· web viewthe implantable defibrillator (icd) is an effective strategy for the primary...
TRANSCRIPT
Towards Cardiac MRI based Risk Stratification in Idiopathic Dilated Cardiomyopathy.
Dr Pamela Browna, Dr Chris Millera, Dr Andrea DiMarcob, Dr Matthias Schmitta
Corresponding author: Pamela Brown, [email protected]
a. Cardiac MRI department, North West Heart Centre, Manchester University Foundation Trust-
Wythenshawe Site, Southmoor Road, Manchester, M23 9LT.
b. Arrhythmia Unit, Heart Disease Institute, Bellvitge University Hospital, Barcelona, Spain
Word Count: 2669
No conflicts of interest
The authors received no specific funding for this work.
1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19

Abstract
Sudden cardiac death (SCD) secondary to arrhythmia remains a risk in those with dilated
cardiomyopathy (DCM), an implantable cardiac defibrillator (ICD) is an effective strategy to prevent SCD.
Current guidelines recommend selection for ICD based on ejection fraction (EF) less than 35%, however,
most SCD occurs in those with EF >35%. Although meta-analysis has demonstrated a survival benefit for
primary prevention ICD in DCM, no randomised trial has shown a significant reduction in overall
mortality including the most recent ‘Danish Study to Assess the Efficacy of ICDs in Patients With Non-
Ischemic Systolic Heat Failure on Mortality’ (DANISH study). Clearly, a more sophisticated selection
strategy is required. CMR is an ideal non-invasive imaging technique which allows calculation of ejection
fraction as well as tissue characterisation with gadolinium contrast, parametric mapping and feature
tracking. Late gadolinium enhancement (LGE) detects mid-wall fibrosis in approximately 30% of those
with DCM, three meta-analyses have demonstrated an association between fibrosis in DCM and SCD,
and those without fibrosis are at low risk of SCD. T1 mapping and extra-cellular volume calculation (ECV)
are methods of demonstrating diffuse fibrosis in the myocardium. Raised ECV and native T1 have been
associated with worse outcomes but the relationship to SCD has not been well studied. Undoubtably,
more research is required but CMR has several tools which offer incremental value above EF to improve
risk stratification and consequent outcomes and resource utilisation in those with DCM.
2
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23

Introduction
Dilated cardiomyopathy (DCM) is defined as ‘left ventricular or biventricular systolic dysfunction and
dilatation that is not explained by abnormal loading conditions or coronary artery disease.’ (1) It is
recognised to be a spectrum of clinical states rather than a single entity; the prevalence of DCM is 1 in
2500 with an incidence of 7 in 100,000. (2) (Image 1)
Image 1. The DCM disease spectrum (Image adapted from Pinto et al 2016 (1))
Sudden cardiac death (SCD) is an unexpected death occurring within one hour of symptom onset or
within 24 hours from when the individual was last seen alive. (3) SCD accounts for 15-20% of all deaths
worldwide with 1.4 deaths per 100,000 person years in women (95% CI 0.95-1.98) and 6.7 deaths per
person years in men (95% CI 6.25-7.14). (4) Approximately 30% of those with DCM will suffer SCD. (5)
The implantable defibrillator (ICD) is an effective strategy for the primary prevention of arrhythmic SCD.
Currently, an ICD is recommended in symptomatic heart failure (NYHA II-III) and a left ventricular
ejection fraction (LVEF) of less than 35%, regardless of aetiology. (6) However, the majority of SCD
occurs in those without severe left ventricular systolic dysfunction (LVSD) (7,8) who have no primary
prevention ICD indication and a significant proportion of patients implanted with an ICD will never
receive appropriate therapy. (9)
3
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17

The broad issue of non-invasive imaging markers associated with SCD across the spectrum of cardiac
disease has recently been reviewed. (10,11) This review will focus on the role of cardiac magnetic
resonance (CMR) and it’s potential for improving risk stratification in DCM.
Left Ventricular Ejection Fraction-the established risk stratification method.
Mortality increases as EF deceases (12) and those with an EF <30% have the most adverse prognosis.
(13, 14) Conversely, the absolute numbers of people who die from SCD is substantially higher in those
with EF >35%. (8) LVEF is clearly a marker of disease severity but is neither specific nor sensitive as a
marker for SCD. When selecting according to LVEF, no randomised trial has shown a significant reduction
in overall mortality with primary prevention ICD in DCM (9, 15-18), even though ICD implantation was
effective in preventing SCD. (9, 18)
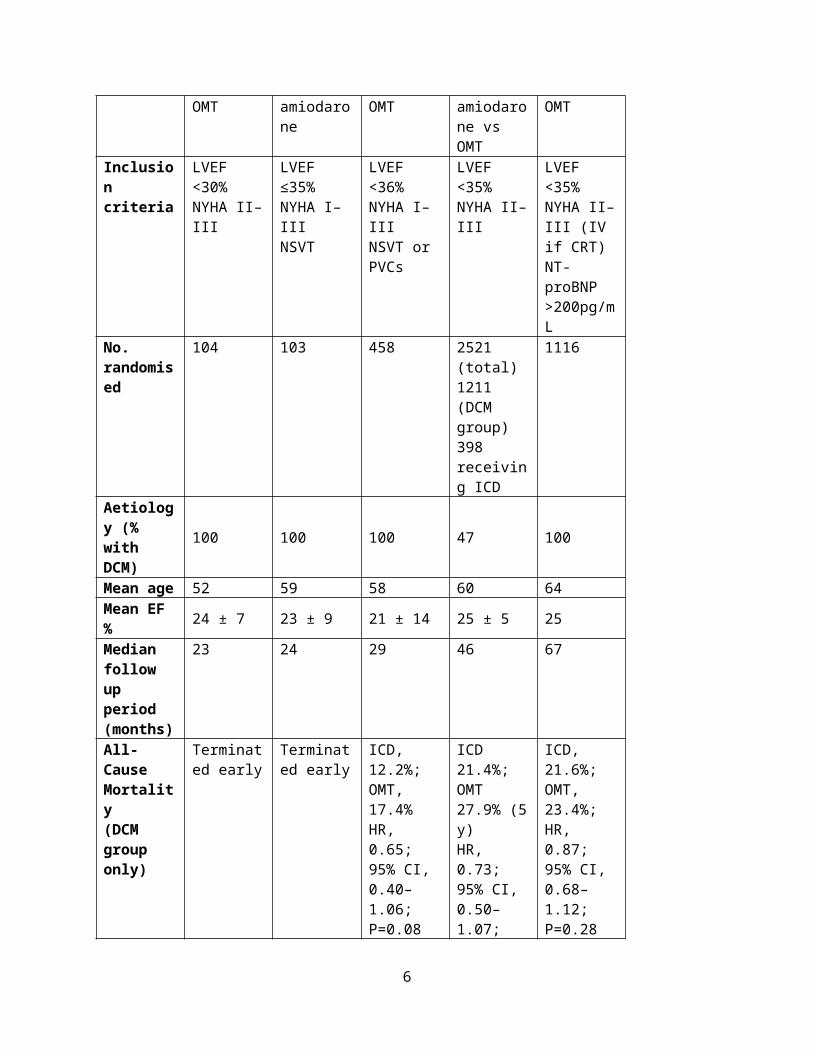
A summary of the trials to date is seen in Table 1.
Table 1.
CAT AMIOVIRT DEFINITE SCD-HeFT DANISHYear 2002 2003 2004 2005 2016Design ICD vs OMT ICD vs.
amiodaroneICD vs OMT ICD vs
amiodarone vs OMT
ICD vs OMT
Inclusion criteria
LVEF <30%NYHA II–III
LVEF ≤35%NYHA I–IIINSVT
LVEF <36%NYHA I–IIINSVT or PVCs
LVEF <35%NYHA II–III
LVEF <35%NYHA II–III (IV if CRT)NT-proBNP >200pg/mL
No. randomised
104 103 458 2521 (total) 1211 (DCM group) 398 receiving ICD
1116
Aetiology (% with DCM)
100 100 100 47 100
Mean age 52 59 58 60 64Mean EF % 24 ± 7 23 ± 9 21 ± 14 25 ± 5 25Median follow up
23 24 29 46 67
4
1
2
3
4
5
6
7
8
9
10
11
12

period (months)All-Cause Mortality(DCM group only)
Terminated early
Terminated early
ICD, 12.2%; OMT, 17.4%HR, 0.65; 95% CI, 0.40–1.06;P=0.08
ICD 21.4%; OMT 27.9% (5 y)HR, 0.73; 95% CI, 0.50–1.07;P=0.06
ICD, 21.6%; OMT, 23.4%;HR, 0.87; 95% CI, 0.68–1.12;P=0.28
Sudden Cardiac Death
NA NA ICD 1.3%; OMT 6.1%HR, 0.20; 95% CI, 0.06–0.71;P=0.006
NA ICD 4.3%; OMT 8.2%HR, 0.50; 95% CI, 0.31–0.82;P=0.005
OMT=optimal medical therapy
Current guidelines based on meta-analysis of these trials managed to demonstrate a significant survival
benefit for primary prevention ICD in patients with DCM and severe LV impairment. (19) A recent meta-
analysis, (20) including the DANISH trial data, confirmed previous results. The fact that survival benefits
can be observed only by pooling data of several studies indicates that we need to improve patient
selection by increasing our ability to discriminate between risk of SCD and risk of death from heart
failure or non-cardiovascular causes. Sub-group analysis in the DANISH trial showed that ICDs provided a
significant survival benefit only to patients younger than 70 years old, not because they had a higher risk
of SCD without the ICD but because they had a lower risk of non-sudden death therefore their sudden vs
non-sudden death ratio was higher. Clearly, a more sophisticated approach is required.
The emerging risk stratification method-late gadolinium enhancement.
CMR with administration of gadolinium based contrast agent allows non-invasive evaluation of localised
cardiac replacement fibrosis, seen when a collagen matrix is laid down in response to myocyte damage,
necrosis and/or apoptosis, leading to a distinct myocardial scar. Gadolinium shortens the T1 relaxation
of the scarred tissue which consequently appears bright when the inversion recovery sequence is set to
null normal myocardium (21). The presence of myocardial replacement fibrosis seen on late gadolinium
5
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
enhanced CMR has been shown to correlate with histological areas of plexiform fibrosis. (22-25) A
midwall pattern of fibrosis (MWF) is the most typical pattern seen in patients with DCM, with 30-40%
having LGE, other patterns are seen, and several studies have classified hyperenhancement as simply
ischaemic or non-ischaemic. (Wu 2008, 26,27) Beyond diagnosis, studies have demonstrated that
fibrosis in DCM can be used to predict prognosis. Importantly, replacement fibrosis seems to be related
to ventricular arrhythmias and SCD.
Image 1 demonstrates MWF on LGE imaging, T1 and post-contrast T1 maps.
Image 1
Assomull et al (28) conducted the first study demonstrating the association of fibrosis with an adverse
prognosis in DCM. 35% of 101 patients studied had MWF and LGE presence was found to be associated
with all-cause mortality and hospital admission for cardiovascular causes (HR 3.4 95% CI 1.4-8.7 p=0.01).
Those with LGE were more likely to have SCD/VT although overall event rates were low (7 in total).
Subsequently, Iles (29), evaluated whether LGE presence predicted appropriate ICD shock in 103
patients who fitted primary prevention ICD criteria, 51% of those with DCM had LGE present. No ICD
discharges were seen in those without LGE compared to 9 of 31 (29%) discharges in those with LGE
(p<0.01). The largest study to date consisted of 472 patients, (25), 30% had MWF. There was a
significant association between MWF and all-cause mortality (p<0.001) even after adjustment for EF;
29.6% of those with fibrosis reached the arrhythmic end points of SCD or aborted SCD vs 7% those
6
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19

without fibrosis (p<0.001). Recently, the question of whether LGE signifies risk in those with DCM and EF
>40% was studied. (30) 399 patients were enrolled 25% had MWF, mean EF was 49% and median follow
up was 4.6 years. The composite primary end point of SCD or aborted SCD occurred in 18 (17.8%)
patients with LGE and 7 (2.3%) patients without LGE (p=<0.0001). This significance continued even after
adjustment for potential confounders such as age, NYHA class and LVEF (HR 9.3). MWF had just a
borderline association with the secondary end point of all-cause mortality (p=0.056), suggesting that LGE
might be a specific marker of ventricular arrhythmia and therefore, could identify patients with a higher
risk of SCD rather than death from other causes. Several other smaller, often single centre studies with
diverse end points have been studied and synthesised into three meta-analyses delivering a consistent
message (27, 31, 32). (Table 2)
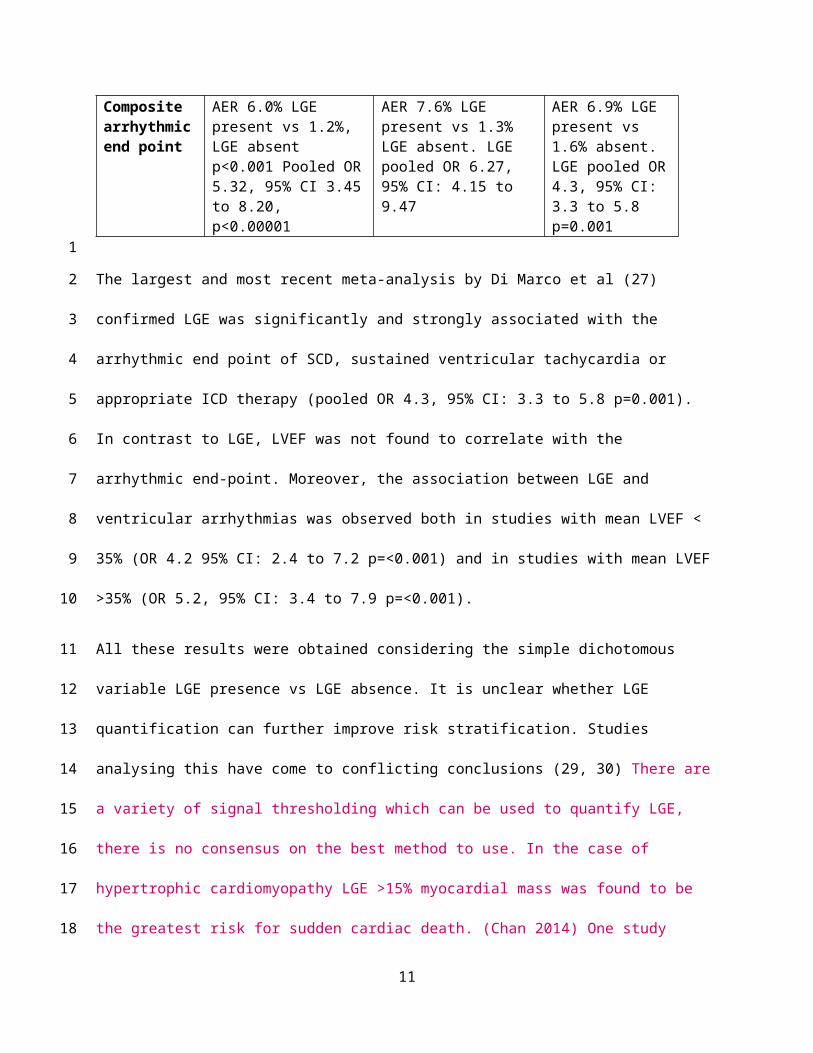
Table 2.
Author Kuruvilla et al Disertori et al DiMarco et alYear 2014 2016 2017Number of studies (DCM only)
9 8 29
Number of patients (DCM only)
1,488 1,443 2948
Mean Age (Years)
52 53 56
Mean EF % 37 33 20-43Mean Follow up (Months)
30 31 36
% with LGE present
38 40 44
Composite arrhythmic end point
AER 6.0% LGE present vs 1.2%, LGE absent p<0.001 Pooled OR 5.32, 95% CI 3.45 to 8.20, p<0.00001
AER 7.6% LGE present vs 1.3% LGE absent. LGE pooled OR 6.27, 95% CI: 4.15 to 9.47
AER 6.9% LGE present vs 1.6% absent. LGE pooled OR 4.3, 95% CI: 3.3 to 5.8 p=0.001
The largest and most recent meta-analysis by Di Marco et al (27) confirmed LGE was significantly and
strongly associated with the arrhythmic end point of SCD, sustained ventricular tachycardia or
7
1
2
3
4
5
6
7
8
9
10
11
12
13
14

appropriate ICD therapy (pooled OR 4.3, 95% CI: 3.3 to 5.8 p=0.001). In contrast to LGE, LVEF was not
found to correlate with the arrhythmic end-point. Moreover, the association between LGE and
ventricular arrhythmias was observed both in studies with mean LVEF < 35% (OR 4.2 95% CI: 2.4 to 7.2
p=<0.001) and in studies with mean LVEF >35% (OR 5.2, 95% CI: 3.4 to 7.9 p=<0.001).
All these results were obtained considering the simple dichotomous variable LGE presence vs LGE
absence. It is unclear whether LGE quantification can further improve risk stratification. Studies
analysing this have come to conflicting conclusions (29, 30) There are a variety of signal thresholding
which can be used to quantify LGE, there is no consensus on the best method to use. In the case of
hypertrophic cardiomyopathy LGE >15% myocardial mass was found to be the greatest risk for sudden
cardiac death. (Chan 2014) One study using the 2 standard deviation and full width half max (FWHM)
methods found that in those with DCM the greatest risk was in those with >6.1% of myocardium
affected by LGE. (Neilan 2013) A further study by the same group (Neilan 2015) of cardiac arrest
survivors (of both ischaemic and non-ischaemic aetiology) found that presence of LGE had the strongest
association with both death and appropriate ICD therapy but that percentage of LGE to myocardium
>8.1% was the most specific and sensitive amount. However, another study in those with DCM (Halliday
2017) concluded that there is no linear increase in SCD risk as extent of LGE increases; the greatest
increase in risk of SCD occurs between no LGE and those with 2.5% LGE. LGE presence vs absence is a
simple, reproducible parameter and the important message is that DCM patients without LGE have low
risk of ventricular arrhythmia or SCD.
T1 mapping and ECV quantification.
LGE relies on local differences in tissue composition and cannot distinguish those who have diffuse
interstitial fibrosis. Endomyocardial biopsy is currently the gold standard for detection of diffuse fibrosis
but carries inherent risk and has limited diagnostic yield. CMR with T1 mapping and ECV calculation
8
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23

allows one to demonstrate diffuse fibrosis in a non-invasive manner. T1 mapping therefore has
diagnostic ability beyond presence of LGE in those with diffuse fibrosis, this is used clinically in the case
of Anderson-Fabry Disease when T1 decreases due to fatty deposition. It also holds promise in
distinguishing between athletic hearts when ECV decreases and hypertrophic cardiomyopathy when ECV
increases. (Swoboda 2016) In a T1 map the T1 value is encoded in each pixel and corresponds to the T1
relaxation time of the corresponding myocardial voxel. T1 maps can be created both pre (native T1) and
post gadolinium contrast. (33)
In general, native T1 values increase in DCM and post-contrast T1 values get shorter. (21, 33) By
comparing signal intensity changes (as a function of contrast concentration changes) in the extracellular
compartment with those in the blood pool and integrating the available blood volume distribution (1-
haematocrit (HCT)) one can calculate the partition coefficient lambda which in turn allows estimation of
the myocardial extracellular volume space using the formula ECV= (1-HCT x lambda).
Post-contrast T1 mapping has been shown to correlate with histological presence of fibrosis on
endomyocardial biopsy and on histological whole heart examinations in patients with heart failure. (23,
24) Aus dem Siepen et al (34) demonstrated that calculated ECV was comparable with histological
collagen volume fraction (CVF) in DCM and that increased ECV and native T1 was seen in those with
DCM compared to controls. Puntmann et al (35) found that in those with cardiomyopathy native T1 was
longer (p<0.01), post contrast T1 was shorter (p<0.01), and ECV was significantly higher (p<0.01). When
the data underwent ROC analysis native T1 was found to be the best independent discriminator
between healthy and diseased myocardium with a specificity of 97% and sensitivity of 100%. Routine
clinical use has been limited, not least by the recommendation that each centre establishes their own
reference ranges given the potential variation in vendor, field strength and acquisition parameters.
Normal values have however been published for T1 and ECV at both 1.5T and 3T field strength. (Sado
9
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23

2012, Dabir 2014, Ray 2017) There are ongoing large scale standardisation and validation studies
including phantom exchange projects.
Do T1 mapping techniques and ECV parallel findings seen in LGE literature?
Wong et al (36) examined those with both ischaemic and non-ischaemic cardiomyopathy and found that
ECV >28.5% was significantly associated with all-cause mortality (HR 1.55 95% CI 1.27-1.88 for every 3%
increase in ECV). This was supported in a later study by the same group (37) which calculated ECV across
a range of ejection fractions. Raised ECV was associated with hospitalisation for heart failure, death or
both. Barison et al (38) studied 89 patients with non-ischaemic cardiomyopathy and found that an ECV
>32% was a prognostic predictor of mortality beyond echo parameters and that ECV was raised
compared to controls even in those without LGE.
In those with dilated cardiomyopathy (39) native T1 was significantly associated with both all-cause
mortality and the secondary end points independently of both LVEF<35% and LGE presence. Indeed,
higher T1 values outperformed presence of LGE in predicting adverse outcomes.
The association between diffuse fibrosis detected by CMR and SCD in DCM has not been widely analysed
yet. One study (40) has scrutinised the link between T1 mapping and ventricular arrhythmia in patients
with ICD implanted for primary or secondary prevention. Sub-group analysis showed that, in the 59 non-
ischaemic patients (53 DCM, 5 HCM and 1 sarcoidosis), native septal T1 was the only independent
predictor of appropriate ICD therapies (HR 1.12 every 10ms increase, p<0.01) and of the composite end-
point of appropriate ICD therapies or death from any cause (HR 1,1 every 10ms increase, p<0.01). In
contrast, ECV was not associated with the end-points analysed.
Detection of fibrosis by CMR is a useful non-invasive diagnostic and prognostic tool in dilated
cardiomyopathy. Native T1 mapping in particular has the potential to negate the need for gadolinium
based contrast examinations in selected patients. It seems unlikely that T1 mapping or ECV will be used
10
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
as a single diagnostic or prognostic parameter and should be used in conjunction with LGE as a
multiparametric approach. One particular T1 or ECV value can indicate a variety of cardiomyopathies
and pseudonormalisation can occur for example in Anderson-Fabry disease when fibrosis replaces fat in
the myocardium.
Strain imaging.
Whilst ejection fraction describes global myocardial function, it is an imprecise measure of regional
myocardial dysfunction, strain imaging on the contrary characterises regional deformation of an area of
myocardium. Strain imaging is less subjective than an eyeball estimate of LVEF and can be used to detect
early regional myocardial dysfunction before ejection fraction decreases. Substantial echocardiography
based data has accumulated highlighting the value of strain based data (specifically global longitudinal
(peak) strain (GLS)) in predicting outcome. One multimodality study (Chimura 2016) found that GLS >-
8.3% calculated by 2D echocardiography combined with positive LGE on CMR heralded the most adverse
prognosis above LVEF.
Regional assessment of myocardial deformation has been available via CMR since the 1980s.
Traditionally, this required dedicated (time consuming) sequences combined with dedicated post-
processing technologies. Various conceptual approaches based on myocardial tagging or displacement
encoding with stimulated echos were developed but did not penetrate into daily clinical routine. This
changed with the arrival of feature tracking technology which is analogous to echocardiographic speckle
tracking but rather than tracking an intramyocardial point it tracks endocardial borders over time and
can be easily applied as part of a standard CMR protocol (43) has been found to be reliable, reproducible
and has been validated against existing techniques such as HARP and SPAMM. (44-46) Buss (47)
conducted a study of 210 patients with dilated cardiomyopathy who had CMR feature tracking based
strain calculated. They found that a GLS >-12.5% was predictive of a combined primary end point of,
11
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23

cardiac death, heart transplantation, and appropriate ICD shock due to ventricular tachycardia or
fibrillation. This was significant regardless of LVEF. In univariate analysis GLS was predictive of the
primary end point (HR 1.33 95% CI 1.21-1.47 p=< 0.0001). After multivariate analysis GLS was predictive
of the primary end point above LVEF and BNP (HR 1.27 95% CI 1.05-1.52 p<0.02). The study also
suggested that those with preserved GLS had a good outlook irrespective of EF and LGE presence. A
further study (48) studied a mixed-aetiology cohort of 1012 patients and EF <50%. It was found that
after adjustment for EF and LGE every 1% decrease in GLS conferred an 89.1% increased risk of death
(HR 1.891 per % p<0.001). When limiting the analysis to those with non-ischaemic cardiomyopathy GLS
was an independent risk factor for death beyond LGE and EF (HR 2.01 per % p<0.001). Preserved GLS
also identified patients with lower risk amongst those with LGE.
GLS calculation by CMR feature tracking has yet to be widely used in clinical practice. Although normal
values have been studied (Taylor 2015) these have yet to be validated on a large scale and cut offs for
specific disease states are yet to be established. CMR feature tracking is limited by it’s lower temporal
resolution meaning that strain values may be underestimated. Certainly, more studies are needed using
CMR based methods of calculating strain to determine the exact prognostic role of GLS in arrhythmia
and SCD prediction in patients with DCM.
Conclusion
Current clinically applied risk stratification for ventricular arrhythmia and SCD death in dilated
cardiomyopathy, purely based on EF as the single imaging parameter, remains inadequate. Cardiac
magnetic resonance allows a complete structural and functional analysis of the heart: some CMR
parameters, such as LGE, have already shown a consistent and strong association with ventricular
arrhythmias and sudden death. Others need to be further investigated for this specific outcome. Future
12
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22

application of a multiparametric approach holds promise to improve and personalise the arrhythmic risk
of DCM patients.
References
1. Pinto, Y. M., et al. (2016). "Proposal for a revised definition of dilated cardiomyopathy,
hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position
statement of the ESC working group on myocardial and pericardial diseases." Eur Heart J 37(23):
1850-1858.
2. Taylor MR, Carniel E, Mestroni L. Cardiomyopathy, familial dilated. Orphanet J Rare Dis.
2006;1:27
3. Deo R, Albert CM. Epidemiology and genetics of sudden cardiac death. Circulation.
2012;125(4):620-37.
4. Eckart RE, Shry EA, Burke AP, McNear JA, Appel DA, Castillo-Rojas LM, et al. Sudden death in
young adults: an autopsy-based series of a population undergoing active surveillance. J Am Coll
Cardiol. 2011;58(12):1254-61
5. Tamburro, P. and D. Wilber (1992). "Sudden death in idiopathic dilated cardiomyopathy." Am
Heart J 124(4): 1035-1045
6. Priori SG, Blomstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC
Guidelines for the management of patients with ventricular arrhythmias and the prevention of
sudden cardiac death: The Task Force for the Management of Patients with Ventricular
Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology
(ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur
Heart J. 2015;36(41):2793-867
13
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
7. Stecker, E. C., et al. (2006). "Population-based analysis of sudden cardiac death with and without
left ventricular systolic dysfunction: two-year findings from the Oregon Sudden Unexpected
Death Study." J Am Coll Cardiol 47(6): 1161-1166
8. Narayanan, K., et al. (2013). "Frequency and determinants of implantable cardioverter
defibrillator deployment among primary prevention candidates with subsequent sudden cardiac
arrest in the community." Circulation 128(16): 1733-1738
9. Kadish, A., et al. (2004). "Prophylactic defibrillator implantation in patients with nonischemic
dilated cardiomyopathy." N Engl J Med 350(21): 2151-2158
10. van der Bijl P, Delgado V, Bax JJ. Noninvasive imaging markers associated with sudden cardiac
death. Trends Cardiovasc Med. 2016;26(4):348-60
11. Halliday BP, Cleland JGF, Goldberger JJ, Prasad SK. Personalizing Risk Stratification for Sudden
Death in Dilated Cardiomyopathy: The Past, Present, and Future. Circulation. 2017;136(2):215-
31.
12. Curtis, J. P., et al. (2003). "The association of left ventricular ejection fraction, mortality, and
cause of death in stable outpatients with heart failure." J Am Coll Cardiol 42(4): 736-742.
13. Komajda, M., et al. (1990). "Factors predicting mortality in idiopathic dilated cardiomyopathy."
Eur Heart J 11(9): 824-831
14. Juilliere, Y., et al. (1988). "Dilated cardiomyopathy: long-term follow-up and predictors of
survival." Int J Cardiol 21(3): 269-277
15. Bansch, D., et al. (2002). "Primary prevention of sudden cardiac death in idiopathic dilated
cardiomyopathy: the Cardiomyopathy Trial (CAT)." Circulation 105(12): 1453-1458.
16. Strickberger, S. A., et al. (2003). "Amiodarone versus implantable cardioverter-
defibrillator:randomized trial in patients with nonischemic dilated cardiomyopathy and
14
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
asymptomatic nonsustained ventricular tachycardia--AMIOVIRT." J Am Coll Cardiol 41(10): 1707-
1712.
17. Bardy, G. H., et al. (2005). "Amiodarone or an implantable cardioverter-defibrillator for
congestive heart failure." N Engl J Med 352(3): 225-237
18. Kober L, Thune JJ, Nielsen JC, Haarbo J, Videbaek L, Korup E, et al. Defibrillator Implantation in
Patients with Nonischemic Systolic Heart Failure. N Engl J Med. 2016;375(13):1221-30.
19. Desai, A. S., et al. (2004). "Implantable defibrillators for the prevention of mortality in patients
with nonischemic cardiomyopathy: a meta-analysis of randomized controlled trials." JAMA
292(23): 2874-2879.
20. Beggs, S. A. S., et al. (2018). "Non-ischaemic cardiomyopathy, sudden death and implantable
defibrillators: a review and meta-analysis." Heart 104(2): 144-150.
21. Mewton, N., et al. (2011). "Assessment of myocardial fibrosis with cardiovascular magnetic
resonance." J Am Coll Cardiol 57(8): 891-903.
22. Schalla, S., et al. (2010). "Replacement and reactive myocardial fibrosis in idiopathic dilated
cardiomyopathy: comparison of magnetic resonance imaging with right ventricular biopsy." Eur J
Heart Fail 12(3): 227-231.
23. Miller, C. A., et al. (2013). "Comprehensive validation of cardiovascular magnetic resonance
techniques for the assessment of myocardial extracellular volume." Circ Cardiovasc Imaging
6(3): 373-383.
24. Iles, L. M., et al. (2015). "Histological validation of cardiac magnetic resonance analysis of
regional and diffuse interstitial myocardial fibrosis." Eur Heart J Cardiovasc Imaging 16(1): 14-22.
25. Gulati, A., et al. (2013). "Association of fibrosis with mortality and sudden cardiac death in
patients with nonischemic dilated cardiomyopathy." JAMA 309(9): 896-908.
15
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23

26. McCrohon JA, Moon JC, Prasad SK, McKenna WJ, Lorenz CH, Coats AJ, et al. Differentiation of
heart failure related to dilated cardiomyopathy and coronary artery disease using gadolinium-
enhanced cardiovascular magnetic resonance. Circulation. 2003;108(1):54-9.
27. Di Marco, A., et al. (2017). "Late Gadolinium Enhancement and the Risk for Ventricular
Arrhythmias or Sudden Death in Dilated Cardiomyopathy: Systematic Review and Meta-
Analysis." JACC Heart Fail 5(1): 28-38.
28. Assomull, R. G., et al. (2006). "Cardiovascular magnetic resonance, fibrosis, and prognosis in
dilated cardiomyopathy." J Am Coll Cardiol 48(10): 1977-1985.
29. Iles, L., et al. (2011). "Myocardial fibrosis predicts appropriate device therapy in patients with
implantable cardioverter-defibrillators for primary prevention of sudden cardiac death." J Am
Coll Cardiol 57(7): 821-828.
30. Halliday, B. P., et al. (2017). "Association Between Midwall Late Gadolinium Enhancement and
Sudden Cardiac Death in Patients With Dilated Cardiomyopathy and Mild and Moderate Left
Ventricular Systolic Dysfunction." Circulation 135(22): 2106-2115
31. Kuruvilla, S., et al. (2014). "Late gadolinium enhancement on cardiac magnetic resonance
predicts adverse cardiovascular outcomes in nonischemic cardiomyopathy: a systematic review
and meta-analysis." Circ Cardiovasc Imaging 7(2): 250-258.
32. Disertori, M., et al. (2016). "Myocardial Fibrosis Assessment by LGE Is a Powerful Predictor of
Ventricular Tachyarrhythmias in Ischemic and Nonischemic LV Dysfunction: A Meta-Analysis."
JACC Cardiovasc Imaging 9(9): 1046-1055.
33. Haaf, P., et al. (2016). "Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: a
comprehensive review." J Cardiovasc Magn Reson 18(1): 89.
16
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22

34. Aus dem Siepen, F., et al. (2015). "T1 mapping in dilated cardiomyopathy with cardiac magnetic
resonance: quantification of diffuse myocardial fibrosis and comparison with endomyocardial
biopsy." Eur Heart J Cardiovasc Imaging 16(2): 210-216.
35. Puntmann, V. O., et al. (2013). "Native T1 mapping in differentiation of normal myocardium
from diffuse disease in hypertrophic and dilated cardiomyopathy." JACC Cardiovasc Imaging
6(4): 475-484.
36. Wong, T. C., et al. (2012). "Association between extracellular matrix expansion quantified by
cardiovascular magnetic resonance and short-term mortality." Circulation 126(10): 1206-1216.
37. Schelbert, E. B., et al. (2015). "Myocardial Fibrosis Quantified by Extracellular Volume Is
Associated With Subsequent Hospitalization for Heart Failure, Death, or Both Across the
Spectrum of Ejection Fraction and Heart Failure Stage." J Am Heart Assoc 4(12).
38. Barison A, Del Torto A, Chiappino S, Aquaro GD, Todiere G, Vergaro G, et al. Prognostic
significance of myocardial extracellular volume fraction in nonischaemic dilated
cardiomyopathy. J Cardiovasc Med (Hagerstown). 2015;16(10):681-7
39. Puntmann, V. O., et al. (2016). "T1-Mapping and Outcome in Nonischemic Cardiomyopathy: All-
Cause Mortality and Heart Failure." JACC Cardiovasc Imaging 9(1): 40-50.
40. Chen, Z., et al. (2015). "Myocardial tissue characterization by cardiac magnetic resonance
imaging using T1 mapping predicts ventricular arrhythmia in ischemic and non-ischemic
cardiomyopathy patients with implantable cardioverter-defibrillators." Heart Rhythm 12(4): 792-
801.
41. Kalam, K., et al. (2014). "Prognostic implications of global LV dysfunction: a systematic review
and meta-analysis of global longitudinal strain and ejection fraction." Heart 100(21): 1673-1680.
42. Biering-Sorensen, T., et al. (2017). "Regional Longitudinal Deformation Improves Prediction of
Ventricular Tachyarrhythmias in Patients With Heart Failure With Reduced Ejection Fraction: A
17
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24

MADIT-CRT Substudy (Multicenter Automatic Defibrillator Implantation Trial-Cardiac
Resynchronization Therapy)." Circ Cardiovasc Imaging 10(1).
43. Hor KN, Baumann R, Pedrizzetti G, Tonti G, Gottliebson WM, Taylor M, et al. Magnetic resonance
derived myocardial strain assessment using feature tracking. J Vis Exp. 2011(48)
44. Hor KN, Gottliebson WM, Carson C, Wash E, Cnota J, Fleck R, et al. Comparison of magnetic
resonance feature tracking for strain calculation with harmonic phase imaging analysis. JACC
Cardiovasc Imaging. 2010;3(2):144-51
45. Breuninger K, Lehrke S, Matheis P, Sander Y, Kammerer R, Rust L, et al. Feature tracking cardiac
magnetic resonance imaging for the evaluation of myocardial strain in patients with dilated
cardiomyopathy and in healthy controls. Journal of Cardiovascular Magnetic Resonance.
2013;15(1):P167
46. Moody WE, Taylor RJ, Edwards NC, Chue CD, Umar F, Taylor TJ, et al. Comparison of magnetic
resonance feature tracking for systolic and diastolic strain and strain rate calculation with spatial
modulation of magnetization imaging analysis. J Magn Reson Imaging. 2015;41(4):1000-12
47. Buss SJ, Breuninger K, Lehrke S, Voss A, Galuschky C, Lossnitzer D, et al. Assessment of
myocardial deformation with cardiac magnetic resonance strain imaging improves risk
stratification in patients with dilated cardiomyopathy. Eur Heart J Cardiovasc Imaging.
2015;16(3):307-15
48. Romano S, Judd RM, Kim RJ, Kim HW, Klem I, Heitner JF, et al. Feature-Tracking Global
Longitudinal Strain Predicts Death in a Multicenter Population of Patients with Ischemic and
Nonischemic Dilated Cardiomyopathy Incremental to Ejection Fraction and Late Gadolinium
Enhancement. JACC Cardiovasc Imaging. 2018
18
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23

Wu KC, Weiss RG, Thiemann DR, Kitagawa K, Schmidt A, Dalal D, et al. Late gadolinium enhancement by cardiovascular magnetic resonance heralds an adverse prognosis in nonischemic cardiomyopathy. J Am Coll Cardiol. 2008;51(25):2414-21.
Chan RH, Maron BJ, Olivotto I, Pencina MJ, Assenza GE, Haas T, et al. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy. Circulation. 2014;130(6):484-95.
Neilan TG, Coelho-Filho OR, Danik SB, Shah RV, Dodson JA, Verdini DJ, et al. CMR quantification of myocardial scar provides additive prognostic information in nonischemic cardiomyopathy. JACC Cardiovasc Imaging. 2013;6(9):944-54.
Neilan TG, Farhad H, Mayrhofer T, Shah RV, Dodson JA, Abbasi SA, et al. Late gadolinium enhancement among survivors of sudden cardiac arrest. JACC Cardiovasc Imaging. 2015;8(4):414-23.
Swoboda PP, McDiarmid AK, Erhayiem B, Broadbent DA, Dobson LE, Garg P, et al. Assessing Myocardial Extracellular Volume by T1 Mapping to Distinguish Hypertrophic Cardiomyopathy From Athlete's Heart. J Am Coll Cardiol. 2016;67(18):2189-90.
Sado DM, Flett AS, Banypersad SM, White SK, Maestrini V, Quarta G, et al. Cardiovascular magnetic resonance measurement of myocardial extracellular volume in health and disease. Heart. 2012;98(19):1436-41.
Dabir D, Child N, Kalra A, Rogers T, Gebker R, Jabbour A, et al. Reference values for healthy human myocardium using a T1 mapping methodology: results from the International T1 Multicenter cardiovascular magnetic resonance study. J Cardiovasc Magn Reson. 2014;16:69.
Roy C, Slimani A, de Meester C, Amzulescu M, Pasquet A, Vancraeynest D, et al. Age and sex corrected normal reference values of T1, T2 T2* and ECV in healthy subjects at 3T CMR. J Cardiovasc Magn Reson. 2017;19(1):72.
Chimura M, Onishi T, Tsukishiro Y, Sawada T, Kiuchi K, Shimane A, et al. Longitudinal strain combined with delayed-enhancement magnetic resonance improves risk stratification in patients with dilated cardiomyopathy. Heart. 2017;103(9):679-86.
Taylor RJ, Moody WE, Umar F, Edwards NC, Taylor TJ, Stegemann B, et al. Myocardial strain measurement with feature-tracking cardiovascular magnetic resonance: normal values. Eur Heart J Cardiovasc Imaging. 2015;16(8):871-81.
19
123
456
789
1011
121314
151617
181920
212223
242526
272829
30