© erw 2011 targeting rumination by changing processing style: experiential and imagery exercises...
TRANSCRIPT

© ERW 2011
Targeting rumination by changing processing
style: Experiential and Imagery exercises
Edward Watkins, PhDUniversity of Exeter
[email protected] 2011

Acknowledgements Research collaborators Mood Disorders Centre co-
directors Dr Celine Baeyens Dr Nick Moberly Professor Willem Kuyken Dr Michelle Moulds Dr Eugene Mullan Rebecca Read Sandra Kennell-Webb All patients and participants Simona Baracaia
Therapy development & trial Dr Katharine Rimes Dr Anna Lavender Dr Janet Wingrove Dr Neil Bathurst Rachel Eastman Professor Jan Scott

Plan of Skills class
Thinking Style and avoidance as key elements driving pathological rumination
A functional-contextual approach – Functional analysis
***Shifting processing mode – Experiential exercises
Video

Why do I feel so bad?
Why did this happen to me?
Why can’t I handle things better?
What does this mean about me?
What am I doing to deserve this?
What will others think of me?
Rumination = recurrent dwelling on feelings, problems, upsetting events, negative aspects of self
Key process in onset and
maintenance of depression &
anxiety

Rumination-focused CBT (RFCBT) RFCBT focuses on increasing effective behaviour
– i.e., not stopping rumination but making it functional
RFBCT grounded within the core principles and techniques of CBT for depression (Beck, Rush, Shaw, &
Emery, 1979) with two adaptations:– a functional-analytical perspective using Behavioural
Activation (BA) approaches (Addis & Martell, 2004; Martell et al., 2001; Watkins, 2009; Watkins et al., 2007; Watkins et al., in press)
– An explicit focus on shifting processing style via imagery and experiential approaches
© ERW 2009
Rumination-focused CBT (RFCBT) 2 Within BA terms, rumination
conceptualized as avoidance (cognitive & actual) that is negatively reinforced (e.g., avoid risk of failure; pre-empt criticism; reduce intensity)
Rumination becomes a learned habitual behaviour
May be reinforced superstitiously, partial reinforcement, poor discrimination helpful thinking (problem-solving) and unhelpful
Rumination-focused CBT (RFCBT) 3 Cues trigger ruminative response automatically
[mood, stress, contexts) Information-giving, thought challenging unlikely to
change a habit Hence treatment only effective if counter-
condition alternative responses to warning signs Hence focus on identification of warning signs
and then repeated practice of an alternative response under mood/stress challenge to develop more functional habit

But dwelling on difficult events is common, normal & often adaptiveWhat determines whether dwelling
on a problem/upset leads to either
gets stuck in a distressing loop that goes nowhere?
constructive resolution, Problem-solving, working through
OR

© ERW 2009
How can I fix this?
What can I learn from this?
What are the positive benefits of this?
What can I do next?
What is important to me now?
How did this happen?
Reduces negative mood & improves planning & problem-solving in experiments
Predicts recovery from upsetting and traumatic events and from depression in some prospective studies
Watkins (2008)– Positive consequences of RT

Rumination-focused CBT (RFCBT) 4 The way that people think during stress and
problems may be part of the learnt habit Either an unhelpful unconstructive processing
style (conceptual, evaluative, existential, abstract, judgemental, passive)
Or a helpful processing style (non-judgemental, non-evaluative, constructive, concrete, action-oriented).
Use experiential exercises and imagery to induce this processing style, as counter to rumination, and as means to develop constructive habit
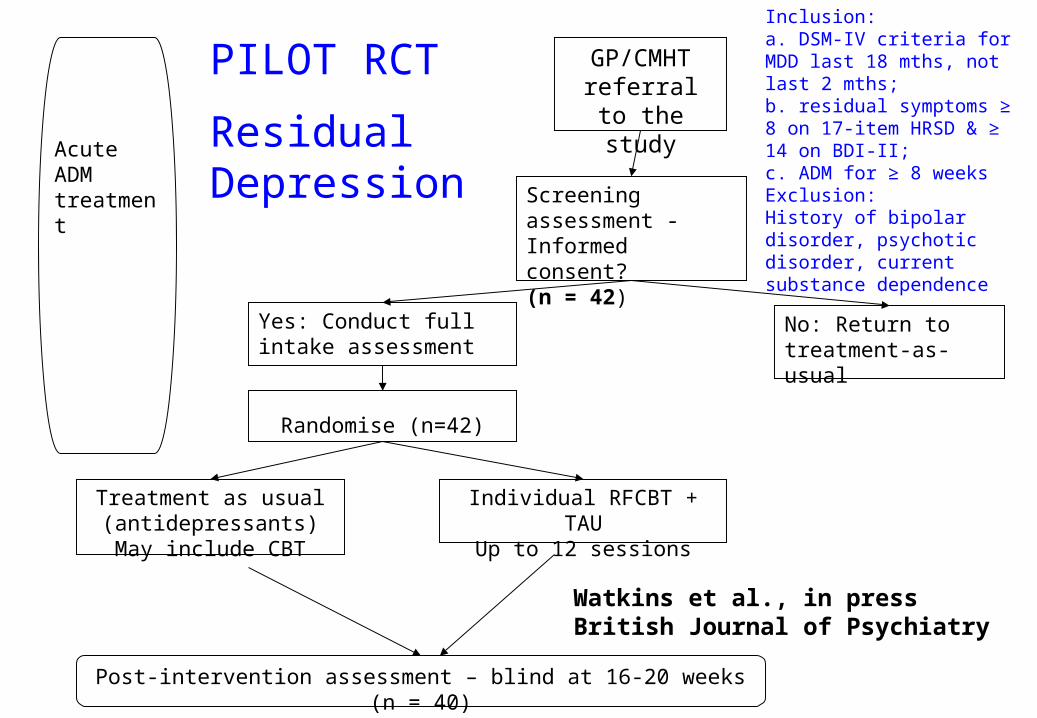
GP/CMHTreferral to the
study
Screening assessment -Informed consent? (n = 42)
No: Return to treatment-as-usual
Yes: Conduct full intake assessment
Acute ADMtreatment
Randomise (n=42)
Treatment as usual (antidepressants)May include CBT
Individual RFCBT + TAUUp to 12 sessions
Post-intervention assessment – blind at 16-20 weeks (n = 40)
PILOT RCT
Residual Depression
Inclusion:a. DSM-IV criteria for MDD last 18 mths, not last 2 mths; b. residual symptoms ≥ 8 on 17-item HRSD & ≥ 14 on BDI-II; c. ADM for ≥ 8 weeksExclusion:History of bipolar disorder, psychotic disorder, current substance dependence
Watkins et al., in press British Journal of Psychiatry
© ERW 2009
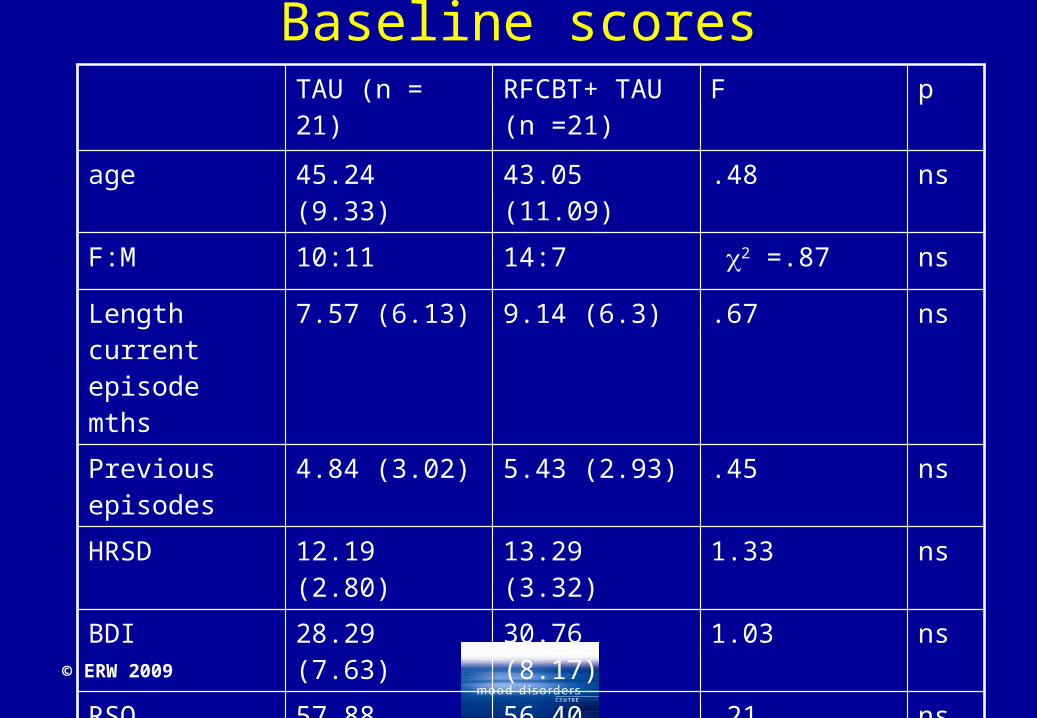
Baseline scoresTAU (n = 21) RFCBT+ TAU
(n =21)F p
age 45.24 (9.33) 43.05 (11.09) .48 ns
F:M 10:11 14:7 2 =.87 ns
Length current episode mths
7.57 (6.13) 9.14 (6.3) .67 ns
Previous episodes
4.84 (3.02) 5.43 (2.93) .45 ns
HRSD 12.19 (2.80) 13.29 (3.32) 1.33 ns
BDI 28.29 (7.63) 30.76 (8.17) 1.03 ns
RSQ 57.88 (8.52) 56.40 (11.92) .21 ns
Axis I diagnoses
1.86 (1.24) 2.05 (0.92) .32 ns
© ERW 2009
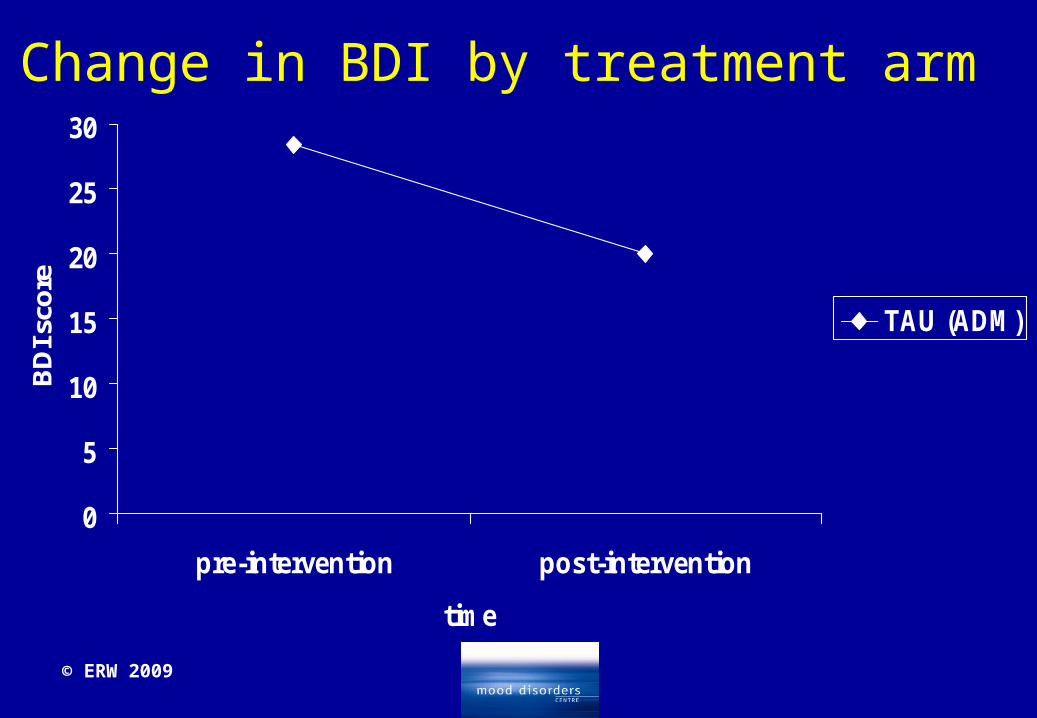
Change in BDI by treatment arm
0
5
10
15
20
25
30
pre-intervention post-intervention
time
BD
I sco
re
TAU (ADM)
© ERW 2009
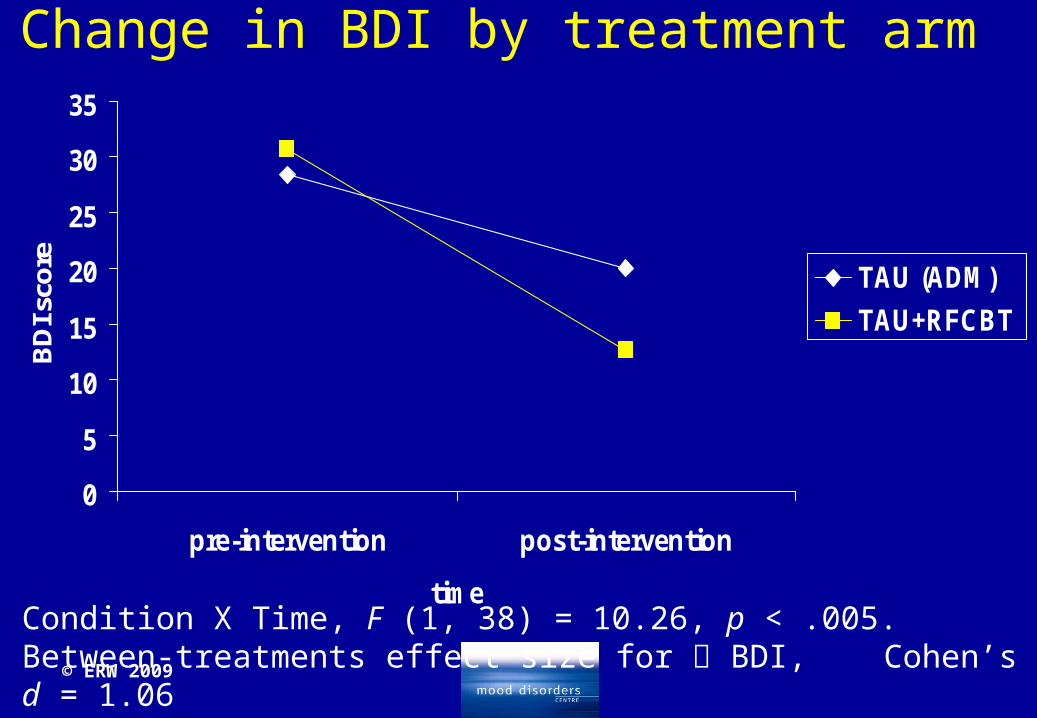
Change in BDI by treatment arm
0
5
10
15
20
25
30
35
pre-intervention post-intervention
time
BD
I sco
re
TAU (ADM)
TAU+RFCBT
Condition X Time, F (1, 38) = 10.26, p < .005. Between-treatments effect size for BDI, Cohen’s d = 1.06

© ERW 2009
Change in BDI by treatment arm –Watkins et al, in press, BJP
0
5
10
15
20
25
30
35
pre-intervention post-intervention
time
BD
I sco
re
TAU (ADM)
TAU+RFCBT
TAU+CBT
TAU-PAYKEL
Condition X Time, F (1, 38) = 10.26, p < .005. Between-treatments effect size for BDI, Cohen’s d = 1.06
RFCBT 12 sessions; CBT 20 sessions

© ERW 2009
Change in HRSD by treatment arm
0
2
4
6
8
10
12
14
pre-intervention post-intervention
time
HR
SD
sco
re
TAU (ADM)
TAU + RFCBT
Condition X Time, F (1, 38) = 7.38, p < .01. Between-treatments effect size for HRSD, Cohen’s d = 0.895
© ERW 2009
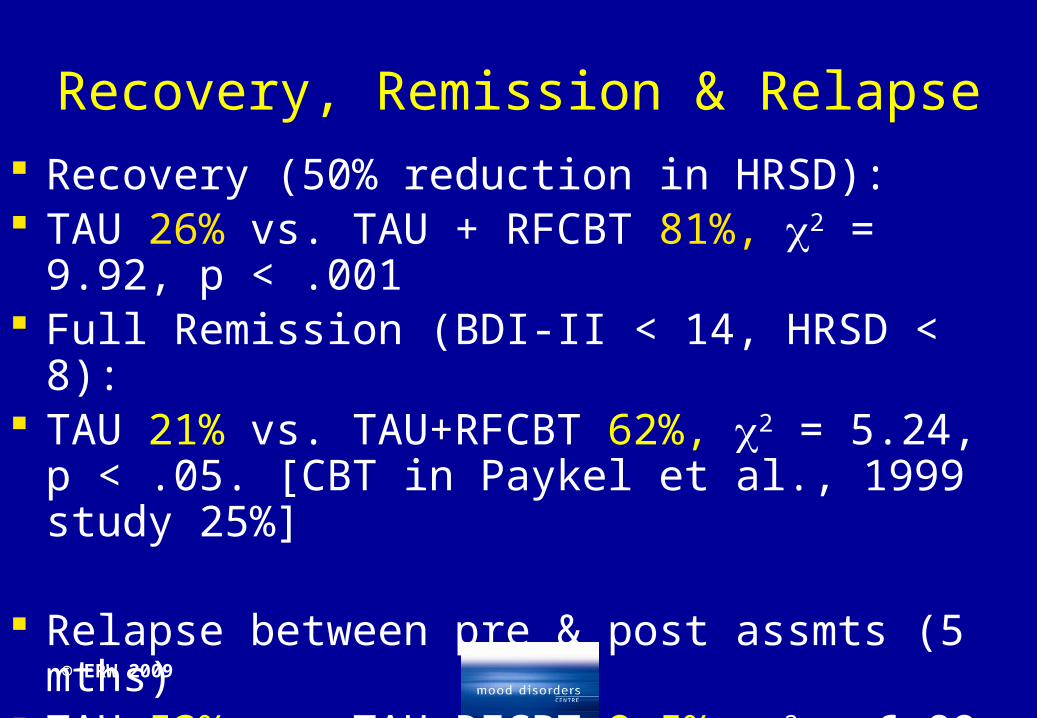
Recovery, Remission & Relapse Recovery (50% reduction in HRSD): TAU 26% vs. TAU + RFCBT 81%, 2 = 9.92, p
< .001 Full Remission (BDI-II < 14, HRSD < 8): TAU 21% vs. TAU+RFCBT 62%, 2 = 5.24, p < .05.
[CBT in Paykel et al., 1999 study 25%]
Relapse between pre & post assmts (5 mths) TAU 53% vs. TAU+RFCBT 9.5%, 2 = 6.89, p < .01

Factors maintaining rumination1. AVOIDANCE
(not addressed today)

Factors maintaining rumination2. Thinking Style
A behaviour experiment
A behavioural experiment used with patientsThe broken down car exercise – recall/imagine time when needed to get somewhere important soon and car would not start . Get as vivid an image of this situation as possible. Imagine that you are in a real hurry
The HOW-WHY behaviour experiment

HOW?
Probably found easier, more natural

WHY?
Processing mode hypothesis
Theory and experiments hypothesis that there are distinct styles of rumination, with distinct functional consequences
Adaptive, constructive ruminative self-focus = concrete, process-focused, specific thinking, focused on the concrete & specific experience & process of how things happen moment-by-moment
Maladaptive, unconstructive ruminative self-focus = abstract, general, evaluative thinking, thinking about why an outcome occurred (Moberly & Watkins, 2006; Rimes & Watkins, 2005; Watkins, 2004; Watkins & Baracaia, 2002; Watkins & Moulds, 2005; Watkins & Teasdale, 2001, 2004, Watkins, 2008, Psych Bull; Watkins, Moberly & Moulds, 2008)
Targeting avoidance & rumination
Treatment approach 2 – mode of processing
Intervention – Shifting processing mode

Switching thinking style
Shifting from evaluative..
to a more process-focused style…
1. Compare effective vs ineffective thinking in functional analysis
2. Use imagery, experiential exercises

Shifting processing style
Coach experiential exercises/ build up activities to shift out of abstract-evaluative rumination style
Focus on recreating experiences of being in a concrete process-focused style (counter to rumination)
Absorption experiences - recreate being caught up in the task, “flow”, “in the zone”, peak experiences (connected world direct way)

Compassion experiences - Recreating feeling compassionate, tolerant, caring, nurturing, non-judgemental
Focus on holistic experiential shift via memories, images: thoughts, feelings, posture, sensory experience, bodily sensations, attitude, motivation, facial expression, action feelings
Key elements of “flow” (Csikszentmihalyi, 2002)
Deep & effortless involvement in activity Merging of action & awareness Balanced ratio between challenge
(opportunities) & skills Focused attention on the task at hand Narrow temporal focus – immediate, present-
moment Clear goals, rules & immediate feedback
Key elements of “flow” (Csikszentmihalyi, 2002)
Loss of self-consciousness Changed perception of time Connection with environment – self-guiding Sense of possibility of control Activity intrinsically rewarding – valued as an end in
itself (autotelic) Focus on discovery, learning, growth – build self-
potential

Key elements in shifting style Requires preparation & socialisation into model, use of relaxation &
imagery work as groundwork Find vivid memories and imagery of being in process-focused
absorbed state – used to a. kick start mode b. Develop habit c. as example for functional analysis to make future plans
Review memory to build up details Recreate mental state using guiding questions to direct imagination
to details – present tense, field perspective:• Sensory experience – As vividly as you can see what you are looking at.
Describe what you can see• Motivation & Attitude• Posture – As you become more absorbed, notice your posture of relaxation• Physical sensations – Notice the sensations in your body• Feelings – Experience and hold onto your feelings, letting them deepen• Facial expressions – • Urges to actions• Attention – What do you notice? Where are you focusing your attention?
Experiential Exercise
Experiential exercise – process-focused versus evaluative experiment Think of an activity that you do fairly often – that you can be totally absorbed in
AND at other times find difficult to focus on “Reflecting on past experience, can you think of times when you were immersed in
an activity/ dwelling on something else & finding it hard to concentrate?” “As best you can, relive and re-experience that situation. Recall and vividly imagine
the setting – look out in that situation. See what you were looking at during that time, recreate how you were thinking, notice what you were attending to. Experience your feelings, and physical sensations. Notice how you feel.. Explore those feelings – what is your posture, facial expression. As best you can, recapture and hold onto that feeling of being absorbed in the process of …. Focus on what you can see in this situation. Notice what you are paying attention to. What is important to you in that situation?”
Compare what doing, experience of each mode

Key elements in shifting style Requires preparation & socialisation into model, use of relaxation &
imagery work as groundwork Find vivid memories and imagery of being compassionate to self or
others – used to a. kick start mode b. Develop habit c. as example for functional analysis to make future plans
Review memory to build up details Recreate mental state using guiding questions to direct imagination
to details – present tense, field perspective:• Sensory experience – As vividly as you can see what you are looking at.
Describe what you can see• Motivation & Attitude• Posture – As you become more absorbed, notice your posture of relaxation• Physical sensations – Notice the sensations in your body• Feelings – Experience and hold onto your feelings, letting them deepen• Facial expressions – • Urges to actions• Attention – What do you notice? Where are you focusing your attention?

Compassion Work Can use imagery building past experience (compassion to
others close, etc) or compassionate imagery (Gilbert) Need to stay with experience and repeat re learning habit Need to allow time to work through it Work up hierarchy from easier points of compassion to
more difficult (e.g., other to self) Avoid conceptual analysis and comparative thinking Break down and adapt to overcome barriers experientially Repeated practice in session and outside of session Use functionally
Summary
Avoidance & rumination play major role in maintenance of depression
Both can be normal & adaptive behaviours Value of adopting contextual, functional
approach – FUNCTIONAL ANALYSIS Function of rumination moderated by
processing style – Value of interventions to SHIFT style
© ERW 2009
Thank you Please feel free to contact me at
with any questions, thoughts, plans about research, for handouts etc

Additional slides from full workshop follow
Group approaches More information on avoidance More information on experimental work More information on functional analysis
© ERW 2009
Initial sessions during RFCBT
Standard CBT assessment interview to determine symptoms and problemsEstablish that rumination is a major problem – i.e. patients report extensive unproductive dwelling on negative materialExamine consequences of ruminationIdentify rumination as the target of therapy – a treatment goalExplain what rumination is, using examples from patients own experience
Rationale – key points1. Recurrent negative thinking and avoidance maintain
depression (the central engine driving depression)2. Both of these responses are quite normal and functional in
limited amounts under the right circumstances – i.e. “it is not surprising that you use them - everyone else uses them too.”
3. However, when used excessively or when they are out of balance, they become problematic.
4. Excessive use occurs because of past learning – either copying others or previous occasions when you learnt that rumination was a useful strategy – i.e. it has perceived benefit.
5. Because it was learnt, it can be replaced/overlearnt with a new more adaptive strategy.
6. Therapy will coach you in learning a new more adaptive approach based on your own experience (lead into functional analysis)
Group RFCBT
Two variants (1) In Exeter, using BA variant explicitly uses BA
terms with some RFCBT elements, avoidance key focus. Used open trial, moderate improvements (BDI reduce 10-15 pts). 90 min sessions
Session 1: Introduction, Mood-avoidance links, self-monitoring
Session 2: Examine avoidance, TRAPs, idea of alternative response. Record TRAPS
Group RFCBT Session 3: take ACTION, plan alternatives, visualise
putting into action Session 4: Breaking down challenges – smaller
steps Session 5: Rumination – form of TRAP, generate
consequences and functions of rumination, Alternatives to rumination –How vs Why?.
Session 6: Connecting with the Present – absorption exercise, use memory of absorption to interrupt rumination. Plan absorbing activities

Group RFCBT Session 7: Self-compassion – interactive
experiential exercise, Plan to be more compassionate
Session 8: Learning from experience – become more aware of triggers. Discriminating context. Notice when each tool works best
Session 9: Values – acting in line values Session 10: Resilience – review skills, plan for
ongoing activity, relapse prevention plans, review experience of group.
Group RFCBT (2) Revised group plan emerged consideration BA
groups plus development of rumination-focused prevention groups. 90 min sessions (?still in pilot). Main focus from beginning is Rumination.
Session 1: Introduction, Handling stress, introduce worry/rumination, examples generated group, rumination as habit, generate consequences, self-monitoring.
Session 2: Noticing warning signs, stepping out of habit – introduce if-then plans, changing circumstances.

Group RFCBT Session 3: Different Styles of thinking, experiential
alternative to rumination-e.g., relaxation, How vs Why? Experiential exercise, link into if-then plan, practice with “hot” warning sign
Session 4: Alternatives to rumination that serve function; useful rules of thumb (unanswerable questions, 30 min rule, lead to action?), absorption
Session 5: Self-compassion, experiential exercise, acting in a more caring way towards self
Session 6: Interpersonal Effectiveness, comparing effective vs ineffective, resilience

Key aspects of environment during functional analysis
The richness of the environment –The time of the day – Solitude – Rituals and routine – disruptionMood triggers –News signals – Evaluating self, plans and outcomes – Lack of structureLack of absorbing/valued activitiesAnniversaries/reminders
Dealing low motivation
Encourage change from the "outside-in" by changing behaviour without waiting for any internal change (“inside-out”)
act according to goals rather than feelings divorce action from mood dependence - act
while acknowledging that they didn't feel like acting at that moment
Set up as experiment – small step
FA & rumination
In group setting (RFCBT group pages 16-21):
A) Emphasize spotting warning signs – by situation, environment, physical response, actions, thoughts
B) Introduce idea of (i) changing the situation (pacing, prioritizing, environmental control, change routine) [facilitate change context to help break habit]
(ii) React differently If I notice this warning sign, then I can do
this ....alternative. Generate warning signs & trigger in
group Generate alternatives in group Generate functions (p. 35-37).
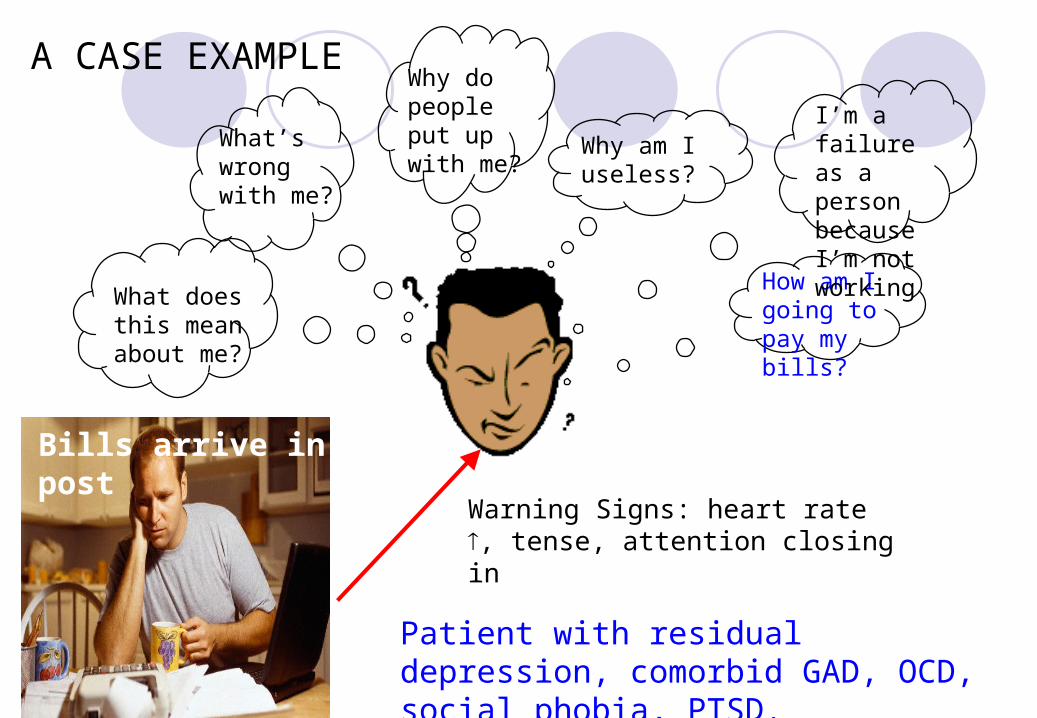
How am I going to pay my bills?
Why am I useless?
Why do people put up with me?
What’s wrong with me?
What does this mean about me?
I’m a failure as a person because I’m not working
Patient with residual depression, comorbid GAD, OCD, social phobia, PTSD.
Bills arrive in post
A CASE EXAMPLE
Warning Signs: heart rate , tense, attention closing in
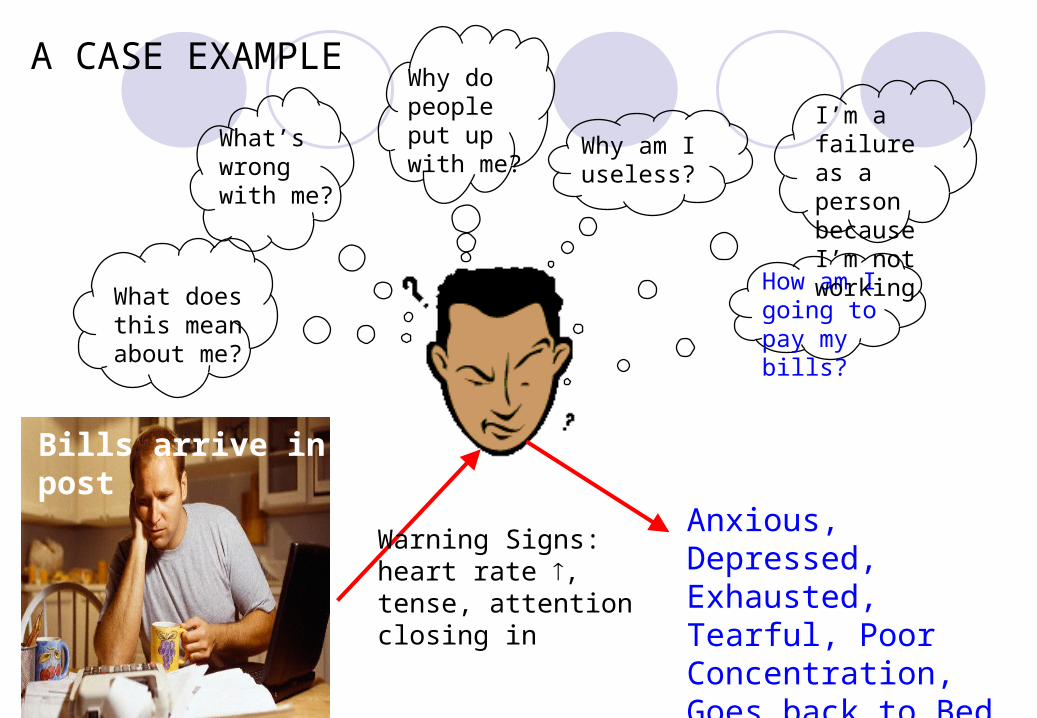
How am I going to pay my bills?
Why am I useless?
Why do people put up with me?
What’s wrong with me?
What does this mean about me?
I’m a failure as a person because I’m not working
Bills arrive in post
A CASE EXAMPLE
Warning Signs: heart rate , tense, attention closing in
Anxious, Depressed, Exhausted, Tearful, Poor Concentration, Goes back to Bed, ruminates over 3 hours
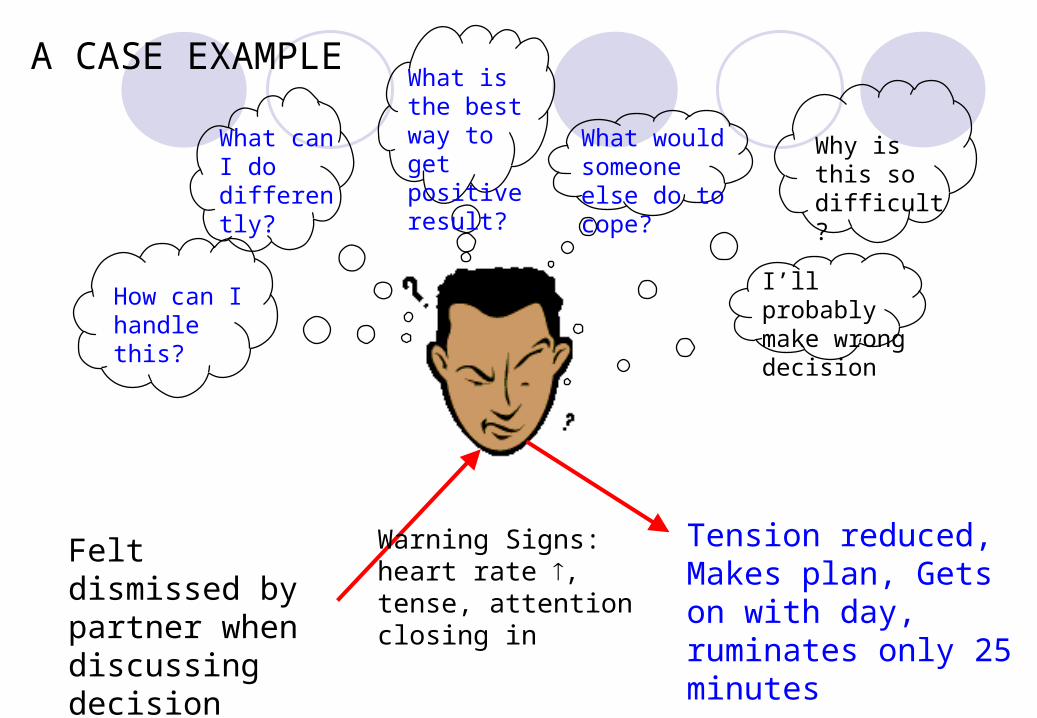
I’ll probably make wrong decision
What would someone else do to cope?
What is the best way to get positive result?
What can I do differently?
How can I handle this?
Why is this so difficult?
A CASE EXAMPLE
Warning Signs: heart rate , tense, attention closing in
Felt dismissed by partner when discussing decision
Tension reduced, Makes plan, Gets on with day, ruminates only 25 minutes

Key elements in switching modeRequires preparation – i.e. socialisation into model, use of functional analysis and contingency plans to start shift, use of relaxation and imagery work as groundwork
Find vivid memories and imagery of being in process-focused absorbed state – used to a. kickstart mode b. as coping strategy c. as example for functional analysis to make future plans – redress balance in life
Review memory to build up details
Recreate mental state using guiding questions to direct imagination to details – present tense, field perspective:• Sensory experience – As vividly as you can see what you are looking at.
Describe what you can see• Motivation & Attitude• Posture – As you become more absorbed, notice your posture of
relaxation• Physical sensations – Notice the sensations in your body• Feelings – Experience and hold onto your feelings, letting them deepen• Facial expressions – • Urges to actions• Attention – What do you notice? Where are you focusing your attention?

Switching styleExperiential exercise – process-focused versus evaluative experiment
Think of an activity that you do fairly often – that you can be totally absorbed in AND at other times find difficult to focus on
“Reflecting on past experience, can you think of times when you were immersed in an activity/ dwelling on something else & finding it hard to concentrate?”
“As best you can, relive and re-experience that situation. Recall and vividly imagine the setting – look out in that situation. See what you were looking at during that time, recreate how you were thinking, notice what you were attending to. Experience your feelings, and physical sensations. Notice how you feel.. Explore those feelings – what is your posture, facial expression. As best you can, recapture and hold onto that feeling of being absorbed in the process of …. Focus on what you can see in this situation. Notice what you are paying attention to. What is important to you in that situation?”
Compare what doing, experience of each mode

Q1. What initiates RT?
Theory: Martin & Tesser (1996), Watkins (2008) – RT triggered by a discrepancy between actual & desired/expected state = unresolved goal, loss, trauma
Discrepancy increases attention to & accessibility of information related to goal – with instrumental function of focusing on goal resolution (cf Zeigarnik effect, e.g., coming to terms, making sense), i.e., attempt at problem solving.
RT ceases if goal is attained or abandoned
© ERW 2010
Q1. What initiates RT? Evidence: recall of interrupted tasks better than of
completed tasks (Zeigarnik, 1938)
current concerns appear in thought if action regarding concern met with unexpected difficulties, if little time remained for action toward the goal (Klinger, Barta, & Maxeiner, 1980)
rumination about person left behind on coming to university predicted by extent to which activities shared with this person not resumed at university (Millar, Tesser, & Millar, 1988)
ESM study found that momentary ruminative self-focus associated with lack of progress on important goals (Moberly & Watkins, 2009)
© ERW 2010
Implications of problematic goal attainment account
Explains RT as a normal cognitive process, with potential instrumental effects
Adaptive or maladaptive depends upon whether increased focus on discrepancy helps to problem solve or not
Problem if goal unattainable & unable to let go of goal – e.g., perfectionism, goal linked self-concept, unanswerable question →
Perseveration of RT results from ineffective processing that prevents problem-solving & coming to terms (See Q3)
© ERW 2010
Lesson for Psychological Treatment 2
Telling people to stop worry & rumination won’t work Thought-stopping & Distraction can only be short-
lived RT will reoccur until goal discrepancy resolved
© ERW 2010
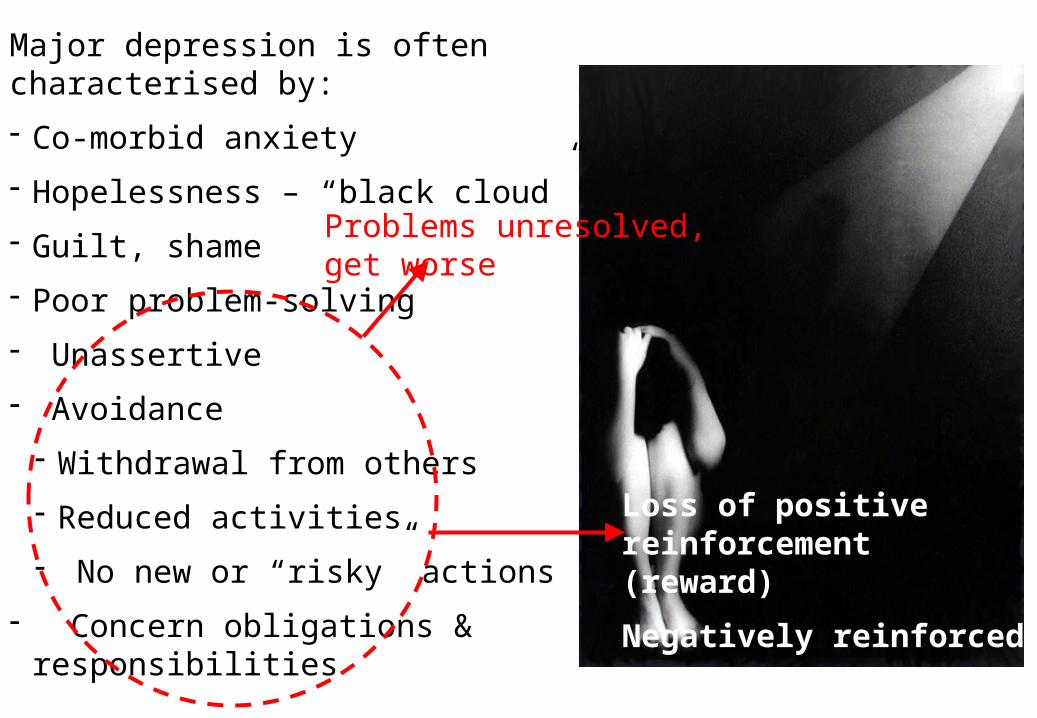
Major depression is often characterised by:
- Co-morbid anxiety
- Hopelessness – “black cloud”
- Guilt, shame
- Poor problem-solving
- Unassertive
- Avoidance
- Withdrawal from others
- Reduced activities
- No new or “risky” actions
- Concern obligations & responsibilities
Problems unresolved, get worse
Loss of positive reinforcement (reward)
Negatively reinforced
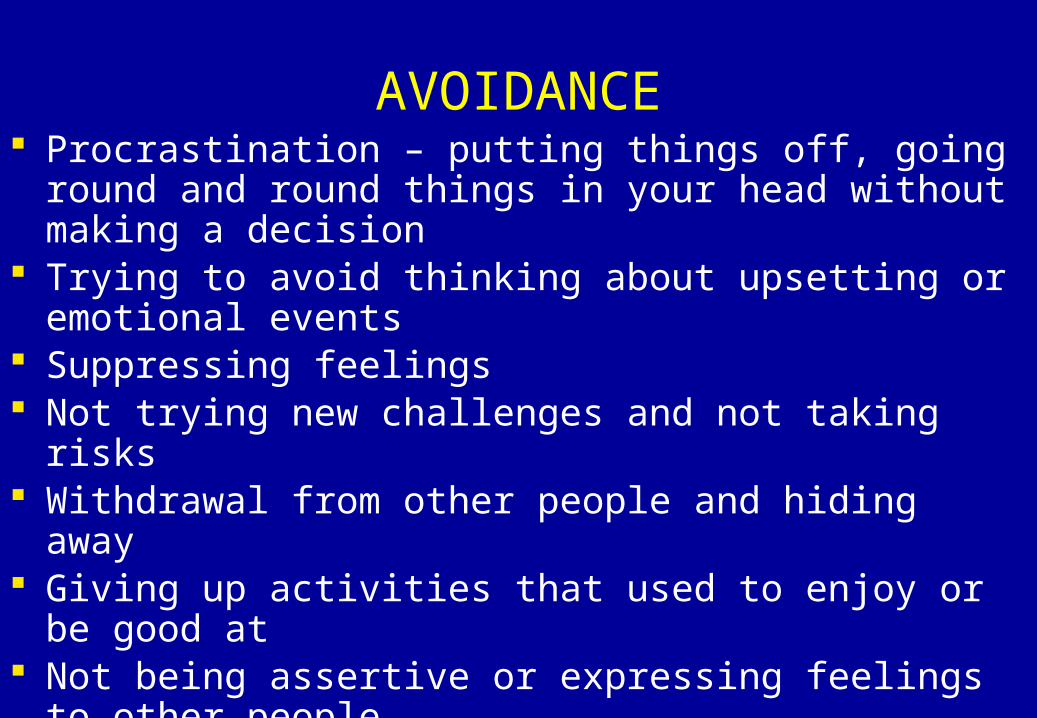
AVOIDANCE Procrastination – putting things off, going round and round
things in your head without making a decision Trying to avoid thinking about upsetting or emotional
events Suppressing feelings Not trying new challenges and not taking risks Withdrawal from other people and hiding away Giving up activities that used to enjoy or be good at Not being assertive or expressing feelings to other people Preferring to think about things rather than doing things Numbing oneself with drugs or alcohol Likely to be linked with rumination

Avoidance can be functional or dysfunctional
a normal response to threats and difficulties - useful for acute, short-lived problems

Dysfunctional Consequences of Avoidance
Avoidance leads to not coming into direct contact with an ongoing problem – no chance to fix it
Avoidance closes life down. Avoidance tends to generalise, leading to a closed, not very fulfilled life
Avoidance prevents exposure to new information that may disconfirm concerns or provide opportunity for learning
All common to rumination (being “stuck” in head rather than in the world)
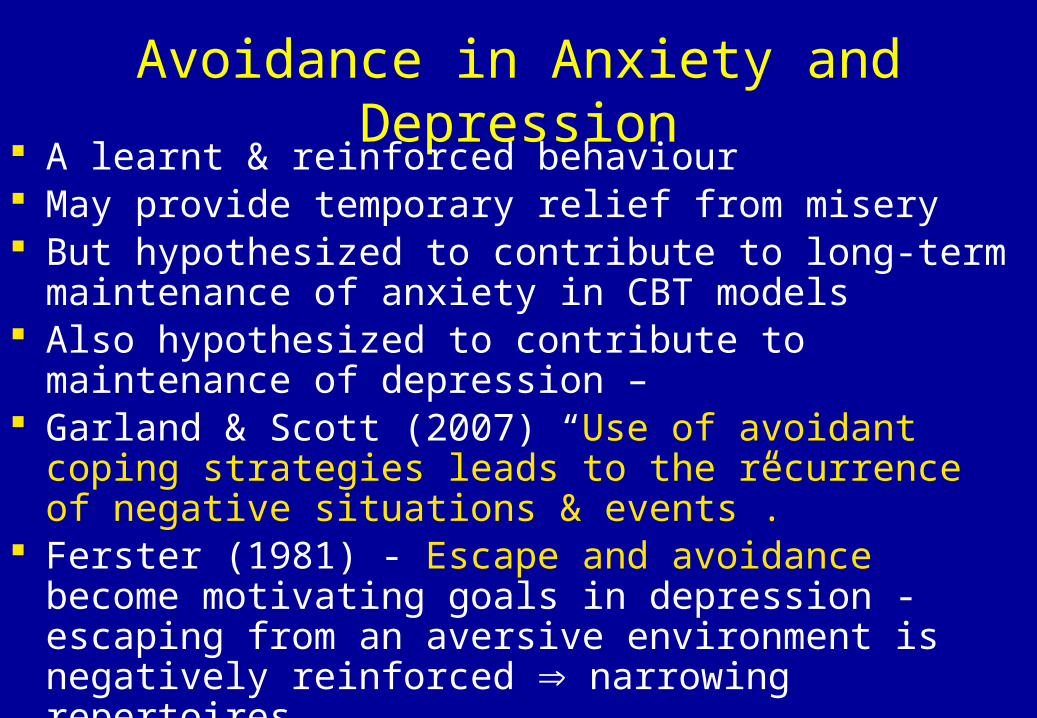
Avoidance in Anxiety and Depression A learnt & reinforced behaviour May provide temporary relief from misery But hypothesized to contribute to long-term maintenance of
anxiety in CBT models Also hypothesized to contribute to maintenance of
depression – Garland & Scott (2007) “Use of avoidant coping strategies
leads to the recurrence of negative situations & events”. Ferster (1981) - Escape and avoidance become motivating
goals in depression - escaping from an aversive environment is negatively reinforced narrowing repertoires

Deprivation (high FR responses before reward)
–ve reinforced (removal distress), freq
Loss of discrimination to contingency
Learn passivity (not learn behaviour +ve reinforcement)
Narrowing repertoires
Ferster 1981 – learning history & depression
Reduced contact +ve reinforcersEscape &
Avoidance
Respond to history of deprivation rather actual environment
DEPRESSION
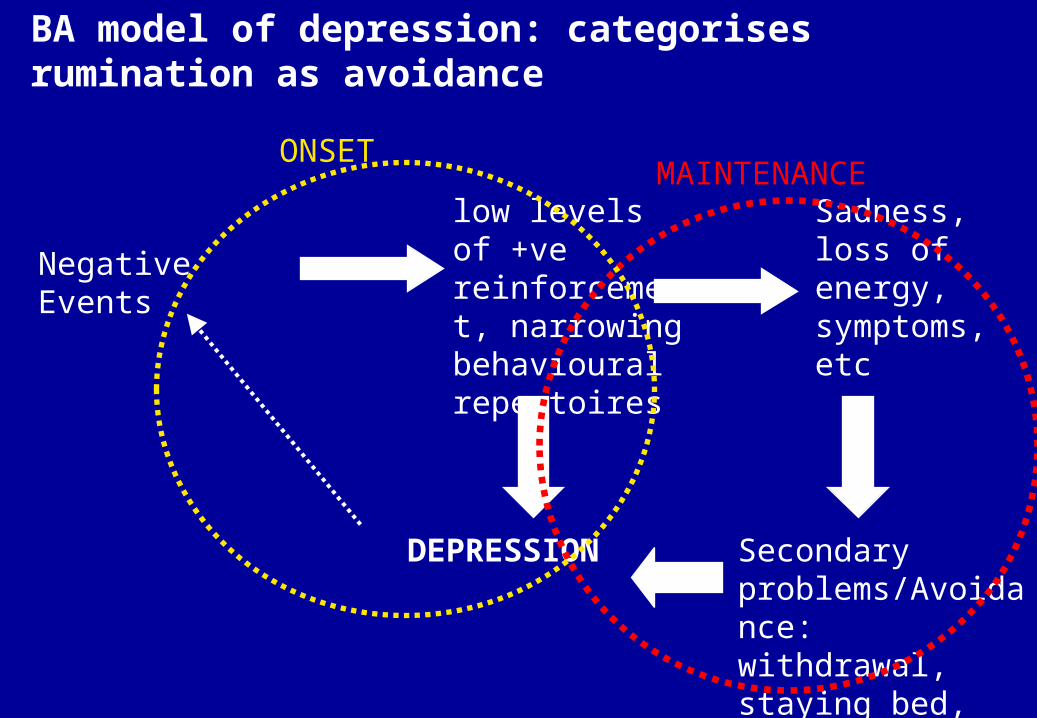
Negative Events
low levels of +ve reinforcement, narrowing behavioural repertoires
DEPRESSION
Sadness, loss of energy, symptoms, etc
Secondary problems/Avoidance: withdrawal, staying bed, rumination
ONSETMAINTENANCE
BA model of depression: categorises rumination as avoidance
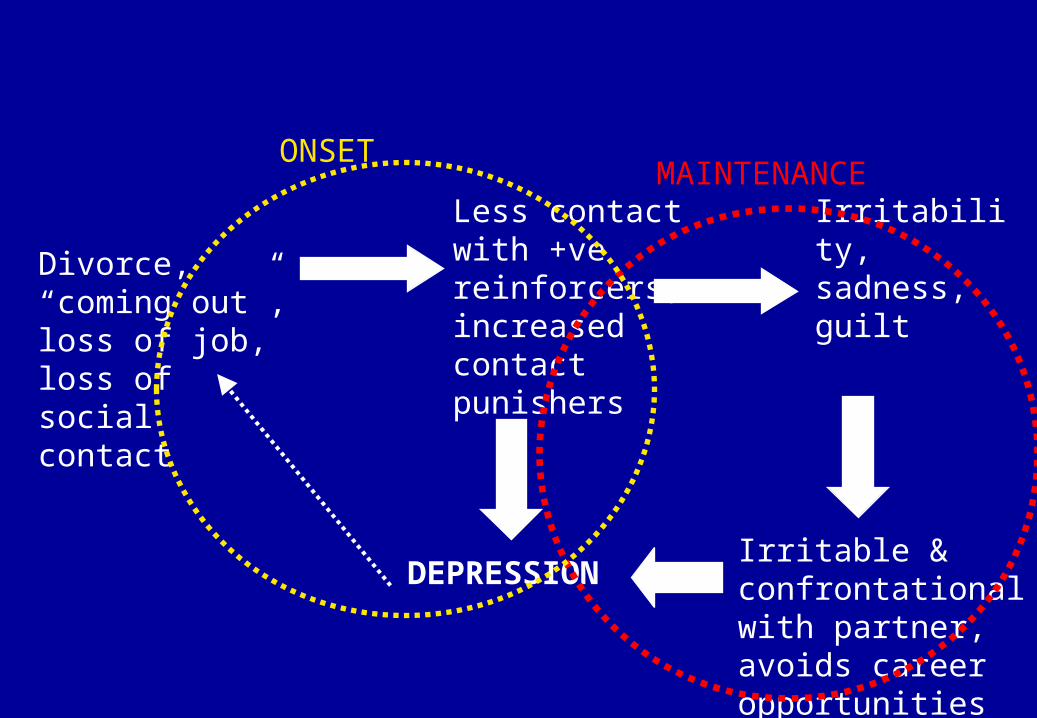
Divorce, “coming out”, loss of job, loss of social contact
Less contact with +ve reinforcers, increased contact punishers
DEPRESSION
Irritability, sadness, guilt
Irritable & confrontational with partner, avoids career opportunities
ONSETMAINTENANCE
Rumination as escape & avoidance Reinforced in the past by removal of aversive experience. Superstitious reinforcement/Partial reinforcement/Poor
discrimination Functions of rumination may include:
– Avoid challenges of job or tedium of daily grind. – Avoid risk of failure or humiliation– Cognitive avoidance (worry) –preparation, planning – Pre-empting other’s criticism / Anticipating potential negative
responses/criticism to avoid actual criticism (second guessing – mind-reading)
– Control of feelings– Making excuses– Motivation – spurring oneself on

Rumination as a learnt habit
Rumination may be become more frequent and extensive if it is a learnt behaviour with perceived positive consequences
i.e. rumination may be a response that someone has learned in the course of their life to particular environments
This is the view taken by contextual-functional approaches to depression e.g. behavioural activation (Martell, Addis & Jacobson, 2001).
Clinical Report
Patients report early experiences of criticism/blame and trying to work out how to avoid it.
Patients report using rumination INSTEAD of confronting problems in actuality.
Using rumination as an excuse not to do things. “I am doing something about it by thinking about it”


Watkins & Teasdale (2001 J.AbPsych, 2004, JAD) modified rumination paradigm (Nolen-Hoeksema & Morrow, 1993; Lyubomirsky & Nolen-Hoeksema, 1995).
Depressed patients:For 8 minutes
“Think about the causes, meanings and consequences of…..” (evaluative-abstract)
“Focus your attention on your experience of……” (concrete-process-focused)
versus
“…the physical sensations in your body”, “the way you feel inside”, etc, etc – ruminative self-focus on same content

00.05
0.10.15
0.20.25
0.30.35
0.40.45
baseline post-ruminationCa
teg
ori
c m
emo
ry (
pro
po
rtio
n)
EvaluativeConcrete
Watkins & Teasdale (2001 J.AbPsych, 2004, JAD)“Think about the causes, meanings and consequences of…..” symptoms & feelings (evaluative-abstract)
“Focus your attention on your experience of……” symptoms & feelings (concrete-process-focused)
versus
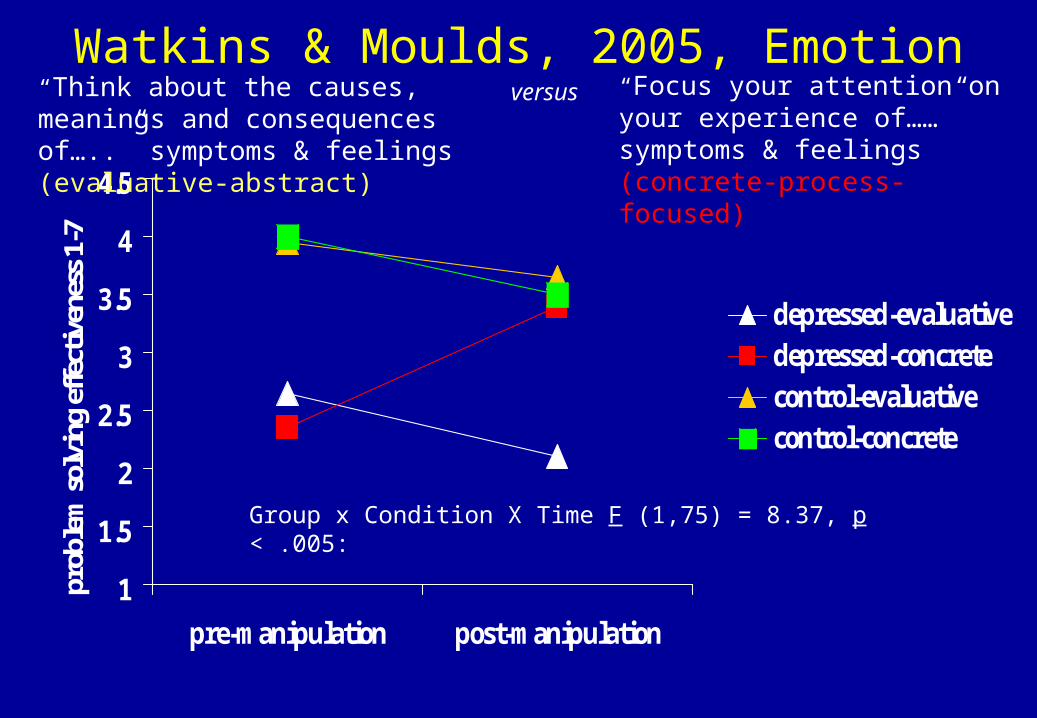
Watkins & Moulds, 2005, Emotion
1
1.5
2
2.5
3
3.5
4
4.5
pre-manipulation post-manipulation
prob
lem
sol
ving
eff
ectiv
enes
s 1-
7
depressed-evaluativedepressed-concretecontrol-evaluativecontrol-concrete
Group x Condition X Time F (1,75) = 8.37, p < .005:
“Think about the causes, meanings and consequences of…..” symptoms & feelings (evaluative-abstract)
versus “Focus your attention on your experience of……” symptoms & feelings (concrete-process-focused)
Targeting avoidance & rumination
Treatment approach 1 – contextual & functional
Intervention – Functional analysis
Behavioural Activation (BA) – Martell et al., 2001
Increasing approach – reducing avoidance
Focus on context/function
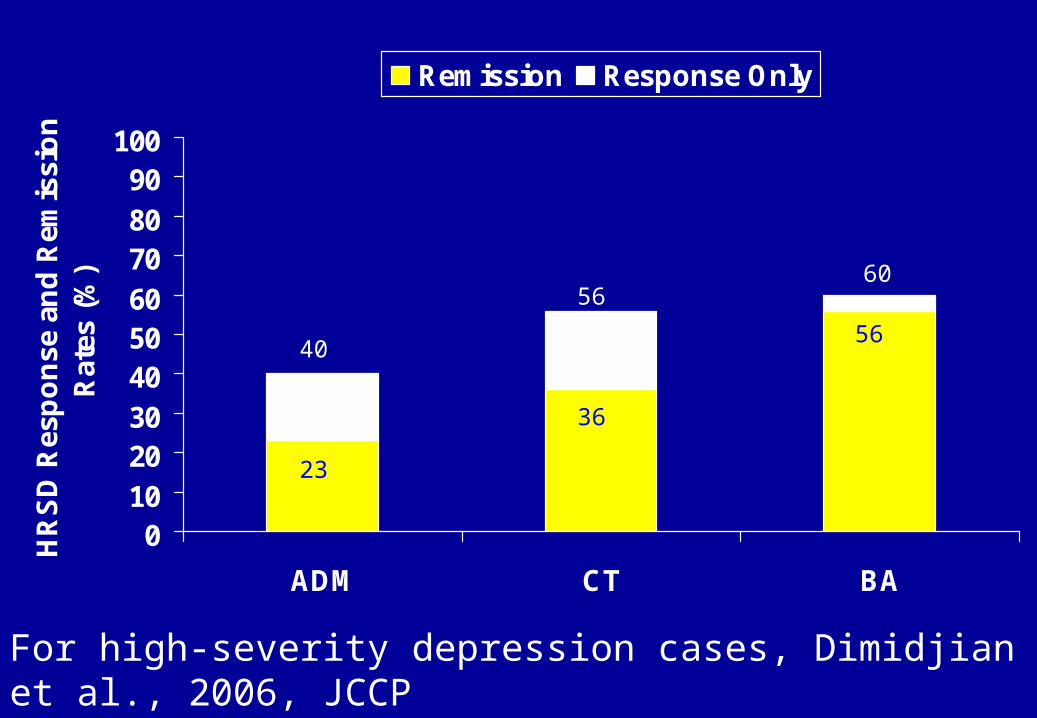
0102030405060708090
100
ADM CT BA
HR
SD
Res
po
nse
an
d R
emis
sio
n
Rat
es (
%)
Remission Response Only
40
5660
23
36
56
For high-severity depression cases, Dimidjian et al., 2006, JCCP

Key principles of contextual-functional approach (BA & RFCBT)
Viewing depression as - a set of actions in context - as understandable and predictable given a
person's life history and current context –e.g. avoiding short-term pain leading to longer-
term negative consequences Looking at function rather than form Looking at process rather than content Looking at rumination as a learnt habit

Implications of Rumination as Habit Habits resist informational interventions (Verplanken &
Wood, 2006)
Hence, focus on thought content alone (e.g., thought challenging) may be insufficient – need to change process.
Successful habit change involves (i) disrupting the environmental factors (time, place, mood) that automatically cue habit (Wood & Neal, 2007); (ii) training to associate cue (warning sign) with incompatible response in conflict unwanted habit
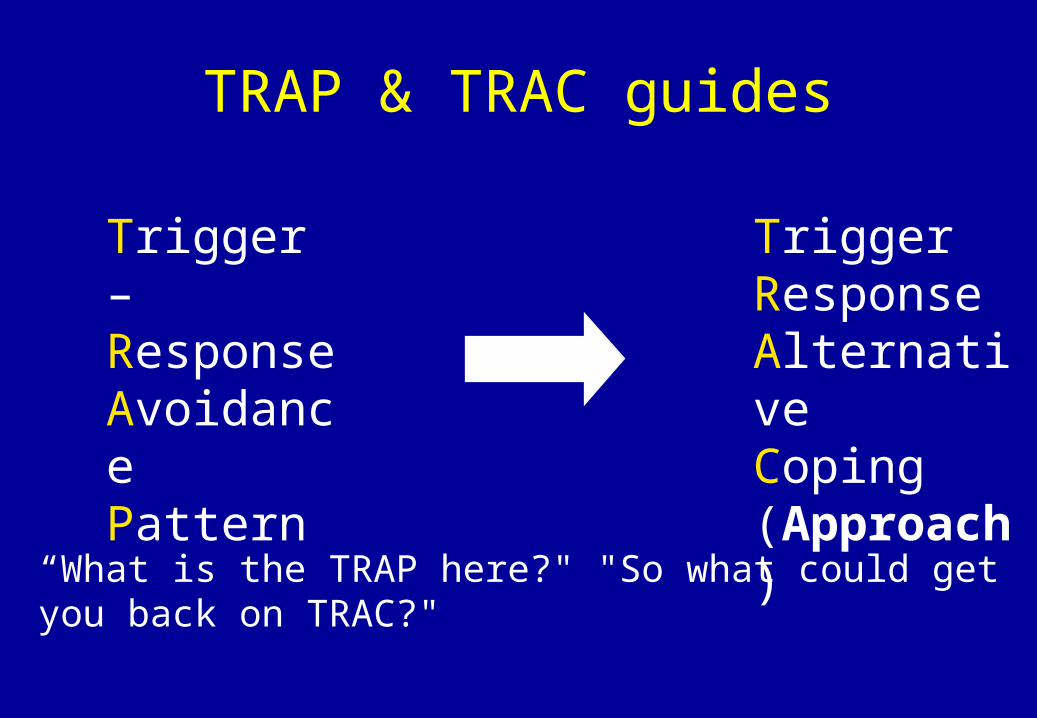
Trigger – ResponseAvoidancePattern
TriggerResponseAlternativeCoping (Approach)
TRAP & TRAC guides
“What is the TRAP here?" "So what could get you back on TRAC?"

Rumination-focused CBT (RFCBT) RFCBT focuses on increasing effective behaviour
– i.e., not stopping rumination but making it functional
RFBCT grounded within the core principles and techniques of CBT for depression (Beck, Rush, Shaw, &
Emery, 1979) with two adaptations:– a functional-analytical perspective using Behavioural
Activation (BA) approaches (Addis & Martell, 2004; Martell et al., 2001)
– An explicit focus on shifting processing style via imagery and experiential approaches

Overview of treatment components
The key elements of the therapy are:– Providing an idiosyncratic assessment tied into a clear rationale
for the focus on rumination, building on the idea that rumination is learnt behaviour. It is important here to incorporate the patients’ developmental history into the rationale.
– Encourage practise at spotting rumination, avoidance and early warning signs of each, using formal homework.
– Functional analysis to examine the context and functions of rumination and avoidance.
– These analyses then lead onto developing contingency plans, involving more functional responses to early warning signs. The format of interventions will often involve imagery and vizualisation exercises.
Overview of treatment components
The key elements of the therapy are:– The use of experiments to examine whether rumination is
adaptive or not and to try out alternative strategies, e.g. the How-Why experiment.
– Increased activity and reduced avoidance, including building up routines and increasing non-ruminative activities. This activity needs to be made as explicit as possible, targeting behavioural changes.
– The use of experiential exercises and vizualisations to provide functional experience of adaptive use of attention as a counter to rumination. Used to establish alternative thinking style.
– A focus on the client’s values to minimise rumination about non-valued areas and to encourage activity in line with values.
Treatment rationale1. Recurrent negative thinking and avoidance maintain depression (the
central engine driving depression)
2. Both of these responses are quite normal and functional in limited amounts under the right circumstances – i.e. “it is not surprising that you use them - everyone else uses them too.”
3. However, when used excessively or when they are out of balance, they become problematic.
4. Excessive use occurs because of past learning – either copying others or previous occasions when you learnt that rumination was a useful strategy – i.e. it has perceived benefit.
5. Because it was learnt, it can be replaced/overlearnt with a new more adaptive strategy.
6. Therapy will coach you in learning a new more adaptive approach based on your own experience (lead into functional analysis)