w s.s#/snv patient information (confidential)
TRANSCRIPT
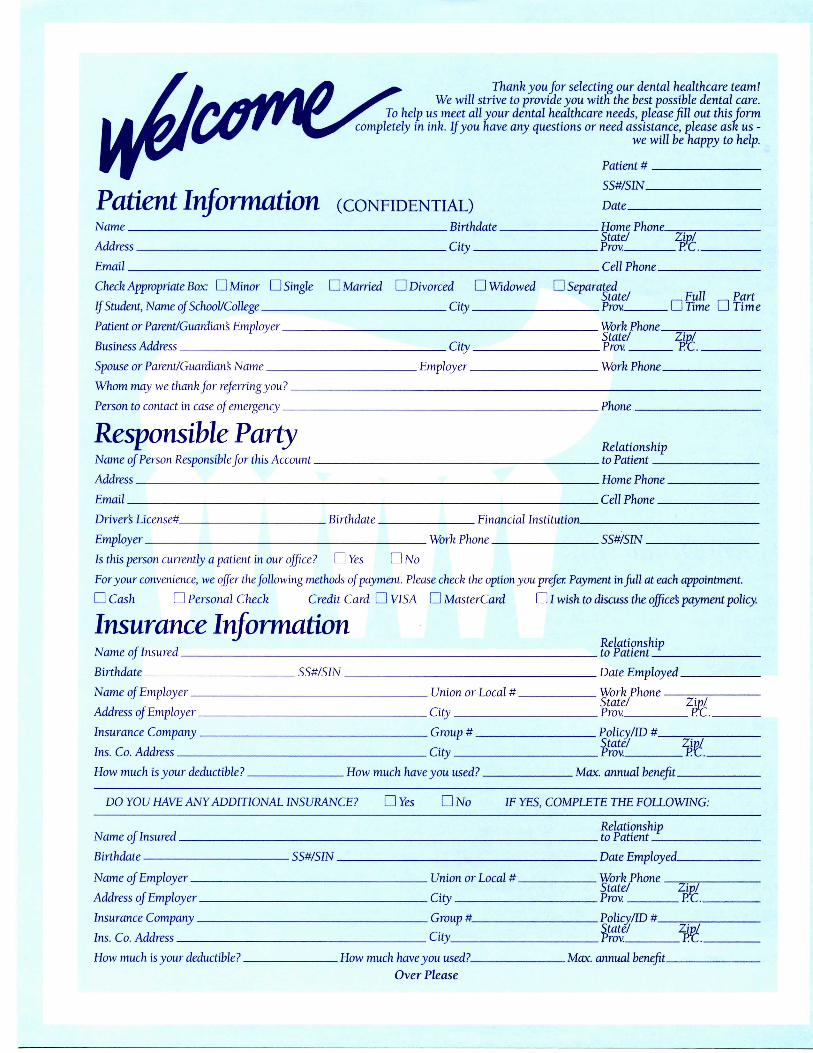
Thank you for selecting our dental healthcare team!We will strive to provide you with the best possible dental care,
help us meet all your dental healthcare needs, please fill out this formely in ink. If you have any questions or need assistance, please ask us -
we will be happy to help.
' W
Patient InformationName:
Address
Chech Appropriate Box: D Minor D Single
If Student Nnme nf School/College
Patient or Parent/Guardian's Emplover
Business Address
Spouse or Parent/Gunrdinn's Nnme
Whom may we thnnk fnr referringyou?
Person to contact in case of emergency
Responsible PartyName of Person Responsible for this Account
Address
Driver's Licensed
Employer
(CONFIDENTIAL)Birthdate
City
D Married D Divorced D Widowed
C.itv
C.itv
Employer
s.s#/snvDate
Home PhoneState/ Zip/Prov PYT
Cell Phone
D SeparatedState/ r-iFu^ r-i PartProv. 1 1 Time 1 1 Time
Work PhoneState/ Zip/Prov PT.
Work Phone.
Phone
Relationshipto Patient
Home Phone
Cell Phone
Birthdate Einamcial Institution
Work Phone SSX/S1N
Is this person currently a patient in our office? D Yes D No
For jour convenience, we ojfer the/oMowing methods of payment. Please check the option you prefer. Payment in full at each appointment.
DCash D Personal Check Credit Card D VISA D MasterCard DI wish to discuss the office's payment policy.
Insurance InformationJ
Name of Insured
Birthdate
Name of Emplover
Address of Emplover
Insurance Company
Ins. Co. Address
How much is your deductible?
SS#/SIN
Union or I oca] #
C.itv
Group #
C.itv
How much have you used?
DO YOU HAVE ANY ADDITIONAL INSURANCE? DYes DNo IF
Name nf Insured
Birthdate
Name of Emplover
Address of Emplover
Insurance Company
Ins Co. Address
How much is your deductible?
SS#/S1N
Union or 1 oral #
C.itv
Group #
Citv
How much have you used?
Over Please
Relationshipto Patient
Date Employed
Work PhoneState/ Zip/Prov. Rr
Policv/lD #
8g£ WMate annual benefit
YES, COMPLETE THE FOLLOWING:
Relationshipto Patient
Date Employed
Work PhoneState/ Zip/Prov PC.
Pnlicy/ID #State/ Zip/Prov PT
Max. annual benefit
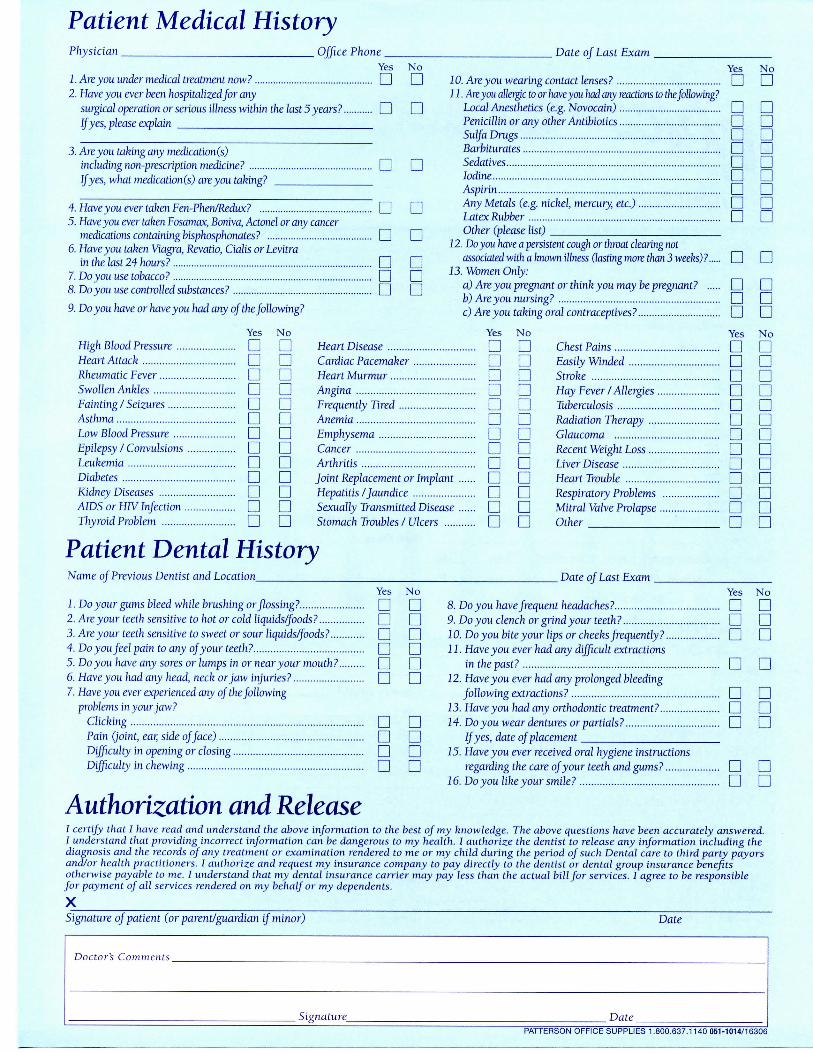
Patient Medical HistoryPhysician _ Office Phone . Date of Last Exam
Yesn No
D1. Are you under medical treatment now?2. Have you ever been hospitalized for any
surgical operation or serious illness within the last 5 years? I I I IIf yes, please explain
3. Are you taking any medicalion(s)including non-prescription medicine? CD CDIf yes, what medication(s) areyou taking?
4. Haveyou ever taken Fen-Phen/Redux?5. Haveyou ever taken Fosamax, Boniva, Actonel or any cancer
medications containing bisphosphonates? D6. Haveyou taken Viagra, Revatio, Cialis orLevitra
in the Iast24 hours? Q7. Do you use tobacco? CD8. Do you use controlled substances? I I
9. Doyou have or haveyou had any of the/ollowing?
n nnnnn
Yes NoJO. Areyou wearing contact lenses? CD CD11. Areyou allergic to or haveyou had any reactions to the following?
Local Anesthetics (e.g. Novocain) I I I IPenicillin or any other Antibiotics CD CDSul/aDmgs CD CDBarbiturates CD CDSedatives CD CDIodine I I I IAspi?in CD CDAny Metals (e.g. nickel, mercury, etc.) CD CDLatex Rubber CD CDOther (please list)
12. Do you have a persistent cough or throat clearing notassociated with a known illness (lasting more than 3 weeks)? I I I I
13. Women Only:a) Areyou pregirant or think you may be pregnant? I I CDb) Areyou nursing? CD CDc) Areyou taking oral contraceptives? CD CD
Yes NoHigh Blood Pressure CD CDHeart Attack CD CDRheumatic Fever CD CDSwollen Ankles I I I IFainting /Seizures CD CDAsthma CD CDLow Blood Pressure CD I IEpilepsy / Convulsions I I I ILeukemia I I CDDiabetes CD CDKidney Diseases CD CDAIDS or HIV Injection CD CDThyroid Problem CD CD
Yes NoHeart Disease CD CDCardiac Pacemaker CD CDHeart MurmurAnginaFrequently TiredAnemia...
a na aa aCD a
Emphysema CD I I
Yes NoCD aa nn Da an a
a nn an aa a
Sexually Transmitted Disease CD CDStomach Troubles /Ulcers CD CD
CancerArthritisJoint Replacement or ImplantHepatitis /Jaundice ..
Patient Dental HistoryName of Previous Dentist and Location
Chest PainsEasily WindedStrokeHay Fever / AllergiesTuberculosisRadiation Therapy I |Glaucoma CD CDRecent Weight Loss Q QLiver Disease CD I IHeart Trouble CD CDRespiratory Problems CD CDMitral Valve Prolapse Q CDOther D D
Date oJ Last ExamYes
L Do yourgiuns bleed \vhile brushing or flossing? [ |2. Are your teeth sensitive to hot or cold liquids/foods? CD3. Are your teeth sensitive to sweet or sour liquids/foods? CD
No YesI | 8. Doyou have frequent headaches? CDI I 9. Doyou clench or grind your teeth? CDCD .10. Do you bite your lips or cheeks frequently? CDCD 11- Have you ever had any difficult extractionsD in the past? CDCD 12. Have you ever had any prolonged bleeding
following extractions? CD13. Haveyou had any orthodontic treatment? CD14. Doyou wear dentures orpartials? CD
IJyes, date of placement15. Haveyou ever received oral hygiene instructions
regarding the care of your teeth and gums ? CD16. Doyou like your smile? CD
aan
Nonnaaan
4. Do you feel pain to any of your teeth? CD5. Doyou have any sores or lumps in or near your mouth? | |6. Haveyou had any head, neck or jaw injuries? | |7. Haveyou ever experienced any of the following
problems in your jaw?Clicking | |Pain (joint, ear, side of face) CDDifficulty in opening or closing CDDifficulty in chewing CD
Authorization and ReleaseI certify that I have read and understand the above information to the best of my knowledge. The above questions have been accurately answered.I understand that providing incorrect information can be dangerous to my health. I authorize the dentist to release any information including thediagnosis and the records of any treatment or examination rendered to me or my child during the period of such Dental care to third party payorsand/or health practitioners. I authorize and request my insurance company to pay directly to the dentist or dental group insurance benefitsotherwise payable to me. I understand that my dental insurance carrier may pay less than the actual bill for services. I agree to be responsiblefor payment of all services rendered on my behalf or my dependents.
XSignature of patient (or parent/guardian if minor) Date
aa
Doctor's Comments
_ Signature_ DatePATTERSON OFFICE SUPPLIES 1.800.637.1140 051-1014/16306
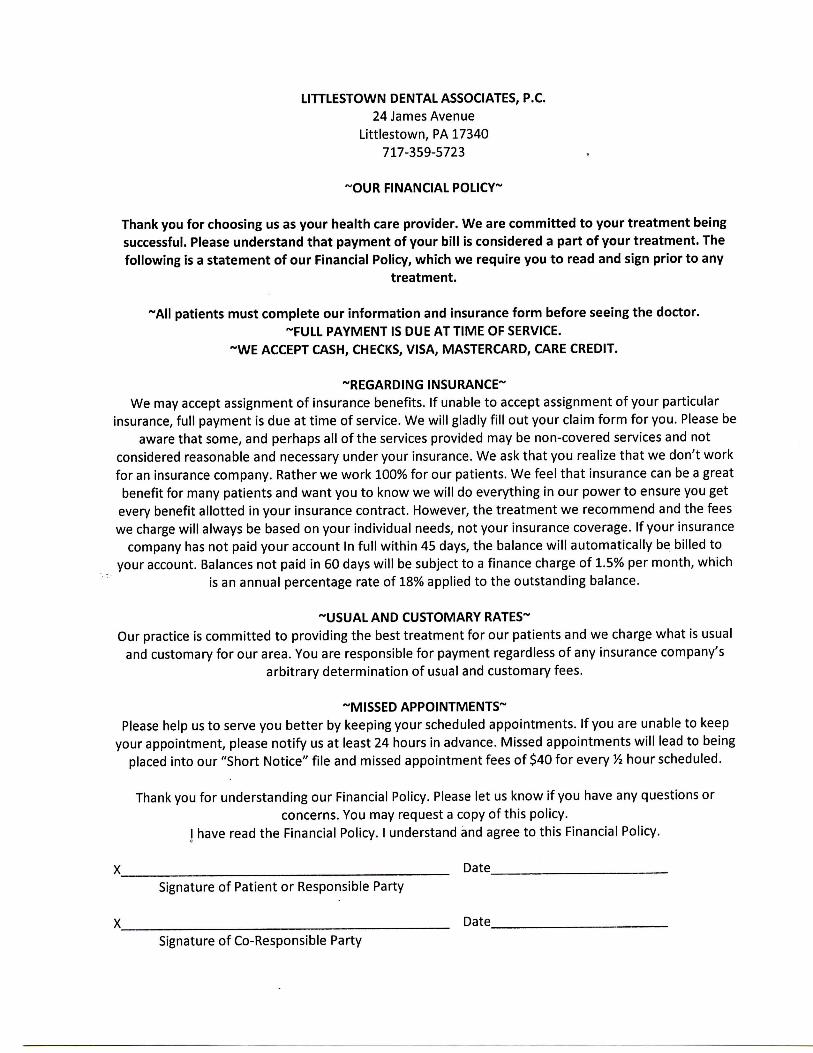
LITTLESTOWN DENTAL ASSOCIATES, P.C.24 James Avenue
Littlestown, PA 17340717-359-5723
-OUR FINANCIAL POLICY~
Thank you for choosing us as your health care provider. We are committed to your treatment beingsuccessful. Please understand that payment of your bill is considered a part of your treatment. Thefollowing is a statement of our Financial Policy, which we require you to read and sign prior to any
treatment.
~AII patients must complete our information and insurance form before seeing the doctor.-FULL PAYMENT IS DUE AT TIME OF SERVICE.
~WE ACCEPT CASH, CHECKS, VISA, MASTERCARD, CARE CREDIT.
-REGARDING INSURANCE-We may accept assignment of insurance benefits. If unable to accept assignment of your particular
insurance, full payment is due at time of service. We will gladly fill out your claim form for you. Please beaware that some, and perhaps all of the services provided may be non-covered services and not
considered reasonable and necessary under your insurance. We ask that you realize that we don't workfor an insurance company. Rather we work 100% for our patients. We feel that insurance can be a greatbenefit for many patients and want you to know we will do everything in our power to ensure you get
every benefit allotted in your insurance contract. However, the treatment we recommend and the feeswe charge will always be based on your individual needs, not your insurance coverage. If your insurance
company has not paid your account In full within 45 days, the balance will automatically be billed toyour account. Balances not paid in 60 days will be subject to a finance charge of 1.5% per month, which
is an annual percentage rate of 18% applied to the outstanding balance.
-USUAL AND CUSTOMARY RATES-Our practice is committed to providing the best treatment for our patients and we charge what is usual
and customary for our area. You are responsible for payment regardless of any insurance company'sarbitrary determination of usual and customary fees.
-MISSED APPOINTMENTS-Please help us to serve you better by keeping your scheduled appointments. If you are unable to keep
your appointment, please notify us at least 24 hours in advance. Missed appointments will lead to beingplaced into our "Short Notice" file and missed appointment fees of $40 for every Vi hour scheduled.
Thank you for understanding our Financial Policy. Please let us know if you have any questions orconcerns. You may request a copy of this policy.
I have read the Financial Policy. I understand and agree to this Financial Policy.
X DateSignature of Patient or Responsible Party
Date_Signature of Co-Responsible Party