safeguarding adults update protecting adults from abuse and neglect
TRANSCRIPT

.Safeguarding Adults update
Protecting adults from abuse and neglect.
Margaret Panting (1923 to 2001) 78yrs
Steven Hoskin (1967- 2007) 40 years
Care Act 2014
From April 1st 2015.Protecting Adults will be Law.
Section 14 of the Act
No longer “vulnerable” adults definition.
The safeguarding duties; apply to an adult who:has needs for care and support (whether or not the local authority is meeting any of those needs) and;is experiencing, or at risk of, abuse or neglect; and as a result of those care and support needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect.
Safeguarding (2005) - umbrella term;Empowerment - Presumption of person led decisions and informed consent. Protection - Support and representation for those in greatest need. Prevention - It is better to take action before harm occurs. Proportionality – Proportionate and least intrusive response appropriate to the risk presented. Partnership - Local solutions through services working with their communities. Communities have a part to play in preventing, detecting and reporting neglect and abuse. Accountability - Accountability and transparency in delivering safeguarding.
10 Categories of AbusePhysical Abuse
NeglectDiscriminationSexual abuse
Financial abusePsychological abuseOrganisational abuse
*Domestic Abuse*Modern Slavery
*Self Neglect
Self- Neglect• Definition:• Self-neglect – this covers a wide range of behaviour; neglecting to care
for one’s personal hygiene, health or surroundings and includes behaviour such as hoarding that causes a risk of harm.
• Cases of severe self-neglect require management of the balance between protecting the adult from self-neglect against their right to self-determination is a serious challenge. It is not unusual for people to refuse a particular form of care due to lack of insight into the need for intervention.
• Examples may be: A person sends away a home care worker who is tasked to do cleaning or
prepare a meal.A person is incontinent but is reluctant to wear pads. A person with diabetes refuses their insulin injection.All cases of self-neglect recognised in the acute hospital must be referred
to Safeguarding Adults Team.
8
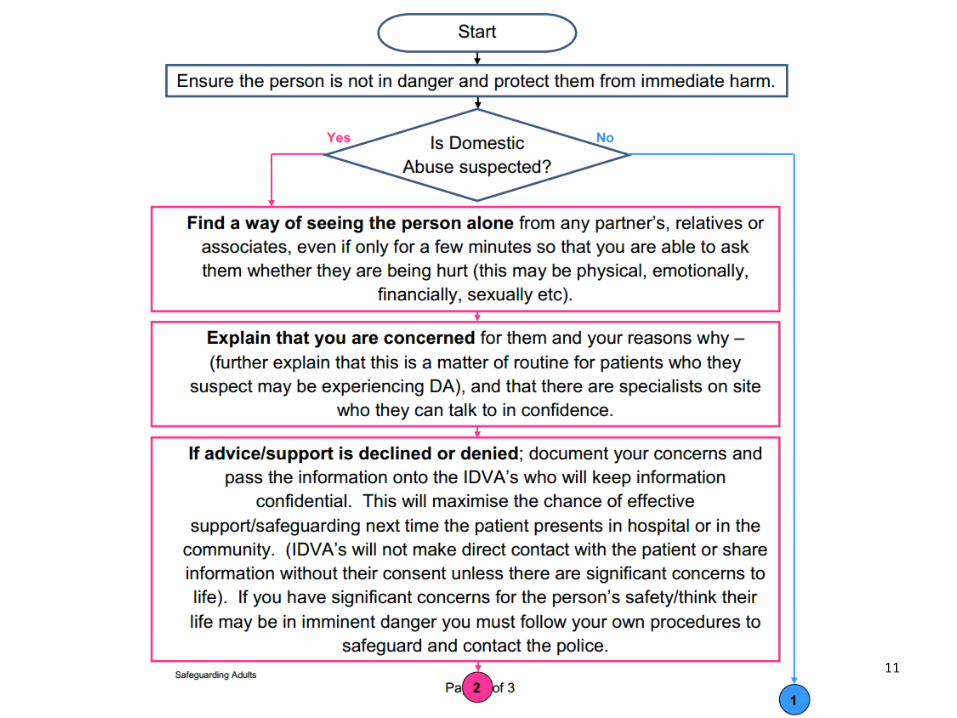
Responding to a Disclosure;• Ask the Adult what they want to happen?
• Follow the Trust’s safeguarding flowchart.Outcomes could be;
Ring Police.
Adult protection referral.
Increase in Package of care
Referral to Domestic violence advocate
Referral for GP or Community matron to follow up
Referral to Adult social care for social worker for assessment.
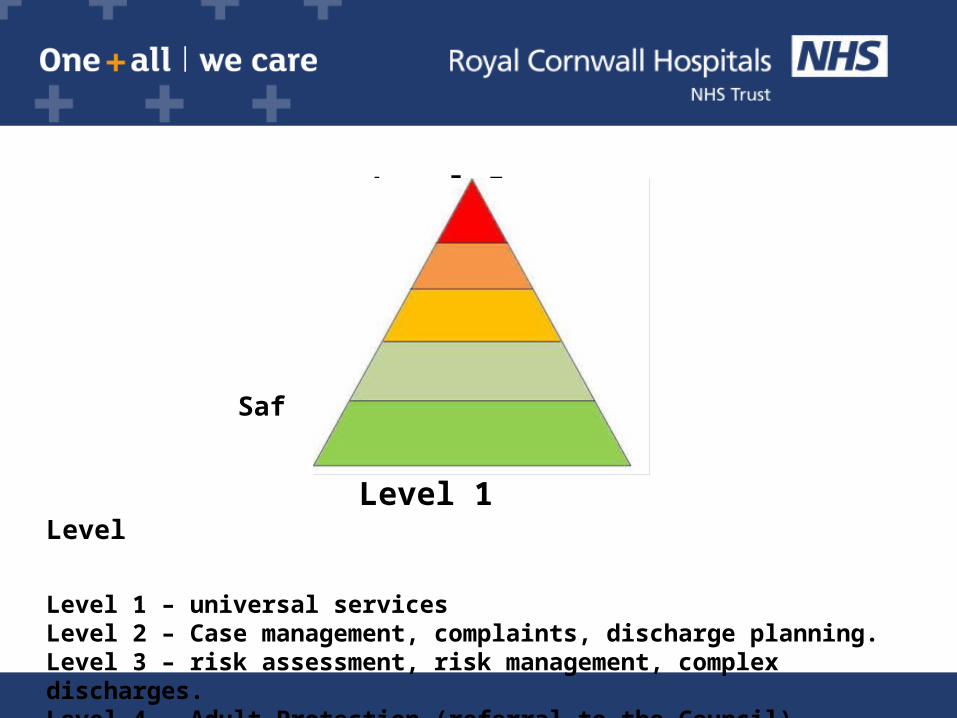
Level 5 Level 4
Level 3
Level 2 Saf Level 1 Level
Level 1 – universal servicesLevel 2 – Case management, complaints, discharge planning.Level 3 – risk assessment, risk management, complex discharges.Level 4 – Adult Protection (referral to the Council)Level 5 – Safeguarding Adults Review (when adults die).
10
Level 4 – Adult Protection (abuse and neglect)
The Role of the Alerter/Referrer.RECOGNISE /RESPOND/REPORT
• If necessary call the police (abuse and neglect is a criminal offence).
• Ensure immediate safety of patient.
• Preserve forensic evidence
• Speak with your line manager – inform the patient – contact Trust’s safeguarding adults team.
• Hand write a report
11
Adult Protection referrals against the Trust.
* Poor discharges, no discharge information, no communication with those looking after the patient post discharge, and they are unable to communicate for themselves.
* Not giving prescribed medication while an inpatient – patient here for 20 hours.
*Patient sent home without recommencing Package of Care. Protection from abuse and neglect
13
Organisational AbuseMid Staffordshire hospital – public enquiry into the
abuse at an acute general hospital.
There was a failure;
•Focus on quality
•Failure to listen to patients
•Failure of the role of the regulator.
14
Organisational Abuse continuedMid Staffordshire hospital – public enquiry of the
abuse in the acute general hospital.
Although, no specific reference to safeguarding; safeguards have been instigated to prevent another mid staffs.
• Francis emphasises the importance of Candour, Openness and Transparency for hospitals.
• Focus on listening to patients.• CQC have improved their inspections, so there is focus on
Quality.• Raising Awareness in the Public Interest policy.

Safeguarding Adults Named Nurse Zoe Cooper – 01872 252446 - Bleep 3048

Email. [email protected] Out of hours leave referrals on answer phone the clinical site co-
ordinators.
Acute Liaison Nurses for Learning Disabilities and / or Autism.
Daniella Rubio-Mayer 07827 903729 Bleep 3054Tristan Coombe 07827 903729 Bleep 3095Jane Rees 07765 221848 Bleep 3053
Learning Disabilities and Autism
For deliberate self harm, mental health assessments or urgent mental health concerns contact the Psychiatric Liaison Team via: Bodmin Hospital Switchboard Ext 1300
For out of hours support contact the Clinical Site Co-ordinators via Switchboard.
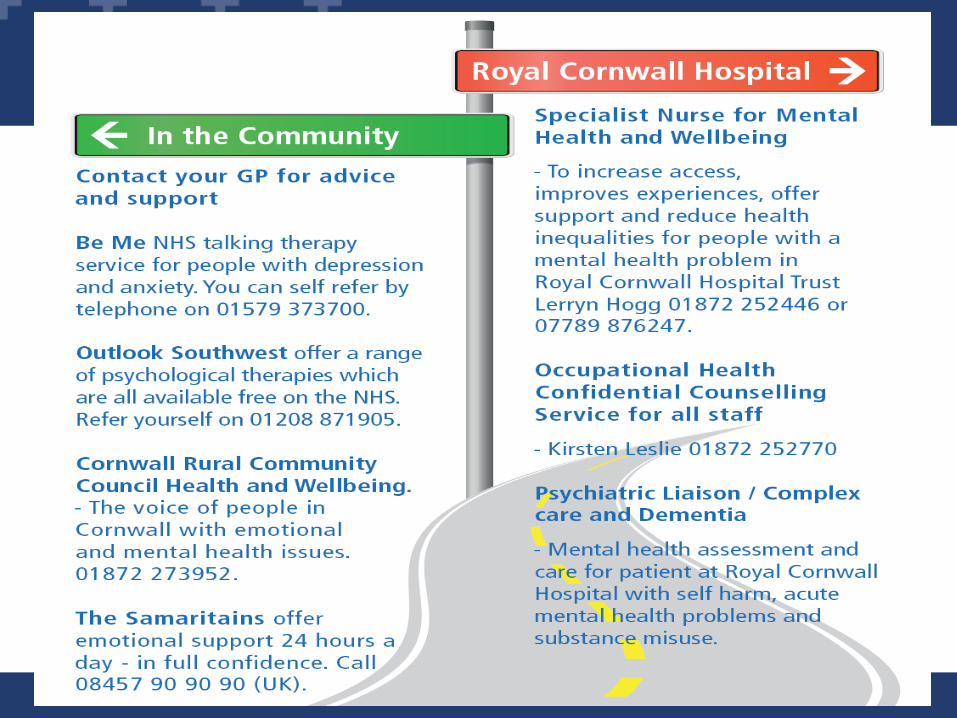
Lerryn Hogg - Specialist Nurse for Mental Health and Wellbeing and Mental CapacityVia: Ext 2446 or Mobile 07789 876247 [email protected]
Mental Health and Mental Capacity
Independent Domestic Violence Advocate (IDVA)
The IDVA is based at RCHTin the safeguarding adults team
Anna Onslow - 07435 752497
Out of Hours leave a message or contactREACH on: 03007774777
Ground Rules
• Confidentiality• Be sensitive to the views and experiences
of others – Challenge the opinion not the person
• Any personal issues around this subject please contact us after the session – or use following contact number/links;
• REACH Project – 01872 241711www.twelvescompany.co.uk
Definition of Domestic AbuseDefinition of Domestic Abuse
“Any incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse between those aged 16 or over who are or have been intimate partners or family members regardless of gender or sexuality. This can encompass, but is not limited to, the following types of abuse:
psychologicalphysicalsexual
financialEmotional
New Government Definition 2013
“Any incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse between those aged 16 or over who are or have been intimate partners or family members regardless of gender or sexuality. This can encompass, but is not limited to, the following types of abuse:
psychologicalphysicalsexual
financialEmotional
New Government Definition 2013
• “Central to the capability required of all NHS staff is the ability to understand the risk factors for, and recognise the signs of, violence and abuse – not all of which are obvious. Clinicians should be more open to the possibility that violence or abuse is an underlying cause of the problems of the patient in front of them.”
• [Role of NHS Taskforce Report]
Some Stats/facts
• We know that there are 7,000 plus Domestic Violence incidents reported to the police in Cornwall each year.
We know that over 50% of Domestic Violence victims don’t report to the police.
• 1 in 4 women and 1 in 6 men will experience DA in their lifetime
• 2 women each week are killed as a result of DV• 35 – the number of times on average that a woman is
assaulted before she will report to the police• A victim will present in E.D approx 30 times before they
are killed• 3 women a week kill themselves as a result of DA, a
further 30 try to.• 90% of children are in the same or next room when DA
takes place.
Scenario• Girl meet boyfriend at 15 years old.• She was now 18 years. IDVA met her in ED (Risk assessment).• Partner very controlling, take her to work, tell her what clothes to wear,
monitor phone calls (high risk factors).• IDVA assessed young girl as high risk - She was at risk of significant harm or
death.• She referred her to MARAC meeting. MARAC plan; alert on address, and
IDVA remained in telephone conversation with victim at work, giving support and advice.
MARAC Multi-Agency Risk Assessment Conference MARAC Multi-Agency Risk Assessment Conference
• Victims referred to a MARAC are of the highest risk with the potential to sustain imminent and serious injury, or to be killed.
• Monthly meetings which take place in each local area.• Currently chaired by the police.• Statutory and Voluntary agencies work together to discuss reducing risk and
increasing safety for victims of DA.• The MARAC considers the HIGHEST risk cases in order to develop a
coordinated safety plan.• This plan may include protection/help for any children or adults (including
the perpetrator) at risk.
MARAC ALERT SYSTEM IN HOSPITAL
• Victims referred to a MARAC are of the highest risk with the potential to sustain imminent and serious injury, or to be killed.
• Monthly meetings which take place in each local area.• Currently chaired by the police.• Statutory and Voluntary agencies work together to discuss reducing risk and
increasing safety for victims of DA.• The MARAC considers the HIGHEST risk cases in order to develop a
coordinated safety plan.• This plan may include protection/help for any children or adults (including
the perpetrator) at risk.
MARAC ALERT SYSTEM IN HOSPITAL
Why Don’t they leave?
• Thinking he/she will change• Fear – afraid of repercussions/Threats• Don’t want to leave the family
home/area/work• Don’t want to disrupt the children• Nowhere to go/Finances• Love & Attachment (Stockholm & trauma
bonding)• Family/religious pressure not to leave/Shame• Believing the violence has been a ‘one off’• Previous experience of reporting/seeking help
– police/social care involvement
To Work effectively with victims of Domestic Abuse,
we MUST have an understanding of
why people remain in abusiverelationships or don’t seek
help.You tube link; Leslie Morgan Steiner; Why DV victims don’t leave.
Safety• Never ask about domestic violence when anybody else is present – this includes
partners, older children and other members of the family.
• You should try and find a way of seeing the patient alone even if they insist on someone else staying with them.
• Ensure privacy – make sure that you cannot be overheard.
• Never advise a person to leave their partner; victims are at high risk of injury or murder when they leave a violent partner.
Some Possible Indicators of Domestic Abuse• Late booking/non-attendance at clinic appointments• Repeated attendances• Non-compliance with treatment regimes/early or self discharge• Minimisation of signs of violence on the body• Repeat presentation with depression, anxiety, self harm, psychosomatic symptoms• Constant presence of partner at examinations who may answer for the patient and be
unwilling to leave the room• Patient is evasive or reluctant to speak in front of or disagree with her/his partner
Health Based Scenario
https://www.youtube.com/watch?v=WgWbPK1L_v0
What would you do?What risk factors can you identify?
Case Study - ‘Mary’74 year old woman admitted to RCHT June 2013 following assault by
husband - disclosed to health staff. Engaged with IDVA; Risk assessment, Safety Plan, MARAC and Adult safeguarding discussed (not ready to leave relationship). No report to police as fearful of being judged for alcohol use. On discharge from RCHT, referral into MARAC and Safeguarding Alert made – processes used to safeguard without raising risk– agreed Social worker would not alert abuser to DA disclosures but use health issues as reason for intervention with whole family.
Mary re-admitted to RCHT again Mar 2014 – further disclosures of DA, fear levels increased, IDVA liaised with Social worker to ascertain patterns of continued controlling behaviour.
With Marys consent IDVA, social care and partner agencies worked together to increase Mary’s confidence and find her alternative, safe, supported housing. Fear levels have decreased, minimal SAFE contact has been maintained with her family.
Further Training
• If in your role you are required to have Child Protection level 3; • You must have Domestic Abuse, Stalking and Harassment and Honour
Based Violence (DASH) awareness training - 1 day training. Please contact [email protected]

Mental Health Awareness
Definition of Mental Health“Mental health is a state of well-being in which every
individual realises his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community.”
"Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.“
2014
True or False?1. 1 in 10 adults will experience a mental health problem in any given year
2. 1 in 10 young people will experience a mental health problem in any given year
3. People with mental health illnesses are usually violent and unpredictable
4. Discrimination against people with mental health problems has reduced significantly in recent years
Mental Health in RCHT
• ¼ of acute inpatients have mental health problems
• Patients with a physical illness are up to 4 times more likely to develop a mental illness
• Patients admitted to a acute setting have a 28% chance of also having a diagnosable psychiatric disorder
(NHS Confederation 2009)
• 41% of patients admitted to a acute setting have symptoms of anxiety or depression
• Treating the mental health needs of acute inpatients has a direct impact on the recovery of their physical health
• Most patients who frequently re-attend the Emergency Department do so because of an untreated mental health problem
(NHS Confederation 2009)
Mental Health in RCHT
What should you do?Assess for risk of suicide or harm
Listen nonjudgmentally
Give reassurance and information
Encourage appropriate professional help
Encourage self-help and other support strategies
Mental Health Act 1983The Mental Health Act 1983 provides a legal framework for the detention of people who are deemed to be suffering from mental disorders.
‘Mental disorder’ means any disorder or disability of the mind
The powers within the Act are mainly used to assess and treat these disorders.
Only a small proportion of people with mental health issues will ever be detained under the Act
Sections of the MHAThe most commonly Used sections of the MHA are:
Section 5(2): Doctors Holding Power – 72 hours
Section 136 and Section 135: Police power – 72 hours
Section 2: Admission for assessment – 28 days
Section 3: Admission for treatment – 6 months
Section 17: Leave of absence – as prescribed
If you would like more support, information or bespoke training with regards to any aspect of mental health contact:
Lerryn Hogg Specialist Nurse Mental Health and WellbeingContact: ext 2638 or 07789 876247 [email protected]
Psychiatric Liaison Team Contact: ext 1300, Bodmin Hospital Switchboard
Out of hours: Clinical Site Co-ordinators Contact: via Switchboard.