1. - foundation center990s.foundationcenter.org/990_pdf_archive/860/... · 1. ; ombno 1545-0047...
TRANSCRIPT

1. ;
OMB No 1545-0047
Form 990 Return of Organization Exempt From Income Tax004
Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lungbenefit trust or private foundation)
Department of the Treasury
Internal Revenue Service 0- The organization may have to use a copy of this return to satisfy state reporting requirements.
A For the 2004 calendar year, or tax year beginning July 1 , 2004. and ending June 30 20 05
B Check it applicable
q Address change
q Name change
q Initial return
q Final return
q Amended return
PleoSo C Name of organization D Employer IdenUllcation numberuse IRS SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION 86: 0527381label orprint or Number and street (or P O box If mall is not delivered to street address) Room/suite E Telephone number
s2800 NORTH CENTRAL AVENUE 400 t 602 ) 798.2531
nstruSpecifi cICity or town stale or count and ZIP + 4nstruc• y ^' F Accounting method q Cash R1 Accrual
dons PHOENIX, AZ 85004 q oiher(epe,tM ►
q Applicat i on pending • Section 501 ( c)13) organizations and 4947( a)(1) nonexempt charitabletrusts must attach a completed Schedule A (Form 990 or 990-E1).
G Website: ► WWW.MERCYCAREPLAN.COM
J ► 501(c) 1 3 14
K Check here - q it the organizations gross receipts are normally not more than 525.000 Theorganization need not file a return with the IRS. but it the organization received a Form 990 Package
in the mail it should rile a return without financial data Some states require a complete return
L Gross receipts: Add lines 6b, Bb, 9b, and 10b to line 12 ► 1,044,734,366
YH and I are not applicable to section 527 organiza tions.H(a) Is this a group return for affiliates? Yes ® No
H(b) If "Yes,- enter number of affiliates ► ...............
H(c) Are all affiliates included? NIA q Yes q No(if No, attach a list See Instructions)
H(d) Is this a separate return filed by anorganization covered by a group ruling? q Yes B No
I Group Exemption Number ►M Check ► © if the organization Is not required
to attach Sch. 8 (Form 990, 990-EZ, or 990-PF).
Revenue, Expenses, and Changes in Net Assets or Fund Balances (See a e 18 of the instructions. )
1 Contributions, gifts grants and similar amounts received:
a Direct public support la
b Indirect public support 1b
c Government contributions (grants) 1c
d Total (add lines 1a through 1c) (cash $ noncash $ ) 1d
2 Program service revenue including government fees and contracts (from Part VII, line 93) 2 986,227,906
3 Membership dues and assessments 3
4 Interest on savings and temporary cash investments 4
5 Dividends and interest from securities 5 3,630,488
6a Gross rents 6a
b Less: rental expenses 6b
c Net rental income or (loss) (subtract line 6b from line 6a) 6c
7 Other investment income (describe ► 7
ea Gross amount from sales of assets other (A) Securities (B) Other
a than inventory _ 54,875,972 Ba
b Less: cost or other basis and sales expenses 55,367,365 Bb
c Gain or (loss) (attach schedule) <491.393> 8c
d Net gain or (loss) (combine line 8c, columns (A) and (B)) ( 8d <491,393>
9 Special events and activities (attach schedule) If any amount is from gaming, check here 0- q REMOVEDru a Gross revenue (not including $ of
contributions reported on line 1a) 9a
b Less direct expenses other than fundraising expenses 9b SAY 2006 O
Q c Net income or (loss) from special events (subtract line 9b from line 9a)9c 9
Ci 10af llG
U)
10a ross sales o inventory, less returns and a owancesco b Less: cost of goods sold 10b OGDEN, UT
c Gross profit or (loss) from sales of inventory (attach schedule) (subtract line 10b from line 10a) 1c
11 Other revenue (from Part VII, line 103) 1112 Total revenue (add lines 10, 2. 3, 4, 5, 6c, 7, Bd, 9c, 10c, and 11 ) 12 989,367,001
13 Program services (from line 44, column (B)) . - 13 902,964,932
14 Management and general (from line 44, column (C)) 14 71,183.845
CL 15 Fundraising (from line 44, column (D)) 15 NONE
u^ 16 Payments to affiliates (attach schedule) - 16 NONE
17 Total expenses (add lines 16 and 44, column (A)) 17 974,148,777
18 Excess or (deficit) for the year (subtract line 17 from line 12) 18 15,218,224
19 Net assets or fund balances at beginning of year (from line 73, column (A)) 19 39 280,875
20 Other changes in net assets or fund balances (attach explanation) ST^^T 20 <7,605,742>Z 21 Net assets or fund balances at end of year (combine lines 18, 19, and 20) 21 46,893,357
For Privacy Act and Paperwork Reduction Act Notice, see the separate instructions. Cat No 11282Y Form 990 (2004)
Z0

Form 990 (2004) Page 2
Statement of All organizations must complete column (A). Columns (B). (C), and (D) are required for section 501(c)(3) and (4) organizations
Functional Expenses and section 4941(aRl) nonexempt charitable tarsts but optional for others (See page 22 of the instructions )
Do not include amounts reported on line6b, 8b, 9b, 1ob, or 16 of Part I. = 3,
is -() Total (a) Program
services(C) Management
and general(0> Fundraising
22 Grants and allocations (attach schedule)
(cash $ noncash S ) 22 ,`°_ N=- y 5;;. ,=; =: ,_
23 Specific assistance to Individuals ( attach schedule ) 2324 Benefits paid to or for members (attach schedule ) 24
directors etc .25 Compensation of officers 25 NONE NONE NONE NONE,,
26 Other salaries and wages 26
27 Pension plan contributions 27
28 Other employee benefits 28
- _29 Payroll taxes 29.. .
30 Professional fundraising fees 30
31 Accounting fees 31 3 , 8611 NONE 3 , 861 NONE
32 Legalfees 32
.33 Supplies - 33, .
34 Telephone 34
.35 Postage and shipping 35-
36 Occupancy 36, . , , .
37 Equipment rental and maintenance 37
38 Printing and publications 38
39 Travel 39
and meetingsconventions40 Conferences 40,,
41 Interest 41
etc (attach schedule)depletion42 Depreciation 42,,
43 Other expenses not covered above (i temize): a STMT 3 43a 974,144 ,916 902 ,964,932 71 , 179,984 NONE
b 43b
43c
d 43d
e 43e
44 Total functional expenses (add lines 22 through 43)_ Organizationscompleting columns (8)•(D), carry these t otals to fines 13-15. 44 974,148 ,777 902 ,964,932 71 , 183,845 NONE
Joint Costs. Check ► q if you are following SOP 98-2
Are any joint costs from a combined educational campaign and fundralsing solicitation reported in (B) Program services? ► q Yes 0 No
If "Yes," enter (1) the aggregate amount of these joint costs S ; (i) the amount allocated to Program services $
(iii) the amount allocated to Management and general $ ; and (iv) the amount allocated to Fundraising $
FUMM Statement of Program Service Accomplishments (See page 25 of the instructions.)
What is the organization's primary exempt purpose? ----- .. .................................... . ....... Program ServiceExpenses
All organizations must describe their exempt purpose achievements in a clear and concise manner Stale the number (Regwled for 501(c)(3) and
of clients served, publications issued, etc Discuss achievements that are not measurable (Section 501(c)(3) and (4) (4) 019S. and 494 113)(1)Uusls. but s.) oroplimal
org an i za ti o ns a nd 4947(a)(1) nonexempt chartable trusts must also enter the amount of grants and allocations to others ) o lbcrs.)
a STMT 4
-------------------------------•-- ............................................... ...................... ..............(Grants and allocations $ NONE
b ......... ............................................................................................................
........... .............................................................................................................
......... ................................................................................................................(Grants and allocations $ }
c .............................................................................................................................. ............................. ..................................................................
........ ............................ .••---................---•--...--.....--...._.--..........--....._...........(Grants and allocations $ }
d ..........................................................................................................................
... ....................................... ................... ..........................................................(Grants and allocations $
e Other program services (attach schedule) (Grants and allocations $
f Total of Program Service Expenses (should equal line 44, column (B), Program services). . ► 902,964,932
Form 990 (2004)

Form 990 (2004) Page 3
j Balance Sheets (See page 25 of the instructions.)
Note: Where required, attached schedules and amounts within the description (A) (B)column should be for end-of-year amounts only. Beginning of year End of year
. . .45 Cash-non-Interest-bearing . 32,493,734 45 22,335,439. .
46 Savings and temporary cash Investments . • . , 6,410,085 46 13,641,381
47a 81,998,44547a Accountsreceivable
b Less: allowance for doubtful accounts 47b 780, 134 48,824,008 47c 81,218,311
48 _ i_..
48a Pledges receivable 48a -°'
b Less: allowance for doubtful accounts 48b 48c
49 Grants receivable 49
50 Receivables from officers, directors, trustees, and key employees
(attach schedule) 50
51a Other notes and loans receivable (attach
schedule) 51a
N b Less: allowance for doubtful accounts 51b 51c
52 Inventories for sale or use . . . . . . 52. . .
53 Prepaid expenses and deferred charges 398,390 53 544,610
54 Investments-securities (attach schedule)S/MT $ ► q Cost q FMV 66,314,475 54 73,897,641
55a Investments-land, buildings, andequipment: basis , . 55a
reciation (attach: accumulated deb L pessschedule) 55b 55c_
56 Investments-other (attach schedule) NONE 56 NONE
and equipment: basisbuildings57a land 57a, ,
b Less: accumulated depreciation (attach
schedule) 57b 57c
58 Other assets (describe ► STMT 6 ) <247,175> 56 713 ,9 32
59 Total assets (add lines 45 throu g h 58) (must equal line 74) 154,193,517 59 192,351,314
60 Accounts payable and accrued expenses 114 075,833 60 143,975,657
61 Grants payable 61
62 Deferred revenue 62
d 63 Loans from officers, directors, trustees, and key employees (attach
schedule) 63
64a Tax-exempt bond liabilities (attach schedule) 64aa
b Mortgages and other notes payable (attach schedule) 64b
65 Other liabilities (describe ► MINIMUM PENSION OBLIGATION ) 836,809 65 1,482,300
66 Total liabilities (add lines 60 through 65) 114,912,642 66 145,457,957
Organizations that follow SFAS 117, check here ► q3 and complete lines
0 67 through 69 and lines 73 and 74
c0/+ . . .. .67 Unrestricted 39,280,875 87 46,893,357
2. . .. . . .
68 Temporarily restricted 68.
m 69 Permanently restricted 69
check here ► q andOrganizations that do not follow SFAS 117
ILL
,complete lines 70 through 74.
0 or current fundstrust principal70 Capital stock 70,,
and equipment fundor land building71 Paid-In or capital surplus 71, ,,
or other fundsaccumulated Incomeendowment72 Retained earnings 72,,,
73 Total net assets or fund balances (add lines 67 through 69 or lines
Z 70 through 72;column (A) must equal line 19; column (B) must equal line 21) 39,280,875
='-s73 46,893,357
74 Total liabilities and net assets / fund balances (add lines 66 and 73) 154,193,517 74 192,351,314
Form 990 is available for public Inspection and, for some people, serves as the primary or sole source of Information about a
particular organization How the public perceives an organization In such cases may be determined by the information presented
on its return. Therefore, please make sure the return Is complete and accurate and fully describes, in Part III, the organization's
programs and accomplishments
Form 990 (2004) Page 4
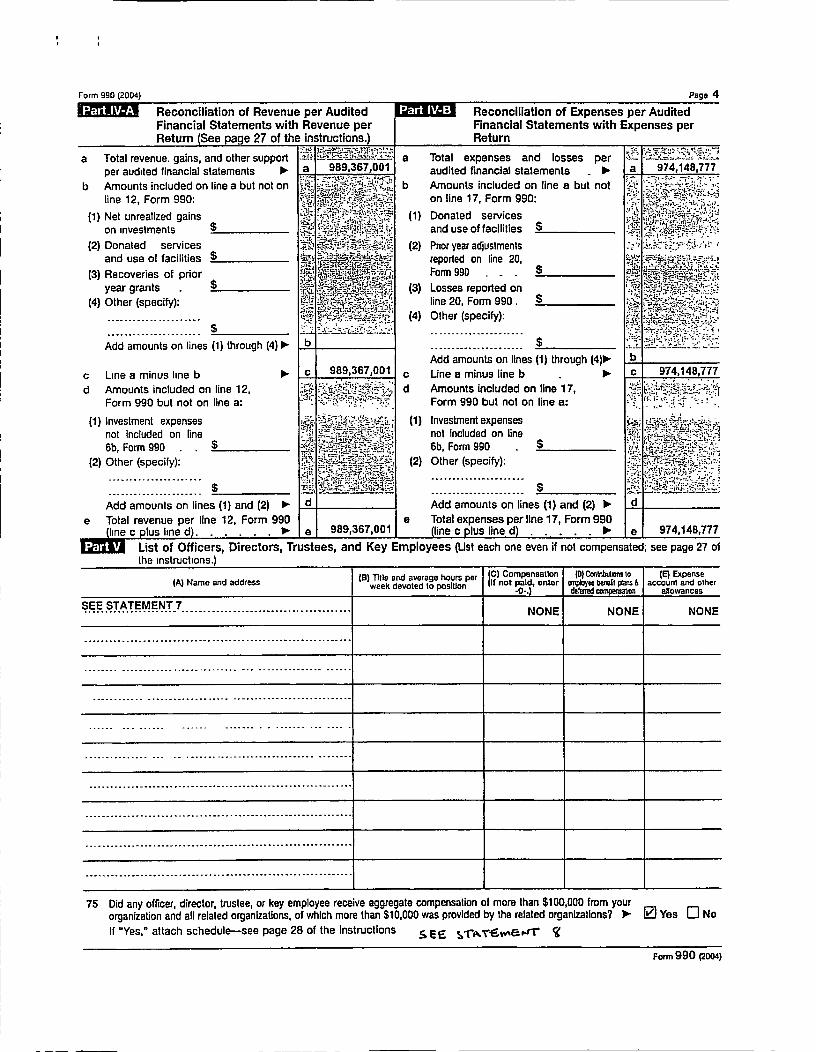
Reconciliation of Revenue per Audited Reconciliation of Expenses per AuditedFinancial Statements with Revenue per Financial Statements with Expenses perReturn (See page 27 of the instructions.) Return
a Total revenue . gains , and other support ='• - - a Total expenses and losses per -per audited financial statements ► 989,367,001 ►audited financial statements a 974,148,777
b Amounts included on line a but not on
-
b Amounts included on line a but not T-line 12 , Form 990 : on line 17, Form 990 :
(1) Net unrealized gains (1) Donated services
on investments $ ; t isl •;' F ,4s and use of facilities
(2) Donated services s ^- - (2) Prior year adjustmentsand use of facilities $ ;
E"reported on line 20,
p(3) Recoveries of prior +N
x ^=a s ti ' ^-Form 990 - r -., ` ^`'' '( ^rgc •5t
$year grants3:.'1•
p '.x,rte'-.,, .^, .•i;._ .=7,r„'t fir..,
, (3) Losses reported onC,• = ^y _y ,; R^^ -
.$(4) Other (specify): t ata; 4, s ,. line 20, Form 990,
=a•<:^a: (4) Other (specify):
Add amounts on lines ( 1) through (4) 111,- b ...................... $
Add amounts on lines (1) through b
c Line a minus line b ► c 989,367,001 c Line a minus line b ► c 974, 148,777
d Amounts included on line 12, d Amounts included on line 17 ,
Form 990 but not on line a: Form 990 but not on line a:
(1) Investment expenses x = `x'^% `- "• (1) Investment expenses
not included on line not included on line
6b, Form 990 6b , Form 990 $
(2) Other (specify): 2 Other (specify):
Add amounts on lines ( 1) and (2) ► d Add amounts on lines (1 ) and (2) ► d
e Total revenue per line 12, Form 990 a Total expenses per line 17, Form 990( line c plus line d. . ► e 989 ,367,001 line c plus lined . ► e 974 , 148,777
List of Officers, Directors, Trustees, and Key Employees (List each one even if not compensated; see page 27 ofthe instructions.)
(A) Name and address(B) Title and average hours per
week devoted to position
C) CompensationI II not paid, enter
-0-.
(D) Contnbutmns tom:pbgce bereU plan &deleted
(E) Expenseaccount and other
allowances
SEE STATEMENT 7...................... ....................................... NONE NONE NONE
--_....----••-• .......................................•-----..
........ ........................... _........ -•----........
............ -•--..._...--• ..... ........................
-•"-•- --• ----•- -•---- ......... .......... ....
............... ... ............. .................. ........
......................... .............................
.................... ..........................................
75 Did any officer , director, trustee , or key employee receive aggregate compensation of more than $100,000 from yourorganization and all related organizations , of whIch more than $10 ,000 was provided by the related organizations ? 1 Z Yes q No
If "Yes," attach schedule-see page 28 of the Instructions s r: E S-rA T-s:w Er•1' '
Form 990 (2004)

Form 990 (2004) Page 5
FU.WM Other Information (See page 28 of the instructions. ) Yes No
76 Did the organization engage in any activity not previously reported to the IRS? If 'Yes,' attach a detailed description of each activity 76 3
77 Were any changes made In the organizing or governing documents but not reported to the IRS? 77 3
If "Yes," attach a conformed copy of the changes .
78a Did the organization have unrelated business gross income of $1,000 or more during the year covered by this return? 78a 3
" has it filed a tax return on Form 990-T for this year?b If "Yes 78b,
79 Was there a liquidation , dissolution, termination , or substantial contraction during the year? If "Yes," attach a statement 79 3
80a is the organization related (other than by association with a statewide or nationwide organization) through common •- =:^membership , governing bodies , trustees, officers , etc., to any other exempt or nonexempt organization? 80a 3
b If "Yes," enter the name of the organization 10- HEALTHCARE WEST &........ .......... ______.CARONDELET HEALTH. ......................... ___. _.. and check whether it is q exempt or El nonexempt
81a Enter direct and indirect political expenditures See line 81 instructions 81a I NONE :? :}
b Did the organization file Form 1120 -POL for this year? . • 81b 3
82a Did the organization receive donated services or the use of materials , equipment, or facilities at no charge 3
or at substantially less than fair rental value? 82a
b If "Yes, " you may Indicate the value of these items here Do not include this amount'.
-r`
i;,• tics*,._:V•=K,::
as revenue in Part I or as an expense in Part II . (See Instructions in Part III ). 1 82b N/A =• s=^'- =: ; `
83a Did the organization comply with the public Inspection requirements for returns and exemption applications? 83a 3
b Did the organization comply with the disclosure requirements relating to quid pro quo contributions? 83b 3
84a Did the organization solicit any contributions or gifts that were not tax deductible? . . , - 84a 3
b If "Yes ," did the organization include with every solicitation an express statement that such contributionsor gifts were not tax deductible ? 84b +J a
or (6) organizations a Were substantially all dues nondeductible by members? . .85 501 (c)(4) (5) 85a h!JA, ,
b Did the organization make only in-house lobbying expenditures of $2,000 or less? - - 85b tJ h
If "Yes" was answered to either 85a or 85b , do not complete 85c through 85h below unless the organization : .; •-,-received a waiver for proxy tax owed for the prior year 1,_ .;;
c Dues, assessments , and similar amounts from members . . . . . . 85c NIA r;_,i V •̂ r̂7. ,Y
d Section 162 (e) lobbying and political expenditures 85d N/A {85e N/Ae Aggregate nondeductible amount of section 6033(e)(1)(A) dues notices _,,^, r,
I Taxable amount of lobbying and political expenditures (line 85d less 85e) 85f N/A
g Does the organization elect to pay the section 6033 (e) tax on the amount on line 85f? 85g N A
h If section 6033 (e)(1)(A) dues notices were sent , does the organization agree to add the amount on line 85f to itsreasonable estimate of dues allocable to nondeductible lobbying and political expenditures for the following taxyear? . . . . . 85h N A
86 501 (c)(7) orgs Enter : a Initiation fees and capital contributions included on line 12 86a N/A
b Gross receipts , included on line 12, for public use of club facilities 86b N/A
87 501 (c)(12) orgs Enter a Gross income from members or shareholders 87a N/A 1
b Gross income from other sources . (Do not net amounts due or paid to otheraz
i' W'__
sources against amounts due or received from them) 87b N/A fY ; "4 r
88 At any time during the year, did the organization own a 50% or greater Interest in a taxable corporation orpartnership , or an entity disregarded as separate from the organization under Regulations sections301 7701-2 and 301 7701 -3? If "Yes." complete Part IX B8 3
89a 501 (c)(3) organizations Enter. Amount of tax imposed on the organization during the year under.N/A N/A NIAsection 4912 lo- section 4955 10-section 4911 ►
b 501 (c)(3) and 501 (c)(4) orgs Did the organization engage in any section 4958 excess benefit transactionduring the year or did it become aware of an excess benefit transaction from a prior year? If "Yes," attach 3
a statement explaining each transaction - . . - . . . . . . . . . 89b
c Enter. Amount of tax imposed on the organization managers or disqualified persons during the year undersections 4912, 4955, and 4958 . . . . . . ► N/A
d Enter. Amount of tax on line 89c, above, reimbursed by the organization ► NIA
90a List the states with which a copy of this return is filed ► ARIZONA
b Number of employees employed In the pay period that Includes March 12, 2004 STMT 9 190b I NONE
91 The books are in care of ► THE ORGANIZATION Telephone no. ► (. 602 ) 798-2531
Located at ► _800 NORTH CENTRAL AVENUE #400; PHOENIX, AZ ZIP + 4 ► .............. 85004................ ..
92 Section 4947(a)(1) nonexempt charitable trusts filing Form 990.in
.lieu
.of
.Form 1041-Check here .
........ .► q
and enter the amount of tax-exempt interest received or accrued during the tax year . ._ . ► (92 ( N/A
Form 990 (2004)

r ,
Form 990 (2004) Page 6
M^l Analysis of Income -Producing Activities (See page 33 of the instructions.
Note: Enter gross amounts unless otherwise Unrelated business income Excluded by sect ion 512 . 513. or 514td
indicated .
93 Program service revenue :
(A)Business code
(B)Amount
(C)Exclusion code
(D)Amount
Rela e orexempt function
Income
a CAPITATION 837,869,155
b SUPPLEMENTAL PAYMENTS 75,884,496
c REINSURANCE 69 579,103
d THIRD PARTY/OTHER 2,895 152
e
f Medicare/Medicaid payments
g Fees and contracts from government agencies
94 Membership dues and assessments - .
95 Interest on savings and temporary cash investments
96 Dividends and Interest from securities 14 3 , 630.488
97 Net rental Income or (loss) from real estate: + _ =^ <'j- '71
<=-• .`_ :; ,__ - C :;
a debt-financed property
b not debt-financed property
98 Net rental income or ( loss) from personal property
99 Other Investment Income
100 Gain or (l oss) from sales of assets other than Inventory 18 <491,393>
101 Net income or Coss) from special events
102 Gross profit or (loss) from sales of inventory
103 Other revenue: a
b
cd
eand (E))(D)104 Subtotal (add columns (B) "" ' = ^''' = = 3,139 , 095 986 , 227,906, ,
105 Total (add line 104 , columns (B), (D), and (E)) . . . ► 989 , 367,001
Note: Line 105 plus line ld, Part I, should equal the amount on line 12, Part 1.
Relationshi p of Activities to the Accomplishment of Exempt Purposes (See page 34 of the instructions. )
Line No.7
Explain how each activity for which Income Is reported in column (E) of Part VII contributed importantly to the accomplishmentof the organization's exempt purposes (other than by providing funds for such purposes).
93 SEE STATEMENT 10
Information Regarding Taxable Subsidiaries and Disreg arded Entities (See a e 34 of the instructions. )
Name , address , andA)EIN of corporation,
partnership , or disregarded ent(tPercentage of
ownership Interest(C)Nature of activities (0)Total income End-ol year
assets
N/A %
o^
tnfnrmatinn Reeardino Transfers Associated with Personal Benefit Contracts (See Daoe 34 of the instructions.)
(a) Did the organization, during the year, receive any funds, directly or Indirectly to
(b) Did the organization, during the year, pay premiums, directl
Note : If "Yes" to (b), file Form 8870 and Form 4720 (see Instrv
Under penallie of perjury, I declare that I have a ad this etwn.and belief it e, corre and complete D tlon o pffilr(oI
Please
Sign atwe of officerHere
LINDA HUNT, CHAIRPERSON
Type or print name and title.
Paid Preparerssignature
Preparer's ms's name ( hklbe & YOUNG LLV^l
^a r.e^e a pia TWO N. CENTRAL . STE 2
(iLiii//Q
o
Use Only it self-employed),
n a personal benefit contract? q Yes q No

SCHEDULE A I Organization Exempt Under Section 501(c)(3)(Form 990 or 990-EZ) (Except Private Foundation) and Section 501(e), 501(f), 501(k),
501(n ), or Section 4947(a)(1) Nonexempt Charitable Trust
Supplementary Information-(See separate instructions.)Department of the TreasuryInternal Revenue sarvlce ► MUST be completed by the above organizations and attached to their Form 990 or 990-EZ
Name of the organization
SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
OMB No. 1545-0047
2004Employer Identification number
86;0527381
Compensation of the Five Highest Paid Employees Other Than Officers, Directors, and Trustees(See page 1 of the instructions. List each one. If there are none, enter "None."
( a) Name and address of each employee paid morethan $50 000
(b) Title and average hoursper week devoted to position ( e) Compensation
( d) Contributions toemployee benefit plans 8deferred compensation
(a) Expenseaccount and other
aAowances
NONE---•--.....-•-•--• ..................................... NONE NONE NONE
.................................... ..........
....---• ................................•-----..
Total number of other employees paid over$50,000 NONE
,. - `;-=th
Compensation of the Five Highest Paid Independent Contractors for Professional Services(See page 2 of the Instructions. List each one (whether individuals or firms). If there are none, enter "None.")
(a) Name and address of each Independent contractor paid more than $50.000 (b) Type of service (c) Compensation
SEE STATEMENT 11---- -....................... ... ...................................................
............................................. .......................... ...............
..................... ..................................................................
........... ..... ........................ ..................... ......... -.-..........
Total number of others receiving over $50 000 forprofessional services ► 268 1,
For Paperwork Reduction Act Notice, see the Instructions for Form 990 and Form 990-Fl. Cat No 11285F schedule A (Form 990 or 990-EZ) 2004

Schedule A (Form 990 or 990-EZ) 2004 cd(o . e.,7--7-3813 8 1 Page 2
Statements About Activities (See page 2 of the Instructions) Yes No
1 During the year , has the organization attempted to Influence national , state, or local legislation, Including anyattempt to influence public opinion on a legislative matter or referendum? If "Yes," enter the total expenses paid 3
or incurred in connection with the lobbying activities ► 5 NONE (Must equal amounts on line 38,Part VI -A, or line I of Part VI-B) . . . . . . . _
Organizations that made an election under section 501 (h) by filing Form 5768 must complete Part VI-A Other !'i ..' : 'zj' :•°J='
organizations checking "Yes" must complete Part VI -B AND attach a statement giving a detailed description ofthe lobbying activities
2 During the year , has the organization , either directly or indirectly , engaged in any of the following acts with any zvfq^ f;=' =substantial contributors , trustees, directors officers , creators, key employees, or members of their families, orwith any taxable organization with which any such person is affiliated as an officer, director, trustee, majority
'owner , or principal beneficiary? Of the answer to any question is "Yes," attach a detailed statement explaining the - =transactions)
a Sale , exchange , or leasing of property? _ 2a 3
b Lending of money or other extension of credit? 2b 3
c Furnishing of goods , services, or facilities? . . - , - . 2c 3
?Ad I' V'd Payment of compensation (or payment or reimbursement of expenses if more than $1,000) 7 SCE 4 3O 2d 3I
e Transfer of any part of its income or assets? 2e 3
3a Do you make grants for scholarships , fellowships , student loans, etc.? (If "Yes," attach an explanation of how 3
you determine that recipients qualify to receive payments.) . _ , _ - _ 3a
b Do you have a section 403(b) annuity plan for your employees? . . . . . . . . . . , . 3b 3
4a Did you maintain any separate account for participating donors where donors have the right to provide advice 3
on the use or distribution of funds? . . . . . . . . . . 4ab Do you provide credit counseling , debt management , credit repair, or debt negotiation services? 415 3
MM Reason for Non-Private Foundation Status (See pages 3 through 6 of the instructions.)
The organization is not a private foundation because it is: (Please check only ONE applicable box.)
5 q A church, convention of churches, or association of churches. Section 170(b)(1)(AXi)
6 q A school Section 170(b)(1)(A)(ii) (Also complete Part V.)
7 q A hospital or a cooperative hospital service organization Section 170(b)(1)(A)(Ii)
8 q A Federal, state, or local government or governmental unit, Section 170(b)(1)(A)(v)
9 q A medical research organization operated In conjunction with a hospital. Section 170(b)(1HA)(1ii) Enter the hospital's name, city,and state ► ........ -• .............................................••----........_..._....._.._
10 q An organization operated for the benefit of a college or university owned or operated by a governmental unit. Section 170(b)(1)(A)(v)(Also complete the Support Schedule In Part IV-A)
11a q An organization that normally receives a substantial part of its support from a governmental unit or from the general public Section
t 70(b)(1)(A)(vi) (Also complete the Support Schedule In Part IV-A)
llb q A community trust Section 170(b)(1)(A)(vi) (Also complete the Support Schedule In Part IV-A.)
12 q An organization that normally receives: (1) more than 33'/3% of Its support from contributions, membership fees, and grossreceipts from activities related to Its charitable, etc , functions-subject to certain exceptions, and (2) no more than 33'h% ofits support from gross investment Income and unrelated business taxable Income (less section 511 tax) from businesses acquiredby the organization after June 30, 1975 See section 509(a)(2) (Also complete the Support Schedule in Part IV-A)
13 ) An organization that Is not controlled by any disqualified persons (other than foundation managers) and supports organizationsdescribed in: (1) lines 5 through 12 above; or (2) section 501(c)(4), (5), or (6), if they meet the test of section 509(a)(2) (Seesection 509(a)(3).)
Provide the following information about the supported organizations. (See page 5 of the instructions.)
(a) Name(s) of supported organization(s)(b) Una number
from above
CATHOLIC HEALTHCARE WEST 07
CARONDELET HEALTHCARE NETWORK 07
14 q An organization organized and operated to test for public safety. Section 509(a)(4). (See page 5 of the Instructions.)Schedule A (Form 990 or 990-EZ) 2004

Schedule A (Form 990 or 990-Q) 2004 p fp- 067--1391 Page 3
' Support Schedule (Complete only If you checked a box on line 10, 11, or 12.) Use cash method of accounting.
Note: You may use the worksheet in the instructions for converting from the accrual to the cash method of accounting. (Jo'r Ai>PLie.AsL4rCalendar year (or fiscal year beginning in) ► (a) 2003 (b) 2002 (c) 2001 (d) 2000 (e) Total
15 Gifts , grants , and contributions received (Donot include unusual grants . See line 28.).
16 Membership fees received
17 Gross receipts from admissions , merchandisesold or services performed , or furnishing offacilities In any activity that is related to theorganization 's charitab le , etc., purpose .
18 Gross Income from Interest , dividends,amounts received from payments on securitiesloans (section 512 (a)(5)), rents , royalties, andunrelated business taxable income (lesssection 511 taxes) from businesses acquiredby the organization after June 30, 1975
19 Net income from unrelated business
activities not included in line 18
20 Tax revenues levied for the organization'sbenefit and either paid to it or expended onIts behalf
21 The value of services or facilities furnished tothe organization by a governmental unitwithout charge Do not Include the value ofservices or facilities generally furnished to thepublic without charge
22 Other income Attach a schedule. Do notinclude gain or (loss) from sale of capital assets
23 Total of lines 15 through 22
24 Line 23 minus line 17
25 Enter 1 % of line 23 = =_- - - ,
26 Organizations described on lines 10 or 11: a Enter 2% of amount in column (e), line 24 26a
b Prepare a list for your records to show the name of and amount contributed by each person (other than a ,R
governmental unit or publicly supported organization) whose total gifts for 2000 through 2003 exceeded the =•-amount shown in line 26a Do not file this list with your return. Enter the total of all these excess amounts ► 26b
column (e) _ . . . . . . . . . ►c Total support for section 509(a)(1) test: Enter line 24 26c,
d Add : Amounts from column (e) for lines : 18 19 L^F
► 122 26b 260 1. .
e Public support (line 26c minus line 26d total ) . . . . , ► 26e
f Public support percentage (line 26e (numerator) divided by line 26c (denominator)) . ► 26f
27 Organizations described on line 12: a For amounts Included in lines 15, 16, and 17 that were received from a "disqualifiedperson," prepare a list for your records to show the name of, and total amounts received In each year from, each "disqualified person "Do not file this list with your return. Enter the sum of such amounts for each year.
(2003) ... (2002) ........................... (2001) ....NOT APPLICABLE....................... (2000) ..........................
b For any amount included in line 17 that was received from each person (other than "disqualified persons"), prepare a list for your records toshow the name of, and amount received for each year, that was more than the larger of (1) the amount on line 25 for the year or (2) $5,000.(Include in the list organizations described in lines 5 through 11, as well as individuals.) Do not file this list with your return. After computingthe difference between the amount received and the larger amount described in (1) or (2), enter the sum of these differences (the excessamounts) for each year.
(2003) .......................... (2002) ........................... (2001) ........................... (2000) ..- .....................
c Add: Amounts from column (e) for lines: 15 16
17 20 21 ►
d Add- Line 27a total and line 27b total , ►
e Public support (line 27c total minus line 27d total) . . . , ►
( Total support for section 509(a)(2) test: Enter amount from line 23, column (e) , ► ( 27f
g Public support percentage (line 27e (numerator) divided by line 27f (denominator)) . - . . , ►h Investment Income oercentane (line 18. column (e) (numerator) divided by line 27f (denominator)). ►
28 Unusual Grants: For an organization described In fine 10, 11, or 12 that received any unusual grants during 2000 through 2003,prepare a list for your records to show, for each year, the name of the contributor, the date and amount of the grant, and a briefdescription of the nature of the grant. Do not file this list with your return . Do not Include these grants In line 15.
Schedule A (Form 990 or 980-EZ) 2004

Schedule A (Form 990 or 990-EZ 2004 96 - 052'1 3? t Page 4
Private School Questionnaire (See page 7 of the instructions)(To be completed ONLY by schools that checked the box on line 6 In Part IV) Ncri' AM-le- 6L-6
anization have a racially nondiscriminatory policy toward students by statement In its charter bylaws29 Does the orYes No, ,g
or to a resolution of its governing body? . . . . . . . . . . . .other governing instrument 29,
30 Does the organization include a statement of its racially nondiscriminatory policy toward students In all Its =y?';
brochures , catalogues , and other written communications with the public dealing with student admissions , '' =='^- ' ' =^and scholarships?programs 30,
31 Has the organization publicized Its racially nondiscriminatory policy through newspaper or broadcast media duringthe period of solicitation for students , or during the registration period If it has no solicitation program, In a way == • ==-'^ --^-v
olicy known to all parts of the general community it serves?that makes the 31p
If "Yes," please describe ; it "No," please explain ( If you need more space, attach a separate statement ) "'^''" ^''•i='•
............................................•. ....---.--...........---..-- .---...--...............
.__..._--_• ...............•-_._..-.....--....--.-------._._..._....._...._.._.....__'•.____•_......__.._....._...... i
... . .. ... . . .... ... ......... . .. . .. ... .. ............ .. ... ....... ............ ....... .............. ...
':s,-'' c'-i'-• _- _•._.--.. ................ ...... _
32 Does the organization maintain the following .
and administrative staff?facultya Records indicating the racial composition of the student body 32a, ,
b Records documenting that scholarships and other financial assistance are awarded on a racially nondiscriminatory
basis? 32b
c Copies of all catalogues, brochures, announcements, and other written communications to the public dealing. . . . . . . . . .and scholarships? .programswith student admissions 32a, . . .,
d Copies of all material used by the organization or on its behalf to solicit contributions? _ . - 32d
If you answered "No" to any of the above, please explain (If you need more space, attach a separate statement)
----- - -• ....... .... ...... ....................................................................................................................... ..................................... ...................... ................................
33 Does the organization discriminate by race in any way with respect to:
a Students' rights or privileges? . . . .
b Admissions policies?
c Employment of faculty or administrative staff? -
d Scholarships or other financial assistance?
e Educational policies?
f Use of facilities? .
g Athletic programs?
h Other extracurricular activities?
If you answered "Yes" to any of the above, please explain . ( If you need more space , attach a separate statement)
.................................. -•......--.----.----....•.--.....---.......------------...---.--- ........
-- ...--•-------------•----............................................................ .................................
------------------- ----------------------------------------------------------------------------•..--------------.---.....
34a Does the organization receive any financial aid or assistance from a governmental agency? - .
b Has the organization's right to such aid ever been revoked or suspended? .
if you answered "Yes" to either 34a or b, please explain using an attached statement
35 Does the organization certify that it has complied with the applicable requirements of sections 4 01 through 4 05 -AM-1 -.;:;4
of Rev . Proc. 75-50 , 1975-2 C. B. 587 , covering racial nondiscrimination ? If "No," attach an explanation 35Schedule A (Form 990 or 990-EZ) 2004

Schedule A (Form 990 or 990-EZ ) 2004 'J(o - o sZ7 3g I Page 5Lobbying Expenditures by Electing Public Charities (See page 9 of the instructions)(To be completed ONLY by an eligible organization that filed Form 5768) Nor A?p ej 8tX
Check ► a q if the organization belongs to an affiliated group , Check ► b q If you checked "a" and " limited control " provisions apply.
Limits on Lobbying Expenditures (°I To be completed
" "Affiliated group
totals for ALL electing(The term expenditures means amounts paid or Incurred .) organizations
36 Total lobbying expenditures to Influence public opinion (grassroots lobbying) 36
37 Total lobbying expenditures to Influence a legislative body (direct lobbying) 37
38 Total lobbying expenditures (add lines 36 and 37) 3839 Other exempt purpose expenditures 39
40 Total exempt purpose expenditures (add lines 38 and 39) 40
41 Lobbying nontaxable amount Enter the amount from the following table-
q t
" = ;:^ 't; 5T•
\
" ' °''
If the amount on line 40 is- The lobbying nontaxable amount Is- ^j^'` ^'' _ _^^ _ SJ:
t rye ` ry r^
={• =i= - -
Not over $500 ,000 20% of the amount on line 40
Over $500 ,000 but not over $1,000 ,000 $100 , 000 plus 15% of the excess over $500 ,000
Over $1,000,000 but not over $1 ,500,000 $175 ,000 plus 10% of the excess over $1,000,000 41
Over $ 1,500,000 but not over $17,000,000 $225 ,000 plus 5% of the excess over $1,500,000 + 3' '
Over $17,000,000 $1 , 000,000;.^; ^, =-, •;T i;___" :,;F;:;;: _ .
42 Grassroots nontaxable amount (enter 25% of line 41 ) . . , . . . . 42
43 Subtract line 42 from line 36 Enter - 0- if line 42 is more than line 36 43
44 Subtract line 41 from line 38 Enter -0- if line 41 Is more than line 38 , . . , . 44
Caution : If there is an amount on either line 43 or line 44, you must file Form 4720.
4-Year Averaging Period Under Section 501(h)(Some organizations that made a section 501(h) election do not have to complete all of the five columns below
See the Instructions for lines 45 through 50 on page 11 of the Instructions.)
ILobbying Expenditures During 4-Year Averaging Period
Calendar year (or (a) (b) (c) (d) (e)
fiscal year beginning in ) ► 2004 2003 2002 2001 Total
45 Lobbying nontaxable amount
i'1t:i.Y:.1,^Y:i `• ':itt.;ri ^%l!J:=- ^^:^.:.ti:•^^ e'TV:'^.,;: _,:t^^=-.=
' =46 Lobbying ceiling amount (150% of line 45(e)) L'!r;-;; 4 ^'4: =:;,r ;"^w i. '^ • . ; •'"'' ''-
47 Total lobbying expenditures ,
48 Grassroots nontaxable amount .- _ •^ '-'^x•-. - ,:v- ; i:ny^:•- n^ro7> ^7Vii: r_y:,i? - 'r 7^a,^: a x
49 Grassroots ceiling amount (150% of line 48(e)) t
50 Grassroots lobbying expenditures .
•jaar/oa LODDying ACTIVITY Dy IVonelecting I'ut7IIC t narttles N/A
(For reporting only by organizations that did not complete Part VI-A) (See page 11 of the instructions.)
During the year, did the organization attempt to Influence national, state or local legislation, Including any yes No Amountattempt to Influence public opinion on a legislative matter or referendum, through the use of:
a Volunteers
b Paid staff or management (include compensation in expenses reported on lines c through h.) _.-^. - _ .._
c Media advertisements
d Mailings to members, legislators , or the public , . . . . . _ _ . .
e Publications, or published or broadcast statements
f Grants to other organizations for lobbying purposes -
g Direct contact with legislators, their staffs, government officials, or a legislative body
h Rallies, demonstrations, seminars, conventions, speeches, lectures, or any other means -I Total lobbying expenditures (Add lines c through h.)
If "Yes" to any of the above, also attach a statement giving a detailed description of the lobbying activities.Schedule A (Form 990 or 990-EZ) 2004
Schedule A (Form 990 or 990-EZ) 2004 1?(o - o SZ'13f l Page 6
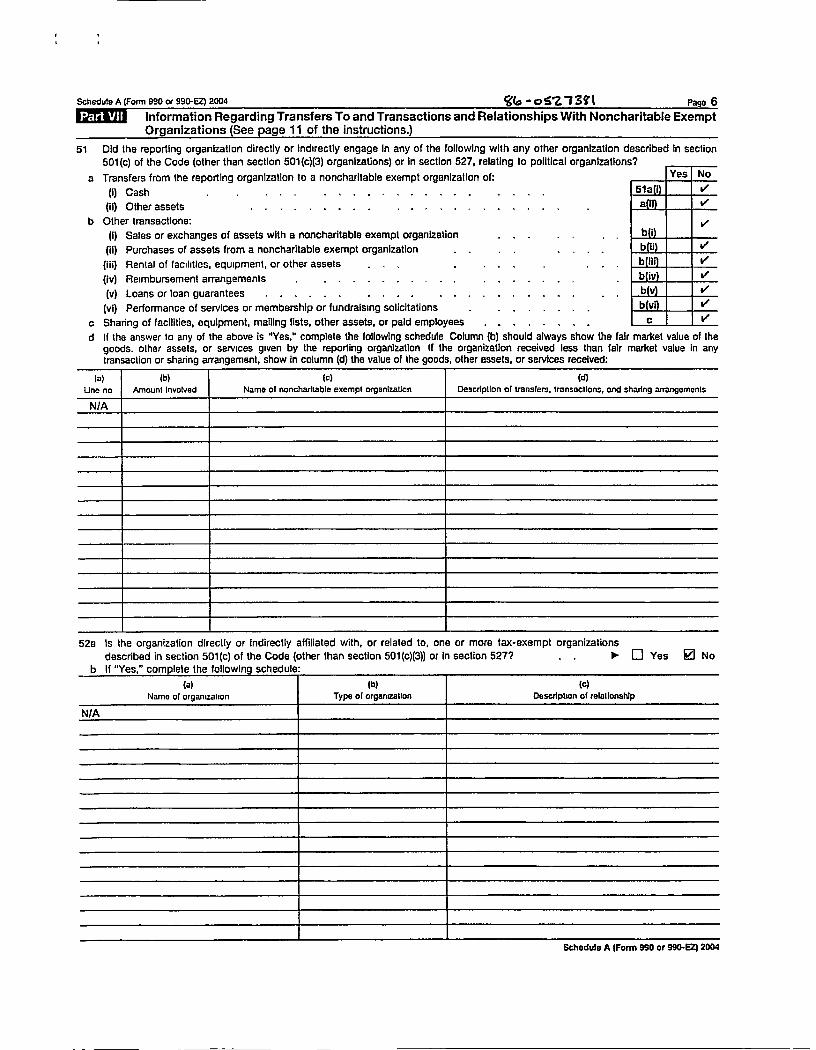
UOT^ Information Regarding Transfers To and Transactions and Relationships With Noncharitable ExemptOrganizations (See page 11 of the instructions.)
51 Did the reporting organization directly or Indirectly engage In any of the following with any other organization described In section501(c) of the Code (other than section 501 (c)(3) organizations) or In section 527, relating to political organizations?
a Transfers from the reporting organization to a noncharitable exempt organization of: Yes No
(I) Cash . . . _ . . . . . 51a 3
(ii) Other assets . . . . . . . . . . . . . . . . . . . . , a 3
b Other transactions: 3
(1) Sales or exchanges of assets with a noncharitable exempt organization b I
(it) Purchases of assets from a noncharitable exempt organization b i 3
(iii) Rental of facilities, equipment, or other assets b Ii 3
(iv) Reimbursement arrangements . . . . . . . . . . . . . . . . . b iv 3
(v) Loans or loan guarantees . . . . . . . b (y) 3
(vi) Performance of services or membership or fundraising solicitations . . . . . b (vi ) 3
c Sharing of facilities, equipment, mailing lists, other assets, or paid employees . - . , . , , . c 3
d If the answer to any of the above is "Yes," complete the following schedule Column (b) should always show the fair market value of thegoods. other assets, or services given by the reporting organization If the organization received less than fair market value In anytransaction or sharing arrangement, show in column (d) the value of the goods, other assets, or services received:
Schedule A (Form 990 or 990-EZ) 2004
52o Is the organization directly or Indirectly affiliated with, or related to, one or more tax-exempt organizations
described in section 501(c) of the Code (other than section 501(c)(3)) or in section 527? . . ► q Yes © No
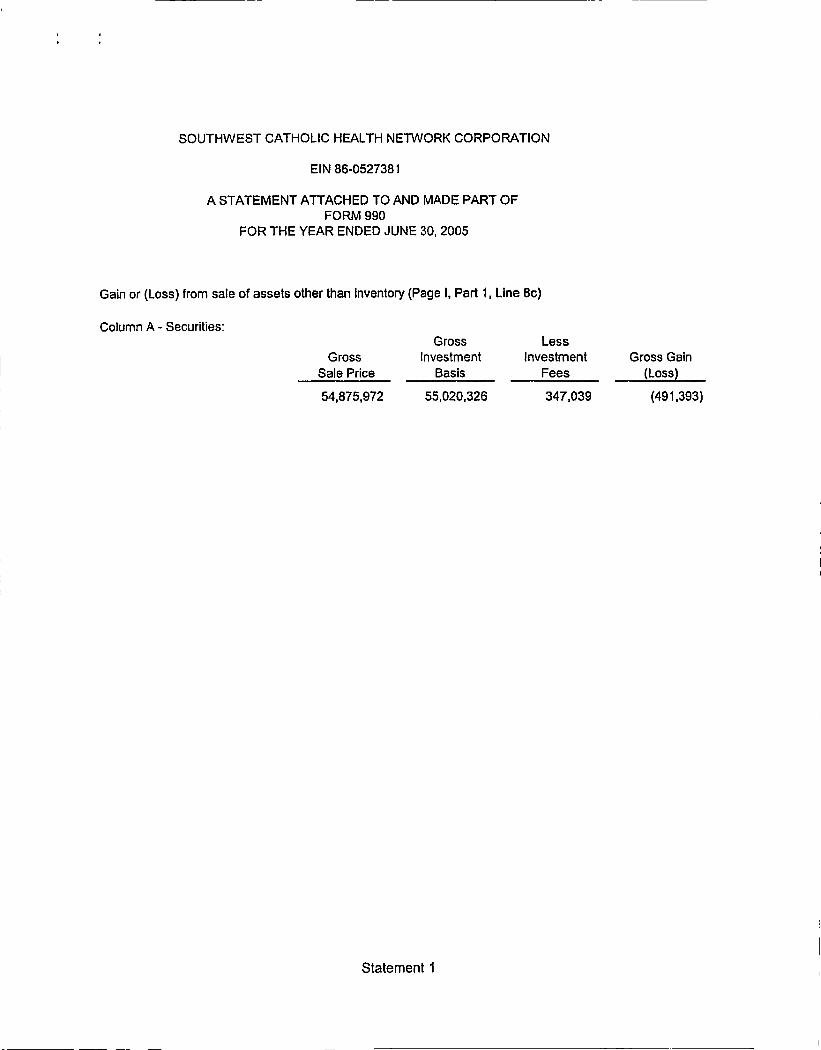
SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Gain or (Loss) from sale of assets other than Inventory (Page I , Part 1, Line 8c)
Column A - Securities:
Gross
Sale Price
54,875,972
GrossInvestment
Basis
55,020,326
LessInvestment
Fees
347,039
Gross Gain(Loss)
(491,393)
Statement 1

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Other Changes in Net Assets or Fund Balances (Page t. Part I, Line 20)
Net change in unrealized gains on investments:
Unrealized Gains at 6130104Unrealized Gains at 6/30/05
840,1354,043,691
$ 3,203,556
Minimum Pension ObligationEquity Distribution to Carondelet Health NetworkEquity Distribution to Catholic Healthcare West
Total Other Changes in Net Assets or Fund Balances
(809,298)(5,000,000)(5,000,000)
(7,605,742)
Statement 2

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Statement of Functional Expenses (Page 2, Part II, Line 43)
Program ManagementFunctional Expense Total Services & General
Hospitalization $ 262,867,332 $ 262,867,332 -Medical compensation 154,356,576 154,356,576 -Ancillary and other medical services 376,791,382 376,791,382 -Institutional 53,344,326 53,344,326 -Home and community based services 52,677,433 52,677,433 -Other healthcare expenses 2,927,883 2,927,883 -Management fees 69,403,958 69,403,958Other administration 1,155,468 1,155,468Insurance 620,558 620,558
Total Other Expenses $ 974,144,916 $ 902,964,932 $ 71,179,984
Statement 3

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Statement of Program Service Accomplishments (Page 2, Part III) and
Relationship of Activities to the Accomplishment of Exempt Purposes (Page 6, Part VIII)
Southwest Catholic Health Network (SCHN) is a not-for-profit venture sponsored by Catholic Healthcare
West - Arizona (CHW-Arizona) and Carondelet Health Care Corporation of Arizona (Carondelet) to.
--Promote and facilitate quality health care services, within the limits of availableresources and guided by fiscal responsibility, to the people of the Southwest withspecific concern for the poor and the disadvantaged
--Enhance the ability of the sponsors to fulfill their mission and to respond tocommunity needs
Through its contracts with Arizona Health Care Cost Containment System (AHCCCS), and the Arizona
Department of Economic Security, SCHN arranges identified health care services for over 250,000
needy residents of Arizona via subcontracts with various health care providers, including CHW-Arlzona
and Carondelet
Healthcare Group of Arizona (HCGA) is a component of the Arizona Health Care Cost ContainmentSystem (AHCCCS) AHCCCS is the state of Arizona ' s prepaid Medicaid program . HCGA is the nameof a prepaid coverage product aimed at small businesses with 40 or fewer employees which do notcurrently offer medical insurance to their employees . The provision authorizing the state to providecoverage for the working uninsured population is found in the the legislation which created AHCCCS
Statement 4

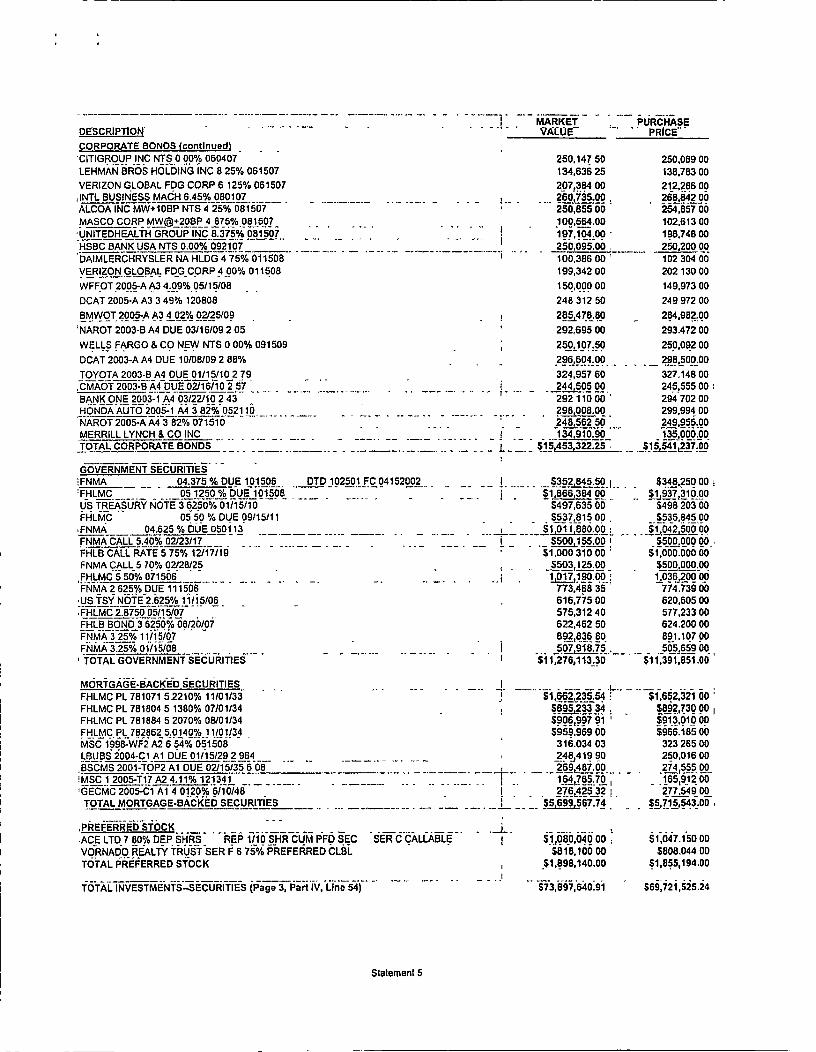
SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATIONEIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OF
FORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Investments-Securities Schedule (Page 3, Part IV, Line 54)
, DESCRIPTION
MARKETABLE SECURITIES
UBS SELECT _MONEY MARKET,ABBOTT LABSAETNA INCAFF IL IATED COMPUTER SVCS INC CL AALCOA INCALLIED CAPITAL CORP NEWALLSTATE CORPAMER INTL GROUP INCBANK O_F AMER CORPCISCO SYS INCCITIGROUP INCCOMCAST CORP NEW SPECIAL CL ACOMPUTER ASSOC INTL INCCONOCOPHILLIPSCVS CORP;DIGITAL R IVER INCEMERSON ELECTRIC COEXXON MOBIL CORPFAMILY DOLLAR STORESFI SHER SC I ENTIFIC INTL NEWGENL ELECTRIC COGRAINGER W W INCINTEL CORPINTL BUSINESS MACHLINCOLN ELEC HOLDINGS NEWLOWES_COMPANIES INCMARTEK BIOSCIENCES CORPMBNA CORP,MICROSOFT COWNEWELL RUBBERMAID INCPATTERSON-UTI ENERGY INCQUES_T_DIAGNOSTICS INCREPUBLIC SERVICES INCSARA LEE CORPSCHEINHENRY INCSUNTRUST BANKS INCTAKE-TWO INTERACTIVE SOFWRETARGET CORPVIACOM INC B NON VTGWASH GROUP INTL NEWWEATHERFORD INTL INC _ (BERMUDA)___ _ACE LTD BERMUDA ORDAETNA RC-_AMEREXPRESSCOAMERADA HESS CORPAPACHE CORPAPPLE COMPUTER INCBERKSHIRE HATHAWAY INC - ' CL BCA_BLEVISION SYSTEMS CORP_NY GROUP CLACAREMARK RX INCCEL_GENE CORPCISCO SYS INC
MARKET PURCHASEVALUE PRICE
$8,651,772 96 $8,651.772 96$308,763 00 $263,034 00
! $538,330 . 00 I $294,913 00$403`590 .00 $38_8,883.00$258,687.00 , $306,803 00$270,723 . 00 5228,179 00
• $633,350 .00 , $407,21600$499,660.00 $588 ,295.00$264,53800̂ $236.022005364,809 60 $342.06400$198,789.00 $204.09500S461 , 230.00 $445,04100$455,34360 F $443,95666 1$796,466 .46 $456,209 00$686,052 .00 5435,482 00$317,500 00 $324,370 00$225,468 00 $237 119 00
L __ $339,073.00 5273,009.00__$156 600 00 $162 565 00
$460_790 . 00 , $419 956 00$627.16500 1 $552,43000
,l 5405 ,446 00 5383,209 005268,006 . 00 $444,940 00$367 , 290.00
'$479,752.00 .
$308 2g5 66 $295 246 00$174,660 .00 , $160,448 00$201,188 00 $212,85100$4 1 8,560 00 $312,473 00$268,272 00 $338 556 00
{ $295,616 00 $273,522 00$247 .68700 5 145.517 00$426,160.00 , $272,87300$432.120 00 $289,586 005449,687 00 , S43 5.152005257 ,42400 , $ 195,41600$382 ,872 00 5357.875 00$171,78750 $149.581005473. 367 00 5386 052 005214.534 00 $229 483 00$393,624 00 $274.06100
_ . $431,951_00 ' $304 825 00$430.56000 $390,406 00$720,534 . 00 i $336,187 00$468,42400
_$426,146 00
$436.69100 $398 946 00$161,500 00 $ 168,82100$265,032.00 $266,29500$342,370 50 $285 949 00$286,580.00 $269,945.00$498,624 00 5324.232 00$634,920 .00 ' $481,127 00$667 600 00 5719,315 00
Statement 5

MARKET PURCHASEDESCRIPTION VALUE PRICE
MARKETABLE SECURITIES fconttnuedl
CONOCOPHILLIPS _ $459,920 .00 X320,848 00EXXON MOBIL CORP $5211,724 00 $484,782 00GENL ELECTRIC CO $516,285 00 $541 36700GILEAD SCIENCES INC $483,890 00 $388,182 00GOLDMAN SACHS GROUP INC $479.49400 $503 400 00GOOGLE INC CL A $794,205 00 $481,998 00INTEL CORP _ _- _ _ • ____. __ ._ _ _ _, _ __ • _____ _ ____i_ - $403,310.0 0 , $388,4 97.0_0_JOHNSON & JOHNSON COM $533.00000 $452,837 00LEHMAN BROS HOLDINGS INC $685 ,032 00 $554.11600MICROSOFT CORP $640,87200 $656,033 00
C CO INC HLDG COPENNEY J $273,416 00 $270 625 00.PEPSICOINC $269,650 .00 $262,56500PREMCOR INC $4 2_ 2,826 00 $2 32,1 79 00PROCTER & GAMBLE CO $385,075 00 $396,829 60.SPRINT CORP (FON) COMMON STOCK $584,597 00
-$562,76300
STARWOOD HOTELS &RESORTS _ , $430,275 00 $34 1082 00TRANSOCEAN IN_C_ORD_ $426,36300 $385,328 00'UNITEDHEALTH GROUP INC $677.820 00 $377,914 00VORNADO REALTY TRUST I $1 60,800 . 00 $161,84500
WALT DISNEY CO (HOLDING CO) DISNEY COM $450,722 00 $481.542 28WELLPOINT INC $320,344 00 $220,87300WYETH $649,700 00 $577,303 00
NCYAHOO I _ $564,795 00 , $504,571 00_ _TOTAL MARK_ETABLE SECURITIES $38,570 ,49742 $35,217,700.24
CORPORATE BONDSRELIASTAR FINCL CORP NTS 05.000% 103006 DTD100899 _ FC043000 $78,52 1 .25 $74 .72900
_FORD MOTOR CREDIT CO NTS B/E 06 .500% 0 12507
-- -_ _ I $503,590 . 00 , $536,480 00
65.250% 020107 DTDO13102BANK OF AMERCOR NTS FC080102 $510 ,275.00_I $4 97,655.00GENL ELEC CAP CORP NTS 05 000% 061507 DTDO60702 FC121502 $508,555 00 $522,775 00GOLDMAN SACHS GROUP INC 04 125% 011508 DTDO11303 FC071503 NTS $499,715 00 $512,220 00
BANK OF AMER CORP NTS 04 875% 091512 DTDO92502 FC031503 $462.825 00 $485,631 00NEW ENGLAND TEL&TELEG CO DEB 6 875% 100123 $510,690 00 $516.62500SPRINT CAPITAL CORP 6 875% 111528 $1 147 .880 00 $1 015 625 00AMER GENL FIN CORP 5 875% 071406 203,458 00 207,686 00
-COUNTRYWIDE HOME LN CCR 5.50% 080106 253,757 . 50.1 258_235 00CSFBDI RECTMW+20BP NTS 5. 875% 080106 255,212 50 260,17000COCA COLA ENTERPRISES 5 375% 081506 252 . 895 00 258,377 00
AMER EXPRESS CO NTS 5.50% 091206 253, 872 . 50 259.500 00
CAMPBELL SOUP CO 6.90% 1 01506 258,620 00 265,631 00BANK OF AMER CORP NTS 4 75% 101506 _ _ • 252_590 00 255,449 00
CONOCO FUNDING 5.45% 101506 _ _ _ _ __ _ __ ^••- _ _254,5 10.00f
2591372 00_
_BELLSOUTH CORP MW+15BP 500% 101506_ _
253.42000 257,35000
BOTTLING GROUP LLC NTS 2_45%° 101606 245.370 . 00 246,485 00
GOLDMAN SACHS GROUP INC 2 850% 102706 ' 197.124 00 198.210 00
WACHOVIA CORP NTS 4. 95% 110106_ 252675 OD 257,265 00
ALLSTATE CORP NTS 5 375% 120105 ^ 254,627 50 259.425 00
GENL ELEC CAP CORP 2 80% 011507 196 .490 00 197.586 00
BEAR STEARNS COS INC NTS 5.70% 011507 _ _ - - - f - 255,717 .50 261,14700OCCIDENTAL PETROLEUM CRP 5. 675%° 011507 102,531 00 104,79600
SPRINT CAPITAL CORP GLBL 6 00% 011507 102,47500 104,883 00
MBNA CORP MED TERM NTS 6.25% 011707 103,180 .00 10800,
UNITEDHEALTH GROUP INC 5 20% 011707 i- - r - 203,218 00 206 850 00
HOUSEHOLD FIN CORP 5 75% 013007
'
256,425 00 261.525 00
NTS 5. 125% 02 1507WELLS FARGO & CONEW 203 ,306 00_- _ 7250.00
:JOHN DEERE CAPITAL CORP 3.875% 03/07/07 144,479 .45 144 ,768 00 ,
MORGAN STANLEY DEAN WITT 5.80% 040107 179,879 00 183.81600LTTME^WARNER INC6.15% 050107AO 103 .472 00 105,969 00_
COMCAST CABLE COMMUNICAT 8 375% 050107 107,27600 110,877 00COUNTRYWIDE HOME LN CCR 5 625% 051507 255,147 50 261,47700CATERPILLAR FIN SERV SR 3 10% 051507 245 . 717 50 248.145 00
FPL GROUP CAPITAL INC 6.125% 051507 258,887 50 264,84700
_ _CHASE & CO 5 .25% 053007 _J P MORGAN _ _ _ _ __ - • _ __-_^_I_ _ _• _ 204,1 80 .00 ! . 20_8,228 00__
DISNEY WALT CO NEW NTS 5 375% 060107 _ - -. _ - - ' 102,257 00 104,333 00
Statement 5
MARKET PURCHASEDESCRIPTION VALUEr PRICE
CORPORATE BONDS fcontlnuedl
CITIGROUP INC NTS 0 00% 060407 250.147 50 250,069 00LEHMAN BROS HOLDING INC 8 25% 061507 134,636 25 138,783 00VERIZON GLOBAL FDG CORP 6 125% 061507 207,384 00 212,286 00J NTL BUSINESS MACH 6.45% 080_107 _ _ _ _ _ - 1 260,735 .00 , 26 8,84 2 00ALCOA INC MW+10BP NTS 4 25% 081507 250,855 00 254,857 00MASCO CORP MW +20BP 4875% 081 507 100,564 .00 102,613 00
•UNITEDHEALTH GROUP INC 8_375% 081507 197,104.00 198,748 00
HSBC BANK USA NTS 0.00% 092 107 250,095.00 , - 250,200 00
DAIMLERCHRYSLER NA HLDG 4 75% 011508 100,386 00
_
102 304 00
VERIZON G_LOBAL FOG CORP 4 00% 011508 199,342 00 202 130 00
WFFOT 2005-A A3 4-.0.9%-05/15/08 150,000 00 149,973 00
DCAT 2005-A A3 3 49% 120808 248 312 50 249 972 00
BMWOT 2005-A A3 4 02% 02/25/09 1 281478.80 284,982.00
NAROT 2003-B A4 DUE 03/16/09 2 05 292,695 00 293.472 00
WELLS FARGO & CO NEW NTS 0 00% 091509 250,107.50 250,092 00
DCAT 2003-A A4 DUE 10/08/09 2 88% - 296,604:00 - 298,500.00
TOYOTA 2003-B A4 DUE 01/15/10 2 79----- - ---- - - -- - - -
324,957 60-
327.14800- ----CMAOT 2003-B A4 DUE 02/16/10 2 57 244,50500 245,555 00
"BANK ONE 2003-1 A4 03122/10 2 43- --- -- - -- - - -
292 110 00 294 702 OD--------
HONDA AUTO 2005-1 A4 3 82% 052110 2 981008. 00 299.994 00NAROT 2005•A A4 3 82% 071510 248,562 50 249,955.00MERRILL LYNCH & CO INC _ _ - _ _ ___- __ - _ • _ _ -. 134,910.90 _ 135,000.00
TOTAL CORPORATE BONDS $15,453,322.25 $15,541Y37 0
GOVERNMENT SECURITIES
! FNMA 04.375 % DUE 101506 0TD 102501 FC 04152002__ 1 • _--_ - - $352,__84550 $348.25000_ _05 1250 % DUE 1 01508_FHLMC • $1,8 66,384 00 $1 937.310.00_
US TREASURY NOTE 3 6250% 01/15/10 $497,635 00 $498 203 00FHLMC 05 50 % DUE 09/15/11 $537.81500 $535.84500.FNMA 04.625 % DUE 050113 _ - - ---_-_ -•_ i_ ____ f,011,880.00 51,04 2,50000
FNMA CALL 5,40% 02/23/17 S500, 15500 !_ _ _ _ _
$500,000 00FHLB CALL RATE 5 75% 12/17119 31500 1 6 65 51,000.000 00FNMA CALL 5 70% 02/28/25 5503,125.00 _ $500,000.00
FHLMC 550% 071506 1,017, 190.00 1_036_200 00FNMA 2 625% DUE 111506 773,468 35 774.739 00-US TSYNOTE 2.625% 1 1/15106 616,775 00 620,605 00.FHLMC 2.8750 05115/07 575,312 40 577,233 00FHLB BOND 3 6250% 06120/07 622,462 50 624.200 00FNMA 3 25% 11/15107 - 892L836 80 89-1.10700FNMA 3.25%0 01/15/08
-507,918.75 505,65900
'TOTAL GOVERNMENT SECURITIES I $11,276,113_30 $11,391,651.00
MORTGAGE-BACKED SECURITIES ,FHLMC PL 781071 52210% 11/01/33 51,662,23 5.54 $1,652,321 00FHLMC PL 781804 5 1380% 07/01/34 - $895,_23334 $892,730 00FHLMC PL 781884 5 2070% 08/01/34 $906,997 91 ' $913,010 00
_ _FHLMC PL 782862 5.0 1 4 0% 11/01/34 $959,969 00 $966.18500MSC 1998 WF2 A2 654% 051508 316.034 03 323 265 00
LBU BS 2004-Cl A l DUE 01/15/29 2 964 248,41990 250,016 00
BSCMS 2001 -TOP2 Al DUE 02/15/35 6 08 __ _ -_ _ __ _-- • __ . __ . _ . 269,48i 60 _ 274,555 00!MSC 1 2005-T 17 A2 4.11% 12 1341 184,765.70 165,9
-1200
GECMC 2005-C1 Al 4 0120% 6/10/48 I . 276.425 32 I - 277_549 00
TOTAL MORTGAGE-BACKED SECURITIES $5&99 5q7_74 • _ • 55,715,543.00 .
, PREFERRED STOCK
-ACE LTD 7 80% DEP SHRS REP 1/10 SHR CUM PFD SEC SER C CALLABLE $1,080,040 00 $1,047.150 00VORNADO REALTY TRUST SER F 6 75% PREFERRED CLBL 5818,100 00 $808.04400TOTAL PREFERRED STOCK , $1,898,140.00 $1,855,194.00
TOTAL INVESTMENTS-SECURITIES (Page 3, Part IV, Line 54) S73,697,640.91 $69,721,525.24
Statement 5

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Other Assets (Page 3, Part IV, Line 58)
GENERAL & OTHERPROVIDER REFUNDSPREPAID PENSION ASSET
June 30, 2005 June 30, 2004
365,732 40,521- (287,696)
348,200 -
TOTAL 713,932 (247,175)
Statement 6

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
List of Officers, Directors and Trustees (Page 4, Part V)
Average ContributionsName and Address Title Hours per Compensation to Employee Allowances
week Benefit Plan
OFFICERS:Stan Aronovitch (1)2800 N. Central #400Phoenix, Arizona 85004
Susan Karlson (1)2800 N. Central #400Phoenix, Arizona 85004
Creighton Donovan (1)2800 N. Central #400Phoenix, Arizona 85004
Mike Klimansky (1)2800 N. Central #400Phoenix, Arizona 85004
DIRECTORS:Msgr. Edward RyleArizona Catholic Conference400 E. Monroe St.Phoenix, Arizona 85004
Linda HuntCatholic Health Care West - SW350 W. Thomas RoadPhoenix, Arizona 85013
Sally JeffcoatCarondelet Health Network2202 N. Forbes Blvd.
Tucson, Arizona 85745
John Orsini
Catholic Healthcare West500 W. Thomas Rd., # 710Phoenix, Arizona 85013
President 40 None& CEO
Chief 40 NoneFinancialOfficer
Chief 40 NoneFinancialOfficer
Chief 40 NoneOperatingOfficer
Chairman 18 per year None
Vice- 18 per year NoneChairman
Secretary 18 per year None
Treasurer 18 per year None
None None
None None
None None
None None
None None
None None
None None
None None
Statement 7

Charles A. Alfano, M.D 18 per year None None None500 W Thomas Road, Suite 850Phoenix, Arizona 85013
Robert Pryor, M.D. 18 per year None None NoneCatholic Healthcare West350 W. Thomas RoadPhoenix, Arizona 85013
Jose M. Santiago, M.D. 18 per year None None NoneCarondelet Health Network
2202 N. Forbes BoulevardTucson, Arizona 85745
Sister Kathleen Mary McCarthy 18 per year None None NoneCarondelet Health Network2202 N Forbes BoulevardTucson, Arizona 85745
Tom Pepping 18 per year None None NoneCarondelet Health Network2202 N. Forbes Blvd.Tucson, Arizona 85745
John Wray 18 per year None None NoneCatholic Healthcare West185 Berry St., Suite 300San Francisico, CA 94107
Sr. Margaret McBride 18 per year None None NoneCatholic Healthcare West350 W. Thomas RoadPhoenix, Arizona 85013
Thomas H. Hicks, M.D. 18 per year None None NoneUrological Assoc. of Southern Arizona6325 E. Tanque Verde Road
Tucson, Arizona 85715
$0 $0 $0
(1) A portion of the management fees paid to Schaller Anderson as listed on Statement Three of this returnis compensation for the provision of services as officers of this organization. The following employees ofSchaller Anderson of Arizona, LLC received compensation for the provision of services as officers of thisorganization: Title Compensation Contrib. AllowancesStan Aronovitch President CEO $351,451 $10,173 $4,985Susan Karlson Chief Financial Officer $193,807 $4,848 NoneCreighton Donovan Chief Financial Officer $ 49,615 None None
Mike Klimansky Chief Operating Officer $255,074 $17,389 None
Statement 7

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990
FOR THE YEAR ENDED JUNE 30, 2005
Officers, Directors,Trustees or Key Employees Receiving Aggregate Compensationof $100,000 or More, Of Which More Than $10,000 Was Provided by a
Related Organization (Page 4, Part V, Line 75)
Contributionsto Employee
Name Compensation Benefit Plan Allowances
Linda Hunt (1) 723,229 134,025 7,200
John Orsini (1) 599,339 178,001 7,200
Robert Pryor, MD (1) 406,825 1,247 0
Sister Margaret McBride (1) 181,817 14,702 0
John Wray (1) 1,028,632 101,445 7,200
Sally Jeffcoat (2) 573,361 32,370 0
Thomas Pepping (2) 279,387 23,962 0
Jose Santiago (2) 354,433 25,032 0
Sister Kathleen McCarthy (2) 207,920 3,822 0
(1) Compensated by an affiliated 501c(3) exempt organization, Catholic Healthcare West No compensationwas received from Southwest Catholic Health Network Corporation
(2) Compensated by an affiliated 501 c(3) exempt organization, Carondelet Health Care Corporation of Arizonaor its affiliates. No compensation was received from Southwest Catholic Health Network Corporation
Statement 8

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OF FORM 990FOR THE YEAR ENDED JUNE 30, 2005
Other Information (Page 5 , Part VI, Line 90b)
Explanation of number of employees employed In the pay period that includes.ine Number March 12, 2004-------------- ---------------------------------------------------------------------------------------------------------
90(b) This entity does not have any direct employees. Salary expense is Included in themanagement fees in Statement Three of this return. All salaries and wages are paidby Schaller Anderson of Arizona, LLC. Form 941 reporting such wages is filed underthe EIN form Schaller Anderson of Arizona, LLC (86-0842559).
Statement 9
SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OF FORM 990FOR THE YEAR ENDED JUNE 30, 2005
Relationship of Activities to the Accomplishment of Exempt Purposes (Page 6 , Part VIII)
Explanation of how each activity for which income is reported in column (E)Line Number ofpa^e 6: part VII contributed importantly to the accomplishment of exemptpurposes...........----------------
93 a, b & c All activity listed is used to coordinate and provide health care services to membersof Arizona's Medicaid and Developmental Disabled Population.
Statement 10

SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION
EIN 86-0527381
A STATEMENT ATTACHED TO AND MADE PART OFFORM 990 , SCHEDULE A
FOR THE YEAR ENDED JUNE 30, 2005
Compensation of five highest paid Independent contractorsfor professional services (Page 1, Part II)
Name and Address Type of Service Compensation
Southwest Diagnostic Imaging, LTD Medical Services 3,617,145
Dallas, TX
Obstetrix Medical Group of Phoenix PC Medical Services 2,283,838
Phoenix, AZ
Hospitalists of Arizona Medical Services 1 ,737,724
Los Angeles, CA
Ralph Green DDS PC Dental Services 1,193,969
Phoenix, AZ
Valley Oncology Associates - Chandler Medical Services 1,079,070
Chandler, AZ
Number paid >$50k = 268
Statement 11
Fes„ 8868 Application for Extension of Time To File an(Rev December 20U) Exempt Organization Return OMB No 1545-1709Department of the TreasuryInternal Revenue Service ► File a separate application for each return.
• If you are filing for an Automatic 3-Month Extension, complete only Part I and check this box ... .. ► U• If you are filing for an Additional ( not automatic ) 3-Month Extension, complete only Part Il (on page 2 of this form).
Do not comete Part 0 unless you have alread y been g ranted an automatic 3-month extension on a previousl y filed Form 8868.Automatic 3-Month Extension of Time - Only submit original (no copies needed)
Form 990 -T corporations requesting an automatic 6-month extension - check this box and complete Part I only .......... ► q
All other corporations (including Form 990-C tilers) must use Form 7004 to request an extension of time to file income tax returns.Partnerships, REMJCs, and trusts must use Form 8736 to request an extension of time to file Form 1065, 1066, or 1041.
Electronic Filing (e -Tile). Form 8868 can be filed electronically if you want a 3-month automatic extension of time to file one of thereturns noted below (6 months for corporate Form 990-T filers ). However , you cannot fde it electronically if you want the additional(not automatic) 3-month extension, instead you must submit the fully completed signed page 2 (Part 11) of Form 8868 . For moredetails on the electronic filing of this form , visit www. irs gov/efile.
Type or Name of Exempt Organization Employer Identification number
print SOUTHWEST CATHOLIC HEALTH NETWORK CORPORATION 86-0527381
File by thedue date forfiling yourreturn SeeInstructions
Number, street, and room or suite no. If a P.O. box see instructions.
town or post office, state. address, see instructions
Check type of return to be flied (file a se crate application for each return):
X Form 990 Form 990-T (corporation) Form 4720
Form 990-BL Form 990-T(sec. 401(a) or 408(a) trust) Form 5227
Form 990-EZ Form 990-T (trust other than above) Form 6069
Form 990-PF Form 1041-A Form 8870
• The books are in the care of ► THE ORGANIZATION
Telephone No ► 602 263-3872 FAX No. ►
• If the organization does not have an office or place of business in the United States , check this box . Ej• If this is for a Group Return, enter the organization 's four digit Group Exemption Number (GEN) . If this isfor the whole group , check this box ► q . If it is for part of the group , check this box ► and attach a list with thenames and EINs of all members the extension will cover.
1 I request an automatic 3-month (6-months for a Form 990-T corporation ) extension of time until 02/15 . 2006to file the exempt organization return for the organization named above . The extension is for the organization 's return for.► 8 calendar year or
► g tax year beginning 07/01 . 2004 , and ending 06/30 . 2005
2 If this tax year is for less than 12 months , check reason: Initial return Final return El Change in accounting period
3a If this application is for Form 990-BL, 990-PF , 990-T, 4720 , or 6069 , enter the tentative tax, less anynonrefundable credits . See instructions , , .. _ . $ NONE
b If this application is for Form 990-PF or 990-T, enter any refundable credits and estimated tax paymentsmade . Include any prior year overpayment allowed as a credit $ NONE
c Balance Due. Subtract line 3b from line 3a . Include your payment with this form, or , If required , depositwith FTD coupon or , if required , by using EFTPS (Electronic Federal Tax Payment System). Seeinstructions . . . . . . . . . . . . .. . . . .. . ... . . ... .. . . . ... . . . . . ... . . . . . . . . $ NODE
Caution. If you are going to make an electronic fund withdrawal with this Form 8868 , see Form 8453-EO and Form 8879-EO
for payment Instructions.
For Privacy Act and Paperwork Reduction Act Notice, see Instructions . Form 8868 (Rev . 12-2004)
ass4F8054 3 000
1546 V04-8
003453364

Form 8868 (Roy. 12.2004) e 2
• If you are filing for an Additional ( not automatic ) 3-Month Extension , complete only Part 11 and check this box X
Note : Only complete Part II if you have already been granted an automatic 3-month extension on a previously filed Form 8868
o If you are filin g for an Automatic 3-Month Extension , com p lete only Part I on page 1 ) .
Additional (not automatic) 3-Month Extension of Time - Must File Original and One Copy.
Typ eof Exempt Organization Employer Identification number
or a'print THWEST CATHOLIC HEALTH NETWORK CORPORATION 86-0527381
D File by the Number. street , and room or suite no If a P O box, see instructions }̂w For IRS use only
ca ,,, aye sate for 2800 NORTH CENTRAL AVENUE r r- fM riling the City , town or post office . state, and ZIP code For a foreign address , see instructions ?+ra -
returnsea
n w„ z=cT =i?° a^ o Instructions PHOENIX , AZ 85004 =iac`- xxt 'Nrv =rte' ?
C3 rn Check type of return to be filed ( File a se arate application for each return):
m Form 990 Form 990 -T(sec 401(a) or 408(a) trust ) Form 5227
Form 990-BL Form 990 -T (trust other than above ) Form 6069
M Form 990 -EZ Form 1041-A Form 8870M
W Form 990 -PF Form 4720
-- STOP : Do not complete Part If if you were not already granted an automatic 3-month extension on a previously filed Form 8868.
Ln • The books are in the care of ► THE ORGANIZATION
Telephone No 0- 602 263-3872 FAX No. ►If the organization does not have an office or place of business in the United States , check this box...... .......... 00.1
o If this is for a Group Return , enter the or anization's four digit Group Exemption Number (GEN ) If this is
for the whole group, check this box ► f . If it is for part of the group , check this box ► Li and attach a list with the
names and EINs of all members the extension Is for.
4 1 request an additional 3-month extension of time until 4 5 / 15 1-2 05 For calendar year , or other tax year beginning 07 / 01 /2004 and ending 06 / 30 /2005
6 If this tax year is for less than 12 months , check reason : Initial return Final return Change in accounting period
7 State in detail why you need the extension
ADDITIONAL TIME IS NEEDED TO COLLECT ALL THE INFORMATION NECESSARY TO
FILE A COMPLETE AND ACCURATE RETURN.
8a If this application is for Form 990-BL , 990-PF, 990-T, 4720 , or 6069, enter the tentative tax, less any
nonrefundable credits See instructions - - - , , , ... , , $ NONE
b If this application Is for Form 990-PF, 990-T, 4720 , or 6069 , enter any refundable credits and estimated
tax payments made . Include any prior year overpayment allowed as a credit and any amount paid
previously with Form 8868 , , , , , , , , , , , , , , , , , , , , , , , ,, , , , , , , , , , , , _ . , $ NONEc Balance Due . Subtract line Sb from line 8a. Include your payment with this form , or, if required , deposit
with FTD coupon or, if required , by using EFTPS ( Electronic Federal Tax Payment System) See
instructions $ NONESignature and Verification
Under ^enalties of perjury. I declare that I have examined this , Including accompanying schedules and statements and to the best of my knowledge and belief.
It Is INe correct andjconlplete and that I am authorized ID prep h form _
"" 1 - Notice 16 Applicant - To Be Completed by the IRSWe have approved this application Please attach this form to the organization ' s return
We have not approved this application . However, we have granted a 10-day grace period from the later of the date shown below or the duedate of the organization 's return ( including any prior extensions). This grace period Is considered to be a valid exie0ttiprl p^totherwise required to be made on a timely return Please attach this form to the organization 's return CA1 Ci' 81 I'J
^l11 f"(j
We have not approved this application After considering the reasons staled In item 7 , we cannot grant your request for an extension of timeto file We are not granting a 10-day grace period
R We cannot consider this application because It was filed after the extended due date of the return for which an extenslorl P"eUOO6
Other. FIELD DIRECTOR
By: SUBMISSION PRCCES: NG OGDEN
Director Date
Alternate Mailing Address - Enter the address if you want the copy of this application for an addilio th extension
returned to an address different than the one entered above.
o VL.1 VJ=L)Name
ERNST & YOUNG LLPType or Number and street ( include suite, room , or apt no.) or a P.O. box numberprint
TWO NORTH CENTRAL AVENUE , STE 2300B
2005City or town , province or state, and country (including postal or ZIP code)
PHOENIX . AZ 85004 O^^^r!'p^. ^T
4F8055 3 GOD
4XZOTD 1546 V04-8