© healthpass 20111 how health insurance exchanges will affect employers and health plans shawn...
TRANSCRIPT

© HealthPass 2011 1
How Health Insurance Exchanges Will Affect Employers and Health PlansShawn Nowicki, MPHDirector, Health PolicyHealthPass | New York Business Group on Health
A Presentation for the National Congress on Health Insurance Reform Pre-Conference on Health Insurance Exchanges
Ritz-Carlton Hotel, Washington, DCJanuary 19, 2011
© HealthPass 2011 2
1. About HealthPass
2. How Exchanges Affect Employers
3. How Exchanges Affect Health Plans
4. Questions
Today’s Agenda
© HealthPass 2011 3
About HealthPass New York
© HealthPass 2011 4
• Commercial health insurance exchange started in 1999
• Joint collaboration between:– Northeast Business Group on Health– Mayor’s Office of the City of New York– Health insurance industry
• Missions:– Grant small businesses greater access to healthcare– Help stem the tide of the working uninsured
A Commercial Health Insurance Exchange for NY Small Businesses
© HealthPass 2011 5
An Employee-Choice Model
• Employee-choice, defined contribution model for small businesses in a pure community-rated environment
• Menu of carriers and benefits• Serve 5 boroughs of NYC, Long Island, Mid-Hudson Valley

© HealthPass 2011 6
How Exchanges Affect Employers
© HealthPass 2011 7
• Must be a simple, streamlined purchasing experience In Utah Exchange pilot, 20% of eligible groups didn’t enroll
because employees couldn’t complete application • Defined contribution model encouraged• Broad, but not overly complicated, range of choices needed• Simplified administration & a suite of solutions
One-page group election and employee enrollment forms Robust member services/call center Ancillary services
• Employee choice (at the point of enrollment) Relieves employer from choosing coverage plan that may or may
not fit employees’ needs and budget
SHOP Exchanges Must Be Attractive to Employers

© HealthPass 2011 8
Exchange Must Streamline Health Benefits Services
ROBUST ADMINISTRATIVE SERVICES
In-House Member Services
COBRA & State Continuation
Admin.
Premium Aggregation & Monthly
Consolidated “List” Billing
Section 125 for Pre-Tax Premium
Contributions
Eligibility Determination
Enrollment &
Subsequent Employer
and Employee Education
S i z e o f s m a l l b u s i n e s s c o r r e l a t e d w i t h H R c a p a b i l i t y

© HealthPass 2011 9
Choice at What Level?
• Mirrors individual exchange options• Small ERs offer cost-sharing options outside of
Exchange (e.g., HDHP/HSA vs. traditional plan)
FULL/BROAD EMPLOYEE CHOICE
ACROSS TIERS
• Explicit option in Affordable Care Act• Enjoys some support because of adverse risk selection
concerns
WITHIN EMPLOYER-DESIGNATED PRECIOUS
METAL TIER
• Traditional method of employer-sponsored coverage• However, system needs to move to individual,
employee choiceEMPLOYER CHOICE
Defined fixed-dollar employer contribution recommended across all options
DE
SIR
AB
ILIT
Y
© HealthPass 2011 10
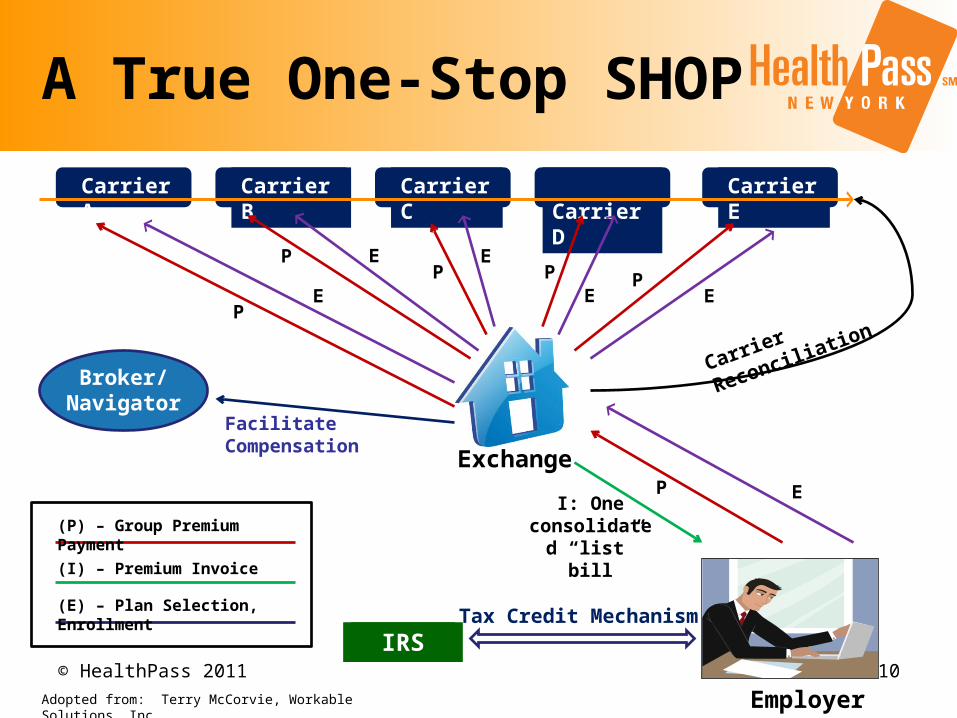
A True One-Stop SHOP
Exchange
Employer
Carrier A Carrier B Carrier C Carrier D Carrier E
Broker/ Navigator
IRSTax Credit Mechanism
(P) – Group Premium Payment
(E) – Plan Selection, Enrollment
(I) – Premium Invoice
I: One consolidated
“list” bill
P E
Facilitate Compensation
P
PP P P
EE
EE
E
Carrier Reconciliation
Adopted from: Terry McCorvie, Workable Solutions, Inc.
© HealthPass 2011 11
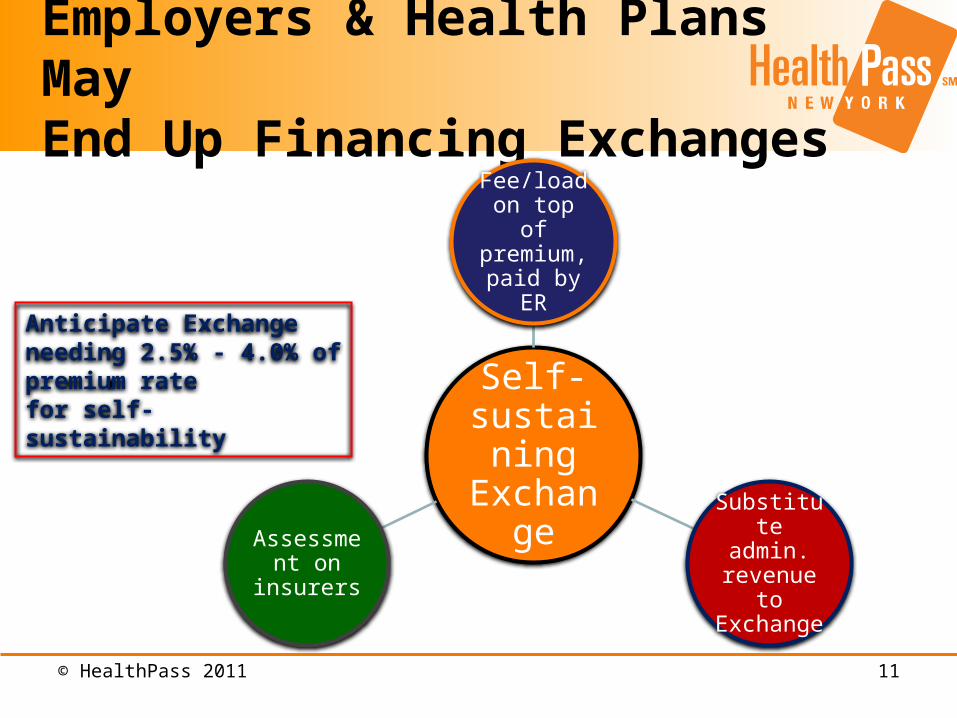
Employers & Health Plans May End Up Financing Exchanges
Self-sustaining Exchange
Fee/load on top of
premium, paid by ER
Substitute admin.
revenue to Exchange
Assessment on insurers
Anticipate Exchange needing 2.5% - 4.0% of premium rate for self-sustainability
© HealthPass 2011 12
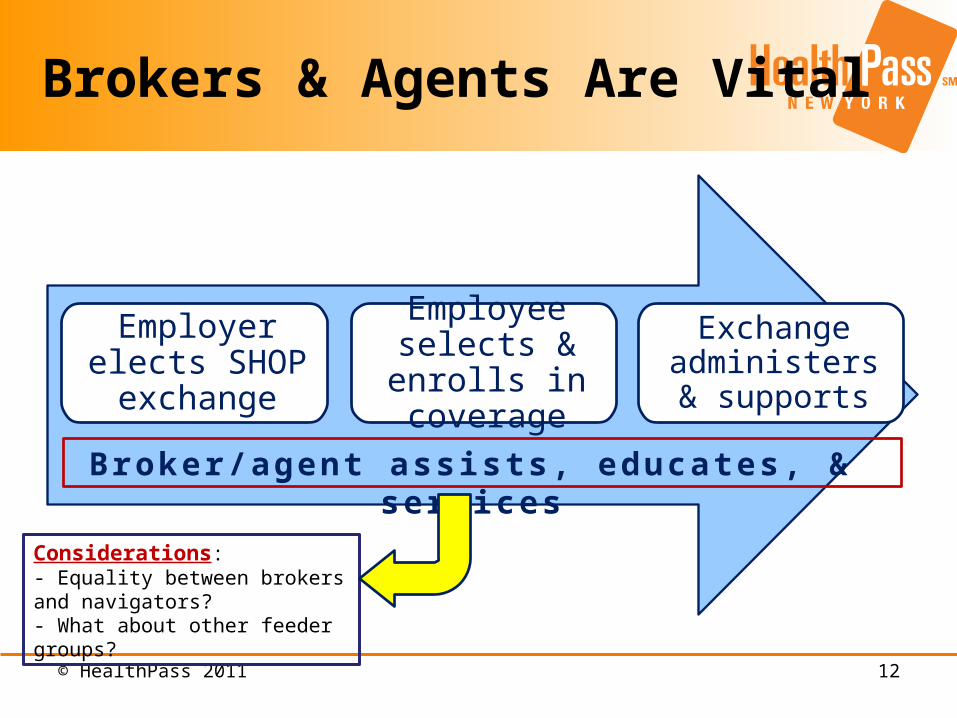
Brokers & Agents Are Vital
Employer elects SHOP exchange
Employee selects & enrolls in
coverage
Exchange administers &
supports
Considerations: - Equality between brokers and navigators? - What about other feeder groups?
B r o ke r /a g e n t a s s i s t s , e d u c a t e s , & s e r v i c e s
© HealthPass 2011 13
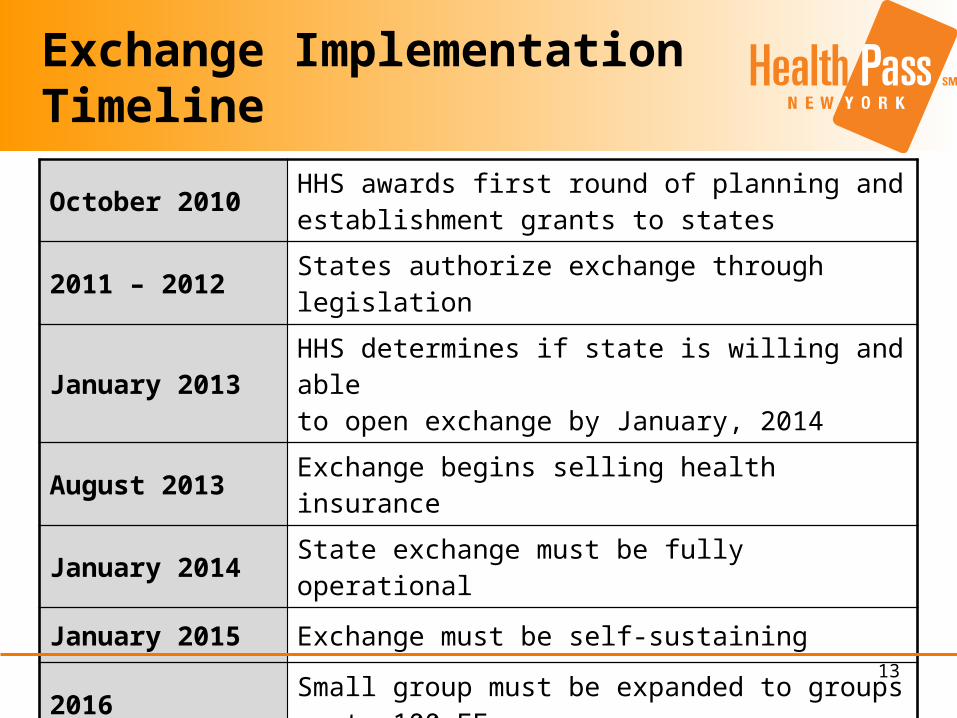
Exchange Implementation Timeline
October 2010 HHS awards first round of planning and establishment grants to states
2011 – 2012 States authorize exchange through legislation
January 2013 HHS determines if state is willing and able to open exchange by January, 2014
August 2013 Exchange begins selling health insurance
January 2014 State exchange must be fully operational
January 2015 Exchange must be self-sustaining
2016 Small group must be expanded to groups up to 100 EEs
2017 State may open exchange to large groups (>100 EEs)

© HealthPass 2011 14
Employer & Employee Benefits
Employer Benefits
• No need to pick one plan for different employees• Curbs wasted healthcare spending• Helps to attract and retain key employees• Empowers employees to participate in making informed healthcare decisions• Defined contribution sets a benefits budget• Simplified administration• Robust client support • Home billing of COBRA and COBRA administration• No need to shop for insurance every year
Employee Benefits• A voice in a personal decision – healthcare • Choice of plan types (e.g., HMO, EPO, POS, PPO, HSA)• Choice of insurer• Annual choice to meet individual healthcare and budget requirements• Pre-Tax contributions (thru Section 125) minimize out of pocket costs• Robust member and advocacy services

© HealthPass 2011 15
How Exchanges Affect Health Plans
© HealthPass 2011 16
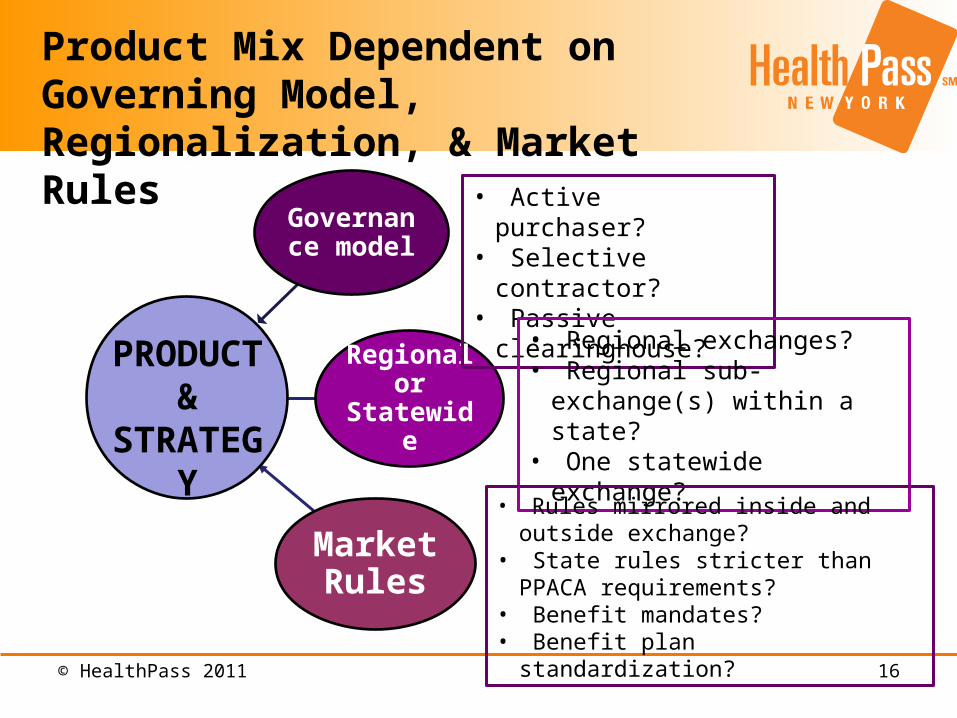
Product Mix Dependent on Governing Model, Regionalization, & Market Rules
Governance model
Regional or Statewide
Market Rules
PRODUCT &
STRATEGY
• Active purchaser?• Selective contractor?• Passive clearinghouse?
• Regional exchanges?• Regional sub-exchange(s) within
a state?• One statewide exchange?
• Rules mirrored inside and outside exchange?
• State rules stricter than PPACA requirements?
• Benefit mandates?• Benefit plan standardization?
© HealthPass 2011 17
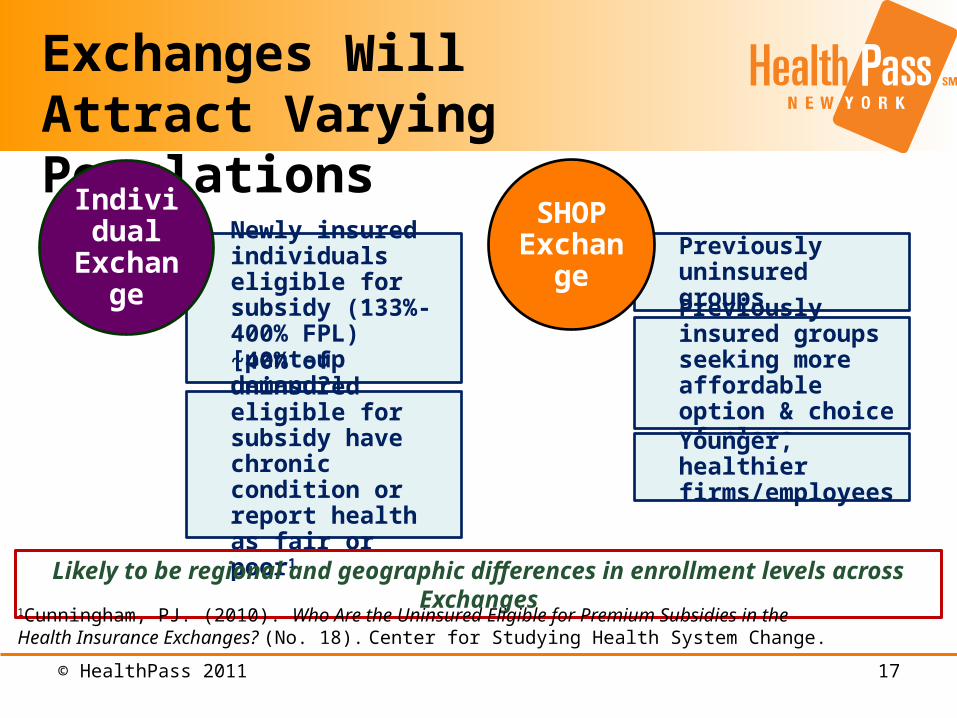
Exchanges Will Attract Varying Populations
Newly insured individuals eligible for subsidy (133%-400% FPL) [pent-up demand?]
~40% of uninsured eligible for subsidy have chronic condition or report health as fair or poor1
Individual Exchange Previously uninsured
groups
Previously insured groups seeking more affordable option & choice of plans
Younger, healthier firms/employees
SHOP Exchange
Likely to be regional and geographic differences in enrollment levels across Exchanges
1Cunningham, PJ. (2010). Who Are the Uninsured Eligible for Premium Subsidies in the Health Insurance Exchanges? (No. 18). Center for Studying Health System Change.
© HealthPass 2011 18
• Exchange enrollment projections CBO: 24-30 million enrollees by 20191
Urban Institute/RWJF: 44 million enrollees by 20172
23 million in AHBE; 21 million in SHOP• Brand & marketing/outreach will matter, especially with
standardized options Competition based on value, quality, & member services Efficient administration
• Demonstrate ongoing value• National & regional start-up carriers will consider entering markets• Medical loss ratio (MLR) considerations
Other Considerations
1Congressional Budget Office. (2010) Estimate of the direct spending and revenue effects of an amendment in the nature of a substitute to H.R. 4872, the Reconciliation Act of 2010. Washington, DC: U.S. Government Printing Office.2Buettgens M, Bowen G and Holahan J. (2010). America Under the Affordable Care Act. Washington, DC: Urban Institute.
© HealthPass 2011 19
SHOP Exchanges must be designed to serve employers & their employees
States must charge their Exchange with a premium aggregation function
It is crucial that States develop their SHOP & AHBE Exchanges simultaneously; give AHBE & SHOP Exchanges equal attention
States should consider full employee choice & a fixed-dollar defined contribution SHOP Exchange model
Design Exchanges to be nimble enough to respond to market forces; their success depends on it
Policy Recommendations
1
2
3
4
5

© HealthPass 2011 20
Questions
Q & A

© HealthPass 2011 21
Contact Information
Shawn Nowicki, MPHDirector, Health Policy
61 BroadwaySuite 2705(212) 252-8010 [email protected]