0104.nccdn.net0104.nccdn.net/.../supplier-expectations-schedule-a-an… · web viewschedule...
TRANSCRIPT

SCHEDULE “A”
STATEMENT OF WORK
Program Background
The Health Services Program is a health benefits program offered by the Department of Social Development to assist eligible Clients to obtain specific health benefits that are not covered by Medicare, private health insurance plans or by other agencies. The coverage provided by the Department is meant to assist Clients to meet their basic medical and safety requirements.
The Health Services Program provides funding to assist Clients to acquire convalescent and rehabilitation equipment. The program also provides Clients with any necessary repairs and maintenance services, so they may maximize the benefits of their equipment. Convalescent equipment includes items such as; ambulation aids, bathroom aids, manual mobility equipment, power mobility equipment, seating and positioning aids, stability aids, transfer aids, homecare beds and pressure relieving surfaces.
The Supplier shall deliver services in the following areas:
Provide assistance to the therapists with assessments
Provide trial equipment
Provide new equipment
Provide rental equipment
Provide service repairs and maintenance
Equipment Rental Policy
The Supplier shall refer to Appendix A – Equipment Rental Policy to determine situations where the rental of equipment may be required.
Cost Sharing Policy
In cost sharing situations the Supplier shall adhere to the policy established by the Department as indicated in Appendix B – Cost Sharing Policy
Convalescent Equipment Supplier
The Supplier shall provide convalescent equipment to Clients of the Department based upon but not limited to the following:
Having extensive knowledge and experience within the convalescent equipment market.
Having an experienced team of sales staff and service technicians with proven abilities, capable of serving Clients within the Convalescent Program.
Having the ability to maintain warranty records for all equipment sold to the Department and access them as required for future services for the duration of their contract.
Able to coordinate the management of equipment recalls.

Having the ability to maintain electronic records of orders and delivery, material requests with time and Client location, and all approvals for auditing purposes;
Use of the most cost efficient approaches while meeting the functional needs of Clients as prescribed by the therapist.
Having a permanent business with established store front located within the Province.
Having demonstrated the ability to meet the Service Standards indicated in Appendix C – Standards for the Provision Equipment and Services.
The Supplier shall follow the eligibility criteria, approval, and purchasing and delivery processes for convalescent items by providing the following services:
Assist therapists with assessments
Provide trial equipment
Provide new equipment
Provide rental equipment
The following outlines the process and the services to be provided by the Supplier.
Step 1 - Referral and initial meeting to determine Client need and Health Card Coverage
Step 2 - Request Trial Equipment
Step 3 - Providing Final Documentation and Quotation
Step 4 - Health Services Review for Equipment Eligibility, Recycling and Approval
Step 5 - Acquire Equipment
Step 6 - Final Delivery and Equipment Setup
Step 7 - Invoice Submission
New and Recycled Equipment Requests
The Supplier shall refer to Appendix D – New and Recycled Equipment Request Process which provides a detailed process map and description of the equipment acquisition process.
Repairs and Maintenance
The Supplier must be authorized by the equipment manufacturer to perform the following.
Perform the repairs on site at the Client’s location; or
Pick up the equipment and repair it in the most cost effective manner and return the equipment to the Client’s location.
Repairs may be completed at the Suppliers place of business or sent to the manufacturer for repair.
The request for repairs and maintenance process is initiated by the Client, the Client’s Representative or by a therapist.

The Supplier shall perform repairs on equipment that may not have been originally purchased from the Supplier.
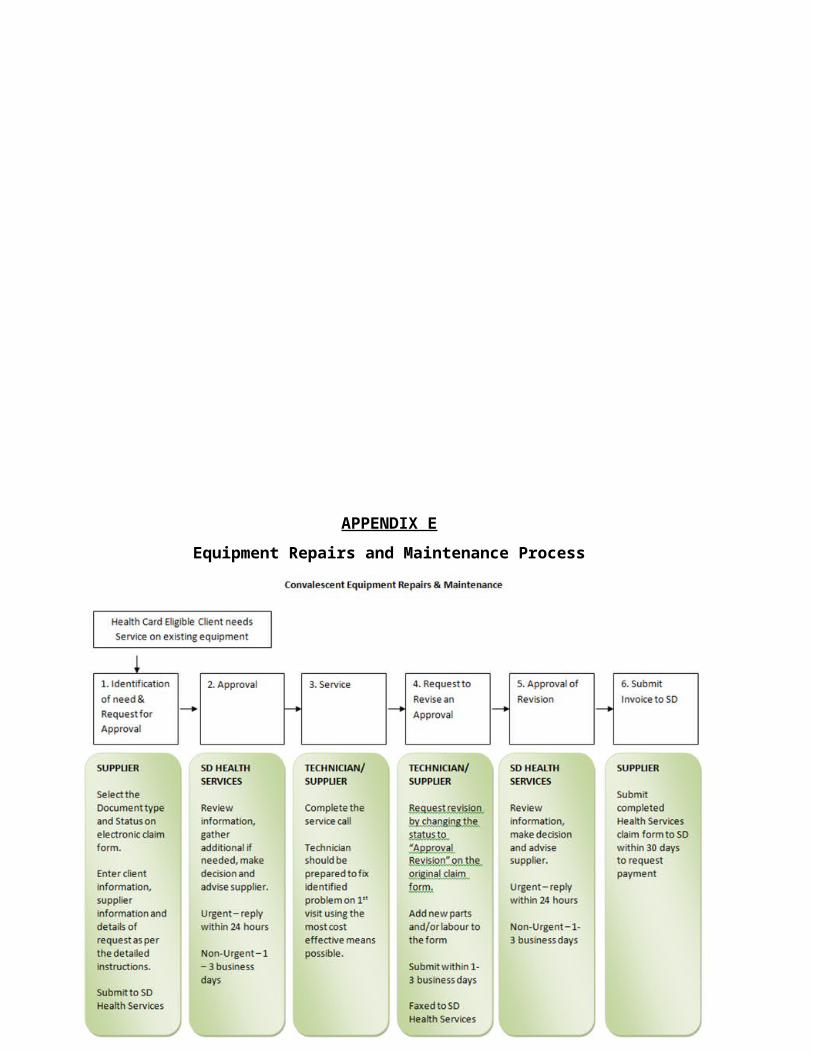
Equipment Repairs and Maintenance Process
The Supplier shall refer to Appendix E – Equipment Repairs and Maintenance Process Map for a detailed process and description of equipment repairs and maintenance.
The following is a summary of the equipment repairs and maintenance process.
Step 1 - Identification of Need and Request for Approval
Step 2 - Approval
Step 3 - Service
Step 4 - Request to Revise an Approval
Step 5 - Approval of Revision
Step 6 - Invoice Submission
Suppliers shall work with the following:
Therapists who are part of the assessment team and prescribe the appropriate equipment for the Client;
The Department who will approve and pay invoices for new equipment, maintenance and repairs of purchased or loaned equipment and equipment accepted for maintenance;
Clients of the Department or their representatives who will be the recipients of equipment. Employees of Adult Residential Facilities and Nursing Home Facilities where some Clients
reside.
The recycling agent who manages the Departments recycling program and delivers recycled convalescent items to Clients.
General Benefits List of Approved Equipment
The Department shall purchase equipment that has been identified within Appendix F – General Benefits List of Approved Equipment.
The approved list of equipment is subject to change based on the needs of Client’s or of the Department.
During the Agreement the Suppliers performance shall be measured to ensure that the Department and its Clients receive all deliverables. Reviews of Supplier performance may include interviews with therapists, written or phone surveys with Clients and a review of written correspondence from Clients.

SCHEDULE “B”COMPENSATION
The Supplier shall receive compensation as per the following pricing table: COMPENSATION SCHEDULE
EQUIPMENT SERVICE – CONVALESCENT PROGRAMWHEELCHAIR / SEATING
Type of Equipment Discount off MSRP Weekly Rental FeeManual mobility 25% $25Power mobility 17% $90Non-Custom Backs and Cushions (Note 1) 20% $25Custom work – materials (Note 2) At cost N/A
Custom seating (Ride) US MSRP + Exchange+$75 freight per component (Note 13) N/A
Accessories (Note 3) 15% $15CONVALESCENT / REHABILITATIVE
Type of Equipment Discount off MSRP Weekly Rental FeeAmbulation Aids 20% $35Bathroom Aids 20% $35Stability Aids 20% $25Transfer Aids 20% $75Home Care/Hospital Beds 20% $50Non-Power Pressure relieving surfaces 20% $20Power Pressure relieving surfaces 20% $100
SERVICE FEESService call (Note 4) $65Labour per half hour on the job (Note 5) $33Ceiling Lift -Installation of permanently installed tracking (Note 6) $475 per installation
Shop supplies (Note 7) 3%Miscellaneous Rentals (Note 14) negotiated with SupplierParts (Note 8) MSRP less 15%Batteries MSRP less 10%Mileage (urgent service calls and remote locations only) (Note 9) Current Provincial mileage grid
Shipping (from Supplier to Client only) (Note 10) At cost
Equipment Relocation (Note 11) Negotiated with SupplierTRIAL EQUIPMENT FEES
Trial fees (new equipment requests only) (Note 12)
Total value of all trial equipment with SD discount < $1500 $0
Total value of all trial equipment with SD discount $1500 - $10,000
$200/per case
Total value of all trial equipment with SD discount > $10.000 $300/per case

Invoices to the Department shall be allocated into four main pricing categories.
Invoices for wheelchair and seating equipment Invoices for convalescent and rehabilitative equipment Invoices for service fees completed by the Supplier Invoices for completing equipment assessments for Clients
All MSRP documentation shall be provided to the therapists or Health Services staff in accordance Appendix H - Provision of Manufacturer’s Suggested Retail Price (MSRP)
Compensation Schedule Notes:
1. All equipment and/or options purchased at the same time using the same order form will be discounted at the same rate.
Example: 2nd cushion cover purchased at the same time as the cushion
2. Fabrication of a unique component for a Client either from raw materials or by modifying commercially available products. If commercially available products are modified, they should be discounted at the rate indicated above and only the additional materials required for the customization would be invoiced at cost. Any labour charges shall be invoiced at the regular labour fee.
3. As defined in Appendix G – Service Agreement Terminology
4. Only one (1) service call fee shall be applied for each service request per program regardless of the number of visits. (See service call definition in Appendix G - Terminology)
Service calls are payable only under the following circumstances:
a. Repairs or maintenance to equipment provided or accepted for maintenance by the Department or loaned through the recycling program.
b. Delivery of new equipment when no installation or set up of the equipment is required and is it more cost effective than shipping.
c. Set up of recycled equipment that has been loaned or transferred to a Client. This may include repairs, modifications or installation of additional parts or components.
d. Delivery of rental equipment.
5. Invoiced per half hour per job, not per technician. Labour shall be invoiced only under the following circumstances.
a. Repairs or maintenance to equipment provided or accepted for maintenance by the Department or loaned through the recycling program.
b. Installation of new equipment that must be permanently installed in a Client’s home (exception - lifts - see # 6 below) c. Set up of recycled equipment that has been loaned or transferred to a Client. This may include repairs, modifications or installation of additional parts or components, as required.

6. Flat fee for the structural installation of tracking. No additional labour or shop fees shall be invoiced.
7. Invoiced as a fixed rate percentage to a maximum of $100 on any invoice that involves repair parts and labour only. Calculated as follows:
Total of equipment parts (MSRP - 15%) + labour x 3%.
Shop supplies are applicable for repair and maintenance invoices where both parts and labour are invoiced. They are not payable on new equipment, service call fees or when parts or labour are invoiced separately.
8. Proof of MSRP is required for any parts in excess of $500 MSRP.
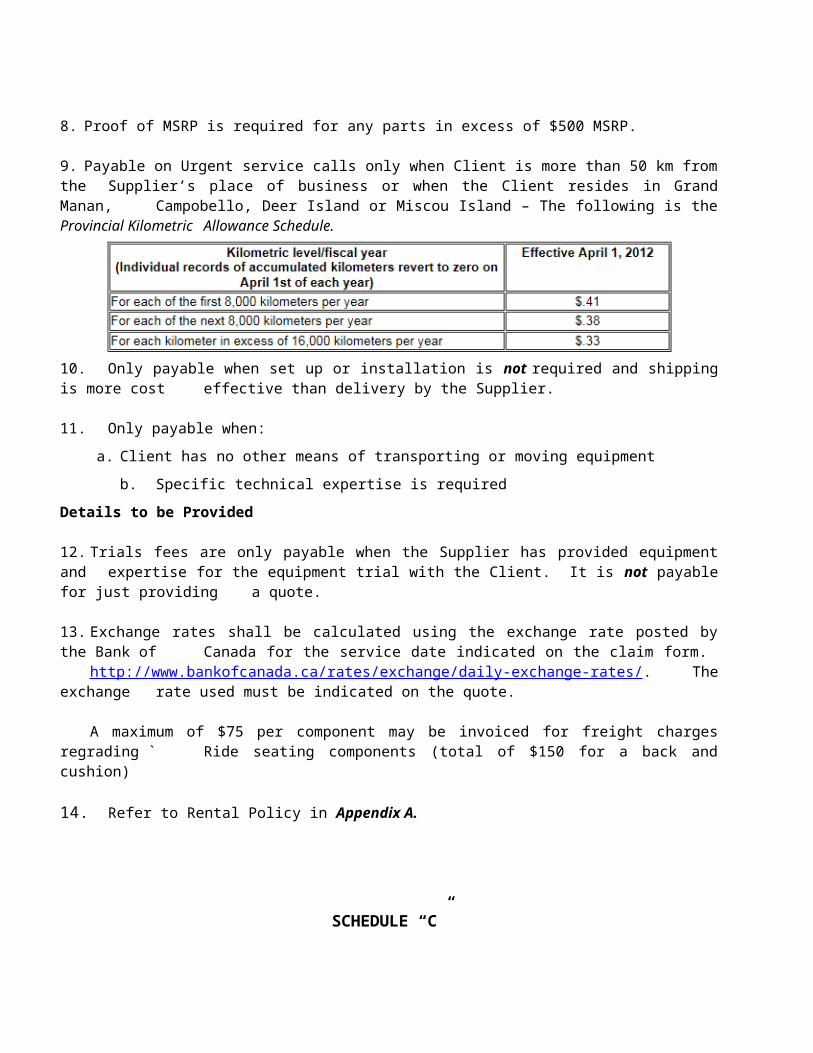
9. Payable on Urgent service calls only when Client is more than 50 km from the Supplier’s place of business or when the Client resides in Grand Manan, Campobello, Deer Island or Miscou Island – The following is the Provincial Kilometric Allowance Schedule.
10. Only payable when set up or installation is not required and shipping is more cost effective than delivery by the Supplier.
11. Only payable when:
a. Client has no other means of transporting or moving equipment
b. Specific technical expertise is required
Details to be Provided
12. Trials fees are only payable when the Supplier has provided equipment and expertise for the equipment trial with the Client. It is not payable for just providing a quote.
13. Exchange rates shall be calculated using the exchange rate posted by the Bank of Canada for the service date indicated on the claim form.
http://www.bankofcanada.ca/rates/exchange/daily-exchange-rates/. The exchange rate used must be indicated on the quote.
A maximum of $75 per component may be invoiced for freight charges regrading ` Ride seating components (total of $150 for a back and cushion)
14. Refer to Rental Policy in Appendix A.

SCHEDULE “C”
REPORTING REQUIREMENTS
The Supplier shall provide the Department with the following reports:
Reports shall be emailed to:
Mary Bartlett Department of Social DevelopmentHealth [email protected]
Social Development Record Check and Criminal Record Check Summary: (Appendix J)
Shall be completed and submitted as per the Social Development Record Check and Criminal Record Check Policy and Procedures. This must also be submitted for each new staff hired.
Social Development Record Checks and Criminal Record Checks for the employees of the Supplier. Employees who require checks shall have them completed within 30 days of the implementation of this Service Agreement.
Privacy Breach Notification: (Appendix K)To be completed and submitted immediately to the Department regarding any unauthorized disclosure of Confidential Information by the Supplier, its employees, associates, servants, agents or any third party.
Equipment Tracking (Trials and New) Report: This electronic report shall be sent every 3 months with the first report being due on January 30, 2018
Equipment Repairs and Maintenance Tracking Report:
This electronic report shall be sent every 3 months with the first report being due on January 30, 2018
APPENDIX A
Equipment Rental Policy
The Department shall consider the rental of equipment for Clients under the following circumstances:
1) The Client is waiting to receive equipment that has been approved for purchase by the Department. 2) The Client’s current equipment (purchased by the Department) requires repairs or modifications
that take more than a day
3) The Client has a medical and daily need for the equipment and has nothing else that is acceptable to use
4) Client uses the equipment on a full time, long term basis
5) The rental period will not exceed 12 weeks.
APPENDIX B
Cost Sharing Policy
1. Cost sharing requirements:
The Client must have an active Health Card with the appropriate coverage for the equipment or service requested.
The equipment or service must be a benefit through the Health Services Program.
The Client must meet all eligibility criteria for the equipment or service requested.
If the Department contribution exceeds 50%, then the Client must agree to the same terms and conditions as a Client who received 100% funding.
2. Cost sharing is considered an exception with cost sharing agencies such as private insurance companies and advocacy groups.
3. Equipment approved for cost sharing shall be purchased, rather than loaned by a recycling agency. There is no requirement for the Department to check for recycled equipment to meet the Client’s needs.
4. Clients shall be eligible for 100% coverage for repairs and maintenance on equipment which the Department has cost shared on if:
The Client has an active Health Card with the proper coverage
The eligibility criteria are met for the repairs or maintenance
The Supplier of the services is currently under contract with the Department.
5. If the Client has private insurance coverage for repairs, cost sharing will only be considered when written confirmation of this coverage is provided by the insurer at the time of the repair or maintenance request.
6. Cost sharing requests for both new equipment and repairs or modifications for children who are covered under a private insurance plan and whose Health Card ID number begins with “6” must be sent to the child’s social worker for a determination of financial eligibility. The social worker shall assess the family’s financial situation and determine if the co-pay amount will create hardship for the Client or their family. If the Social Worker approves, they will send the Exceptional Circumstances Form to the Department who will then process the request.
7. Documentation required to request cost sharing:
The Equipment Request Form, completed in full
Written confirmation of the funding in place which clearly indicates the amount of funding approved and how it will be applied to the request in question i.e. Explanation of Benefit, letter of confirmation, etc.
The Application for Cost Sharing Form, completed in full
Final quote from the Supplier which lists each piece of equipment and showing pricing at full cost.

Additional documentation as required – manufacturer’s order form(s), installation diagram, landlord’s permission to install, etc. as appropriate for the equipment
8. Occupational Therapist procedures for requesting approval for cost sharing requests:
Complete the assessment of the Client’s needs
Obtain written confirmation or denial of funding from the other funding agency
Complete the ERF
Complete the Application for Cost Sharing Form
Submit all documentation listed above to the Department for review unless the request is for a child who is covered by private insurance with an ID number beginning with “6”. Then the request must go to the child’s social worker first. (see #6 above)
If the request is approved, the therapist and the Supplier will be advised. If the request is refused only the therapist will be advised
9. Supplier procedures for cost sharing requests:
Assist the Therapist with the equipment trial
Provide a detailed, equipment specific quote to the Therapist.
This quote shall be provided using the full cost of the equipment as quoted to the other funding agency. The Department shall subtract the amount payable by the other funding agency to obtain their final payable amount.
Amount Payable = Price quoted to other funding source – portion paid by other funding agency
Note:
Clients covered by a private insurance policy but their policy does not cover the equipment being requested, a Statement of Benefits must be provided confirming their denial of the request and indicating the reason.
APPENDIX C: Standards for the Provision of Equipment and ServicesSERVICE STANDARD
Acknowledge receipt of TERF and arrange appointment with therapist for set up of trial equipment
Within 2 calendar days of receipt
Negotiate with therapist and set up trial equipment for Client with therapist
Within 14 calendar days of receipt of TERF
Delivery and set up of additional trial equipmentWithin 7 calendar days of request for additional equipment
Pick up of trial equipment Within 14 calendar days of initial set up
Delivery of new, assemble ambulation aids once approved for purchase by the Department
Within 14 calendar days of approval
Delivery of new, assembled bathroom aids once approved for purchase by the Department
Within 14 calendar days of approval
Delivery of new, assembled manual and basic power wheelchair s and related seating and positioning once approved for purchase by the Department
Within 4 calendar weeks of approval
Delivery of new, assembled complex power wheelchairs & related seating and positioning once approved for purchase by the Department
Within 6 calendar weeks of approval
Delivery of all new, assembled stability aids once approved for purchase by the Department
Within 14 calendar days of approval
Delivery of all new, assembled transfer aids once approved for purchase by the Department
Within 21 calendar days of approval
Delivery of all new, assembled home care beds or pressure relieving surfaces once approved for purchase by the Department
Within 21 calendar days of approval
Completion of service calls deemed urgent Within 2 working days of initial call
Completion of non-urgent service calls Within 5 working days of initial call
Complete resolution of service issue Within 21 working days of initial call
Delivery of rental equipment Within 2 days calendar days of approval
APPENDIX DNew and Recycled Equipment Request Process

Step 1: Referral and initial meeting to Determine Patient/Client Need & Health Card Coverage:
This process is initiated by identifying the Client needs. A Therapist shall complete a discipline specific assessment to determine that equipment is required to meet a Client’s needs in the most cost effective manner. In order to receive the benefits of this program, the Therapist confirms that the Client has a valid Health Card with appropriate coverage and verifies start and end dates.
A Therapist may consult a Supplier in order to assist them in determining the equipment options that will meet the needs of the Client and/or confirm availability of trial equipment.
Step 2: Requesting Trial Equipment
A Therapist may request trial equipment to determine if the equipment recommended will meet the specific medical needs of their Client. However, there may be situations where trial equipment will not be required. The equipment requested for trial must be a benefit item within the program in accordance to Appendix F - General List of Approved Equipment. Suppliers shall provide trial equipment when requested by a therapist. The equipment may be exactly as requested or the Suppler may suggest equipment that is comparable in function and features.
Exceptions may be considered in the following situations:

custom made equipment and seating
equipment that Suppliers are unable to provide for trial due to cost or complexity
The therapist is aware that all criteria have not been met (and that the Department could refuse the request) but wishes to submit a request for an exception.
If a Therapist determines that a trial is necessary they will contact a Supplier.
Suppliers shall receive a faxed copy of the Trial Equipment Request Form (TERF) from the therapist.
Suppliers will review the TERF and determine if the requested equipment, comparable equipment or a reasonable substitution is available in their trial inventory or readily available through a manufacturer for trial purposes. The final determination of what equipment is deemed acceptable for trial is done in consultation with the therapists.
Suppliers shall leave the trial equipment with the Client for up to two (2) weeks (14 calendar days) and shall schedule a pick up appointment time at delivery.
If additional or alternate equipment is requested during the trial, the Therapist and the Supplier shall schedule a time within a week to deliver the new equipment. The Client will have a maximum of one additional week to trial the additional or alternate equipment.
If at any time during the trial the Therapist determines that the equipment is no longer needed (either because they have determined it works or it doesn’t work for the Client) they shall contact a Supplier to arrange for the pick-up of the equipment.
At the end of the two weeks, if no amended TERF for additional trial equipment has been received, the Supplier shall pick up the equipment at the time that was previously arranged.
Step 3: Providing Final Documentation – Quote Suppliers shall provide the Therapist with a quote for all equipment prescribed on a Health Services e-claim form. This quote shall be completed as per the instructions in the Health Services Convalescent Program Procedures Guide and include the trial fee. The Supplier shall include acceptable proof of MSRP* for each piece of equipment, when sending the quote to the Therapist.
*refer to Appendix G - Terminology and * MSRP documentation policy in Appendix H - Provision of Manufacturer’s Suggested Retail Price (MSRP).
Step 4: Review for Equipment Eligibility, Recycling and Approval
The Department shall review and process the request from the therapist according to their policies and guidelines. Suppliers are guaranteed compensation for the trial they have completed, regardless of whether the equipment that is ultimately provided is new or recycled.
The Department shall utilize a non-profit organization that stores, redistributes and completes minor repairs and loan equipment. The purpose of the recycler is to reduce waste by reusing equipment and matching it to Clients’ needs.
Eligible Requests Process:

Equipment that is Custom or under $250:
The Department shall approve the request and fax the approval directly to the Supplier without checking with the recycling agent. The Department shall also advise the Therapist and Supplier of the approval by email.
Suppliers shall order equipment to the requested specifications and then notify the Therapists via email when the requested equipment has been ordered. The Supplier shall also confirm the expected delivery date and if any equipment has been back ordered.
Once all of the equipment has been obtained the Supplier shall arrange for delivery and set-up with the Therapist in the location designated by the Therapist. The Therapist (or designate) shall sign the equipment packing slip once the equipment is set-up.
Equipment that is Non-Custom or Over $250:
Recycling Agent Can Supply NONE of the EquipmentThe Department shall approve the quote and then fax the approval to the Supplier and advise the Therapist and the Supplier of the approval by email. The Suppliers shall then order all approved equipment.
Recycling Agent Can Supply SOME of the EquipmentThe Department shall approve the equipment that is not available through the Recycling Program then fax the approval to the Supplier and advise the Therapist and the Supplier by email. The Supplier shall then order the equipment approved for purchase only.
Recycling Agent Can Supply ALL of the EquipmentThe Department shall approve the trial fee only and then fax the approval to the Supplier and also advise by email. Suppliers may be requested to set up the recycled equipment for the Client’s use. Suppliers may request approval from the Department for any costs associated with the equipment set up.
Step 5: Acquire Equipment
As indicated above Suppliers shall acquire all remaining equipment that is not available via the recycling agent.
Step 6: Equipment Setup and Final Delivery
Once all of the equipment has been obtained the Supplier shall make arrangements with the Therapist to prepare and set-up the equipment at the designated location.
At the time of delivery of the approved equipment, the Therapist shall sign the Equipment Acceptance Form (EAF) (for purchased mobility devices only) or the packing slip for all other equipment provided. This verifies that the equipment received is the equipment that was ordered.
Step 7: Submission of Invoice

Suppliers shall submit their invoices to the Department for payment within 30 days of the equipment delivery and set up. Requests for payment must be mailed and shall include:
the completed Health Services e-claim form
a copy of the Suppliers’ own invoice stapled to the back of the E-form
the signed Equipment Acceptance Form (EAF) when billing a mobility device or signed packing slip for all other equipment.
Refer to Appendix I for a sample electronic claim form and for directions on how to complete it.
APPENDIX EEquipment Repairs and Maintenance Process

Step 1: Identification of Need and Request for Approval
Suppliers shall be contacted by a Client or therapist regarding an issue with a piece of equipment.
Suppliers shall acquire the following information:
a. Client name, address, Health Card number and expiry date
b. Manufacturer and model of equipment
c. Details of the problem:
i. What is the problem? What is broken or not functioning properly?ii. Is the equipment functional or completely broken?iii. Has the Client anything to use in the interim?
d. If a Therapist is requesting the service call, Suppliers shall include the Therapist’s name and any written documentation they have provided to explain the issue.
Suppliers shall complete the Health Services E-claim form (Excel based) to request approval for the service call, providing all of the information obtained from the Client or Therapist in the “Additional Information” field.
e. If the request is urgent, select “Urgent” as the status at the top of the claim form and provide details in the “Additional Information” section.
Note: Urgent requests are defined as meeting all the following conditions:
The Client’s current equipment is not functional
The equipment cannot be used until it is repaired
The Client requires the equipment to function on a daily basis
The Client cannot wait until the dealer’s next regular service run
The Client has nothing else that can be used as a replacement, even on a short term basis
Suppliers shall be required to submit the approval request to the Department by fax after the call requesting repair.
E-forms that are submitted that are incomplete or incorrect shall be returned unprocessed with a note explaining the issue.
Step 2: Approval
Suppliers shall receive a reply from the Department regarding the approval of the request for urgent requests within 1 business day and non-urgent requests within 3 business days.
Once approval has been received the Supplier shall complete the service call within 1 business day for urgent requests and 3 business days for non-urgent requests.
Note: Wheelchair / Seating equipment:
Approval from the Department for the service call for wheelchair/seating equipment implies approval to repair the issue(s) mentioned in the original submission unless the total invoiced cost (i.e. MSRP minus discount) of the parts exceeds $500 or the Department has indicated otherwise on the approval document. The Supplier does not need to resubmit for a revised approval and may invoice once the service(s) have been completed.
If additional issues are noted, and the total invoiced cost of the parts will not exceed $500 the Supplier may proceed with these repairs on the same visit. Should the total invoiced cost of the parts, exceed $500, the Supplier must submit a request to revise the approval before proceeding.
Refer to the “Request to Revise an Approval” in section 4 below for details on the revision process.
Should the MSRP of any one part exceed $500, proof of MSRP for this part shall be included with the request for approval.
Note: Convalescent/ Rehab equipment:

Approval from the Department for the service call for convalescent/rehab equipment implies approval to repair the issue(s) mentioned in the original submission unless the total invoiced cost exceeds $100 or the Department has indicated otherwise on the approval document. The Supplier does not need to resubmit for a revised approval and may invoice the Department once the service(s) have been completed.
If additional issues are noted, and total invoiced cost of the parts will not exceed $100 for the entire invoice, the Supplier may proceed with these repairs on the same visit. Should the total invoiced cost of the parts exceed $100, the Supplier shall submit a request to revise the approval before proceeding.
Refer to the “Request to Revise an Approval” in Step 4 for details on the revision process.
Should the MSRP of any one part exceed $500, proof of MSRP for this part shall be included with the request for approval.
Step 3: Service
Once approval has been provided by the Department the Supplier shall go to the service call prepared to fix the problem identified by the Client and to complete the repair in the most cost effective manner possible.
The Supplier shall always check to verify if the Manufacturer’s Warranty can be applied. The Department reserves the right to question requests when the possibility of warranty coverage exists and shall require justification for any refusals within the warranty periods published on the manufacturers’ websites. If no published warranty information exists, the Department shall require written justification from the manufacturer specific to the Client and equipment in question.
The Supplier shall always consider repairing equipment before requesting approval for replacement parts. If the part requiring repair is sealed, then the equipment shall be returned to the manufacturer for repair, if more feasible or cost effective.
Step 4: Request to Revise an Approval
The Supplier is required to complete the following steps when submitting a revision to an original request.
If additional approval is required once a technician has seen the Client, a revision shall be sent on the original claim form within 3 business days following the technician returns to the office.
Revise the original Excel based claim to include service dates for the work completed and add any parts, labor or other services that have not yet been completed. If the MSRP of any one part exceeds $500, proof of MSRP from the manufacturer shall be included. Supplier shall also enter any updates or additional information on the claim form that will assist the Department with assessing the revision.
Revisions shall be flagged by selecting “Approval Revision” for the document type.
The Supplier shall send the revision to the Department by fax. Revisions shall be reviewed and if approved, shall be dated in the Revision Date field. If refused, the reason will be in indicated in the Refused section of the claim form. If more information is required, the Department shall email the Supplier with the relevant questions.

Step 5: Approval of Revision
The Supplier shall receive a reply from the Department regarding the revision on urgent requests within 1 business day and within 3 business days for non-urgent requests.
Step 6: Submission of Invoice
When preparing the E-form for submission for payment, the Supplier shall:
Change the invoice status to “Request for Payment”
Enter all parts required indicating MSRP pricing
Enter labor and shop supply fees, where applicable
Enter the service dates.
Once the E-form is properly completed the Supplier shall print the invoice and mail to the Department within 30 day of completion of the work (i.e. date of service). The Supplier shall submit the completed Health Services claim form with a copy of their invoice stapled to the back to request payment.
Refer to Appendix I for a sample electronic claim for and for directions on how to complete it.
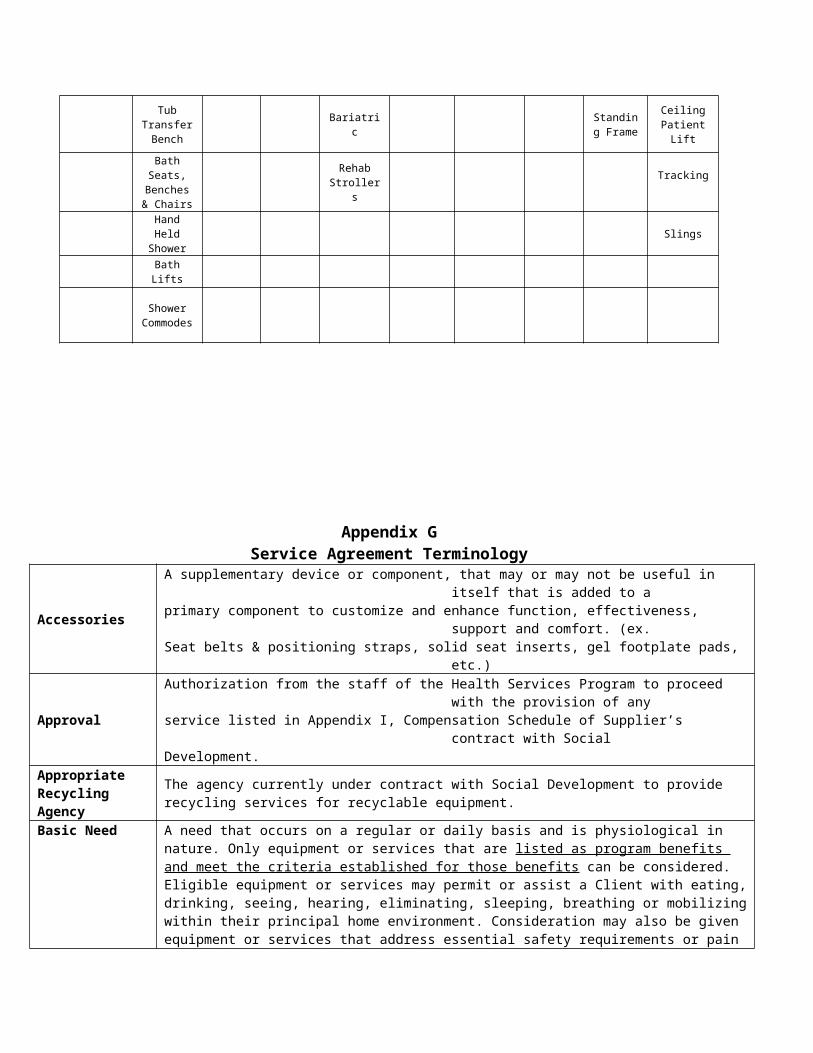
APPENDIX F
Benefits List of Approved Equipment
Ambulation Aids
Bathroom Aids
Custom Seating
Home Care Beds
Manual Mobility
Pressure Relief
SurfacesPower
Mobility Seating Stability Aids
Transfer Aids

2 Wheeled Walkers
Reducer Rings
Ride Designs
Electric-Single
Basic Folding
High Density Foam
BasicBack & Cushion
s
Trapeze Bar
Transfer Board
4 Wheeled Walkers
Toilet Risers
Electric-Double Lightweight Overlays Rehab Accessor
iesTub Grab
BarTransfer
Belt
Gait Trainers
Toilet Safety Frame
Bariatric Adjustable Axle
Reactive Surfaces
4 Wheeled Scooters Covers Bed Rails Transfer
Disc
Basic Commodes
Ultra-Light Weight
Active Surfaces
Power Conversion Products
Grab BarsStanding Transfer
Aid
Raised Toilet Seat
Tilt in Space
Wall Mounted Support
Patient Lift-power or manual
Rehab Commode Reclining Super
PolesPortable
Patient Lift
Tub Transfer Bench
Bariatric Standing Frame
Ceiling Patient Lift
Bath Seats, Benches &
Chairs
Rehab Strollers
Tracking
Hand Held Shower Slings
Bath Lifts
Shower Commodes
Appendix G Service Agreement Terminology
AccessoriesA supplementary device or component, that may or may not be useful in itself that is added to aprimary component to customize and enhance function, effectiveness, support and comfort. (ex.Seat belts & positioning straps, solid seat inserts, gel footplate pads, etc.)
ApprovalAuthorization from the staff of the Health Services Program to proceed with the provision of anyservice listed in Appendix I, Compensation Schedule of Supplier’s contract with SocialDevelopment.
Appropriate The agency currently under contract with Social Development to provide recycling services for

Recycling Agency recyclable equipment.
Basic Need
A need that occurs on a regular or daily basis and is physiological in nature. Only equipment or services that are listed as program benefits and meet the criteria established for those benefits can be considered. Eligible equipment or services may permit or assist a Client with eating, drinking, seeing, hearing, eliminating, sleeping, breathing or mobilizing within their principal home environment. Consideration may also be given equipment or services that address essential safety requirements or pain management issues.
Benefit A specific piece of equipment or service. Ex. wheelchair, service call, grab bar, etc.Billed cost MSRP minus the applicable DEPARTMENT discount
Business Day Any day other than Saturday, Sunday or Statutory Holiday in the Province of NewBrunswick.
Category of coverage
The various types of health coverage provided to Clients via the Health Card issued by Social Development which include Supplementary, Convalescent/ Rehab and Wheelchair/ Seating.
Home environment
Includes: Inside the Client’s primary place of residence i.e. house or residential facility Outside the primary place of residence including driveway, sidewalk and immediate yard
surrounding the house or facilityNote: Consideration may also be given to a child’s school environment so long as it does not exceed the eligibility criteria for the benefit requested.
Convalescent/ Rehab Program
A Health Services Program which provides Clients of Social Development with coverage for the provision and maintenance of specific convalescent and rehabilitation items and services which fulfill a basic need for a Client. Please refer to http://www2.gnb.ca/content/gnb/en/departments/social_development/health_services.html for details on benefits.
Cost sharing Paying the portion of the cost of equipment that is not covered by alternate funding source.
Custom Made Equipment
Made to order items fabricated from raw materials that are designed to meet the specific needsand measurements of an individual Client. (Commercially available items that can be ordered incustom sizes are not considered “custom”)
Custom WorkFabrication of a unique component for an individual Client either from raw materials of bymodifying commercially available products. See Appendix I, Note 2 for more details.
Date of Service The date the Client receives new equipment or that equipment repairs or modifications are completed.
Department The Department of Social Development (SD) Province of New Brunswick
EAFEquipment Acceptance Form – signed by a Therapist to confirm that a mobilitydevice has been provided to a Client as it was requested by the Therapist. It mustbe included in any billing that a Supplier submits to SD for a mobility device.
Eligible Benefit A piece of equipment or service which is listed as a program benefit for Clients ofSocial Development
Eligible ClientA Social Development Client who:
holds a valid health card has the proper category of coverage to cover the benefit requested meets the eligibility criteria for the benefit requested
Eligibility criteria a list of circumstances or conditions which a Social Development Client must meet in order to be approved to receive a benefit
EquipmentAny item that is complete and useful by itself that has been designed for a specific activity or purpose. It can be composed of several replaceable parts which make up one final unit (ex. Wheelchairs, lifts) OR an item that is self-contained and is designed to be used on its own (ex. Backs, grab bars).
ERF Equipment Request Form – used by therapists to request approval to provideConvalescent or Wheelchair related equipment and/or services to an SD Client.
Estimate A statement of approximate cost which takes into consideration all equipment and major options that a Client is expected to require.

Estimates should be provided in situations where a trial cannot be completed with the Client prior to submitting the request for approval or for ALL exception requests.
Exception request A request for coverage of a benefit/item when the Client does not meet all the eligibility criteria.
Explanation of Benefits
An official statement from a private insurance company which indicates the benefits and amounts they will cover for a Client.
Health Services Exceptions Committee
A committee established by Social Development to review and determine eligibility for all exceptional requests for equipment and services that have been submitted to the Health Services Program. Meetings are held on a monthly basis.
Health Services electronic claim form
An Excel based electronic claim form provided to Suppliers by the Health Services Program for the purposes of providing quotes, requesting approval, requesting approval revisions and requesting payment.
LabourThe time a technician spends actually repairing equipment. It does not include travel or waiting time and is only billed by the job, not the number of technicians. Please refer to the Compensation Schedule, Appendix I, Note 5 for further details.
Manufacturer’s Order form
A pre-printed form provided by the manufacturer which is specific to a make and model of equipment which provides the manufacturer’s suggested retail price for the base model of the equipment as well as the upcharges for the various options that may be ordered.
MileageThe distance between the city where the Supplier’s business is located and the location of a Client as per the Provincial Mileage Grid. Mileage is ONLY payable for service call requests which meet the criteria for “Urgent”
Modification Any change made to the original design, set up or prescription of the equipment. This change may or may not be permanent.
MSRPManufacturers’ suggested retail price – used by Health Services staff as a base price to calculate amounts payable for equipment and services offered through the Convalescent Program. Please refer to the MSRP Policy for further details.
New Equipment Equipment that no one has ever used
Option An additional feature which is not necessarily essential but can be ordered to enhance or complement the function of a piece of equipment.
PartSpecific pieces used to make one final unit. (Ex. Tires, brakes).A piece that is not normally useful by itself and is used in conjunction with other pieces to make one final unit (ex. Tires, brakes on a wheelchair.).
Primary device The device that the therapist has determined best meets the needs of the Client. If a Client uses more than one device equally, then one must designates as “primary”.
QuoteAn official statement of cost provided by an authorized Supplier which includes all the equipment and options prescribed by the therapist.
Quotes must be provided on the Health Services electronic claim form
Recyclable Equipment
Equipment that is specified as recyclable as per the contract between SD and has an MSRP greater than $250 is in a good state of repair (i.e. could be used by another person) is a complete item (i.e. not a part of a piece of equipment) is not custom fabricated
Repairs Restoring a piece of equipment (or a component of a piece of equipment) to a functional condition using physical labour and/or replacement parts.

Appendix H
Provision of Manufacturer’s Suggested Retail Price (MSRP)
The Supplier shall include the MSRP with each application for new equipment and for repair parts when the MSRP exceeds $500 for wheelchairs and $100 for convalescent/rehab equipment.
The following are acceptable methods of providing MSRP data.
Replacement Equipment
New or recycled equipment that will: replace equipment the Client already has
AND will serve the same purpose or meet the same basic need as the current equipmentPLEASE NOTE that only parts or accessories may be replaced as a result of wear and tear. All other equipment requires a therapist’s assessment.
Safe and Secure Storage Facilities
The equipment will be stored in a location where it cannot be stolen or damaged and where it will be protected from the elements (rain, snow, etc.)
Service Call A visit by a Supplier to a Client’s location to provide services as specified in the Compensation Schedule B.
ShippingFee payable to transport equipment to a Client when:
no set up or installation is required when is it more cost effective than delivery by the Supplier
Shop supplies Billed at the fixed rate of 3% of the total cost of repair parts and labour on repair and maintenance invoices only. Please refer to the Compensation Schedule B.
Special Authorization Request
A request for consideration of approval of a benefit/ item listed under Special Authorization Benefits which has special eligibility criteria. Many special authorization benefits must be found eligible by the Health Services Exceptions Committee before they can be processed.
Supplier/ Contractor
The successful proponents to this RFP who enter into a written contract with theDepartment of Social Development (SD) and the Province.
TERF Trial Equipment Request Form – completed by therapist to provide information to a Supplierregarding the exact specifications necessary for equipment trials or quotes.
Trial Equipment
Equipment used by a therapist to help determine the most appropriate prescription to meet aClient’s needs.
Suppliers are only expected to provide equipment from their own trial inventory or an inventory provided by a manufacturer. If the requested equipment is unavailable, they should offer the therapist equipment that is similar in function or design.
Any equipment provided by a Supplier should only be left with the Client for a maximum of 14 days.
Trial Fee Compensation to a Supplier for the temporary provision of trial equipment and expertise for the purpose of assessing a Client’s equipment needs.
Urgent
A request for repairs is considered urgent if ALL of the following conditions are met.: The Client’s primary equipment is not functional The equipment cannot be used until it is repaired The Client requires the equipment to function on a daily basis The Client cannot wait until the Supplier’s next regular service run The Client has nothing else that can be used as a replacement, even on a short term
basis.
Valid Health Card A medical benefit card issued by the Department of Social Development which has a “from” date in the past and a “to” date in the future and has the appropriate coverage for the benefit requested.
Wheelchair/ Seating Program
A Health Services Program which provides Clients of Social Development with coverage for the provision and maintenance of wheelchairs, seating components and accessories which fulfill a basic need for a Client. Please refer to http://www2.gnb.ca/content/gnb/en/departments/social_development/health_services.html for details on benefits.

A website link to the MSRP information. In cases where the website is password protected, access information shall be provided.
MSRP provided directly from the manufacturer and printed on their letterhead.
a. The model number must match the model number included in the ERF or repair price quote; and
b. The document must be clear and legible;
An email from the manufacturer which provides the relevant MSRP information. The complete email thread must be included if this option is used. If it is not possible to provide the MSRP using one of the methods described above, the therapist must select a manufacturer or a make and model of the required equipment that the Supplier can provide MSRP for and will serve the same/similar purpose as the original equipment.
Appendix I
Electronic From
The Department shall provide a sample of the Sample Electronic Form with instructions on how to implement the form prior to the scheduling of Supplier training.
Appendix J
Record Check Summary Form

Employee or Volunteer
Surname / Prénom de l'employé -
bénévole
First Name/Nom
Date of Birth/DDN
Date of Employment/
Date d'embauche
Date of Latest SD Record Check/
Date de la dernière Vérification du dossier de DS
Date of Latest Criminal Record Check/Date de la
dernière vérification du Casier judicaire
Social Development and Criminal Record Check Employee SummarySommaire Verification du Dossier DS et Du Casier Judiciaire
Name of Service Provider: ______________________________
Appendix K
Privacy Breach Notification

GENERAL INFORMATION
1) Public body information
Name of public body: _________________________________________________
Contact information (address, telephone number): ______________________________
Contact name and title: _________________________________________________
Contact’s telephone number:______________________________________________
Contact’s e-mail address: _________________________________________
2) Incident description
Date of Incident: ______________________________________________________
Date Incident was discovered: __________________________________________
How was the Incident discovered? _______________________________________
Location of Incident: ___________________________________________________
Briefly describe the breach. What happened?
______________________________________________________________________
STEP 1: CONTAINMENT OF THE BREACH
a. Have the records been retrieved? Yes _____ No ______
b. Have unauthorized copies been made? Yes __ No __ Not sure __
c. Are unauthorized copies kept by unofficial Persons? Yes __ No__ Not sure ___
d. Does Incident allow unauthorized access to other information? Yes __ No __
e. Describe the immediate steps taken to contain the breach:
________________________________________________________________________________
____________________________________________________________
STEP 2: IMPACT OF THE BREACH
a. Description of Personal information involved:
NOTE: Do not include or send any identifiable Personal information

______________________________________
______________________________________
______________________________________
b. Format of records involved:
□ Paper
□ Electronic (example: e-mail, word processing documents, computer database) If records are electronic, please state how they were protected (examples: password protected, encrypted, de-identified data):
□ Other (please describe): _______________________________________________________
c. Why did the breach occur? ________________________________________________________________________________
____________________________________________________________
d. Is there a risk of further exposure of the information? Yes ___ No___
e. Is this an isolated Incident? Yes ___ No ___
f. Number of individuals whose Personal information has been disclosed: _______
STEP 3: NOTIFICATION
a. Have the affected individuals been notified? Yes ___ No ___
If yes, please describe how notice was provided (e.g. who was notified, how they were notified, and what was included in the notice):
______________________________________________________________________
If not, why have they not been notified?
______________________________________________________________________
b. If you are not the Privacy Officer/Right to Information and Privacy Coordinator, has he or she been notified? Yes ___ No ___
If yes, who was notified and when? __________________________________________
If no, when will he/she be notified? __________________________________________

c. If applicable, have the police been notified? Yes ___ No ___
If yes, who was notified and when? __________________________________________
If no, why not? __________________________________________________________
d. Which other authorities have you notified, if any, and why?
_________________________________________________________________