1 fixed and wireless nurse calls; - sources for awareness and interrupts nokobit2010, gjøvik,...
TRANSCRIPT

1
Fixed and wireless nurse calls; - sources for awareness and interrupts
NoKoBit2010, Gjøvik, Norway
Lill Kristiansen, telematikk, ntnu, [email protected]

2
Content
Introduction to nurse calls and the context in health care
Former work from health care and research questions
Generalization out of health care with more general RQs
Methods
Findings
A general finding on the role of technical descriptions in IS papers

3
The old nurse call system simplified (pasientsignalsystem)
Manual presence (tilstede)
Manual whiteboard
Opt.:’Overhead page’And/or Intercom-calling

4
The old/ new nurse call system simplified (pasientsignalsystem) (use animation)
Manuell tilstede
Manuell whiteboard
Opt.:’Overhead page’/ Intercom
M / display
Nurse call plan
Mottak pas. signal
Telefoni
5
Collective work vs individual phone
Continuity of care vs quickest possible response
Previously: Collective displays Nurses ’picked up’ a signal and answered
Now: Delivery to individual personal phone Aim: ”Focus the delivery of the nurse call, which will again
benefit the patient” Early idea:
If primary nurse did not accept, send call to ”available” nurse with ”shortest task list”
This is now given up, manually set call plan controls the sequence (in the round robin hunts)

6
Former work from health care
Redundancy is useful in hospitals For coordination (Cabitza++, Tjora) For reliability (Monteiro&Ellingsen)
Interrupts and suboptimal communication is a problem in hospitals Coiera and Tombs, McGillis Hall, Pedersen and Fairley,
Health care workers are highly mobile Bardram and Bossen, ++ New ’sengetun’ is aimed at reducing walking, Aslaksen

7
RQ for the health care setting
Which (nuanced, contextual) choices were carried out by the nurses in those cases when several patients were needing help at the same time, in old system?
Is there a good division of function between (nuanced, contextual) choices done by the nurses and choices done by the ICT system(s) for nurse calls?
Is there a good division of function between fixed displays (panels and PCs) and wireless devices (phones) in the new system?

8
Picture from training material
I am presenting a CSCW-study, but here HCI seems to be a problem as well!
In the real system things are different, remember the phone is inside the pocket! (see animation next slide)
Tone Tonsrud
Tilkalling rom 204
OK Avvis
14:45 12-05
SENG 102 14:40
Signalet må jeg nok
avvise!
Pasientsignal
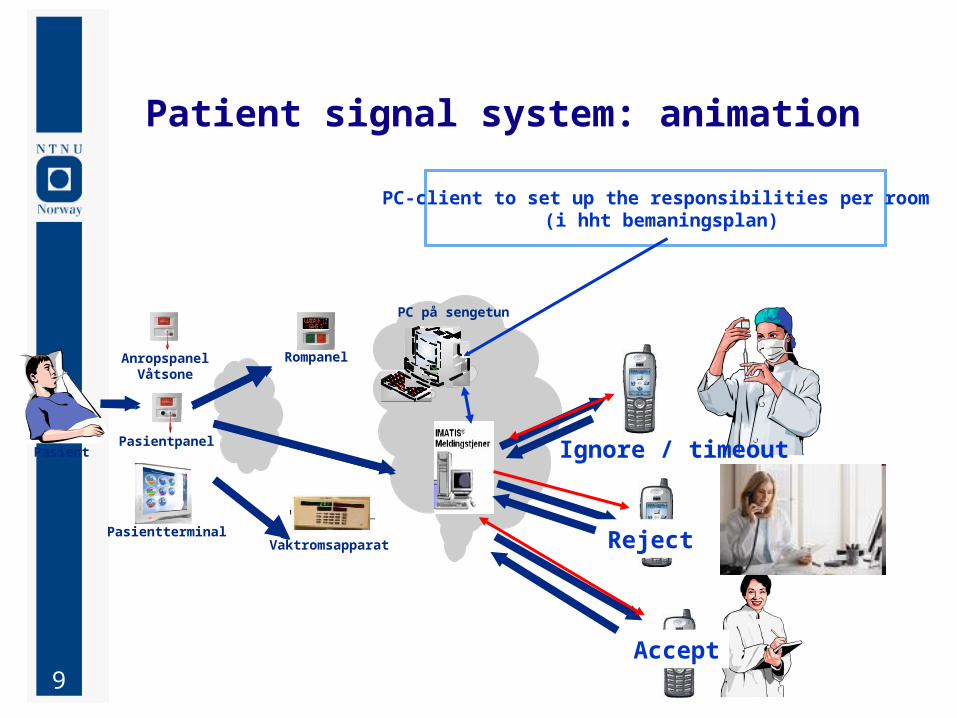
9
Pasient
PC på sengetun
Vaktromsapparat
PC-client to set up the responsibilities per room (i hht bemaningsplan)
Rompanel
Pasientterminal
AnropspanelVåtsone
Pasientpanel
Patient signal system: animation
Ignore / timeout
Reject
Accept

10
General former work and RQ
Fixed and wireless phone calls are different Belotti and Bly, Agre (’where are you’) ++ Wireless phone is a source for interrupt in hospital,
Scholl, 2007
Scanario: Building a ”context sensitive phone” that does not ring during a passionate embrace...
Brown and Randell: This is a false scenario, it is equivalent to building an intelligent computer Proposes to use context ’defensively’
Ackerman: The socio-technical gap RQ: How can a technical system successfully ignore the
need for context and nuances

11
Generalized questions for mobile workers in tight teams, local mobility
How does a change from fixed and public to personal and wireless devices impact: Group awareness and coordination Including a change in unwanted interrupts and/or the
ability to handle the interrupt
How can redundancy of data among various devices be utilized to redunce the impact of the interrupt?
Is ”context-awareness” (adaption inside the technical system) needed?
What are the success criteria for automatic context changes and when should that be avoided and leave the judgement to the humans?

12
Methods
Litterature studies from research field IS / CSCW / health informatics / pervasive&context-aware
3 hours participation on telephony training for doctors
Document studies notes on experiences from nurses during phase 1 Doc. studies of training material emails
Obsevations at 2 wards (total of 12 hours approx.) Approved by REK
Interviews with 2 head nurses (2 x 50 min. approx.)

13
Analytical concept: redundancy
Cabitza et al. (2005): Redundancy of effort (human or computer)
double checking of medication, two computers carrying out independent calculations (more resources, more reliable)
Redundancy of data (human, paper or computer) The same nurse call is displayed on several fixed and
wireless devices. The same (or related data) on whiteboard and in an ICT
system Several nurses know (in their head) about the same patient
Redundancy of function (humans or computers) Several entities are capable of carrying out the same function Basic nursing skills (standardization of education) Several applications running on the same type of servers The statistical mechanism ”the law of big numbers”

14
Group Awareness in general
Definition: The understanding of who is working with you, what they are doing, and how your own actions interact with theirs [Dourish and Bellotti, 1992].
Group awareness may be totally ’virtual’ (ICT-mediated) As in distributed open source projects: emails, IM, forum,..
Often partly obtained via informal sources F2F, oral communication, visual line of sight, …
Formal sources in hospital may be: handover meeting (vaktskifte), EPR
ICT sources in hospital may be: EPR, call plan/ nurse responsibility allocation
(whiteboard), …

15
St.Olav: Call plan / bemanningsplan
Redundancy of function is directly related to the bemanningsplan in sengetunsklient (Imatis client/ nurse call station) Ignore, reject: Who serves as backup nurses? The tension between quick response and ’continuity of
care’
Obviously also redundancy of data typically via fixed devices contributes to awareness and flexibility in real work (and the building’s floor plan / line of sights matters as well)

16
Interview guide: Redundancy and unplanned busy
Assume that Pål in room 102 has called for help, and that nurse Anne is currently helping Pål. What will happen when Pelle is activating a nurse call? What do you believe that happen? What do you want to happen?
Open questions like: Are nurses sometimes using ICT in a creative way?

17
Unplanned business / Mobility
“The best thing with the system is that I am available everywhere. “ Useful to receive phone calls when mobile May be an issue to receive (irrelevant) nurse calls in such
situations Absence is not totally unplanned, oral agreements exists
Backup nurse knows that she needs to take these nurse calls
The 15 sec. ringing is mentioned as interruptive by several nurses: When inside a patient room, when talking to a relative ++
Mobile device caters for mobility in positive ways, but may infringe on privacy and be interruptive

18
Interrupts from nurse calls during phone conversations: Proposal
The most important negative finding highlighted by almost all of the nurses was the following:
It is interruptive and also rude to the communication partner to receive nurse calls during a phone call.
Bip! Bip! Bip!
Suggestions:
Automatically avoid the nurse call to be delivered on phone (server side). Or avoid the sound on the ear (on the endpoint)
Use the presence panel in silent mode for peripheral group awareness

19
Automatic vs human judgement
Silent/no delivery of nurse call during phone call seems sensible to automate, The system knows when a phone call is ongoing Do not know the topic of the conversation Still: Similar to phone call during call without delivering ’call
waiting indication’
When hands are busy / user inside patient room: Impossible to ’guess’ this for the ICT system Do not automate this Do not assume manual updates at all times for this either Keep the system ”fitted for all types of contexts”
3 choices ’accept’, ’reject’ , ’ignore’ at all times
At lunch: allow manual setting of ’absence’, as this does not happen so frequently. Share this absence to all to increase group awareness

20
On CSCW and IS research: Implication for design of reserach papers
I lack technology descriptions and pictures in several IS/CSCW papers. 3 examples:
B&W does not show picture of the fixed buttons, impossible to judge level of awareness via fixed buttons and
lamps from their description
Scholl et al: writes about “call forwarding” from phone to pages Does not distinguish between CFU (unconditional) and CFNR
(on no reply, after a timer), which matters when context is mediated through a ringing phone
Technical architecture impacts the reliability of the systems, All new proposals should stick to existing architecture or have
very good reason to deviate All our proposals keeps old technical architecture

21
Questions?