1-800-411-pain referral service, llc - … · 1-800-411-pain referral service, llc ... enclosed...
TRANSCRIPT

1-800-411-PAIN REFERRAL SERVICE, LLC2544 N. STATE ROAD 7 (441), HOLLYWOOD, FLORIDA 33021
PH#: 954-963-1899 FAX#: 954-963-5613
September 27, 2012
Tameika GainousAdministrative SecretaryLawyer RegulationThe Florida Bar651 Jefferson StreetTallahassee, FL 32399-2300
Dear Ms. Gainous,
Enclosed please find our quarterly submission for the quarter ending September 30, 2012.
I have also enclosed a copy of the letter you sent me, dated July 9, 2012, regarding our quarterlysubmission for quarter ending June 30, 2012. I had listed, incorrectly, the law firm of Prieto, Prieto &Goen under Florida Bar No. 192137. I have fixed this entry on this submission. The correct law firm isPreito, Prieto & Goan. I have listed the attorneys on this submission individually, along with theircorrect Florida Bar number. And please not I have corrected the last name of attorney Goan.
Also, for the law firm Morgan and Morgan out of Tampa, Florida. I have attached their insurance Decpage, along with a list of the attorneys in that firm, and their Florida Bar numbers. I have also includedthem on my quarterly report, but I wanted you to know which attorneys are associated with that firmsince it is a large list.
have any questions please do not hesitate to call me at 954-963-1899.
rds.
Fogaros1-800-411 Pain Referral Service, Inc.
Enclosures
cc: Tim Chinaris
Lawyer Referral Service
SEP 2 8
RULE 4-7.10 (LAWYER REFERRAL SERVICE)
This form is submitted pursuant to Rule 4-7. 10 of the Rules Regulating The Florida Bar for thequarter ending ^\ ?£)( I>OUX • I hereby certify the following:
_ 1 . The names and bar numbers of all attorneys associated with the lawyer referralservice is attached as Exhibit "A"; and
_ 2. This service only refers clients to persons lawfully permitted to practice law inFlorida when the services to be rendered constitute the practice of law in Florida; and
_ 3 . This service carries or requires each lawyer participating in the service to carrym~an~affl
Date
Name of Referral Service \ ~^^>~ HA VRepresentative^Print Name
nifte-(C~— —•'
Address ag"MM M • ^Vc\.V^ "%A-~"l VWKM&kft APhone Number C^vy-O^b "l\A°l • ^>
Please furnish contact information if different than listed above.
Contact NameAddresPhone
Return to: The Florida BarAttention: Tameika Gainous, Lawyer Regulation651 East Jefferson StreetTallahassee, Florida 32399-2300
If you have any questions, please contact Tameika Gainous at (850) 561-5753 or [email protected]

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
L- PAWN
vcio.iV
tuv u S -
^^ L-

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
fy^OMx £y\MV\ <\cicl'Sri^
1WCt—
jM O nvsM ts*
Giru V
o \ I co
W\ 0
\?
n
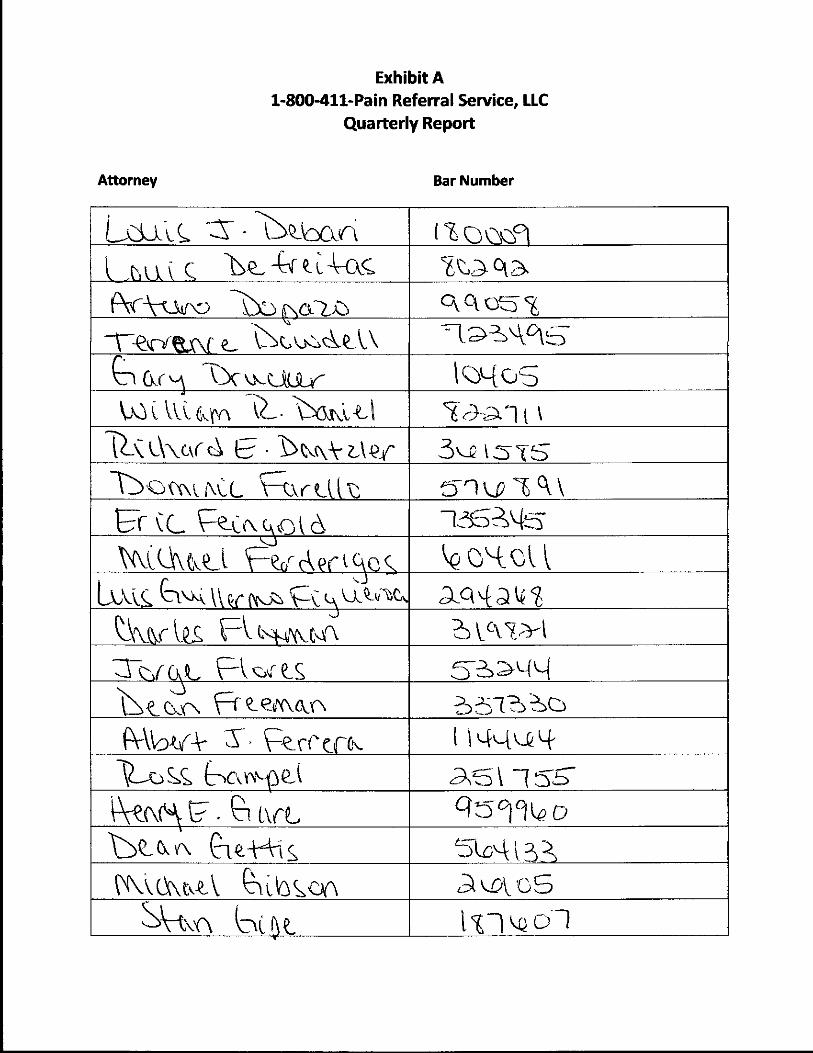
Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
1 0)4 o
3"-

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
\Sst-ian'5-
SUOM

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
v 11 \ a rw !>• VWoa r100
fV\.4>H d o
UC-W 1Q141
\Cc\u \
lo

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
4
T-
1 n i a-n
(WaH-S
a i

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
(Wcm
M
c\
IL MVvaiY\
34^ (1o
52OIO5411^7
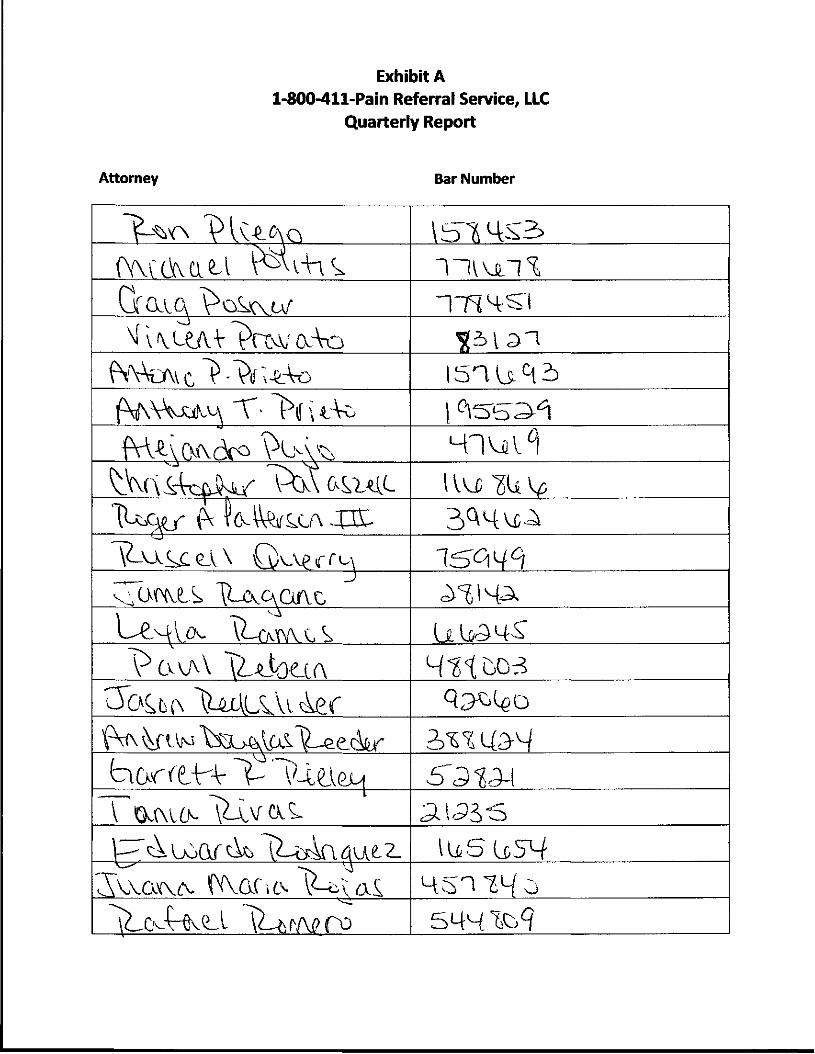
Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
^3
T-
4^03
bar f t-K-\

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
to
(V-A

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
P ? v rt-4 vxxx\
o 0( (V H^
an L-

Exhibit A1-800-411-Pain Referral Service, LLC
Quarterly Report
Attorney Bar Number
IY
(\\L\\ oVa^
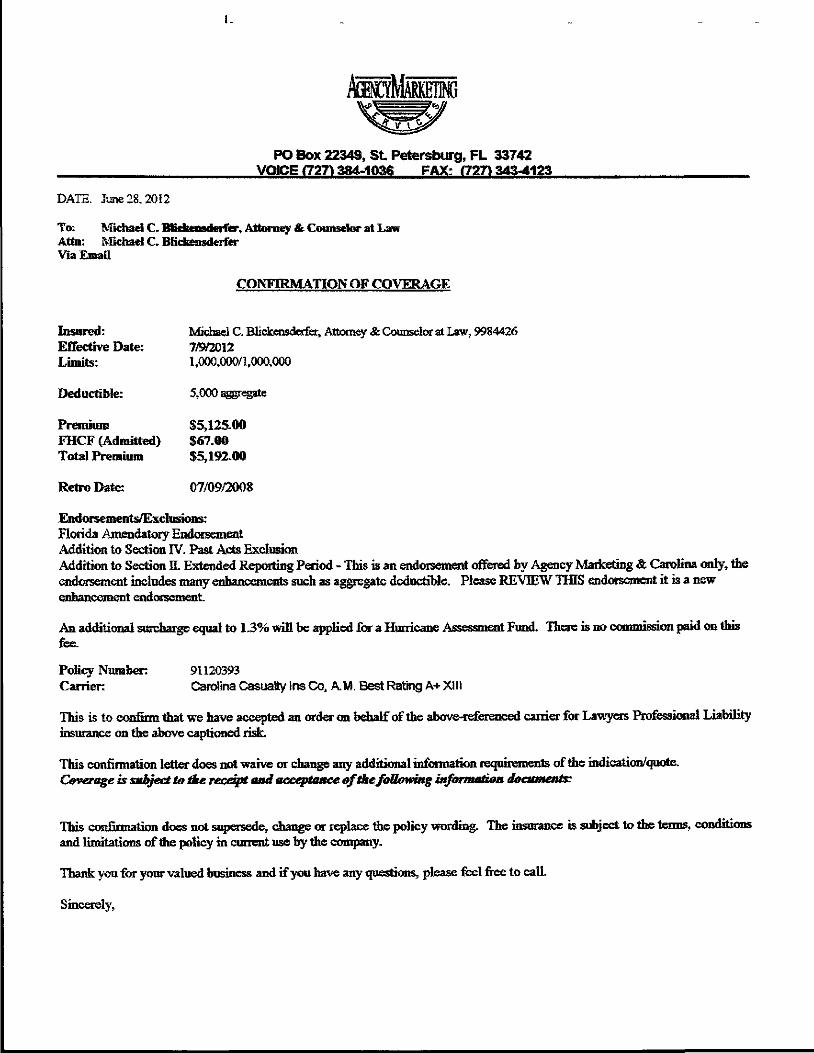
PO Box 22343, St Petersburg, FL 33742VOICE (727) 384-1036 FAX: f7271 343-4123
DATE. June 28,2012
To: Michael C. Blidwnsderfer, Attorney & Counselor at LawAtta: Michael C. BiickensderferVia Email
CONFIRMATION OF COVERAGE
Insured: Michael C. BHekensderfesr, Attorney & Counselor at Law, 9984426Effective Date: 7/9/2012Limits: 1,000,000/1,000,000
Deductible: 5,000 a^regale
Premium $5,125.00FHCF (Admitted) $67.00Total Premium $5,192.00
Retro Date: 07/09/2008
Endorsements/Exclusions:Florida Amendatory EndorsementAddition to Section IV. Past Acts ExclusionAddition to Section EL Extended Reporting Period - This is an endorsement offered by Agency Marketing & Carolina only, theendorsement includes many enhancements such as aggregate deductible. Please REVIEW THIS endorsement it is a newenhancement endorsement
An additional surcharge equal to 1.3% will be applied &r a Hurricane Assessment Fund. There is no commission paid on thisfee.
Policy Number. 91120393Carrier: Carolina Casualty Ins Co, A. M, Best Rating A+ X! 11
This is to confirm that we have accented an order on behalf of the above-referenced carrier for Lawyers Professional Liabilityinsurance on the above captioned risk.
This confirmation letter does not waive or change any additional information requirements of the indication/quote.Coverage is subject to tke receipt and acceptance of thefoUowwg information documents:
This confirmation does not supersede, change or replace the policy wording. The insurance is subject to the terms, conditionsand limitations of the policy in current use by the company.
Thank you for your valued business and if you have any questions, please feel free to call.
Sincerely,

CATA&CA-01 MARLANDA
~£2*Kg^ CERTIFICATE OF LIABILITY INSURANCE "ISSTTHIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NX) RIGHTS UPON THE CERTIFICATE HOLDER. THJSCERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIESBELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING 1NSURER(S), AUTHORIZEDREPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER.IMPORTANT: If the certificate holder is an ADDITIONAL INSURED, ththe terms and conditions of the policy, certain policies may require an e
PRODUCER
Insurance Office of America, Inc.P.O. Box 162207Attamonte Springs, FL 32716-2207
INSURED
Catania & Catania PA101 E Kennedy BlvdSte 2400Tampa, FL 33602-5187
e poticyfies) must be endorsed. If SUBROGATION IS WAIVED, subject tondorsement A statement on this certificate does not confer rights to the
SSSe01 Andrea MarlandSC"&E«* (800) 243-6899 | f<£. ** (407) 788^933ADDRESS: [email protected]
INSURERS) AFFORDING COVERAGE
msuRERA:Otd Dominion Insurance CompanyINSURER B: Owners Insurance CompanyINSURERC :Southern-Qv«iers Insurance CompanyINSURER o: Zenith Ins CoINSURER E : Colony Insurance CompanyINSURER?:
NAK#4023132700101901326939993
COVERAGES CERTIFICATE NUMBER: REVISION NUMBER:THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIODINDICATED. NOTWITHSTANDING ANY REQUIREMENT, TERM OR CONDITION OF ANY CONTRACT OR OTHER DOCUMENT WfTH RESPECT TO WHICH THISCERTIFICATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIES DESCRiBED HEREIN IS SUBJECT TO ALL THE TERMS,EXCLUSIONS AND CONDITIONS OF SUCH POLICIES. LIMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS.
TYPEOF INSURANCE IH5R jsxa POLICY NUMBER larrsGENERAL UABUTY
COMMERCIAL GENERAL LIABILITY
OCCUR
EACH OCCURRENCEBPG80334 9/1/2012 9/1/2013 PREMISES <Ea eeeuiranort
UEDEXP(Anyonepereofi)
PERSONAL & AW INJURY
GENERAL AGGREGATE
PRODUCTS-COMP/OP AGG
1,000,000500,000
5,0001,000,0002,000,0002,000,000
AUTOMOBILE LIABILITY SI MGLE LIMIT 1,000,000ANY ALTOALL OWNEDAUTOS
WREO AUTOS
4196054101 1/1/2012 1/1/2013 BOOO.Y INJURY (P«r person]
SCHEDULEDAUTOSNOHOWNEDAUTOS
BODB.Y INJURY (P<racdd«rt)
PROPERTY DAMAGE(Peracddent)
UMBRELLA 1MB
EXCESS UAB
OCCUR
CLA1MS4IAOE
EACH OCCURRENCE 5,000,000*1960S4108 9/1/2012 9/1/2013 ASGSEGATE
PEP RETENTIONS 5,000 5,000,000ADOK
AND EMPLOYERS' LIABILITY Y/K
TWCSTATU- II TORY LIMITS I
(UtatKtotoiylnNH)Wyes, describe undwASCRIPTION Of OPERATIONS iMtow
N/AZ836382814 10/1/2012 10/1/2013 6.LEACHACCJDENT 100,000
E.L DISEASE - EA EMPLOYEE 100,000E.L DISEASE-POLICY UMIT 500,000
E General Liability EO406375 7/2W2012 7/28/2013 Perdaan 1,000,000
DeSCMPTIOHOfOPERATIOMS/LOCATIONS/Vl
CERTIFICATE HOLDER CANCELLATION
Florida InjuryAttn: Judy Lopez6220 S Orange Blossom Trail Suite 196lOriando.FL 32809
SHOULD AMY OF THE ABOVE DESCRIBED POLICIES BE CANCELLED BEFORETHE EXPIRATION DATE THEREOF. NOTICE WILL BE DELIVERED INACCORDANCE WITH THE POLICY PROVISIONS.
AUTHORREO REPRESENTATIVE
ACORO 25 (2010/05)
© 1988-2010 ACORD CORPORATION. All rights reserved.The ACORD name and logo are registered marks of ACORD

Lawyers Professional Liability InsurancePolicy Declarations
Darwin National Assurance Company Policy Number 0304-8196
Main Administrative Office Address:9 Farm Springs RoadFarmington, CT 06032
Corporate Address:1807 North Market StreetWilmington, DE 19802
THIS IS A CLAIMS MADE POLICY WHICH APPLIES ONLY TO CLAIMS RRST MADE DURING THEPOLICY PERIOD OR ANY EXTENDED REPORTING PERIOD, AND REPORTED IN ACCORDANCEWITH SECTION IV.L OF THE POLICY. THE LWIT OF LIABILITY AVAILABLE TO PAY DAMAGESWUJL BE REDUCED AND MAY BE EXHAUSTED BY CLAIMS EXPENSES AND CLAIMS EXPENSESWILL BE APPLIED AGAINST THE RETENTION AMOUNT. IN NO EVENT WILL THE INSURER BELIABLE FOR CLAIMS EXPENSES OR DAMAGES IN EXCESS OF THE APPLICABLE LIMIT OFLIABILITY. PLEASE READ THE ENTIRE POLICY CAREFULLY.
Item 1. Name and Maiing Address of Named Insured:
Pawlowski & Brewer, PA1718 East Tlh Avenue, Suite 201Tampa, FL 33605
Item 2. Policy Period:
Inception Date:Expiration Date:
July 23,2012July 23, 2013At 12 1 AM Standard Time at the Mailing Address shown above
Item 3. Limit of Liability {inclusive of Claims Expenses):
(a) $1,000,000 maximum limit of liability per CLAIM
(b) $1,000,000 maximum aggregate limit of liability for ail CLAIMS
Hem 4. Retention:
$20,000 each and every CLAIM
Hern 5. Notices required to be given to the Insurer must be addressed to:
For Notice of Claims and Circumstances:[email protected]
For AH Other Notices:9 Farm Springs RoadFamnington, CT 06032
item 6. Premium:
Total Premium: $6,252
FHCF1.30% $81.28
DRWN E4405 (9/2008)
Item 7. Retroactive Date:
June 1,1996
item 8. Endorsements Attached at Issuance:
1. e1032 (06/2009) Florida State Amendatory2. v2115 (05/2009) Privacy Wrongful Acts Coverage, With Notice And Credit Monitoring Costs3. v2671 (01/2011) Omnibus Endorsement
THESE DECLARATIONS, THE POLICY FORM, ANY ENDORSEMENTS AND THE APPLICATIONCONSTITUTE THE ENTIRE AGREEMENT BETWEEN THE INSURER AND THE INSURED RELATINGTO THIS INSURANCE.
In Witness Whereof, the Insurer has caused this Policy to be executed by its authorized officers.
SECRETARY PRESIDENT
AUTHORIZED SIGNATURE
Licensed Agent License Number
if the policyholder wishes to present inquiries or obtain information about coverage or to provideassistance in resolving complaints, please contact Darwin Professional Underwriters at {860} 284-1300.
DRWN E4405 (9/2008)

SEP-12-E012(BED3 13:55 SRUCHULfl STflTE BflNK P. 002
Century Surety Company465 CleveJond Avenue
*Jxtttusyivntr.c a
POUWI«J.:CCP 78tt59
3705 N HiMESAVE_.,,_. «TAMPA FL
CQWHWOMPOUCY DECLARATIONS !'Renewal of 1 CCF* 7229S3
• CODE Na:5ra8AJ; 11NSUREDS AGENT: i j•COMMONWEALTH JNSLRANC^ ACSBJCy LtGJCBrtN HARRINGTON S } "
3360? 144 HiTAICRRQAD, SUITE B
If S
iVSteneiara fime «t yo* maflin^address shown above. ;';Bi riass Desorifrtion: pFRCeajii 3CNff • • | | I s
QSidMfflial QJ««1«ft»ir»: OR*Ws*K» ©Uj«MU«)Kiy.cai»««(yW;O O**»nla^KiBte»^kB$ifa4$^^^
!!i !! ! ™^ l* ?^p|fffllfl^T 11? WM^CW«aS»fOPTfts^TOI W l»VBlAl >AimJ^WWOI PREMIUM IS INDICATED.
Oxntnefcial PiBj*ttJ3rCen»«6Qe Pact
insitmt*.K.^ -3JKJriKWBj
Romfal
;LtGa;Csmtttt!»_..._erfl».- |S 1Gtttrsarty-Aettotte
SwviceFee
EMPA
25 %oft»-P^yPf«niumfeftil eart!edasrfihB;e*fei Bdatetf_ihis pd.i jand .is not subject tcr return qr rafurxi.
TOTAL" I
"T'TFr.
iTWs:!I i:iPREWQPM
^OP" f f
i>i f
J
$3500S126J1D'•S2SS2$32%
MacNeJIJ Group^ inc.SunrtaS FL 33323
-ormC3}arH3BTdorsa7ient( madBa part of thte policy attime of issue*:OOb'C32 02
itai >ecmcC53VBrB8e.ponASj n^FormPcertfStlorRfe i -: I | : rAny.pcr *ho.i»jm»ilenttocleftm»dortoi3w .mathcfafe^^^(iocepHvsststement'Is guilty oilitsijni«eo!toiiij, * '— t ! i-
=«K,«nc.
Suite 0Sunrise FL $308/2012-
IKVWTOESSWHEREOF, thbCcnjpBnvrhwex«^edOT(l 8««^Uw^pPWents;to*bpo^•<toi>ntnffhte tVnin«>.v<« IKp, a~-ri Jfc.:.- >«rf>.~ »»aini.art ^ ' '--i' i* I I I I !
CSCP10010S03
<'
Jl
J
P99|tofl|

PREMIER BUSINESSOWNERS POLICY
Policy Number ACP BPOZ581S003404
PREMIER OFFICE
PROPERTY DECLARATIONS Policy Period:From 07-07-12 To 07-07-13
Description of Premises Number 001 Building Number: 001Premises Address 1*550 N DALE MABRY HWYOccupancy OO Classification: ATTORNEYS
Described as: ATTORNEYS - OFFICE-NO PL
Construction: FRAMELUTZ FL 23548-7900
WE PROVIDE INSURANCE ONLY FOR THOSE COVERAGES INDICATED BY A LIMIT OR BY HNCLUDEP*.
The Property Coverage provided at this premises is subject to a $2,500 Deductible, unless otherwise slated.COVERAGESBuilding- Replacement costBusiness Personal Property - Replacement cost
LIMITS OF INSURANCE$990,818*100,000
ADDITIONAL COVERAGES - the Coverage Fonn Includes other AAfiflonaf Coverages not shown.Business Income-ALS-12 Months-72 HourWaitingPeriod-60Day Ordinary Payroll LimitExtra Expense - Actual Loss Sustained {ALS} - 12 Months - 72 Hour Watting PeriodEquipment BreakdownAutomatic Increase in Insurance - BuildingAutomatic increase in Insurance - Business Personal PropertyBack Up of Sewer and Drain Water {limit shown per Building, subject to $25.000 policy aggregate)Appurtenant Structures -10% of Building Limit of Insurance - maximum $50,000 any one structure
INCLUDEDINCLUDEDINCLUDED
6*2.9%
45,000INCLUDED
OPTIONAL INCREASED LIMITS Included LimitAccount Receivable £25,000Valuable Papers and Records (At the Described Premises) $25,000Forgery and Alteration $10,080Money and Securities - inside the Premises $10,090
Outside the Premises (Limited) *10, 000Outdoor Signs $2,500Outdoor Trees, Shrubs, Plants and Lawns $10/000Business Personal Property Away From Premises $15,000Business Personal Property Away From Premises - Transit $15,000
Additional Limit$25,000$25,000$10,000•10,000$10,000#2,500010,000015,000*15,000
OPTIONAL COVERAGES - Otter frequently purchased coverage options.Employee DishonestyOrdinance or Law -1 - Loss to Undamaged Portion
2 - Demolition Cost and Broadened Increased Cost of ConstructionHurricane Deductible - PB5442 - 02%Sinkhole Loss Coverage
NOT PROVIDEDINCLUDED$198,164INCLUDEDINCLUDED
PROTECTIVE SAFEGUARDSThis premise has one or more PROTECTIVE SAFEGUARDS identified by symbols herein. Insurance at thispremise will be suspended if you do not notify us immediately if any of these safeguards are impaired.See PB 04 30 for a description of each symbol. APPLICABLE SYMBOLS: NOT APPLICABLE
PB 81 01 (01-01)
DIRECT HU- OSS WSURBiCOPY UKt 18
Page 1 of 2
SB M017
- 541 E'Mitchel1 Hammock Road • Oviedo, Florida 32765
S phone: 800-633'6458 *Fax:wwwJmic.com
I n s u r a n c e C o m p a n y , ,
Created by The Florida Bar for its members.
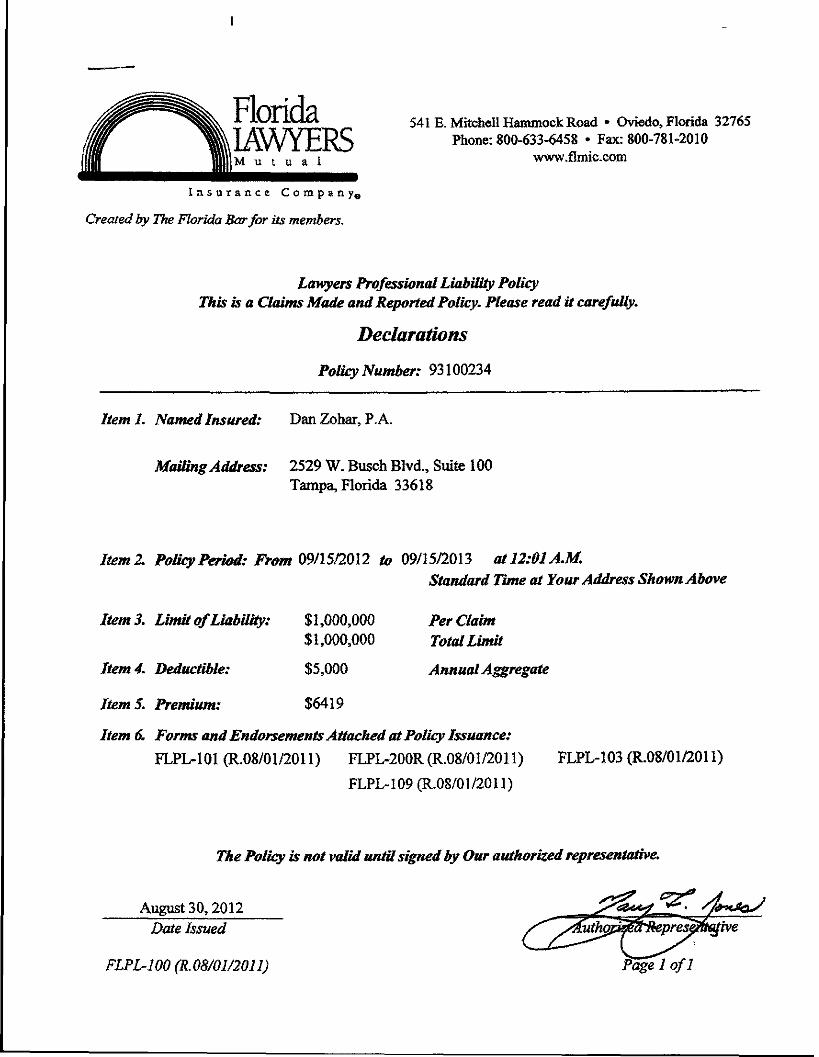
Lawyers Professional Liability PolicyThis is a Claims Made and Reported Policy. Please read it carefully.
Declarations
Policy Number: 93100234
Item I. Named Insured: Dan Zohar, P. A.
Mailing Address: 2529 W. Busch Blvd., Suite 100Tampa, Florida 33618
Item 2. Policy Period: From 09/15/2012 to 09/15/2013 at 12:01 AM,Standard Time at Your Address Shown Above
ItemS. Limit of Liability: $1,000,000 Per Claim$1,000,000 TotalLimit
Item 4. Deductible: $5,000 Annual Aggregate
Item 5. Premium: $6419
Item 6. Forms and Endorsements Attached at Policy Issuance:
FLPL-101 (R.08/01/2011) FLPL-200R (R.08/01/2011) FLPL-103 (R.08/01/2011)
FLPL-109 (R.08/01/2011)
The Policy is not valid until signed by Our authorized representative.
August 30,2012Date Issued
FLPL-100 (R.08/01/2011) Page 1 of I

CHARTISNational Onion Fire Insurance Company of Pittsburgh, Pa,*
175 Water Street
PROFESSIONAL LIABILITY POLICYPOLICY NUMBER; 018155544REPLACEMENT OF: 084151368
THtStSA CLAt8IS-!«ASe AftJ REPGfHHJ FQ» E.^-gpTTOSBCH EJCISfT &S5SAY OTOSSSKE BEPRQVifJHJTHECQyERASe OF THIS TOUCY !S G£ 'H4JT yiiSTEt) T0 UABiUTYKSR THOSE CiAJSSS THAT ARE
FtRSf MASS AfiAIMST INSU8EDS 0USRWS THE P0U< f>ER!OO AJ«3 f PCWtmj TO THE BSSURER AS THE POLICYREQUIRES. DEFSNSE COSTS I JOCE Tl« UWT OF OAaSLfTY, PJJEASE I«M> THE POUCY CAREFUttT AKDOlSOi tHE COVERAGE WJT« YOUR »»UISWICE ASQCr OR STOKER TO OETERMttie WHAT IS JW® WWAT IS NOT
pa^s^EQFFliSf
ADDRESS: 581 1 fnferrasriaJ H iwaySuaei04Tamp®. Ft 33615
it &. PRH)gC^SSQR_FfflaKaPOLICY PS^Oe
.(tieinception Date: 11/£r30t1 Exptafoa Oafec 1MJ2/2G1212:OljtA.M..gt the ay .; ess stated ifl Hero 1. above.
1? Narne acsd Address for Nbf3cs/£aknsAFPDCfcs HoJtew Lane. Suite 284Late Suosess, l ws? York 11042Reference 018155544Maws and AddressMglloraf Uatoa Fira fnstirance Gomf Kjy of Pttsbur - ••*&.
AFPO
Aikirsss: .Ore Hojiow Lake Suces^y *W 1 1042
f 31421 (4/0&) 1012

smr
AHVXSHD3S

•IH1S INSURANCE eiSSUHJPURSUMrrTO THEFLORIDA SURPLUS LINES IAW. PERSONSINSURE) BY SURPUUS LINES CARRIERS DO NOTHAVE THE PTOTECTIOM OF TOE FLORIDA
-ANYRHSHfTOFREOOVSiYFORTHEOBUGATIOMO F A M W S O L V e W T O H U C K S W -
Karen B. Lampson433 Centra! Ave, 4" flra. Petersburg, FL 33701License* D040184
IRONSHORE SPECIALTY INSURANCE COMPANY75 Federal St
Boston, MA 02110ToU Free: (877) IRON4J1
SURPLUS UNES INSURERS' POUCY RATES AND FORMS ARE NOT APPROVED BY ANYFLORIDA REGULATORY AGENCY.
Policy *fc 000231802Expiring Policy * 000231801
Premium: $14.561.00Policy Fee: $35.00State Tax; $729.80Service Fae: $14.60Hurricane Fee: $189.75Total: $15,530.15
THIS IS ISSUED BY THE INSURANCE COMPANY SELECTED ABOVE
LAWYERS PROFESSIONAL LIABILITY POUCY
WITH OAIM EXPENSES INCLUDED IN THE LIMIT OF LIABILITY
DECLARATIONS
PRODUCER:Janice HMery1115 US 98 SLakeland FL 33801#0073024
This 'a a Claims Made and Reported Policy, please read ft carefully. Amounts incurred as Oalm Expenses shatt reduce thelimftoflfaWrtyavaUaltetopayjudsrneirtsOT
r
ITEM 1. NAMED INSURED AND PRINCIPAL ADDRESS:
Brush, Pujol & Coyte, P.A.825 E. Main StreetLakeland, FL 33801
Item 2. POLICY PERIOD
(a) Inception Date: April 03, 2012
(b) Expiration Date: April 03, 2013
at 12:01 a.m. both dates at the PrincipalITEM 3. LIMIT OF UABIUTY (inclusive of Claim Expenses)
$3,000,000 Each Claim
$3,000,000 aggregate limit of tiabUity for all Claims made or deemed made during Policy Period
ITEM 4. DEDUCTIBLE:
$10,000
ITEMS.Premium: Coffipfencew^a^st^toOnespfecem^re^renwnfs, trxAdi
stamping tf» Potoyand eofedion and payment of surpfte toes taxes,in me responsaaty of tfe flroter.
Praimirrc
Toted Amount Due:See Invoice for the date Premium is due and payable. Failure to payWeprennuminftJfmayresrft/nHjidanceofcoveraoe.
ITEM 6, RETROACTIVE DATE: JHiH Prior Acts
LPLDEC002 (05/09) Page 1 of 2

1 n & v. f a r. < e C o nt p ,i i
Created by The Florida Bar for its members.
541 Fi. Mitchell Hammock Road * Oviedo, Horida 32765Phoae: 800-633-6458 • Fax;8Q&-?8i-20lO
www.flmtc-com
Lsmyers Professional Liability PolicyThis a a CMms Made and Reported Polity, Please read it carefitffy.
Decl&r&tiom
Policy Number: 20070242
ItemL Named f mured:
Matting Address: P.O. Box 22604Tampa, Florida 33622-2604
Hem Z PoUey Periods From 08^7/2012 to 08^27^W3 at 12&1 AM.Standard Time at ¥&ar Address Shown Above
, Limit of Liability
Item 4, Deductible:
ftemS, Premium:
$100,000$300,000
55,000
$3230
Per ClaimTotal Limit
Annual Aggregate
item 6, Forms and Endorsements Attacked at Ptttity issuance:FLPL-IOI (R.08/01/20! I) FLPT.-200R (R.08/OI/201 1) FLPL-103 (R.08/01/201 1)
Dais Issued
FLPL-100 fR.OS^J/20! 1)
The Policy is not valtd until signed by Oar GtttJt&rized representative.
X/ of I
_

CERTIFICATE OF LIABILITY INSURANCE DATE (MWW30/VYYY)
07/1W2C12JTHIS CERTIFICATE ISISSUED AS A SHATTER OF INFORMATION ONLY ANO CONFERSNORIGHTSUPON THE CERTIFICATE HOLDER.iTWS CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELV AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE(POLICIES BELOW, THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING 8*$UKER{S>•AUTHORIZED REPRgSairrATIVg OR PRODUCgR. AMD THE CERTIFICATE HOLDER; IMPORTANT: If the oerfificaKs holder Is an ADDITIONAL INSURED, the po»cy{fes) mast bs endorsed. If SUBROGATION f S WAIVED, sobje« toithe teims and condJSoas of ttie policy, certain policies may require an endorsement A statement on tWs certiorate does «ot confer rights tojtfre certificate iioktermJfeaof such endorsements).irooouesa
First ZniSesnity insurance67 Oxford Streetiyiui, as. 01902
T8T-511-2500
INSURED•KStiSERS AFKJRDiNO COVERAGE
6H 5 Csstmseree DriveSuite 205
Lafceiand, FL 33SI3
State National Insurance
1NSURSRB:
COVERAGES CERTIFiCATE NUMBER: REVISION NUMBER:: THiS IS TO CERTIFY THAT THE POUC'-ES CF INSURANCE USTEO BELOWMAVE BEEN ISSUED TO THE JNSURED NAMES ABOVE FOR TOE POLCY PERIODj MDtCATHO. N0TWMS7 ANOiNG ANY REQUIREMENT. TERM OR CONDITION OF ANY CONTRACT OR OTHER DOCUMENT VMTH RESPECT TO WHICH THIS
CERTIFICATE MAY SS ISSUED OR MAY PERTAIN, THE INSURANCE AFFGSDED BY THS PQUaES OESCR5SE3 H5?EfN iS SUBJECT TO ALL THE TERMS,£XC .US:O«S AND CQNDiTIONS OF SUCH POLICES. UM-TS SHOVMN MAYHAVE BEEN REDUCED 3Y PAID C1A«S.
j* ,K j TYPECFffSURANCS
I
*
nGEN w AGC^E^ATE USSlT APlfXIES PER;
•v^"I 3OutCv : t^ROJECT 1 "!U3C
nDocc"
WORKERS COMP6JJSAT!CNANO SMPLOlfEHS1 UAfflLlTY
W..V. ^^,
O=ERATK3KS 01SOW
KHOfi. iSUCK j a-,..—,.,....,-™WSRO t«9V0 • «»«¥"«»««
Lawyers Frofessional ij 01
P0UCYSFF
07/22/12
PCSJCYEXP utms
• •%!£, - *
U«S«A£5t TO KfcNSta
BiED EXP (Aiy aa&fetmfi
PfeSSO^LSANOaciUfW |
GSMEBAI-AGGRSS^TS
PRraaCTB - COMFVOP A3G
cowai\€O SINGLE UKIT ;sa
SOStYoaURVtPefpw^)
SOOtY INJURY por actstenRJwopeRrt o«w«5S (PWWCOBril]
6ACH OCCURAKCE
AOSBSGA^i
|
| TORYUMlTS {OTH£R|
Ei. EACH ACCIDENT i
EMPLOYEE i£.1- -DSSSIVS6 -POCOV OWT;
"" ; Owi«flS/Vggr«^Ms: §5GGy GOO
DgSCRJFnON OF OPERATIONS / LOCATIONS I VEHICLES (Attach ACCORD 101, Additional Remarks Sc&edute, » more space is required}Ciaiwa J'ade Coverage, Covering 3 Attoraeys , Sstroactive Date: G7/22/2C-09. Deductible i.s 510,000.00Per Claira and applies to toss and Oefease, Claims Expenses inside the Units of liability.
CERTIFICATE HOLDS? CANCELLATIONSMUU3 AWT OF THE A8CVE0 DEKT^SO POUCKS 6E OWOEUJED ffi«3«6 THE BS^RATWIK CWT
T^RgQF TrlE ISSMSG !NS!WESR Wa EJO6AVOR TO VAtt. W QAYS WSStTSK KOTaX TO T>«C8R*inC*'EHOU£S NAMB5 TO IHEL&T, «IT •
AUTHORSZED REPRES^JTATiVE
ACORD 25 {2009/01}The ACCORD name and logo ara registered marks of ACCORD

~ CERTIFICATE OF LIABILITY INSURANCE "J
CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND. EXTEND OR ALTER THE COVERAGE AFFORDED BYTHE POLICIESSELOW. THIS CERTIFICATE OF INSURANCE DOES MOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURERfS), AUTHORIZEDREPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER.
IMPORTANT: tf*eci fica!eht«erBanADDrrK)N^B«URED.ftepcicy }mustbeandOfsed. if SU8RCKWTION IS WAIVED, subject totie terms and oondffions of the policy, certain polities may require an endorsement A statement on this certificate does ma confer rights to 8wcertificate holder in fieu of such endorsements).
PRODUCER
Dean Insurance Agency, Inc.230 N Westroonte OrSuite 2100Altasonte Springs, FL 32714INSURED
Boyette, Cunnrins & Nailos, PLLC1635 E Highway 50SuiteSOOaenaont, FL 34711
gSl*CT Steven Majowitz
IE(MMfW»mY)
9/11/2012
git, **»: C407)86S-7477 x-112 [ 8£ „. (407)865-7557
^pOftESS:PRODUCERCUSTOMER n^f:
INSURERS) AFFORDING COVERAGE i HAIC»INSURER A: Medmarc Casualty Insurance Cam jINSURERS i
INSURER C:
INSURER D:
INSURER E:
INSURER F:
j
COVERAGES CERTIFICATE NUMBER: 12/13 REVISION NUMBER:
CERTIFICATE MAY BE ISSUED OR MAYPERTA9I, THE WSURANCE AFFORDED BYTHE POLICES DESCRIBED HEREW IS SUBJECT TO ALL THE TERMS.EXCLUSIONS AND CONDmONS OF SUCH POLICIES. LMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAMS.
1;nf! TYP60FWSURANI•X. f001
' GENERAL LIABILITY
"1 COMMERCIAL GENERAL LIABILITY
I j 1 CLAIMS-MADE j j OCCURi
--
A
. L.G£»f L AGGREGATE LIMIT APPLIES PER'
AUTOMOBILE U ABILITY
_] ALLOWED AUTOS
{ SCHEDULED AUTOS
H HIRED AUTOS
NC*KDWNED AUTOS
j UMBRELLA UAS
i EXCSSSU4B
! DEDUCTBLE
] RETEMtiON S
OCCUR
CLAIMS4IAOE
WORKERS COMPENSATIONAND EMPLOYERS" LIABILITY -f,NANY PROPBETOi»PARTOER«EXeCUTO« ~\
if yes, descnbe und«CfeSCRIPTlON OF OPERATIONS twKwProfessional LiabilityClaims Made Coverage
K1A
SUSfim» POLICY NUIH8ER
12HCFL007608
POLICY 6FF PGUCYECP«B«pBYyVYt
0!SJ/14/26l2 r 09/14/2013
LIMITS
EACHOcaiRfffiNce > sUAMAGS VO«HNTEDPREMISES {=9 ocomoM!MED S<P <Anj one pereoni
PERSONAL iADV INJURY
GSHERAL AGGREGATE
PRODUCTS -COWW AGG
COMBINED SINGLE LIMIT(Ea acciaart}
BOXY HURT {Per pa-son]
BODILY INJURY {PttacOasnQ
PROPERTY DAMAGE
EACH OCCURRENCE
AGGREGATE
j WCSTATU- j IOTH-FTOftYLHSTS! I 6R
£L.EACHACC(D6(4T
Ei. DISEASE -EA EMPLOYES
&L DISEASE -POUCY LIMIT
ssJ:
s
*s
ss
ss3
S
$
J
S
$ss
$1,000,000 Each Claim$1,000,000 Aggregate
OESCfOFTIOM Of OPERATIONS (LOCATK3NS/ VEHICLES (Attach ACORD 101, AdaJfion"! (tenariasSchcduto. If more apace 15 rcqu)r«i)
Legal Services include acts as a title insurance agent,'olicy covers attorneys: Norman C. Cunnrins, Heath B. Nailos .Kenneth W. Boyette, Kristen C. Nailos,Jinny 0. Crawford, Nancy A. Oavito, Paul Cipparone, Ernesto Bait rain, Aileen MazanetzCERTIFICATE HOLDER CANCEUATON
Insured 's CopyBoyette, Cunnrins & Nailos, PLLC1635 E. Highway 50Suite 300Clerraont, FL 34711
SHOULD ANY OF THE ABOVE DESCRIBED POUCES BE CANCELLED BEFORETHE EXPJRAT1ON DATE THEREOF, NOTICE WILL BE DELIVERED INACCORDANCE WITH THE POLICY PROVISIONS.
AUTHWUZED REPRESENTATIVE C~\, n /.ii- pt.
Deborah Turner/MKH
ACORD 25 (2009/09)© 1988-2009 ACORD CORPORATION. AB rights reserved.
The ACORD name and logo are registered marks of ACORD
_

Market Insurance CompanyfA Stock Company") Deertekl. IL 60015
Lawyers Professional Liability DeclarationsThis is a cbims made and reported policy.
e read this poNcy and a* endorsements and attachments carefully.
THE POtJOTBUWTH) TO UABflJTY FOR ONLY THOSE CUUM^INSURED AND REPORTED TO THE COMPANY DURMG THE POLICY PERIOD OR AUTOMATIC EXTENDEDREPORTING PERIOD, UNLESS, AND TO THE EXTENT, THE EXTENDED REPORTING PERIOD OPTION APPLIES.
PofeyNwnta: LA-300195 Renewal rfPofcy: NS0
1. NAMEDWSURGD: PoWsLawFlrrnDBA:PoOtis&Matov8ia.RA.
lUUNG ADDRESS: 730 Duntewton AvePort Orange, FL 32127
2. POLICY PERIOD: From 254ue4M2 to
IN RETURN FOR THE PAYMENT OF THE PREMUM, AND SUBJECT TO ALL THE TERMS OF THB POLICY, WEAGREE WTO YOU TO PROVIDE THE INSURANCE AS STATED M THE POLICY.
UHrrOFUAOLITY: BKhCfdm $1,000.000$1,000,000
4. DEDOCTBBLE $25.000
5 MOHMLPRamM: $10.493.00FHCF $13041
Total Premkim $10.629.41
RETROMCHMEOATE: Augusttfadate teindkated, this insurance w« not Jiy to any act, error, ofrtssion or Peraonal tojuiywhich occuired before such date
pofcy*th^MLP00010611 ME8-54(»(»10MU>140Wn.0412
MLP 0001 (TOO) 061OanageeOnfyDedudMe Cfaima Expenses in MSion lota Umt of Uab»yMLP 1302 02 11
Claims SenfceCMtar: MvkdSwtoftlnc; Ten Partcway North, DeerfieW, Bncw80015Fac (847)5724338 6-maft neiNcUmsOniattatGOiiuxM Ptwie: (847) 572-6000; (888) 5<»3200
TbeeeDm^ntfiai togetlwrwBlitlwCammcinPelcy
The Plus Cotnf»ntes,lnc^ 520USHglMny22.Martcel Producer* 210092
MOIH1000Q211 _ Cowitetaitpwdby Date
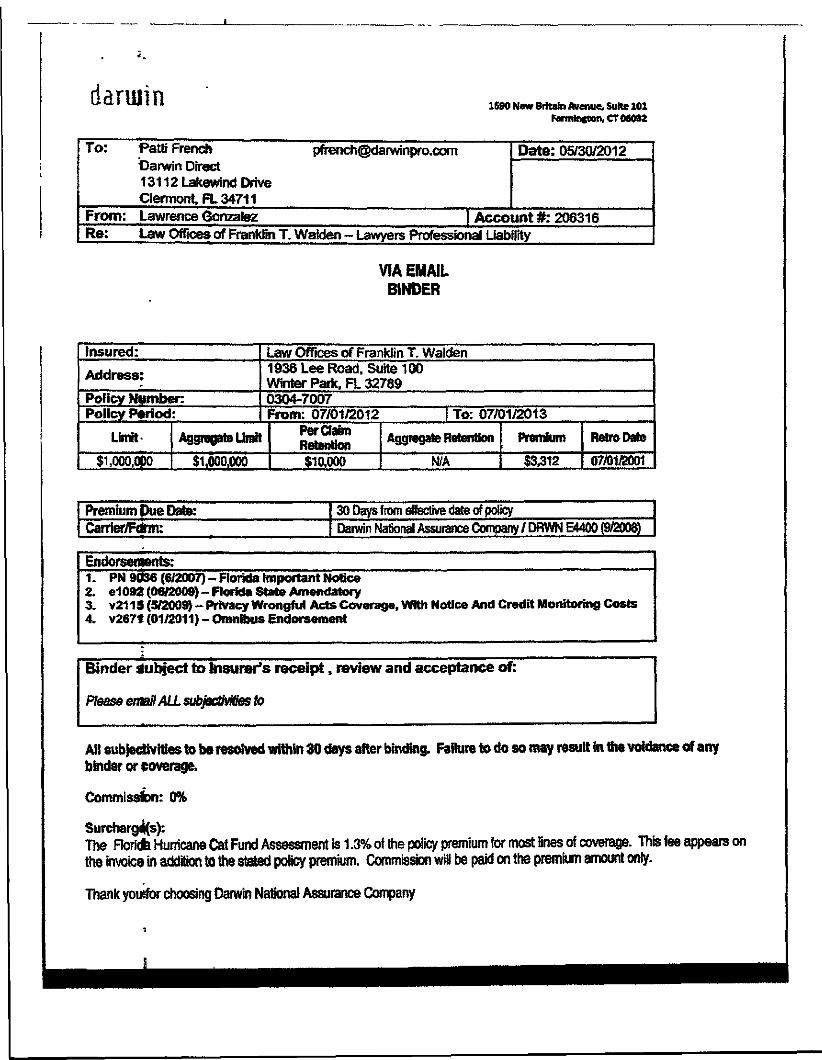
daruiin 1690 New Britain Avenue. Suite 101Forminfton, CT 06032
To:
From:Re:
Patfi French [email protected] Direct131 12 Lakewind DriveClermont, FL 34711Lawrence GonzalezLaw Offices of Franklin T. Walden - Lawyers
Date: 05/30/2012
| Account #:206316Professional Liability
VIA EMAILBINDER
Insured:
Address:
Policy Number:Policy Period:
Limit
$1,000,000
Law Offices of Franklin T. Walden1936 Lee Road, Suite 100Winter Park, FL 327890304-7007From: 07/01/2012 | To: 07/01/2013
Aggregate Omit
$1,000,000
Per ClaimRetention$10,000
Aggregate Retention
N/A
Premium
$3,312
Retro Date
07/01/2001
Premium Due Date:Carrier/Form:
30 Days from effective date of policyDarwin National Assurance Company / DRWN E4400 (9/2008)
Endorsements:1. PN 9036 (6/2007)-Florida Important Notice2. e1092(06/2009)-Florida State Amendatory3. v21 IS (5/2009) - Privacy Wrongful Acts Coverage, With Notice And Credit Moratoring Costs4. v267t (01/2011) - Omnibus Endorsement
Binder Subject to Insurer's receipt, review and acceptance of:
Please email ALL subjectivities to
AH subjectivities to be resolved within 30 days after binding, Failure to do so may result in the voidance of anybinder or coverage.
Commission: 0%
Surcharges):The Ftoridfe Hurricane Cat Fund Assessment is 1.3% of the policy premium for most fines of coverage. This fee appears onthe invoice in addition to ttie stated poficy premium. Commission wiB be paid on the premium amount only.
Thank yousfor choosing Darwin National Assurance Company

Lawyers5
Professional LiabilityInsurance
LAW ' Protective Policy DeclarationsInsurance Company
Hereinafter known as the Company
THIS IS A CLAIMS MADE AND REPORTED POLICY. PLEASE REVIEW THE POUCY CAREFULLY.
NOTICE: EXCEPT AS MAY BE OTHERWISE PROVIDED HEREIN, THE COVERAGE OF THIS POLICY IS LIMITED TO LIABILITYFOR COVERED ACTS COMMITTED SUBSEQUENT TO THE RETROACTIVE DATE, IF APPLICABLE, FOR WHICH CLAIMS AREFIRST MADE AGAINST YOU WHILE THE POLICY IS IN FORCE AND WHICH ARE REPORTED TO US NO LATER THAN SIXTY(60) DAYS AFTER THE TERMINATION OF THIS POLICY. THE COVERAGE OF THIS POUCY DOES NOT APPLY TO CLAMSFIRST MADE AGAINST YOU AFTER THE TERMINATION OF THIS POLICY UNLESS, AND IN SUCH EVENT ONLY TO TH£EXTENT, AN EXTENDED REPORTING PERIOD OPTION APPLIES.
POUCY NUMBER: LPL-4874-0812 Replacing: LPL-3570-0811Producer Code: COASTAL
1. NAMED INSURED: Law Offices of Chalik & Chaiik, PA.ADDRESS: 10063 N. W. 1 st Court
Plantation, FL 33324
2. PERIOD OF INSURANCE FROM: 08/10/12 TO: 08/10/13teOIAM STANDARD TIME AT THE ADDRESS SHOWN IN ITEM 1 ABOVE.
3. UMTS OF LIABILITY(a) $1,000,000.00 EACH CLAIM(b) $1.000.000.00 in the AGGREGATE
including Defense Costs
4. DEDUCTIBLE{a) $26,000.00 EACH CLAIM(b) $0.00 in the AGGREGATE
including Defense Costs
5. PREMIUM US $10,477.00 plus applicable taxes
6. RETROACTIVE DATE: Full Prior Acts
7. Notice to insurer Protective Insurance CompanyP.O. Box 7099 Tel.: (800)410-3694Indianapolis, IN 46204-7099 Fax: (800)497-6338
8. Forms and endorsements attached at inception of coverage. Refer to schedule of forms.
Disclosure 9.2011 LPLPOL 01 LPLNOT 01LPLNOT02 LPLENOO LPLEN39
Issued on: August 17,2012 at Aliendale, New Jersey
for Jorgensen & CompanyAuthorized Representative artf Managers forThe Legal Professionals'Purchasing Group,
Countersigned st Aliendale. New Jersey by:.on: August 17.2012 '
LPLDEC 01 {10/101 Page 1 of 1

LAWYERS PROFESSIONAL LIABILITY POLICYDECLARATIONS
Branch: Policy Number: Insurance is provided by Continental Casualty Company,700324 912 287152359 333 S. WabashAve, Chicago 11.60604
A Stock Insurance Company.
1A. NAMED INSURED AND ADDRESS: NOTICI- TO I'OI.ICYHOI.DI-RS:MonLs Law, P.L. Tin's is> a Claim* M-ide and Reported policy. It applies only to2605 West Lake Mary Boulevard those claim;, that are both firsl made against the insured andSuite 115 reported in writing to the Company during the policy period.Lake Mary. VI. 327-16 Please review the polity carefully and discuss this coverage
with your insurance a gen I or broker.
IB. PREDECESSOR I'TK.VI(S): See Declarations Addendum
2, POLICY PERIOD:Inception: 07/18/2012 fixpiration' 07/18/2013at 12:01 A.M. Standard Tune at the address siiown above
3. LIMITS OF LIABILITY: 1-adi Claim: S250.000inclusive of Claims Kxpenses Aggregate: $500,000
Deatli or Disability and Non-Practicing liach Claim: $250.000Extended Reporting Period Limit of Liability: Aggregate: $500.000
4. DEDLCTIBLES: Aggregate: S3.000Inclusive of Claims Expenses
5. POLICY PREMIUM:
Annual Premium: $3385.00
Surcharges/Taxes; Amount:Florida Hurricane Catastrophe Fund S44.01
Total Amount: S3.429.01
Includes CNA Risk Management Seminar Credit of S- 132.00Includes Net Protect Premium, see coverage endorsement if applicable
6, FORMS AND ENDORSEMENTS ATTACHED AT INCEPTION:G-118011-A (Ed. 08/2009X G-118012-A (Ed. 03/1999), G-118014-AC (Ed. 04/2008). G-118016-A (Ed. 04/2008). G-118024-A (Ed. 04/2008), G-118029-A (Ed. 04/2008), G-118039-A09 (Ed. 06/2008), G-118065-A09 (Ed. 11/2011), G-14S184-A (Ed. 06/2003). GSL-11512-XX (Ed. 10/2008).GSL-12439-XX(Ed.03/2009)
7, WHO TO CONTACT: To report a claim:CNA Specialty ClaimP.O. Box 8317 Chicago. 1L 60680-8317Email: [email protected].: 866-419-6308 / Online: wmv.cna.coin/claimsLawyers Claim Reporting Questions: 800-540-0762
06/06/2012Authorized Representative Date
G-118012-A (Ed 03/99)Page)

8 986
This Spectrum Policy consists of the Declarations, Coverage Forms, Common Policy Conditions and anyother Forms and Endorsements issued to be a part of the Policy. This insurance is provided by the stockinsurance company of The Hartford Insurance Group shown below.
SBA
INSURER: HARTFORD CASUALTY INSURANCE COMPANY
HARTFORD PLAZA, HARTFORD, CT 06115COMPANY CODE: 3
Policy Number: 21 SBA W8689 DV
SPECTRUM POLICY DECLARATIONS
1HE -HARTFORD
Named Insured and Mailing Address:(No., Street, Town, State, Zip Code)
GREGORY & CLARK, PLLC
1938 BOOTHE CIRCLELONGWOOD PL 32750
Policy Period: From 11/02/11 TO 11/02/12 i YEAR12:01 a.m., Standard time at your mailing address shown above. Exception: 12 noon in New Hampshire.
Name of Agent/Broken ONEIL LEE & WEST INC/PHSCode: 225279
Previous Policy Number. 21 SBA VJ8689
Named Insured is: CORPORATION
Audit Period: NON-AODITABLE
Type of Property Coverage: SPECIAL
insurance Provided: In return for the payment of the premium and subject to all of the terms of this policy, weagree with you to provide insurance as slated in this policy.
TOTAL ANNUAL PREMIUM IS: $1,856
FLORIDA FC SURCHARGE:FL EMERG MGMT SURCH:2011 FHCF ASSESS CL:FCIT EMERG ASSESS
$$$$
1Countersigned by
1.86 FL FIGA REG 2008:4.00
24.0015.28
Authorized Representative
$ 5.19
09/07/11Date
Form SS 00 02 12 06Process Date: 09/07/n
Page 001 (CONTINUED ON NEXT PAGE)Policy Expiration Date: 11/02/12

SPECTRUM POLICY DECLARATIONS (Continued)POLICY NUMBER: 21 SBA VJ8689
BUSINESS LIABILITY
LIABILITY AND MEDICAL EXPENSES
MEDICAL EXPENSES - ANY ONE PERSON
PERSONAL AND ADVERTISING INJURY
LIMITS OF INSURANCE
$1,000,000
$ 10,000
$1,000,000
DAMAGES TO PREMISES RENTED TO YOU $ 300,000ANY ONE PREMISES
AGGREGATE LIMITSPRODUCTS-COMPLETED OPERATIONS $2,000,000
GENERAL AGGREGATE $2,000,000
BUSINESS LIABILITY OPTIONALCOVERAGES
HIRED/NON-OWNED AUTO LIABILITYFORM: SS 04 38
$1,000,000
Form SS 00 0212 06Process Date: 09/07/11
005 (CONTINUED ON NEXT PAGE)Policy Expiration Date: 11/02/12
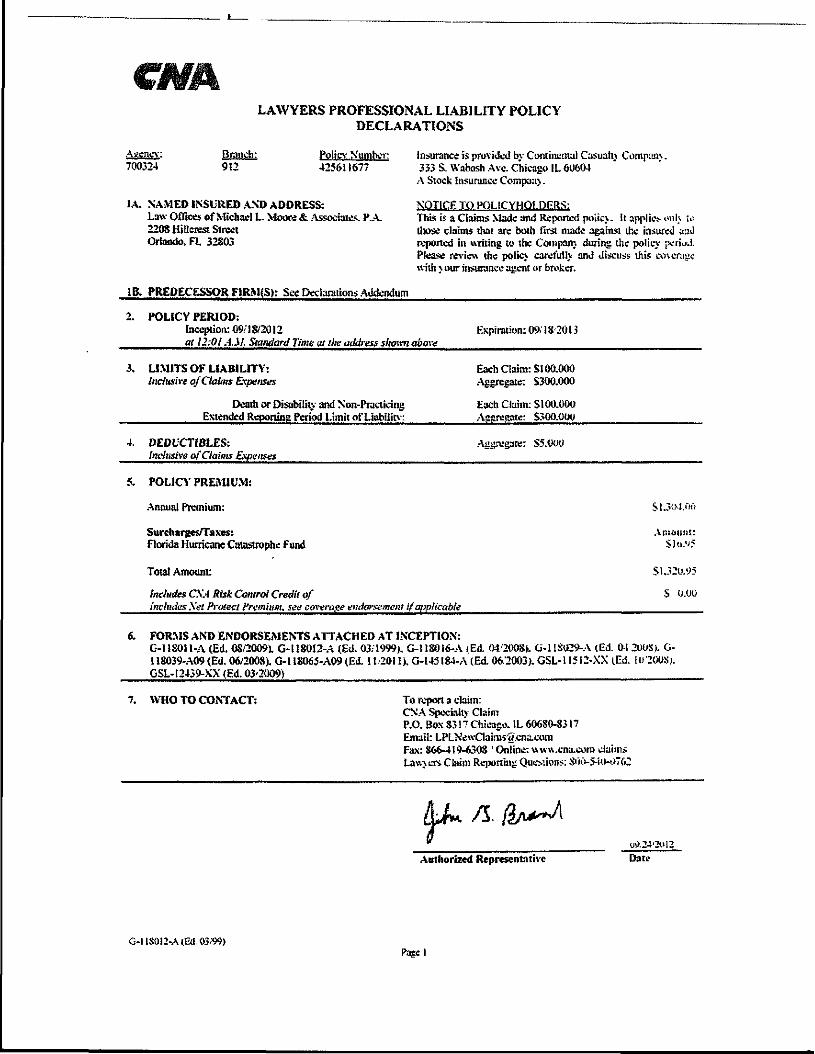
LAWYERS PROFESSIONAL LIABILITY POLICYDECLARATIONS
Agency:700324
Branch:912
Policy Number425611677
1A. NAMED INSURED AND ADDRESS:Law Offices of Michael L. Moore & Associates. P.A.220SHillerestSlrectOrlando. FL 32S03
Insurance is provided by Continental Casualn Coraponj.333 S. YVabash Avc. Chicago IL 60604
A Stock insurance Compau}.
NOTICE TO POLICYHO1.DERS:This is a Claims Made and Reported poiic\. It applies oni> u>those claims that arc both first made against the insured a:iJreported in writing to the Compam during the policy perPlease review the polic> caret'ully and discuss thiswith > our insurance agem or broker.
IB. PREDECESSOR FIRM(S): See Declarations Addendum
2. POLICY PERIOD:Inception: 09/18/2012at 12:01 A.M. Standard Time at the address sliamn above
Expiration: 09..'18-2013
3. LIMITS OF LIABILITY:Inclusive of Claims Expetises
Death or Disability and Non-PracticingExtended Reporting Period Limit of Liabilitv:
Each Claim: SI 00.000Aggregate: S300.000
Each Claim: SI00.000Asareaate: S300.001*
4. DEDtCTIBLES:Inclusive of Claims Expenses
5. POLICY PREMIUM:
Annual Premium:
Aggregate: S5.WU
Sl.30-I.0fi
Surcharges/Tases:Florida Hurricane Catastrophe Fund
Total Amount:
Includes CXA Risk Control Credit ofIncludes .Vgi Protect Premium, see cwera^t endorsement if applicable
Amount:
Sl.32u.95
S 0.00
6. FORMS AND ENDORSEMENTS ATTACHED AT INCEPTION:G-l 18011-A (Ed. 08/20091 G-l 180I2-A (Ed. 03/I999>. G-l IS016-A (Ed. 04/2008). G-l 1S«2»-A (Ed. 04 200S). G-U8039-A09 (Ed. 06/2008). G-l 1S065-A09(Ed. 11,2011). G-145184-A (Ed. 06/2003). GSL-11512-XX (Ed. io'200S).GSL-12439-XX (Ed. 03'2009)
7. WHO TO CONTACT: To report a claim:CXA Specialty ClaimP.O. Box S3! 7 Chicago. IL 606SO-S317Email: LPLNewClaims-g.cna.comFax: 866-419-630S ' Online: ww\\ .cna-eoin claimsLaw> ers Claim Reporting QueMions; S'iO-5-i|>ii762
Authorized RepresentativeU!>.24-2ol2_.Date
G-llS012-A(Eii.Page I
FlUI ILLd 541 E Mitchell Hammock Road • Oviedo, Florida 32765
S Phone: 80°-633-6458 * Fax: 800-781-2010M u t u a i www.flmic.com
I n s u r a n c e C o m p a n y ®
Created by The Florida Bar for its members.
Lawyers Professional Liability PolicyThis is a Claims Made and Reported Policy. Please read it carefully.
Declarations
Policy Number: 20010283
Iteml. Named Insured: Law Offices of Nicholas M. Athanason, Esq., P.A.
Mailing Address: 1236 66th Street NorthSaint Petersburg, Florida 33710
Item 2. Policy Period: From 10/01/2012 to 10/01/2013 at 12:01 AM.Standard Time at Your Address Shown Above
Item3. Limit of Liability: $1,000,000 Per Claim$1,000,000 Total Limit
Item 4. Deductible: $5,000 Annual Aggregate
Item 5. Premium: $9529
Item 6. Forms and Endorsements Attached at Policy Issuance:
FLPL-101 (R.08/01/2011) FLPL-200R (R.08/01/2011) FLPL-103 (R.08/01/2011)
The Policy is not valid until signed by Our authorized representative.
September 11, 2012Date Issued
FLPL-100 (R. 08/01/2011) Page 1 of I

75 federdi StBoston, MA 02110
Toil Fare-(."/?; IRON4U
1•9
a)V
Policy ff:CC07§2C()2Expiring PoficyS; 003752001
Th>< o Sa_>£0 3V ?K" Vf1 tf.V f r t rCTf
WfTH OAlMi EXPEfSfS IWCIUOEO N THE UMil Of UAEIltTY
DECLARATIONS
Tbk is a Ctalms Mitt* and Report*! Puiky, ptsss-e mud it cvtofuily. Amount*, incurred as Claim f,xft>.ntta tlwil rs«}«cB ttiftlimit of iwbllfty awlfafcle to pay ]«Jfm*rjti or sutttertteftts tm4 shall sfco be «ij«pKBd «g*in$f tht do-duetlbio,
fTEM X WAMFO INSURED AND PSfNCfPAiL AM5RESS:
Morgan Ffrw, PA tsba Morgan S Morgan, RA2C N'. O*ai|»e Avs, 16th FtQ'l'sr-tfo, fl a2BOI
I Sere 2, POUCT PtRIODj: fa) Incaptton Data. r-lov«wt«»r03»2Gil
(b) Fkpirtrtfon £iafe; Novombof 01,2012l; as "U31 a.m. both datejatftc principal
fTEM 3, UMJT OF UAfilUTy (inclusive at CWm
10,C<>0 O10 aggregate .«m t of U-fc'ifty 'c? s! (!«"ns mid; or rfte'rsiid mca.- <jun 12 Pcitcy pcnod
ft£M «. RETROACn« DATE; Full Pne A
DfC.C')/ flB/C-4?]

"fTEM 7. FORMS AND ENDOftSfMENTS ATTACHED AT ISSUANCE;
1, LPl.END.OS6 (0409) Spedffc Iraurtid totfoacUve Date2, LPL.EMD.067 (0409) Specific Person or Entity Exclusion3, Manuscript: Additional Nailed Insured endorsement
ITEMS. INSURERAOORCSS: c/c 'W'hcr
Or,c St.; tt 5tsf ie Scrvkei, LLC
i
JTFM 9. BROKER:! A00HESS:
THESE OEOARATIOfiS, TOSETHER VUrfH TOE COMPiETED AND S1GK60 APi3UCAT!»i> POR WJS POUCY AND THEFOUOWED PoyCY; iNCLUOiNG (NFOfiJViArtON FURNfSHED IS CO«NICT»N THEREWfTH WHETHER DIRECTLY ORTHROUGH PUBUC F1UNG, AND TOE WJUCV TOflt ATTACHED HtRETO, COfOSBTUFETtSE WSURAK'CE fOUCV,
jjgvgmtj.gr,S.MO/DAY/YR. Autliorteed Representativft
LPl.DEC.S02 {05/09}

March 2012Ust of attorneys: Tampa
Name1. James D. Arnold2. Russell Artille3. Thomas L Bodie4. Scott Borders5. William B.Bowles, Jr.6. Andrew Bragg7. Adam Brum8. Joseph R. Bryant9. Donald W. Buckler10. Keith M. Carter11. Charles J. Crist12. John R. Cummings III13. William R. Daniel14. Richard L Dantzler15. Albert J.Ferrera16. TamraGivens17. Michael S. Goetz18. David G.Henry19. Herbert H. Hofmann II20. Michael K. Houtz21. William P. Howard22. Dawn Hulbert23. Heather H. Jones24. Stephen R. Kanzer25. Sumeet Kaul26. Sarah R. Kinnett27. DarrellW.KropogJr.28. Armando T. Lauritano29. Jared M. Lee30. Vilma Martinez31. J. Andrew Meyer32. Charles T. Moore33. Christopher Pafaszek34. Roger A. Patterson, 11135. Oarryl E. Rouson36. PotorSarirsteln
Florida Bar Number04671460561290093628607465681229980330530099951205614447973240500364036219008982608227113615850114464657638096398408967560937355043812101033300294100011897407821800905682003759300522750902519005228400759160056766007580911686600394620312207(new York) 2044550
37. Rachel Soffln 001805438. Craig O'Neal Stewart 010844839. Brian L Thompson 97296740. Michael J. Vitoria 013553441. Ivan D. Voronec 007994442. Joseph Waechter 009259343. Scott M. Whitley 052068341 Inmrit R Wlftnn 'fflfrTOfn

45. John Aden Yanchunis 0324681