04 why health care server virtualization is...
TRANSCRIPT
vvirtu lDATA CENTER
04 Why Health Care Server Virtualization Is Different
Providers considering virtualization must know which platforms their EHR vendors support. As their implementation advances, a private cloud will emerge. By Don Fluckinger
10 Planning for Virtualized Disaster Recovery in Health Care
Many enterprises have embraced virtualized DR. Health care organizations can, too, if they keep HIPAA in mind. By Brien Posey
13 Lessons Learned: Virtualization Case Study
Three health care providers discuss the ups and downs of server virtualization. First lesson: The work doesn’t end after you’ve consolidated the server room. By elisaBeth horwitt
health care It edItIon
2 vIRTuAl DATA cEnTER E-zInE MARcH 2011
10 lines between bottom base of deck and first base of text
Drop cap is 5 lines
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
Making Server Virtualization Work for Health Care
s health care or-ganizations increase their reliance on electronic health record systems
and other powerful software applica-tions, the need to virtualize servers becomes readily apparent. These facilities can reap the same benefits that enterprises in other industries enjoy, but there are some precautions that health care providers should take before they embark on a server virtu-alization project.
SearchHealthIT.com features writer Don Fluckinger examines those chal-lenges in “Why Health Care Server Virtualization Is Different.”
Along with lowering data center costs, virtualization technology is an inexpensive and easy option for disaster recovery because it lets en-terprises recover data, applications and even entire operating system instances and restore them on any available hardware. However, as writer and former CIO Brien Posey
points out in “Planning for Virtualized Disaster Recovery in Health Care,” providers need to pay close attention to the Health Insurance Portability and Accountability Act when incor-porating virtualized disaster recovery technology.
Ultimately, virtualization is a work in progress. Upgrades will be neces-sary as health care providers add clin-ical services and the applications that support them. In “Lessons Learned: Virtualization Case Studies,” Search-HealthIT.com contributing writer Elisabeth Horwitt tells the story of three facilities in the midst of ongoing server virtualization implementations.
Has your organization succeeded in bringing virtualization technology into the server room? Did you do things differently from the facilities featured here? Drop me a line and share your best practices with your peers: [email protected] p
Brian Eastwood
Site Editor, SearchHealthIT.com
A
Server virtualization is getting a lot of attention
as hospitals and other healthcare organizations
increase IT usage and seek better ways to
control data center costs. Virtual and private
cloud deployments of patient care applications
and databases are mission-critical. And so is
the uptime and reliability of the IT infrastructure
that supports them.
Uptime Assurance. Without thehigh cost or complexity.Resilient Stratus servers and high-availability
software deliver proven, affordable uptime for
physical servers, virtual servers, and private
clouds in healthcare data centers of every size.
These highly automated solutions also greatly
reduce the cost and complexity of configuring
and managing multiple virtual machines — a
primary concern of healthcare IT organizations.
Stratus ftServer systemsThe fault-tolerant ftServer® family guarantees
industry-leading uptime and plug-and-play
simplicity for Microsoft® Hyper-V®, and
VMware® vSphere™ operating environments.
Unlike clusters, you get automatic 24/7 uptime
without application modifications or multiple
software licenses.
Stratus Avance softwareStratus® Avance® software with built-in
virtualization is the most simple, cost-effective,
high-availability solution for x86 servers. Built-in
virtualization enables smaller organizations to
install and manage virtual machines in minutes
— without specialized IT skills or certification.
Uptime. All the time.
Uptime Assurance forVirtualized Healthcare IT
V I R T U A L I Z AT I O N B R I E F
Cost-effective virtualization in the healthcare data center
“We were quick to recognize that ftServersystems offered the reliability, simple operation,and VMware support necessary to underpin aprivate cloud model for EHRs.”
Cathy CrowleyChief Information OfficerColumbia Memorial Hospital
LEARN MORE
CASE STUDY LINKS
• Columbia Memorial Hospital
• Alice Peck Day Health Systems
WHITE PAPER LINKS
• Best Practices for Mission-Critical Virtualization
• Avance HA Software and Virtualization
VIRTUALIZATION PAGE
• www.stratus.com/go/virtualization
Stratus, Avance, ftServer and the Stratus logo are registered trademarks of Stratus TechnologiesBermuda Ltd. All other trademarks and registered trademarks are the property of their respective holders.© 2011 Stratus Technologies Bermuda Ltd. All rights reserved.

4 vIRTuAl DATA cEnTER E-zInE MARcH 2011
10 lines between bottom base of deck and first base of text
Drop cap is 5 lines
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
H
Why Health Care Server Virtualization Is DifferentProviDers ConsiDering virtualization must knoW WhiCh Platforms their ehr venDors suPPort. as their imPlementation aDvanCes, a Private ClouD Will emerge. By Don FLuCkIngeR
ealth care organi-zations are mov-ing forward with server virtualization whether electronic
health record (EHR) vendors are ready or not. In fact, many vendors aren’t supporting a virtualized en-vironment yet. Nevertheless, the technology offers so many benefits over physical servers—from lowering hardware costs to facilitating systems interoperability and health informa-tion exchange (HIE) to faster disaster recovery—that health care providers simply cannot wait for EHR software vendors to catch up.
Yet health care is a little different from other businesses because of the life-and-death needs of pa-tients and their caregivers. Virtual-ization helps build redundancy of resources into the network while saving space and energy, said Pacer Hibler, network engineer at New Hanover Regional Medical Center
in Wilmington, N.C.“In every decision we make in re-
gards to virtualization … we think about whom we’re impacting on the other end,” Hibler said.
Most medical software vendors Hibler deals with are either support-ing virtualization or planning to in the near future because they under-stand most hospitals will be doing it to relieve data center overload. “We’re not trying to be a beta envi-ronment. … We can’t just start throw-ing stuff into a virtualized environ-ment,” he said.
Below, Hibler and two peers—Todd Bruni, director of identity and con-figuration management at Christus Health in Irving, Texas; and Bill Gillis, eHealth technical director at Boston-based Beth Israel Deaconess Medical Center—have advice for hospitals that are virtualizing their network servers in preparation for the great health IT expansion that EHR systems invariably bring.

5 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
MiXinG and MatCHinG VEndorsMicrosoft, VMware Inc. and Citrix Systems Inc. are the big players in server virtualization. VMware is far and away the market leader, but a case can be made for using each ven-dor in certain situations, Bruni said. About 60% of the 2,500 servers in Christus Health, which runs 40 hospi-tals in six U.S. states and Mexico, are virtualized, he estimates.
Network administrators run virtual environments with hypervisors, ap-plications that allow multiple operat-ing systems to run on a single piece of hardware. All the major vendors offer free versions of their hypervi-sors, and that allows administrators to experiment with configurations. Citrix XenServer Free Edition and the VM-ware vSphere Hypervisor have limited features compared with their for-pay counterparts, but the full-featured version of Microsoft Hyper-V R2 is available for free with the Windows Server OS.
Administrators’ needs vary from site to site. One site might want the features of a particular hypervisor; another might prefer a different hy-pervisor based on its greater com-patibility with the applications and operating systems it will control. Once environments outgrow their free hypervisor, still others might want to base their decision on pricing and licensing needs. Each hypervisor has its trade-offs, so experimenting with the free ones helps.
Some shops, including Hibler’s and Bruni’s, use both Citrix and VMware virtual server-hypervisor
setups. Christus Health is looking into whether Hyper-V makes sense in certain applications. It all comes down to how well applications perform.
“What we’ve tried to do is say, ‘We’re going to be a hypervisor- agnostic shop,’” Bruni said. “We origi-nally put our stake in the ground and said, ‘VMware-only,’ but we started
finding out that not only do we have requirements, but … vendors [also have] different hypervisor require-ments.”
For instance, some independent software vendors are pushing his or-ganization to use Microsoft’s Hyper- V instead of VMware, Bruni said. His team members want to build flexibil-ity into the network to accommodate that as best they can.
In the meantime, the hybrid model works well—though it takes two groups of IT specialists to run it, and they don’t always speak each other’s language, Hibler said. “We’re broken up into VMware teams and Citrix teams. Our VMware virtualization
What we’ve tried to do is say, “We’re going to be a hypervisor- agnostic shop.”toDD Bruni, identity and configuration management director, Christus Health
6 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
guys do not manage our Citrix virtual-ization and vice versa,” he said.
PLanninG For and EXPandinG a VirtUaL EnVironMEntSo, how does one figure out what to virtualize and whether to create a single-vendor or hybrid setup? Pa-tience is a virtue when it comes to virtualizing health care networks. Consult software vendors and find out whether an upcoming version of an application will support virtualiza-tion. Wait until the release to roll that app into your own virtualized environ-ment, said Hibler, whose facility took several years to complete its 200-plus virtual server network.
Getting your electronic health re-cord vendor at the planning table is “a prerequisite for the success” of any virtualization project, Bruni said.
If the vendor says it doesn’t support server virtualization but offers a Soft-ware as a Service choice among its product lines, talk to your contact and find out which virtualization platform the SaaS EHR uses. Odds are that platform will work best for your shop.
Some legacy software vendors might throw up their hands and say, “If it works, it works” in a virtualized environment, Hibler said. Chances are, however, your facility won’t be relying on those apps for use in criti-cal patient care, but, rather, to support critical apps.
Because different vendors’ sys-tems—and their capabilities—vary so widely, hospitals looking to con-solidate and virtualize servers should
hire outside help with the project, “so they’re not constrained by their lack of knowledge,” Gillis said.
Hospital IT leaders should seek out similarly sized peers in similar circum-stances and ask them how they made the transition from physical to virtu-
alized environments, Hibler advised. “When we went forward,” he said, “we knew we weren’t the only people trying to do this.”
adVanCEd VirtUaLiZation MEans PriVatE CLoUd …Start small in virtualization, Bruni said. Make it a noncritical application that doesn’t affect patient care. The more advanced—and consolidated—an organization’s virtual environment gets, the closer it gets to creating a private cloud. In addition to virtual-ization, a private cloud offers the ben-efits of on-demand resource delivery, application automation, resource
“in every decision we make in regards to virtualization … we think about whom we’re impacting on the other end.”PaCer hiBler, network engineer, New Hanover Regional Medical Center
7 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
pooling and broad network access. For health care organizations, it also allows for direct control of security, which is important in light of the Health Insurance Portability and Ac-countability Act (HIPAA) and other security and privacy laws.
That’s what happened at Beth Israel Deaconess. A few years ago, as part of an eClinicalWorks LLC EHR deploy-ment to roughly 200 affiliated ambu-latory physicians, the hospital virtual-ized servers on VMware technology. One at a time, one virtual server—including the EHR software integrated
with a practice management app and billing system—was deployed to each practice. The hospital originally con-sidered building a server farm for the physicians but opted for a virtualized model instead.
In those days before meaningful use, adopting an EHR system was optional, so building a server farm would have been tantamount to con-structing a grand hotel and risking low occupancy if, for example, only 50 physicians bought in, Gillis said. Vir-tualizing made it more like a housing development in which the hospital’s
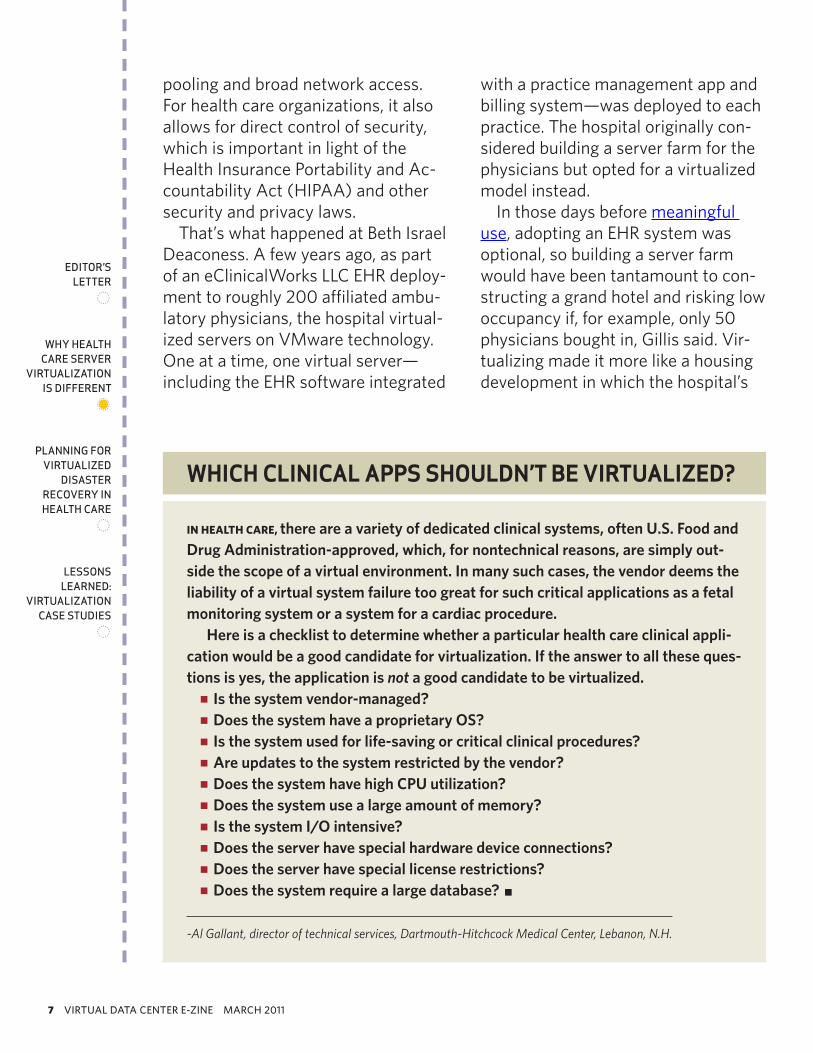
in HEaLtH CarE, there are a variety of dedicated clinical systems, often u.s. Food and Drug administration-approved, which, for nontechnical reasons, are simply out-side the scope of a virtual environment. in many such cases, the vendor deems the liability of a virtual system failure too great for such critical applications as a fetal monitoring system or a system for a cardiac procedure.
here is a checklist to determine whether a particular health care clinical appli-cation would be a good candidate for virtualization. if the answer to all these ques-tions is yes, the application is not a good candidate to be virtualized.
is the system vendor-managed? pp
Does the system have a proprietary os? pp
is the system used for life-saving or critical clinical procedures? pp
are updates to the system restricted by the vendor? pp
Does the system have high cPu utilization? pp
Does the system use a large amount of memory? pp
is the system i/o intensive? pp
Does the server have special hardware device connections? pp
Does the server have special license restrictions? pp
Does the system require a large database? pp p
-Al Gallant, director of technical services, Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
WHICH CLInICaL aPPS SHouLDn’t Be VIRtuaLIzeD?
8 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
IT staff built little houses as needed, he said.
A couple of years into the project, Beth Israel Deaconess realized it in-advertently had built the first—or one of the first—private clouds in health care, said Gillis with a laugh. As in-novative as it was coincidental, the hospital’s virtualized private cloud model has many attributes that are attractive to other health care net-works looking for a model from which to crib their own EHR infrastructure: It’s scalable, but it doesn’t require a huge hardware outlay or data center footprint at the start.
“Lo and behold, apparently we built a private cloud. At least that’s what everybody told us,” Gillis said. “We didn’t go into this thinking, ‘Hey, let’s build a cloud.’ It was, ‘We want a sub-scription-type service,’” in which phy-sicians could get rid of their home-grown technology and tap into Beth Israel Deaconess’ infrastructure with only an Internet connection and their desktop machines.
… and PriVatE CLoUd Can MEan HiE Beth Israel Deaconess’ server virtu-alization made good on some of its potential: For example, it cut energy costs and requires a much smaller data center footprint than the physical server setup it replaced. At first, 200 physicians’ worth of servers and stor-age area network hardware took up less than one full rack at a colocation facility. Now the cloud takes up two and a half racks and is built to accom-
modate approximately 350 physicians by year’s end.
Beth Israel Deaconess still is con-strained by client requirements, Gil-lis said. For example, end users still
need a minimal set of hardware and applications on their end. Ideally, the hospital also would like to deploy vir-tual desktops in a hardware-agnostic way so physicians could manage apps from their laptops, tablets and smartphones without any hardware requirements. That could happen in the future. For now, IT staff members are trying to make all the systems talk to each other.
“Interoperability is where [we are] steaming toward today,” Gillis said, referring to the general movement in health care IT to combine data from various proprietary systems into a patient-accessible EHR. Virtualiza-tion can help enable interoperability, which, in turn, can enable HIE—the
“if something happens—whether it’s a small or big disaster—we can swing this environment over to an off-site data center and be back up and running as usual.”PaCer hiBler, network engineer, New Hanover Regional Medical Center

9 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
holy grail of federal health IT author-ities—among hospitals across the country.
Beth Israel Deaconess’ virtualiza-tion implementation will let physi-cians within its private cloud ex-change data. That’s the first step in the hospital network’s HIE project, which eventually will extend outside its cloud to other area hospitals and later to the whole country.
“I’m talking about it as if it’s easy,” Gillis said. “Quite frankly, we’ve been working on it for a month or two, and it’s probably the most complex clinical health information thing I’ve ever tried to achieve—more complex than build-ing this cloud. There are so many mov-ing parts, so many pieces that need to work and flow. It is challenging.”
LittLE nEEd For HardwarE ConFiGUrationMeanwhile, virtualization doesn’t re-quire a lot of hardware configuration when a user or application requires more memory or storage; it requires only the assignment of more virtual resources, Hibler pointed out. Testing, customizing and adjusting become
simpler—and more forgiving—than when you’re working with physical servers. “You just have to trend your environment, watch your servers, and give and take as you need,” he said.
Server virtualization helps compli-ance with Joint Commission require-ments for disaster preparedness plan-ning, said all those interviewed for this story. (Joint Commission accreditation qualifies hospitals to receive Medicare and Medicaid reimbursements.)
A virtualization implementation does not guarantee swift disaster re-covery. But it does make recreating a network from a remote location much faster, spooling up a server per minute in Gillis’ facility, for example, com-pared with hours or days to recon-figure a physical server on the exact same hardware.
“Our plan with virtualization,” Hibler said, “is if something happens, whether it’s a small or big disaster, we can swing this environment over to an off-site data center and be back up and running as usual.” p
don FLUCkinGEr is features writer for SearchHealthIT.com. contact him at [email protected].
10 vIRTuAl DATA cEnTER E-zInE MARcH 2011
10 lines between bottom base of deck and first base of text
Drop cap is 5 lines
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
A
Planning for Virtualized Disaster Recovery in Health Caremany enterPrises have emBraCeD virtualizeD Dr. health Care organizations Can, too, if they keeP hiPaa in minD. By BRIen PoSey
lthough once mar-keted solely as a technology for de-creasing hardware costs, server virtu-
alization has proved to be an excellent technology to use in disaster recovery situations. If an organization’s physi-cal servers have been destroyed, it is usually relatively easy to restore back-ups of those systems to virtual hard-ware. This allows the organization to restore functions quickly without having to worry too much about the underlying physical hardware.
Even though server virtualization might work well for disaster recov-ery, health care organizations do not have the luxury of deploying a vir-tualized disaster recovery site on a whim. Changes to such an organiza-tion’s disaster recovery efforts require thorough planning. It must maintain Health Insurance Portability and Ac-countability Act (HIPAA) compliance and could be required to comply with
Payment Card Industry (PCI) and Joint Commission standards.
So, does this mean that health care organizations cannot use virtualized disaster recovery sites? Absolutely not. It simply means that they have to take regulatory compliance into consideration whenever they make a change to their disaster recovery in-frastructure.
In order to maintain HIPAA compli-ance, the law requires organizations to create and maintain three plans related to disaster recovery. If an or-ganization makes any change to its disaster recovery efforts, such as to incorporate virtualized disaster recov-ery technology, these plans will have to be revised to reflect the changes.
First PLan: data BaCkUPThe first plan a HIPAA-covered en-tity is required to maintain is a data backup plan. This is intended to serve as proof that the organization has
11 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
documented and implemented pro-cedures for creating and maintain-ing exact copies of electronic health information. In other words, the data backup plan should provide a detailed description of backup procedures.
It is fully expected that an organiza-tion’s backup requirements will evolve over time, so HIPAA auditors will look for the plan to be updated regularly.
The plan’s most recent revision must match the procedures currently in use in the organization.
It is worth noting that if a health care organization decides to incor-porate server virtualization into its disaster recovery efforts, it might not have to worry about revising its data backup plan. That’s because the data backup plan focuses on backing up data, not restoring it. With that focus, a data backup plan probably would not be affected by the use of server
virtualization technology unless a company found itself running backup software on a virtual server or writ-ing backups to a virtual server (such as a virtualized instance of Microsoft System Center Data Protection Man-ager).
sECond PLan: disastEr rECoVErYThe second plan that health care or-ganizations are required to document is a disaster recovery plan. While the data backup plan focuses on proce-dures for backing up data, the disaster recovery plan documents the proce-dures used to restore data after a di-saster strikes.
Keep in mind that a disaster recov-ery plan does not focus on restoring files that have been deleted acciden-tally by a user but, rather, on dealing with catastrophic situations. The plan should describe the resources and procedures required to resume critical business processes after a natural or man-made disaster occurs.
As is the case with the data backup plan, HIPAA compliance requires that a disaster recovery plan include de-tailed procedures. Organizations are expected to revise these documented procedures as their recovery plans evolve.
If a disaster strikes, you ideally should be able to restore your data to its original location. Depending on the scale of the disaster, however, this could prove to be impossible. After all, if your entire data center has been wiped out in a hurricane, the odds of
even though server virtualization might work well for disaster recovery, health care organizations do not have the luxury of deploying a virtualized disaster recovery site on a whim.
12 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
being able to reuse your server hard-ware are pretty slim.
With that in mind, if you decide to use virtual servers as a part of your contingency plan, your disaster recov-ery plan will need to include proce-dures for restoring backups to virtual hardware. You also will be required to specify under what conditions the vir-tual machines will be used.
tHird PLan: EMErGEnCY ModE oPErations PLanThe emergency mode operations plan, the third and final one that health care organizations are required to maintain, describes how the or-ganization will continue to operate after a disaster, such as a fire or flood. Whether the emergency mode opera-tions plan will need to be changed to reflect the use of virtual servers de-pends only on how the organization plans to use the virtual servers in the event of a disaster.
Suppose, for instance, that your plan is to restore your backups to virtual machines in the local data center if possible but to fail over operations to a remote data center if necessary. In such a situation, the emergency mode operations plan probably would not require much revision, because your use of server virtualization is irrelevant to the remote data center (which pre-sumably is already in place).
On the other hand, let’s say that if your data center is destroyed, your plan
is to build a remote data center on the fly by using virtual server technology. In this situation, using virtual servers would be directly involved in emer-gency mode operations, so your emer-gency mode operations plan would
need to address server virtualization.Overall, virtualized servers can be
extremely beneficial in disaster re-covery situations. Even so, a HIPAA-covered entity cannot legally use this approach unless its data backup, di-saster recovery and emergency mode operations plans are updated (as necessary) to reflect its new disaster recovery strategy. p
BriEn PosEY is a freelance technical writer who has received Microsoft’s MvP award six times for his work with Exchange Server, Windows Server, Internet Information Services and File Systems storage. Posey is a former cIO for a national chain of hospitals and health care companies. Write to him at [email protected].
it is fully expected that an organization’s backup requirements will evolve over time, so hiPaa auditors will look for the plan to be updated regularly.
13 vIRTuAl DATA cEnTER E-zInE MARcH 2011
10 lines between bottom base of deck and first base of text
Drop cap is 5 lines
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
I
Lessons Learned: Virtualization Case Studiesthree health Care ProviDers DisCuss the uPs anD DoWns of server virtualization. first lesson: the Work Doesn’t enD after you’ve ConsoliDateD the server room. By eLISaBetH HoRWItt
n February 2010, Mount Sinai Medical Center was in the early stages of rolling out a VMware-based virtualized server infrastruc-ture. Asked at the time when she
expected the project to be completed, Vice President of IT Lynn Kasner Mor-gan replied, “Never.”
For health care organizations, many of which are late adopters of the tech-nology, server virtualization is very much an ongoing effort and learn-ing experience, IT experts say. Even pioneers who virtualized years ago must continue to make changes and additions—sometimes fundamental ones. The changes come in response to new applications, changing capac-ity demand and evolving technology, as well as to business changes within their organization and the health care industry, such as disaster recovery and health information exchange.
The following case studies trace the progress of health care organizations
from the early stages of their virtual-ization projects to present-day opera-tions.
MoUnt sinai MEdiCaL CEntErMount Sinai Medical Center launched its virtualization project to save on data center real estate and energy, both of which are costly in New York City. Virtualization enabled the center to consolidate 150 physical servers into 11 physical servers housed in one rack, according to David Holloway, its senior director of IT operations.
The IT team is working with busi-ness users to determine which exist-ing and new applications are suited to running on a virtual server.
One stubborn issue is that a few medical application vendors even now don’t officially support VMware, Hol-loway said. Their products still can be virtualized, but if a problem develops, it’s up to the customer to prove the
14 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
application is at fault, rather than the virtualization platform, he added.
The next task for Mount Sinai’s IT staff is to prepare a process to de-termine the cost of a virtual machine based on the physical servers, storage capacity and licensing considerations.
nEw HanoVEr rEGionaL MEdiCaL CEntErNew Hanover Regional Medical Cen-ter in North Carolina began virtual-izing its servers on VMware six or seven years ago, making the medical center something of a pioneer in the health care industry.
Since then, the installation has un-dergone a series of major changes, according to Network Engineer Pacer Hibler. About four years ago, NHRMC brought in Citrix Systems Inc.’s Xen-App application virtualization platform. XenApp will work with VMware serv-ers, but NHRMC’s IT department de-cided to bring in Citrix XenServer, the hypervisor optimized to support Citrix virtual desktops and XenApp servers. Furthermore, the hypervisor comes free with XenApp, precluding the need to purchase more VMware licenses to support desktops, Hibler added.
A fair number of NHRMC’s servers remained unvirtualized until about three years ago, when several factors provided the incentive for a major buildout:
The organization was experienc-pp
ing rapid growth with several incoming projects that required additional server capacity.
Microsoft’s support for Windows pp
2000 was waning. “While we were bringing in a new server platform and getting rid of leg-acy products,” Hibler said, “we thought, ‘Why not virtualize those servers instead of buying more hardware and using more power and increasing the data center footprint?’”
The IT department was revamp-pp
ing NHRMC’s disaster recovery setup and saw the advantages of using virtualized images on backup devices, as opposed to having to do bare-metal reinstal-lations or in-place restorations.
At this point, about 80% of NHRMC’s applications, as well as its entire data center, are virtualized, enabling the organization to cut data center space and energy use pretty much in half, Hibler said. “Everything is humming along.”
Changes and additions these past few years have mainly been upgrades “to make sure there are no bottle-necks as we grow,” Hibler said. For its VMware servers, for example, the IT team replaced 1 Gbps network in-terface cards with Cisco’s Nexus 10 Gbps Fibre Channel over Ethernet Cisco Network Assistant cards.
Not that the job is done now. NHRMC continues to deal with re-source allocation and chargeback models, particularly because it con-tinues to provide IT services to a growing number of small hospitals and practices in the Wilmington, N.C.,
15 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
area. “For some of our clients, we run just one application, but for others, we provide 100% of their IT services,” Hibler said.
The medical center currently charges a one-time fee, based on the number of users of a given server. Down the road, however, the center will probably need a more precise usage model that would monitor re-source utilization for each client and charge accordingly, Hibler said.
okLaHoMa artHritis CEntErWhen Josh Randels took over as di-rector of IT at Oklahoma Arthritis Center last May, he inherited a five-month-old virtualized server and desk-top environment that worked overall but badly needed some trimming.
His predecessor, Chris Nelson, built redundancy and extra capacity into the underlying infrastructure in the form of a Dell EqualLogic storage area network (SAN) and three Dell PowerEdge Servers. “[It] was kind of overkill, but it left us a lot of room to grow,” Nelson said.
Randels agreed with the overkill as-sessment, but not necessarily with the need to grow. One of the first things he did was sell the SAN. “It was very expensive, with a lot more disk storage space than we needed,” he said.
More importantly, I/O couldn’t keep up with demand, particularly from database applications. “Our per-formance logs showed constant de-lays,” Randels said. Virtualized servers now have dedicated storage until such
time as IT can find a suitable SAN with higher I/O and a lower price tag.
Randels also has eliminated a large number of applications that he con-siders low-value or unnecessary, “so that core applications can function at the highest level possible.” For exam-
ple, too much management software was slowing down the center’s net-work. Four management applications have been jettisoned. “With only 50 users, we really don’t need them,” he said.
On the virtual desktop side, OAC now uses Citrix Systems’ XenDesktop to complement VMware View. The Citrix platform handles wide-area connections and such USB devices as scanners and microphones quite well, Randels said. On the other hand, VMware does a better job of desktop provisioning and management.
Randels also has consolidated OAC’s six server hardware platforms
“With technology constantly evolving and improving, if you don’t stay on top of it all, your it infrastructure can become obsolete very quickly.”Josh ranDels, director of IT, Oklahoma Arthritis Center
16 vIRTuAl DATA cEnTER E-zInE MARcH 2011
eDitor’s letter
7
Why health Care server
virtualization is Different
7
Planning for virtualizeD
Disaster reCovery in health Care
7
lessons learneD:
virtualization Case stuDies
7
into four, one of which supports vir-tual desktops. In doing so, OAC has seen additional energy savings and heat reduction.
Another major goal is finding a low-cost, peripheral component intercon-nect, or PCI, Express SAN that uses solid-state drives. “Solid-state perfor-mance is massive compared to a tra-ditional hard drive,” Randels said.
Faster disk access is crucial to meet escalating demand from OAC’s data-bases and newly virtualized desktops. “That will complete the whole loop, and we’ll be pretty much in a good place,” Randels added.
Asked if this meant the project would be complete at that point, Ran-dels replied, “I wish! With technology constantly evolving and improving, if you don’t stay on top of it all, your IT infrastructure can become obsolete very quickly.” p
ELisaBEtH Horwitt is a freelance writer based in Waban, Mass., who covers such IT topics as infor-mation security, disaster recovery, business intel-ligence and health care information technology. Write to her at [email protected].
Linda kouryDirector of Online Design
Elisabeth HorwittBrien Posey
contributing Writers
Jean derGurahianExecutive Editor
Brian EastwoodSite Editor
anne steciwAssistant Site Editor
don FluckingerFeatures Writer
rachel LebeauxAssistant Managing Editor
For saLEs inQUiriEs
stephanie CorbyAssociate Publisher
[email protected](617) 431-9354
TechTarget275 Grove Street
newton, MA 02466 www.techtarget.com
Server Virtualization Strategies for the Health IT Pro is produced by Health
care IT Media, © 2011 by TechTarget.
randels consolidated oaC’s six server hard-ware platforms into four for additional energy savings and heat reduction.
RESOURCES FROM OUR SPONSOR
See ad page 3
• Best Practices for Server Virtualization in Mission-Critical Healthcare IT
• eBook: 5 Questions to Ask About Server Virtualization and High Availability
• Columbia Memorial Case Study
About Stratus Technologies:Stratus Technologies delivers uptime for the applications its customers depend on most fortheir success. With its ultra-reliable servers, software and services, Stratus products help tosave lives and protect the business and reputations of companies, institutions, and governmentsthe world over.
With hundreds of installations in hospitals, clinics and physician practices, Stratus providesaward-winning uptime solutions to support the demands of critical healthcare solutions acrossthe globe. From our fault-tolerant ftServer systems to our high-availability Avance software, weoffer plug and play solutions that maximize uptime for critical EHR applications.
With every Stratus availability offering, you benefit from superior uptime for traditional andvirtualized environments, no data loss, reduced IT complexity and lower support costs.
We build in the reliability so healthcare organizations can focus on what they do best: deliveringquality patient care.
Discover more about worry-free computing at www.stratus.com/go/healthcare