document02
DESCRIPTION
zigomáticoTRANSCRIPT

Brånemark and coworkers introduced zygomaticimplants to restore function in persons with
severely atrophic edentulous maxillae.1 Numerousstudies have shown zygomatic implants to be a pre-dictable treatment option with very few technicaland biologic complications.1–13 However, it was notuncommon to encounter maxillary sinusitis in zygo-matic implant patients. The reported incidence ofmaxillary sinusitis after zygomatic implants rangesfrom 0% to 37.5%. In the present study, therefore, anew method was proposed to eliminate the maxillarysinusitis risk in zygomatic implants.
MATERIALS AND METHODS
Consecutive patients with severely atrophic maxillaewho were treated with zygomatic implants between
June 2007 and December 2008 were included in thisstudy. Patients who required extraction of theirremaining teeth were treated conventionally withoutthe use of a surgical template; patients who werealready edentulous were given the option of beingtreated by computer-assisted planning and template-based guided surgery.
All patients were free of signs and symptomsrelated to acute maxillary sinus infection at the initialconsultation. All patients were assessed preopera-tively for any medical contraindications that mightprevent them from undergoing general anesthesia.Both smokers and nonsmokers were included.Patients who had sufficient bone volume for conven-tional implant placement were excluded.
Cone Beam Computed Tomography ImagingCone beam computed tomography (CBCT ) wasemployed for preoperative imaging for every patient(Fig 1). The digital CBCT files were rendered for com-puter-based planning using Procera software (NobelBiocare). In selected patients, stereolithographic tem-plates were produced for guided zygomatic implantplacement according to a previously published pro-tocol.8 All patients were followed up with serial CBCTexaminations. CBCT was performed immediately afterimplant placement and repeated at the 3-month, 6-month, and 12-month follow-up appointments.
A New Method to Eliminate the Risk of Maxillary Sinusitis with Zygomatic Implants
James Chow, BDS, MDS, MBBS1/Peter Wat, BDS, LDS2/Edward Hui, MBBS, BDS, MDS1/Philip Lee, BDS, MDS1/William Li, BDS, MDS, Adv Dip OMS1
Purpose: A new approach for zygomatic implant placement was proposed to eliminate the risk of maxil-lary sinusitis related to the procedure. Materials and Methods: A prospective study of this new approachwas conducted, and consecutive patients treated between June 2007 and December 2008 wereincluded. An extended sinus lift with retained bone window was performed, such that zygomatic implantswere placed completely outside the displaced maxillary sinuses. All patients were followed up radiologi-cally at regular intervals using cone beam computed tomography to evaluate the status of the zygomaticimplants and the condition of the maxillary sinuses. Results: Sixteen patients (9 women and 7 men witha mean age of 60) were treated with 37 zygomatic implants. Within the period of investigation from 6 months to 24 months, there were no failed zygomatic implants, and no instances of maxillary sinusitiswere reported. Conclusions: The new approach that combined the zygomatic implant placement with theextended sinus lift procedure was predictable and fulfilled the purpose of lowering the risk of maxillarysinusitis. INT J ORAL MAXILLOFAC IMPLANTS 2010;25:1233-1240
Key words: bone regeneration, maxillary sinusitis, sinus elevation, sinusitis, zygomatic implants
The International Journal of Oral & Maxillofacial Implants 1233
1Director, Brånemark Osseointegration Center, Hong Kong, China.2Consultant Implant Prosthodontist, Brånemark OsseointegrationCenter, Hong Kong, China.
Correspondence to: Dr James Chow, Associated BrånemarkOsseointegration Center, 1901-1905, 1912-1913, The Center, 99 Queen’s Road Central, Hong Kong SAR. Fax: +852-28514700.Email: [email protected]
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Zygomatic Implant PlacementAll patients received general anesthesia for zygo-matic implant placement. Vital signs of all patientswere monitored, and all patients were observed fortheir depth of anesthesia using an electroencephalo-graphic bispectral index. All patients received pro-phylactic amoxicillin clavulanate (1.2 g intravenously)after induction of anesthesia.
Patients were divided into two groups: one groupreceived guided zygomatic implant placement andthe other received conventional zygomatic implantplacement. The patients who underwent guided zygo-matic implant placement were treated with Nobel-Guide stereolithographic templates. The guidedprotocol,8 previously published, made use of SimPlantsoftware (Materialise Dental) instead of Procera soft-ware (Nobel Biocare).
A crestal incision was made with vertical releasingincisions in the midline and second molar regions forpatients undergoing conventional flap surgery. Afterthe flap was raised and retracted, an extended rectan-gular bone window was cut according to the level ofthe sinus floor and sinus roof (Fig 2). The purpose ofthis bone window was to allow adequate exposure ofthe entry and exit points for zygomatic implants atthe crestal/palatal level and the zygomatic bone,respectively. The bone window was retained on theunderlying mucosa while the sinus membrane wasslowly and carefully elevated from the sinus walls. Theretained bone window acted as a shield that couldprotect the sinus membrane from direct damage byrotary instruments, such as the round bur and twistdrills (Fig 3).
1234 Volume 25, Number 6, 2010
Chow et al
Fig 1 CBCT for preoperative assessment.Coronal view demonstrates the anatomy ofthe zygomas and the status of the maxillarysinuses.
Fig 2 An extended sinus lift is performed with a retained bonewindow.
Fig 3 (Right) The retained bone window functions as a shield toprotect the sinus membrane from direct damage by the drills.
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

In patients treated with conventional flap surgery,zygomatic implant osteotomies were carried outstarting with a round bur, followed by a 2.9-mm-diam-eter twist drill, 3.5-mm-diameter pilot drill, and finallya 3.5-mm-diameter twist drill. The entire osteotomyprocedure was completed under direct visual control.In patients treated using the NobelGuide stereolitho-graphic template, the zygomatic implant osteotomywas performed through the palatal drill sleeve on thesurgical template 8 (Figs 4a and 4b).
In situations when more than one zygomaticimplant was placed on the same side, the posteriorzygomatic implant was placed first, followed by theanterior one. Conventional implants (NobelReplace orBrånemark System, Nobel Biocare) were placed in theanterior maxillary region between the zygomaticimplants according to the standard protocols recom-mended by the manufacturer. All patients were given5-day prescriptions for antibiotics, analgesics, andmouthwash (chlorhexidine 0.2%).
Loading of the Zygomatic ImplantsAll patients were given a fixed provisional prosthesisfor immediate or early loading. When a fixed prosthe-sis was attached to the zygomatic implants forocclusal loading within 24 hours after the surgery,
these zygomatic implants were considered immedi-ately loaded implants. If the prosthesis was placedafter this 24-hour period, zygomatic implants wereconsidered to be early loaded.
When the guided surgery protocol was employed,a provisional prosthesis was prefabricated and con-nected immediately or shortly after surgery. In otherpatients, an impression was made immediately aftersurgery. A provisional prosthesis made of a castcobalt-chromium framework and acrylic resin teethwas fabricated in the laboratory and was delivered tothe patient within a few days.
Patients were seen on a regular basis for woundcare and occlusal adjustment. All patients wereadvised to avoid hard or bony food during the initialhealing period of 3 months. Zygomatic implants wereexamined individually for stability before the finalimpression was made.
Success Criteria for Zygomatic ImplantsZygomatic implants were considered successfulwhen they met the following criteria: (1) asympto-matic function with a fixed prosthesis, (2) clinical sta-bility without mobility when examined individually,and (3) no sinus infection as detected clinically andradiologically.
The International Journal of Oral & Maxillofacial Implants 1235
Chow et al
Fig 4a A NobelGuide surgical template in place for guidedimplant placement. Two palatal drill sleeves are incorporated forzygomatic implants in the posterior region.
Fig 4b (Right) With the NobelGuide surgical template, a guidedtwist drill is placed through the drill sleeve and used to penetratethe crestal bone at the entry area for the zygomatic implant.
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

RESULTS
Sixteen consecutive patients were included (9women and 7 men, ranging in age from 38 to 83years, with a mean age of 60) and 37 zygomaticimplants were placed (Tables 1 and 2). Nine patientswere edentulous, while the others required extrac-tions on the day of surgery. Four patients underwentguided implant surgery, while the remaining patientsreceived conventional flap surgery. Two patientsreceived their prostheses immediately after surgery,while the others were given their prostheses 1 to 8days postoperatively. All zygomatic implants fulfilled
the success criteria. None of the 16 patients devel-oped any clinical signs or symptoms of maxillarysinusitis during the investigation period.
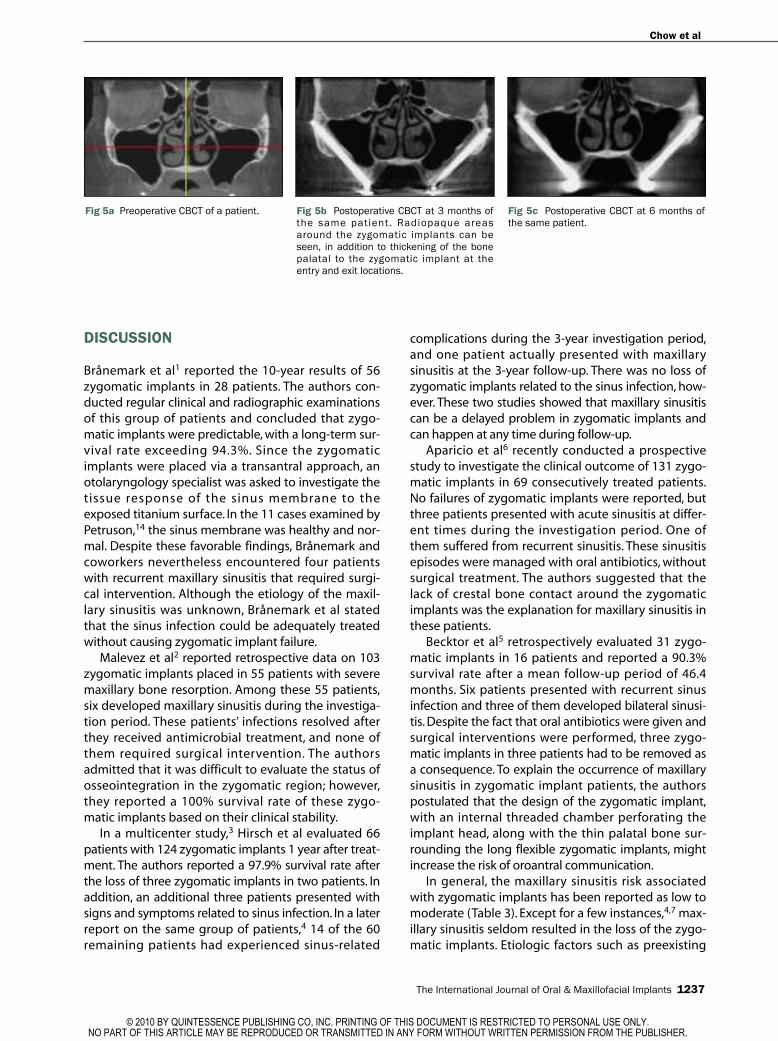
CBCT examinations were employed to evaluatethe maxillary sinuses and the zygomatic implants. Noradiologic signs of maxillary sinusitis were found. Inci-dentally, there were radiologic signs of new bone for-mation around the zygomatic implants in all patients.These radiologic signs (Fig 5) included the following:(1) existence of a radiopaque area surrounding thezygomatic implants and (2) thickening of the bone atthe entry and exit areas of the zygomatic implants.
1236 Volume 25, Number 6, 2010
Chow et al
Table 1 Patient Data
Patient no. Sex Age (y) Medical history Smoking NobelGuide Extraction
1 F 59 Clear No Yes Not required2 M 74 Ischemic heart disease No Yes Not required3 F 68 Osteoporosis No No Not required4 F 61 Clear No No Yes5 F 80 Epilepsy No No Yes6 F 38 Clear No No Not required7 M 65 Clear No Yes Not required8 M 54 Diabetes mellitus and hepatitis B No No Yes9 M 50 Hepatitis B No No Yes10 F 83 Congestive heart failure No No Not required11 M 47 Hypertension Yes No Yes12 F 52 Clear No No Not required13 F 70 Clear No No Not required14 M 51 Clear Yes No Yes15 M 56 Hypertension and ischemic heart disease No No Yes16 F 58 Hypertension No Yes Not required
Table 2 Implant and Prosthetic Data for Patients
No. of implants placed
Patient no. Anterior Zygomatic Date of surgery Date of loading Delay (d)
1 4 2 Jun 12, 07 Jun 12, 07 02 4 2 Jun 25, 07 Jun 26, 07 13 4 2 Jul 12, 07 Jul 13, 07 14 4 2 Oct 17, 07 Oct 20, 07 35 3 2 Oct 25, 07 Oct 29, 07 46 4 2 Dec 12, 07 Dec 14, 07 27 4 2 Dec 31, 07 Dec 31, 07 08 2 4 Jan 22, 08 Jan 23, 08 19 4 2 Jan 22, 08 Jan 25, 08 310 4 2 Feb 18, 08 Feb 26, 08 811 3 3 Mar 5, 08 Mar 6, 08 112 4 2 Mar 12, 08 Mar 20, 08 813 0 4 Jun 3, 08 Jun 5, 08 214 4 2 Sep 2, 08 Sep 3, 08 115 4 2 Nov 27, 08 Dec 1, 08 416 4 2 Dec 15, 08 Dec 17, 08 2Total 53 37
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
DISCUSSION
Brånemark et al1 reported the 10-year results of 56zygomatic implants in 28 patients. The authors con-ducted regular clinical and radiographic examinationsof this group of patients and concluded that zygo-matic implants were predictable, with a long-term sur-vival rate exceeding 94.3%. Since the zygomaticimplants were placed via a transantral approach, anotolaryngology specialist was asked to investigate thetissue response of the sinus membrane to theexposed titanium surface. In the 11 cases examined byPetruson,14 the sinus membrane was healthy and nor-mal. Despite these favorable findings, Brånemark andcoworkers nevertheless encountered four patientswith recurrent maxillary sinusitis that required surgi-cal intervention. Although the etiology of the maxil-lary sinusitis was unknown, Brånemark et al statedthat the sinus infection could be adequately treatedwithout causing zygomatic implant failure.
Malevez et al2 reported retrospective data on 103zygomatic implants placed in 55 patients with severemaxillary bone resorption. Among these 55 patients,six developed maxillary sinusitis during the investiga-tion period. These patients’ infections resolved afterthey received antimicrobial treatment, and none ofthem required surgical intervention. The authorsadmitted that it was difficult to evaluate the status ofosseointegration in the zygomatic region; however,they reported a 100% survival rate of these zygo-matic implants based on their clinical stability.
In a multicenter study,3 Hirsch et al evaluated 66patients with 124 zygomatic implants 1 year after treat-ment. The authors reported a 97.9% survival rate afterthe loss of three zygomatic implants in two patients. Inaddition, an additional three patients presented withsigns and symptoms related to sinus infection. In a laterreport on the same group of patients,4 14 of the 60remaining patients had experienced sinus-related
complications during the 3-year investigation period,and one patient actually presented with maxillarysinusitis at the 3-year follow-up. There was no loss ofzygomatic implants related to the sinus infection, how-ever. These two studies showed that maxillary sinusitiscan be a delayed problem in zygomatic implants andcan happen at any time during follow-up.
Aparicio et al6 recently conducted a prospectivestudy to investigate the clinical outcome of 131 zygo-matic implants in 69 consecutively treated patients.No failures of zygomatic implants were reported, butthree patients presented with acute sinusitis at differ-ent times during the investigation period. One ofthem suffered from recurrent sinusitis. These sinusitisepisodes were managed with oral antibiotics, withoutsurgical treatment. The authors suggested that thelack of crest al bone contact around the zygomaticimplants was the explanation for maxillary sinusitis inthese patients.
Becktor et al5 retrospectively evaluated 31 zygo-matic implants in 16 patients and reported a 90.3%survival rate after a mean follow-up period of 46.4months. Six patients presented with recurrent sinusinfection and three of them developed bilateral sinusi-tis. Despite the fact that oral antibiotics were given andsurgical interventions were performed, three zygo-matic implants in three patients had to be removed asa consequence. To explain the occurrence of maxillarysinusitis in zygomatic implant patients, the authorspostulated that the design of the zygomatic implant,with an internal threaded chamber perforating theimplant head, along with the thin palatal bone sur-rounding the long flexible zygomatic implants, mightincrease the risk of oroantral communication.
In general, the maxillary sinusitis risk associatedwith zygomatic implants has been reported as low tomoderate (Table 3). Except for a few instances,4,7 max-illary sinusitis seldom resulted in the loss of the zygo-matic implants. Etiologic factors such as preexisting
The International Journal of Oral & Maxillofacial Implants 1237
Chow et al
Fig 5a Preoperative CBCT of a patient. Fig 5b Postoperative CBCT at 3 months ofthe same patient. Radiopaque areasaround the zygomatic implants can beseen, in addition to thickening of the bonepalatal to the zygomatic implant at theentry and exit locations.
Fig 5c Postoperative CBCT at 6 months ofthe same patient.
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

sinus pathology, perforation of the sinus membrane,marginal bone loss around zygomatic implants, andinadequate oral hygiene at zygomatic implant siteshave been suggested, without scientific proof.
The original protocol1 for zygomatic implant place-ment did not emphasize the importance of theintegrity of the sinus membrane. The subsequentendoscopic study by Petruson14 strengthened thegeneral belief that titanium zygomatic implants werecompatible with sinus mucosal health and normalsinus function. In the literature, there have been inter-esting observations about how to manipulate themaxillary sinus membrane during zygomatic implantplacement. In many studies, the sinus membraneswere always perforated.3,9,10,15 Many other studies pro-vided no information about the integrity of the sinusmembrane during zygomatic implant placement.Although many clinicians attempted to preserve thesinus membrane, others believed that it was better toremove the sinus membrane to avoid possible trap-ping of soft tissue remnants between the implant andthe zygoma.3,10
Because maxillary sinusitis in zygomatic implantpatients has been a common observation, varioustechniques have been proposed to prevent sinusinfection. Peñarrocha et al15 employed the “slot tech-nique” to place 40 zygomatic implants in 21 patients.The advantages of this technique included the elimi-nation of a sinus window while preparing the zygo-matic implant osteotomy.16 However, in spite of thisadvantage, the authors stated that sinus membraneperforation could not be avoided. The sinus mem-branes in all 21 patients were invariably perforated,
and postoperative sinusitis was reported in twopatients. However, there was no evidence in the litera-ture suggesting that sinus membrane perforation wasassociated with postoperative sinusitis in zygomaticimplant patients.
In a recent publication, Aparicio and coworkers17
reported their experience with extrasinus placementof zygomatic implants in 20 patients. All patients pre-sented with pronounced buccal concavities lateral tothe maxillary sinuses. The contour of the maxillarywalls allowed the authors to perform zygomaticimplant placement without creating an opening intothe maxillary sinuses. In addition to 100% successafter a follow-up of 18 months, the authors did notencounter a single case of maxillary sinusitis.
In another study, Maló et al18 described an originalmethod of using extramaxillary implants with a newdesign to avoid the maxillary sinus while obtainingdirect bone anchorage in the zygomatic region. Malóet al presented 29 patients who had received 67extramaxillary implants and reported a 2-year sur-vival rate of 98.4%. Four patients who had developedpostoperative maxillary sinusitis were treated suc-cessfully by medical or surgical intervention. Malóreported that it was not possible to keep the sinusmembrane intact in some patients because ofanatomical factors. It would seem that when the max-illary sinus was perforated during the implantsurgery, the risk of maxillary sinusitis in conjunctionwith extramaxillary implants could not be ignored.
Although there is no evidence in the literature con-firming a cause-and-effect relationship between zygo-matic implants and maxillary sinusitis, it is reasonable
1238 Volume 25, Number 6, 2010
Chow et al
Table 3 Findings from Studies of Zygomatic Implants
Incidence of Sinus No. of No. of Loading Survival sinus membrane
Study patients implants Smokers protocol rate infection integrity
Brånemark et al (2004)1 28 56 Nonsmokers Two-stage 94.3% 4 (14.3%) Not knownMalevez et al (2004)2 55 103 18 smokers Two-stage 100% 6 (10.9%) Not knownHirsch et al (2004)3 66 145 15 smokers Two-stage 97.9% 3 (4.5%) All perforatedKahnberg et al (2007)4 60 145 15 smokers Two-stage 96% 14 (23.3%) All perforatedBecktor et al (2005)5 16 31 Not known Two-stage 92.3% 6 (37.5%) IntactAparicio et al (2006)6 69 131 27 smokers Two-stage 100% 3 (4.3%) Not knownZwahlen et al (2006)7 18 34 Not known Two-stage 94.1% 1 (5.6%) IntactChow et al (2006)8 5 10 Nonsmokers Immediate 100% 0 Not knownDuarte et al (2007)9 12 48 Not known 6 h 100% 0 All perforatedBedrossian et al (2002)10 22 44 Not known Two-stage 100% 0 All perforatedBedrossian et al (2006)11 14 28 Not known 2 h 100% 0 Not knownDavó et al (2007)12 18 36 Not known 48 h 100% 1 (5.6%) Not knownMozzati et al (2008)13 7 14 Nonsmokers 24 h 100% 0 Not knownPeñarrocha et al (2007)15 21 40 3 smokers Two-stage 100% 2 (9.5%) All perforatedAparicio et al (2008)17 20 36 12 smokers 24 h 100% 0 Not knownMaló et al (2008)18 29 67 3 smokers 24 h 98.5% 4 (13.8%) Not known
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

to think that the passage of a long and flexible zygo-matic implant through the thin crestal/ palatal bonecould increase the risk of oroantral communication.This risk of oroantral communication could be relatedto the residual bone thickness at the zygomaticimplant entry point. However, no information is avail-able about residual bone thickness in the literature forfurther analysis.
Theoretically, it is logical to try keeping the zygo-matic implants outside the maxillary sinuses. Theextrasinus placement technique17 was promising, butit only worked in patients with certain extremeanatomic characteristics. The new use of implants forextramaxillary anchorage by Maló et al18 was aninteresting attempt; however, there was a concernregarding the long-term stability of the soft tissueseal surrounding the implant heads.
In this study, an extended sinus lift was performedwith a retained bone window. In leaving the bonewindow attached to the sinus membrane, the mem-brane was kept intact during the zygomatic implantosteotomy. This short-term study showed promisingresults in avoiding maxillary sinusitis in zygomaticimplants. The extrasinus position of the zygomaticimplants was crucial for this success.
In addition to eliminating the risk of maxillarysinusitis in zygomatic implant patients, the newapproach revealed the possibility of new bone forma-tion around the zygomatic implants underneath theelevated maxillary sinus. CBCT images obtained after 3and 6 months suggested that new bone had beenformed around the zygomatic implants. These radio-logic features included a radiopaque area surroundingthe zygomatic implant bodies and increased thicknessof bone at the palatal entry and exit areas of the zygo-matic implants. These features were seen in everypatient, but they were more pronounced in somepatients. It was not possible to confirm that these radi-ologic features were mineralized tissues; however, sev-eral clinical and experimental studies19,20 couldprovide some insight regarding the probable boneformation underneath the elevated maxillary sinus.
Lundgren and coworkers19 conducted a prospectiveinvestigation of the potential of bone formationaround dental implants underneath an elevated sinuswithout using any graft material in 10 patients. Thisstudy demonstrated that new bone formation arounddental implants could be predictably achieved inside aspace created by sinus membrane elevation withoutgrafting. In an experimental study, Palma et al20 pro-vided histologic evidence of de novo bone formationunderneath the elevated sinus with or without simulta-neous implant placement. The study also showed thatbone formation was more pronounced around tita-nium implants with an oxidized surface. Although this
information could not be extrapolated directly to thecurrent study, it is reasonable to expect that zygomaticimplants with a similar surface may promote bone for-mation underneath an elevated maxillary sinus.
The potential advantages of the new method are:(1) elimination of the risk of maxillary sinusitis inzygomatic implants, and (2) increased zygomaticimplant stability through the promotion of sponta-neous bone formation underneath the elevated max-illary sinus membrane.
CONCLUSION
The risk of maxillary sinusitis related to zygomaticimplant placement can be avoided by performing anextended sinus lift with a retained bone windowbefore placing the implants. Follow-up studies arerequired to evaluate long-term outcomes of this newmethod. Moreover, clinical and experimental researchis needed to further investigate the probable boneformation around zygomatic implants underneaththe elevated sinus membrane.
REFERENCES
1. Brånemark PI, Gröndahl K, Öhrnell L-O, et al. The zygomaoption. Clinical procedure and long-term results. Scand J PlastReconstr Surg Hand Surg 2004;38:70–85.
2. Malevez C, Abarca M, Durdu F, Daelemans P. Clinical outcomeof 103 consecutive zygomatic implants: A 6–48 months fol-low-up study. Clin Oral Implants Res 2004;15:18–22.
3. Hirsch J-M, Öhrnell L-O, Henry PJ, et al. A clinical evaluation ofthe zygoma fixture. One-year follow-up at 16 clinics. J OralMaxillofac Surg 2004;62:22–29.
4. Kahnberg K-E, Henry PJ, Hirsch J-M, et al. Clinical evaluation ofthe zygoma implant: 3-year follow-up at 16 clinics. J Oral Max-illofac Surg 2007;65:2033–2038.
5. Becktor JP, Isaksson S, Abrahamsson P, Sennerby L. Evaluationof 31 zygomatic implants and 74 regular dental implants usedin 16 patients for prosthetic reconstruction of the atrophicmaxilla with cross-arch fixed bridges. Clin Implant Dent RelatRes 2005;7:159–165.
6. Aparicio C, Ouazzani W, Garcia R, Arevalo X, Muela R, Fortes V. A prospective clinical study on titanium implants in the zygo-matic arch for prosthetic rehabilitation of the atrophic eden-tulous maxilla with a follow-up of 6 months to 5 years. ClinImplant Dent Relat Res 2006;8:114–122.
7. Zwahlen RA, Gratz KW, Oechslin CK, Studer SP. Survival rate ofzygomatic implants in atrophic or partially resected maxillaeprior to functional loading: A retrospective clinical report. Int JOral Maxillofac Implants 2006;21:413–420.
8. Chow J, Hui E, Lee PK, Li W. Zygomatic implants—Protocol forimmediate occlusal loading: A preliminary report. J Oral Max-illofac Surg 2006;64:804–811.
9. Duarte LR, Filho HN, Francischone CE, Peredo LG, Brånemark P-I.The establishment of a protocol for the total rehabilitation ofatrophic maxillae employing four zygomatic fixtures in an im -mediate loading system—A 30-month clinical and radio -graphic follow-up. Clin Implant Dent Relat Res 2007;9:186–196.
The International Journal of Oral & Maxillofacial Implants 1239
Chow et al
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

10. Bedrossian E, Stumpel L III, Beckely ML, Indresano T. The zygo-matic implant: Preliminary data on treatment of severelyresorbed maxillae. A clinical report. Int J Oral MaxillofacImplants 2002;17:861–865.
11. Bedrossian E, Rangert B, Stumpel L, Indresano T. ImmediateFunction with the zygomatic implant: A graftless solution forthe patient with mild to advanced atrophy of the maxilla. Int JOral Maxillofac Implants 2006;21:937–942.
12. Davò Rodriguez R, Malevez C, Rojas J. Immediate function inatrophic upper jaw using zygoma implants. J Prosthet Dent2007;96(6, suppl):44–51 [erratum 2008;99:167].
13. Mozzati M, Monfrin SB, Pedretti G, Schierano G, Bassi F. Imme-diate loading of maxillary fixed prostheses retained by zygo-matic and conventional implants: 24-month preliminary datafor a series of clinical case reports. Int J Oral MaxillofacImplants 2008;22:308–314.
14. Petruson B. Sinoscopy in patients with titanium implants inthe nose and sinuses. Scand J Plast Reconstr Surg Hand Surg2004;38:86–93.
15. Peñarrocha M, García B, Martí E, Boronat A. Rehabilitation ofseverely atrophic maxillae with fixed implant-supported pros-theses using zygomatic implants placed using the sinus slottechnique: Clinical report on a series of 21 patients. Int J OralMaxillofac Implants 2007;22:645–650.
16. Stella PJ, Warner MR. Sinus slot technique for simplificationand improved orientation of zygomatic dental implants: Atechnical note. Int J Oral Maxillofac Implants 2000;15:889–893.
17. Aparicio C, Ouazzani W, Hatano N. The use of zygomaticimplants for prosthetic rehabilitation of the severely resorbedmaxilla. Periodontol 2000 2008;47:162–171.
18. Maló P, de Araujo Nobre M, Lopes I. A new approach to rehabil-itate the severely atrophic maxilla using extramaxillaryanchored implants in immediate function: A pilot study. J Prosthet Dent 2008;100:354–366.
19. Lundgren S, Andersson S, Gualini F, Sennerby L. Bone reforma-tion with sinus membrane elevation: A new surgical techniquefor maxillary sinus floor augmentation. Clin Impl Dent RelatRes 2004;6:165–173.
20. Palma VC, Magro-Filho O, de Oliveira JA, Lundgren S, Salata LA,Sennerby L. Bone reformation and implant integration follow-ing maxillary sinus membrane elevation: An experimentalstudy in primates. Clin Implant Dent Relat Res 2006;8:11–24.
1240 Volume 25, Number 6, 2010
Chow et al
© 2010 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Copyright of International Journal of Oral & Maxillofacial Implants is the property of Quintessence Publishing
Company Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission. However, users may print, download, or email articles for
individual use.