Βελτιώνοντας την έκβαση στο nstemi...ua nstemi stemi unstable angina qwmi st...
TRANSCRIPT

Βελτιώνοντας την έκβαση στο NSTEMI : Αξιολόγηση και αποτελεσματική
επαναγγείωση
ΠΕΤΡΟΣ Σ. ΔΑΡΔΑΣ, MD, FESC
ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ
35ο ΠΑΝΕΛΛΗΝΙΟ ΚΑΡΔΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ, ΑΘΗΝΑ 2014

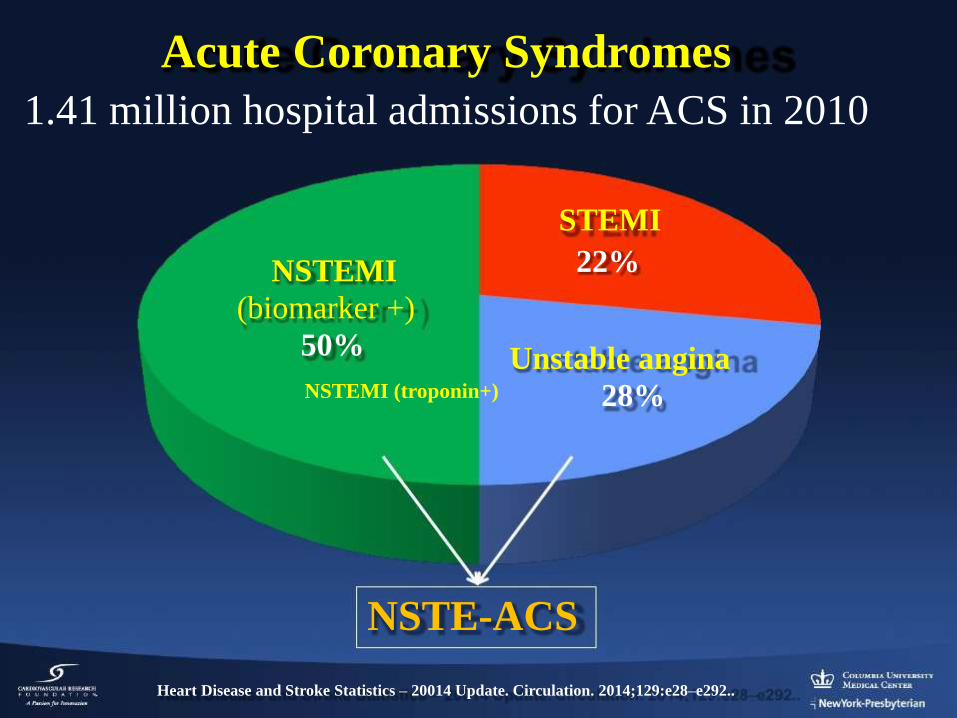
Acute Coronary Syndromes
1.41 million hospital admissions for ACS in 2010
STEMI
NSTEMI
(biomarker +)
50%
NSTEMI (troponin+)
22%
Unstable angina
28%
NSTE-ACS
Heart Disease and Stroke Statistics – 20014 Update. Circulation. 2014;129:e28–e292..

UA and NSTEMI: Pathophysiology
Ruptured plaque with non occlusive thrombus

Myocardial Infarction
NSTE-ACS
Secondary Prevention/
Long-Term ManagementManagement Prior to
NSTE-ACS
Onset of NSTE-ACS-Initial recognition and management in the
ED by first responders or ED personnel
-Risk stratification
-Immediate management
Hospital Management-Medication-Conservative versus invasive strategy
-Special groups
-Preparation for discharge
Final Dx
Cardiac Biomarker
ECG
Working Dx
Presentation Ischemic Discomfort
ACS
No ST Elevation
NQMI
STEMINSTEMIUA
Unstable Angina
QwMI
ST Elevation
Noncardiac
Etiologies
* *
Acute Coronary Syndromes


Early Risk Stratification
History and Physical Examination
EKG
Biomarkers
Risk Scores
Conservative vs. Invasive Management
Timing of Invasive Management
Treatment of Non-ST-Elevation ACS
Outline
Early Risk Stratification
History and Physical Examination
EKG
Biomarkers
Risk Scores
Conservative vs. Invasive Management
Timing of Invasive Management
Treatment of Non-ST-Elevation ACS
Outline



Biomarkers: Diagnosis
Recommendations COR LOE
Cardiac-specific troponin (troponin I or T when a
contemporary assay is used) levels should be measured at
presentation and 3 to 6 hours after symptom onset in all
patients who present with symptoms consistent with ACS to
identify a rising and/or falling pattern.
I A
Additional troponin levels should be obtained beyond 6
hours after symptom onset in patients with normal
troponins on serial examination when electrocardiographic
changes and/or clinical presentation confer an intermediate
or high index of suspicion for ACS.
I A
With contemporary troponin assays, creatine kinase
myocardial isoenzyme (CK-MB) and myoglobin are not
useful for diagnosis of ACS.
III: No
BenefitA
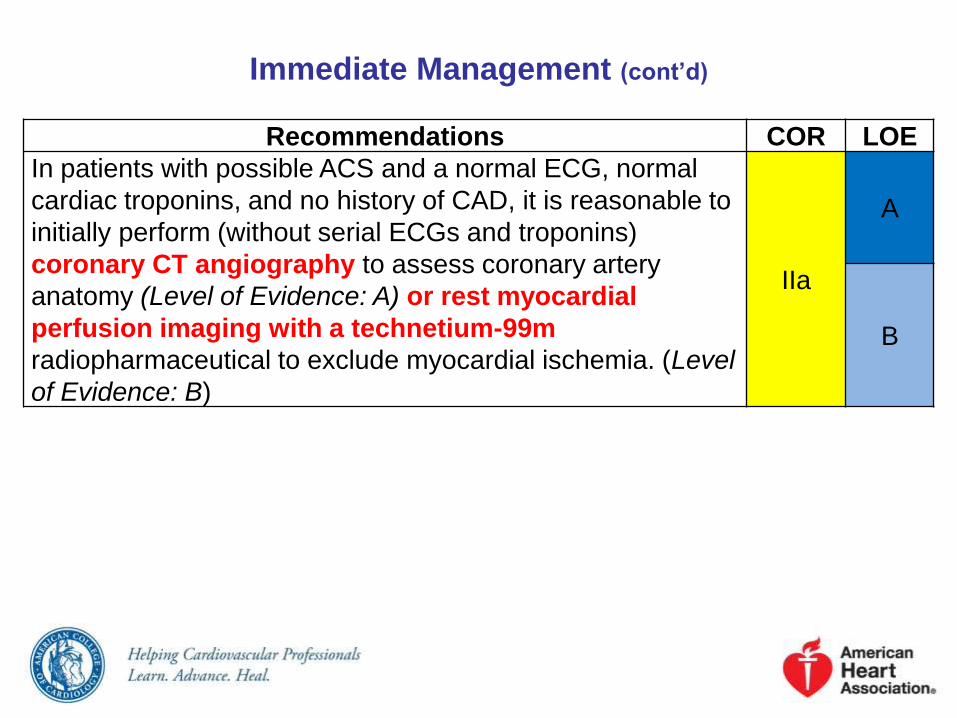
Immediate Management (cont’d)
Recommendations COR LOE
In patients with possible ACS and a normal ECG, normal
cardiac troponins, and no history of CAD, it is reasonable to
initially perform (without serial ECGs and troponins)
coronary CT angiography to assess coronary artery
anatomy (Level of Evidence: A) or rest myocardial
perfusion imaging with a technetium-99m
radiopharmaceutical to exclude myocardial ischemia. (Level
of Evidence: B)
IIa
A
B

Prognosis: Early Risk Stratification
Recommendations COR LOE
Risk scores should be used to assess prognosis in patients
with NSTE-ACS. I A

TIMI Risk Score* for NSTE-ACS
TIMI Risk
Score
All-Cause Mortality, New or Recurrent MI, or
Severe Recurrent Ischemia Requiring Urgent
Revascularization Through 14 d After
Randomization, %
0–1 4.7
2 8.3
3 13.2
4 19.9
5 26.2
6–7 40.9
*The TIMI risk score is determined by the sum of the presence of 7
variables at admission; 1 point is given for each of the following variables:
≥65 y of age; ≥3 risk factors for CAD; prior coronary stenosis ≥50%; ST
deviation on ECG; ≥2 anginal events in prior 24 h; use of aspirin in prior 7
d; and elevated cardiac biomarkers.

Antman EM, et al. JAMA 2000;284:835–42
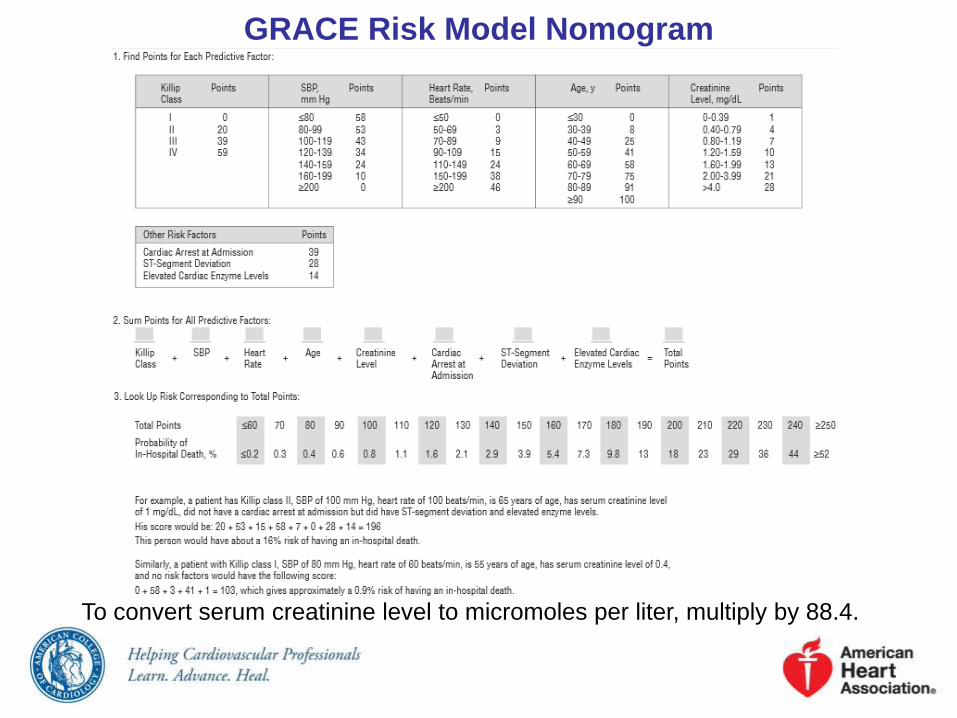
GRACE Risk Model Nomogram
To convert serum creatinine level to micromoles per liter, multiply by 88.4.




Early Risk Stratification
Risk Score App
GRACE risk score 2.0
• provides prognosis at six months, one year, and three years
• developed in over 30,000 patients with ACS and validated externally in a registry of nearly 3000 patients
• Risks are given directly as propabilities

VERY HIGH-RISK PATIENTShigh risk that formal early risk stratification is not necessary These patients typically need to
proceed to urgent coronary angiography
• Cardiogenic shock
• Overt heart failure (HF) or severe left ventricular dysfunction
• Recurrent or persistent rest angina despite intensive medical therapy
• Hemodynamic instability due to mechanical complications (eg, acute mitral regurgitation, ventricular septal defect)
• Unstable ventricular arrhythmias

Early Risk Stratification
History and Physical Examination
EKG
Biomarkers
Risk Scores
Conservative vs. Invasive Management
Timing of Invasive Management
Treatment of Non-ST-Elevation ACS
Outline

Cumulative Percentage
Fox KAA et al. J Am Coll Cardiol 2010;55:2435–45
Pint-HR = 0.10High risk: 13% of pts
HR: [95%CI] =
0.68 [0.53, 0.86]
Risk diff =
–11.1% [–18.4%, –3.8%)
Int risk: 34% of pts
HR: [95%CI] =0.81 [0.66, 1.01]
Risk diff =
–3.8% [–7.4%, –0.1%)
Low risk: 53% of pts
HR: [95%CI] =
0.80 [0.63, 1.02]
Risk diff =
–2.0% [–4.1%, 0.1%)
Selective invasive
Routine invasive
Selective invasive 2746Routine invasive 2721
24522485
23512410
21782235
20772166
20052079
542 3Follow-up time (years)
10
High
Intermediate
Low
50%
40%
30%
20%
10%
0%
5 Year FU After Routine vs. Selective Invasive
Strategy in ACS
FRISC-II, ICTUS, and RITA-3 (n=5,457)
CV Death or MI by risk group

O’Donoghue M. JAMA 2008;300:71-80
12-month follow-up
Early Invasive vs Conservative Treatment Strategies
in Women and Men with Unstable Angina and Non-
ST-Segment Elevation Myocardial Infarction:
A Meta-analysis

In NSTE ACS, an invasive strategy has a
comparable benefit in men and high-risk
women for reducing the composite end point
of death, MI, or rehospitalization with ACS
O’Donoghue et al., JAMA 2008; 300:71

Early Risk Stratification
History and Physical Examination
EKG
Biomarkers
Risk Scores
Conservative vs. Invasive Management
Timing of Invasive Management
Treatment of Non-ST-Elevation ACS
Outline

Cath >36 hrs
Median 50 hrs
N=1438
Cath <24 hrs
Median 14 hrs
N=1593
TIMACSTiming of Intervention in Patients with Acute Coronary Syndromes
3,031 patients with UA/NSTEMI
25% XO to early cath
Mehta SR et al. NEJM 2009;360:2165-75





Ischemia-Guided Strategy Versus Early Invasive
Strategies
Early Hospital Care

Factors Associated With Appropriate Selection of Early Invasive
Strategy or Ischemia-Guided Strategy in Patients With NSTE-ACS
Immediate
invasive
(within 2 h)
Refractory angina
Signs or symptoms of HF or new or worsening mitral regurgitation
Hemodynamic instability
Recurrent angina or ischemia at rest or with low-level activities despite
intensive medical therapy
Sustained VT or VF
Ischemia-
guided
strategy
Low-risk score (e.g., TIMI [0 or 1], GRACE [<109])
Low-risk Tn-negative female patients
Patient or clinician preference in the absence of high-risk features
Early
invasive
(within 24
h)
None of the above, but GRACE risk score >140
Temporal change in Tn (Section 3.4)
New or presumably new ST depression
Delayed
invasive
(within
2572 h)
None of the above but diabetes mellitus
Renal insufficiency (GFR <60 mL/min/1.73 m²)
Reduced LV systolic function (EF <0.40)
Early postinfarction angina
PCI within 6 mo
Prior CABG
GRACE risk score 109–140; TIMI score ≥2

Risk Stratification Before Discharge for Patients
With an Ischemia-Guided Strategy of NSTE-ACS
Early Hospital Care

Risk Stratification Before Discharge for Patients With an
Ischemia-Guided Strategy of NSTE-ACS
Recommendations COR LOE
Noninvasive stress testing is recommended in low- and
intermediate-risk patients who have been free of ischemia
at rest or with low-level activity for a minimum of 12 to 24
hours.
I B
Treadmill exercise testing is useful in patients able to
exercise in whom the ECG is free of resting ST changes
that may interfere with interpretation.I C
Stress testing with an imaging modality should be used
in patients who are able to exercise but have ST changes
on resting ECG that may interfere with interpretation. In
patients undergoing a low-level exercise test, an imaging
modality can add prognostic information.
I B

Risk Stratification Before Discharge for Patients With an
Ischemia-Guided Strategy of NSTE-ACS (cont’d)
Recommendations COR LOE
Pharmacological stress testing with imaging is
recommended when physical limitations preclude adequate
exercise stress.
I C
A noninvasive imaging test is recommended to evaluate LV
function in patients with definite ACS. I C

Initial Antiplatelet/Anticoagulant Therapy in
Patients With Definite or Likely NSTE-ACS
Early Hospital Care



Antiplatelet and Anticoagulant Therapy:
Oral and Antiplatelet Agents
Recommendations COR LOE
It is reasonable to choose ticagrelor over clopidogrel for
P2Y12 inhibition treatment in patients with NSTE-ACS
treated with an early invasive strategy and/or coronary
stenting.
IIa B
It is reasonable to choose prasugrel over clopidogrel for
P2Y12 treatment in patients with NSTE-ACS who undergo
PCI who are not at high risk of bleeding complications.IIa B

Conclusions
• NSTEACS comprises >75% of all ACS admissions
• Early risk stratification should be performed using
symptoms, risk factors, EKG and biomarkers
• Risk scores: TIMI or GRACE
•A routine early invasive strategy results in
reduction in death, MI, and rehospitalization for
ACS, especially in high-risk pts
• Catheterization and revascularization within 12 to
24 hours may be preferred in high-risk pts
Cannon CP, et al. N Engl J Med 2001;344:1879–87.
Treatment of NSTEACS
LATE RISK STRATIFICATION
• among all major cardiac events that occur in the first six weeks, approximately one-fourth occur after discharge
• left ventricular ejection fraction
• in medically managed patients, stress testing to detect possible residual ischemia

59 male, Unstable anginahemodynamically stable, 2 episodes of pain last 24 hours, renal function normal, EF 55%
hs troponine +ve - mild ECG changesprevious PCI LAD – RCA, 3 risk factors
GRACE score 109 – TIMI risk score 5 (risk of event by 14 days 26.2%)

Unstable anginahs troponine +ve - no ECG changes
previous PCI LAD – RCA patent
Patent LAD stent Patent RCA stent
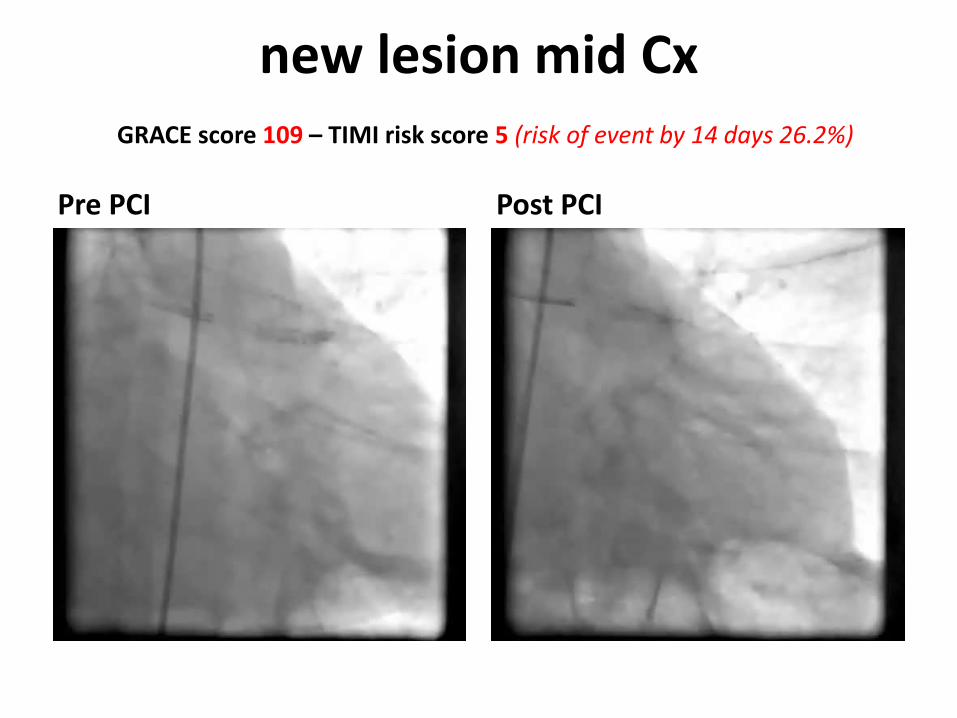
new lesion mid CxGRACE score 109 – TIMI risk score 5 (risk of event by 14 days 26.2%)
Pre PCI Post PCI
