cord presentation this occurs when the umbilical cord lies in front of the presenting part, with...
TRANSCRIPT
Presentation and prolapse of the umbilical cord Cord presentation This occurs when the umbilical cord lies
in front of the presenting part, with the fetal membranes still intact.
Cord prolapse
The cord lies in front of the presenting part and the fetal membranes are ruptured
Occult cord prolapse This is said to occur when the cord lies
alongside, but not in front of, the presenting part.

Predisposing factors high parity& High head : High or ill-fitting presenting part: If the membranes rupture
spontaneously when the fetal head is high, a loop of cord may be able to pass between the uterine wall and the fetus resulting in its lying in front of the presenting part
- As the presenting part descends the cord becomes trapped and occluded.

Prematurity
The size of the fetus in relation to the pelvis and the uterus allows the cord to prolapse.
- Babies of very low birth weight (<1500 g) are particularly vulnerable for cord presentation.

Multiparity
The presenting part may not be engaged when the membranes rupture and malpresentation is more common.
Malpresentation -Cord prolapse is associated with breech
presentation, especially complete or footling breech.
-This relates to the ill-fitting nature of the presenting parts and also the proximity of the umbilicus to the buttocks.
- In this situation, the degree of compression may be less than with a cephalic presentation, but there is still a danger of asphyxia.
-Shoulder and compound presentation and transverse lie carry a high risk of prolapse of the cord, occurring with spontaneous rupture of the membranes.
-Face and brow presentations are less common causes of cord prolapse
Multiple pregnancy -Malpresentation, particularly of the
second twin, is more common in multiple pregnancy.
-Polyhydramnios The cord is liable to be swept down in a
gush of liquor if the membranes rupture spontaneously.
-Controlled release of liquor during artificial rupture of the membranes is sometimes performed to try to prevent this.

Cord presentation diagnosis
This is diagnosed on vaginal examination when the cord is felt behind intact membranes.
-It is, however, rarely detected but may be associated with aberrations in fetal heart monitoring such as decelerations, which occur if the cord becomes compressed.


Management Under no circumstances should the
membranes be ruptured. -The midwife should discontinue the
vaginal examination, in order to reduce the risk of rupturing the membranes.
-Medical aid should be summoned. To assess fetal well-being continuous electronic fetal monitoring should be commenced or the fetal heart should be auscultated as continuously as possible.
- The mother should be helped into a position that will reduce the likelihood of cord compression.
-Caesarean section is the most likely outcome.
Cord prolapseDiagnosis Whenever there are factors present that
predispose to cord prolapse a vaginal examination should be performed immediately on spontaneous rupture of membranes.
Bradycardia - variable or prolonged decelerations of
the fetal heart are associated with cord compression

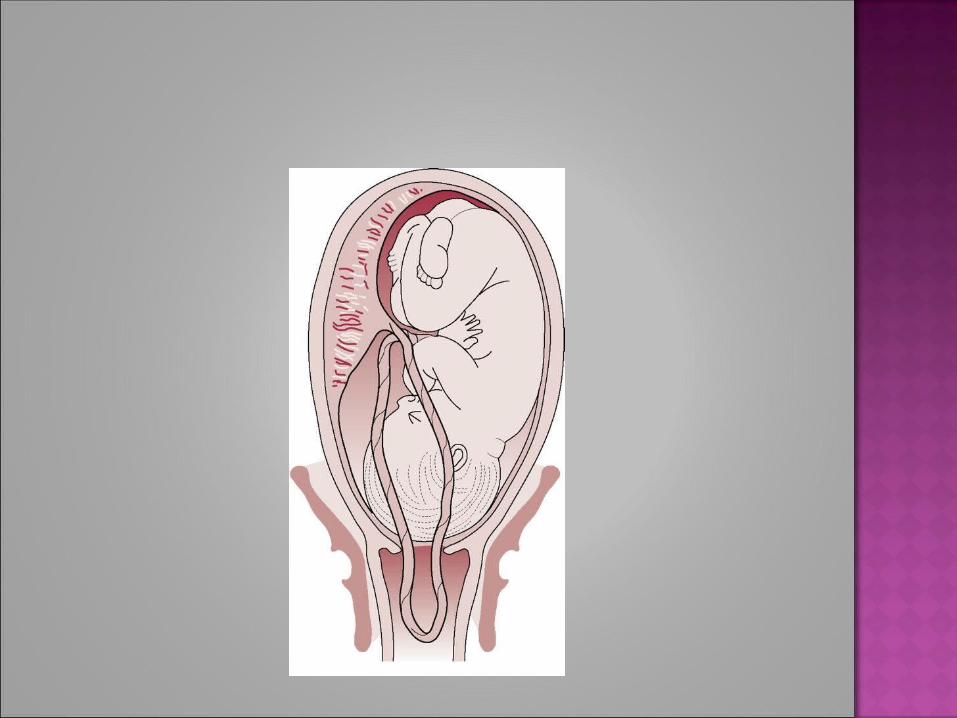
-The diagnosis of cord prolapse is made when the cord is felt below or beside the presenting part on vaginal examination.
-The cord may be felt in the vagina or in the cervical os or a loop of cord may be visible at the vulva
Immediate action the midwife should call for urgent
assistance. - The midwife should explain her
findings and emergency measures that may be needed to the mother and her birth partner.
If an oxytocin infusion is in progress this should be stopped.
- If the cord lies outside the vagina, then it should be gently replaced to oxygenation
prevent spasm to maintain temperature and prevent drying. Administering oxygen to the mother by
face mask at 4 L/min may improve fetal

Knee- chest position

Relieving pressure on the cord -The risks to the fetus are hypoxia and
death as a result of cord compression. -The risks are greatest with prematurity
and low birth weight - The midwife may need to keep her
fingers in the vagina and hold the presenting part off the umbilical cord, especially during a contraction.
-The mother can be helped to change position to further reduce pressure on the cord.

- Raising her pelvis and buttocks or adopting the knee–chest position will cause the fetus to gravitate towards the diaphragm
- The foot of the bed may also be raised (Trendelenburg position) to relieve compression on the cord.
- Alternatively, the mother can be helped to lie on her left side, with a wedge or pillow elevating her hips (exaggerated Sims' position)

-There is some evidence to suggest that bladder filling may also be an effective technique for managing cord prolapse
-A self-retaining 16G Foley catheter is used to instil approximately 500–700 mL of sterile saline into the bladder.
-The full bladder can relieve compression of the cord by elevating the presenting part about 2 cm above the ischial spines
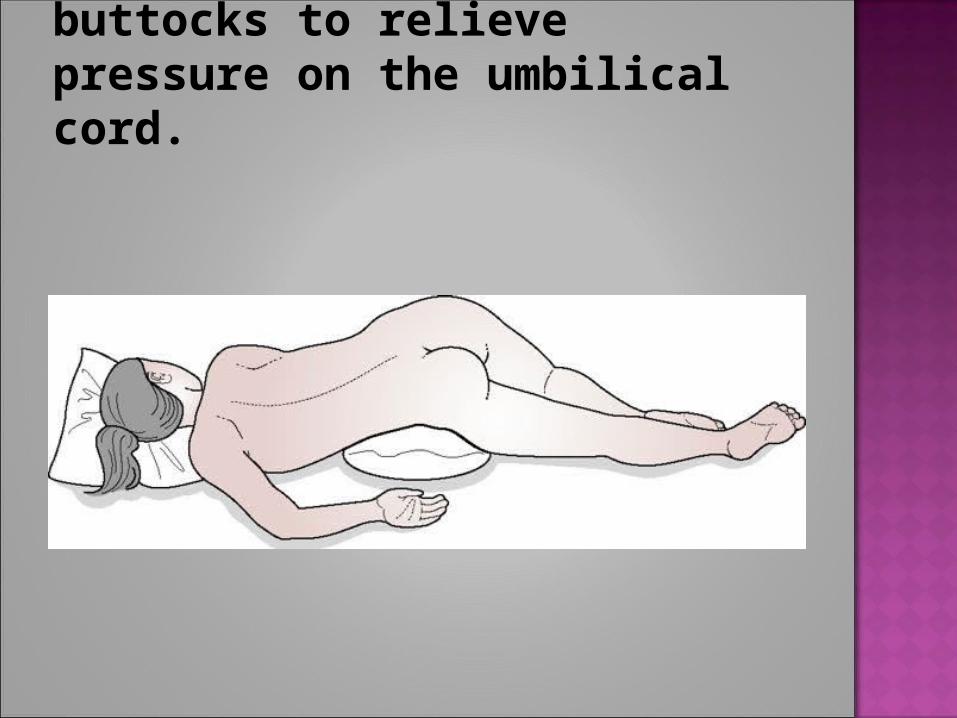
Exaggerated Sims' position. Pillows or wedges are used to elevate the woman's buttocks to relieve pressure on the umbilical cord.

-The bladder would be drained in theatre immediately before delivery.
-Birth must be expedited with the greatest possible speed to reduce the mortality and morbidity associated with this condition.
-Caesarean section is the treatment of choice in those instances where the fetus is still alive and vaginal birth is not imminent.

-If cord prolapse is diagnosed in the second stage of labour, with a multiparous mother, the midwife may perform an episiotomy to expedite the birth.
-Where the presentation is cephalic, assisted birth may be achieved through ventouse or forceps.
-If cord prolapse occurs in the community, emergency transfer to hospital is essential.

- The midwife should carry out the same procedures to relieve the compression on the cord.
-Consultant unit staff should be informed and be prepared to perform an emergency caesarean section.
Thank you