images.nature.com · web view“electrical stimulation in the bed nucleus of the stria terminalis...
TRANSCRIPT

Supplementary Appendix“Electrical stimulation in the bed nucleus of the stria terminalis
alleviates severe obsessive-compulsive disorder”Laura Luyten, Sarah Hendrickx, Simon Raymaekers, Loes Gabriëls & Bart Nuttin
Table of contents
Supplementary Methods 2Clinical study 2
Patient selection 2Surgical procedure 2Initial electrical stimulation 3Double-blind randomized crossover design 3Follow-up 3Patient evaluation 3Neuroimaging 4
Statistical analyses 4Psychiatric outcome (crossover trial, after 4 years of follow-up and at last follow-up) 4Neuropsychological outcome (crossover trial) 4Stimulation target versus outcome at last follow-up 5
Neuroanatomical analyses 5Localization of active electrode contacts 5Determination of stimulated volume 5
Supplementary Results 6Serious adverse, device-related and adverse events 6
Serious adverse events 6Device-related adverse events 6Adverse events 6Table S1: Serious adverse events 7Table S2: Complete list of adverse events 8Conclusion 10
Stimulation parameters and electrode polarity – crossover trial 11Table S3: Stimulation characteristics crossover ON phase 11
Neuropsychological tests – crossover trial 12Results 12Conclusion 12Table S4: Neuropsychological test scores 13
Qualitative analysis – crossover trial 14Introduction & Method 14Results 14Conclusion 15Fig. S1: Summary of the qualitative analysis 15Table S5: Exhaustive list of the reported observations 16
Active contacts during crossover, optimal open-label period and at last follow-up 18Optimal open-label period 18Comparison of stimulation targets during crossover and optimal open-label period 18Comparison of stimulation targets during optimal open-label period and at last follow-up 18Conclusion 18
Patient data included in previously published papers 19
Supplementary References 20
Supplementary Appendix Luyten et al. 2015 – DOI: tbd 1/20

Supplementary Methods
Clinical study
Patient selection
Between 1998 and 2010, 24 patients were selected by a Committee for Neurosurgery for Psychiatric Disorders according to strict selection criteria . Inclusion criteria were a principal diagnosis of OCD of disabling severity, based upon a structured clinical interview for the Diagnostic and Statistical Manual of Mental Disorders: DSM-IV , with a Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) score of at least 30/40 and a Global Assessment of Functioning (GAF) score of 45 or less . This level of impairment should have persisted for a minimum of 5 years, despite adequate trials (except in case of intolerance) with two selective serotonin reuptake inhibitors and clomipramine, augmentation strategies (i.e. antipsychotics), and cognitive behavioral therapy. Patients had to be between 18 and 60 years of age, and able to understand and comply with instructions and provide their own written informed consent to be included in the study. Patients were excluded in case of a current or past psychotic disorder, any clinically significant disorder or medical illness affecting brain function or structure (other than motor tics or Gilles de la Tourette syndrome), or current or unstably remitted substance abuse. Comorbid anxiety or depressive disorder was not an exclusion criterion. Clinical evaluations and surgeries were performed at the University Hospitals of Antwerp (psychiatric assessment until 2007) and Leuven (psychiatric assessment from 2007 onwards and all surgeries), Belgium. During a period of at least 4-6 weeks before surgery, medication was tapered off to a minimum and no psychotherapy was administered.The study protocol was reviewed and approved by the University Hospitals’ Ethics Committees and is in accordance with the Declaration of Helsinki of 1975 (Rev. 1983).
Surgical procedure
Two quadripolar electrodes (Models 3887, 3387 or 3391; Medtronic, Inc., Minneapolis, MN, USA) were stereotactically implanted into the bilateral anterior limbs of the internal capsule (ALIC), similar to the targets used for anterior capsulotomy . The most ventral contact (contact 0) was implanted in the grey matter ventral to ALIC and the other contacts (1-2-3) were placed in ALIC. Preliminary analyses correlating electrode position and Y-BOCS scores indicated a better outcome with a slightly more posterior target. For subsequent patients, this was formalized in a new protocol that was approved by the Ethics Committee (Clinical Trial NCT01985815). The optimized target was more posterior, ventral and medial, with at least one contact (usually contact 0) in the bed nucleus of the stria terminalis (BST). Taking into account vascularization, both electrodes were implanted symmetrically through precoronal burr holes. Note that Patient 5 received additional electrodes bilaterally aimed at the mediodorsal thalamus, on account of its role in the CSTC circuit and because its connections with the prefrontal cortex are interrupted with classical anterior capsulotomy . Prophylactic antibiotics were administered. Surgery was performed under general (n = 4) or local (n = 20) anesthesia, depending on the patient’s choice. Within two weeks after electrode implantation, bilateral implantable pulse generators (IPGs) (Itrel 2, Synergy, or Kinetra; Medtronic, Inc.) were implanted in the abdominal (n = 21) or subclavicular (n = 3) area and connected to the electrodes.
Supplementary Appendix Luyten et al. 2015 – DOI: tbd 2/20

Initial electrical stimulation
After implantation of the electrodes, initial stimulation parameters were explored by the neurosurgeon and psychiatrist, using an external programming device. Several combinations of the four electrode contacts, using different frequencies, amplitudes and pulse widths were assessed, based on acute (within 5 minutes) mood improvement or reduction of anxiety or obsessive thoughts, while the patient was unaware of the stimulation parameters. Contact combinations with the lowest threshold for these favorable effects were used. After 1-2 weeks, the IPGs were implanted. During the next weeks or months, stimulation parameters were further optimized. This time-consuming procedure evaluated virtually all contact combinations, high and low frequencies and pulse widths. Amplitudes were increased slowly or quickly, sometimes up to 10.5 V, which is the maximal voltage delivered by the IPG. The aim of this optimization period was to determine stimulation parameters resulting in satisfactory alleviation of OCD symptoms, without adverse effects. The parameters should have a relatively stable effect, in order to be of use during the crossover phase of this clinical study.
Double-blind randomized crossover design
After the initial optimization period, patients entered the crossover design, with 3 months of stimulation ON and 3 months of stimulation OFF. This part of the study was double-blind (patient and evaluating psychiatrist were not informed about the stimulation condition) and randomized (patients were assigned to an ON-OFF or OFF-ON order) . The optimized stimulation parameters and electrode polarity were maintained throughout the crossover ON phase, while in the OFF phase no stimulation (0 V) was delivered. An ‘escape procedure’ was foreseen if a crossover phase led to intolerable suffering. For instance, it was possible that during the optimization period or potentially a preceding stimulation ON phase, patients experienced clear therapeutic effects and that returning to a status without stimulation (OFF phase) would be unbearable. If this was the case, the patient was thoroughly evaluated by the blinded psychiatrist, who then decided if the crossover phase could be prematurely ended. If the shortened phase was the first crossover period, the neurosurgeon changed the parameters and started the next phase, without unblinding the patient and psychiatrist.After completing both crossover phases, the patient and psychiatrist were unblinded, and the patient could choose to be continuously stimulated. Fine-tuning of stimulation is a continuing process, and, if indicated, parameters (i.e., amplitude, pulse width, frequency, choice of cathodes) were adapted during follow-up.
Follow-up
The first patients have now been followed up for 16 years, while the last patients have had a follow-up of 4 years. In this paper, we will report on the stimulation effects for all patients, 4 years after implantation and at last follow-up (May 2014).In addition, we determined the optimal open-label period (and corresponding stimulation parameters), i.e. a period of at least 2 months during which the patient experienced the lowest Y-BOCS scores since implantation. Detailed descriptions and analyses of the patients’ long-term clinical evolution are ongoing and will be reported separately.
Patient evaluation
At several time points, patients were evaluated using standardized psychiatric and neuropsychological questionnaires and tests.The primary outcome measure, assessing the treatment effect on obsessions and compulsions, was the psychiatrist-rated Y-BOCS , which was obtained 2 weeks before surgery, during the ON and OFF phases
Supplementary Appendix Luyten et al. 2015 – DOI: tbd 3/20

of the crossover, and approximately 4 years after implantation. In addition, it was regularly rated during psychiatric consultations. A 35% decrease in Y-BOCS was defined as the responder criterion . At the same time, we evaluated the patients’ depressive and anxiety symptoms (Hamilton Depression Rating Scale (HAM-D) and Hamilton Anxiety Rating Scale (HAM-A)) and their overall functioning (Global Assessment of Functioning (GAF)) .In addition to these psychiatric assessments, several neuropsychological evaluations were performed before surgery and during the ON and OFF phases: Complex Figure Test of Rey, Audio Verbal Learning Test, Wisconsin Card Sorting Test, Word Fluency test, Raven Standard progressive matrices, STROOP and Trail Making Tests A en B .Besides these standardized, quantitative evaluations, patients were regularly seen by the neurosurgeon and psychiatrist, resulting in qualitative reports of how the patient was doing, including favorable and potential side effects of the treatment. These lists of (serious) adverse events were classified as being device-related, surgery-related, (probably) (not) stimulation-induced or unrelated to DBS.
Neuroimaging
Structural magnetic resonance imaging (MRI), computed tomography (CT) and/or functional MRI (fMRI) scans were obtained before and after surgery. In addition, part of the patients underwent 18F-fluorodeoxy-glucose positron emission tomography (PET), before surgery and during the crossover study . The nuclear imaging results have been reported elsewhere .
Statistical analyses
Psychiatric outcome (crossover trial, after 4 years of follow-up and at last follow-up)
Crossover trial (n = 17). Percentage improvement was calculated as (OFF minus ON)/OFF for Y-BOCS, HAM-A and HAM-D scores. Improvement in GAF score was calculated as ON minus OFF. Preoperative, ON and OFF scores were compared using a Friedman ANOVA (p < .05), followed by Wilcoxon matched pairs tests with correction for multiple testing (Bonferroni: .05/3, p < .017).Four-year follow-up (n = 18) and last follow-up (n = 24). Percentage improvement was calculated as (preoperative minus follow-up score)/preoperative score for Y-BOCS, HAM-A and HAM-D data. Improvement in GAF score was calculated as follow-up minus preoperative score. Preoperative and follow-up scores were compared using a Wilcoxon test (p < .05). Correlation between the Y-BOCS score during the crossover ON phase and at follow-up was calculated using a Spearman coefficient (p < .05).
Neuropsychological outcome (crossover trial)
Test scores (7 tests, resulting in a total of 22 subscores) were analyzed using repeated measures one-way ANOVA (preoperative vs ON vs OFF) with Tukey's posthoc tests. If the sphericity assumption was violated (Mauchly's test p < .05), a Greenhouse-Geisser correction was applied. If the normality and/or equal variance assumptions were violated, data were analyzed using a non-parametric Friedman ANOVA, followed by Wilcoxon tests with correction for multiple testing (Bonferroni: .05/3, p < .017). For exploratory purposes, the significance level of the ANOVA main effects was set at .05. Using a more stringent criterion, we also checked significance of the main effects after correction for multiple testing (Bonferroni: .05/22 subtests, p < .002). Analyses were conducted on data from 16 patients (neuropsychological tests were not carried out in one patient who completed the crossover design).
Supplementary Appendix Luyten et al. 2015 – DOI: tbd 4/20

Stimulation target versus outcome at last follow-up
Using the predefined criterion of at least 35% Y-BOCS improvement to define a satisfactory effect of stim-ulation, we investigated if one of both brain targets (i.e., ALIC or BST) resulted in a better outcome than the other at last follow-up, in a 2x2 contingency table with a Fisher's exact test (p < .05). Note that this trial was not conceived as a study to compare two targets. Nevertheless, the relative variation of the active contacts’ location does allow us to evaluate the target-outcome relation with this posthoc analysis.
Neuroanatomical analyses
Localization of active electrode cathodes
It is generally assumed that stimulation effects mainly take place at the negative contacts (cathodes), while clinically relevant effects near the positive anode(s) are negligible . Accordingly, if only one contact is used, it is programmed as a cathode, while the case of the pulse generator is positive. In DBS for movement disorders, it is common to use this type of monopolar stimulation, as it results in radial current diffusion, with relatively low stimulation intensities compared to other electrode configurations . Other options include bipolar (one cathode and one anode on the same lead) or multipolar (more than one cathode and/or anode on the same lead) stimulation. Bipolar stimulation creates a more focused stimulated area, mainly near the cathode, which can be useful to limit side effects elicited by more diffuse monopolar stimulation. In addition, it can be indicated to have several adjacent cathodes, to create a larger, elongated stimulated volume .To investigate the locus of action of DBS in more depth, we indicated the center of the active contacts (cathodes) on Mai’s brain atlas . Using pre- and post-operative MR and CT scans, we localized the cathodes for each patient during crossover, the optimal open-label period and at last follow-up. If available, we merged pre-operative MR and post-operative CT scans using Medtronic FrameLinkTM Software (Medtronic Inc., Minneapolis, MN, USA). For the other patients, post-operative MR scans were used. All digital images were manually reformatted along the AC-PC plane. Finally, contact positions were determined by two observers (LL & BN) and transferred to the atlas plates.
Determination of stimulated volume
In addition to the localization of the active contacts, we also estimated the extent of brain tissue influenced by stimulation. The stimulated volume is largely spherical or ellipsoid, and depends on several factors, e.g., stimulation parameters, electrode impedance and size, localization of the contact in gray or white matter and mono-, bi- or multipolar stimulation . However, it can be assumed that, for monopolar stimu-lation and stimulation with non-adjacent cathodes, about 1 mm per volt (starting from the center of the negative contact) will be influenced, up till a voltage of about 4 V. With higher voltages, the radius will be proportionally smaller. See Table S3 for an overview of the estimated radii for each contact, based upon . Adjacent cathodes produce a broader, more elliptical field of stimulation, with a radius perpendicular to the lead of about 1.2 mm per volt and a major axis extending about 1 mm per volt from the cathodes. For bipolar stimulation, the field spreading from the cathode has a radius of about 0.6 mm per volt.We preferred a conservative and approximate calculation of the stimulated tissue, rather than attempting to model the volume in a more detailed way. First, because the existing complex models are primarily based on DBS targets for Parkinson’s disease, which differ in their anatomical properties from our target . Second, because the additional clinical value of detailed estimations is most likely limited for our purposes.
Supplementary Appendix Luyten et al. 2015 – DOI: tbd 5/20
Supplementary Results
Serious adverse, device-related and adverse events
Serious adverse events
Table S1 shows the 25 serious adverse events that were recorded during 180 patient-years of follow-up in the full cohort of 24 patients. Note that one of the patients who experienced a tonic-clonic insult had a history of head and spine trauma, and was under influence of alcohol (5 units) and sleep deprivation. The other patient was not sleep-deprived, but was known to be a moderate alcohol abuser (2-3 units daily). One patient stated that she only experienced absences during stimulation, while another patient continued to have seizures after turning off stimulation. Another patient only developed symptoms after one electrode was replaced and implanted in a slightly posterior target.In addition to the 25 serious events, we counted 23 hospitalizations (11 patients) which were illness-related and in some instances worsened by difficult family circumstances.
Device-related adverse events
There were several device failures and device-related adverse events during the long-term follow-up of our patients. Although most of them resulted in surgery (which is not surprising given that the devices are implanted), there were no life-threatening events, nor was there any permanent physical impairment.In 2 patients, one of the leads was broken and therefore replaced. Three patients had faulty extensions (5 defects in total) which were revised. One patient had a malfunctioning stimulator which was replaced. In one patient, repositioning of the stimulator was indicated because of irritation and skin atrophy, due to weight loss. In 3 patients, stimulators were turned off (2 patients, on repeated occasions) or had been reset to factory settings (1 patient). The reasons for these unwanted changes in stimulation parameters were unknown, but in these cases, patients were reminded to avoid strong electric or magnetic fields (e.g. large stereo speakers with magnets, airport/security screening devices).
Adverse events
Apart from the abovementioned serious and device-related adverse events, patients reported many other complaints. In Table S2, these adverse events are listed and categorized as being surgery-related, stimulation-induced, probably (not) stimulation-induced or unrelated to DBS. To not overload the text with an enumeration of all complaints, we will only mention adverse events that were reported by at least 10 patients.A common surgery-related complaint was an uncomfortable feeling around the extension cables (12/24 patients). Frequent stimulation-induced adverse events included fatigue (18/24), memory complaints (16/24, although this could not be objectified with neuropsychological tests in the crossover study, cf infra), disinhibition (12/24), increased assertiveness (12/24), logorrhea (10/24) and hyperactivity (10/24). Adverse events that were probably stimulation-induced, comprised weight gain (13/24), weight loss (10/24), insomnia (13/24), irritability (16/24), tension/nervousness (13/24) and family problems (13/24, probably partially stimulation-induced). Finally, there were some adverse events which were probably not stimulation-induced, e.g., depressed feelings (13/24), suicidal thoughts (12/24) and headache (11/24).
Supplementary Appendix Luyten, Gabriëls & Nuttin 6/20

Serious adverse eventsPatient number
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 # patients
Intracerebral hemorrhage NSI 0 0 2
Suicide attempt PNSI 10 123 125 4 3
Fracture (ankle, foot, arm, leg, hand, rib) (P)NSI 63 39 9 24 7 23 6
Polytrauma (cliff diving, car accident) PNSI 45 1 2
Tonic-clonic epileptic seizure PSI 64 32 2
Absences or partial epileptic seizure PSI 57 22 51 3
Severe obstructive sleep apnea PNSI 17 6 2
Morbid obesity (gastric bypass) PSI 72 1
Pyelonephritis and pyonephrosis PNSI 6 1
Transient ischemic attack PNSI 67 1
Prostate carcinoma (brachytherapy) NSI 41 1
# serious adverse events (total = 25) 0 3 0 1 3 0 0 1 2 0 2 1 1 0 0 2 1 1 1 2 0 1 2 1
Table S1: Serious adverse events.An overview of the serious adverse events recorded until last follow-up. Serious adverse events are shown per patient, including the moment of occurrence (number of months after implantation, italic, in light gray boxes). NSI: not stimulation-induced; PNSI: probably not stimulation-induced; PSI: probably stimulation-induced.
Supplementary Appendix Luyten, Gabriëls & Nuttin 7/20

Table S2: Complete list of adverse events.Complete list of (device-unrelated) adverse events for all 24 patients, until last follow-up, classified as being either surgery-related, stimulation-induced, probably stimulation-induced, probably not stimulation-induced or unrelated to DBS.
ADVERSE EVENTS, SURGERY-RELATED # patients
Surgical Misplacement electrode, intraoperative correction 1Rash iodine alcohol 1
SensationsUncomfortable feeling around extension cables 12Pain around implantable pulse generator (IPG) 7Painful luxation IPG below ribs 3
Infections Skin infection coagulase negative S. aureus (treated with antibiotics) 1Local transient inflammation of suture after IPG replacement 1
ADVERSE EVENTS, STIMULATION-INDUCED # patients
Psychiatric orcognitive
Memory complaints 16Disinhibition 12Increased assertiveness 12Logorrhea 10Hyperactivity 10Hypomania 4Confusion 4
Neurological
Patient smells something transiently 7Paresthesia, pain or twitches in cheek or jaw, teeth grinding 6Transient perseveration in foreign language 1Micrographia 1
Sexual
Decreased libido 7Increased libido 4Ejaculation problems 5Erection problems 4
Gastro-intestinal Diarrhea 3Slow gastric emptying 1
Other Fatigue 18Cough 2
ADVERSE EVENTS, PROBABLY STIMULATION-INDUCED # patientsWeight increase 13Weight decrease 10Insomnia 13Hypersomnia 7Vivid dreams 2Nightmares 1Family problems 13Irritability 16Tension/nervousness 13Apathy 7Aggressivity 6Derealization/depersonalization 4Transpiration 7Nausea 7Tremor 6Disturbed balance 5Palpitations
5
Supplementary Appendix Luyten, Gabriëls & Nuttin 8/20
(Table S2 continued)

Increased tics 4Akathisia 3Transient urinary incontinence 3Nose bleed 2Body odor change 1Song stuck in head 1
ADVERSE EVENTS, PROBABLY NOT STIMULATION-INDUCED # patientsDepressed 13Suicidal thoughts 12Headache 11Anergy 8Amotivation 8Arterial hypertension 5Arterial hypotension 1Vomiting 4Hypercholesterolemia 4Increased urinary frequency 3Medication abuse 2Panic attack 2Dyspnea 2Sprained ankle 2Feeling warm 1Feeling cold 1Blackout 1Episodic retrosternal pain 1Stuttering 1Hyperventilation 1Prolonged QTc-interval 1Hallucinations (bereavement induced) 1Fall from truck resulting in back pain 1Fall from stairs resulting in hematomas 1Minor head injury 1
ADVERSE EVENTS, UNRELATED TO DBS # patients
Infectious
Sinusitis 4Throat infection 3Influenza (H1N1) 2Cystitis 2Pneumonia (treated with antibiotics) 2Chronic prostatitis 1Acute prostatitis 1Herpes labialis 1Verruca vulgaris (heel) 1Mild fever (several weeks, idiopathic) 1
NeuropsychiatricParanoia/oversensitivity 3Binge drinking 2Flashbacks 1
Orthopedic Lumbar pain 4Pain in elbow, knee, heel or shoulder 3Cervicobrachialgia 2Arthrosis hands, knee or hip 2
Supplementary Appendix Luyten, Gabriëls & Nuttin 9/20
(Table S2 continued)

Tennis elbow 1Tendon cyst in wrist 1
Dermatological
Lichen erosivus (leukoplakia) 1Moderate hair loss (telogenic effluvium) 1Psoriasis 1Capillary hemangioma (removed) 1Skin lesions (serpentine form, transient) 1
Gastro-intestinal
Constipation 4Hiatus hernia, gastro-esophageal reflux with cough or esophagitis 3Epigastric pain 1Anal blood loss, small erosions sigmoid 1Cholecystolithiasis 1Fundic gland polyps 1
Gynecological Vaginal discharge 1Endometriosis and ovarian cyst 1
Conclusion
In our sample of 24 patients, we counted 25 serious adverse events during a total of 180 patient-years of follow-up. In addition, there were several device-related events, e.g., replacement of defective electrode leads or extension cables. Other adverse events, including fatigue, weight changes, decreased sleep quality, et cetera, should be examined in clinical practice and in future studies.
Supplementary Appendix Luyten, Gabriëls & Nuttin 10/20
Stimulation parameters and electrode polarity – crossover trial
LEFT RIGHT
Pt Lead IPG Freq (Hz)
PW (µs)
CD (µC/cm²)
ContactsVolt (V)
Estimated volumePolarity
ContactsVolt (V)
Estimated volumePolarity
0 1 2 3 C Shape R1 (mm)
R2 (mm) 0 1 2 3 C Shape R1
(mm)R2
(mm)
1 3887 Itrel 2 100 210 7.4 - - - + 4.3 4.8 12.5 multi - - - + 4.3 4.8 12.5 multi
2 3887 Itrel 2 100 210 13.7 + - + 8.0 3.2 3.2 multi + - + 8.0 3.2 3.2 multi
4 3887 Synergy 100 450 38.6 - + 10.5 3.7 3.7 bi - + 10.5 3.7 3.7 bi
5 3887 Synergy 100 450 25.7 - - + 7.0 6.1 10.1 multi - - + 7.0 6.1 10.1 multi
6 3887 Synergy 100 450 38.6 - + 10.5 3.7 3.7 bi - + 10.5 3.7 3.7 bi
7 3887 Synergy 130 450 27.2 N/A N/A N/A N/A N/A - + 7.4 5.2 5.2 bi
9 3887 Synergy 100 210 6.0 - + 3.5 2.1 2.1 bi - + 3.5 2.1 2.1 bi
10 3887 Kinetra 130 210 6.0 - + 3.5 3.5 3.5 mono - + 3.5 3.5 3.5 mono
11 3887 Synergy 130 90 2.4 - + 3.3 2.0 2.0 bi - + 3.3 2.0 2.0 bi
12 3887 Kinetra 130 330 16.8 - + 6.0 4.8 4.8 mono - + 6.5 4.9 4.9 mono
13 3387 Kinetra 130 330 38.6 - + 7.0 5.1 5.1 mono - + 7.0 5.1 5.1 mono
14 3387 Kinetra 85 240 31.5 - - + 7.1 5.1 5.1 multi - - + 8.6 5.7 5.7 multi
15 3387 Kinetra 130 150 10.0 + - 4.0 2.4 2.4 bi - + 4.0 2.4 2.4 bi
18 3387 Kinetra 100 270 22.6 - - + 5.0 5.2 5.8 multi - - + 5.0 5.2 5.8 multi
19 3387 Kinetra 130 240 28.1 - + 7.0 5.1 5.1 mono - + 7.0 5.1 5.1 mono
20 3387 Kinetra 130 150 16.3 - + 6.5 2.9 2.9 bi - + 6.5 2.9 2.9 bi
21 3391 Kinetra 130 150 8.1 - + 6.5 2.9 2.9 bi - + 6.5 2.9 2.9 bi
Table S3: Stimulation characteristics crossover ON phase.For each patient, the DBS lead model (Medtronic), implantable pulse generator type (Medtronic), stimulation parameters and contact polarity are shown. Contacts 0-3 represent the 4 electrode contacts on each lead and C refers to the metal case of the IPG. In addition, this table shows the dimensions of the approximate stimulated volume surrounding the cathode(s) (see Fig. 1). R1 and R2 are the radii of the estimated ellipse originating from the negative contact(s). Note that Patient 1 was stimulated with different intensities (4.0 – 3.0 – 4.4 – 5.5 V) during the ON phase, resulting in a weighted average voltage of 4.3 V. Pt: patient; IPG: implantable pulse generator; Freq: frequency; PW: pulse width; CD: charge density, estimated per contact using a 1-kOhm impedance; Volt: voltage; mono: monopolar; bi: bipolar; multi: multipolar; N/A: not applicable.Supplementary Appendix Luyten, Gabriëls & Nuttin 11/20

Neuropsychological tests – crossover trial
Results
Table S4 shows the neuropsychological (sub)test scores. Preoperative measurements were obtained on average 34 days before implantation. ON data were collected at a median of 60 days after the start of the ON phase, and OFF data 38 days after the start of the OFF phase.
Comparison of preoperative and OFF-phase data found no significant differences, indicating that preoperative and non-stimulation neuropsychological function was comparable (except for the Complex Figure Test of Rey - Late Recall, which indicated slightly better values during OFF than preoperatively (19 vs 17, p = .03)).There were no significant differences between preoperative, ON or OFF measurements for the following tests: Wisconsin Card Sorting Test, Word Fluency Test and Raven's Standard Progressive Matrices.Repeated measures ANOVA did indicate differences in all subtests of the Complex Figure Test of Rey: Copy (F(2,30) = 4.14, p = .03), Immediate Recall (F(1.4, 21.4) = 7.20, p < .01) and Late Recall (F(2,30) = 7.65, p < .01). Tukey's posthoc tests showed higher values during stimulation ON compared to the OFF phase (Copy: p = .03) or compared to the preoperative measurement (Immediate Recall: p < .01, Late Recall: p < .01).Repeated measures ANOVA showed significant main effects in two subscores of the Auditory Verbal Learning Test: First Trial List A (F(2,30) = 4.25, p = .02) and Interference List B (F(2,30) = 12.02, p < .001). Tukey's posthoc tests indicated higher values during stimulation ON compared to the OFF phase (Interference List B: p < .01) or compared to the preoperative measurement (First Trial List A: p = .02, Interference List B: p < .001).Repeated measures ANOVA found significant main effects in all subtests of the Stroop test: Chart B Words (F(1.2,18.5) = 6.95, p = .01), Chart C Words (F(2,30) = 18.48, p < .0001) and Interference C-B (F(1.4,21.6) = 5.33, p = .02). Tukey's posthoc tests showed lower values during stimulation ON compared to the OFF phase (Chart C Words: p = .001) or compared to the preoperative measurement (Chart B Words: p < .01, Chart C Words: p < .001, Interference C-B: p = .01).Scores from the Trail Making Test were analyzed using a Friedman ANOVA, indicating main effects in the Trail Making Test A (Χ²(2) = 9.10, p = .01) and B (Χ²(2) = 22.58, p < .0001). Wilcoxon posthoc tests showed lower values during stimulation ON compared to the OFF phase (both Tests A and B: p < .01) or compared to the preoperative measurement (Test B: p < .01).
Conclusion
Taken together, we have preliminary evidence that stimulation increases scores on the Complex Figure Test of Rey and subtests of the Auditory Verbal Learning Test. The first indicates favorable effects of stimulation on visuospatial constructional ability and visual memory, the latter supports improved verbal learning and memory . In addition, stimulation appears to lower scores on the Stroop tests (suggesting less interference and improved executive functioning) and on the Trail Making Test (indicating better performance on this assessment of visual search, scanning, speed of processing, mental flexibility, and executive functions).Note that, after correction for multiple testing, the effects of only 3 subtests remain significant: the Auditory Verbal Learning Test (Interference List B), Stroop test (Chart C Words) and Trail Making Test B.We can conclude that the neuropsychological tests provide no evidence for stimulation-induced cognitive or memory impairment, but rather the opposite.
Supplementary Appendix Luyten, Gabriëls & Nuttin 12/20

Neuropsychological (sub)test Mean Preop (range) Mean ON (range) Mean OFF (range)
Complex Figure Test of ReyCopy 34 (28-36) 35* (32-36) 34 (26-36)
Immediate Recall 16 (4-36) 21# (4-35) 19 (4-35)
Late Recall 16 (4-34) 20# (5-36) 19# (3-35)
Auditory Verbal Learning Test
First Trial List A 6 (1-10) 8# (1-14) 7 (1-14)
Total of 5 Trials List A 49 (23-65) 53 (28-73) 50 (24-72)
Interference List B 5 (1-10) 7**,## (1-11) 5 (1-10)
List A Immediate Recall 10 (5-15) 11 (5-15) 10 (5-15)
List A Late Recall 11 (5-15) 11 (5-15) 11 (5-15)
List A Recognition 14 (8-15) 14 (9-15) 14 (9-15)
Stroop test
Chart B Words 67 (47-133) 58# (40-80) 63 (39-104)
Chart C Words 111 (70-175) 91**,## (60-136) 105 (58-193)
Interference C-B 44 (22-73) 34* (18-59) 42 (19-89)
Trail Making TestTrail Making Test A 42 (26-77) 34* (17-83) 40 (17-178)
Trail Making Test B 90 (53-234) 86**,## (41-210) 97 (42-240)
Wisconsin Card Sorting TestTotal Errors 40 (15-76) 34 (5-75) 35 (9-72)
Perseverative Errors 24 (8-55) 20 (0-46) 21 (0-59)
Conceptual Level Response 56 (27-78) 60 (24-86) 59 (40-75)
Number of Complete Categories 5 (1-6) 4 (0-6) 4 (0-6)
Trials to Complete First Category 13 (10-18) 18 (10-91) 26 (11-128)
Failures to Maintain Set 1 (0-3) 1 (0-3) 1 (0-4)
Word Fluency TestWord Fluency Test 35 (19-55) 37 (15-58) 36 (17-61)
Raven's Standard Progressive MatricesStandard Progressive Matrices 45 (22-57) 46 (22-58) 45 (23-57)
Table S4: Neuropsychological test scores.Mean (and range) neuropsychological (sub)scores, preoperatively and during ON and OFF phases of the crossover period (16 patients). Note that for the Trail Making Tests medians are shown instead of averages, as these scores were analyzed with nonparametric tests. *Significantly different from OFF measurement (**significance retained after correction for multiple testing). #Significantly different from preoperative measurement (##significance retained after correction for multiple testing). Preop: preoperative.
Supplementary Appendix Luyten, Gabriëls & Nuttin 13/20

Qualitative analysis – crossover trial
Introduction & Method
In addition to the main quantitative analyses, we also examined qualitative data. Although standardized psychiatric tests (Y-BOCS, HAM-A, HAM-D, GAF) were the primary outcomes of this study, it is worthwhile to take a closer look at other reported consequences of stimulation. More specifically, we wanted to ensure that we did not miss any significant favorable or adverse effects which were not measured by standardized tests during the crossover trial. This information may be especially valuable for the selection of questionnaires and tests in future studies .
A medical student, who was unaware of the exact electrode locations and quantitative data, went through all available psychiatric and neurosurgical reports for each patient (n = 17) during the ON and OFF phases of stimulation. All reported observations were listed and afterwards grouped into clusters, in consultation with LG, BN and LL (Table S5). If a patient reported several symptoms (e.g. crying and loss of interest) that were designated to one cluster (e.g. negative mood or mood deterioration), this was counted as 1 observation for this cluster. Thus, the maximum number of observations per cluster was 17, i.e. the seventeen patients that completed the crossover study.Table S5 shows all observations with their corresponding clusters. Clusters were classified as being adverse/undesirable, favorable/desirable or neutral/unclassifiable.
This qualitative analysis has several limitations. First, for the seven initial patients, there were only neurosurgical reports available (and the neurosurgeon was aware of the experimental condition), while for the later patients, there were narrative psychiatric reports as well (the psychiatrist did not know if the patient was in the ON or OFF phase). Thus, for the earlier patients, the qualitative analysis was based on unblinded observations, while for the later patients, we had a combination of blinded and unblinded observations. Second, because of the novelty of this treatment, the initial patients in this study were seen more often than later patients, resulting in several reports per phase per patient. Note however that we grouped the symptoms into clusters and counted maximum one observation per patient. Third, as this qualitative analysis is based on unstructured interviews, there is a double reporting bias: the patients probably did not describe all experienced effects, and the psychiatrist or neurosurgeon might not have written down everything. On the other hand, this analysis has its strengths as well, since the observations were listed by an impartial medical student and were clustered by the authors while they were unaware of the crossover phase. Despite the shortcomings, we feel that these qualitative data are informative, as they reflect what is on patients’ minds and may reveal certain effects of DBS that were not picked up by the standardized quantitative analyses .
Results
Fig. S1 summarizes the qualitative data of the crossover study. Only observations that were counted at least 3 times were included in this figure. The upper panel of Fig. S1 depicts clusters that showed both positive status or improvement, and deterioration or persistence of negative symptoms during the ON and OFF phases. The lower panel strictly shows adverse or undesirable observations.
Given the small numbers for some clusters and the fact that we do not have observations for each patient during each phase, it is not possible to statistically analyze these qualitative data. Visual inspection of the data (Fig. S1) supports positive effects of stimulation on obsessions, compulsions, mood and energy level. During the OFF phase, there are more anxiety complaints. Stimulation seems to have a slightly negative
Supplementary Appendix Luyten, Gabriëls & Nuttin 14/20

effect on sleep quality and coordination. In addition, some stimulated patients reported feeling warmer or colder than usual, or experiencing some physical inconveniences (e.g. sensation of the implanted stimulator or cables and transient paresthesias). For more details, see Fig. S1 and Table S5.
Fig. S1: Summary of the qualitative analysis. Dark gray bars indicate adverse or undesirable observations (negative or deteriorated symptoms), white bars indicate favorable or desirable observa-tions (positive or improved symptoms). Open bars are observations during the stimulation ON phase, and hatched bars during the OFF phase. For each observation, the number of patients (out of 17 in total) that reported it, is shown.
Apart from the observations shown in Fig. S1, there were additional clusters with fewer than 3 patients. For the sake of completeness, we will enumerate them here. Two patients experienced favorable weight loss; one patient mentioned this during the ON phase, the other patient during both phases. One patient reported undesirable weight loss with decreased appetite during the ON phase. Three patients reported unwanted weight gain during the ON (2 patients) or OFF phase (1 patient). Other symptoms that were reported by only one patient each, were urinary incontinence, agitated speech and hallucinations (all during the ON phase). In addition, there were a few neutral or unclassifiable observations: libido changes (3 observations during ON phase, 1 during OFF phase), sleep changes (1 observation during each phase) and transient feeling as if the light was turned on (2 patients during ON phase).
Conclusion
These qualitative data provide additional support for beneficial effects of stimulation on obsessions, compulsions, mood, anxiety and energy level.
Moreover, they point out several potential consequences of stimulation that might be examined in more detail in future studies and followed up on in clinical practice. These include sleep quality, weight changes, libido changes and urinary incontinence. In addition, it remains important to keep an eye on physical inconveniences that may be inherent to DBS .
Supplementary Appendix Luyten, Gabriëls & Nuttin 15/20
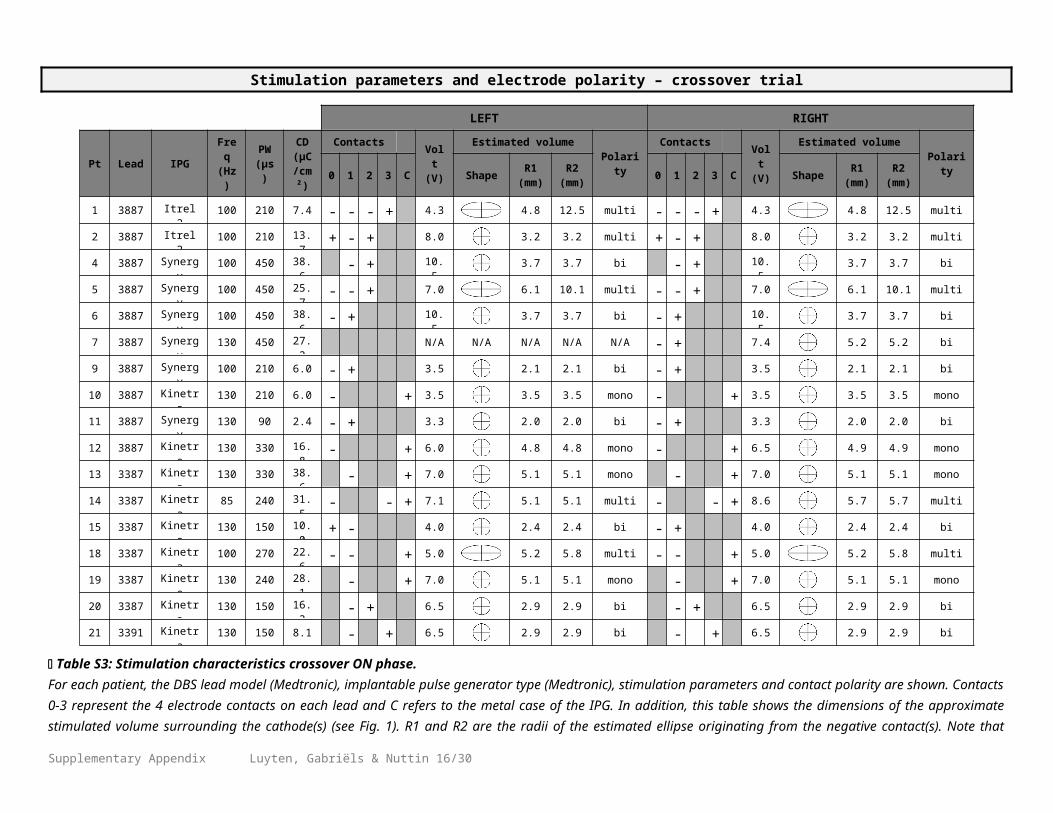
Table S5: Exhaustive list of the reported observations during the ON and OFF phases, used for the qualitative analysis.If possible, observations were clustered (e.g. mood or anxiety symptoms). These clusters are used in Fig. S1. Each cluster of observations was classified as being adverse/undesirable, favorable/desirable or neutral/unclassifiable.
ADVERSE OR UNDESIRABLE OBSERVATIONS FAVORABLE OR DESIRABLE OBSERVATIONS
Deterioration or persistence of obsessions/compulsions
Improvement of obsessions/compulsions
Obsessions; compulsions; safety-seeking; magical thinking
Less obsessions; less compulsions
Negative mood or mood deterioration Positive mood or mood improvement
Doing worse; depressive; sad; crying; loss of interest; unhappy; less happy; uncertain; guilt; apathetic; bad temper; hopeless; less confident; disappointed; doubting; downhearted; taciturn
Doing better; more peaceful; putting things into perspective; laughing; chatty; less crying; happy; hope; prospects; braver; more confident
Deterioration or persistence of anxiety symptoms
Improvement of anxiety symptoms
Anxious; avoidance behavior; restlessness; procrastination; nervous; panic; hyperventilation; fear of failure
Less anxious
Deterioration or persistence of suicidal thoughts Improvement of suicidal thoughts
More suicidal thoughts Less suicidal thoughts
Low or deteriorated sleep quality Good or improved sleep quality
Nightmares; disturbed sleep; 12-14 hours of sleep (combined with low energy levels); difficulties getting up before 11 AM; difficulties sleeping late; yawning; spending a lot of time in bed; difficulties falling asleep; snoring; increased sleep need (combined with low energy levels)
Possibility to sleep late or take a nap
Low or deteriorated energy level Good or improved energy level
Often tired; loss of energy; less activity More energy; more activity
Deterioration or persistence of poor coordination Improvement of coordination
Falling; clumsy; write illegibly Clearer handwriting
Gastrointestinal complaints Improvement of gastrointestinal complaints
Nausea; diarrhea; constipation Normalization of diarrhea
Deterioration or persistence of poor social functioning
Favorable weight loss
Social phobia; anxious to come outdoors; difficulties making contact with other people
Weight loss due to normalized chocolate consumption; weight loss in overweight patient
Supplementary Appendix Luyten, Gabriëls & Nuttin 16/20

NEUTRAL OR UNCLASSIFIABLE OBSERVATIONS
Untoward personality traits Libido changes
Aggressive behavior; jealous; impulsive; theatrical; possessive
Increased libido/masturbation frequency; decreased libido
Changed appetite Sleep changes
Decreased or no appetite; increased appetite, feeling hungry; increased appetite (chocolate overconsumption)
12-14 hours of sleep (no specific statement of low energy levels)
Deterioration or persistence of poor concentration and memory
Other physical effects
Memory deficits; difficulties concentrating; chaotic; reading and writing errors; less alert; confusion
Transient feeling as if the light was turned on
Feeling warmer or colder than usual
Feeling warmer than usual; feeling colder than usual
Physical inconveniences related to implant
Sensation of the cables; sensation of the stimulator in abdomen; shifting of the stimulator
Other physical inconveniences
Agitation/tremor; transpiration; paresthesias in head or abdomen; feeling of switching on/off the stimulator; dysesthesia; tinnitus; rash; pain; feeling of pressure in head
Adverse weight gain
Weight gain up to new maximum; due to chocolate overconsumption; to control appetite
Adverse weight loss
Weight loss combined with decreased appetite
Urinary incontinence
Urinary incontinence
Agitated speech
Increased speed of speech, rambling
Hallucinations
Hallucinations
Supplementary Appendix Luyten, Gabriëls & Nuttin 17/20
(Table S5 continued)

Active contacts during crossover, optimal open-label period and at last follow-up
Optimal open-label period
The optimal period was defined as the open-label period of at least two months, during which the patient reached his or her lowest Y-BOCS score after implantation. Although the optimal period may be influ-enced by additional external factors, besides electrical stimulation (e.g. improved family situation, altered medication, the fact that it was open-label instead of blinded), we deemed it interesting to take a look at the active electrode contacts during this period and the corresponding neuroanatomical target.
Note that Patient 1 never experienced an "optimal period". His lowest Y-BOCS score was 30, still indicat -ing very severe OCD. Note that his electrodes were located 10-15 mm more anterior than the active contacts of all other patients.
Comparison of stimulation targets during crossover and optimal open-label period
Nine out of 17 patients had identical negative contacts during the crossover and their optimal period. Seven patients were stimulated in a slightly different brain area while experiencing optimal effects. Three of them were stimulated in ALIC during the crossover, but were stimulated more ventrally on the border of ALIC and BST during their optimal period. Two patients were stimulated in BST during the crossover, and were stimulated more dorsally in BST during their optimal period. One patient was stimulated in ALIC during the crossover, and was stimulated with an additional contact extending more dorsally into ALIC during the optimal period. Finally, one patient was stimulated in BST during the crossover, and more dorsally in ALIC during his optimal period. Note that this last patient never experienced very good effects, both during the crossover (Y-BOCS = 22) and during his "optimal" open-label period (Y-BOCS = 25).
Comparison of stimulation targets during optimal open-label period and at last follow-up
If we compare the active contacts of the optimal period with those at last follow-up (excluding the first patient, cf supra), we find that 20 out of 23 patients have unchanged negative contacts. One patient has two additional active cathodes at last follow-up, with the stimulated area extending from the border of BST and ALIC, more dorsally into ALIC. One patient has returned to her crossover settings, with stimulation in ALIC, but extending less dorsally than during the optimal period. One patient has an extra negative contact on the left side at last follow-up, and is being stimulated bilaterally in BST, with the stimulated area extending more ventrally into BST on the left side.
Conclusion
Some patients were stimulated in slightly different targets during their optimal period as compared with the crossover trial. In three of these patients, the active contacts shifted from ALIC towards the border with BST and for one patient, with suboptimal effects, from a position adjacent to BST towards a more dorsal location in ALIC. For all other patients, the stimulated area remained largely the same.Furthermore, when comparing the optimal period with last follow-up, we find that the stimulated area remains largely unchanged.
Supplementary Appendix Luyten, Gabriëls & Nuttin 18/20

Patient data included in previously published papers
Data included in publication Patients RefFirst report on 4 patients indicating beneficial effects in a few prelimi-nary tests.
1-4
15-39 months follow-up (Y-BOCS) of 3 patients, open-label. 1-3Subjective reports and adverse events of 6 patients. 1-6Descriptive statistics (Y-BOCS) during ON and OFF of 6 patients, and 1-31 months follow-up (Y-BOCS) in all 8 patients, open-label.
1-8
Metabolic imaging in 6 patients, preoperative status versus stimulation on.
1-3, 5-7
3-36 months follow-up (Y-BOCS, HAM-A, HAM-D, GAF) of 11 patients, open-label. Pooled with patient data from other centers.Descriptive evaluation of the relation between electrode lead position and outcome.
1-11
Discrepancy between planned and postoperative position of electrode leads in 8 patients.
14-15, 18, 20-24
Local field potential recordings in 5 patients. 13, 16-17, 23-24Metabolic imaging in 16 patients, preoperative status versus stimula-tion on, and ON versus OFF in a subset of 9 patients.
1-3, 5-7, 10-15, 18-19, 20, 22
Supplementary Appendix Luyten, Gabriëls & Nuttin 19/20

Supplementary References
Supplementary Appendix Luyten, Gabriëls & Nuttin 20/20