1. 2 adhd & behavioral challenges in tuberous sclerosis complex candida m. brown, md diablo...
TRANSCRIPT

1

2

ADHD & Behavioral Challenges in Tuberous Sclerosis Complex
Candida M. Brown, MDDiablo Valley Child NeurologyAn affiliate of Stanford Children’s Health Alliance
June 27th, 2015 3

Objectives• To review the genetics of TSC
• To review the neurologic presentation of TSC
• To discuss the cognitive and behavioral challenges of TSC
• To discuss potential treatments of behavioral disorders of TSC
4

Tuberous Sclerosis Complex
• A genetic condition with multisystem involvement
• Development of tumors and other abnormalities in multiple organs
• Incidence: 1:6000
5

Tuberous Sclerosis Genes
6
• 70% are new mutations
• 30% are familial and inherited in an Autosomal Dominant fashion

Tuberous Sclerosis Complex Genes
7
TSC1: hamartin
TSC2: tuberin

Tuberous Sclerosis Complex Genes
8

Tuberous Sclerosis Presentation
20
Cardiac
Renal
Cerebral
Skin
Lungs
800 40 60
Courtesy of Dr. Stephen Ashwal, Loma Linda University School of Medicine

Tuberous Sclerosis Presentation
10
• Causes hamartomas in various organs: brain, skin, kidneys and heart
• Harmartoma= group of abnormally formed, disorganized cells within an organ with some growth potential

TSC Neurologic Manifestations• CNS involvement is a hallmark of the disease,
and is seen in 95% of affected individuals – Infantile spasms– Partial seizures, often multifocal, independent (80%)– Cognitive Delay/Learning Problems (50%)– Autistic Spectrum Disorder– Behavior/Psychiatric Comorbidities (anxiety, depression)– Sleep disturbances
11

TSC Neurologic Manifestations• Intelligence correlated with seizure frequency & type• Outcome poorer with infantile spasms• Greater numbers of tubers associated with lower IQ• Brain Malformations (hemimegancephaly)• Cortical tuber• Subependymal nodule (88-95%)• Giant cell astrocytoma (5-15%)• White matter radial migration lines
12

Cortical tubers
13
1. Subependymal nodules 2. Cortical tubershttp://www.socialstyrelsen.se/rarediseases/tuberoussclerosis
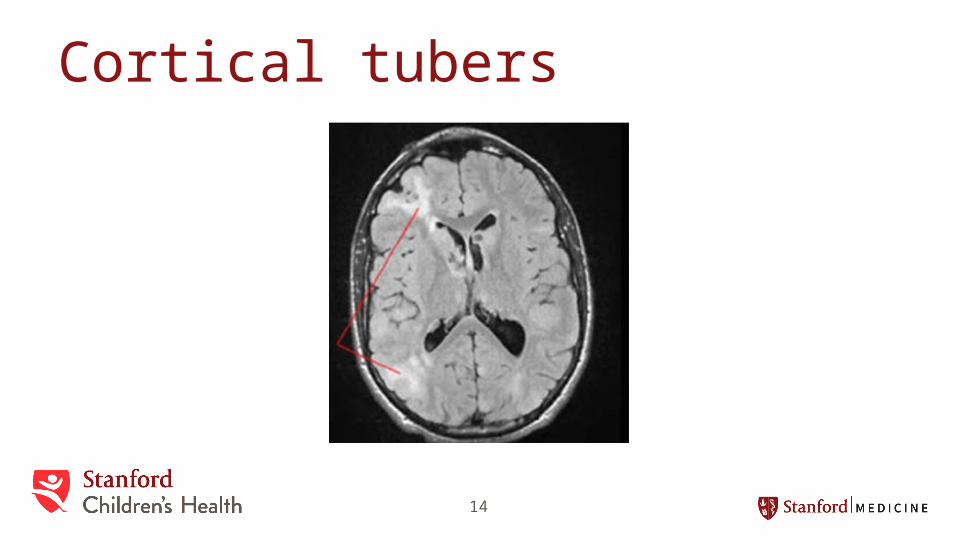
Cortical tubers
14
Diagnosis, Screening & Clinical Care of Individuals with TSC, published by the Tuberous Sclerosis Alliance.

Subependymal Nodues
Diagnosis, Screening & Clinical Care of Individuals with TSC, published by the Tuberous Sclerosis Alliance.

Subependymal Giant Cell Astrocytoma (SEGA)
16
Courtesy of David Franz, MD, Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio, USA

White Matter Radial Migrational Lines
http://www.biomedsearch.com/attachments/00/19/88/10/19881070/IJRI-19-135-g018.jpg
17

Hemimegancephaly
18
Role of MRI in Epilepsy in Radiology Assistant, NeuroradiologyLaurens De Cocker, Felice D'Arco and Philippe Demaerel and Robin Smithuis

Pathology of tubers and SEGAs
19
Hum. Mol. Genet. (15 October 2005) 14 (suppl 2): R251-R258. doi: 10.1093/hmg/ddi260

Cognitive and Behavioral Difficulties in TSC
20
November 2011 | Vol. 23 No. 4 | Annals of Clinical 268 Psychiatry

Cognitive and Behavioral Difficulties in TSC• ADHD• Autistic spectrum disorder• Aggression, rage outbursts and temper tantrums• Negativity (temporary resistance to change)• Emotional lability• Depression• Anxiety and OCD• Sleep disorders• Epilepsy-related psychotic disorders
21

Cognitive and Behavioral Difficulties in TSC• Global cognitive deficits: intellectual delay and learning
disabilities• Receptive and expression language delays• Social-communication deficits• Attentional deficits: selective attention, sustained attention
and attention switching• Executive deficits: planning, poor sequencing, perseveration• Memory deficits: working memory and episodic memory• Motor deficits: Fine motor, gross motor and movement
disorders
22

Cognitive and Behavioral Difficulties in TSC• Correlation between seizures and
neuropsychiatric comorbidities, including ADHD and ASD
• Cortical tubers in temporal and insular areas play a significant role in TSC patients with ASD
• Higher prevalence of cystic-like tumors in patients with TSC and ASD
23
Huang C-H, et al., The relationship of neuroimaging findings and neuropsychiatric comorbidities inchildren with tuberous sclerosis complex, Journal of the Formosan Medical Association (2014), http://dx.doi.org/10.1016/j.jfma.2014.02.008

• Temporal lobe associated with:– Social perception– Language
• Insular cortex associated with:– Interoceptive processes– Affective processes– Empathy
• Clear association between ASD and TSC2 missense mutations
• Tuber count: controversial: – History of infantile spasms– Higher tuber burden– Early age of onset of seizures
24
Cognitive and Behavioral Difficulties in TSC• ADHD
• Autistic Spectrum Disorder
• Mood disorder: anxiety, OCD and aggressive behaviors
• Sleep disruption
25

Attention Deficit Hyperactivity Disorder• ADHD-Inattentive Type
• ADHD-Hyperactive Type
• ADHD-Combined Type
26

Attention Deficit Hyperactivity Disorder• Inattention
• Hyperactivity
• Impulsivity
27

• Inattention– Be easily distracted, miss details, forget things, and frequently switch from
one activity to another– Have difficulty focusing on one thing– Become bored with a task after only a few minutes, unless they are doing
something enjoyable– Have difficulty focusing attention on organizing and completing a task or
learning something new– Have trouble completing or turning in homework assignments, often losing
things (e.g., pencils, toys, assignments) needed to complete tasks or activities
– not seem to listen when spoken to– Daydream, become easily confused, and move slowly– Have difficulty processing information as quickly and accurately as others– Struggle to follow instructions.
28

Attention Deficit Hyperactivity Disorder• Hyperactivity
– fidget and squirm in their seats– talk nonstop– Dash around, touching or playing with anything and everything in sight– Have trouble sitting still during dinner, school, and
story time– Be constantly in motion– Have difficulty doing quiet tasks or activities.
29

Attention Deficit Hyperactivity Disorder• Impulsivity
– Be very impatient– Blurt out inappropriate comments, show
their emotions without restraint, act without regard for consequences
– Have difficulty waiting for things they want or waiting their turns in games
– often interrupt conversations or others’ activities.
30

Attention Deficit Hyperactivity Disorder• Incidence in TSC patients: 30-60%
• Causes hypothesized:
– Localization of CNS lesions in associative areas
– Comorbidity with epilepsy– Comorbidity with ASD and intellectual
disabilities (60%)
31

• Diagnosis– Based on history provided by the
patient, parents and teachers– Several different tools available• Vanderbilt ADHD Diagnostic Rating Scales• Connor Questionnaire
32

Attention Deficit Hyperactivity Disorder• Treatment
– Behavioral• Schedule
– Keep the same routine every day, from wake-up time to bedtime. Include time for homework, outdoor play, and indoor activities. Keep the schedule on the refrigerator or on a bulletin board in the kitchen. Write changes on the schedule as far in advance as possible.
• Organize everyday items– Have a place for everything, and keep everything in its place. This includes clothing,
backpacks, and toys.• Use homework and notebook organizers• Stress to your child the importance of writing down assignments and bringing
home the necessary books.• Be clear and consistent
– Children with ADHD need consistent rules they can understand and follow.• Give praise or rewards
– Children with ADHD often receive and expect criticism. Look for good behavior, and praise it.
33

Attention Deficit Hyperactivity Disorder• Medications:
– Derivatives of Ritalin an Dexedrine• Ritalin (amphetamines: Concerta, Focalin)• Dexedrine (methylphenidates: Adderall, Vyvanse)• Common side effects:
– Decreased appetite– Sleep difficulties– Mood lability
– Non-stimulants (Strattera)• Common side effects:
– GI distress
– Alpha adrenergic agonists• Clonidine, guanfascine (Intuniv, Kapvay)• Sleepiness
– Other therapies• Buproprion• Imipramine• Nortriptyline
34

Autistic spectrum disorder• Diagnostic criteria:– Impairment in social communication
function
– Presence of restricted, repetitive patterns of behaviors or interests
35

Autistic Spectrum Disorder• Impairment in social
communication function– Deficits in social-emotional reciprocity– Deficits in non-verbal communication– Deficits in developing, maintaining and
understanding relationships
36

Autistic Spectrum Disorder• Restricted, repetitive patterns of behavior,
interests or activities, as manifested by at least two of the following:– Stereotyped or repetitive motor movements– Insistence on sameness, inflexible adherence to
routine or ritualized patterns of verbal or non-verbal behaviors
– Highly restricted, fixated interests that are abnormal in intensity or focus
– Hyperactivity or hypo-activity to sensory input or unusual interest in sensory aspects of the environment
37

Autistic Spectrum Disorder• Treatment:– Behavioral: Applied Behavioral Analysis (ABA)– Medications:
• Only FDA-approved medications for ASD are the atypical antipsycholitcs– Respiridone (Respirdal) and ariprazole (Abilify)– Approved for the treatment of irritability: physical
aggression and tantrum behaviors
38

Mood disorders• Anxiety and OCD without or with depression
(16%)– Anxiety: a feeling of worry, nervousness, or unease, typically about an
imminent event or something with an uncertain outcome– Obsessive Compulsive Behaviors: repetitive thoughts or the need to do
behaviors that help to alleviate anxiety
• Aggressive behaviors due to mood regulation issues (37%)– Aggression toward others: hitting, biting, kicking– Self-injurious behaviors: hitting self, head banging– Fight risk: bolting
39

Mood disorders• Applied Behavioral Analysis
• Cognitive Behavioral therapy– Anxiety– Depression– OCD
• Medications
40

Sleep disruption• Most common sleep problem in children with ASD is insomnia, or lack of sufficient sleep• Typical patterns:
– Delayed sleep onset– Maintenance of sleep
• Prevalence in ASD: 53-78%– Look for causes: GI (reflux) and pulmonary (apnea)
– Behavioral interventions• Keeping a bedtime routine and schedule• Quieting activities prior to bedtime• Limiting daytime naps
– Medication interventions• Melatonin• Benadryl• Clonidine• Trazadone
41

Medications commonly used to treat patients with TSC:• Based on the study of “Psychiatric Comorbidity
and Treatment Response in Patients with TSC” (Annals of Clinical Psychiatry: Vol 23, No 4, November 2011, pp. 263-69)
42

Medications commonly used to treat patients with TSC:• Antipsychotics:
– Risperidone (30/46, 65.2%)– Quetiapine (10/32, 59.4%)– Ariprazole (7/10, 70%)– Haloperidol (0/1, 0%)– Olanzapine (2/3, 66.7%)– Perphanazine (1/1, 100% )– Metirosine (0/1, 0%)– Pimozide (1/2, 50%)
43

Medications commonly used to treat patients with TSC:• Antidepressants:
– Escitalopram (16/38: 42.1%)– Buproprion (8/10, 80%)– Citalopram (2/2, 100%)– Fluoxetine (3/5, 60%)– Venlafexine (0/2, 0%)– Amitriptyline (7/10, 70%)– Trazodone (0/1, 0%)– Doxepin (0/1, 0%)– Impipramine 1/1, 100%)
44

Medications commonly used to treat patients with TSC:• Mood stabilizers:– Lithium (2/2, 100%)– Lamotrigine (14/18, 77.8%)– Oxcarbazepine (11/14, 78.6%)– Valproic Acid (16/23, 69.3%)
45

Medications commonly used to treat patients with TSC:• Alpha-adrenergic agonists:– Guanfacine (2/5, 40%)– Clonidine (1/5. 20%)
46

Medications commonly used to treat patients with TSC:• Anxiolytics:– Lorazepam 10/14 (71.4%)– Clonazepam 0/2 (0/2, 0%)– Chordiazepoxide (0/1, 0%)
47

Medications commonly used to treat patients with TSC:• Other:
– Naltrexone (2/2, 100%)– Sirolimus (1/1, 100%)– Everolimus (2/2, 100%)
48
Medications commonly used to treat patients with TSC:• Total:
– 73/113 (64.6%)
49

Summary• Tuberous Sclerosis Complex is:– AD inherited disorder– Due to mutations in the TSC1 or TSC2 genes– Affects the inhibition of cell growth resulting in
hamartomas of various organs
50

Summary• The most common behavioral
presentations in the order of severity are:– Behavioral disorders (37%)– Autistic spectrum disorders (24%)– Anxiety disorders (16%)– ADHD (13%)
51

Summary• Treatment may include:
– Behavioral therapy• Applied Behavioral Analysis• Behavioral techniques for ADHD• Cognitive Behavioral Therapy (CBT) for anxiety, OCD and depression
– Medications• Antipsychotics• Antidepressants• Mood stabilizers• Stimulants• Alpha-adrenergic agonists• Anxiolytics• Other medications
52
The End
53