1. fri 8am-break (cll, hl)
TRANSCRIPT

Hodgkin’sLymphomaChair:MichaelCrump,MDPrincessMargaretCancerCentre

CurrentManagementofLocalizedHodgkin’sLymphoma
MichaelCrump,MDPrincessMargaretCancerCentre
Toronto,Ontario,Canada

content
• DatafromprevioustrialsoftherapyinearlystageHL• Becauseweshouldn’tforgetwhatwelearnedinthepast
• NewdataonuseoffunctionalimagingtomanagelimitedstageHL• PETscansmightactuallybeingdoingforourpatientswhatwethoughttheycoulddo!
• Conclusions(sotherewillbetimeforquestions)
• Disclosures:none(exceptstrongopinions)

Whataretheusefulendpoints?• Freedomfromtreatmentfailure (FFTF)- thetimefromrandomassignmenttotheoccurrenceofoneofthefollowingevents:deathasaresultofanycause,progressivedisease,noCRattheendofprotocoltreatment,relapse,ornon-studytreatment
• Progression-freesurvival(PFS)- timefromstartoftreatmentuntilprogressionoflymphomaordeathfromanycause
• Event-freesurvival(EFS) – timefromstartofstudytreatmentuntildiseaseprogression,treatmentdiscontinuation(toxicity,preference,newRxwithoutprogression),deathfromanycause
• Timetoprogression(TTP)—startoftreatmenttoprogressionofdiseaseordeathfromlymphoma(othercausesofdeathcensored)

OlderdataaboutstageI,IIHL(thingsweknow….)• ClinicalriskfactorsdefinepatientpopulationswithearlystageHLwhocanbemanagedwithmoreorlessintensetherapy
• Omissionofradiation(inrespondingpatients)canresultingoodlongtermoutcomes;ie treatmentwithABVDalone
• OmissionofagentsfromABVDinearlyfavourableHLcancompromiseoutcomes
• InitialintensificationoftreatmentforearlyunfavourableHLimprovesprogression-freesurvival;lesscertaintyaboutoverallsurvival
• Breastcancerriskinyoungwomenafterradiationissignificantlylesswithsmaller(involved)radiationfields

Definition of Limited HL (stage I, II) Used in this Talk
GHSG early unfavourable – any of:- elevated ESR (>50)- 3 or more nodal areas- large mediastinal mass- extranodal lesions
EORTC early unfavourable – at least one:- age ≥ 50- 3 or more nodal areas- M-T ratio ≥ 0.35- ESR ≥ 50 (or B Sx: ≥ 30)
favourable – all others

HD10: without risk factors
Riskfactors:• Largemediastinal
mass• Extranodal
extension• ESR>50(30ifB’s)• >3nodalareas ABVDvsBEACOPP
20vs30Gy
HD11: with risk factors
Forearlyfavourable:2ABVD+20Gyisenough
Forearlyunfavourable:4ABVD+30Gyisoptimal…
AEngert,NEJM2010HTEich,JClin Oncol 2010

StandardArmTreatmentbyStrata
Favorable: STNI(35Gy)Unfavorable: ABVDx2+
STNI
ExperimentalArm:BothStrata:ABVDx2IfCR:x2more=4IfPR:x4more=6
PrimaryOutcome:12yroverallsurvival
CCTGHD-6:Design
Randomize
FavorableorUnfavorablebasedonanyof:
• Age> 40•MC/LDhistology• > 4sites• ESR> 50

MainFindings:HD.6extendedfieldRT(+/- ABVD)vsABVDalone
Meyer,NEnglJMed2012

ComparisonofHD.6(ABVDalone)vsGHSGHD10/11(2or4ABVD+20/30Gy IRFT)
Timetoprogression:HRfavoursIFRTProgression-freesurvival:HRfavoursIFRTbut95%CIexceeds1.0
EmergenceoflatedeathsnotrelatedtoHL
AEHayetal,AnnOncol 2013

EarlyCR(CTimaging)maypredictfavourableoutcome:HD.6subsetanalysis
CR<CR

HD13:omissionofdacarbazine orbleomycin,orboth,fromtheABVDregimenintreatmentofearly-stagefavorableHodgkin’slymphoma.
• Randomizednon-inferioritytrialwithfour-groupparalleldesign(assuming<6%difference predefinednon-inferioritymarginHR1.72)
• 2cyclesof:ABVD(n=566)vsABV(n=198)vsAVD(n=571)vsAV(n=167)
• Followedby30GyIFRTwithin4-6weeksofchemotherapy• RecruitmentofABVandAVwasstoppedearlyduetoexcesseventrate(thus,non-inferiorityanalysiscouldnotbedone)
• Primaryobjectives:FFTF• IncludedearlyfavourableclassicalHLandNLP(<10%)HLpatients
Behringeretal,Lancet2015

HD13:omissionofdacarbazineorbleomycin,orboth,fromtheABVDregimenintreatmentofearly-stagefavorableHodgkin’slymphoma.
ABVDCR:97%5yearPFS:93%5-yearFFTF:93.1%Early(1year)relapse:1%Laterelapse4%
AV ABV AVDCR:89% CR:95% CR:98%78.9% 82.1% 89.6%77.1% 81.4% 89.2%5% 5% 1%11% 9% 1%PD:5% PD:2% PD:<1%
NOTE:AVDgroupdidNOTmeetprotocolnon-inferioritydefinitionNOdifferenceinOSbetweengroupsBleomycinlungtoxicitywasrareoverall(1%) KBehringeretal,Lancet2015

Dose-IntensificationinEarlyUnfavorableHodgkin’sLymphoma:GHSGHD14Trial2escBEACOPP +2ABVDvs4ABVD(+30Gy IFRT)
G3-4toxicity:50.7%vs87.1%;TRMinarmB(2+2):0.52%Infection:3.4%vs7.3%SPM:2.2%vs2.0% VonTresckow etal.JCO2012

EfficacyRelapserate- 8.4%vs2.5%
FFTFat5years:87.7%vs94.8%:absolutedifferenceof7.2%;95%CI:3.8%to10.8%
PFSdifferenceof6.2%95%CI(3-9.5%)
NOdifferenceinOverallSurvivalOSat5years:97%

BreastcancerriskinfemalesurvivorsofHodgkin'slymphoma:Lowerriskaftersmallerradiationvolumes
MLDeBruinetal,JCO20095yearsurvivors,age<50attimeofHLtreatment

Predicting PFS of HL with Interim PETGallamini Criteria, Different Cohorts
Timing, criteria influence PPV and NPV
Le Roux Eur J Nucl Med Mol Imaging 2011 Gallamani et al J Clin Oncol 2007
PET post ABVD x 2 PET post ABVD x 4

NewdataonPET-guidedtreatmentofLimitedstageHL

PET Scan Criteria Used
EORTC H10: International Harmonization Project
- mass ≥ 2 cm: +ve if > mediastinal blood pool
- mass < 2 cm/normal size node: +ve if > background
RAPID trial: Deauville score
- positive if score 3,4,5 (> mediastinal blood pool)

Patients: Stage IA or IIA non-bulky HL (2/3: favourable by EORTC, GHSG criteria)
Initial treatment: ABVD x 3 → PET scan
4th cycleABVDthen30Gy IFRT
Randomize
30Gy
IFRT
Nofurthertreatment
PET +ve
PET -ve
UKRAPIDtrialdesign:CanFDG-PETinformtheuseofIFRTafterchemo?
D1,275%
D3-525%

ResultsofaTrialofPET-DirectedTherapyforEarly-StageHodgkinLymphoma(RAPID)• Randomizedcontrollednon-inferiority (pre-specifiedat7%)trial instageIA-IIAHodgkinLymphoma(excluded:bulkydisease(>33%internalthoracicdiameteratT5-T6))
• PETdirectedapproachofomittingradiotherapy- performedattheendofCycle3
• NegativePET:Deauvillescore1,2(lessthanorequaltomediastinalbloodpool)• Primaryoutcome:progression-freesurvival• 602patientsenrolledbetween2003-2010intheUK" 420randomized:183receivedIFRToutof209assigned
• Medianfollowupof60months• ITTandperprotocolanalyses
JRadfordetal.NEJM2015

PETnegativegroup(74.6%)
3-yearPFS94.6%vs90.8%ARdifference-3.8%(-8.8– 1.3)Per-protocolanalysis:3-yearPFS97.1%vs90.8%P=0.02
PET+group(25.4%)Median5-yearPFS87.6%
CONCLUSION:StageIAandIIAHLpatientswithoutmediastinalbulkwithnegativePETpost3cycleshaveaverygoodprognosisevenafteromittingradiotherapy.However,non-inferiorityofomittingradiationstrategytherapywasNOTmet
3-yearOS97.1%vs99%(NS)
JRadfordetal.NEJM2015

EarlyPositronEmissionTomographyResponse-AdaptedTreatmentinStageIandIIHodgkinLymphoma:FinalResultsoftheRandomizedEORTC/LYSA/FILH10Trial
• RandomizedphaseIIItrialofStageI-II(byCTscan)patientswithHL,favorable(F)andunfavorable(U)(EORTCdefinition)
Primaryobjective:safetyofINRTomissionafterePET responsetoABVDSecondaryobjective:efficacyofescBEACOPP intensification• FandUgroupsanalyzedseparately• 1o objective:PFSnon-inferiorityinPET- group• 2o objective:PFSsuperiorityinPET+group
• PETperformedonD22-25ofCycle2CriteriabyInternationalHarmonizationProjectifresidualmass≧2cm,+ve if>mediastinalbloodpoolnode<2cm:+ve ifuptake>surroundingbackground
Medianfollowupof4.5years MAndreetal.JCO2017

EORTCH10trialdesign
N=754
N=1196
Nrandomized*
371
376
583
595
MAndreetal.JCO2017*505PET–ve patientstreatedwithABVD+INRTfollowingsafetyamendment

PFSforePET negativepatientsITTanalysis
F-group:5yearPFS99%vs87%HR15.8CI(3.8-66.1)>prespecified non-inferiorityOS100%vs99.6%
U-group:5yearPFS92.1%vs89.6%HR1.45CI(0.8– 2.5)>prespecified non-inferioritymarginof2.1
OS96.7%vs98.3%
PFSforePET positivepatients(18.8%)ITTanalysis
5-yearPFS77.4%vs90.6%HR0.42(0.23– 0.74)OS89.3%vs96%(p=0.062)
**Morerelapsesoccurredinthepreviouslyinvolvednodesinbothradiationandnon-radiationgroups
***NoHD-relateddeathsoccurred6deathsduetoSPM

LimitedstageHLtherapy2017+
Limitedstage:• EF:2ABVD" PET:neg:IFRT20Gyor2ABVD
pos:escBEACOPP x2+30GyIFRT• EU:2ABVD" PET:neg:2ABVD+30GyIF(n)RTor6
pos:2escBEACOPP +30GYIF(n)RTAdvancedstage:• BulkystageI/II:ABVDx6+IFRT• (IIBE:escBEACOPP x6+RTforpositiveendoftreatmentPET)
EORTCH10
E2496
GHSGHD15
GHSGHD10,13,HD.6

LimitedstageHLtherapy2017+
• Earlyfavourable:2ABVD" IFRT20Gy2ABVD" PET:neg:IFRT20Gyor2ABVD
pos:escBEACOPP x2+30GyIFRT
• EU:2ABVD" PET:neg:2ABVD+30GyIF(n)RTor6pos:2escBEACOPP +30GYIF(n)RT
• BulkystageI/II:ABVDx6+IFRT(IIBE:escBEACOPP x6+RTforpositiveendoftreatmentPET)
EORTCH10
E2496/HD.7
GHSGHD15
GHSGHD10,13,HD.6
EORTCH10

Whatifradiationisn’tpartoftheplan,andtheinterimPETispositive?• eg patient1:youngwoman,earlyunfavorableHL:
• IFRTwouldinvolveaxilla,mediastinum,hilum" potentialdosetoRbreast
• WouldhavetotreatasadvancedHL• RATHLtrial:escBEACOPP x3-4• 73/172 (42%)withpositivePETscanhadstageIIHLatdiagnosis
• 3yrPFS67.5%(vs90%inH10withIFRT)(…1/3ofpatientswillneedASCT:reducedneedifIFRTincluded?)

Otherthingstofactorin
• EffectofageonprognosisofHL,riskofsecondcancer,CVD
• BaselinePETCTnowstandard(notpartofRAPIDorH10)• Morefavourablepatientswithlowerriskofrelapseoutsideradiationfield
• Fertilitypreservationoptionsforwomen,men:moreresourcesavailable(oocyteretrieval,IVFnowfunded)
• Choiceofchemotherapy,escalationapproachifPET+ve

References• 1.Carde Petal.EightCyclesofABVDVersusFourCyclesofBEACOPPescalated PlusFourCyclesofBEACOPPbaseline inStageIIItoIV,International
PrognosticScore≥3,High-RiskHodgkinLymphoma:FirstResultsofthePhaseIIIEORTC20012IntergroupTrial. JClinOncol. 2016Jun10;34(17):2028-36.
• 2.AndreMPEetal.Early PositronEmission Tomography Response-Adapted TreatmentinStageIand IIHodgkinLymphoma:Final Results oftheRandomized EORTC/LYSA/FILH10Trial.JClinOncol. 2017Mar14:JCO2016686394
• 3.Behringer Ketal.Omission ofdacarbazine orbleomycin,orboth,fromtheABVDregimen intreatmentofearly-stagefavourable Hodgkin'slymphoma (GHSGHD13):anopen-label,randomised,non-inferiority trial.Lancet. 2015Apr11;385(9976):1418-27.
• 4.vonTresckow etal.Dose-intensification inearly unfavorable Hodgkin's lymphoma:finalanalysis of the GermanHodgkinStudyGroupHD14trial.JClinOncol. 2012Mar20;30(9):907-13.
• 5.Borchmann Petal.Progression-freesurvivalofearlyinterimPET-positivepatientswithadvancedstageHodgkin'slymphomatreatedwithBEACOPPescalated aloneorincombinationwithrituximab(HD18):anopen-label,international,randomised phase3studybytheGermanHodgkinStudyGroup.LancetOncol. 2017Apr;18(4):454-463.
• 6.Advani RHetal.Randomized Phase IIITrialComparing ABVDPlusRadiotherapy With the StanfordVRegimen inPatients With Stages Ior IILocallyExtensive,Bulky Mediastinal Hodgkin Lymphoma:ASubset Analysisofthe NorthAmerican Intergroup E2496Trial. JClinOncol. 2015Jun10;33(17):1936-42.
• 7.PressOWetal.USIntergroup TrialofResponse-Adapted Therapy for StageIIIto IVHodgkinLymphoma UsingEarly InterimFluorodeoxyglucose-PositronEmission Tomography Imaging:Southwest Oncology GroupS0816. JClinOncol. 2016Jun10;34(17):2020-7.
• 8.JohnsonP.atal.Adapted TreatmentGuided by InterimPET-CTScaninAdvancedHodgkin's Lymphoma.NEnglJMed. 2016Jun23;374(25):2419-29.
• 9.Radfordetal.ResultsofatrialofPET-directedtherapyforearly-stageHodgkin'slymphoma.NEnglJMed. 2015Apr23;372(17):1598-607.

H10trialslides

74.6%hadnegativePETafterC3(vs.10.4%hadDeauville4-5)
Overall,similarpatientcharacteristicsofPET+andPET- groups
RAPIDPatientCharacteristics

RiskAdaptedTherapyinAdvancedHL:CurrentApproachesJonathanFriedberg- M.D.,M.M.Sc.
SamuelDurandProfessorofMedicine,UniversityofRochesterDirector,WilmotCancerInstitute,Rochester,NY,USA

Disclosures
• Bayer:DSMCactivities;Honoraria• SeattleGenetics:Researchsupport(toinstitution)

Defining risk in Advanced stage Hodgkin lymphoma in modern era
• IPS 7 (age, stage, hemoglobin, lymphocytes, WBC, sex, albumin) remains prognostic, but range has narrowed.
• IPS 3:• Age• Stage• Hemoglobin
Diefenbach et al, BJH 171:530

HD9trial10yearfollow-upResultsbyIPSgroup
• Randomized trial:• COPP/ABVD• BEACOPP• BEACOPPesc
• 10 year follow-up
• OS advantage for BEACOPPesc
Engert et al, JCO 27:4548

The premise of risk-adapted therapy
• It is desirable to avoid over-treatment in favorable risk patients to avoid late toxicities.
•Early identification of high risk patients may prevent treatment failure
•PET after 2 cycles appears highly predictive of treatment failure with ABVD.

Early PET in HL Combined Gallamini+ Hutchings Data PFS by PET2 and IPS
PET-
PET+
Gallamini, J Clin Oncol. 25:3746, 2007.

S0816 Intergroup Trial in Advanced HL
Group Clinical PET/CT Pathology/Biology
Accrual
SWOG Oliver PressJ. Friedberg
Richard Brown
James CookLisa Rimsza
155
CALGB Nancy BartlettAnn LaCasce
Heiko Schoder
Eric Hsi 97
ECOG Andy Evens J. Sweetenham
Andrei Iaguru
Randy Gascoyne
94
Others* -- -- -- 25
*NCCTG17,NSABP4,AMC4

S0816 Schema for HIV-negative patients
PET-Register ABVD x 2
PET+
ABVD x 4
BEACOPPescalated x 6
Primary end-points (2 year PFS)1. 2-year PFS will be improved from the historical 70% with
ABVD to 78% with risk adapted therapy.
2. Projected 48% 2 yr PFS for PET+ pt switched to e-BEACOPP (15-30% estimated PFS if continued on ABVD).
Press et al, JCO 34:2020

S0816: Demographics: N=371
Medianage: 32(range18-60)Gender 57%malesRace 80%whiteStageIII/IV 51%III;49%IVBsymptoms 61%Bulk>10cm 18%IPSScore 49%0-2;51%3-7HIV-positive 4%(N=13)
Press et al, JCO 34:2020

S0816: PFS/OS Outcomes
• The median length of follow-up among patients last know alive is approximately 49 months (range 2.1 – 82.5 months)
• Eighty-two patients have either progressed or died, for an estimated 4-year progression-free survival of 76% (95% CI: 71.1%, 80.5%)
• There have been 19 deaths, for an estimated 4-year overall survival of 95% (95% CI: 95.2%, 98.8%).
Friedberg,ISHL-Cologne,2016

0%
20%
40%
60%
80%
100%
0 24 48 72 96Months After Registration
Overall Survival
Progression-Free Survival
Patients at Risk Failed 4-Year Estimate
Overall Survival 336 19 95%
Progression-Free Survival
336 82 76%
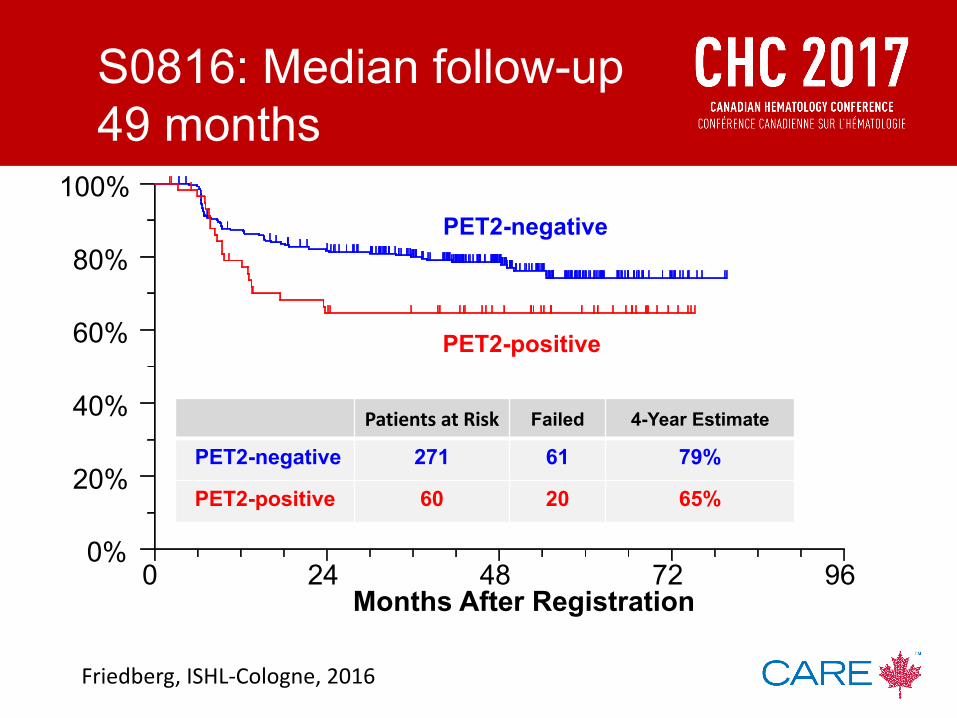
S0816: Median follow-up 49 months
Friedberg,ISHL-Cologne,2016
0%
20%
40%
60%
80%
100%
0 24 48 72 96Months After Registration
PET2-negative
PET2-positive
PatientsatRisk Failed 4-Year Estimate
PET2-negative 271 61 79%
PET2-positive 60 20 65%
S0816: Median follow-up 49 months
Friedberg,ISHL-Cologne,2016

0%
20%
40%
60%
80%
100%
0 24 48 72 96
Months After Final PET/CT performed
PatientsatRisk Failed 2-Year Estimate
PET3-negative 243 37 88%
S0816 PFS of patients who achieved CR (PET-3 negative)
Friedberg,ISHL-Cologne,2016

Secondary Malignancies
ContinuedABVD eBEACOPP
NonHodgkinLymphoma 1 1
KidneyCancer 1 1
Melanoma 1
SkinCancer 1
MedullaryThyroidCarcinoma
1
BoneMarrow/MDS 1
CervicalCancer 1
Nine of 336 eligible patients (2.7%) developed secondary malignancies, including 3 of 270 patients receiving ABVD (1%) and 6 of 49 (12.2%) who received at least 1 Cycle of eBEACOPP

S0816 long-term follow-upConclusions
• Response-adapted therapy appears to improve overall outcome over historic ABVD.
• Three quarters of the PFS events occurred in PET2 negative patients, indicating the limitations of this response-adapted approach, and emphasizing the need for additional biomarkers of failure at diagnosis.
• Twelve percent of patients who had a negative end of treatment PET ultimately had a progression event.
• It is still early, but second malignancies appear to be occurring at high rates in the BEACOPPesc arm.

The RATHL Trial: Summary
• In advanced HL, with a negative interim PET scan after two cycles of ABVD, it is safe to omit further bleomycin (↓ pulm toxicity) and reduce use of consolidation radiotherapy.
• Escalating therapy to escBEACOPP or BEACOPP14 for the 16% interim PET-positive patients delivers a promising PFS.
• Overall RATHL results better than previous ABVD trials, using more selective chemotherapy and much less radiotherapy.
PFS OS
Johnsonetal,NEJM,374:25

2 cycles ABVD Full dose, on schedule
PET 2-negative*PET 2-positive
4 cycles ABVD
PET2
PET 1 (Staging)Stage II (adverse), III, IV PS 0-3
Randomize
4 cycles AVD
Follow-up (no RT)
4 cycles BEACOPP-14
or 3 eBEACOPP
PET3
PET 3 -vePET 3 +ve
RT or salvageregimen
2 cycles BEACOPP-14
or 1 eBEACOPP
No RT
Studydesignedfora90%powertoexcludeAVDhavinga>5%
inferiorPFSthanABVD
*PET-negative=Score1-3

Primary endpoint: 3yr PFS for PET-negative randomized eligible patients
PFS
5yrPFSof81.6%(79– 84)
OS
5yrOS95.1%(93-96)
ABVD- AVD=1.2%(-3.7to+4.8)withinpre-definednon-inferioritymarginof5%
Trotmanetal,ICML,2017

PFS and OS in patients with positive PET2
5yrOS%5yrPFS%
• 16% patients PET2-positive• 5yr PFS 65.7% (58 – 73), 5yr OS 85.1% (78 - 90)• No significant difference between ESC and BEACOPP-14
Trotmanetal,ICML,2017

RATHL Conclusions
• In advanced HL with a negative interim PET after 2x ABVD, it is safe to omit further bleomycin, with minimal consolidation radiotherapy.
• Escalation for 16% interim PET+:• 5yr PFS 66% & OS 85%
• Overall results from RATHL: 5yr PFS 79.5% and OS 93.5%, support an interim PET-adapted approach.
• Similar to SWOG experience, there are still about 20% of patients who ultimately will relapse with this approach.
Trotmanetal,ICML,2017

1xeBEACOPP
5xRituximab/eBEACOPP
ArmA
The GHSG HD18 study:PET-guided therapy of advanced-stage HL
2xeBEACOPP
FDG-PET-2positive:
Endof therapy ANDresidualdisease ≥2.5cmANDpositivePET:RT
1xeBEACOPP 6
eBEACOPP
2xeBEACOPP
FDG-PET-2negative:
centrally reviewed FDG-PET/CT
5eBEACOPP
2xeBEACOPP
centrally reviewed PET/CT
ArmB ArmC ArmD
119
Final analysis of the GHSG HD18 trialBorchmann etal,Lugano2017

217 212 200 189 180 151 82
217 209 196 184 172 137 67
Pts. at risk
╵╵ ╵ ╵ ╵ ╵╵╵ ╵╵ ╵╵ ╵ ╵ ╵ ╵╵ ╵ ╵ ╵ ╵ ╵ ╵╵╵ ╵ ╵╵╵ ╵╵ ╵ ╵╵╵ ╵╵╵╵ ╵╵╵╵╵╵╵ ╵╵╵ ╵╵╵ ╵╵╵ ╵╵╵╵ ╵╵╵╵ ╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵ ╵╵╵ ╵╵ ╵ ╵╵╵╵╵ ╵ ╵╵╵╵╵╵╵ ╵╵╵╵ ╵╵ ╵╵╵╵ ╵ ╵ ╵ ╵ ╵
╵╵╵ ╵╵ ╵ ╵ ╵ ╵ ╵╵ ╵╵ ╵╵ ╵╵ ╵ ╵╵╵ ╵╵ ╵ ╵╵ ╵ ╵ ╵ ╵╵ ╵ ╵╵╵ ╵╵╵╵╵ ╵╵╵╵ ╵ ╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵ ╵ ╵╵╵ ╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵ ╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵ ╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵ ╵╵╵╵╵╵ ╵╵╵ ╵ ╵ ╵ ╵╵ ╵╵╵╵╵ ╵ ╵╵ ╵ ╵ ╵
0 12 24 36 48 60 72
Time [months]
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Ov
era
ll S
urv
iva
l ra
te
8x R-eBEACOPP, PET+8x eBEACOPP, PET+
5-yearestimate[95%-CI]8xeBEACOPP: 96.4%[93.8%to99.0%]8xR-eBEACOPP: 93.9%[90.6%to97.3%]difference: -2.5%[-6.8%to+1.7%]
UpdatedResultsoftheHD18Trial
Overall survival HD 18ITT analysis, median observation time 67 months
HR[95%-CI]1.62[0.70to3.75]Log-ranktest:p=0.3
HD15(no PET-2)8xeBEACOPP: 91.9%(89.4%to94.4%)
Borchmann etal,Lugano2017

The GHSG HD18 study:PET-guided therapy of advanced-stage HL
2xeBEACOPP
FDG-PET-2positive:
Endof therapy ANDresidualdisease ≥2.5cmANDpositivePET:RT
4xeBEACOPP
4xeBEACOPP
2xeBEACOPP
FDG-PET-2negative:
centrally reviewed FDG-PET/CT
2xeBEACOPP
centrally reviewed PET/CT
ArmC ArmD
121
Final analysis of the GHSG HD18 trialBorchmann etal,Lugano2017

270 240 206 133 84236 203 180 107 63
Pts. at risk
╵ ╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵ ╵╵╵╵ ╵╵ ╵╵╵ ╵╵╵ ╵ ╵╵ ╵╵╵ ╵ ╵ ╵ ╵╵ ╵╵╵ ╵ ╵╵╵╵ ╵╵╵ ╵╵╵╵╵ ╵╵ ╵╵ ╵╵ ╵ ╵╵╵ ╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵ ╵╵╵╵╵╵╵╵╵ ╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵ ╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵ ╵╵╵╵╵ ╵ ╵╵╵ ╵╵╵ ╵ ╵ ╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵ ╵ ╵╵╵╵╵╵╵ ╵╵╵╵╵ ╵╵ ╵ ╵╵ ╵╵ ╵╵╵╵╵ ╵ ╵╵
╵ ╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵
╵╵ ╵ ╵ ╵╵ ╵ ╵ ╵╵ ╵ ╵ ╵╵ ╵╵╵ ╵╵╵╵╵╵╵ ╵ ╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵ ╵╵ ╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵ ╵╵╵╵╵╵ ╵╵╵╵╵╵╵ ╵ ╵╵╵ ╵╵╵╵╵ ╵╵╵ ╵ ╵╵╵╵ ╵╵ ╵╵ ╵ ╵╵ ╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵ ╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵ ╵
╵╵╵ ╵ ╵╵ ╵ ╵ ╵╵ ╵╵ ╵
0 12 24 36 48
Time [months]
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
PFS
rate
uptake > liveruptake > mediastinum but <= live
FinalanalysisoftheHD18trial,03/2017
Progression-free survival HD18ITT analysis, PET-2-positive patients after amendment 2
3-yearestimate[95%-CI]Deauville3: 95.9%[93.2%to98.6%]Deauville4: 87.6%[83.0%to92.3%]difference: -8.3%[-13.6%to+2.9%]
HazardRatio[95%-CI] 3.08[1.54to6.18]Log-ranktest p=0.001Medianobservationtime36months
8cycles(priortoamend.2)
3-yearestimate[95%-CI]93·8%[90·0–97·7]90·7%[95%CI86·7–94·8]
Borchmann etal,Lugano2017

123UpdatedResultsoftheHD18Trial
Overall survival HD18ITT analysis after 6x eBEACOPP
506 475 422 264 166Pts. at risk
╵ ╵╵╵╵ ╵ ╵╵╵╵╵╵╵╵ ╵╵╵ ╵ ╵ ╵ ╵╵╵╵╵ ╵╵ ╵╵╵ ╵╵ ╵╵╵ ╵╵ ╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵ ╵ ╵╵╵╵╵ ╵╵ ╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵ ╵╵ ╵╵ ╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵ ╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵ ╵ ╵╵╵╵ ╵╵╵╵╵╵╵╵╵╵╵╵╵ ╵╵╵╵ ╵ ╵
0 12 24 36 48
Time [months]
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Ove
rall
Surv
ival
rate
6x eBEACOPP, PET+
3-yearestimate[95%-CI]6xeBEACOPP: 98.0%[96.7%to99.3%]
Medianobservationtime37months
8xeBEACOPP:97.1%[94.8%to99.4%]
Borchmann etal,Lugano2017

UpdatedResultsoftheHD18Trial 124
-PFS for PET-2-positive patients treated with eBEACOPP is better than expected also with 5 years FU. Definition of PET-positivity in HD18 might have been too conservative.
-Toxicity was manageable in this large phase III trial, there not a single case of TRM, and a low incidence of SN.
-Reduced treatment intensity of only 6 cycles of eBEACOPP does not result in a relevant loss of efficacy in this patient cohort, but significantly reduces the incidence of severe toxicities.
ØVery favorable overall survival results.
ØEagerly await de-escalation question for PET-2 negative patients.
HD18 for PET-2-positive patients
Summary and Conclusion
124

Summary: response-adapted trials in advanced stage HL
• Pet-2positivepatientsappeartohavesuperioroutcomesifusingBEACOPPesc comparedtohistoricaldatawithABVD.
• EliminatingbleomycinforPET-2negativepatientsissafeanddoesnotimpactefficacy.
• AsdataevolveonPET-2negativepatientsinGermantrials,Iexpectwearemovingtowardamoreunifiedapproachformostpatients.
• However,PETisnotfinalanswerforABVD-treatedpatients,as20%ofpatientstreatedwithaPET-adaptedapproachstillrelapse;majorityPET-2negative.

The future:Risk-adapted therapy
• 23-genepredictorscorenotvalidated.• Otherpossiblepredictors:
• Metabolictumorvolume• SerumTARC• Macrophagecontent• Uniquepredictorsforimmunotherapy
• Weneedvalidatednovelbiomarker(s)todefinepatientsatdiagnosisdestinedtofail,tofacilitateprecisionmedicinetrials.
• Untilthen,“bruteforce”trialsenrollingallpatientswithadvancedstagediseasewillbetherule.
ThankYou
EnjoyTorontoandCHC2017!