aaglaagl.org/2012syllabus/pg103.pdf · sponsored by aagl advancing minimally invasive gynecology...
TRANSCRIPT

Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Pelvic Anatomy: Skill Set for the
Savvy Minimally Invasive Surgeon –
Generalist, Urogynecologist, Oncologist
(Didactic)
PROGRAM CHAIR
Jubilee Brown, MD
Peter M. Lotze, MD R. Wendel Naumann, MD

Professional Education Information Target Audience Educational activities are developed to meet the needs of surgical gynecologists in practice and in training, as well as, other allied healthcare professionals in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 3 Pelvic Sidewall Anatomy and Retroperitoneal Spaces J. Brown ........................................................................................................................................................ 4 Anatomy of the Pelvic Floor P.M. Lotze .................................................................................................................................................. 14 Dissecting the Ureter R.W. Naumann ........................................................................................................................................... 18 Identifying Blood Vessels and Controlling Hemorrhage J. Brown ...................................................................................................................................................... 24 Nerves: Finding and Avoiding Them R.W. Naumann ........................................................................................................................................... 32 Vaginal Support and Uterosacral Ligaments P.M. Lotze .................................................................................................................................................. 41 Ligaments and Anatomy Important in Pelvic Reconstructive Surgery P.M. Lotze .................................................................................................................................................. 45 Identifying Retroperitoneal Structures to Stay Safe and Get Out of Trouble J. Brown ...................................................................................................................................................... 49 Cultural and Linguistics Competency ......................................................................................................... 52

PG 103 Pelvic Anatomy: Skill Set for the Savvy Minimally Invasive Surgeon –
Generalist, Urogynecologist, Oncologist (Didactic)
Jubilee Brown, Chair Faculty: Peter M. Lotze, R. Wendel Naumann
Course Description
This course is designed for advanced minimally invasive gynecologic surgeons who want to enhance their knowledge base and apply it to minimally invasive surgical procedures. The didactic portion of this course will provide detailed instruction on intra- and retroperitoneal pelvic anatomy as it applies to successful general, urogynecologic, and oncologic surgery. Experts in each subspecialty will focus on anatomy and dissection techniques to improve the surgical skills of generalists and subspecialists alike. Practical anatomy will be highlighted with MIS videos throughout, and tips and tricks of optimal dissection will be emphasized.
Learning Objectives At the conclusion of this course, the participant will be able to: 1) Identify and interpret pelvic and retroperitoneal structures; 2) discuss and analyze pelvic support defects, minimally invasive repair techniques, and avoidance of injury during such procedures; 3) detect successful approaches for surgical dissection of pelvic sidewall and retroperitoneal anatomical structures (e.g., ureter, nerves, blood vessels) in patients with complex anatomy; and 4) distinguish retroperitoneal spaces and apply these landmarks to minimally invasive surgical dissection.
Course Outline 8:00 Welcome, Introduction, and Course Overview J. Brown 8:10 Pelvic Sidewall Anatomy and Retroperitoneal Spaces J. Brown 8:35 Anatomy of the Pelvic Floor P.M. Lotze 9:00 Dissecting the Ureter R.W. Naumann 9:25 Identifying Blood Vessels and Controlling Hemorrhage J. Brown 9:50 Questions & Answers 10:00 Break 10:15 Nerves: Finding and Avoiding Them R.W. Naumann 10:40 Vaginal Support and Uterosacral Ligaments P.M. Lotze
1

11:05 Ligaments and Anatomy Important in Pelvic Reconstructive Surgery P.M. Lotze 11:30 Identifying Retroperitoneal Structures to Stay Safe and Get Out of Trouble J. Brown 11:55 Questions & Answers 12:00 Course Evaluation and Lunch
2
PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor Consultant: Conceptus Incorporated Frank D. Loffer, Executive Vice President/Medical Director, AAGL* Linda Michels, Executive Director, AAGL* Jonathan Solnik Other: Lecturer - Olympus, Lecturer - Karl Storz Endoscopy-America SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: CooperSurgical, Ethicon Women's Health & Urology, Intuitve Surgical Other: Royalties - CooperSurgical Linda Bradley Grants/Research Support: Elsevier Consultant: Bayer Healthcare Corp., Conceptus Incorporated, Ferring Pharmaceuticals Speaker's Bureau: Bayer Healthcare Corp., Conceptus Incorporated, Ferring Pharm Keith Isaacson Consultant: Karl Storz Endoscopy Rosanne M. Kho Other: Honorarium - Ethicon Endo-Surgery C.Y. Liu* Javier Magrina* Ceana H. Nezhat Consultant: Intuitve Surgical, Lumenis, Karl Storz Endoscopy-America Speaker's Bureau: Conceptus Incorporated, Ethicon Women's Health & Urology William H. Parker Grants/Research Support: Ethicon Women's Health & Urology Consultant: Ethicon Women's Health & Urology Craig J. Sobolewski Consultant: Covidien, CareFusion, TransEnterix Stock Shareholder: TransEnterix Speaker's Bureau: Covidien, Abbott Laboratories Other: Proctor - Intuitve Surgical FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Jubilee Brown* R. Wendel Naumann* Peter M. Lotze* Dobie L. Giles* Asterisk (*) denotes no financial relationships to disclose.
3

Pelvic Sidewall Anatomy and Retroperitoneal Spaces
Pelvic Sidewall Anatomy and Retroperitoneal Spaces
Jubilee Brown, M.D.Jubilee Brown, M.D.Associate ProfessorAssociate Professor
Jubilee Brown, M.D.Jubilee Brown, M.D.Associate ProfessorAssociate ProfessorAssociate ProfessorAssociate Professor
Department of Gynecologic OncologyDepartment of Gynecologic Oncology
Associate ProfessorAssociate Professor
Department of Gynecologic OncologyDepartment of Gynecologic Oncology
I have no financial relationships to I have no financial relationships to disclosedisclose
ObjectivesObjectives
●To review pelvic sidewall anatomy including retroperitoneal spaces
●To describe the approach for safe●To describe the approach for safe laparoscopic dissection
●To view examples of dissection using minimally invasive surgery
►Geared for all gynecologic surgeons
Avascular tissue planesAvascular tissue planesAvascular tissue planesAvascular tissue planes
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
Avascular tissue planesAvascular tissue planesAvascular tissue planesAvascular tissue planes
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
4

Left paravesical spaceLeft paravesical space
Medial wall:
Anterior wall: superior pubic ramus
Medial wall: bladder & vagina
Lateral wall: ext.iliacs, obturator fossa, levator ani
Posterior wall: cardinal ligament
Right paravesical space dissectionRight paravesical space dissection
Right paravesical space dissectionRight paravesical space dissection Right paravesical space dissectionRight paravesical space dissection
Avascular tissue planesAvascular tissue planesAvascular tissue planesAvascular tissue planes
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
Left pararectal spaceLeft pararectal space
Medial wall: rectum & ureter
Lateral wall: i t l ili
Anterior wall: cardinal and uterines
ureterinternal iliacs
Posterior wall: sacrum
5
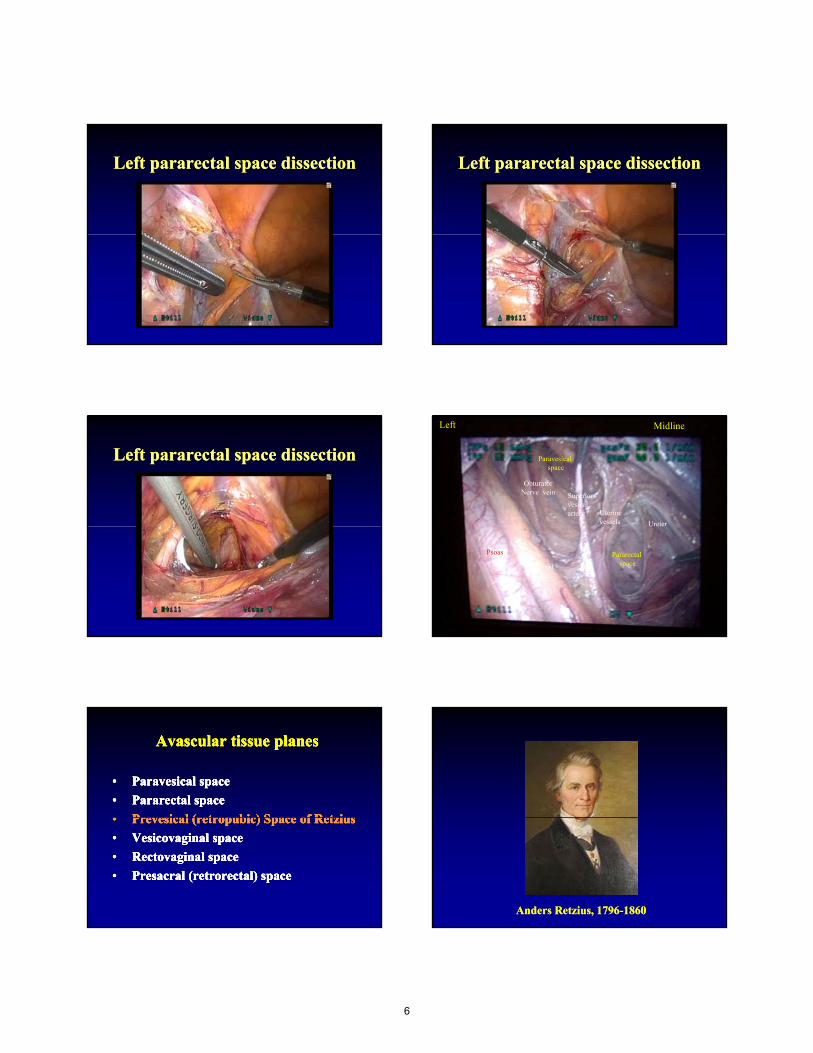
Left pararectal space dissectionLeft pararectal space dissection Left pararectal space dissectionLeft pararectal space dissection
Left pararectal space dissectionLeft pararectal space dissection Paravesical space
Superior vesical artery Uterine
vessels
ObturatorNerve vein
Left Midline
Ureter
Pararectal spaceExternal
iliac artery
Psoas
U ete
Avascular tissue planesAvascular tissue planesAvascular tissue planesAvascular tissue planes
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
Anders Anders RetziusRetzius, 1796, 1796--18601860
6

Anatomic borders of the space of Anatomic borders of the space of RetziusRetziusAnatomic borders of the space of Anatomic borders of the space of RetziusRetzius
•• AvascularAvascular potential space behind the pubic potential space behind the pubic symphysissymphysis and in front of the urinaryand in front of the urinary
•• AvascularAvascular potential space behind the pubic potential space behind the pubic symphysissymphysis and in front of the urinaryand in front of the urinarysymphysissymphysis and in front of the urinary and in front of the urinary bladderbladdersymphysissymphysis and in front of the urinary and in front of the urinary bladderbladder
Space of Space of RetziusRetzius ((retropubicretropubic space)space)
Lateral bordersLateral borders
•• Pubic Pubic symphysissymphysis
•• ObturatorObturator•• ObturatorObturatorinternusinternusmusclemuscle
7

Borders of space of Borders of space of RetziusRetziusBorders of space of Borders of space of RetziusRetzius
•• Urethra and bladder Urethra and bladder rest on anterior rest on anterior vaginal wall (floor)vaginal wall (floor)
•• Urethra and bladder Urethra and bladder rest on anterior rest on anterior vaginal wall (floor)vaginal wall (floor)vaginal wall (floor)vaginal wall (floor)
•• Vagina attaches to Vagina attaches to arcusarcus tendineustendineus fasciafasciapelvis laterally pelvis laterally (becomes lateral (becomes lateral border)border)
vaginal wall (floor)vaginal wall (floor)
•• Vagina attaches to Vagina attaches to arcusarcus tendineustendineus fasciafasciapelvis laterally pelvis laterally (becomes lateral (becomes lateral border)border)
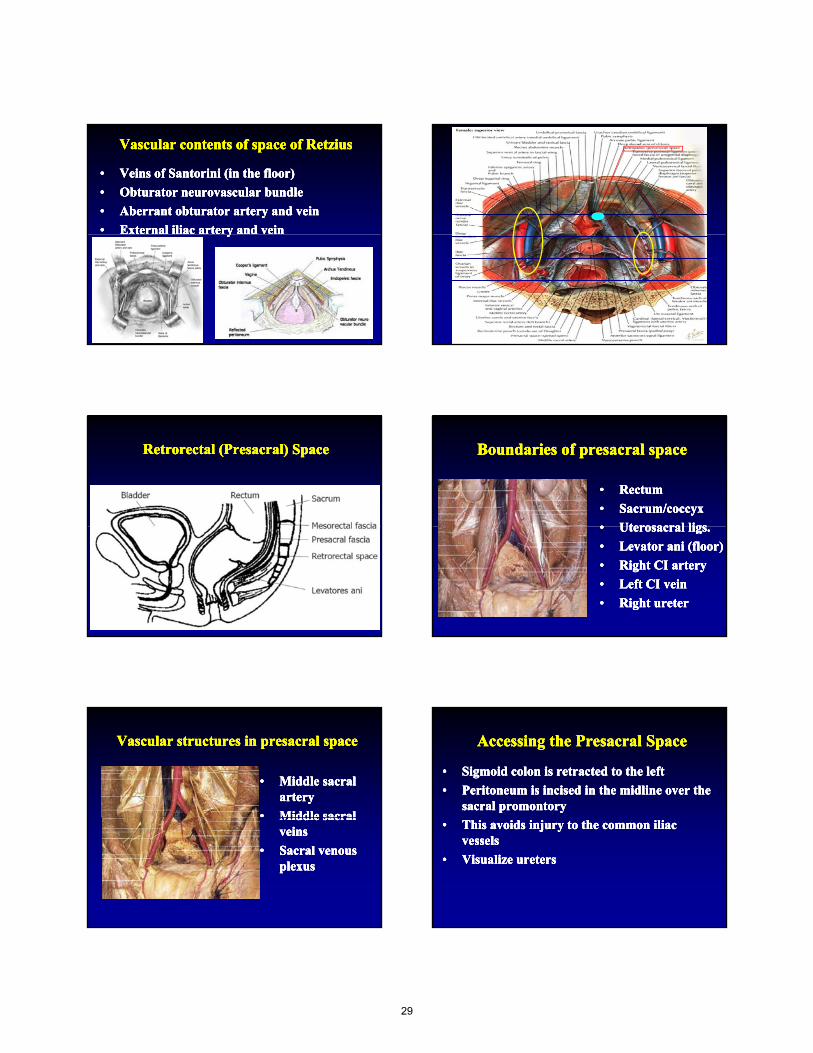
Vascular contents of space of Vascular contents of space of RetziusRetziusVascular contents of space of Vascular contents of space of RetziusRetzius
•• Veins of Veins of SantoriniSantorini (in the floor)(in the floor)
•• ObturatorObturator neurovascular bundleneurovascular bundle
•• Aberrant Aberrant obturatorobturator artery and veinartery and vein
•• External iliac artery and veinExternal iliac artery and vein
•• Veins of Veins of SantoriniSantorini (in the floor)(in the floor)
•• ObturatorObturator neurovascular bundleneurovascular bundle
•• Aberrant Aberrant obturatorobturator artery and veinartery and vein
•• External iliac artery and veinExternal iliac artery and veinyyyy
Access to space of Access to space of RetziusRetziusAccess to space of Access to space of RetziusRetzius
•• Open: divide the rectus muscle in the Open: divide the rectus muscle in the midlinemidline
•• Dissect between the rectus muscleDissect between the rectus muscle
•• Open: divide the rectus muscle in the Open: divide the rectus muscle in the midlinemidline
•• Dissect between the rectus muscleDissect between the rectus muscleDissect between the rectus muscle Dissect between the rectus muscle superficallysuperfically and the peritoneum deep and the peritoneum deep toward pubic toward pubic symphysissymphysis
Dissect between the rectus muscle Dissect between the rectus muscle superficallysuperfically and the peritoneum deep and the peritoneum deep toward pubic toward pubic symphysissymphysis
8
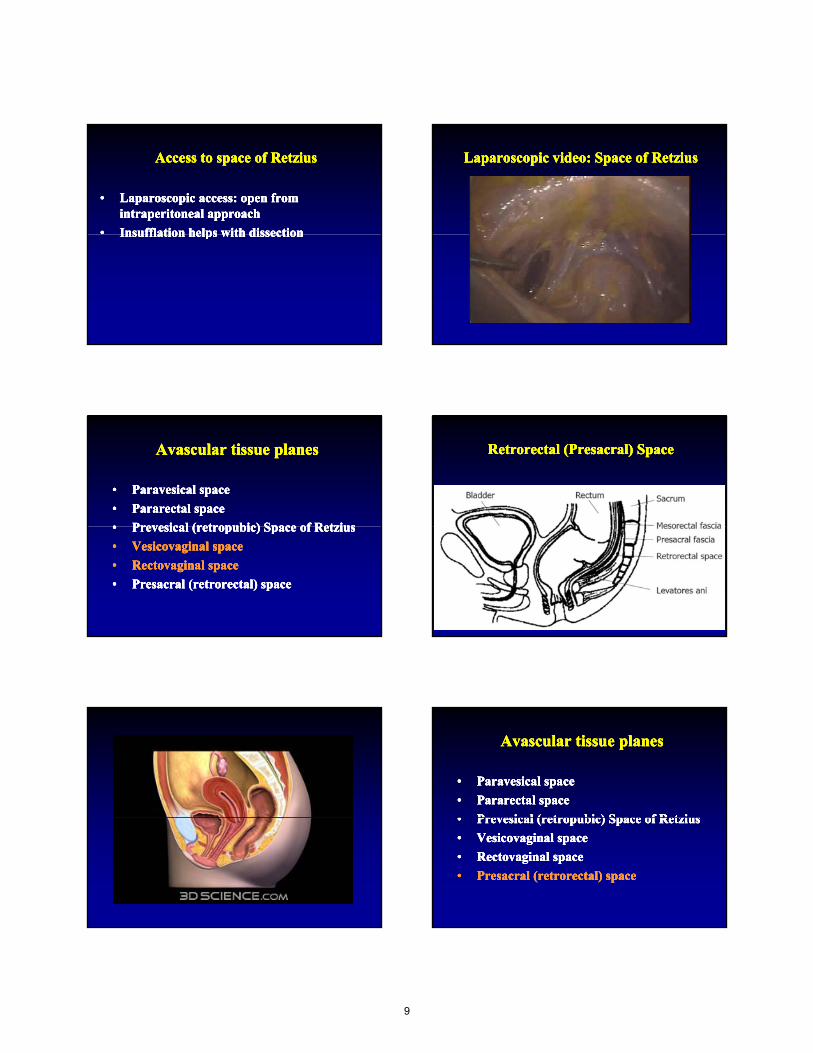
Access to space of Access to space of RetziusRetziusAccess to space of Access to space of RetziusRetzius
•• Laparoscopic access: open from Laparoscopic access: open from intraperitonealintraperitoneal approachapproach
•• InsufflationInsufflation helps with dissectionhelps with dissection
•• Laparoscopic access: open from Laparoscopic access: open from intraperitonealintraperitoneal approachapproach
•• InsufflationInsufflation helps with dissectionhelps with dissectionInsufflationInsufflation helps with dissectionhelps with dissectionInsufflationInsufflation helps with dissectionhelps with dissection
Laparoscopic video: Space of Laparoscopic video: Space of RetziusRetziusLaparoscopic video: Space of Laparoscopic video: Space of RetziusRetzius
Avascular tissue planesAvascular tissue planesAvascular tissue planesAvascular tissue planes
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
RetrorectalRetrorectal ((PresacralPresacral) Space) SpaceRetrorectalRetrorectal ((PresacralPresacral) Space) Space
Avascular tissue planesAvascular tissue planesAvascular tissue planesAvascular tissue planes
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Paravesical spaceParavesical space
•• Pararectal spacePararectal space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
•• Prevesical (retropubic) Space of RetziusPrevesical (retropubic) Space of Retzius
•• Vesicovaginal spaceVesicovaginal space
•• Rectovaginal spaceRectovaginal space
•• Presacral (retrorectal) spacePresacral (retrorectal) space
9
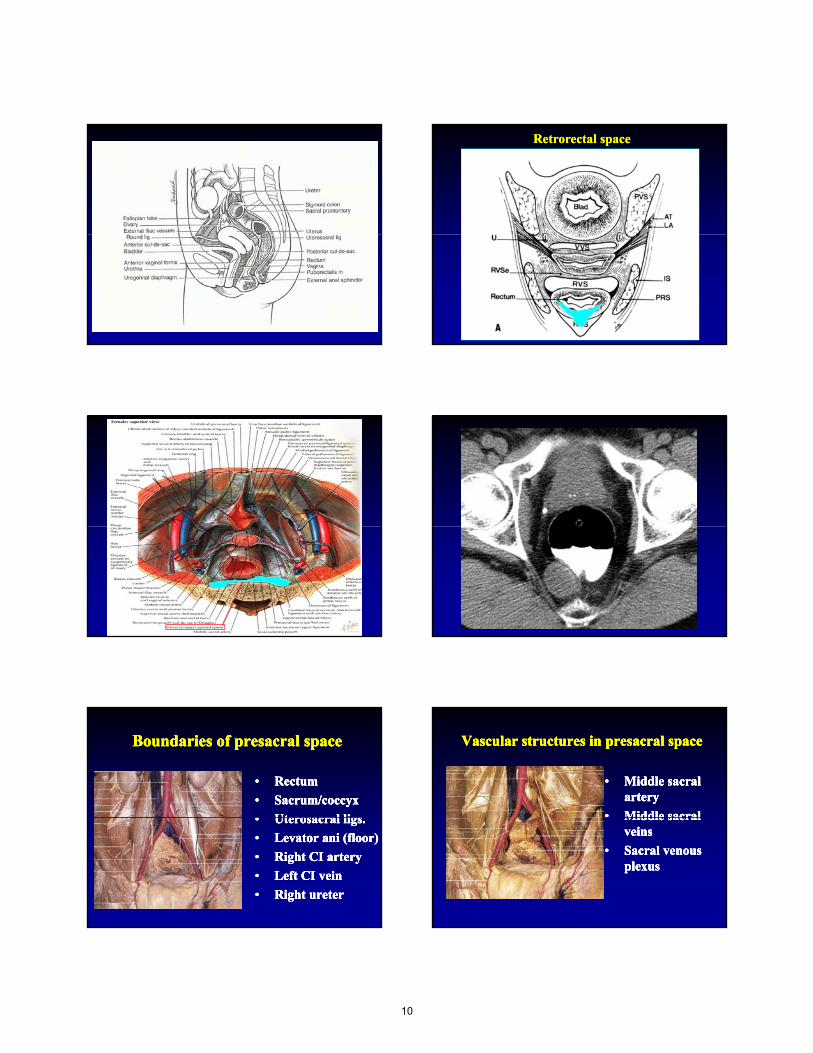
RetrorectalRetrorectal spacespace
Boundaries of Boundaries of presacralpresacral spacespaceBoundaries of Boundaries of presacralpresacral spacespace
•• RectumRectum
•• Sacrum/coccyxSacrum/coccyx
•• UterosacralUterosacral ligsligs
•• RectumRectum
•• Sacrum/coccyxSacrum/coccyx
•• UterosacralUterosacral ligsligs•• UterosacralUterosacral ligsligs..
•• LevatorLevator aniani (floor)(floor)
•• Right CI arteryRight CI artery
•• Left CI veinLeft CI vein
•• Right Right ureterureter
•• UterosacralUterosacral ligsligs..
•• LevatorLevator aniani (floor)(floor)
•• Right CI arteryRight CI artery
•• Left CI veinLeft CI vein
•• Right Right ureterureter
Vascular structures in Vascular structures in presacralpresacral spacespaceVascular structures in Vascular structures in presacralpresacral spacespace
•• Middle sacral Middle sacral arteryartery
•• Middle sacralMiddle sacral
•• Middle sacral Middle sacral arteryartery
•• Middle sacralMiddle sacralMiddle sacral Middle sacral veinsveins
•• Sacral venous Sacral venous plexusplexus
Middle sacral Middle sacral veinsveins
•• Sacral venous Sacral venous plexusplexus
10
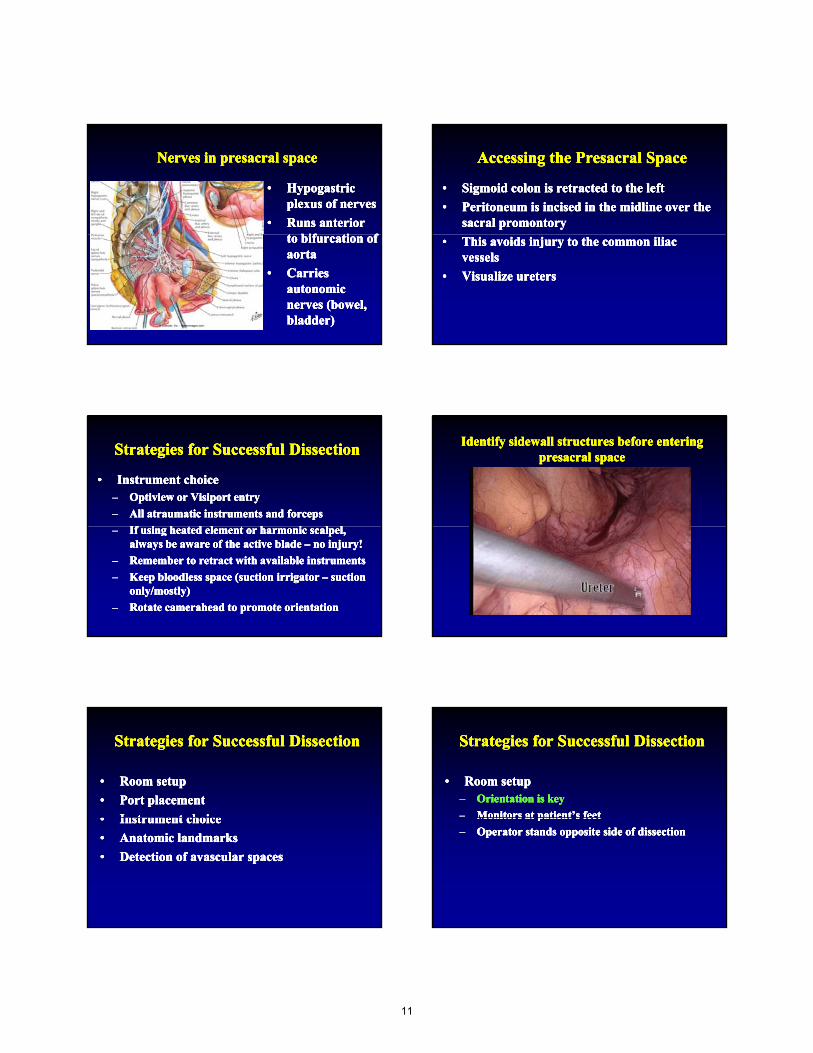
Nerves in Nerves in presacralpresacral spacespaceNerves in Nerves in presacralpresacral spacespace
•• HypogastricHypogastricplexus of nervesplexus of nerves
•• Runs anterior Runs anterior t bif ti ft bif ti f
•• HypogastricHypogastricplexus of nervesplexus of nerves
•• Runs anterior Runs anterior t bif ti ft bif ti fto bifurcation of to bifurcation of aortaaorta
•• Carries Carries autonomic autonomic nerves (bowel, nerves (bowel, bladder)bladder)
to bifurcation of to bifurcation of aortaaorta
•• Carries Carries autonomic autonomic nerves (bowel, nerves (bowel, bladder)bladder)
Accessing the Accessing the PresacralPresacral SpaceSpaceAccessing the Accessing the PresacralPresacral SpaceSpace
•• Sigmoid colon is retracted to the leftSigmoid colon is retracted to the left
•• Peritoneum is incised in the midline over the Peritoneum is incised in the midline over the sacral promontorysacral promontory
•• Sigmoid colon is retracted to the leftSigmoid colon is retracted to the left
•• Peritoneum is incised in the midline over the Peritoneum is incised in the midline over the sacral promontorysacral promontory
•• This avoids injury to the common iliac This avoids injury to the common iliac vesselsvessels
•• Visualize Visualize uretersureters
•• This avoids injury to the common iliac This avoids injury to the common iliac vesselsvessels
•• Visualize Visualize uretersureters
Strategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful Dissection
•• Instrument choiceInstrument choice–– Optiview or Visiport entryOptiview or Visiport entry
–– All atraumatic instruments and forcepsAll atraumatic instruments and forceps
If i h d l h i l lIf i h d l h i l l
•• Instrument choiceInstrument choice–– Optiview or Visiport entryOptiview or Visiport entry
–– All atraumatic instruments and forcepsAll atraumatic instruments and forceps
If i h d l h i l lIf i h d l h i l l–– If using heated element or harmonic scalpel, If using heated element or harmonic scalpel, always be aware of the active blade always be aware of the active blade –– no injury!no injury!
–– Remember to retract with available instrumentsRemember to retract with available instruments
–– Keep bloodless space (suction irrigator Keep bloodless space (suction irrigator –– suction suction only/mostly)only/mostly)
–– Rotate camerahead to promote orientationRotate camerahead to promote orientation
–– If using heated element or harmonic scalpel, If using heated element or harmonic scalpel, always be aware of the active blade always be aware of the active blade –– no injury!no injury!
–– Remember to retract with available instrumentsRemember to retract with available instruments
–– Keep bloodless space (suction irrigator Keep bloodless space (suction irrigator –– suction suction only/mostly)only/mostly)
–– Rotate camerahead to promote orientationRotate camerahead to promote orientation
Identify sidewall structures before entering Identify sidewall structures before entering presacralpresacral spacespace
Identify sidewall structures before entering Identify sidewall structures before entering presacralpresacral spacespace
Strategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful Dissection
•• Room setupRoom setup
•• Port placementPort placement
•• Instrument choiceInstrument choice
•• Room setupRoom setup
•• Port placementPort placement
•• Instrument choiceInstrument choice•• Instrument choiceInstrument choice
•• Anatomic landmarksAnatomic landmarks
•• Detection of avascular spacesDetection of avascular spaces
•• Instrument choiceInstrument choice
•• Anatomic landmarksAnatomic landmarks
•• Detection of avascular spacesDetection of avascular spaces
Strategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful Dissection
•• Room setupRoom setup–– Orientation is keyOrientation is key
–– Monitors at patient’s feetMonitors at patient’s feet
•• Room setupRoom setup–– Orientation is keyOrientation is key
–– Monitors at patient’s feetMonitors at patient’s feetMonitors at patient s feetMonitors at patient s feet
–– Operator stands opposite side of dissectionOperator stands opposite side of dissection
Monitors at patient s feetMonitors at patient s feet
–– Operator stands opposite side of dissectionOperator stands opposite side of dissection
11

Strategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful Dissection
•• Port placementPort placement–– Do not struggleDo not struggle
–– 5 or 10 mm port in umbilicus; bilateral port5 or 10 mm port in umbilicus; bilateral port
•• Port placementPort placement–– Do not struggleDo not struggle
–– 5 or 10 mm port in umbilicus; bilateral port5 or 10 mm port in umbilicus; bilateral port5 or 10 mm port in umbilicus; bilateral port 5 or 10 mm port in umbilicus; bilateral port placement 2placement 2--3 fingerbreadths in and cephalad to 3 fingerbreadths in and cephalad to ASIS, angled to pelvisASIS, angled to pelvis
–– In obese patient, avoid tunnellingIn obese patient, avoid tunnelling
5 or 10 mm port in umbilicus; bilateral port 5 or 10 mm port in umbilicus; bilateral port placement 2placement 2--3 fingerbreadths in and cephalad to 3 fingerbreadths in and cephalad to ASIS, angled to pelvisASIS, angled to pelvis
–– In obese patient, avoid tunnellingIn obese patient, avoid tunnelling
Strategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful Dissection
•• Instrument choiceInstrument choice–– Optiview or Visiport entryOptiview or Visiport entry
–– All atraumatic instruments and forcepsAll atraumatic instruments and forceps
If i h d l h i l lIf i h d l h i l l
•• Instrument choiceInstrument choice–– Optiview or Visiport entryOptiview or Visiport entry
–– All atraumatic instruments and forcepsAll atraumatic instruments and forceps
If i h d l h i l lIf i h d l h i l l–– If using heated element or harmonic scalpel, If using heated element or harmonic scalpel, always be aware of the active blade always be aware of the active blade –– no injury!no injury!
–– Remember to retract with available instrumentsRemember to retract with available instruments
–– Keep bloodless space (suction irrigator Keep bloodless space (suction irrigator –– suction suction only/mostly)only/mostly)
–– Rotate camerahead to promote orientationRotate camerahead to promote orientation
–– If using heated element or harmonic scalpel, If using heated element or harmonic scalpel, always be aware of the active blade always be aware of the active blade –– no injury!no injury!
–– Remember to retract with available instrumentsRemember to retract with available instruments
–– Keep bloodless space (suction irrigator Keep bloodless space (suction irrigator –– suction suction only/mostly)only/mostly)
–– Rotate camerahead to promote orientationRotate camerahead to promote orientation
Strategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful DissectionStrategies for Successful Dissection
•• Anatomic landmarksAnatomic landmarks–– Round ligamentRound ligament–– Psoas musclePsoas muscle
External Iliac ArteryExternal Iliac Artery
•• Anatomic landmarksAnatomic landmarks–– Round ligamentRound ligament–– Psoas musclePsoas muscle
External Iliac ArteryExternal Iliac Artery–– External Iliac ArteryExternal Iliac Artery
•• Detection of avascular spacesDetection of avascular spaces–– Paravesical space entered between Paravesical space entered between
external iliac vein laterally and external iliac vein laterally and superior vesical artery mediallysuperior vesical artery medially
–– Pararectal space follows curve of Pararectal space follows curve of sacrumsacrum
–– External Iliac ArteryExternal Iliac Artery
•• Detection of avascular spacesDetection of avascular spaces–– Paravesical space entered between Paravesical space entered between
external iliac vein laterally and external iliac vein laterally and superior vesical artery mediallysuperior vesical artery medially
–– Pararectal space follows curve of Pararectal space follows curve of sacrumsacrum
Lateral pelvic wall dissectionLateral pelvic wall dissection
Lateral pelvic wall dissectionLateral pelvic wall dissection Lateral pelvic wall dissectionLateral pelvic wall dissection
12

Lateral pelvic wall dissectionLateral pelvic wall dissection
Thank You !
13

Anatomy of the Pelvic Floor
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
DisclosureDisclosureDisclosureDisclosure
• Consultant: Boston Scientific Corp. Inc., Gynecare
2
Lecture ObjectivesLecture ObjectivesLecture ObjectivesLecture Objectives
•• Describe the Bony Anatomy of the Pelvic FloorDescribe the Bony Anatomy of the Pelvic Floor
•• Describe the Skeletal Muscle of the Pelvic FloorDescribe the Skeletal Muscle of the Pelvic Floor
•• Describe the Bony Anatomy of the Pelvic FloorDescribe the Bony Anatomy of the Pelvic Floor
•• Describe the Skeletal Muscle of the Pelvic FloorDescribe the Skeletal Muscle of the Pelvic Floor
3
•• Discuss the Role of the Pelvic Floor MusculatureDiscuss the Role of the Pelvic Floor Musculature•• Discuss the Role of the Pelvic Floor MusculatureDiscuss the Role of the Pelvic Floor Musculature
Pelvic BonesPelvic BonesPelvic BonesPelvic Bones Ilium• Uppermost / largest bone
• Divisible into body, ala• Separation indicated on top surface by curved line (arcuate line), and on external surface by margin of acetabulum
• Body - part of acetabulum (< 2/5)• Wing (ala) - large expanded portion; bounds greater pelvis laterally
4
Ischium• Lower / back part of hip bone (os coxae)
• Situated below ilium / behind pubis• Superior portion forms ~1/3 of acetabulum
Pubis• Covered by mons pubis.• Body, superior and inferior ramus• Body forms 1/5 of acetabulum
SacrumSacrumSacrumSacrum• Typically 5 vertebrae - initially unfused and fuses at ~16–18 y/o (done by 34)
• Sacral promontory - projects forward and articulates with last lumbar vertebra (sacrovertebral angle)
• Centrally - curved posteriorly (allows greater room in pelvis)
• Ala (“wings”) - project laterally
5
Ala ( wings ) project laterally and articulate with ilium at sacroiliac joints
• Upper vs. Lower Half– Lower forms greater angle – Upper half nearly straight– Lower half with greatest
amount of curvature
• In the female sacrum is shorter and wider than a male
Bony AnatomyBony AnatomyBony AnatomyBony Anatomy
6
14

Bony AnatomyBony AnatomyBony AnatomyBony Anatomy
7
Bony AnatomyBony AnatomyBony AnatomyBony Anatomy
8
Important ligamentsImportant ligamentsImportant ligamentsImportant ligamentsSacrospinous ligament (SSL)
• Ischial spine to margins of sacrum / coccyx
• Fibers intermingle with STL
• Covered by Coccygeus muscle
• Greater / Lesser Sciatic Notch defined by
SSL and STL
• Pudendal vessels / nerve behind SSL
• Inferior gluteal artery behind SSL
9
Sacrotuberous ligament (STL)• Ischial tuberosity to lower transverse sacral
tubercles, inferior margins sacrum / upper
coccyx
• Narrow in middle portion of ligament
• Pudendal nerve potentially entrapped
between STL and SSL (perineal pain)
g y
• Prevents posterior rotation of ilium with
respect to sacrum
SSL STL
Skeletal MusculatureSkeletal MusculatureSkeletal MusculatureSkeletal Musculature
10
11
Skeletal MusculatureSkeletal MusculatureSkeletal MusculatureSkeletal MusculaturePiriformisPiriformis
OriginOrigin: S2: S2--4 vertebrae4 vertebraeInsertionInsertion: greater trochanter of femur: greater trochanter of femurInnervationInnervation: S1, S2: S1, S2ActionAction: Rotates thigh laterally: Rotates thigh laterally
CoccygeusCoccygeusOriginOrigin: ischial spine: ischial spine
12
Obturator internusObturator internusOriginOrigin: surface of pelvic bone, : surface of pelvic bone, margin of obturator foramen, ischial margin of obturator foramen, ischial ramus, inferior pubic ramusramus, inferior pubic ramus
InsertionInsertion: greater trochanter of femur: greater trochanter of femurInnervationInnervation: L5, S1, S2: L5, S1, S2ActionAction: rotates thigh laterally: rotates thigh laterally
OriginOrigin: ischial spine: ischial spineInsertionInsertion: lateral sacral border: lateral sacral borderInnervationInnervation: S3, S4: S3, S4ActionAction: Supports / raises coccyx: Supports / raises coccyx
15
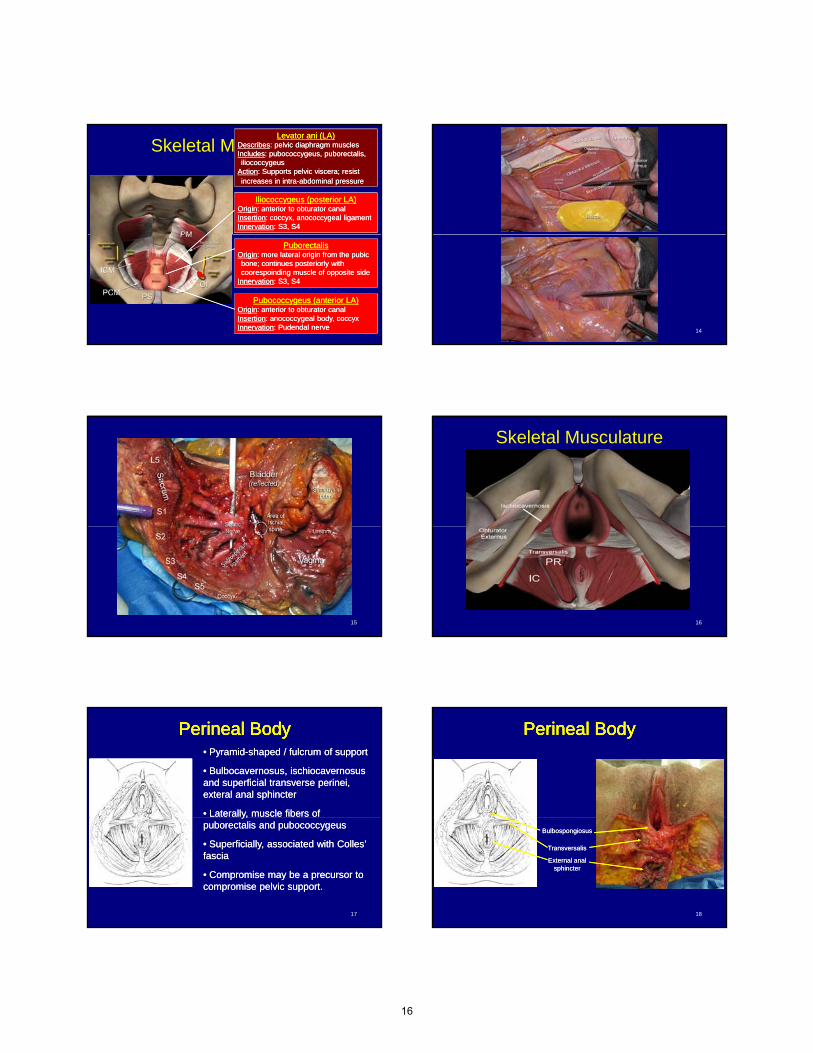
Skeletal MusculatureLevator ani (LA)Levator ani (LA)
DescribesDescribes: pelvic diaphragm muscles : pelvic diaphragm muscles IncludesIncludes: pubococcygeus, puborectalis, : pubococcygeus, puborectalis, iliococcygeus iliococcygeus
ActionAction: Supports pelvic viscera; resist : Supports pelvic viscera; resist increases in intraincreases in intra--abdominal pressureabdominal pressure
Iliococcygeus (posterior LA)Iliococcygeus (posterior LA)OriginOrigin: anterior to obturator canal: anterior to obturator canalInsertionInsertion: coccyx, anococcygeal ligament: coccyx, anococcygeal ligamentInnervationInnervation: S3, S4: S3, S4
13
Pubococcygeus (anterior LA)Pubococcygeus (anterior LA)OriginOrigin: anterior to obturator canal: anterior to obturator canalInsertionInsertion: anococcygeal body, coccyx: anococcygeal body, coccyxInnervationInnervation: Pudendal nerve: Pudendal nerve
PuborectalisPuborectalisOriginOrigin: more lateral origin from the pubic : more lateral origin from the pubic bone; continues posteriorly with bone; continues posteriorly with coorespoinding muscle of opposite sidecoorespoinding muscle of opposite side
InnervationInnervation: S3, S4: S3, S4
14
15
Skeletal Musculature
16
Perineal BodyPerineal BodyPerineal BodyPerineal Body•• PyramidPyramid--shaped / fulcrum of supportshaped / fulcrum of support
•• Bulbocavernosus, ischiocavernosus Bulbocavernosus, ischiocavernosus and superficial transverse perinei, and superficial transverse perinei, exteral anal sphincterexteral anal sphincter
•• Laterally, muscle fibers of Laterally, muscle fibers of
17
y,y,puborectalis and pubococcygeuspuborectalis and pubococcygeus
•• Superficially, associated with Colles’ Superficially, associated with Colles’ fascia fascia
•• Compromise may be a precursor to Compromise may be a precursor to compromise pelvic support.compromise pelvic support.
Perineal BodyPerineal BodyPerineal BodyPerineal Body
18
TransversalisTransversalis
External anal External anal sphinctersphincter
BulbospongiosusBulbospongiosus
16

DeLancey’s level of support
Level I - Uterosacral / Cardinal ligaments - maintain apical positioning of pelvic organs • Compromise risks apical prolapse
Level II - Visceral connective tissue located Anteriorly / Posteriorly / Laterally• Posterior visceral connective tissue referred to as Rectovaginal fascia (Denonvillier’s fascia)
– Attaches laterally to pelvic sidewall beginning at perineal body. – Converges with arcus tendineus fasciae pelvina (ATFP) midway between symphysis and ischial spine – Creates a Y configuration on sidewall
19
Visceral Connective Tissue (“Fascia”)Visceral Connective Tissue (“Fascia”)– Components include elastin & collagen fibers in polysaccharide ground substance– Dynamic tissue which undergoes constant turnover and remodeling – Regarded to be sensitive to hormonal changes
• Compromise risks anterior, lasteral, posterior compartment defects
Level III - Perineal body• Compromise may be a precursor to compromise pelvic support
Connective Tissue SupportConnective Tissue SupportConnective Tissue SupportConnective Tissue Support
AnteriorAnterior
20
Level II Support:Level II Support:Visceral Connective Tissue Visceral Connective Tissue (Anterior, Posterior, Lateral)(Anterior, Posterior, Lateral)
Level I Support:Level I Support:Uterosacral / Cardinal Ligament Uterosacral / Cardinal Ligament
ComplexComplex
AnteriorAnterior
LateralLateral
PosteriorPosteriorUterosacralUterosacralligamentsligaments
The Role of the Levator Ani MusclesThe Role of the Levator Ani MusclesThe Role of the Levator Ani MusclesThe Role of the Levator Ani Muscles
•• Components of “support”:Components of “support”: Levator ani / ligaments and “fascia”Levator ani / ligaments and “fascia”
•• The role of the Levator AniThe role of the Levator Ani
–– Along with visceral connective tissue, it provides support to Along with visceral connective tissue, it provides support to vagina and bladdervagina and bladder
21
•• The pelvic organs rest on the Levator plateThe pelvic organs rest on the Levator plate
–– These muscles contract during increases in abdominal These muscles contract during increases in abdominal pressure, maintaining support pressure, maintaining support
–– Pelvic floor injuries compromises support risking onset of Pelvic floor injuries compromises support risking onset of pelvic organ prolapsepelvic organ prolapse
Anatomy of the Pelvic Floor
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
17
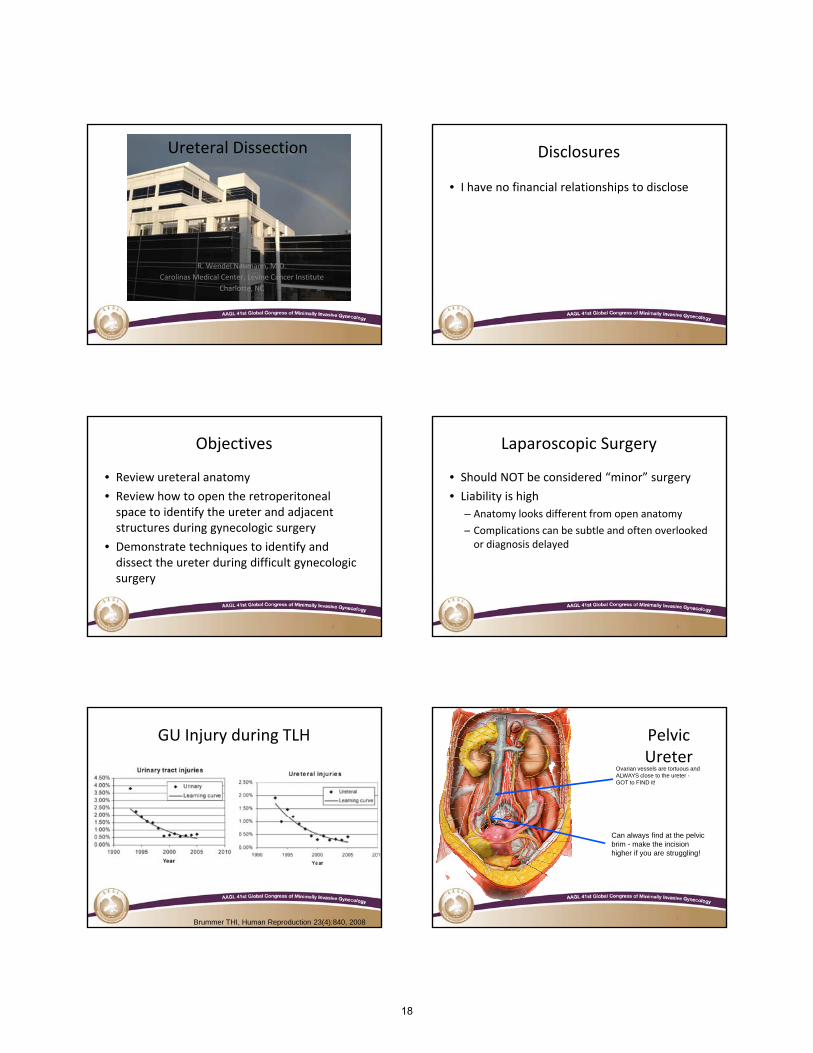
Ureteral Dissection
R. Wendel Naumann, M.D.
Carolinas Medical Center, Levine Cancer Institute
Charlotte, NC
Disclosures
• I have no financial relationships to disclose
22
Objectives
• Review ureteral anatomy
• Review how to open the retroperitoneal space to identify the ureter and adjacent structures during gynecologic surgery
3
structures during gynecologic surgery
• Demonstrate techniques to identify and dissect the ureter during difficult gynecologic surgery
3
Laparoscopic Surgery
• Should NOT be considered “minor” surgery
• Liability is high
– Anatomy looks different from open anatomy
l b b l d f l k d
4
– Complications can be subtle and often overlooked or diagnosis delayed
4
GU Injury during TLH
5Brummer THI, Human Reproduction 23(4):840, 2008
Pelvic Ureter
Ovarian vessels are tortuous and ALWAYS close to the ureter -GOT to FIND it!
6
Can always find at the pelvic brim - make the incision higher if you are struggling!
18
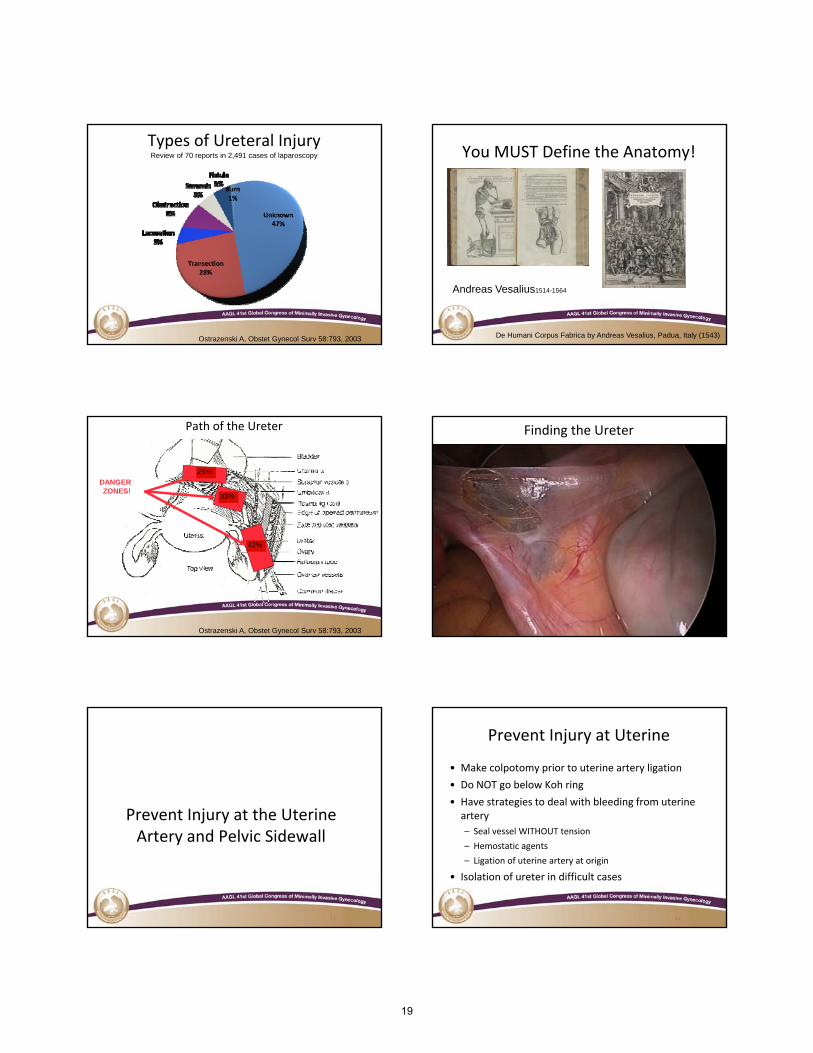
Types of Ureteral InjuryReview of 70 reports in 2,491 cases of laparoscopy
7Ostrazenski A, Obstet Gynecol Surv 58:793, 2003
You MUST Define the Anatomy!
8De Humani Corpus Fabrica by Andreas Vesalius, Padua, Italy (1543)
Andreas Vesalius1514-1564
Path of the Ureter
DANGERZONES!
33%
25%
9
42%
Ostrazenski A, Obstet Gynecol Surv 58:793, 2003
Finding the Ureter
1010
Prevent Injury at the Uterine
11
Prevent Injury at the Uterine Artery and Pelvic Sidewall
Prevent Injury at Uterine
• Make colpotomy prior to uterine artery ligation
• Do NOT go below Koh ring
• Have strategies to deal with bleeding from uterine artery
12
artery
– Seal vessel WITHOUT tension
– Hemostatic agents
– Ligation of uterine artery at origin
• Isolation of ureter in difficult cases
12
19
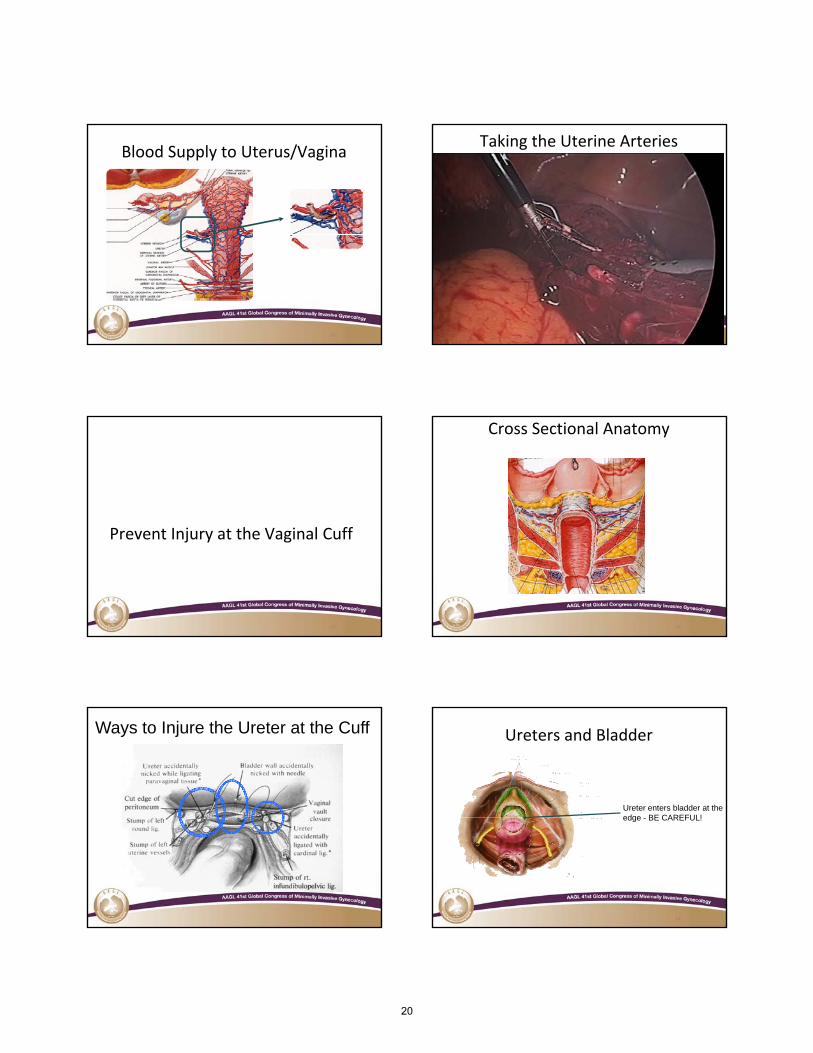
Blood Supply to Uterus/Vagina
13
Taking the Uterine Arteries
1414
15
Prevent Injury at the Vaginal Cuff
Cross Sectional Anatomy
16
Ways to Injure the Ureter at the Cuff Ureters and Bladder
Ureter enters bladder at the edge BE CAREFUL!
18
edge - BE CAREFUL!
20
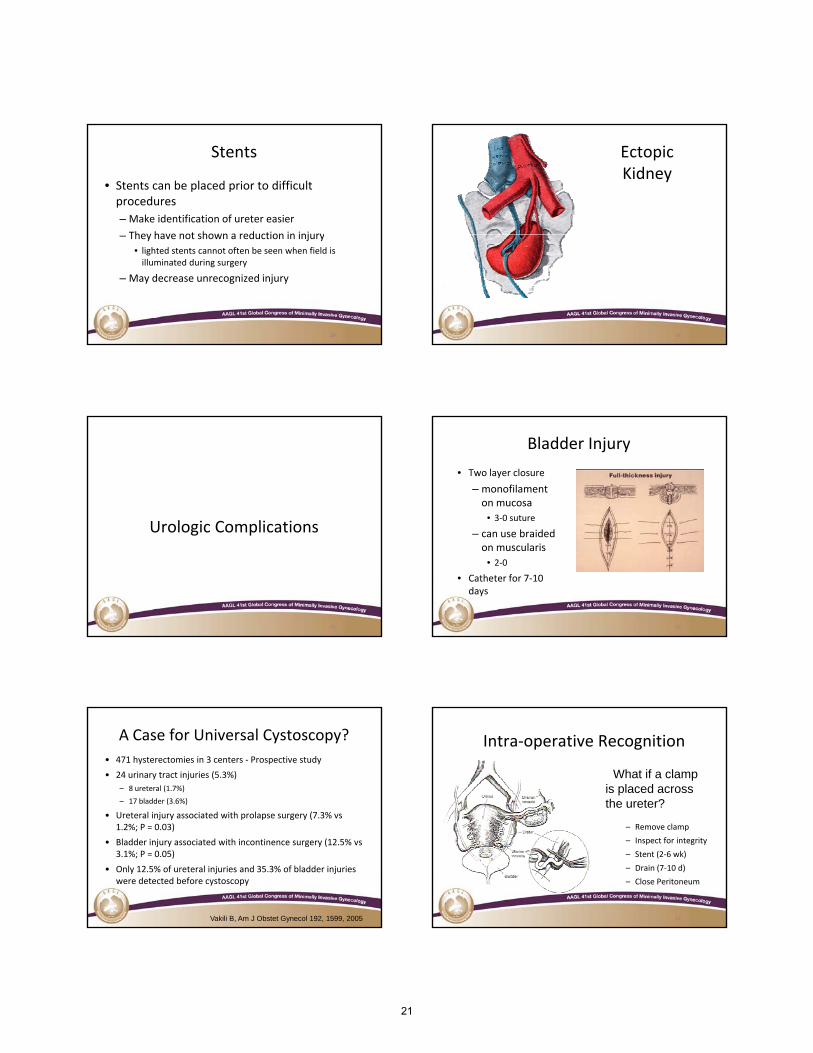
Stents
• Stents can be placed prior to difficult procedures
– Make identification of ureter easier
They have not shown a reduction in injury
19
– They have not shown a reduction in injury
• lighted stents cannot often be seen when field is illuminated during surgery
– May decrease unrecognized injury
19
Ectopic Kidney
20
Urologic Complications
21
Urologic Complications
Bladder Injury
• Two layer closure
– monofilament on mucosa
• 3‐0 suture
22
– can use braided on muscularis
• 2‐0
• Catheter for 7‐10 days
A Case for Universal Cystoscopy?
• 471 hysterectomies in 3 centers ‐ Prospective study
• 24 urinary tract injuries (5.3%)
– 8 ureteral (1.7%)
– 17 bladder (3.6%)
• Ureteral injury associated with prolapse surgery (7.3% vs
23
Ureteral injury associated with prolapse surgery (7.3% vs 1.2%; P = 0.03)
• Bladder injury associated with incontinence surgery (12.5% vs 3.1%; P = 0.05)
• Only 12.5% of ureteral injuries and 35.3% of bladder injuries were detected before cystoscopy
Vakili B, Am J Obstet Gynecol 192, 1599, 2005
Intra‐operative Recognition
• What if a clamp is placed across the ureter?
24
– Remove clamp
– Inspect for integrity
– Stent (2‐6 wk)
– Drain (7‐10 d)
– Close Peritoneum
21
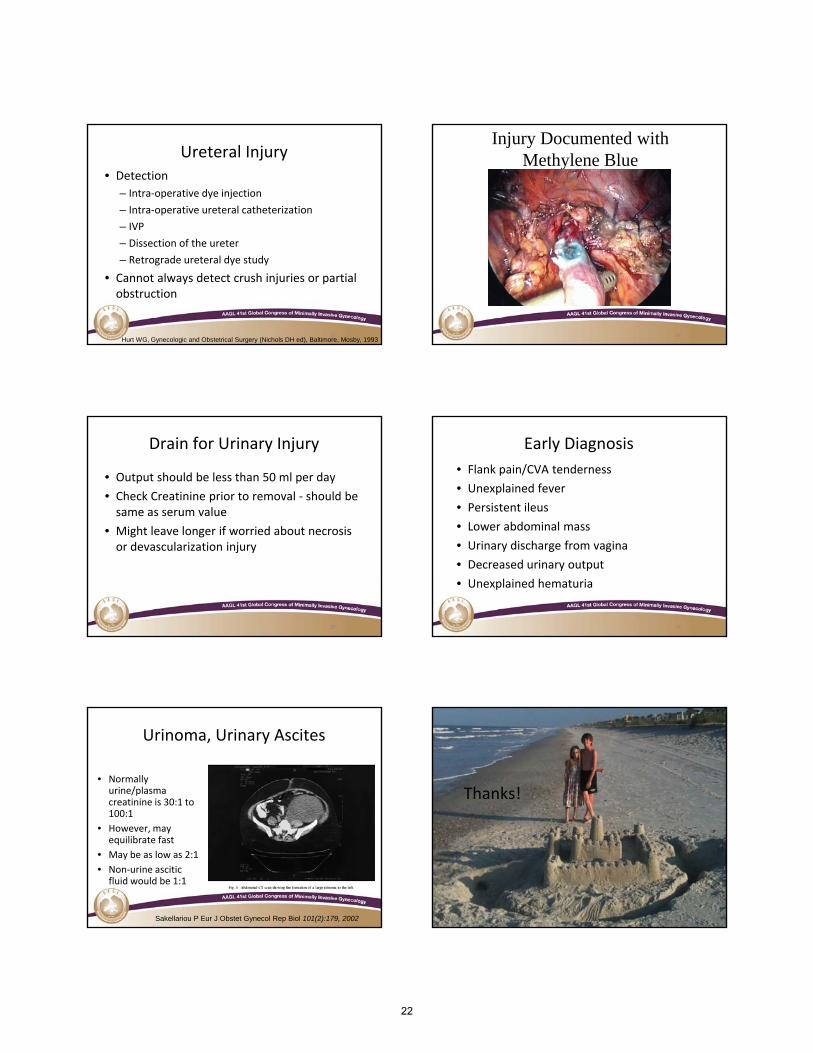
Ureteral Injury• Detection
– Intra‐operative dye injection
– Intra‐operative ureteral catheterization
– IVP
25
– Dissection of the ureter
– Retrograde ureteral dye study
• Cannot always detect crush injuries or partial obstruction
Hurt WG, Gynecologic and Obstetrical Surgery (Nichols DH ed), Baltimore, Mosby, 1993
Injury Documented with Methylene Blue
26
Drain for Urinary Injury
• Output should be less than 50 ml per day
• Check Creatinine prior to removal ‐ should be same as serum value
h l l f d b
27
• Might leave longer if worried about necrosis or devascularization injury
27
Early Diagnosis
• Flank pain/CVA tenderness
• Unexplained fever
• Persistent ileus
• Lower abdominal mass
28
• Lower abdominal mass
• Urinary discharge from vagina
• Decreased urinary output
• Unexplained hematuria
• Normally urine/plasma creatinine is 30:1 to 100:1
Urinoma, Urinary Ascites
29
• However, may equilibrate fast
• May be as low as 2:1
• Non‐urine ascitic fluid would be 1:1
Sakellariou P Eur J Obstet Gynecol Rep Biol 101(2):179, 2002
Thanks!
3030
22

References
• Brummer THI, Human Reproduction 23(4):840, 2008
• Ostrazenski A, Obstet Gynecol Surv 58:793, 2003
• De Humani Corpus Fabrica by Andreas Vesalius, Padua, Italy (1543)
31
• Vakili B, Am J Obstet Gynecol 192, 1599, 2005
• Hurt WG, Gynecologic and Obstetrical Surgery (Nichols DH ed), Baltimore, Mosby, 1993
• Sakellariou P, Eur J Obstet Gynecol Rep Biol 101(2):179, 2002
31
23
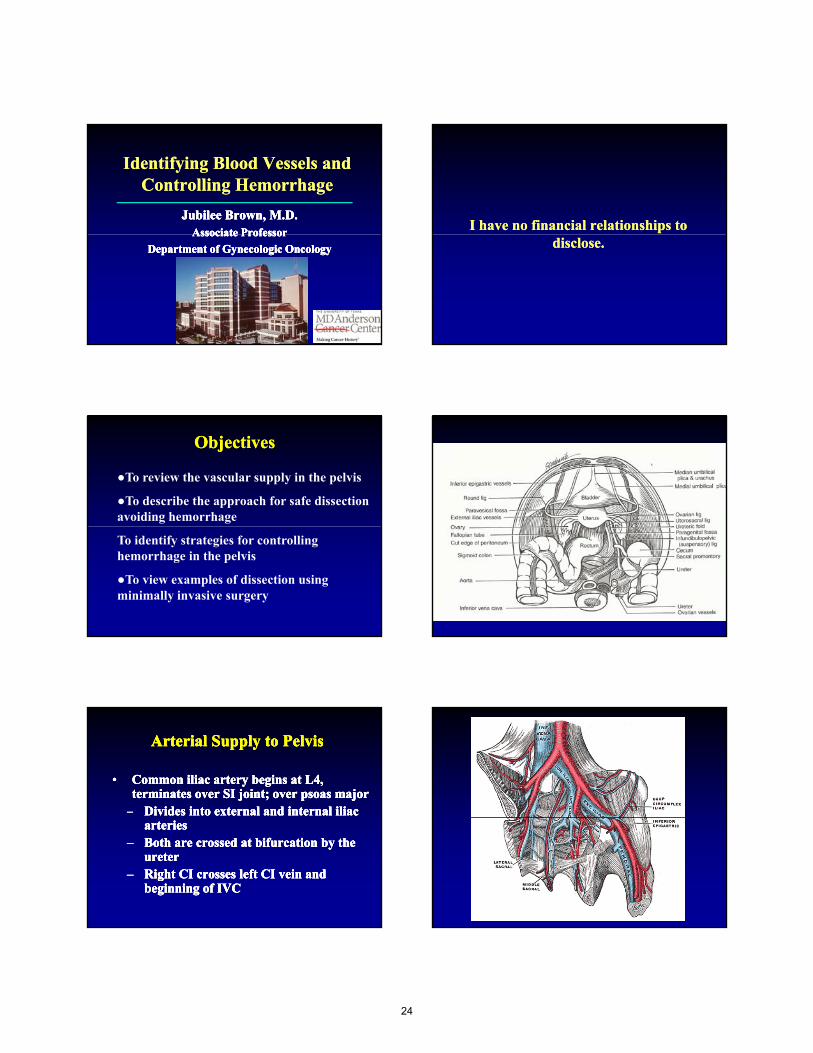
Identifying Blood Vessels and Controlling Hemorrhage
Identifying Blood Vessels and Controlling Hemorrhage
Jubilee Brown, M.D.Jubilee Brown, M.D.Associate ProfessorAssociate Professor
Jubilee Brown, M.D.Jubilee Brown, M.D.Associate ProfessorAssociate ProfessorAssociate ProfessorAssociate Professor
Department of Gynecologic OncologyDepartment of Gynecologic Oncology
Associate ProfessorAssociate Professor
Department of Gynecologic OncologyDepartment of Gynecologic Oncology
I have no financial relationships to I have no financial relationships to disclose.disclose.
ObjectivesObjectives
●To review the vascular supply in the pelvis
●To describe the approach for safe dissection avoiding hemorrhage
To identify strategies for controlling hemorrhage in the pelvis
●To view examples of dissection using minimally invasive surgery
Arterial Supply to PelvisArterial Supply to PelvisArterial Supply to PelvisArterial Supply to Pelvis
•• Common iliac artery begins at L4, Common iliac artery begins at L4, terminates over SI joint; over psoas majorterminates over SI joint; over psoas major
–– Divides into external and internal iliac Divides into external and internal iliac
•• Common iliac artery begins at L4, Common iliac artery begins at L4, terminates over SI joint; over psoas majorterminates over SI joint; over psoas major
–– Divides into external and internal iliac Divides into external and internal iliac arteriesarteries
–– Both are crossed at bifurcation by the Both are crossed at bifurcation by the ureterureter
–– Right CI crosses left CI vein and Right CI crosses left CI vein and beginning of IVCbeginning of IVC
arteriesarteries–– Both are crossed at bifurcation by the Both are crossed at bifurcation by the
ureterureter–– Right CI crosses left CI vein and Right CI crosses left CI vein and
beginning of IVCbeginning of IVC
24
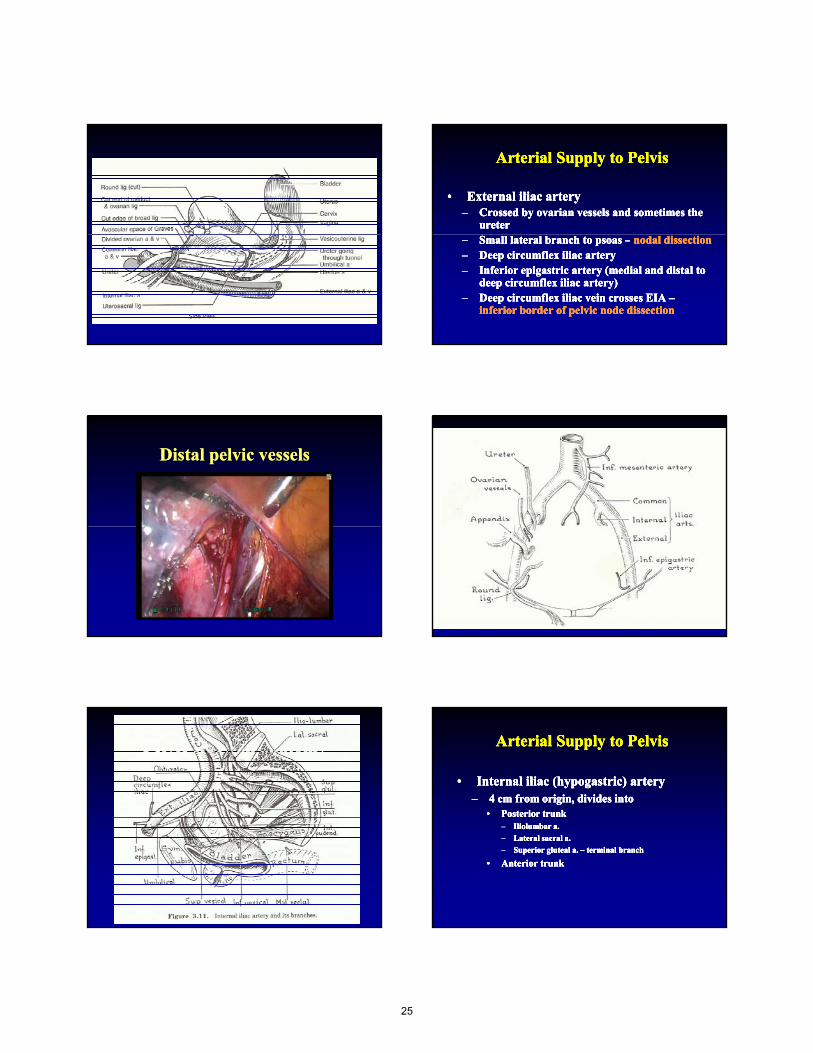
Arterial Supply to PelvisArterial Supply to PelvisArterial Supply to PelvisArterial Supply to Pelvis
•• External iliac arteryExternal iliac artery–– Crossed by ovarian vessels and sometimes the Crossed by ovarian vessels and sometimes the
ureterureter
•• External iliac arteryExternal iliac artery–– Crossed by ovarian vessels and sometimes the Crossed by ovarian vessels and sometimes the
ureterureter–– Small lateral branch to psoas Small lateral branch to psoas –– nodal dissectionnodal dissection–– Deep circumflex iliac arteryDeep circumflex iliac artery–– Inferior epigastric artery (medial and distal to Inferior epigastric artery (medial and distal to
deep circumflex iliac artery)deep circumflex iliac artery)–– Deep circumflex iliac vein crosses EIA Deep circumflex iliac vein crosses EIA ––
inferior border of pelvic node dissectioninferior border of pelvic node dissection
–– Small lateral branch to psoas Small lateral branch to psoas –– nodal dissectionnodal dissection–– Deep circumflex iliac arteryDeep circumflex iliac artery–– Inferior epigastric artery (medial and distal to Inferior epigastric artery (medial and distal to
deep circumflex iliac artery)deep circumflex iliac artery)–– Deep circumflex iliac vein crosses EIA Deep circumflex iliac vein crosses EIA ––
inferior border of pelvic node dissectioninferior border of pelvic node dissection
Distal pelvic vesselsDistal pelvic vessels
Pelvic sidewall anatomyPelvic sidewall anatomy Arterial Supply to PelvisArterial Supply to PelvisArterial Supply to PelvisArterial Supply to Pelvis
•• Internal iliac (hypogastric) arteryInternal iliac (hypogastric) artery–– 4 cm from origin, divides into4 cm from origin, divides into
•• Posterior trunkPosterior trunk
•• Internal iliac (hypogastric) arteryInternal iliac (hypogastric) artery–– 4 cm from origin, divides into4 cm from origin, divides into
•• Posterior trunkPosterior trunk–– Iliolumbar a.Iliolumbar a.
–– Lateral sacral a.Lateral sacral a.
–– Superior gluteal a. Superior gluteal a. –– terminal branchterminal branch
•• Anterior trunkAnterior trunk
–– Iliolumbar a.Iliolumbar a.
–– Lateral sacral a.Lateral sacral a.
–– Superior gluteal a. Superior gluteal a. –– terminal branchterminal branch
•• Anterior trunkAnterior trunk
25
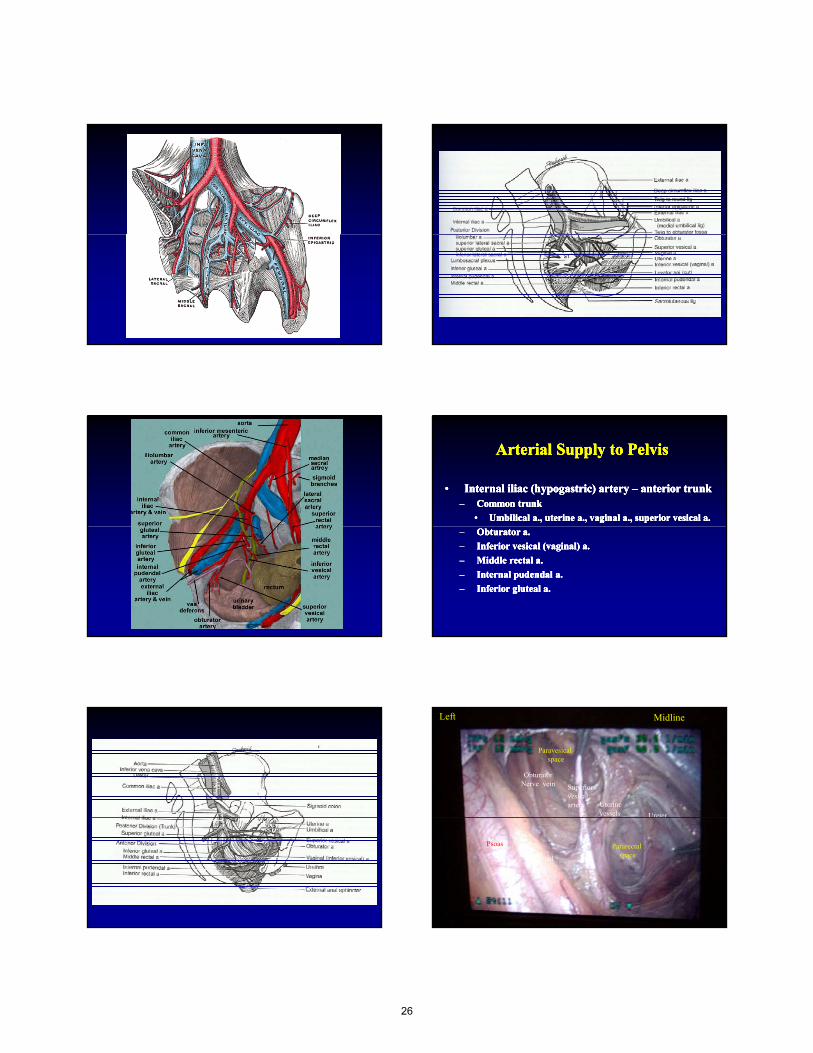
Arterial Supply to PelvisArterial Supply to PelvisArterial Supply to PelvisArterial Supply to Pelvis
•• Internal iliac (hypogastric) artery Internal iliac (hypogastric) artery –– anterior trunk anterior trunk –– Common trunkCommon trunk
•• Umbilical a., uterine a., vaginal a., superior vesical a.Umbilical a., uterine a., vaginal a., superior vesical a.
•• Internal iliac (hypogastric) artery Internal iliac (hypogastric) artery –– anterior trunk anterior trunk –– Common trunkCommon trunk
•• Umbilical a., uterine a., vaginal a., superior vesical a.Umbilical a., uterine a., vaginal a., superior vesical a.
–– Obturator a.Obturator a.
–– Inferior vesical (vaginal) a.Inferior vesical (vaginal) a.
–– Middle rectal a.Middle rectal a.
–– Internal pudendal a.Internal pudendal a.
–– Inferior gluteal a.Inferior gluteal a.
–– Obturator a.Obturator a.
–– Inferior vesical (vaginal) a.Inferior vesical (vaginal) a.
–– Middle rectal a.Middle rectal a.
–– Internal pudendal a.Internal pudendal a.
–– Inferior gluteal a.Inferior gluteal a.
Paravesical space
Superior vesical artery Uterine
vessels
ObturatorNerve vein
Left Midline
Ureter
Pararectal spaceExternal
iliac artery
Psoas
U ete
26
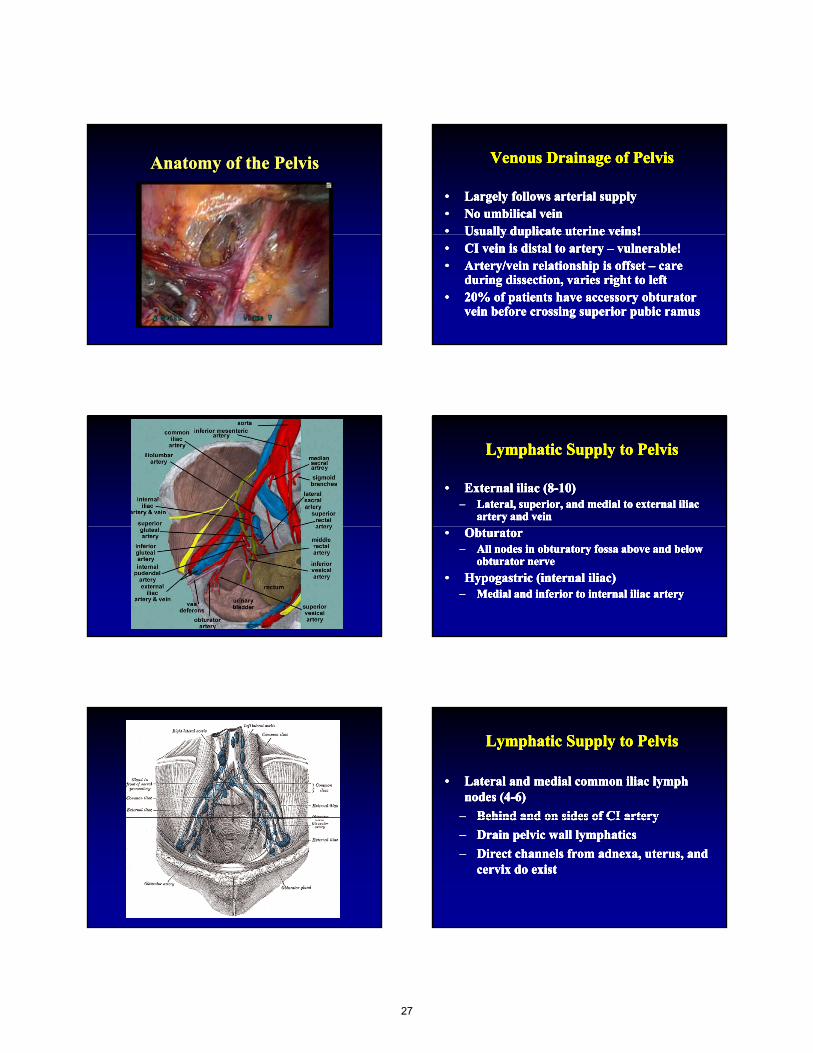
Anatomy of the PelvisAnatomy of the Pelvis Venous Drainage of PelvisVenous Drainage of PelvisVenous Drainage of PelvisVenous Drainage of Pelvis
•• Largely follows arterial supplyLargely follows arterial supply•• No umbilical veinNo umbilical vein•• Usually duplicate uterine veins!Usually duplicate uterine veins!
•• Largely follows arterial supplyLargely follows arterial supply•• No umbilical veinNo umbilical vein•• Usually duplicate uterine veins!Usually duplicate uterine veins!Usually duplicate uterine veins!Usually duplicate uterine veins!•• CI vein is distal to artery CI vein is distal to artery –– vulnerable!vulnerable!•• Artery/vein relationship is offset Artery/vein relationship is offset –– care care
during dissection, varies right to leftduring dissection, varies right to left•• 20% of patients have accessory obturator 20% of patients have accessory obturator
vein before crossing superior pubic ramusvein before crossing superior pubic ramus
Usually duplicate uterine veins!Usually duplicate uterine veins!•• CI vein is distal to artery CI vein is distal to artery –– vulnerable!vulnerable!•• Artery/vein relationship is offset Artery/vein relationship is offset –– care care
during dissection, varies right to leftduring dissection, varies right to left•• 20% of patients have accessory obturator 20% of patients have accessory obturator
vein before crossing superior pubic ramusvein before crossing superior pubic ramus
Lymphatic Supply to PelvisLymphatic Supply to PelvisLymphatic Supply to PelvisLymphatic Supply to Pelvis
•• External iliac (8External iliac (8--10)10)–– Lateral, superior, and medial to external iliac Lateral, superior, and medial to external iliac
artery and veinartery and vein
•• External iliac (8External iliac (8--10)10)–– Lateral, superior, and medial to external iliac Lateral, superior, and medial to external iliac
artery and veinartery and vein
•• ObturatorObturator–– All nodes in obturatory fossa above and below All nodes in obturatory fossa above and below
obturator nerveobturator nerve
•• Hypogastric (internal iliac)Hypogastric (internal iliac)–– Medial and inferior to internal iliac arteryMedial and inferior to internal iliac artery
•• ObturatorObturator–– All nodes in obturatory fossa above and below All nodes in obturatory fossa above and below
obturator nerveobturator nerve
•• Hypogastric (internal iliac)Hypogastric (internal iliac)–– Medial and inferior to internal iliac arteryMedial and inferior to internal iliac artery
Lymphatic Supply to PelvisLymphatic Supply to PelvisLymphatic Supply to PelvisLymphatic Supply to Pelvis
•• Lateral and medial common iliac lymph Lateral and medial common iliac lymph nodes (4nodes (4--6)6)
–– Behind and on sides of CI arteryBehind and on sides of CI artery
•• Lateral and medial common iliac lymph Lateral and medial common iliac lymph nodes (4nodes (4--6)6)
–– Behind and on sides of CI arteryBehind and on sides of CI arteryBehind and on sides of CI arteryBehind and on sides of CI artery
–– Drain pelvic wall lymphaticsDrain pelvic wall lymphatics
–– Direct channels from adnexa, uterus, and Direct channels from adnexa, uterus, and cervix do existcervix do exist
Behind and on sides of CI arteryBehind and on sides of CI artery
–– Drain pelvic wall lymphaticsDrain pelvic wall lymphatics
–– Direct channels from adnexa, uterus, and Direct channels from adnexa, uterus, and cervix do existcervix do exist
27
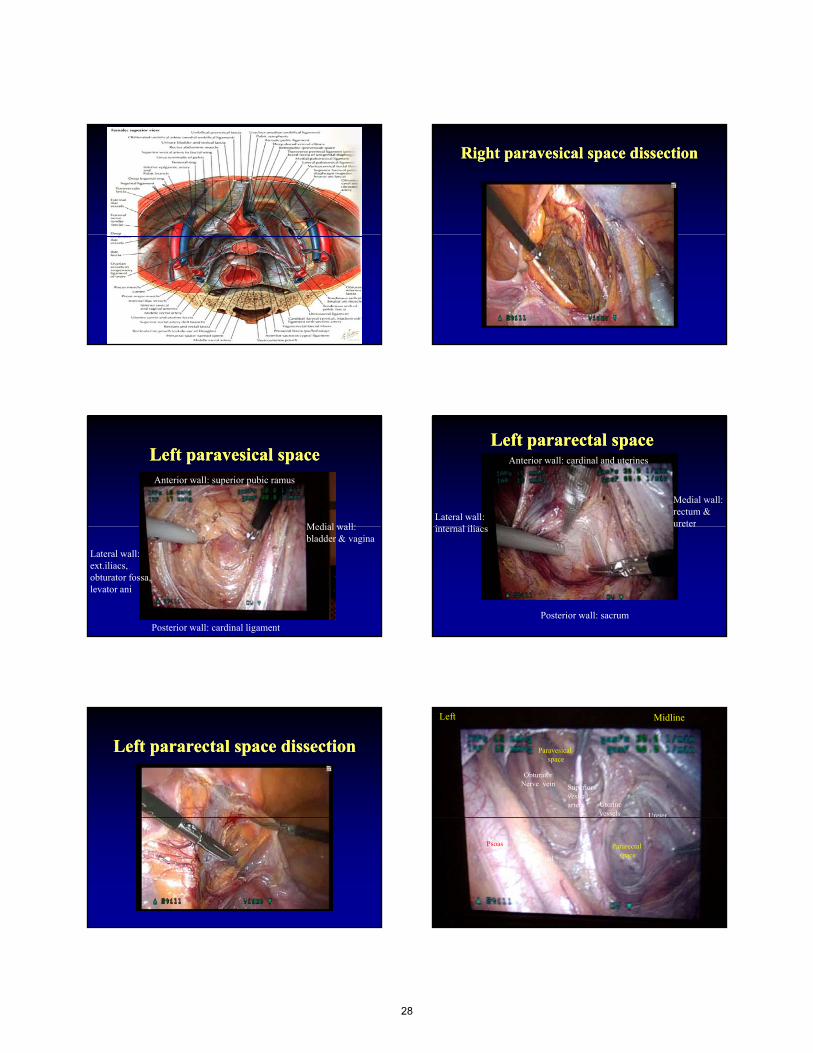
Right paravesical space dissectionRight paravesical space dissection
Left paravesical spaceLeft paravesical space
Medial wall:
Anterior wall: superior pubic ramus
Medial wall: bladder & vagina
Lateral wall: ext.iliacs, obturator fossa, levator ani
Posterior wall: cardinal ligament
Left pararectal spaceLeft pararectal space
Medial wall: rectum & ureter
Lateral wall: i t l ili
Anterior wall: cardinal and uterines
ureterinternal iliacs
Posterior wall: sacrum
Left pararectal space dissectionLeft pararectal space dissection Paravesical space
Superior vesical artery Uterine
vessels
ObturatorNerve vein
Left Midline
Ureter
Pararectal spaceExternal
iliac artery
Psoas
U ete
28
Vascular contents of space of Vascular contents of space of RetziusRetziusVascular contents of space of Vascular contents of space of RetziusRetzius
•• Veins of Veins of SantoriniSantorini (in the floor)(in the floor)
•• ObturatorObturator neurovascular bundleneurovascular bundle
•• Aberrant Aberrant obturatorobturator artery and veinartery and vein
•• External iliac artery and veinExternal iliac artery and vein
•• Veins of Veins of SantoriniSantorini (in the floor)(in the floor)
•• ObturatorObturator neurovascular bundleneurovascular bundle
•• Aberrant Aberrant obturatorobturator artery and veinartery and vein
•• External iliac artery and veinExternal iliac artery and veinyyyy
RetrorectalRetrorectal ((PresacralPresacral) Space) SpaceRetrorectalRetrorectal ((PresacralPresacral) Space) Space Boundaries of Boundaries of presacralpresacral spacespaceBoundaries of Boundaries of presacralpresacral spacespace
•• RectumRectum
•• Sacrum/coccyxSacrum/coccyx
•• UterosacralUterosacral ligsligs
•• RectumRectum
•• Sacrum/coccyxSacrum/coccyx
•• UterosacralUterosacral ligsligs•• UterosacralUterosacral ligsligs..
•• LevatorLevator aniani (floor)(floor)
•• Right CI arteryRight CI artery
•• Left CI veinLeft CI vein
•• Right Right ureterureter
•• UterosacralUterosacral ligsligs..
•• LevatorLevator aniani (floor)(floor)
•• Right CI arteryRight CI artery
•• Left CI veinLeft CI vein
•• Right Right ureterureter
Vascular structures in Vascular structures in presacralpresacral spacespaceVascular structures in Vascular structures in presacralpresacral spacespace
•• Middle sacral Middle sacral arteryartery
•• Middle sacralMiddle sacral
•• Middle sacral Middle sacral arteryartery
•• Middle sacralMiddle sacralMiddle sacral Middle sacral veinsveins
•• Sacral venous Sacral venous plexusplexus
Middle sacral Middle sacral veinsveins
•• Sacral venous Sacral venous plexusplexus
Accessing the Accessing the PresacralPresacral SpaceSpaceAccessing the Accessing the PresacralPresacral SpaceSpace
•• Sigmoid colon is retracted to the leftSigmoid colon is retracted to the left
•• Peritoneum is incised in the midline over the Peritoneum is incised in the midline over the sacral promontorysacral promontory
•• Sigmoid colon is retracted to the leftSigmoid colon is retracted to the left
•• Peritoneum is incised in the midline over the Peritoneum is incised in the midline over the sacral promontorysacral promontory
•• This avoids injury to the common iliac This avoids injury to the common iliac vesselsvessels
•• Visualize Visualize uretersureters
•• This avoids injury to the common iliac This avoids injury to the common iliac vesselsvessels
•• Visualize Visualize uretersureters
29
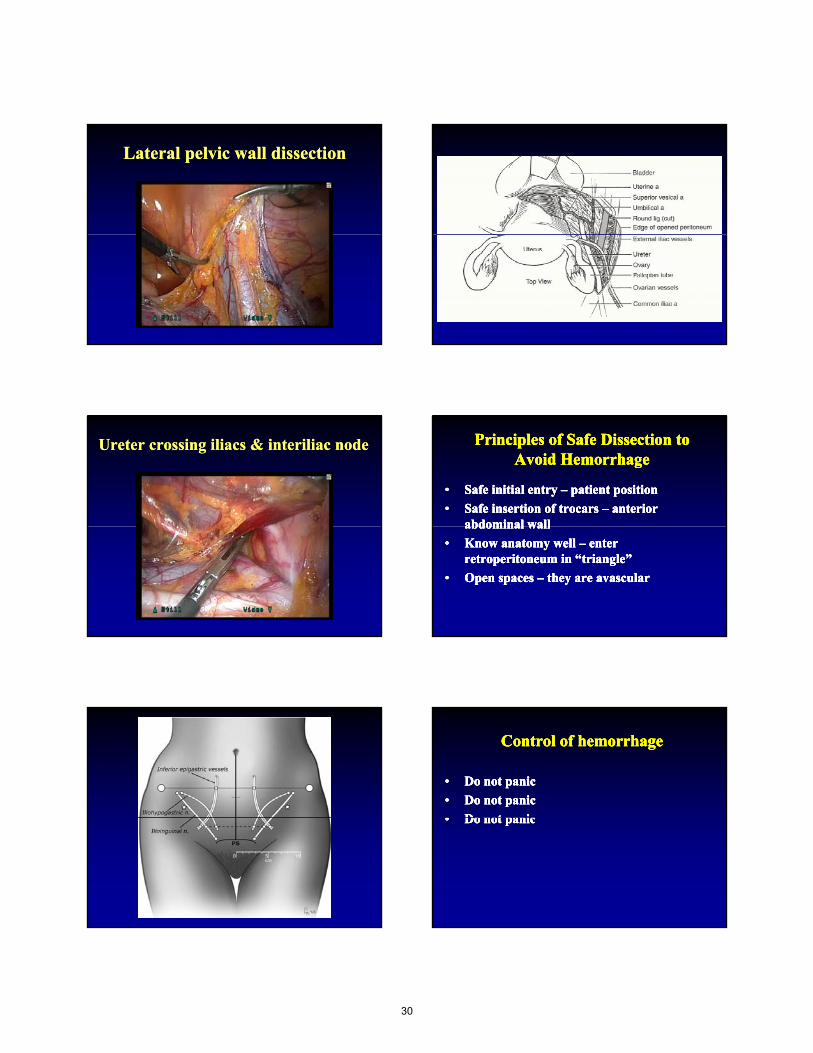
Lateral pelvic wall dissectionLateral pelvic wall dissection
Ureter crossing iliacs & interiliac nodeUreter crossing iliacs & interiliac node Principles of Safe Dissection to Principles of Safe Dissection to Avoid HemorrhageAvoid Hemorrhage
Principles of Safe Dissection to Principles of Safe Dissection to Avoid HemorrhageAvoid Hemorrhage
•• Safe initial entry Safe initial entry –– patient positionpatient position
•• Safe insertion of trocars Safe insertion of trocars –– anterior anterior abdominal wallabdominal wall
•• Safe initial entry Safe initial entry –– patient positionpatient position
•• Safe insertion of trocars Safe insertion of trocars –– anterior anterior abdominal wallabdominal wallabdominal wallabdominal wall
•• Know anatomy well Know anatomy well –– enter enter retroperitoneum in “triangle”retroperitoneum in “triangle”
•• Open spaces Open spaces –– they are avascularthey are avascular
abdominal wallabdominal wall
•• Know anatomy well Know anatomy well –– enter enter retroperitoneum in “triangle”retroperitoneum in “triangle”
•• Open spaces Open spaces –– they are avascularthey are avascular
Control of hemorrhageControl of hemorrhageControl of hemorrhageControl of hemorrhage
•• Do not panicDo not panic
•• Do not panicDo not panic
•• Do not panicDo not panic
•• Do not panicDo not panic
•• Do not panicDo not panic
•• Do not panicDo not panic•• Do not panicDo not panic•• Do not panicDo not panic
30
Control of hemorrhageControl of hemorrhageControl of hemorrhageControl of hemorrhage
•• Hold pressureHold pressure
•• Discuss with anesthesiologist and teamDiscuss with anesthesiologist and team–– IV access, blood availability, staffingIV access, blood availability, staffing
•• Hold pressureHold pressure
•• Discuss with anesthesiologist and teamDiscuss with anesthesiologist and team–– IV access, blood availability, staffingIV access, blood availability, staffing, y, g, y, g
•• Access to bleeding siteAccess to bleeding site–– Enough visualization, may have to dissect moreEnough visualization, may have to dissect more
•• Low threshold for conversionLow threshold for conversion–– Don’t need much to make a quick lap and put Don’t need much to make a quick lap and put
pressure on the sitepressure on the site
, y, g, y, g
•• Access to bleeding siteAccess to bleeding site–– Enough visualization, may have to dissect moreEnough visualization, may have to dissect more
•• Low threshold for conversionLow threshold for conversion–– Don’t need much to make a quick lap and put Don’t need much to make a quick lap and put
pressure on the sitepressure on the site
Control of hemorrhageControl of hemorrhageControl of hemorrhageControl of hemorrhage
•• Pressure: 4x4, fatty flap, grasperPressure: 4x4, fatty flap, grasper
•• ProductsProducts
•• ClipsClips
•• Pressure: 4x4, fatty flap, grasperPressure: 4x4, fatty flap, grasper
•• ProductsProducts
•• ClipsClipsClipsClips
•• SutureSuture
ClipsClips
•• SutureSuture
Thank You !
31

Nerve Injury: Identification and Prevention
R. Wendel Naumann, M.D.
Carolinas Medical Center, Levine Cancer Institute
Charlotte, NC
Disclosures
• I have no financial relationships to disclose
22
Objective
• Review mechanisms and prevention of common nerve injuries in Pelvic Surgery including
–Brachial Plexus Injury
–Cutaneous nerves of the anterior abdominal wall
3
Cutaneous nerves of the anterior abdominal wall
–Bladder
–Obturator
–Femoral
–Peroneal
3
Nerve Injury ‐ Remember!!!!
• The patient is paralyzed
• The patient is immobile
• The patient feels no pain
4
• The procedure may be long
4
Brachial Plexus and Ulnar Nerve Injury
5
ju y
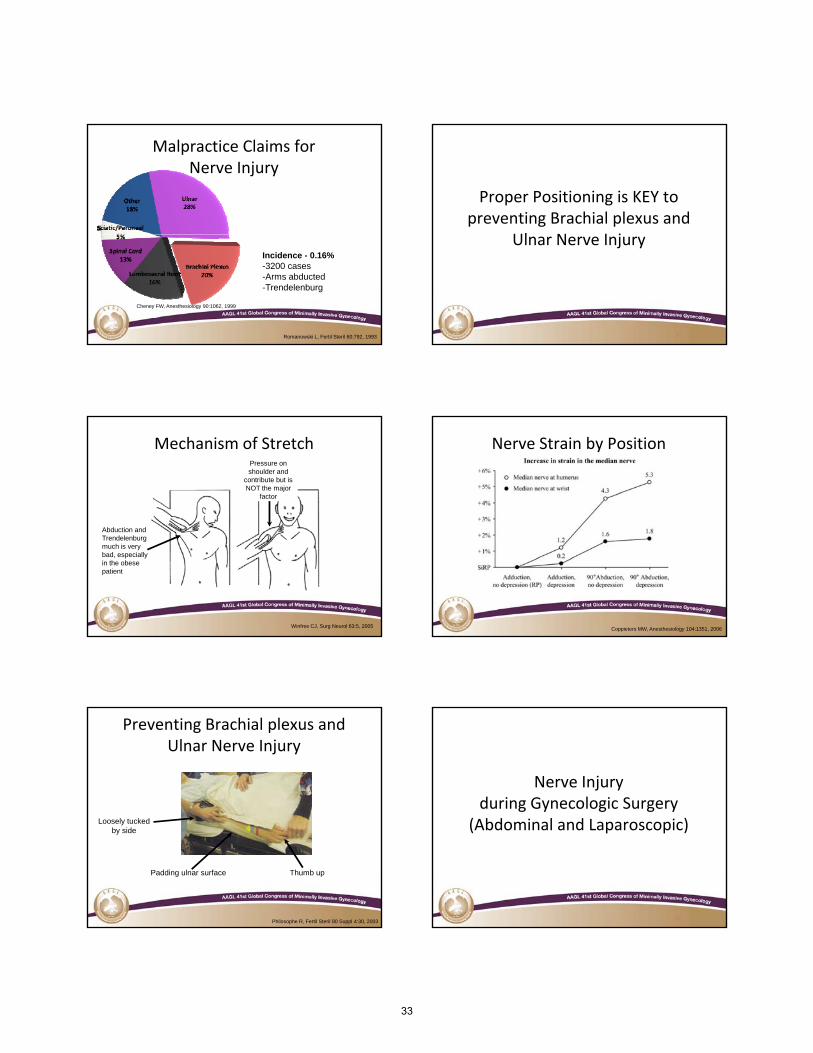
Malpractice Claims for Nerve Injury
% Male % Female Median Age
All 50% 49% 44
Ulnar 75% 23% 50
B hi l l 40% 58% 41
6
Brachial plexus 40% 58% 41
Nerve Root 29% 71% 37
Spinal Cord 52% 48% 54
Other 42% 58% 40
Cheney FW, Anesthesiology 90:1062, 1999
32
Malpractice Claims for Nerve Injury
7
Cheney FW, Anesthesiology 90:1062, 1999
Incidence - 0.16%-3200 cases-Arms abducted-Trendelenburg
Romanowski L, Fertil Steril 60:792, 1993
Proper Positioning is KEY to preventing Brachial plexus and
Ul N I j
8
Ulnar Nerve Injury
Mechanism of StretchPressure on shoulder and
contribute but is NOT the major
factor
9
Abduction and Trendelenburg much is very bad, especially in the obese patient
Winfree CJ, Surg Neurol 63:5, 2005
Nerve Strain by Position
10Coppieters MW, Anesthesiology 104:1351, 2006
Preventing Brachial plexus and Ulnar Nerve Injury
11
Thumb upPadding ulnar surface
Loosely tucked by side
Philosophe R, Fertil Steril 80 Suppl 4:30, 2003
Nerve Injuryduring Gynecologic Surgery
( )
12
(Abdominal and Laparoscopic)
33
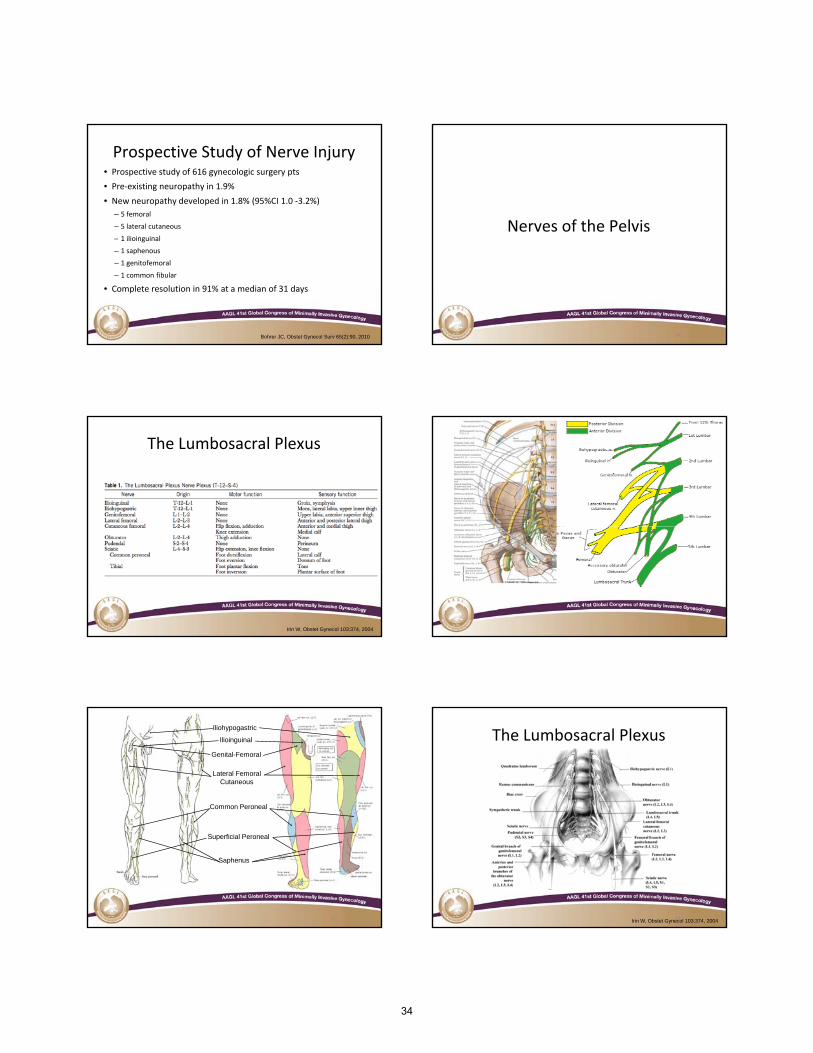
Prospective Study of Nerve Injury• Prospective study of 616 gynecologic surgery pts
• Pre‐existing neuropathy in 1.9%
• New neuropathy developed in 1.8% (95%CI 1.0 ‐3.2%)
– 5 femoral
– 5 lateral cutaneous
13
– 1 ilioinguinal
– 1 saphenous
– 1 genitofemoral
– 1 common fibular
• Complete resolution in 91% at a median of 31 days
Bohrer JC, Obstet Gynecol Surv 65(2):90, 2010
Nerves of the Pelvis
14
The Lumbosacral Plexus
15Irin W, Obstet Gynecol 103:374, 2004
Iliohypogastric
Lateral FemoralCutaneous
Ilioinguinal
Genital-Femoral
Common Peroneal
17
Superficial Peroneal
Saphenus
The Lumbosacral Plexus
18Irin W, Obstet Gynecol 103:374, 2004
34
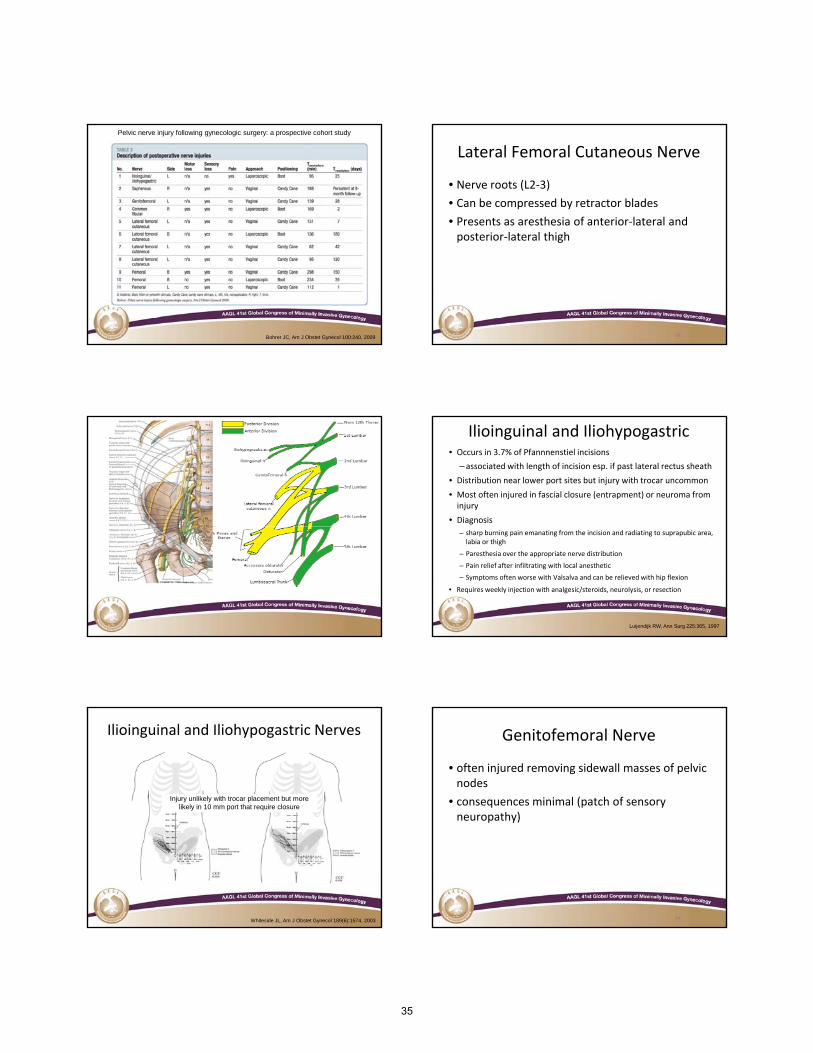
Pelvic nerve injury following gynecologic surgery: a prospective cohort study
19Bohrer JC, Am J Obstet Gynecol 100:240, 2009
Lateral Femoral Cutaneous Nerve
• Nerve roots (L2‐3)
• Can be compressed by retractor blades
• Presents as aresthesia of anterior‐lateral and posterior lateral thigh
20
posterior‐lateral thigh
20
Ilioinguinal and Iliohypogastric• Occurs in 3.7% of Pfannnenstiel incisions
– associated with length of incision esp. if past lateral rectus sheath
• Distribution near lower port sites but injury with trocar uncommon
• Most often injured in fascial closure (entrapment) or neuroma from injury
• Diagnosis
22
– sharp burning pain emanating from the incision and radiating to suprapubic area, labia or thigh
– Paresthesia over the appropriate nerve distribution
– Pain relief after infiltrating with local anesthetic
– Symptoms often worse with Valsalva and can be relieved with hip flexion
• Requires weekly injection with analgesic/steroids, neurolysis, or resection
Luijendijk RW, Ann Surg 225:365, 1997
Ilioinguinal and Iliohypogastric Nerves
Injury unlikely with trocar placement but more likely in 10 mm port that require closure
23Whiteside JL, Am J Obstet Gynecol 189(6):1574, 2003
Genitofemoral Nerve
• often injured removing sidewall masses of pelvic nodes
• consequences minimal (patch of sensory neuropathy)
24
neuropathy)
24
35
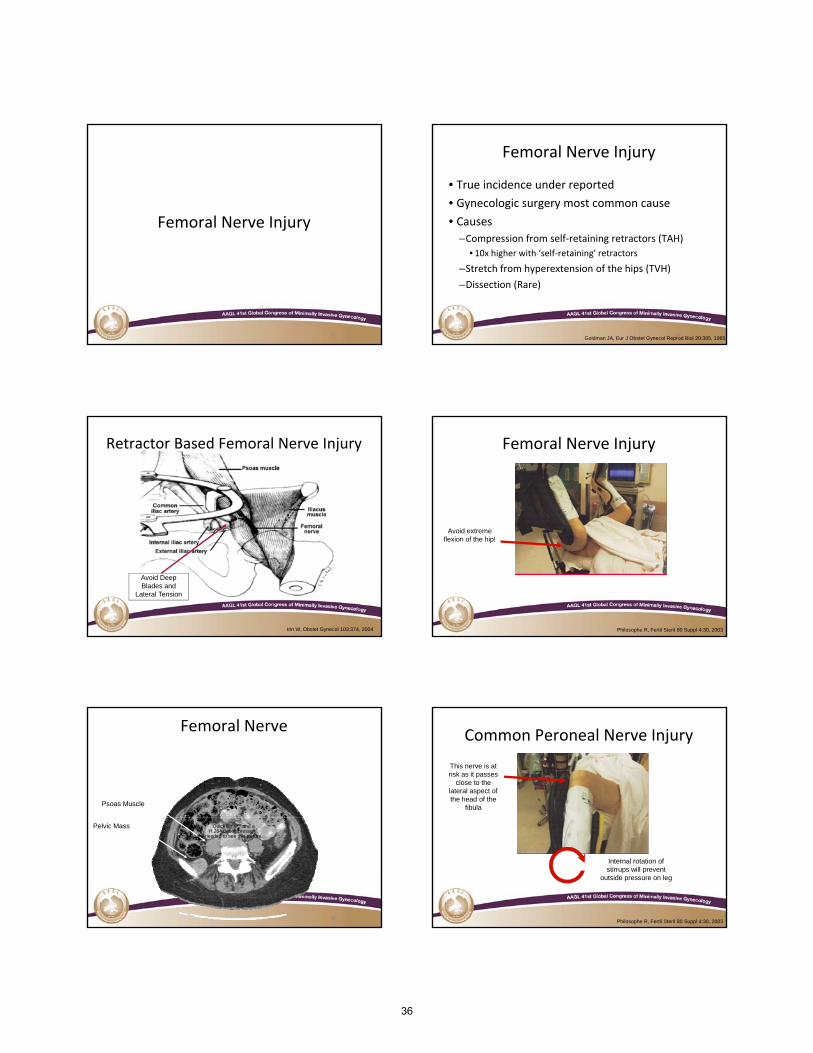
Femoral Nerve Injury
25
Femoral Nerve Injury
• True incidence under reported
• Gynecologic surgery most common cause
• Causesf lf ( )
26
–Compression from self‐retaining retractors (TAH)
• 10x higher with ‘self‐retaining’ retractors
–Stretch from hyperextension of the hips (TVH)
–Dissection (Rare)
26Goldman JA, Eur J Obstet Gynecol Reprod Biol 20:385, 1985
Retractor Based Femoral Nerve Injury
27Irin W, Obstet Gynecol 103:374, 2004
Avoid Deep Blades and
Lateral Tension
Femoral Nerve Injury
28
Avoid extreme flexion of the hip!
Philosophe R, Fertil Steril 80 Suppl 4:30, 2003
Femoral Nerve
Psoas Muscle
29
Pelvic Mass QuickTime™ and aH.264 decompressor
are needed to see this picture.
29
Common Peroneal Nerve Injury
This nerve is at risk as it passes
close to the lateral aspect of the head of the
fibula
30
Internal rotation of stirrups will prevent
outside pressure on leg
Philosophe R, Fertil Steril 80 Suppl 4:30, 2003
36
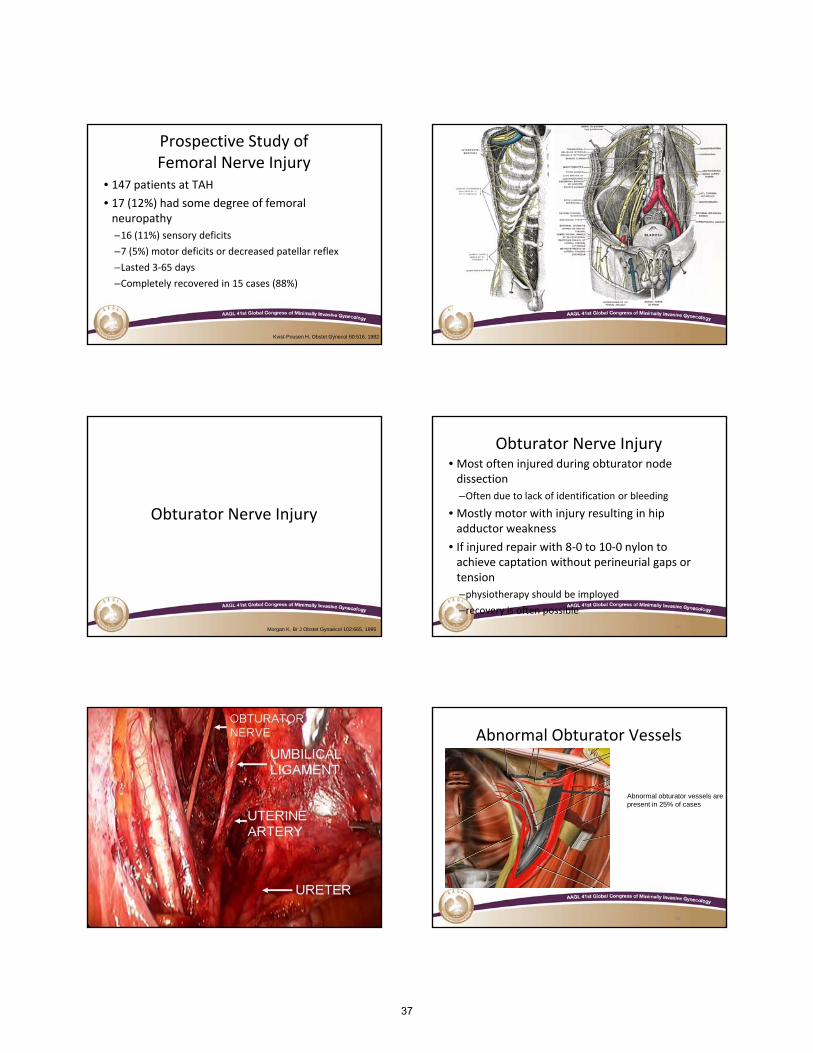
Prospective Study of Femoral Nerve Injury
• 147 patients at TAH
• 17 (12%) had some degree of femoral neuropathy
16 (11%) sensory deficits
31
–16 (11%) sensory deficits
–7 (5%) motor deficits or decreased patellar reflex
–Lasted 3‐65 days
–Completely recovered in 15 cases (88%)
31Kvist-Pousen H, Obstet Gynecol 60:516, 1982 32
Obturator Nerve Injury
33Morgan K, Br J Obstet Gynaecol 102:665, 1995
Obturator Nerve Injury• Most often injured during obturator node dissection
–Often due to lack of identification or bleeding
• Mostly motor with injury resulting in hip dd t k
34
adductor weakness
• If injured repair with 8‐0 to 10‐0 nylon to achieve captation without perineurial gaps or tension
–physiotherapy should be imployed
–recovery is often possible
Hypogastric Nerve Trunk Abnormal Obturator Vessels
Abnormal obturator vessels are present in 25% of cases
3636
37
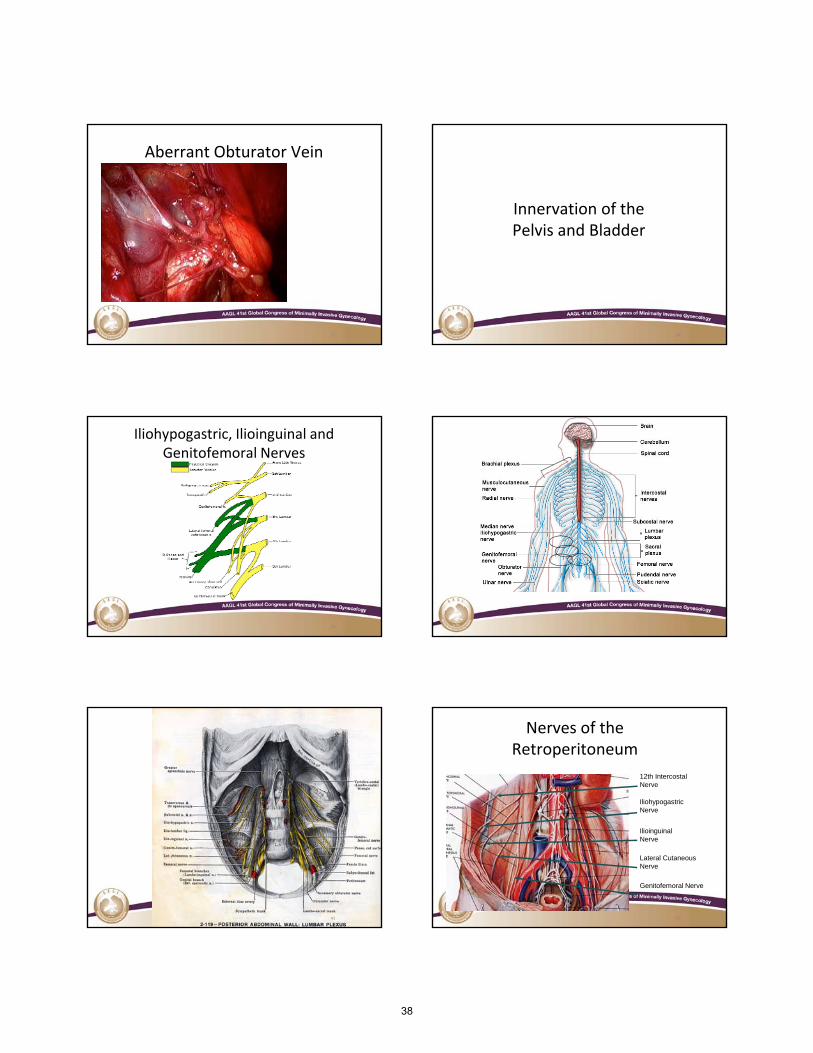
Aberrant Obturator Vein
37
Innervation of the Pelvis and Bladder
38
Pelvis and Bladder
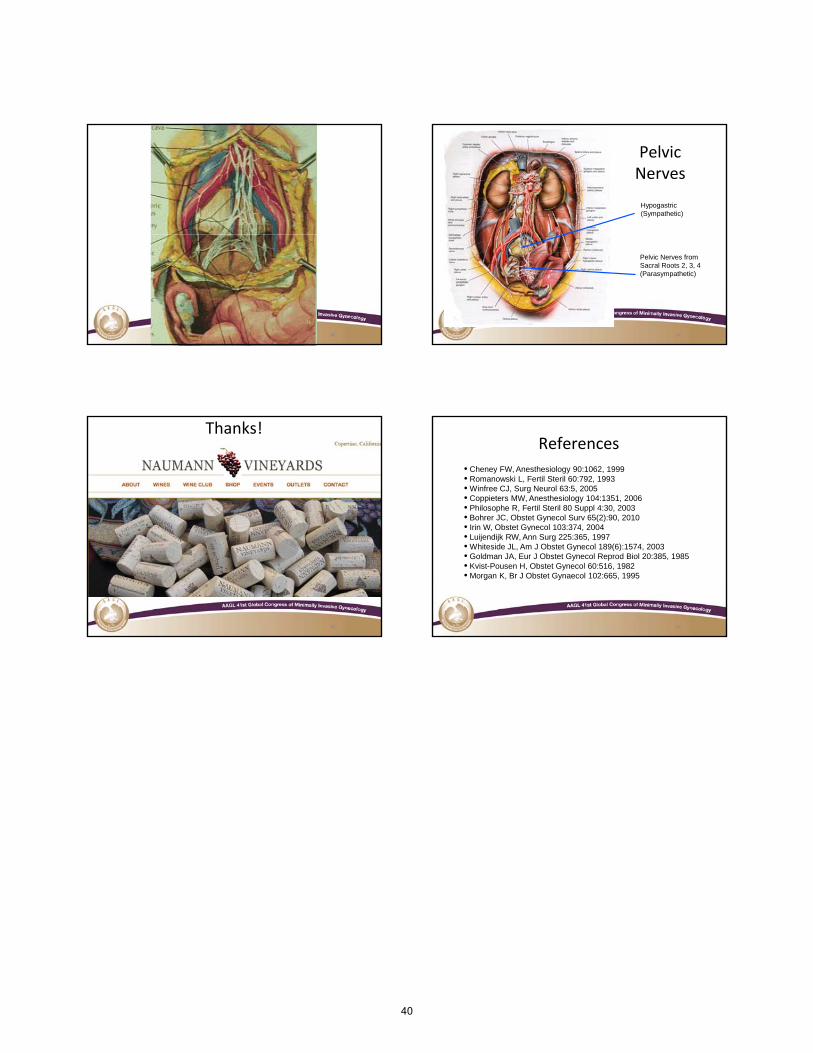
Iliohypogastric, Ilioinguinal and Genitofemoral Nerves
39
4141
Nerves of the Retroperitoneum
IliohypogastricNerve
12th IntercostalNerve
42
Genitofemoral Nerve
Ilioinguinal Nerve
Lateral CutaneousNerve
38
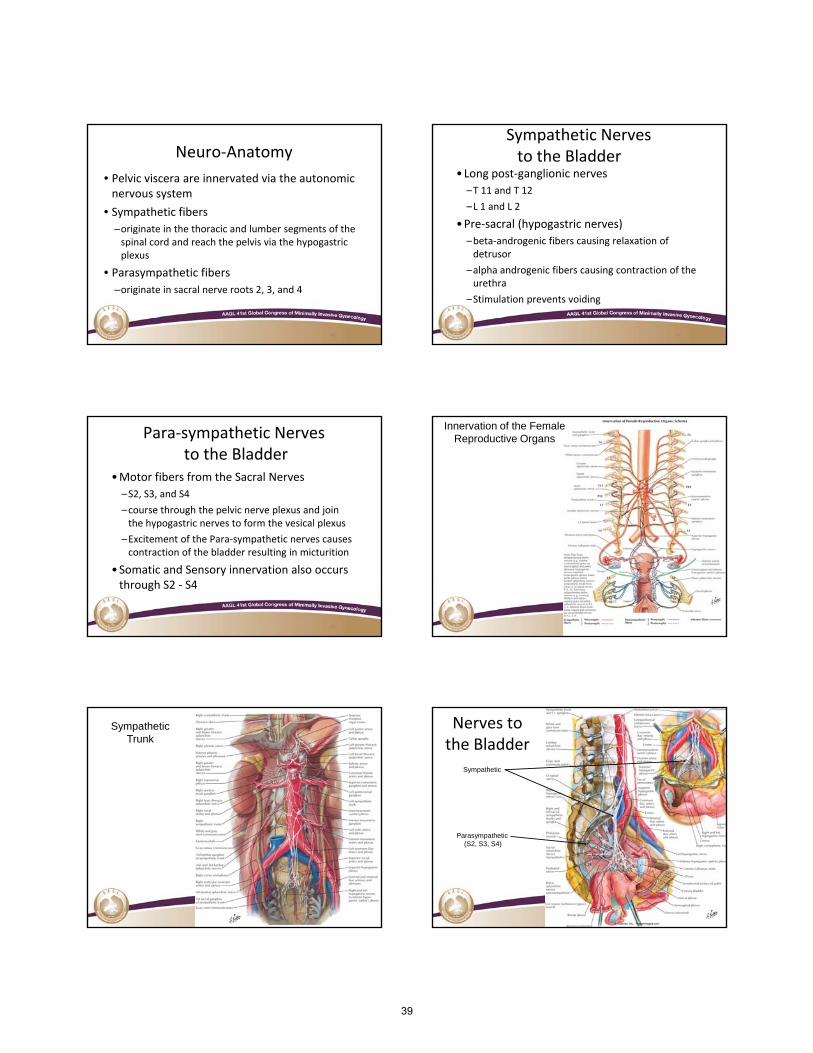
Neuro‐Anatomy
• Pelvic viscera are innervated via the autonomic nervous system
• Sympathetic fibers
–originate in the thoracic and lumber segments of the
43
spinal cord and reach the pelvis via the hypogastric plexus
• Parasympathetic fibers
–originate in sacral nerve roots 2, 3, and 4
43
Sympathetic Nerves to the Bladder
•Long post‐ganglionic nerves
–T 11 and T 12
–L 1 and L 2
•Pre‐sacral (hypogastric nerves)
44
–beta‐androgenic fibers causing relaxation of detrusor
–alpha androgenic fibers causing contraction of the urethra
–Stimulation prevents voiding
Para‐sympathetic Nervesto the Bladder
•Motor fibers from the Sacral Nerves
–S2, S3, and S4
–course through the pelvic nerve plexus and join the hypogastric nerves to form the vesical plexus
45
the hypogastric nerves to form the vesical plexus
–Excitement of the Para‐sympathetic nerves causes contraction of the bladder resulting in micturition
•Somatic and Sensory innervation also occurs through S2 ‐ S4
Innervation of the Female Reproductive Organs
Sympathetic Trunk
Sympathetic
Nerves to the Bladder
Parasympathetic(S2, S3, S4)
39
4949
Pelvic Nerves
Hypogastric(Sympathetic)
50
Pelvic Nerves fromSacral Roots 2, 3, 4(Parasympathetic)
Thanks!
5151
References
• Cheney FW, Anesthesiology 90:1062, 1999• Romanowski L, Fertil Steril 60:792, 1993• Winfree CJ, Surg Neurol 63:5, 2005• Coppieters MW, Anesthesiology 104:1351, 2006• Philosophe R, Fertil Steril 80 Suppl 4:30, 2003• Bohrer JC, Obstet Gynecol Surv 65(2):90, 2010• Irin W Obstet Gynecol 103:374 2004
52
• Irin W, Obstet Gynecol 103:374, 2004• Luijendijk RW, Ann Surg 225:365, 1997• Whiteside JL, Am J Obstet Gynecol 189(6):1574, 2003• Goldman JA, Eur J Obstet Gynecol Reprod Biol 20:385, 1985• Kvist-Pousen H, Obstet Gynecol 60:516, 1982• Morgan K, Br J Obstet Gynaecol 102:665, 1995
40
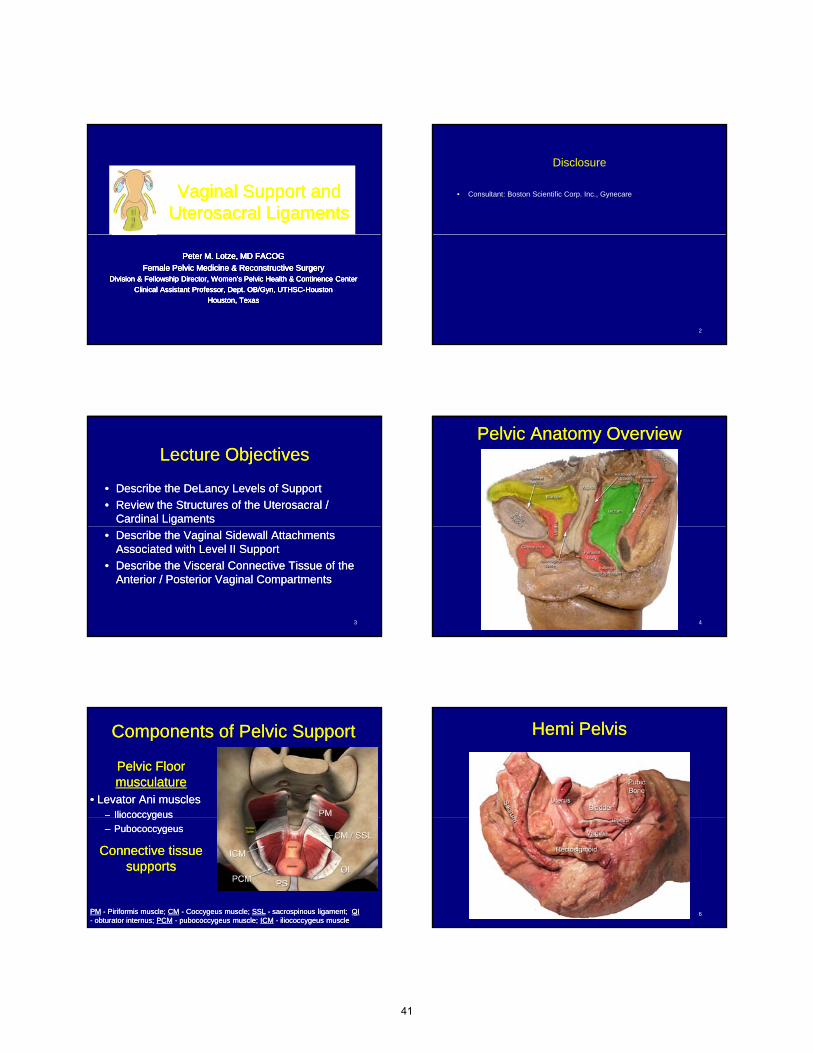
Vaginal Support and Vaginal Support and Uterosacral LigamentsUterosacral LigamentsVaginal Support and Vaginal Support and
Uterosacral LigamentsUterosacral Ligaments
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
Disclosure
• Consultant: Boston Scientific Corp. Inc., Gynecare
2
Lecture ObjectivesLecture Objectives
•• Describe the DeLancy Levels of SupportDescribe the DeLancy Levels of Support
•• Review the Structures of the Uterosacral / Review the Structures of the Uterosacral / Cardinal LigamentsCardinal Ligaments
3
•• Describe the Vaginal Sidewall Attachments Describe the Vaginal Sidewall Attachments Associated with Level II SupportAssociated with Level II Support
•• Describe the Visceral Connective Tissue of the Describe the Visceral Connective Tissue of the Anterior / Posterior Vaginal CompartmentsAnterior / Posterior Vaginal Compartments
Pelvic Anatomy OverviewPelvic Anatomy Overview
4
Components of Pelvic SupportComponents of Pelvic Support
Pelvic Floor Pelvic Floor musculaturemusculature
•• Levator Ani musclesLevator Ani muscles–– IliococcygeusIliococcygeus
5
ococcygeusococcygeus
–– PubococcygeusPubococcygeus
Connective tissue Connective tissue supportssupports
PMPM -- Piriformis muscle; Piriformis muscle; CMCM -- Coccygeus muscle; Coccygeus muscle; SSLSSL -- sacrospinous ligament; sacrospinous ligament; OIOI-- obturator internus; obturator internus; PCMPCM -- pubococcygeus muscle; pubococcygeus muscle; ICMICM -- iliococcygeus muscleiliococcygeus muscle
Hemi PelvisHemi Pelvis
6
41
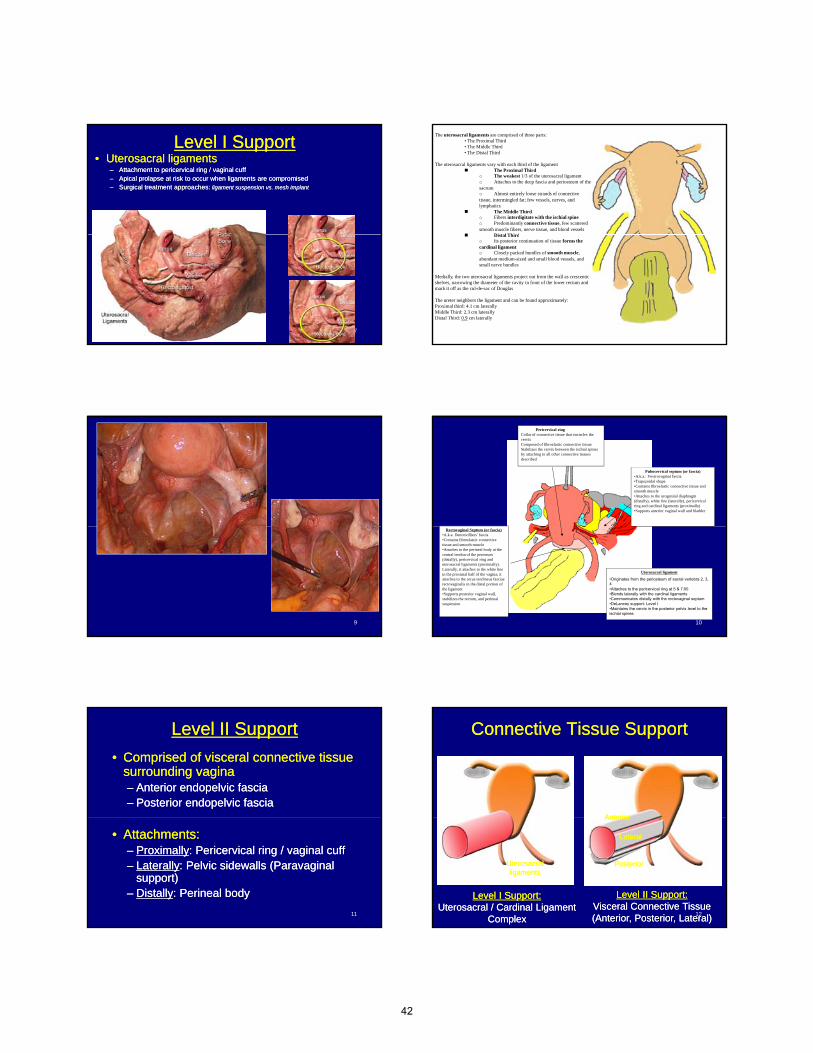
Level I SupportLevel I Support•• Uterosacral ligamentsUterosacral ligaments
–– Attachment to pericervical ring / vaginal cuffAttachment to pericervical ring / vaginal cuff–– Apical prolapse at risk to occur when ligaments are compromisedApical prolapse at risk to occur when ligaments are compromised–– Surgical treatment approaches: Surgical treatment approaches: ligament suspension vs. mesh implantligament suspension vs. mesh implant
7
The uterosacral ligaments are comprised of three parts:• The Proximal Third• The Middle Third• The Distal Third
The uterosacral ligaments vary with each third of the ligament The Proximal Third
o The weakest 1/3 of the uterosacral ligamento Attaches to the deep fascia and periosteum of the sacrumo Almost entirely loose strands of connective tissue, intermingled fat; few vessels, nerves, and lymphatics
The Middle Thirdo Fibers interdigitate with the ischial spineo Predominantly connective tissue, few scattered smooth muscle fibers, nerve tissue, and blood vessels
Distal Third
8
Distal Thirdo Its posterior continuation of tissue forms the cardinal ligamento Closely packed bundles of smooth muscle, abundant medium-sized and small blood vessels, and small nerve bundles
Medially, the two uterosacral ligaments project out from the wall as crescentic shelves, narrowing the diameter of the cavity in front of the lower rectum and mark it off as the cul-de-sac of Douglas
The ureter neighbors the ligament and can be found approximately:Proximal third: 4.1 cm laterallyMiddle Third: 2.3 cm laterallyDistal Third: 0.9 cm laterally
9
Pericervical ringCollar of connective tissue that encircles the cervixComposed of fibroelastic connective tissueStabilizes the cervix between the ischial spines by attaching to all other connective tissues described
Pubocervical septum (or fascia)•A.k.a.: Vesicovaginal fascia•Trapezoidal shape•Contains fibroelastic connective tissue and smooth muscle•Attaches to the urogenital diaphragm (distally), white line (laterally), pericervical ring and cardinal ligaments (proximally)•Supports anterior vaginal wall and bladder
10
Uterosacral ligament
•Originates from the periosteum of sacral vertebra 2, 3, 4•Attaches to the pericervical ring at 5 & 7:00•Blends laterally with the cardinal ligaments•Communicates distally with the rectovaginal septum•DeLancey support: Level I •Maintains the cervix in the posterior pelvis level to the ischial spines
Rectovaginal Septum (or fascia)•A.k.a. Denonvilliers’ fascia•Contains fibroelastic connective tissue and smooth muscle•Attaches to the perineal body at the central tendon of the perineum (distally), pericervical ring and uterosacral ligaments (proximally). Laterally, it attaches to the white line in the proximal half of the vagina; it attaches to the arcus tendineus fasciae rectovaginalis in the distal portion of the ligament•Supports posterior vaginal wall, stabilizes the rectum, and perineal suspension
Level II SupportLevel II Support
•• Comprised of visceral connective tissue Comprised of visceral connective tissue surrounding vaginasurrounding vagina–– Anterior endopelvic fasciaAnterior endopelvic fascia–– Posterior endopelvic fasciaPosterior endopelvic fascia
11
•• Attachments:Attachments:–– ProximallyProximally: Pericervical ring / vaginal cuff: Pericervical ring / vaginal cuff–– LaterallyLaterally: Pelvic sidewalls (Paravaginal : Pelvic sidewalls (Paravaginal
support)support)–– DistallyDistally: Perineal body: Perineal body
Connective Tissue SupportConnective Tissue Support
AnteriorAnterior
12
Level II Support:Level II Support:Visceral Connective Tissue Visceral Connective Tissue (Anterior, Posterior, Lateral)(Anterior, Posterior, Lateral)
Level I Support:Level I Support:Uterosacral / Cardinal Ligament Uterosacral / Cardinal Ligament
ComplexComplex
AnteriorAnterior
LateralLateral
PosteriorPosteriorUterosacralUterosacralligamentsligaments
42

Space of Retzius & Paravaginal SpaceSpace of Retzius & Paravaginal Space
•• MusclesMuscles–– Obturator internusObturator internus–– Iliococcygeus Iliococcygeus (Principle “Kegel” muscle)(Principle “Kegel” muscle)
–– Piriformis Piriformis (Neurovascular structures on top of muscle (Neurovascular structures on top of muscle -- e.g. Sciatic e.g. Sciatic nerve, inferior rectal artery)nerve, inferior rectal artery)
–– CoccygeusCoccygeus (overlies the Sacrospinous ligament)(overlies the Sacrospinous ligament)
13
–– Coccygeus Coccygeus (overlies the Sacrospinous ligament)(overlies the Sacrospinous ligament)
•• Arcus tendineous fascia pelvica Arcus tendineous fascia pelvica (ATFP; “Arcuate line”)(ATFP; “Arcuate line”)
–– Line of fascia attachment Line of fascia attachment (overlies attachment of iliococcygeus (overlies attachment of iliococcygeus to obturator internus muscles)to obturator internus muscles)
•• Ischial spineIschial spine
•• Sacrospinous ligamentSacrospinous ligament
Level II SupportLevel II Support Anterior fascia
(?)
OIOI
14
Pericervicalring
Anterior / PosteriorFascia
Perinealbody
Paravaginal support(fascia
endopelvina)
Posterior fascia
(Rectovaginal septum)
IC
OI - obturator internus muscleIC - iliococcygeus muscle
Space of Retzius & Paravaginal SpaceSpace of Retzius & Paravaginal Space
15
Level III SupportLevel III Support
16
Perineal body Perineal body -- in a standing patient, it in a standing patient, it helps to support the vagina and uterushelps to support the vagina and uterus
Pelvic Organ ProlapseWhy did this occur? Why did this occur? Where is the damage?Where is the damage?
•• Pelvic Floor MusclePelvic Floor Muscle•• Visceral Connective TissueVisceral Connective Tissue
Where is the tear?Where is the tear?
17
Where is the tear?Where is the tear?
• Uterosacral ligamentsUterosacral ligaments•• Pericervical ringPericervical ring•• Anterior / Posterior Anterior / Posterior compartmentcompartment
•• TransverseTransverse•• Lateral Lateral •• MidlineMidline
Pelvic Organ ProlapseProper WorkProper Work--upup
HistoryHistory•• How long has it been there?How long has it been there?
•• Felt it? Seen it?Felt it? Seen it?
•• What size does it seem to be?What size does it seem to be?
18
BadenBaden--WalkerWalker•• Must be understoodMust be understood
POPPOP--QQ•• Great accessoryGreat accessory
Assessment of ApexAssessment of Apex•• Mandatory Mandatory regardless of regardless of techniquetechnique
43

Vaginal Support and Vaginal Support and Uterosacral LigamentsUterosacral LigamentsVaginal Support and Vaginal Support and
Uterosacral LigamentsUterosacral Ligaments
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
Peter M. Lotze, MD FACOGPeter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryFemale Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence CenterDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSCClinical Assistant Professor, Dept. OB/Gyn, UTHSC--HoustonHouston
Houston, TexasHouston, Texas
44
Ligaments and Anatomy Important in Pelvic
Reconstructive Surgery
Peter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSC-Houston
Houston, Texas
Disclosure
• Consultant: Boston Scientific Corp. Inc., Gynecare
2
Lecture Objectives
• Describe anatomy neighboring surgical procedures for each pelvic organ compartment
3
p
• Describe the impact of injury to nearby structures on the course of the surgical procedure
Level II
4
5
Level I
6
45
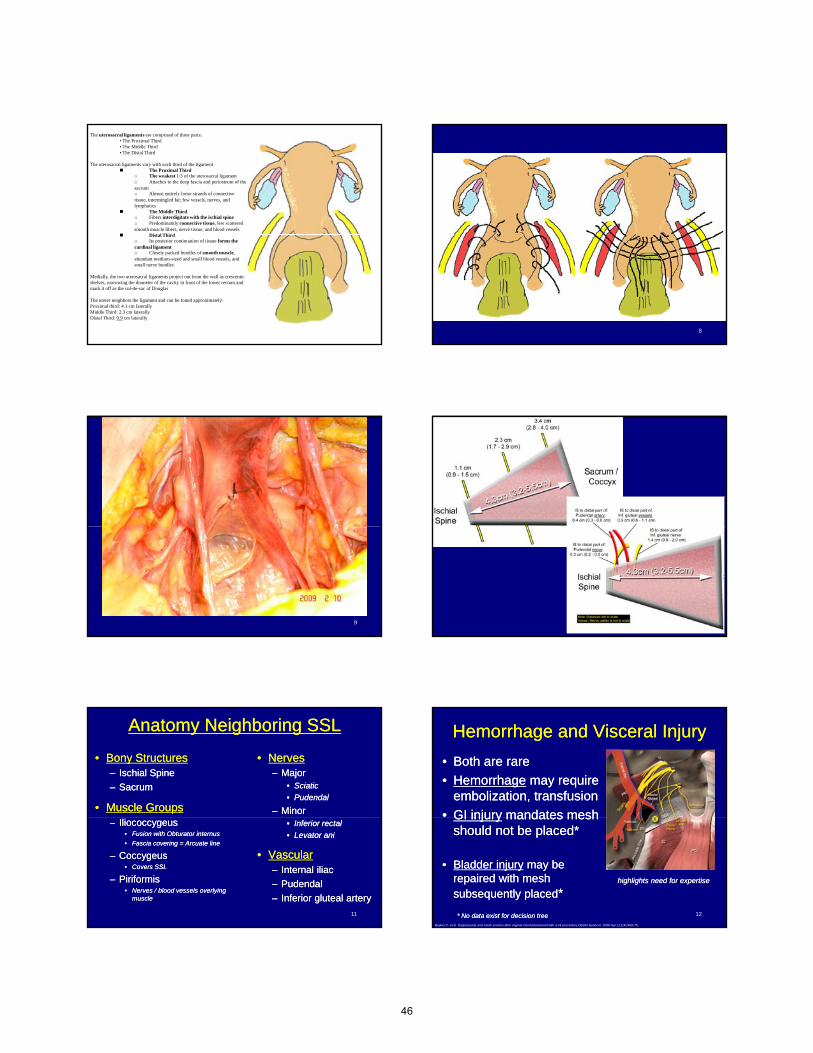
The uterosacral ligaments are comprised of three parts:• The Proximal Third• The Middle Third• The Distal Third
The uterosacral ligaments vary with each third of the ligament The Proximal Third
o The weakest 1/3 of the uterosacral ligamento Attaches to the deep fascia and periosteum of the sacrumo Almost entirely loose strands of connective tissue, intermingled fat; few vessels, nerves, and lymphatics
The Middle Thirdo Fibers interdigitate with the ischial spineo Predominantly connective tissue, few scattered smooth muscle fibers, nerve tissue, and blood vessels
Distal Third
7
Distal Thirdo Its posterior continuation of tissue forms the cardinal ligamento Closely packed bundles of smooth muscle, abundant medium-sized and small blood vessels, and small nerve bundles
Medially, the two uterosacral ligaments project out from the wall as crescenticshelves, narrowing the diameter of the cavity in front of the lower rectum and mark it off as the cul-de-sac of Douglas
The ureter neighbors the ligament and can be found approximately:Proximal third: 4.1 cm laterallyMiddle Third: 2.3 cm laterallyDistal Third: 0.9 cm laterally
8
9 10
Anatomy Neighboring SSLAnatomy Neighboring SSL
•• Bony StructuresBony Structures–– Ischial SpineIschial Spine
–– SacrumSacrum
•• Muscle GroupsMuscle Groups
•• NervesNerves–– MajorMajor
•• SciaticSciatic
•• PudendalPudendal
–– MinorMinor
11
–– Iliococcygeus Iliococcygeus •• Fusion with Obturator internus Fusion with Obturator internus
•• Fascia covering = Arcuate lineFascia covering = Arcuate line
–– CoccygeusCoccygeus•• Covers SSLCovers SSL
–– Piriformis Piriformis •• Nerves / blood vessels overlying Nerves / blood vessels overlying
musclemuscle
•• Inferior rectalInferior rectal
•• Levator aniLevator ani
•• VascularVascular–– Internal iliacInternal iliac
–– PudendalPudendal
–– Inferior gluteal arteryInferior gluteal artery
Hemorrhage and Visceral InjuryHemorrhage and Visceral Injury
•• Both are rareBoth are rare
•• HemorrhageHemorrhage may require may require embolization, transfusionembolization, transfusion
•• GI injuryGI injury mandates meshmandates mesh
12
GI injuryGI injury mandates mesh mandates mesh should not be placed*should not be placed*
•• Bladder injuryBladder injury may be may be repaired with mesh repaired with mesh subsequently placedsubsequently placed**
* No data exist for decision tree* No data exist for decision tree
highlights need for expertisehighlights need for expertise
Boyles C, et al. Dyspareunia and mesh erosion after vaginal mesh placement with a kit procedure.Obstet Gynecol. 2008 Apr;111(4):969-75.
46
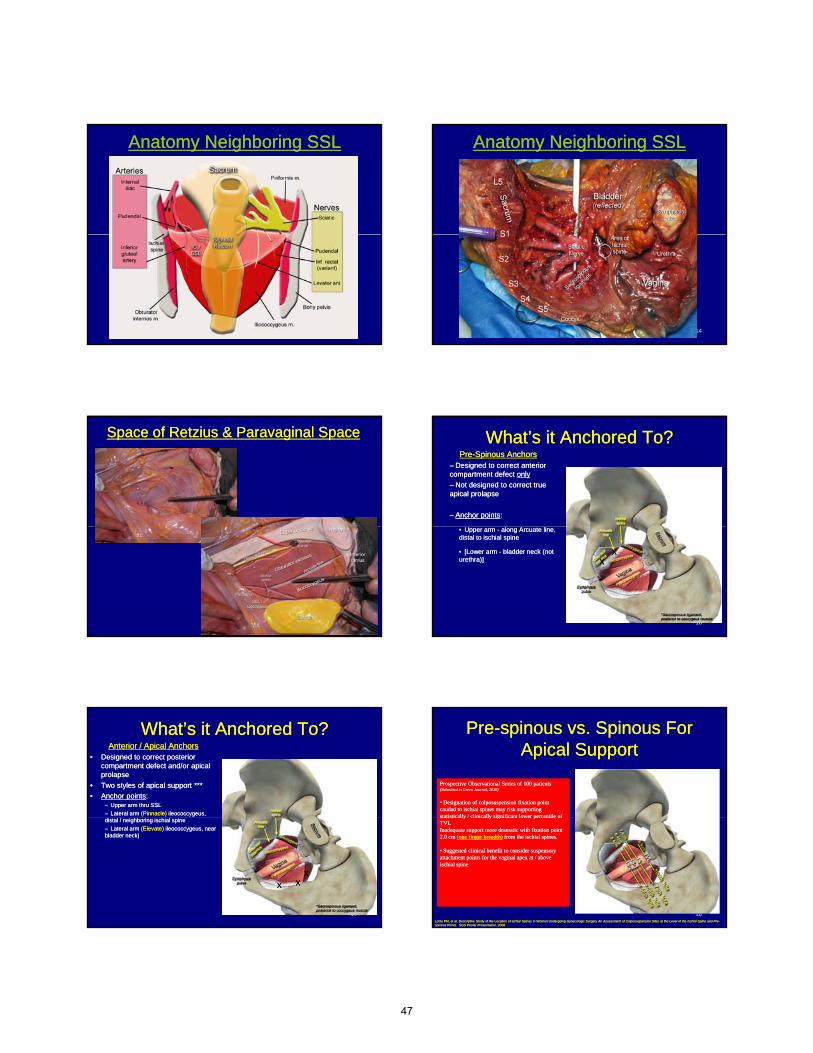
Anatomy Neighboring SSLAnatomy Neighboring SSL
13
Anatomy Neighboring SSLAnatomy Neighboring SSL
14
Space of Retzius & Paravaginal SpaceSpace of Retzius & Paravaginal Space
15
What’s it Anchored To?What’s it Anchored To?PrePre--Spinous AnchorsSpinous Anchors
–– Designed to correct anterior Designed to correct anterior compartment defect compartment defect onlyonly
–– Not designed to correct true Not designed to correct true apical prolapseapical prolapse
–– Anchor pointsAnchor points::
16
•• Upper arm Upper arm -- along Arcuate line, along Arcuate line, distal to ischial spine distal to ischial spine
•• [Lower arm [Lower arm -- bladder neck (not bladder neck (not urethra)]urethra)]
XXXX
What’s it Anchored To?What’s it Anchored To?Anterior / Apical AnchorsAnterior / Apical Anchors
•• Designed to correct posterior Designed to correct posterior compartment defect and/or apical compartment defect and/or apical prolapseprolapse
•• Two styles of apical support ***Two styles of apical support ***
•• Anchor pointsAnchor points::–– Upper arm thru SSLUpper arm thru SSL
–– Lateral arm Lateral arm (Pinnacle)(Pinnacle) ileococcygeus, ileococcygeus,
17
distal / neighboring ischial spine distal / neighboring ischial spine
–– Lateral arm Lateral arm (Elevate)(Elevate) ileococcygeus, near ileococcygeus, near bladder neck) bladder neck)
XXXXXX
PrePre--spinous vs. Spinous For spinous vs. Spinous For Apical SupportApical Support
Prospective Observational Series of 100 patients Prospective Observational Series of 100 patients (Submitted to Green Journal, 2010)(Submitted to Green Journal, 2010)
•• Designation of colposuspension fixation point Designation of colposuspension fixation point caudad to ischial spines may risk supporting caudad to ischial spines may risk supporting statistically / clinically significant lower percentile ofstatistically / clinically significant lower percentile of
Prospective Observational Series of 100 patients Prospective Observational Series of 100 patients (Submitted to Green Journal, 2010)(Submitted to Green Journal, 2010)
•• Designation of colposuspension fixation point Designation of colposuspension fixation point caudad to ischial spines may risk supporting caudad to ischial spines may risk supporting statistically / clinically significant lower percentile ofstatistically / clinically significant lower percentile of
18
statistically / clinically significant lower percentile of statistically / clinically significant lower percentile of TVLTVLInadequate support more dramatic with fixation point Inadequate support more dramatic with fixation point 2.0 cm 2.0 cm (one finger breadth)(one finger breadth) from the ischial spines. from the ischial spines.
•• Suggested clinical benefit to consider suspensory Suggested clinical benefit to consider suspensory attachment points for the vaginal apex at / above attachment points for the vaginal apex at / above ischial spineischial spine
statistically / clinically significant lower percentile of statistically / clinically significant lower percentile of TVLTVLInadequate support more dramatic with fixation point Inadequate support more dramatic with fixation point 2.0 cm 2.0 cm (one finger breadth)(one finger breadth) from the ischial spines. from the ischial spines.
•• Suggested clinical benefit to consider suspensory Suggested clinical benefit to consider suspensory attachment points for the vaginal apex at / above attachment points for the vaginal apex at / above ischial spineischial spine
Lotze PM, et al. Descriptive Study of the Location of Ischial Spines in Women Undergoing Gynecologic Surgery Lotze PM, et al. Descriptive Study of the Location of Ischial Spines in Women Undergoing Gynecologic Surgery An Assessment of Colposuspension Sites at the Level of the Ischial Spine and PreAn Assessment of Colposuspension Sites at the Level of the Ischial Spine and Pre--spinous Points. SGS Poster Presentation, 2008.spinous Points. SGS Poster Presentation, 2008.
47
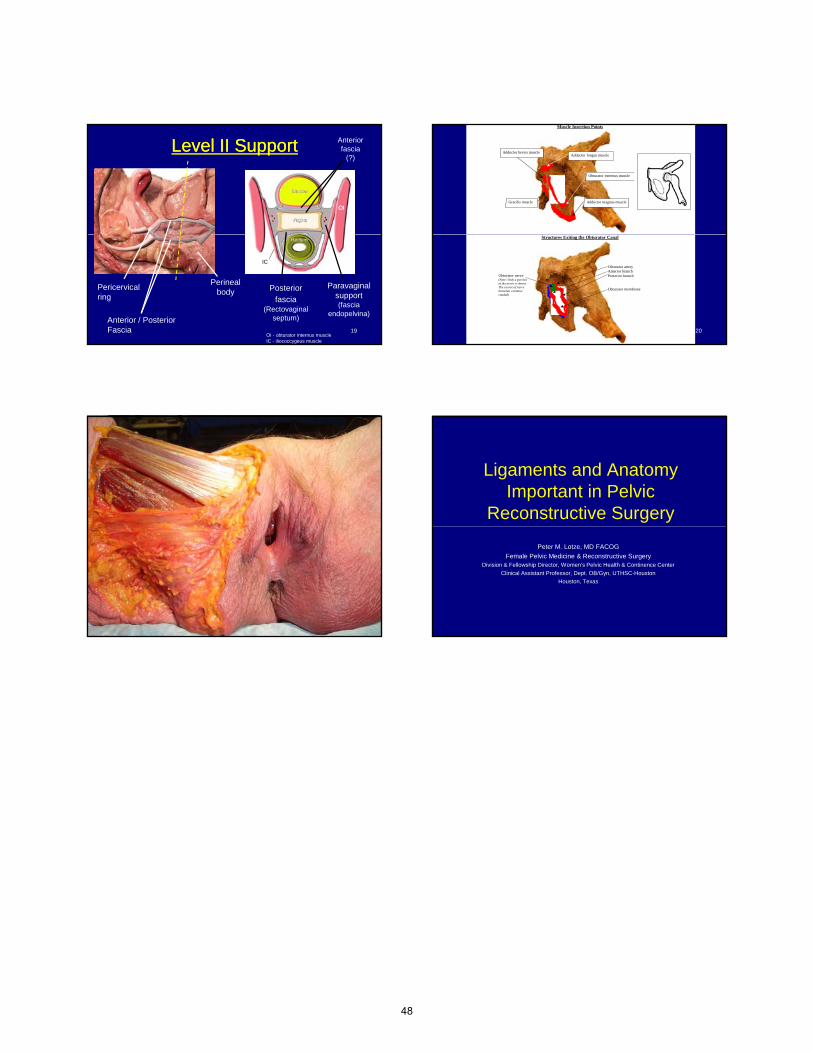
Level II SupportLevel II Support Anterior fascia
(?)
OIOI
19
Pericervicalring
Anterior / PosteriorFascia
Perinealbody
Paravaginal support(fascia
endopelvina)
Posterior fascia
(Rectovaginal septum)
IC
OI - obturator internus muscleIC - iliococcygeus muscle
Muscle Insertion Points
Adductor longus muscle
Adductor magnus muscle
Obturator externus muscle
Adductor brevis muscle
Gracilis muscle
20
Structures Exiting the Obturator Canal
Obturator artery Anterior branch Posterior branch Obturator membrane
Obturator nerve (Note: Only a portion of the nerve is shown. The course of nerve branches continue caudad)
21
Ligaments and Anatomy Important in Pelvic
Reconstructive Surgery
Peter M. Lotze, MD FACOG
Female Pelvic Medicine & Reconstructive SurgeryDivision & Fellowship Director, Women’s Pelvic Health & Continence Center
Clinical Assistant Professor, Dept. OB/Gyn, UTHSC-Houston
Houston, Texas
48

Identifying Retroperitoneal Structures to Stay Safe and Get
Out of Trouble
Identifying Retroperitoneal Structures to Stay Safe and Get
Out of TroubleJubilee Brown, M.D.Jubilee Brown, M.D.
Associate ProfessorAssociate Professor
Jubilee Brown, M.D.Jubilee Brown, M.D.Associate ProfessorAssociate ProfessorAssociate ProfessorAssociate Professor
Department of Gynecologic OncologyDepartment of Gynecologic Oncology
Associate ProfessorAssociate Professor
Department of Gynecologic OncologyDepartment of Gynecologic Oncology
I have no financial relationships to I have no financial relationships to disclose.disclose.
ObjectivesObjectives
• To utilize the anatomy already reviewed in order to preserve all normal structures even in difficult dissections
• To incorporate known anatomy into complex pelvic surgery in order to reverse a complication
• To view examples of dissection using minimally invasive surgery
Safe Access to Retroperitoneal Safe Access to Retroperitoneal StructuresStructures
Safe Access to Retroperitoneal Safe Access to Retroperitoneal StructuresStructures
•• 4 ports4 ports
•• Atraumatic instrumentsAtraumatic instruments
•• Open peritoneumOpen peritoneum
•• 4 ports4 ports
•• Atraumatic instrumentsAtraumatic instruments
•• Open peritoneumOpen peritoneum–– Landmarks are round ligament, EI artery, Landmarks are round ligament, EI artery,
bifurcation of CI arterybifurcation of CI artery
–– Beware ureterBeware ureter
–– Easiest way if disoriented is to grasp round Easiest way if disoriented is to grasp round ligament, lift, and open cephaladligament, lift, and open cephalad
–– Landmarks are round ligament, EI artery, Landmarks are round ligament, EI artery, bifurcation of CI arterybifurcation of CI artery
–– Beware ureterBeware ureter
–– Easiest way if disoriented is to grasp round Easiest way if disoriented is to grasp round ligament, lift, and open cephaladligament, lift, and open cephalad
Open peritoneum – transect round ligament or enter next to it
Open peritoneum – transect round ligament or enter next to it Extend incision along external iliac arteryExtend incision along external iliac artery
49
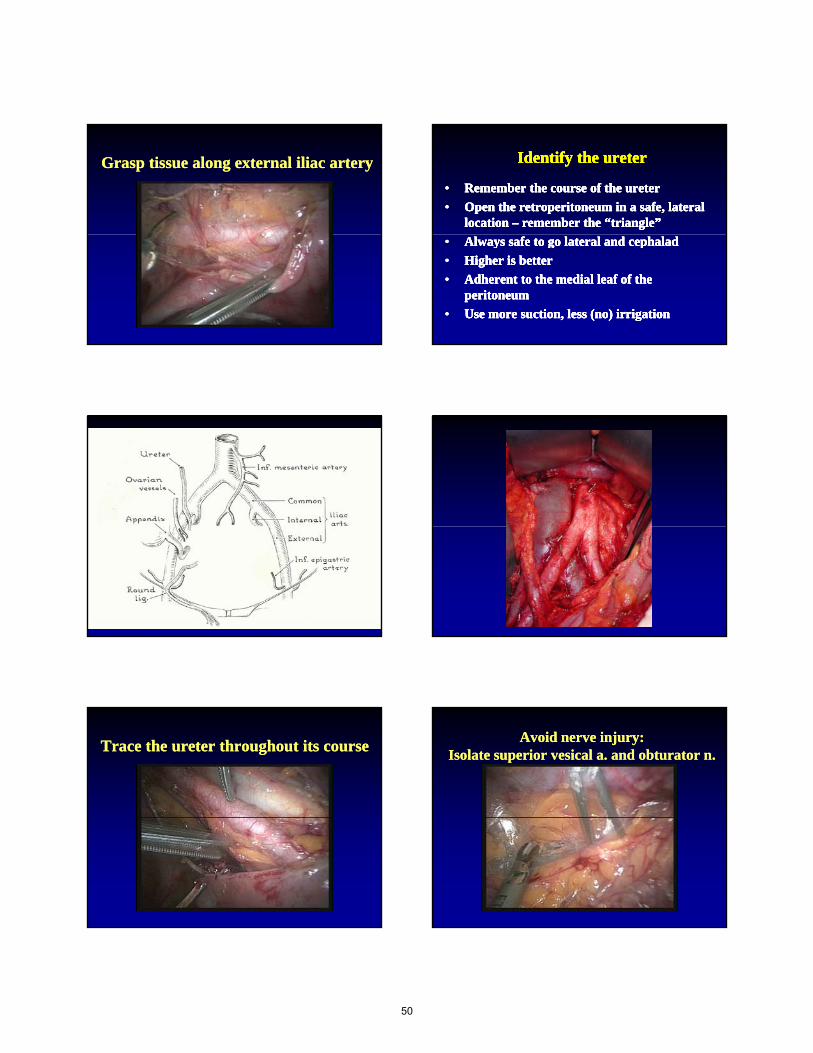
Grasp tissue along external iliac arteryGrasp tissue along external iliac artery Identify the ureterIdentify the ureterIdentify the ureterIdentify the ureter
•• Remember the course of the ureterRemember the course of the ureter
•• Open the retroperitoneum in a safe, lateral Open the retroperitoneum in a safe, lateral location location –– remember the “triangle”remember the “triangle”
•• Remember the course of the ureterRemember the course of the ureter
•• Open the retroperitoneum in a safe, lateral Open the retroperitoneum in a safe, lateral location location –– remember the “triangle”remember the “triangle”
•• Always safe to go lateral and cephaladAlways safe to go lateral and cephalad
•• Higher is betterHigher is better
•• Adherent to the medial leaf of the Adherent to the medial leaf of the peritoneumperitoneum
•• Use more suction, less (no) irrigationUse more suction, less (no) irrigation
•• Always safe to go lateral and cephaladAlways safe to go lateral and cephalad
•• Higher is betterHigher is better
•• Adherent to the medial leaf of the Adherent to the medial leaf of the peritoneumperitoneum
•• Use more suction, less (no) irrigationUse more suction, less (no) irrigation
Trace the ureter throughout its courseTrace the ureter throughout its courseAvoid nerve injury:
Isolate superior vesical a. and obturator n.Avoid nerve injury:
Isolate superior vesical a. and obturator n.
50
Thank You !
51

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsianIndo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
52