1 1 improving the quality and value of health care friday, may 30, 2008 national association of...
TRANSCRIPT
1 1
Improving the Quality and Value of Health Care
Friday, May 30, 2008
National Association of Insurance Commissioners Summer Meeting
Health Innovations (B) Working Group
San Francisco, CA
Applying What Works Best
A Health Plan’s View
Steven Halpern, MD
CIGNA HealthCare

2 2
The Problems that Health Plans are Trying to Solve and the Solutions They Provide
• Problem: Fragmentation and under-delivery of evidence-based care in the health care system.
Solution:
– Disease and case management programs
– Gaps in care programs
• Problem: Wide variation in the performance (quality and total costs of care) of providers and the lack of competition on value (quality and total costs).
Solution:
– Consumer information on provider quality and costs
– Benefit incentives to seek high quality, low cost providers
– Pay for value
• Problem: Lack of individual incentives for health and wellness.
Solution:
– Health risk appraisals and health coaching programs
– Benefit designs that provide incentives for health lifestyles – e.g. Health risk appraisal participation, disease management participation, smoking cessation.

0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
Q -12
Q -10
Q -8
Q -6
Q -4
Q -2
Q 0
Q+2
Q+4
Q+6
Q+8
Q+10
Q+12
High Risk
Medium Risk
Low Risk Case Management
Centers of Excellence and
High Performing Specialists
Opportunity to mitigate cost exists
through earlierintervention
15-20% of employees drive 65-70% of costs, but that segment of employees is different every year
“A system that waits for disease and illness to occur can never be optimally effective. The logical strategy is to maintain people at the lowest or most appropriate level of health care use possible.” Dee Edington,Ph.D., Director, Health Management Resource Center, University of Michigan, as quoted in the Detroit News, April 2004.
Proactive vs. Reactive Approach Can Change Medical Cost Trend
$
Disease mgmtLifestyle Modification
Health Risk AssessmentsBiometric Screenings
Wellness

4 4
Disease Management Improving Outcomes and Driving Significant Savings
AdmissionRate
Reduction
MedicalCost
Savings*
Asthma
Diabetes
Cardiac
Low Back
Pulmonary (COPD)
Total:
9.0%
8.0%
15.9%
20.3%
5.0%
12.6%
5.7%
8.7%
16.5%
17.3%
10.0%
11.0%
Condition
• 7 – 12% improvement in clinical measures
• Behavioral screening identifies risk of depression in 37% of low back patients and 5-6% of diabetics and cardiac patients.
• 90% patient satisfaction across all plans
• 11% of medical cost savings for disease managed conditions.
A 2004 study published in Health Affairs validates Well Aware diabetes program quality improvements and cost savings.
* CIGNA BoB averages; actual customer experience will vary based on number of members with conditions and number of cases.
5 5
What Provider Information is Available to CIGNA Members Nationwide
• Hospitals - nationwide, for 29 most common admissions
– quality based on JCAHO, Leapfrog, CMS measures and risk-adjusted, all-payor, mortality and complication rates
– Risk-adjusted total hospital costs per admission
• Physicians - nationwide, for 21 most common specialists
– Quality based on NQF and/or AQA measures. Board certification and NCQA physician recognition
– Total episode cost – ETG groupers
• High tech radiology – nationwide, price transparency for CT, MRI and PET scans
• Ambulatory procedures – nationwide, price transparency for 16 most common ambulatory care procedures
• Pharmacy – nationwide, price transparency for all CIGNA pharmacy drugs – both employer’s cost and member’s cost
6 6
What is Provider Competition on Value (Quality and Total Cost of Care) Worth?
• Specialist physicians who are designated high value (approximately top one-third) consistently outperform average specialists
– 4-5% improvement in clinical quality indicators– 29% reduction in re-admission rates– 8-12% lower total medical costs
• Hospitals designated as high value (Centers of Excellence), approximately top one third, consistently outperform average hospitals.
– 30% fewer deaths– 28% fewer complications– 39% lower costs per admission

7 7
HospitalEstimated
Average Facility Cost Range
EstimatedAverage Out Of
Pocket Cost Range
Virginia Hospital Center ArlingtonPatient outcomes: Cost efficiency:
$5,994 - $10,995 $4,199 - $4,700
Washington Adventist HospitalPatient outcomes: Cost efficiency:
$10,995 - $15,997 $4,700 - $5,200
George Washington University HospitalPatient outcomes: Cost efficiency:
$17,199 - $23,269 $5,320 - $5,927
Washington Hospital CenterPatient outcomes: Cost efficiency:
$5,994 - $10,995 $4,199 - $4,700
Total Hip Replacement, 25 mile radius from zip code 20005
8 8
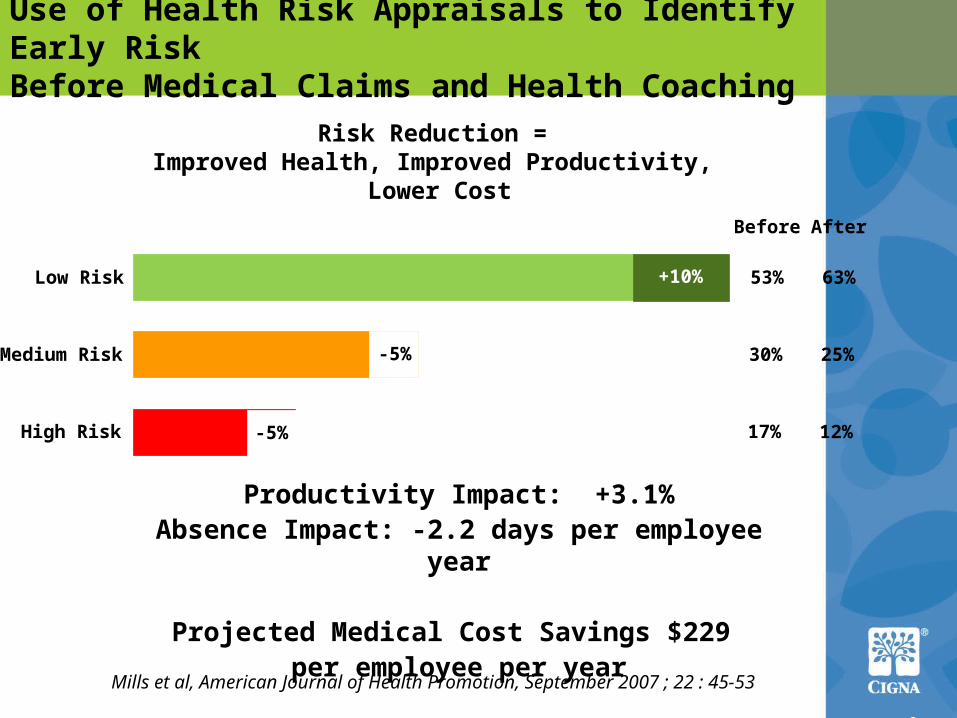
Low Risk
Medium Risk
High Risk
53%
30%
17%
Before
Risk Reduction = Improved Health, Improved Productivity, Lower Cost
Productivity Impact: +3.1%Absence Impact: -2.2 days per employee year
Projected Medical Cost Savings $229 per employee per year
Mills et al, American Journal of Health Promotion, September 2007 ; 22 : 45-53
Use of Health Risk Appraisals to Identify Early RiskBefore Medical Claims and Health Coaching
63%
25%
12%
After
+10%
-5%
-5%

9 9
Results from Health Savings and Reimbursement Plans, Plus Disease Management, Provider Transparency, and Health Coaching
Use of preventive care increased
First year visits increased
Second year visits remained higher than traditional
Use of Evidence Based Medicine was similar to traditional plans
Increase in use of maintenance medications that support chronic conditions
Total medical cost trends were lower for both first year and second year CDHP members
Member out-of-pocket costs were similar
First year members similar out-of-pocket costs
Second year CDHP out-of-pocket costs reduced for both HRA and HSA members
10 10
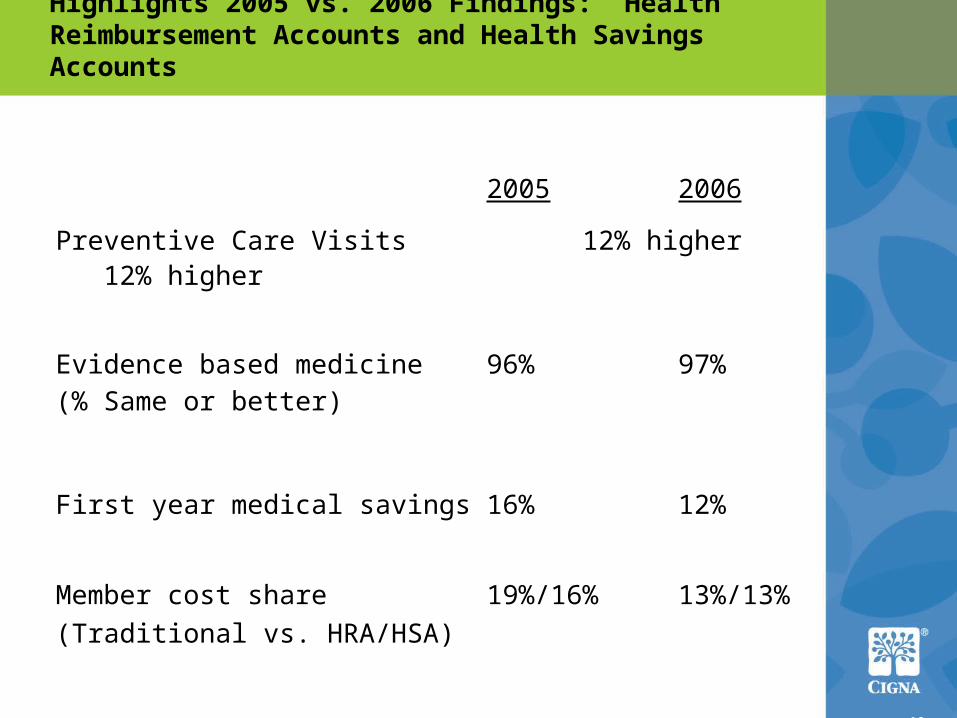
Highlights 2005 vs. 2006 Findings: Health Reimbursement Accounts and Health Savings Accounts
2005 2006
Preventive Care Visits 12% higher 12% higher
Evidence based medicine 96% 97%(% Same or better)
First year medical savings 16% 12%
Member cost share 19%/16% 13%/13%
(Traditional vs. HRA/HSA)
11 11
Barriers or Accelerators
• Barriers– Legislation or regulation that stifle transparency and
disclosure of consumer health information– Legislation or regulation that caps MLR (medical loss ratio)
that prevents health plans from performing added value services
– Limitations to the ability to offer wellness incentives
• Accelerants– Comparative effectiveness legislations– Multi-stakeholder data aggregation and profiling efforts– Health information exchange within HIPAA’s privacy and
security protections– A pathway for generic biologics and specialty drugs– Initiatives to encourage value-based purchasing within
public payors

12 12
Discussion