J Clin Oncol; 23:6387-6393 2005
Low Risk
0-1
High risk
2-3

Copyright © American Society of Clinical Oncology
Thieblemont, C. et al. J Clin Oncol; 25:1916-1923 2007
Fig 2. Five-year follow-up results of the Groupe d'Etude des Lymphomes de l'Adulte study in patients 60 to 80 years old comparing cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) with the rituximab plus CHOP (R-CHOP) regimen

Copyright © American Society of Clinical Oncology
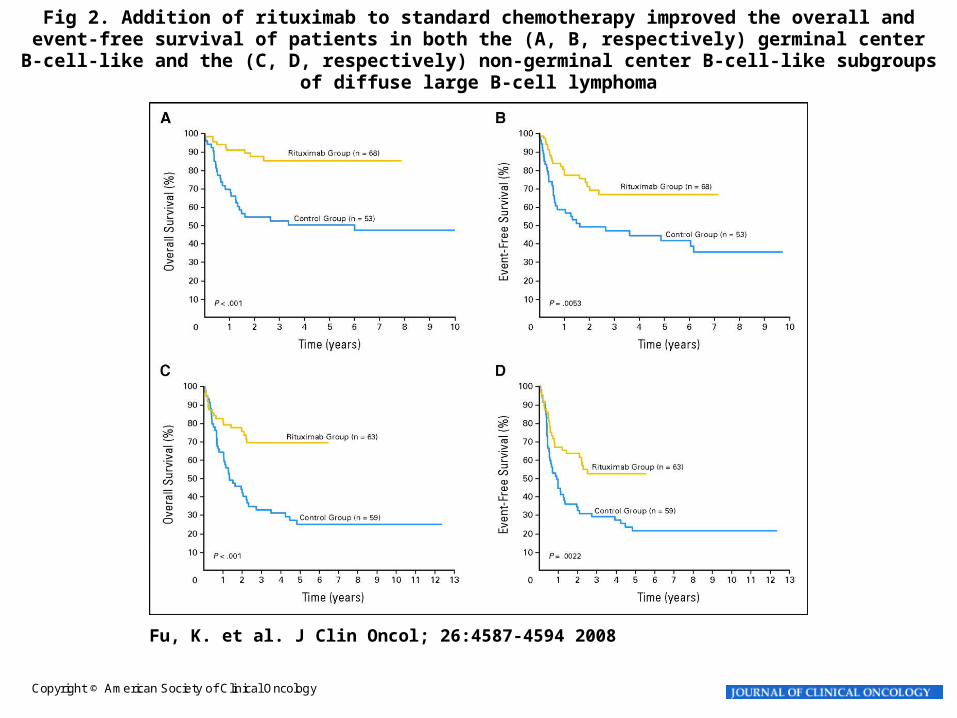
Fu, K. et al. J Clin Oncol; 26:4587-4594 2008
Fig 3. Subclassification on the basis of the cell of origin was predictive of (A) overall and (B) event-free survival in patients with diffuse large B-cell lymphoma who were treated with rituximab plus standard
chemotherapy
Copyright © American Society of Clinical Oncology
Fu, K. et al. J Clin Oncol; 26:4587-4594 2008
Fig 2. Addition of rituximab to standard chemotherapy improved the overall and event-free survival of patients in both the (A, B, respectively) germinal center B-cell-like and the (C, D, respectively) non-
germinal center B-cell-like subgroups of diffuse large B-cell lymphoma

CD20+ DLBCL18-60 years
IPI 0,1Stages II-IV,I with bulk
6 x CHOP-like+ 30-40 Gy (Bulk, E)
6 x CHOP-like+ Rituximab
+ 30-40 Gy (Bulk, E)
Random.
Trial
Design

Chemo(n=411)
R-Chemo(n=413)
Complete remission (CR/CRu) 68%* 86%*
Partial remission (PR) 12% 7%
No change (NC) 4% 1%
Progressive disease (PD) 11%** 4%**
** p=0.0018 (Fisher’s exact test)* p<0.0005 (Fisher’s exact test)
Remission
Rates

R-CHEMO
CHEMO
p < 0.000005crit = 0.00192*
81%
58%
Median time of observation: 24 months
0.0
5 10 15 25 30 35 45 50
0.10.2
0.3
0.40.50.60.7
0.80.9
0
M o n t h s
Pro
bab
ility
FT
F
1.0
20 40
*: -crit for updated interim analysis
Time to Treatment Failure
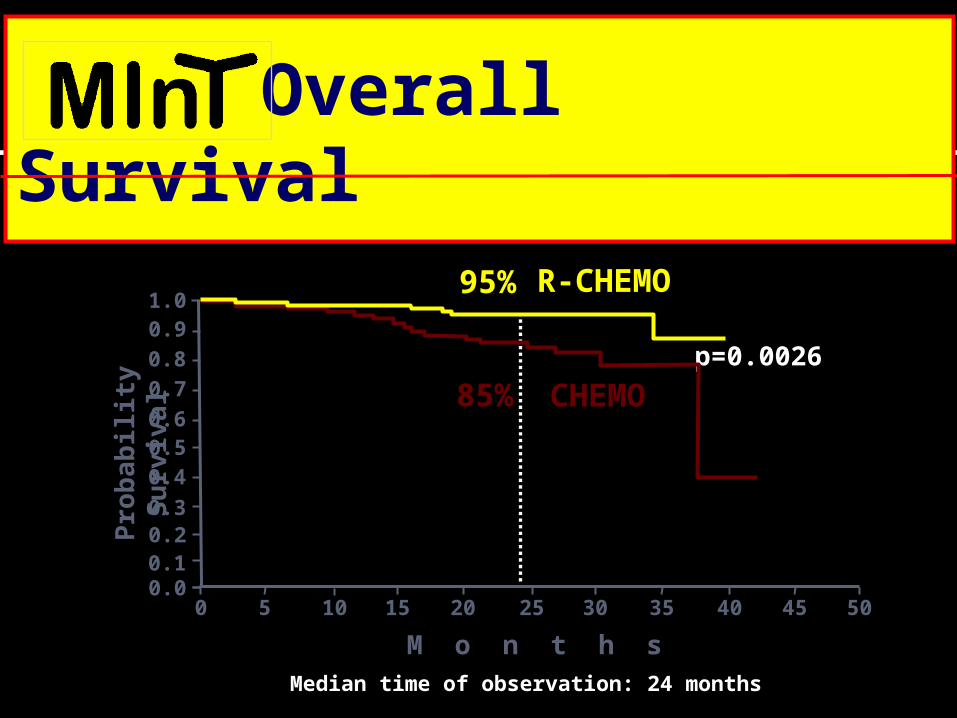
p=0.0026
Median time of observation: 24 months
0.05 10 15 25 30 35 45 50
0.10.20.3
0.40.50.6
0.7
0.8
0.9
0
M o n t h s
Pro
bab
ility
Su
rviv
al
1.0R-CHEMO
CHEMO
20 40
95%
85%
Overall Survival

The standard of care for newly diagnosed large B cell lymphomas is CHOP-R
Improved overall survival of 10-14%
Improved progression-free survival of 20-23%
Well tolerated, safe with no excess increased toxicity
Adds roughly $16,000 extra to cost of CHOP

Should he have 6 or eight cycles of CHOP-R?

Six, not eight cycles of bi-weekly CHOP with rituximab (R-CHOP-14) is the preferred treatment for elderly patients with DLBCL: results of the
RICOVER-60 trial of the German High-Grade Non-Hodgkin Lymphoma
Study Group (DSHNHL)
RICOVER 60
M. Pfreundschuh, M. Kloess, R. Schmits, S. Zeynalova, E. Lengenfelder, A. Franke, H. Steinhauer, M. Reiser, M. Clemens, C. Nickenig, M. de Wit, A. Ho, H. Eimermacher, L. Truemper, M. Hoffmann, R. Mertelsmann, B.
Metzner, H. Mergenthaler, R. Liersch, U. Duehrsen, L. Balleisen, F. Hartmann, V. Poeschel, N. Schmitz, M. Loeffler for the DSHNHL

Questions addressed
• Can CHOP-14 be improved by
rituximab?
• Are 8 cycles better than 6?
RICOVER 60:
objectives

CD20+ DLBCL
stages I–IV
61–80 years
Random2x2
Factorialdesign
RICOVER 60: trial design
6 x CHOP-14+ 36 Gy (Bulk, E)
8 x CHOP-14+ 36 Gy (Bulk, E)
6 x CHOP-14+ 36 Gy (Bulk, E)
+ 8 x rituximab
8 x CHOP-14+ 36 Gy (Bulk, E)
+ 8 x rituximab
8 doses of rituximab regardless ofnumber of cycles of chemotherapy

CHOP-14 vs R-CHOP-14
Fai
lure
-fre
e su
rviv
al (
%)
8 x (R)-CHOP-14(n=415)
6 x (R)-CHOP-14(n=413)
p=0.000025 -crit* = 0.031
57%
70%64%
62%
p=0.23
Fai
lure
-fre
e su
rviv
al (
%)
100
80
60
40
20
0
100
80
60
40
20
0
6/8 x R-CHOP-14(n=414)
6/8 x CHOP-14(n=414)
0 5 10 15 20 25 30 35 40 45 0 5 10 15 20 25 30 35 40 45
Months Months
6 cycles vs 8 cycles
RICOVER 60: time to treatment failure
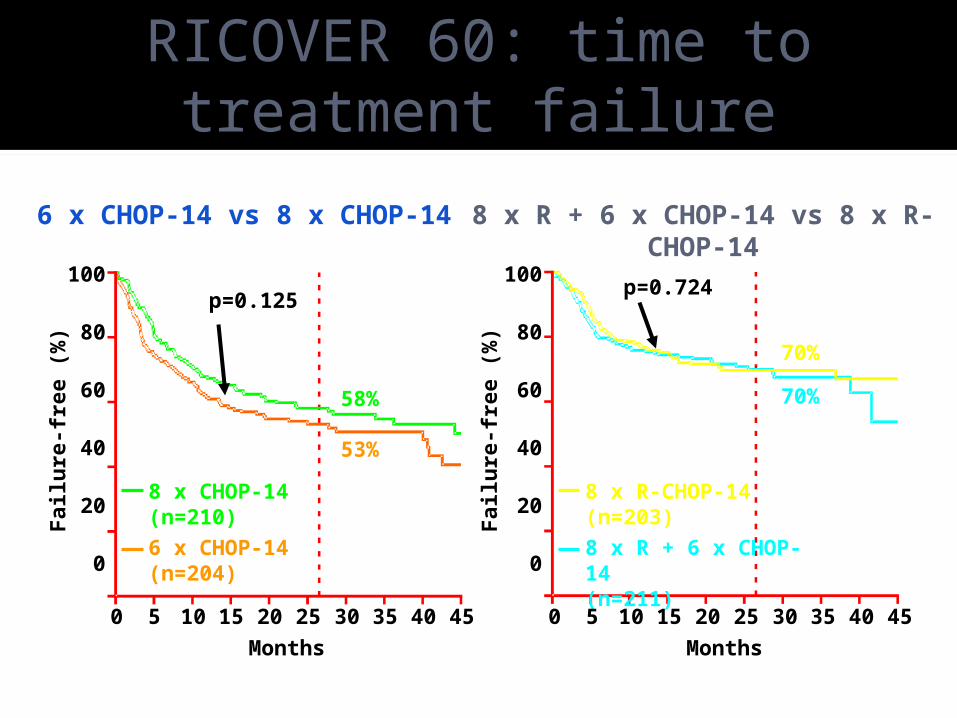
53%
58%
p=0.125p=0.724
70%
70%
8 x R + 6 x CHOP-14 vs 8 x R-CHOP-14
100
80
60
40
20
0
0 5 10 15 20 25 30 35 40 45
Months
Fai
lure
-fre
e (%
)
8 x CHOP-14(n=210)
6 x CHOP-14(n=204)
Fai
lure
-fre
e (%
)
100
80
60
40
20
0
8 x R-CHOP-14(n=203)
8 x R + 6 x CHOP-14(n=211)
0 5 10 15 20 25 30 35 40 45
Months
6 x CHOP-14 vs 8 x CHOP-14
RICOVER 60: time to treatment failure

Median time of observation: 26 months
Su
rviv
ing
(%
)
100
80
60
40
20
0
0 5 10 15 20 25 30 35 4045 Months
6 x CHOP-14 (n=204)8 x R + 6 x CHOP-14 (n=211)8 x CHOP-14 (n=210)8 x R-CHOP-14 (n=203)
RICOVER 60: survival

Case
Should He Have Maintenance Therapy?

ECOG 4494 Phase III Trial:
R-CHOP v CHOP +/- MR
RANDOMIZED
Stratified by IPI(0-1 vs 2-4)
CHOP
1 2 3cycle 4 5 6 7 8
Rituximab
RANDOMIZED
Stratified by IPICR/PR; Induction
Maintenance Rituximab
(MR) q 6 m x 2 yr
Observation
(N=632) (N=415)1 2 3cycl
e 4 5 6 7 8

Outcome According toInduction and Maintenance Therapy
Treatment 2 year FFS* 2 year OS
R-CHOP + MR 79% 87%
R-CHOP + OBS 77% 85%
CHOP + MR 74% 83%
CHOP + OBS 45% 72%
* Significant FFS interaction (HR=2.10, p=0.05) This is the data on responding patients.

You recommend 6 cycles of CHOP-R……

You repeat his CT scans and he is in complete remission after his chemotherapy

He has many questions….
How common is this cancer?What does his sub-type mean?What causes it? Are his kids at risk?What is his prognosis?What treatments are available?Can we predict if he will relapse?What if he does relapse?

Copyright © American Society of Clinical Oncology
Spaepen, K. et al. J Clin Oncol; 19:414-419 2001
Fig 4. Kaplan-Meier estimate of PFS in 26 patients with a positive [18F]FDG-PET after therapy compared with 67
patients with a negative [18F]FDG-PET after therapy
N=26
N=67

Copyright © American Society of Clinical Oncology
Spaepen, K. et al. J Clin Oncol; 19:414-419 2001
Fig 2. Prognostic value of [18F]FDG-PET scan in a patient with presumed CR on CDM. Residual FDG-uptake cervical (left) and mesenteric (right). Patient relapsed after 838 days; a cervical biopsy was positive for NHL

Case continued……
John returns to workHe is followed every 3 months for
the first 2 yearsAt his 18 month visit, he complains
of a new 2 cm neck nodeAn excisional biopsy confirms
DLBCL identical to initial biopsyOn re-staging, he is found to be
stage IIA, IPI LI

What do we do now?
Options: Salvage chemotherapy
Cisplatin or gemcitabine based Salvage chemotherapy followed by
ASCT 25% chance of 2 year disease free survival
Palliative radiation or low dose chemotherapy Survival 6 months
Rituxan alone Overall response 35%; time to progression 2
months Radioimmunoconjugates

His best bet is high dose chemotherapy
Autologous
Allogeneic
Availability 90% 25%
Exploits dose-response
yes yes
Graft vs. lymphoma
no yes
Graft vs. Host no yes
Graft contamination
likely no
Treatment Related Mortality
2-5% 20-30%
Curative 30% 50%

Philip, T. et al. N Engl J Med 1995;333:1540-1545
Kaplan-Meier Curves for Event-free Survival of Patients in the Transplantation and Conventional-Treatment Groups

Philip, T. et al. N Engl J Med 1995;333:1540-1545
Kaplan-Meier Curves for Overall Survival of Patients in the Transplantation and Conventional-Treatment Groups

Rituximab Plus AuHCT in Patients With DLBCL
Fenske TS, et al. ASH 2007. Abstract 19.
Patients with DLBCL in GBMTR database,
1996-2003
(N = 1006)
Rituximab within 3 months of AuHCT
(n = 188)AuHCT
No Rituximabwithin 3 months of AuHCT
(n = 818)Characteristic Rituximab
(n = 188)No Rituximab
(n = 818)P Value
Median age, yrs (range) 58 (20-76) 52 (18-75) < .001
Karnofsky performance score < 90%, % 39 37 .52
Largest mass size ≥ 5 cm before AuHCT, % 28 35 .28
> 2 chemotherapy regimens given, % 56 40 < .001
Year of AuHCT Between 1996 and 1998 Between 1999 and 2001 Between 2002 and 2003
44749
59347
< .001
Retrospective analysis

Rituximab Plus AuHCT in Patients With DLBCL
Fenske TS, et al. ASH 2007. Abstract 19.
Progression-Free Survival
Per
cen
tag
e o
f P
atie
nts
Rituximab (n = 188) No Rituximab (n = 818)
Overall Survival
6249
3949
38 32
0
20
40
60
80
100
Year 1
P = .002P = .01
P = .16
Year 3 Year 5
6857
4860
45 40
P = .032P = .003
P = .13
Year 1 Year 3 Year 50
20
40
60
80
100

What if he had presented with localized disease at diagnosis (stage 1-2)?

Limited stage DLBCL
Study N Design PFS (p value) OS (p value)
Miller NEJM 1998
401 CHOP x 3 + IF RTCHOP x 8
77%64% (.03)
82%72% (.02)
BonnetJCO 2007
576 (age > 60)
CHOP x 4CHOP x 4 + IF RT
61%64% (NS)
72%68% (NS)
ReyesNEJM 2005
648(age < 61)
CHOP x 3 + IF RTACVBP + Seq consolidation
74%82%(<.001)
81%90%(.001)

Copyright © American Society of Clinical Oncology
Persky, D. O. et al. J Clin Oncol; 26:2258-2263 2008
Fig 1. (A) Progression-free and (B) overall survival of 60 eligible patients enrolled in a Southwest Oncology Group (SWOG) trial of three cycles of R-CHOP followed by involved-field radiation therapy

Copyright © American Society of Clinical Oncology
Persky, D. O. et al. J Clin Oncol; 26:2258-2263 2008
Fig 3. Overall survival of 60 eligible patients receiving R-CHOP(3) plus IFRT (from S0014) is compared with that of 68 eligible patients receiving CHOP(3) plus IFRT (from S8736), matched for limited disease,
aggressive B-cell histologies, and presence of at least one stage-modified International Prognostic Index (IPI) risk factor
Stage Modified IPI: age, stage 2, LDH and ECOG

Conclusions: limited stage IPI
CHOP-R x 3 + IF RTPatients with more than 1 RF on
stage modified IPI might do as well with chemo alone x 6-8 cycles
This excludes bulky diseaseNo benefit to IF rads if 6-8 cycles
chemo
New agents and approaches
RadioimmunotherapyProtein Kinase-C inhibitorsVelcadeAngiogenesis InhibitorsAnti-BCL-2RevlimidGaliximab and epratuzumabNewer humanized RituxanEPOCH-R

Current or Pending Aggressive NHL Trials at Sunnybrook
LY-11: RCT of CHOP-r x 8 vs. CHOP-R x 6 then ASCT in newly diagnosed age < 65 with DLBCL with 2-3 aaIPI factors
Ly-12: RCT of R-DHAP vs. R-GDP in relapsed DLBCL or transformed NHL f/B ASCT then 2nd randomization to R maintenance or observation
Sunitinib in relapsed DLBCL or primary mediastinal large cell NHL (pending)
Risk stratification by PET scans with modified therapy?

Summary
NHL is the fifth most common cancer Large cell lymphoma comprises 30% of all
lymphomas Untreated, survival in months 60% are curable today
Rituxan + anthracycline containing chemotherapy standard upfront
New techniques for prognosis and prediction of relapse
High dose chemotherapy and stem cell transplant is recommended for young relapsed patients
The roles of RIT and PET and new agents are emerging
The role of maintenance immunotherapy unknown at this time