| slide 1 of 25 dr rägo 28 april – 2 may 2008 pharmaceutical development with focus on paediatric...
TRANSCRIPT
| Slide 1 of 25 Dr Rägo 28 April – 2 May 2008
Pharmaceutical Development with Focus on Paediatric formulations
Pharmaceutical Development with Focus on Paediatric formulations
WHO/FIP Training Workshop
Hyatt Regency Hotel
Sahar Airport Road
Andheri East, Mumbai, India
28 April 2008 – 2 May 2008
| Slide 2 of 25 Dr Rägo 28 April – 2 May 2008
Pharmacovigilance and safety of medicines in children
Pharmacovigilance and safety of medicines in children
Presented by:
Lembit Rägo MD, PhD
Contact details:Dr Lembit Rägo
Coordinator,
Quality Assurance and Safety: Medicines
Medicines Policy and Standards
World Health Organization
Geneva
Switzerland
E-Mail: [email protected]
| Slide 3 of 25 Dr Rägo 28 April – 2 May 2008
Pharmacovigilance and safety of medicines in children
Pharmacovigilance and safety of medicines in children
Background
What is a problem?
What is WHO doing and planning to do?
Ways forward
| Slide 4 of 25 Dr Rägo 28 April – 2 May 2008
The Erice Manifesto: for global reform of the safety of medicines in patient care
Drug Safety, 2007;30(3):187-90
The Erice Manifesto: for global reform of the safety of medicines in patient care
Drug Safety, 2007;30(3):187-90
The science of pharmacovigilance--monitoring and evaluating drug safety issues and communicating them effectively--is a vital activity of worldwide significance in the safeguarding of patient welfare and public health.
Its clinical, public health and economic importance has been demonstrated, but it needs to be better understood and appreciated by politicians, the media and the public.
Pharmacovigilance is evolving from being a largely reactive discipline, concentrating on the discovery of harm caused by marketed drugs, to a proactive study of their safety, effectiveness and associated risk factors in normal medical practice and use by patients.
| Slide 5 of 25 Dr Rägo 28 April – 2 May 2008
Pharmacovigilance definitionPharmacovigilance definition
Pharmacovigilance is the science and activities relating to the detection, assessment, understanding, and prevention of adverse effects or any other possible medicine-related problems (1)
| Slide 6 of 25 Dr Rägo 28 April – 2 May 2008
BackgroundBackground
Safety monitoring of medicine use in children is of paramount importance since during the clinical development of medicines, only limited data is generated through clinical trials.
Use of medicines outside the specifications described in the license (in terms of formulation, indications, contra-indications, age, etc.) constitutes off-label and off-licence use and these are a major area of concern.
The use of unlicensed and off-label medicines for children has been a common practice for decades, which does not offer the children the same quality, safety and efficacy of medicines as is available for adults
Is the present situation against the UN Convention on the Rights of the Child?
| Slide 7 of 25 Dr Rägo 28 April – 2 May 2008
Safety of paediatric medicines: unrecognized challenge?
Safety of paediatric medicines: unrecognized challenge?
Relatively less or absent safety data as compared to adult use
– Off-label use – no clinical trials, no safety information from trials– Off-label use – reliance on spontaneous reporting, but …– Difficulties of identifying ADRs in paediatric populations
Specific safety issues due to – Anatomy– Physiology

| Slide 8 of 25 Dr Rägo 28 April – 2 May 2008
Pharmaceutical development and safety:suitability of dosage forms
Pharmaceutical development and safety:suitability of dosage forms
Tablets not optimal below 3 yrs, even for 3-6 yrs– Four children under 36 months died by choking on albendazole tablets
during a deworming campaign in Ethiopia in 2007. Forcing very small children to swallow large tablets may cause choking and asphyxiation. For younger than 36 months tablets are discouraged. The formulation should be a safe single dose formulation (e.g. granules, liquid for oral use etc.) to replace the tablets currently in use.
Development of formulations of strengths suitable for administration to neonates, infants and young children should be considered. Administration of adult formulations requires dilution or administration of
miniscule volumes to be administered over a period of time. This leads to administration errors (intra-venous drips running fast, errors in dosage calculation and dilution), especially in circumstances that require urgent actions (as in emergency units, premature units and paediatric and neonatal intensive care units).
| Slide 9 of 25 Dr Rägo 28 April – 2 May 2008
Pharmaceutical development and safety:suitability of excipients
Pharmaceutical development and safety:suitability of excipients
Benzyl alcohol is commonly used as preservative in multidose injectable pharmaceutical preparations. For this purpose, concentrations in the range of 0,5 – 2% are used and the whole amount of benzyl alcohol injected is generally very well tolerated. Concentrations of 0,9% are used in Bacteriostatic Sodium Chlorine (USP) and Bacteriostatic Water for intravenous use (USP).
Toxic effects of benzyl alcohol including respiratory vasodilatation, hypertension, convulsions and paralysis have been known for years. However, little is known about the toxic effects or levels of benzyl alcohol and the metabolic acidosis caused by accumulation of the metabolite benzoic acid in neonates, especially in sick premature infants. Deaths in neonates were associated with administration of 99 to 234 mg/kg/day in large volume parenteral solutions or endotracheal solutions.
FDA has recommended that neither intra-muscular flushing solutions containing benzyl alcohol nor dilutions with this preservative should be used in newborn infants.
| Slide 10 of 25 Dr Rägo 28 April – 2 May 2008
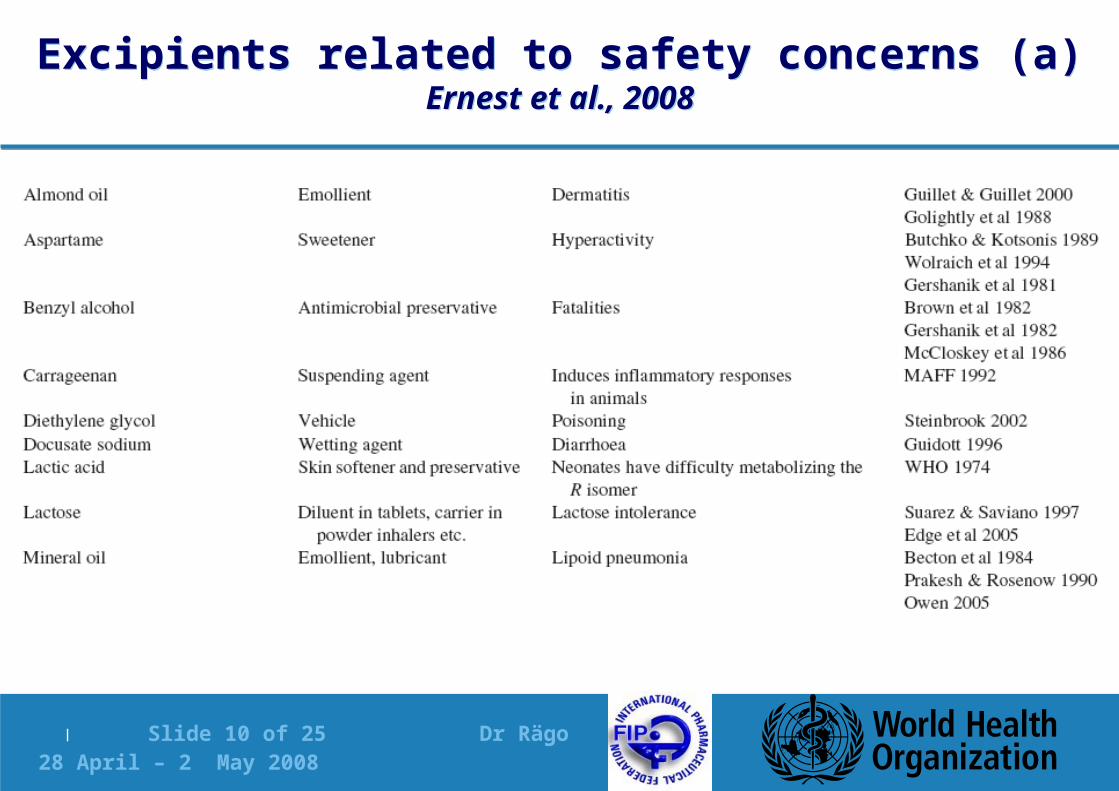
Excipients related to safety concerns (a)Ernest et al., 2008
Excipients related to safety concerns (a)Ernest et al., 2008
| Slide 11 of 25 Dr Rägo 28 April – 2 May 2008
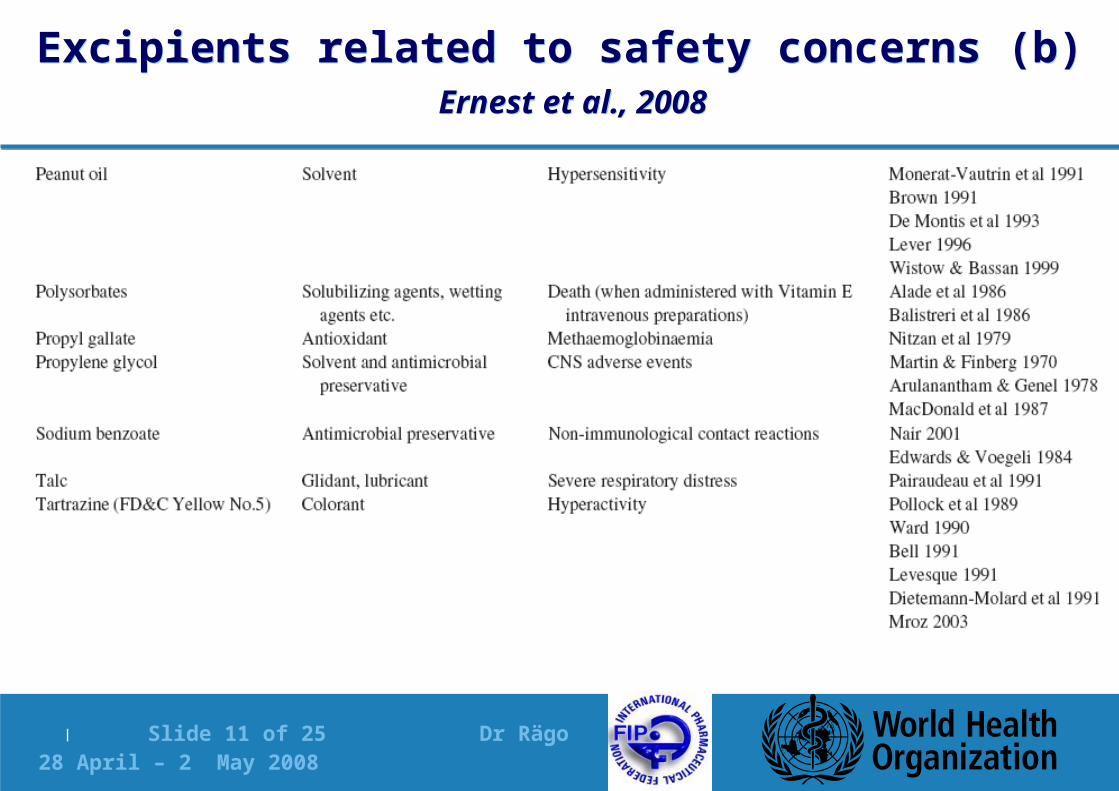
Excipients related to safety concerns (b) Ernest et al., 2008
Excipients related to safety concerns (b) Ernest et al., 2008
| Slide 12 of 25 Dr Rägo 28 April – 2 May 2008
Are regulations addressing the problem?Are regulations addressing the problem?
Legislative initiatives to stimulate paediatric research: push (legal obligations) and pull (positive incentives)
– US has been ahead of Europe– Recently European Commission took a legislative initiative:
Regulation 1901/2006 which entered into force on 26 January 2007 is not ideal but hopefully boosts paediatric research
Specific guidelines such as ICH guidelines
Not enough activities in well resourced settings (ICH countries – EU, Japan and US) and practically no activities in non-ICH countries
| Slide 13 of 25 Dr Rägo 28 April – 2 May 2008
US legislative actions: more clinical data in children US legislative actions: more clinical data in children
US provision in the 1997 Food and Drug Administration (FDA) Modernisation Act. The American "pediatric exclusivity" provision provides a 6 month patent extension for companies willing to perform paediatric clinical investigations at the request of the FDA.
In 2001 it was said to have resulted in studies being undertaken on over 70 diseases and conditions specific to children, with 32% of these studies covering neonates and infants. According to the FDA, "the pediatric exclusivity provision has done more to generate clinical studies and useful prescribing information for the pediatric population than any other regulatory or legislative process to date"
The USA has since enacted two further pieces of legislation: the 2002 Best Pharmaceuticals for Children Act (BPCA) and the 2003 Pediatric Research Equity Act (PREA). The former extended the paediatric exclusivity provision and provided incentives for off-patent products, while the latter granted the FDA the authority to demand that companies provide paediatric studies in specific cases, changing what had been a voluntary scheme.
| Slide 14 of 25 Dr Rägo 28 April – 2 May 2008
EU initiativesEU initiatives
Legislation came into force in January 2007 (Regulation (EC) (15) 1902/2006 of the European Parliament and of the Council, amending Regulation (EC) (16) 1901/2006 on medicinal products for paediatric use).
Aims to enhance the safety of medicines for children by increasing research, development and authorisation of medicines based on specific paediatric experience, without subjecting the paediatric population to unnecessary clinical trials.
It creates requirements for the pharmaceutical industry regarding the development of medicines for paediatric use, as well as providing incentives to industry for such developments. A framework to manage the operation of the legislation, including creation of a scientific paediatric committee is also addressed.
| Slide 15 of 25 Dr Rägo 28 April – 2 May 2008
ICH E11: Clinical Investigation of Medicinal Products in the Paediatric Population
ICH E11: Clinical Investigation of Medicinal Products in the Paediatric Population
Addresses the clinical investigation of medicinal products in the paediatric population but it does not address the problem of off-label use.
Children undergo various stages of physiological development. Moreover, they represent a wide spectrum of physiological and developmental stages from the newborns through adolescents, before they become adults.
Each of these stages may have a different need and response to any drug. Studies performed in adults do not always reflect what happens in children. Extrapolating information from studies that have been carried out in adults can only be done to a limited extent
| Slide 16 of 25 Dr Rägo 28 April – 2 May 2008
Adverse drug reactions in clinical trialsSammons et al, 2008
Adverse drug reactions in clinical trialsSammons et al, 2008
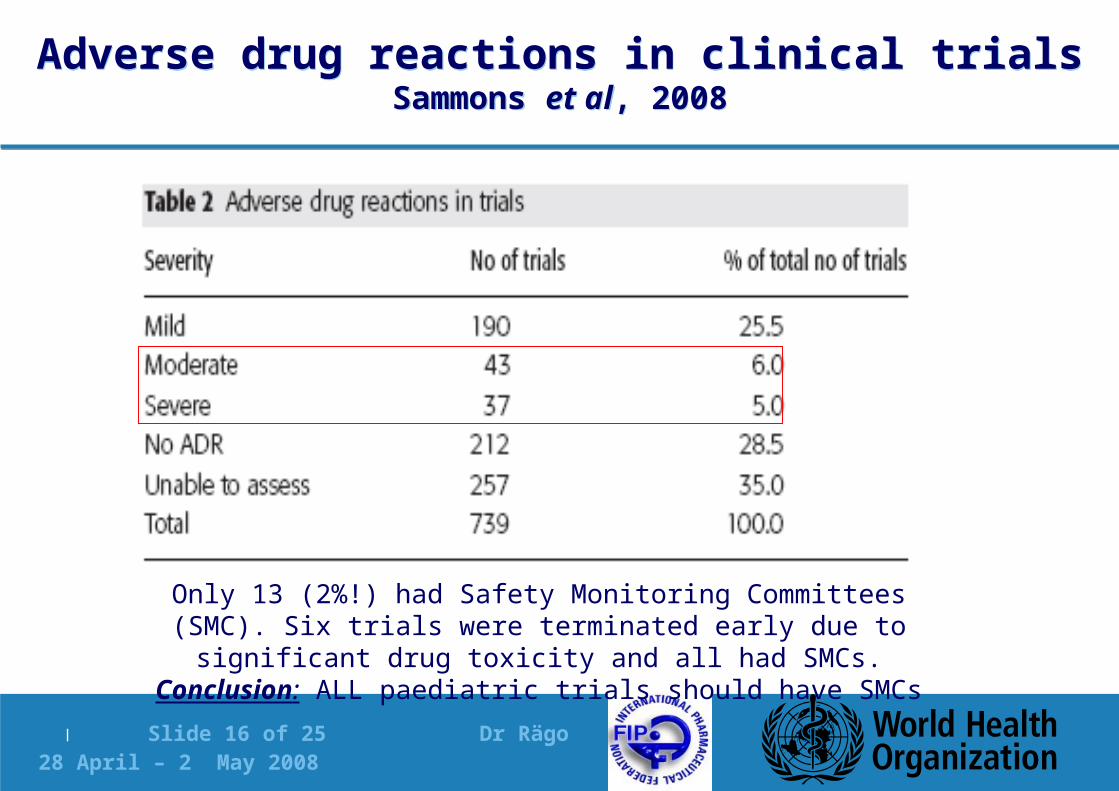
Only 13 (2%!) had Safety Monitoring Committees (SMC). Six trials were terminated early due to significant drug toxicity and all had
SMCs. Conclusion: ALL paediatric trials should have SMCs
| Slide 17 of 25 Dr Rägo 28 April – 2 May 2008
ICH E2E: Pharmacovigilance Planning ICH E2E: Pharmacovigilance Planning
The ICH E2E addresses the issue of paediatrics as an important subpopulation to be taken into account in developing a risk management plan.
The safety specification addresses the populations potentially at-risk (where the product is likely to be used) such as children, and outstanding safety questions which warrant further investigation to refine understanding of the benefit-risk profile during the post-approval period.
The pharmacovigilance plan provides details of planned pharmacoepidemiological studies to be performed (more details in the EMEA guideline on Conduct of Pharmacovigilance for Medicines used by the Paediatric Population, 28 June 2006).
However, this all concerns ONLY new medicines
| Slide 18 of 25 Dr Rägo 28 April – 2 May 2008
Obstacles related to ADR reporting in paediatric patients in resource poor settings
Obstacles related to ADR reporting in paediatric patients in resource poor settings
Lack of medically qualified staff
Lack of incentives, experience and skills in reporting ADRs and ADEs
High proportion of off-label and unlicenced use
Virtually all medicines OTC
High level of poorly evaluated phytotherapeutic, ayurvedic, anthroposophic, traditional and homeopathic medications, which are considered as “soft” and less toxic medicines among parents, caretakers and even health professionals
Irrational use of medicines, including overuse of antibiotics etc.
| Slide 19 of 25 Dr Rägo 28 April – 2 May 2008
WHO and medicines safety in childrenWHO and medicines safety in children
2nd meeting of the Advisory Committee on Safety of Medicinal Products (ACSoMP), 27-29 October 2004, WHO, Geneva
– Recommended that the issue of safety of medicines in children is an important issue that needs to be addressed
– Several actions were also recommended …including promoting safety of medicines in children
| Slide 20 of 25 Dr Rägo 28 April – 2 May 2008
Promoting Safety of Medicines for ChildrenWHO, 2007 (pp 1- 60)
Promoting Safety of Medicines for ChildrenWHO, 2007 (pp 1- 60)
Text on the web as follows: www.who.int/entity/medicines/publications/essentialmedicines/Promotion_safe_med_childrens.pdf
WHO Book Shop for orders: http://www.who.int/bookorders/anglais/detart1.jsp?sesslan=1&codlan=1&codcol=15&codcch=705
| Slide 21 of 25 Dr Rägo 28 April – 2 May 2008
Content (2) Content (2)
1. Introduction
2. Current situation
2.1 Present status of medicine treatment in children and adolescents around the world
2.2 Consequences of present status
2.3 General risk factors that predispose children to develop an ADR
2.4 Differences between the paediatric subpopulations and adults
2.5 The need for additional, independent paediatric medicines development studies
2.6 Legal and regulatory framework
2.7 Consequences of the lack of medicine development studies in children and authorization of paediatric medicines
3. The essential role of safety monitoring in the life cycle of a medicine
3.1 Pre-marketing medicine safety assessment
3.2 Post-marketing medicine safety monitoring for all medicines available in the market including those used “off-label”
3.3 Risk to benefit considerations in children
| Slide 22 of 25 Dr Rägo 28 April – 2 May 2008
Content (2)Content (2)
4. Medication errors
5. Primary responsibility of stakeholders
6. Guidance: Measures to be taken
6.1 Improvement of awareness among stakeholders
6.2 Methods, approaches, and structural changes for an effective medicine safety monitoring system at the national level
6.3 Installation of methods and structural changes for an effective medicine safety monitoring system at the national level
6.4 Impact measurement and audit
7. Measures to be taken by WHO
Annex I
Pharmacovigilance methods
Annex 2
Recent information on ADRs to marketed medicines in children
| Slide 23 of 25 Dr Rägo 28 April – 2 May 2008
ConclusionsConclusions
Safety of medicines in paediatric populations remains challenging for both well resourced and resource poor settings
All stake holders have a role and obligation to improve safety of medicines in children
Developing proper paediatric formulations can contribute to the safety of medicines in children, reduce suffering and save lives
| Slide 24 of 25 Dr Rägo 28 April – 2 May 2008
ReferencesReferences
1. The Importance of Pharmacovigilance; Safety Monitoring of Medicinal Products, WHO Geneva, 2002
2. Ernest TB et al.(2007), Developing paediatric medicines: identifying the needs and recognizing the challenegs. Journal of Pharmacy and Pharmacology, 59:1043-1055