1 euroqol eq-5d jan j. v. busschbach, ph.d psychotherapeutic centrum ‘de viersprong’, halsteren...
TRANSCRIPT

1
EuroQol EQ-5D
• Jan J. V. Busschbach, Ph.D
• Psychotherapeutic Centrum ‘De Viersprong’, Halsteren
• Department of Medical Psychology and Psychotherapy, Erasmus MC

2
EQ-5D
• MOBILITY– I have no problems in walking about
– I have some problems in walking about
– I am confined to bed
• SELF-CARE– I have no problems with self-care
– I have some problems washing or dressing myself
– I am unable to wash or dress myself
• USUAL ACTIVITIES (e.g. work, study, housework family or leisure activities)
– I have no problems with performing my usual activities
– I have some problems with performing my usual activities
– I am unable to perform my usual activities
• PAIN/DISCOMFORT– I have no pain or discomfort
– I have moderate pain or discomfort
– I have extreme pain or discomfort
• ANXIETY/DEPRESSION– I am not anxious or depressed
– I am moderately anxious or depressed
– I am extremely anxious or depressed

3
The clinical perspective
• It is not the doctor who reports
• Quality of life is subjective…..– “Given its inherently subjective nature, consensus was quickly
reached that quality of life ratings should, whenever possible, be elicited directly from patients themselves. “ (Aaronson, in B Spilker (Ed): Quality of life and Pharmacoeconomics in Clinical Trails, 1996, page 180)
– As a CONSUMER of care, the patient is the best judged about the quality of care
• The patient values count in clinical quality of life research

4
The economic perspective
• In a normal market: the consumer values count
• The patient seems to be the consumer– Thus the values of the patients….
• If indeed health care is a normal market…
• But is it….?

5
Health care is not a normal market
• Supply induced demands
• Subsidies (egalitarian structure)
• Government control
• Health care is an insurance market– A compulsory insurance market
• The patient does not pay– Patient Consumer
– Potential patients are paying
– Consumer = General public

6
Who determines the payments of unemployment insurance?
• Civil servant– Knowledge: professional
– But strategy
» more money, less problems
» identify with unemployed persons
• The unemployed persons themselves– Knowledge: specific
– But strategy
• General public (politicians)– Knowledge: experience
– Payers

7
Who’s values (of quality of life) should count in the health insurance?
• Doctors– Knowledge: professional
– But strategy
– But see only selection of patient (the complainers)
• Patients– Knowledge: disease specific
– But strategy
– But coping
• General public– Knowledge: experience
– Payers

8
Patient values seem high
• Stensman– Scan J Rehab Med
1985;17:87-99.
• Scores on a visual analogue scale
– 36 subjects in a wheelchair
– 36 normal matched controls
• Mean score– Wheelchair: 8.0
– Controls: 8.3

9
Is there a problem? • There is no
problem...– if effect is linear– In the past, the general
perspective was seen as a proxy for patient perspective
• There is a problem...– If there is no linear
transformation– Patient and general public
perspective reveal different results
– Loss of power in patient perspective 0
5
10
15
20
25
30
35
40
45
baseline T 1
General public
Patient no coping
Patient with coping
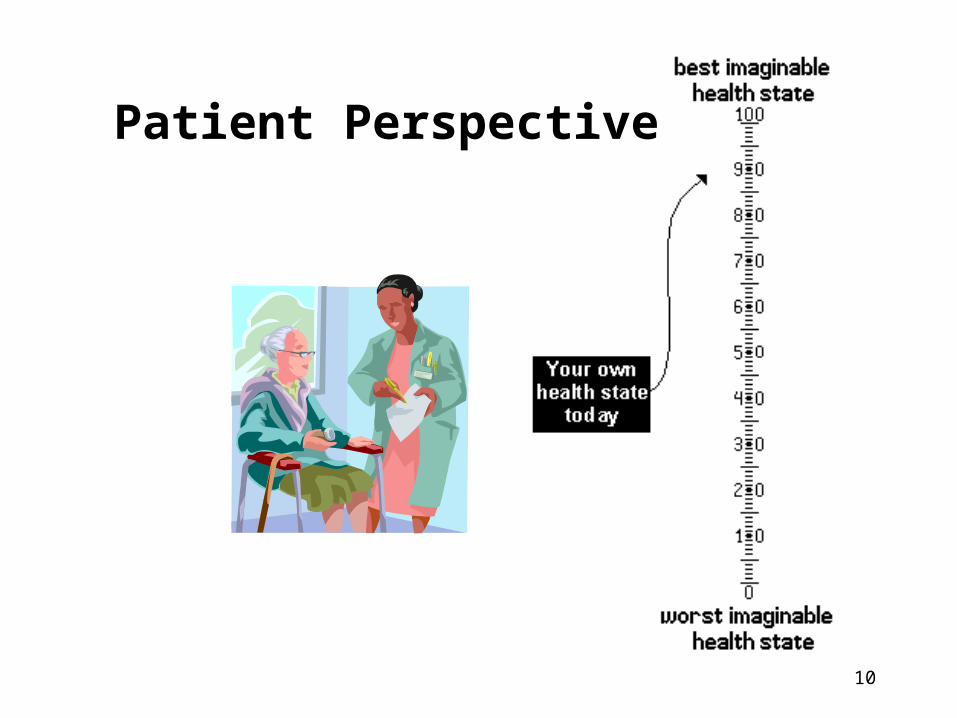
10
Patient Perspective
11
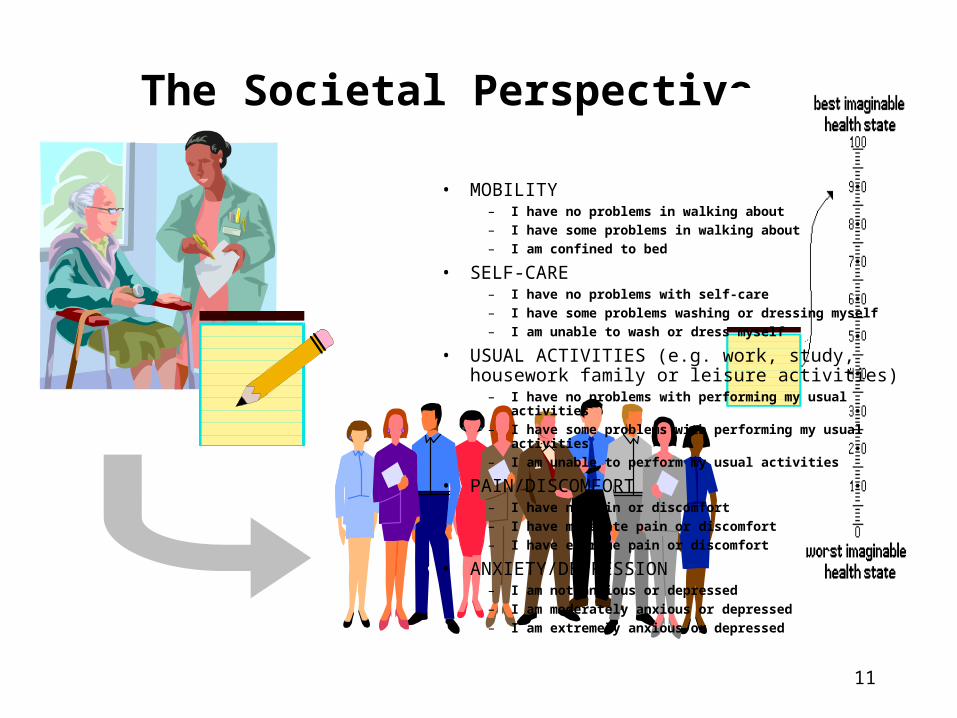
The Societal Perspective
• MOBILITY– I have no problems in walking about
– I have some problems in walking about
– I am confined to bed
• SELF-CARE– I have no problems with self-care
– I have some problems washing or dressing myself
– I am unable to wash or dress myself
• USUAL ACTIVITIES (e.g. work, study, housework family or leisure activities)
– I have no problems with performing my usual activities
– I have some problems with performing my usual activities
– I am unable to perform my usual activities
• PAIN/DISCOMFORT– I have no pain or discomfort
– I have moderate pain or discomfort
– I have extreme pain or discomfort
• ANXIETY/DEPRESSION– I am not anxious or depressed
– I am moderately anxious or depressed
– I am extremely anxious or depressed

12
Validated Questionnaires
• Describe health states
• Have values from the general public– Rosser
– QWB
– 15D
– HUI Mark 2
– HUI Mark 3
– EuroQol EQ-5D

13
EQ-5D
• MOBILITY– I have no problems in walking about
– I have some problems in walking about
– I am confined to bed
• SELF-CARE– I have no problems with self-care
– I have some problems washing or dressing myself
– I am unable to wash or dress myself
• USUAL ACTIVITIES (e.g. work, study, housework family or leisure activities)– I have no problems with performing my usual activities
– I have some problems with performing my usual activities
– I am unable to perform my usual activities
• PAIN/DISCOMFORT– I have no pain or discomfort
– I have moderate pain or discomfort
– I have extreme pain or discomfort
• ANXIETY/DEPRESSION– I am not anxious or depressed
– I am moderately anxious or depressed
– I am extremely anxious or depressed

14
EuroQol
• EuroQol Group
• Latest version: EQ-5D– 5 dimensions
» Mobility, self-care, usual activities, pain / discomfort, anxiety / depression
– 3 levels per dimension
– 243 health states
• Validation– Finland, Netherlands, Norway, Sweden, UK, Spain,
Germany, Greece, US, Japan, New Zealand, Zimbabwe, Denmark
– N = 200 - 3000

15
How to get these societal values?
• Patient fills in questionnaire
• Choose the value function from the literature
• Calculate societal value
COMPUTE MVH_A1 = 1.VARIABLE LABELS MVH_A1 'York A1 tariff'. DO IF (NVALID(mo, sc, ua, pd, ad) < 5 ).RECODE MVH_A1 (1 = SYSMIS).END IF.IF (MAX(mo, sc, ua, pd, ad) > 1) MVH_A1 = MVH_A1 -.081.IF (mo = 2) MVH_A1 = MVH_A1 - .069.IF (mo = 3) MVH_A1 = MVH_A1 - .314.IF (sc = 2) MVH_A1 = MVH_A1 - .104.IF (sc = 3) MVH_A1 = MVH_A1 - .214.IF (ua = 2) MVH_A1 = MVH_A1 - .036.IF (ua = 3) MVH_A1 = MVH_A1 - .094.IF (pd = 2) MVH_A1 = MVH_A1 - .123.IF (pd = 3) MVH_A1 = MVH_A1 - .386.IF (ad = 2) MVH_A1 = MVH_A1 - .071.IF (ad = 3) MVH_A1 = MVH_A1 - .236.IF (MAX(mo, sc, ua, pd, ad) > 2) MVH_A1 = MVH_A1 - .269.

16
An example of a value function
* SPSS syntax Dolan 1997, Medical Care, 1997;35:1095-108.* mo = mobility, sc= self care, ua = usual activities, pd = pain & discomfort , ad = anxiety and depression.
COMPUTE MVH_A1 = 1.VARIABLE LABELS MVH_A1 'York A1 tariff'. DO IF (NVALID(mo, sc, ua, pd, ad) < 5 ).RECODE MVH_A1 (1 = SYSMIS).END IF.IF (MAX(mo, sc, ua, pd, ad) > 1) MVH_A1 = MVH_A1 -.081.IF (mo = 2) MVH_A1 = MVH_A1 - .069.IF (mo = 3) MVH_A1 = MVH_A1 - .314.IF (sc = 2) MVH_A1 = MVH_A1 - .104.IF (sc = 3) MVH_A1 = MVH_A1 - .214.IF (ua = 2) MVH_A1 = MVH_A1 - .036.IF (ua = 3) MVH_A1 = MVH_A1 - .094.IF (pd = 2) MVH_A1 = MVH_A1 - .123.IF (pd = 3) MVH_A1 = MVH_A1 - .386.IF (ad = 2) MVH_A1 = MVH_A1 - .071.IF (ad = 3) MVH_A1 = MVH_A1 - .236.IF (MAX(mo, sc, ua, pd, ad) > 2) MVH_A1 = MVH_A1 - .269.

17
Some values
• Broken arm
• 12211– no problems in walking about
– some problems washing or dressing
– some problems with performing usual activities
– no pain or discomfort
– not anxious or depressed
• Societal value = 0.779

18
Some values
• Broken hip
• 22222– some problems in walking about
– some problems washing or dressing
– some problems with performing usual activities
– moderate pain or discomfort
– moderately anxious or depressed
• Societal value = 0.516

19
Impact on quality of life
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
EQ-5D utilities
Patent graft
Symptomatic occlusion
Primary amputation
Secondary amputation
Cerebrovascular accident
Myocardial infarction
Intake clinic psychotherapy

20
Effect psychotherapy
0.5
0.6
0.7
0.8
0.9
1.0
Intake 1 year after 2 years
EQ
-5D
soc
ial v
alu
es
Clinic 12 monthsClinic 6 monthsClinic 3 monthsOut-patient clinic

21
Reimbursement arguments
• Dunning’s Funnel– 1990
– Government declaration 2002
– Necessary care
» Need
» Equity elements
– Efficacy
– Cost effectiveness
– Own account and responsibility

22
Reimbursement arguments
Impact on QoL
Effect on QoL
Cost effectiveness ?
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
EQ-5D utilities0.5
0.6
0.7
0.8
0.9
1.0
Intake 1 year after 2 years
EQ
-5D
so
cia
l va
lue
s
QALYs

23
Quality Adjusted Life Years (QALY)
• Multiply life years with quality index
• Quality of life index– 1.0 = normal health
– 0.0 = extremely bad health (death)
• Example – Losing sense of sight
– Quality of life index is 0.5
– Life = 80 years
– 0.5 x 80 = 40 QALYs
• Accepted measure of health – Used by the WHO (DALY)

24
QALY league tableIntervention $ / QALY
GM-CSF in elderly with leukemia 235,958
EPO in dialysis patients 139,623
Lung transplantation 100,957
End stage renal disease management 53,513
Heart transplantation 46,775
Didronel in osteoporosis 32,047
PTA with Stent 17,889
Breast cancer screening 5,147
Viagra 5,097
Treatment of congenital anorectal malformations 2,778

25
EQ-5D and cost effectiveness
• EQ-5D specially designed– Social perspective
– Generic
– 0 to 1 scale
• Use EQ-5D for QALY analysis