lv dysfunction vasospasm and ischemia hypertension vte conduction disease arrhythmias
TRANSCRIPT

MUGA scans &
monitoring of chemotherapy

Cardiovascular complications of Chemotherapy

LV dysfunction Vasospasm and ischemia Hypertension VTE Conduction disease Arrhythmias
Cardiac effects of Chemotherapy

Chemotherapeutic agents associated with LV dysfunction
Anthracyclines Doxorubicin
(Adriamycin) Epirubicin (Ellence) Idarubicin (Idamycin
PFS)
Alkylating agents Cyclophosphamide
(Cytoxan) Ifosfamide (Ifex)
Antimetabolites Clofarabine (Clolar)
Antimicrotubule agents Docetaxel (Taxotere)
• Monoclonal antibody-based tyrosine kinase inhibitors• Bevacizumab (Avastin)• Trastuzumab (Herceptin)
• Proteasome inhibitor• Bortezomib (Velcade)
• Small molecule tyrosine kinase inhibitors• Dasatinib (Sprycel)• Imatinib mesylate
(Gleevec)• Lapatinib (Tykerb)• Sunitinib (Sutent)
Yeh et al, Circulation 2004
Chemotherapeutic agents associated with Ischemia Antimetabolites
◦ Capecitabine (Xeloda)◦ Flurouracil (Adrucil)
Mab based-TKI◦ Bevacizumab (Avastin)
Small molecule TKI◦ Erlotinib (Tarceva)◦ Sorafenib (Nexavar)
Antimicrotubule agents◦ Paclitaxel (Taxol)◦ Docetaxel (Taxotere)

Chemotherapeutic agents associated with Hypertension
Mab based-TKI◦ Bevacizumab (Avastin)
Small molecule TKI◦ Sorafenib (Nexavar)◦ Sunitinib (Sutent)
Chemotherapeutic agents associated with venous thromboembolism Alkylating agents
◦ Cisplatin Angiogenesis inhibitors
◦ Lenalidomide (Revlimid)◦ Thalidomide (Thalomid)
Small molecule TKI◦ Erlotinib (Tarceva)
Histone deacetylase inhibitor◦ Vorinostat (Zolinza)
Chemotherapeutic agents associated with conduction disease/bradycardia Angiogenesis inhibitors
◦ Thalidomide (Thalomid) Antimicrotubule agents
◦ Paclitaxel (Taxol)

Chemotherapeutic agents associated with QTc prolongation Histone deacetylase inhibitor
◦ Vorinostat (Zolinza) Misc
◦ Arsenic trioxide• Small molecule tyrosine kinase inhibitors
• Dasatinib (Sprycel)• Lapatinib (Tykerb)• Nilotinib (Tasigna)
LV dysfunction and chemotherapy

Type 1 Type II
Doxorubicin Trastuzumab
Cellular destruction Cellular dysfunction
Cumulative /Dose dependent Non-cumulative /Non dose dependent
Usually irreversible Usually reversible.
Types of cardiotoxicity
Ewer 2008
Anthracyclines

Dose related toxicity Incidence of Doxorubicin-induced HF is
3% to 5% with 400 mg/m2, 7% to 26% at 550 mg/m2, 18% to 48% at 700 mg/m2 Maximum lifetime cumulative dose for
doxorubicin is 400 to 550 mg/m2 . Epirubicin or Idarubicin appear to have
less incidence of HF

Risk factors for anthracycline toxicity Cumulative dose; intravenous bolus administration; higher single doses; history of prior irradiation; the use of other concomitant cardiotoxic agents female gender; Underlying cardiovascular disease; age (young
and old age increased length of time since anthracycline
completion

Anthracycline Cardiotoxicity


Trastuzumab

Source and actions of NRG-1 in the heart
Lemmens, K., K. Doggen, and G.W. De Keulenaer, Role of neuregulin-1/ErbB signaling in cardiovascular physiology and disease:
implications for therapy of heart failure. Circulation, 2007. 116(8): p. 954-60.

Electron microscopy evaluation ofendomyocardial biopsy on a patient whodeveloped Trastuzumab-induced cardiactoxicity.
Guarneri, V., et al., Long-term cardiac tolerability of trastuzumab in metastatic breast cancer: the M.D. Anderson Cancer Center
experience. J Clin Oncol, 2006. 24(25): p. 4107-15.
Enlarged and edematous vacuole
Pleomorphic mitochondrion
Z band widening and splitting

Wide variation in definition of cardiotoxicity. Wide range of incidence of asymptomatic LV
dysfunction (3.2% - 33%)
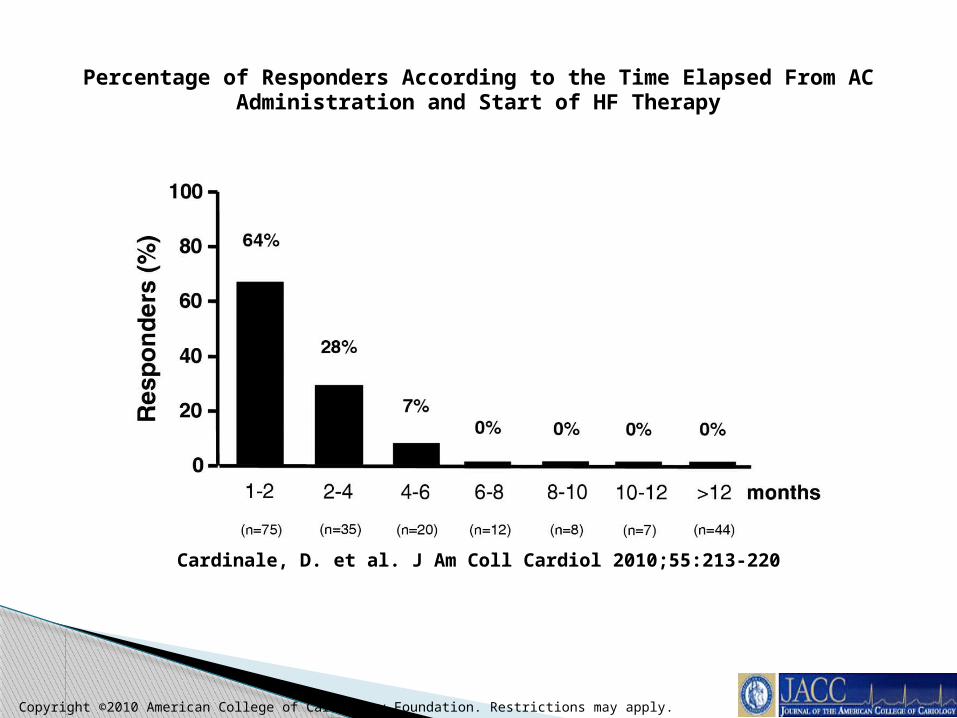
Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Cardinale, D. et al. J Am Coll Cardiol 2010;55:213-220
Percentage of Responders According to the Time Elapsed From AC Administration and Start of HF Therapy

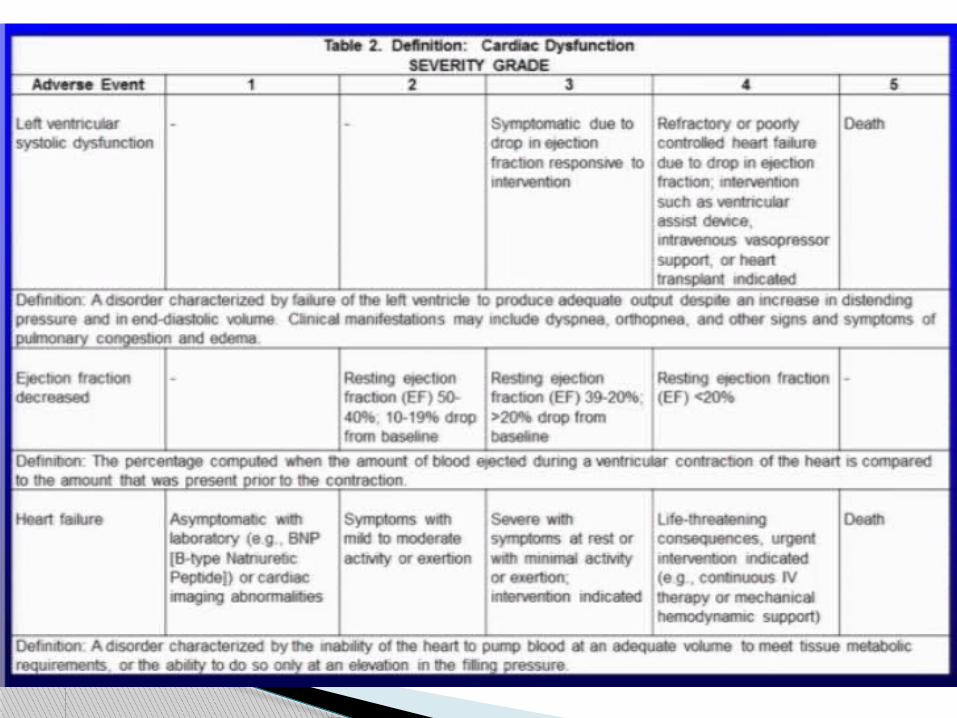
Guidelines….(depends on who you ask)

So, how do you define cardiotoxicity?

The oncologist’s perspective
ACC/AHA?

Stages in the evolution of HF and recommended therapy by stage.
et al. Circulation 2001;104:2996-3007
Copyright © American Heart Association
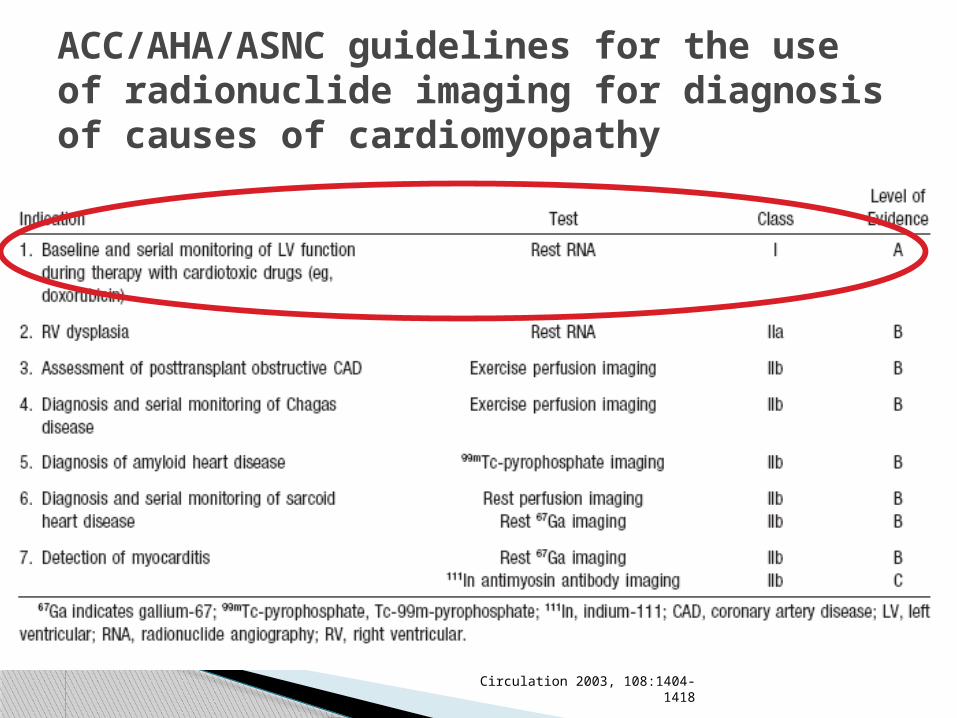
ACC/AHA/ASNC guidelines for the use of radionuclide imaging for diagnosis of causes of cardiomyopathy
Circulation 2003, 108:1404-1418

Normal LVEF >50% at baseline◦ Baseline MUGA within first 100 mg/m2 in all
patients. ◦ Next MUGA 200-300 mg/m2. ◦ Next MUGA 450 mg /m2◦ (400 mg/m2 if high risk- Cyclophosphamide, CAD,
abnormal ECG, mediastinal radiation)◦ MUGA prior to every dose >450 mg/m2
◦ DISCONTINUE IF EF reduces ≥ 10% from baseline AND reaches ≤ 50%
ANSC - monitoring Doxorubicin therapy with serial resting RNA
Schwartz RD et al, Amer J. Med. 82;1109 -1118, 1987

Abnormal LVEF <50% at baseline◦ Baseline MUGA within first 100 mg/m2 in all
patients. ◦ Serial MUGAs prior to each subsequent dose.
◦ DISCONTINUE if LVEF ≥10% from baseline or
absolute LVEF ≤ 30%
ASNC - monitoring Doxorubicin therapy with serial resting RNA

Monitoring
Assessment of EF at 0, 3, 6, 9, 12 months MUGA or Echo with Tissue Doppler assessment Use the same modality in follow up If >10% absolute LVEF reduction but >50% EF, please
follow up with yearly echos . If >10% reduction to <50%, please institute heart
failure therapy and refer to a Cardiologist. If hypertension or DM coexist, please consider ACEI as
first line.


MUGAs are not perfect
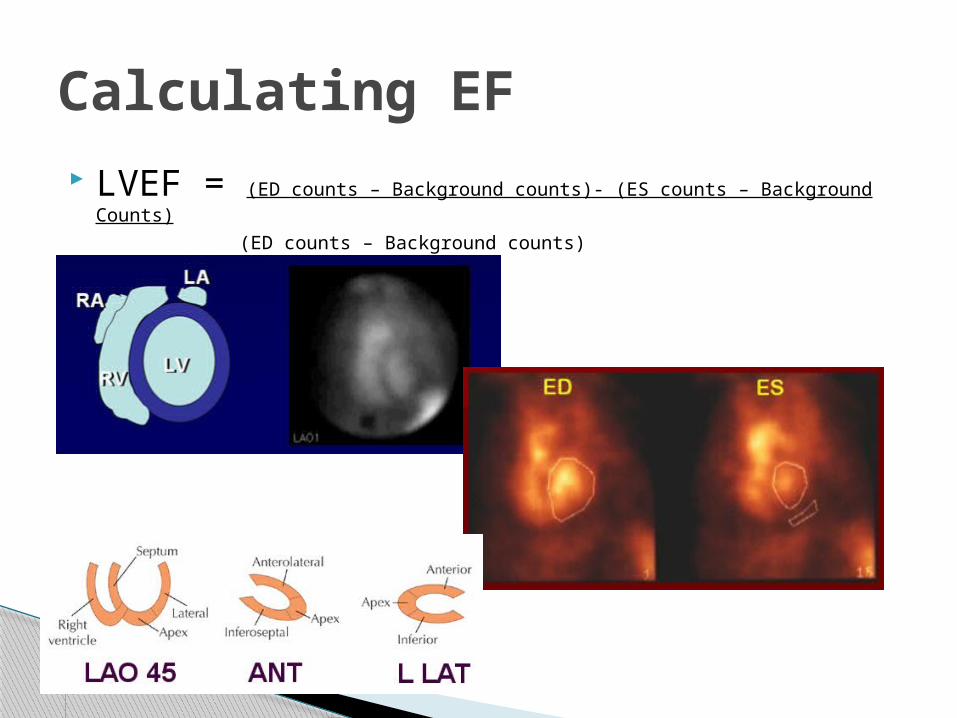
LVEF = (ED counts – Background counts)- (ES counts – Background Counts)
(ED counts – Background counts)
Calculating EF

Digoxin Heparin Hydralazine Penicillin Quinidine Prazosin Methyldopa Quinidine
Poor RBC labelling
Inclusion of LA in ES ROI Inclusion of ascending aorta in ROI Background too dark (falsely low counts) Anterior wall motion abnormality. Temporal smoothing of LV volume curve.
Understimation of EF

Exclusion of LV apex in ES ROI Background counts too high. Inferoposterior wall motion abnormality.
Overestimation of EF

MUGAPros Cons
Easy Inaccurate in many situations (Arrhythmias, drugs, inaccurate ROIs)
“Highly reproducible” Radiation exposure.
“Low interobserver and intraobserver variability. “
Costly – Medicare $291.3SPECT MUGA $759
Standardized against contrast ventriculography EF.
Low temporal and spatial resolution.
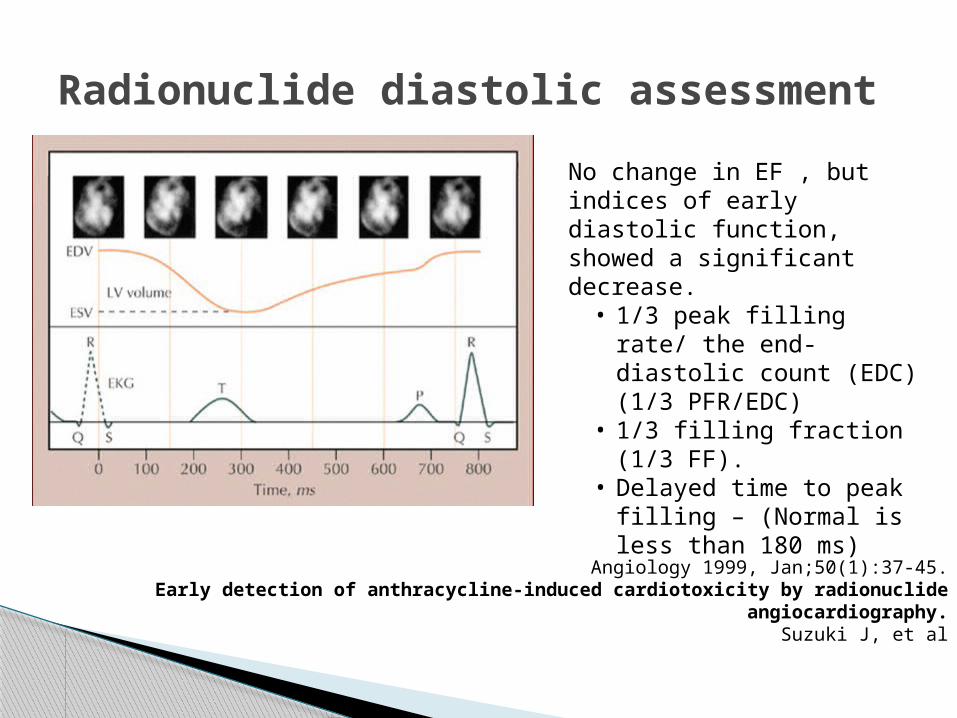
Radionuclide diastolic assessment
No change in EF , but indices of early diastolic function, showed a significant decrease.
• 1/3 peak filling rate/ the end-diastolic count (EDC) (1/3 PFR/EDC)
• 1/3 filling fraction (1/3 FF).
• Delayed time to peak filling – (Normal is less than 180 ms)
Angiology 1999, Jan;50(1):37-45.Early detection of anthracycline-induced cardiotoxicity by radionuclide
angiocardiography.Suzuki J, et al

Salerno M. Multi-modality imaging of diastolic function. J Nucl Cardiol. 2010;17:316–27
Count time curves from a patient prior to (A) and after (B) anthracycline treatment, with marked reduction in the slope of the curve (TPFR) representing abnormal diastolic filling
3 D TTE

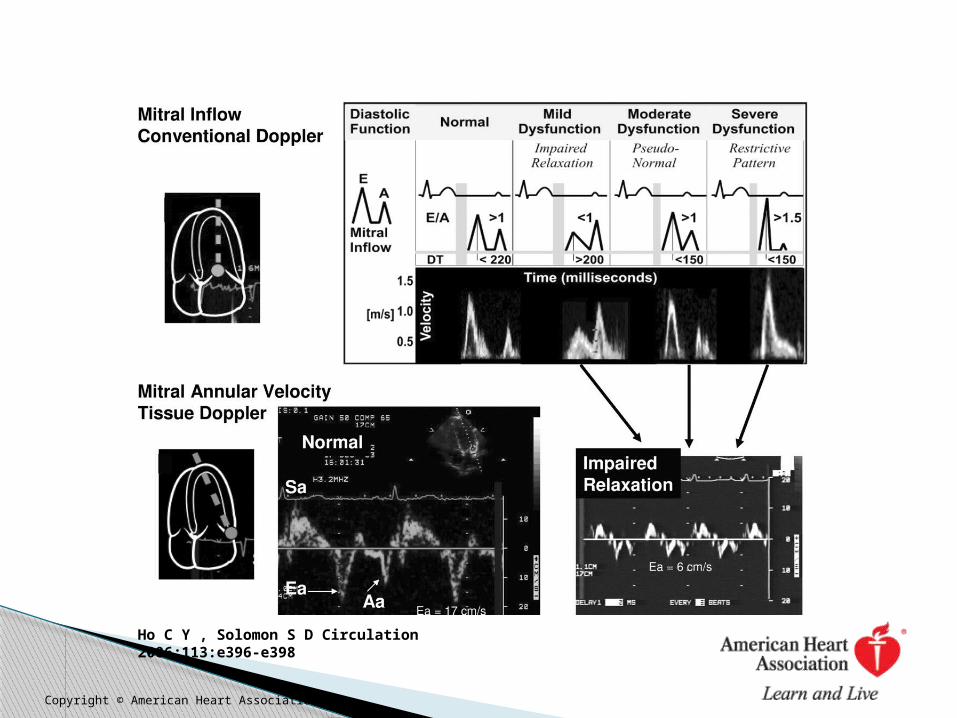
Ho C Y , Solomon S D Circulation 2006;113:e396-e398
Copyright © American Heart Association

Early detection using TDI: Clinical studies
42 Women , mean age 47± 9 years 25 % women developed Trastuzumab mediated
cardiac toxicity at 3 months. TDI parameters: (S′), early diastolic (e′), and late
diastolic (a′) velocities. Doppler-independent strain

Significant difference in the lateral S′ between normals and pts with LV dysfn.
Both peak global longitudinal and radial strain decreased as early as 3 months in the CM group
Biomarkers did not predict injury MUGA EF was decreased in all 10 at 6
month follow up.
Results

www.clinicaltrials.gov >28 open studies looking at monitoring of
cardiotoxicity. 11 looking at CMRI with 4 actively
recruiting.
Future directions