1 imaging of monstrous m. haghighi md2 … · craniopharyngioma: a pictorial essay ... basilar...
TRANSCRIPT

Iran J Radiol 2010, 7(2) 79
NEURORADIOLOGY
Imaging of Monstrous Craniopharyngioma: A Pictorial Essay Craniopharyngioma is usually a mixed solid and cystic suprasellar tumor, which usually occurs in children and adults in the fourth and fifth decades of life. The tumors are histologically benign and slow growing, but focal invasion and peritumoral fibrosis leads to high tumoral recurrence after surgery. We had 11 patients admitted with different symptoms such as headache, nausea, vomiting and visual loss in whom extensive craniopharyngioma was proved after surgery. In some patients, primary imaging studies were reviewed. In others who presented with new onset symptoms several years after surgery, brain CT scan and MRI studies were performed. On brain CT scan of most cases, a mixed cystic and solid suprasellar mass with calcifications in both solid and cystic parts was detected. In this article, we present some cases of large cra-niopharyngioma with interesting extensions and invasions to adjacent brain structures.
Keywords: Craniopharyngioma, Computed Tomography, Magnetic Reson-ance Imaging
Introduction
raniopharyngioma is a histologically benign slow-growing tumor (WHO
grade Ι),1,2 which accounts for approximately 3% of all intracranial tumors.3,4
It has a bimodal age distribution with the first peak in children and the second in
adults at age 40-60 years. It is not predominant in any sex or race.1
It originates from the embryonic precursor of adenohypophysis which is called
Rathke’s pouch.1,5,6 The adenohypophysis and infandibulum migrate from the
pharynx to the sella turcica during fetal life. This fact shows that craniopharyn-
giomas may occur anywhere along this migration tract.1
Craniopharyngioma has three histological types: adamantinomatous, papillary
and mixed.1 The adamantinomatous type predominantly occurs in children.
They are classically cystic tumors with a solid component.1,2,7 The fluid in the
cyst is usually similar to motor oil.8,9 It contains high protein materials, choles-
terol crystals and blood products. The solid part contains calcification, squamous
or columnar epithelium, fibrosis and inflammation. Complete resection of the
tumor is difficult because of this fibrosis and dense adhesion to adjacent struc-
tures. This issue leads to frequent recurrence of tumor in patients treated with
surgery. The papillary type predominantly occurs in adults. It has only a solid
component typically without calcification.1,7 This type is more encapsulated and
has less recurrence after surgical resection.1
Because of the slow-growing nature of tumors, the symptoms develop insi-
diously and the common interval between onset of symptoms and diagnosis is 1-
2 years.2 The most frequent reported symptoms are headache, nausea, vomiting
and visual disturbance. Growth failure and hypogonadism are also encountered
frequently. Bitemporal hemianopia is the most frequent disturbance of the visual
C
H.R. Haghighatkhah MD1 M. Sanei Taheri MD1 M. Haghighi MD2 S. Shahzadi MD3 Sh. Birang MD4
1. Associate Professor, Department of Radiology, Shohada Tajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. 2. Resident of Radiology, Shohada Tajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. 3. Professor of Neurosurgery, Shohada-Tajrish Hospital, Shahid Beheshti Uni-versity of Medical Sciences, Tehran, Iran. 4. Associate Professor, Department of Radiology, Loghman Hospital, Shahid-Beheshti University of Medical Sciences, Tehran, Iran. Corresponding Author Shirin Birang Department of Radiology, Loghman Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Tel: +9821 5541 1411 Fax: +9821 5541 1411 E-mail: [email protected] Received September 2, 2009; Accepted after revision March 8, 2010 Iran J Radiol 2010;7(2):79-89

Haghighatkhah et al.
80 Iran J Radiol 2010, 7(2)
field. Other presentations include seizures, preco-
cious puberty, inappropriate secretion of ADH, hear-
ing loss and epistaxis.10
In patients with raised intracranial pressure or rapid
visual function deterioration, we must focus on sur-
gical treatment of hydrocephalus or tumor cyst de-
compression. The main management of tumor is sur-
gery with an attempt to gross total resection of tu-
mor, but in cases with extensive tumors in which to-
tal resection is impossible, limited resection with tu-
moral debulking is recommended to reduce the tu-
moral compression of optic pathways and to help CSF
drainage. Limited surgical resections are followed by
radiotherapy.2
One of the most interesting issues in craniopharyn-
gioma imaging is its extension and invasion to mul-
tiple brain structures, which is best appreciated on
MRI. These tumors have different patterns of exten-
sion such as superior extension from the suprasellar
region with compression of the third or lateral ven-
tricles, lateral extension to parasellar areas, cavernous
sinuses and temporal lobes, anterior extension to
frontal lobes with superior displacement of A1 seg-
ment of the anterior cerebral artery and anterior
communicating artery, posterior extension to perime-
sencephalic cisterns, brain stem, compression of the
basilar trunk and involvement of cerebellum and su-
perior cerebellar cistern and finally inferior extension
to sella, sphenoid and ethmoidal sinuses and nasopha-
rynx. Identifying these patterns of extension can help
us in the surgical management of craniopharyngi-
omas to decide whether total or partial resection is
recommended and to differentiate these tumors from
other extensive skull-base tumoral lesions.
We encountered 11 patients with surgically con-
firmed craniopharyngioma. These are extensive tu-
mors with unusual extension to their neighboring
brain structures. Their brain CT scan and MR images
are reviewed.
Case Presentation
Patient 1
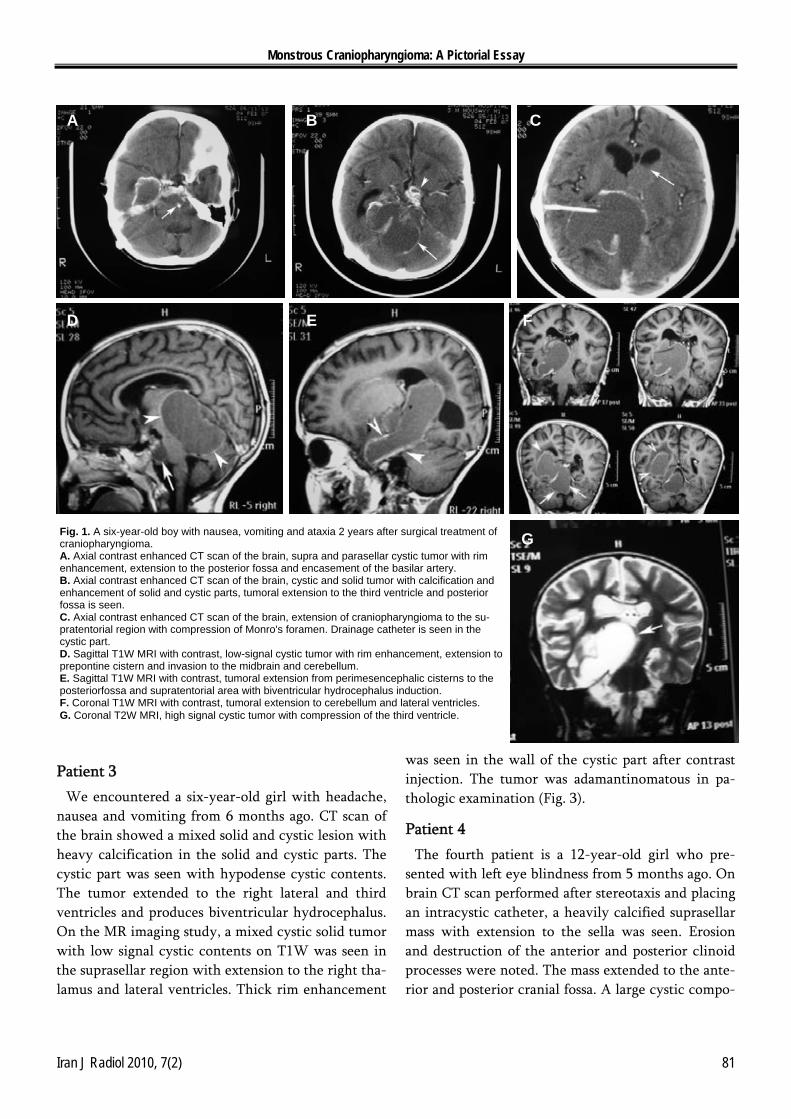
The first patient is a six-year-old boy who presented
with nausea, vomiting and ataxia 2 years after surgic-
al treatment of craniopharyngioma. Brain CT scan
showed a tumoral lesion in the suprasellar region
with extension to the middle and posterior cranial
fossa. The tumor is predominantly cystic with solid
components. Eggshell calcification is seen in the cys-
tic part. The solid part is also calcified in both pop-
corn and solid lump appearances. Right temporal cra-
niotomy and an intracystic catheter are noted as well.
On brain MRI study, the mass is seen with both sol-
id and cystic parts. The cystic part is hypointense on
T1W and hyperintense on T2W images. After con-
trast injection, homogeneous enhancement is seen in
the solid part and rim enhancement is also seen in the
cystic part. The tumor extends from the suprasellar
region to sella and then from the perimesencephalic
cisterns to the posterior fossa, superior cerebellar cis-
tern and cerebellum. It also extended to the right lat-
eral ventricle and third ventricle and produces biven-
tricular hydrocephalus due to compression of fora-
men of Monro. Pathologic examination revealed an
adamantinomatous craniopharyngioma (Fig. 1).
Patient 2
The second patient is an 11-year-old boy who pre-
sented with visual loss 1.5 years ago. Brain CT scan
revealed a tumoral lesion with both solid and cystic
parts in the suprasellar and sellar regions. Calcifica-
tion is seen in the lesion, which has eggshell configu-
ration in the cystic part and lumpy appearance is also
seen in the solid part. The tumor extends to the post-
erior cranial fossa. It also extends to the third ven-
tricle from its superior margin. On MRI study, a T1
isointense and T2 hyperintense cystic lesion is seen in
the suprasellar region with extension to sella turcica
and involvement of the left parasellar region with left
carotid artery encasement and left cavernous sinus
invasion. The tumor extended to the posterior fossa
and compressed the brain stem at its posterior mar-
gin. It deviated the pons, midbrain and fourth ven-
tricle to the right. In addition, it compressed the basi-
lar trunk at its posterior margin. At the superior mar-
gin, the tumor extended to the third ventricle and
produced biventricular hydrocephalus. After contrast
injection, thin rim enhancement was seen in the cys-
tic component and nodular enhancement was en-
countered in the solid part (Fig. 2).
Monstrous Craniopharyngioma: A Pictorial Essay
Iran J Radiol 2010, 7(2) 81
Patient 3
We encountered a six-year-old girl with headache,
nausea and vomiting from 6 months ago. CT scan of
the brain showed a mixed solid and cystic lesion with
heavy calcification in the solid and cystic parts. The
cystic part was seen with hypodense cystic contents.
The tumor extended to the right lateral and third
ventricles and produces biventricular hydrocephalus.
On the MR imaging study, a mixed cystic solid tumor
with low signal cystic contents on T1W was seen in
the suprasellar region with extension to the right tha-
lamus and lateral ventricles. Thick rim enhancement
was seen in the wall of the cystic part after contrast
injection. The tumor was adamantinomatous in pa-
thologic examination (Fig. 3).
Patient 4
The fourth patient is a 12-year-old girl who pre-
sented with left eye blindness from 5 months ago. On
brain CT scan performed after stereotaxis and placing
an intracystic catheter, a heavily calcified suprasellar
mass with extension to the sella was seen. Erosion
and destruction of the anterior and posterior clinoid
processes were noted. The mass extended to the ante-
rior and posterior cranial fossa. A large cystic compo-
Fig. 1. A six-year-old boy with nausea, vomiting and ataxia 2 years after surgical treatment of craniopharyngioma. A. Axial contrast enhanced CT scan of the brain, supra and parasellar cystic tumor with rim enhancement, extension to the posterior fossa and encasement of the basilar artery. B. Axial contrast enhanced CT scan of the brain, cystic and solid tumor with calcification and enhancement of solid and cystic parts, tumoral extension to the third ventricle and posterior fossa is seen. C. Axial contrast enhanced CT scan of the brain, extension of craniopharyngioma to the su-pratentorial region with compression of Monro's foramen. Drainage catheter is seen in the cystic part. D. Sagittal T1W MRI with contrast, low-signal cystic tumor with rim enhancement, extension to prepontine cistern and invasion to the midbrain and cerebellum. E. Sagittal T1W MRI with contrast, tumoral extension from perimesencephalic cisterns to the posteriorfossa and supratentorial area with biventricular hydrocephalus induction. F. Coronal T1W MRI with contrast, tumoral extension to cerebellum and lateral ventricles. G. Coronal T2W MRI, high signal cystic tumor with compression of the third ventricle.
A B C
D E F
G

Haghighatkhah et al.
82 Iran J Radiol 2010, 7(2)
nent was seen in the left frontal region with mass ef-
fect and midline shift to the right. The MRI study
was performed one year after surgery, the tumoral
remnant was seen in the left thalamus and deep tem-
poral lobe which has low signal intensity on T1W
and high signal intensity on T2W images. Nodular
enhancement was seen in the periphery of the cystic
part after contrast injection. Pathologic examination
Fig. 2. An 11-year-old boy with visual loss from 1.5 years ago. A. Axial brain CT scan, suprasellar lesion with calcification of the solid and cystic parts and extension to the posterior fossa. B. Axial brain CT scan, tumoral extension to the third ventricle and compression of the foramen of Monro. C. Axial T1W MRI, tumoral extension to the left parasellar area and left temporal lobe. Invasion to the posterior fossa and brainstem is noted as well. D. Coronal T2W MRI, tumoral extension to the left parasellar area and encasement of the left carotid artery.
Fig. 3. A six-year-old girl with headache, nausea and vomiting from 6 months ago. A. Axial brain CT scan, heavily calcified tumor with extension to the third ventricle and biventricular hydrocephalus induction. B. Axial brain CT scan, cystic and calcified tumor with compression of the right lateral ventricle and midline shift to the left. C. Axial T1W MRI, low signal cystic lesion with involvement of the right tha-lamus. D. Sagittal T1W MRI with contrast, thick rim enhancement of the lesion.
D
B C
B CA
A
D

Monstrous Craniopharyngioma: A Pictorial Essay
Iran J Radiol 2010, 7(2) 83
revealed adamantinomatous craniopharyngioma (Fig.
4).
Patient 5
A 17-year-old female was admitted with headache
and epistaxis from one year ago. Seven years ago she
was operated because of craniopharyngioma. Brain
CT scan showed a heavily calcified mixed solid and
cystic mass in the suprasellar area with extension to
the right cerebellopontine angle and third ventricle.
Brain MRI revealed a mixed low and high signal in-
tensity mass on T2W images in the suprasellar area
with extension of cystic part to left temporal lobe and
right cerebellopontine angle and interpeduncular cis-
terns. It is extended to anterior part of midbrain and
cerebral peduncles. Low signal areas are seen in tu-
moral mass due to calcification. After contrast injec-
tion, the solid tumoral portion was enhanced densely
and homogeneously. Comprehension of the basilar
trunk was seen in the posterior aspect of the tumor as
well as superior displacement of A1 segment of ante-
rior cerebral artery (ACA) (Fig. 5).
Patient 6
A 15-year-old boy was admitted to hospital with
headache and bitemporal hemianopia from 14
months ago. Brain CT scan study was performed 3
years after surgery. A heterogeneous calcified cystic
and solid mass was seen in the sellar and suprasellar
regions with extension to the anterior and posterior
cranial fossae and also to sphenoidal and posterior
ethmoidal sinuses and nasopharynx. Anterior and
posterior clinoid processes, sellar floor and sphenoidal
and ethmoidal bones are eroded. At the superior mar-
gin, the mass extended to the interpeduncular cistern.
A hypodense area is seen in the right frontal lobe in
favor of post-surgical encephalomalacic changes. A
drainage device is also seen in the cystic part of the
mass. Brain MRI revealed an isointense mass with
gray matter on T1W images with nodular and rim
enhancement and low signal areas in favor of calcifi-
cation. The mass extended to the nasopharynx, post-
erior ethmoidal, left maxillary and sphenoidal sinuses
from its inferior margin. It also extended to the post-
erior fossa and compresses the brain stem and the ba-
silar trunk. From the superior margin, it extended to
the interpeduncular cistern. Deviation of both inter-
nal carotid arteries and invasion of both cavernous
sinuses are noted as well. A porencephalic area in the
right frontal lobe and the drainage catheter are seen
on MRI and CT scan. Pathologic examination re-
vealed an adamantinomatous craniopharyngioma
(Fig. 6).
Patient 7
A 5-year-old girl presented with visual loss 3 years
after surgical treatment of craniopharyngioma. A cal-
cified mixed solid and cystic mass was seen in the su-
prasellar area on brain CT scan. The tumor extended
to the third ventricle and posterior fossa in the right
cerebellopontine angle. Biventricular hydrocephalus
was also noted. On T1W brain MRI study, right tem-
poroparietal craniotomy is noted. A mixed solid-
cystic mass is seen in the suprasellar area with exten-
sion to the third ventricle and compression of lateral
ventricles with hydrocephalus induction in the right
lateral ventricle. Low signal cystic materials are noted
on T1W images. The solid part is seen with high sig-
nal intensity in some parts on T1W images probably
due to calcification. A multi-cystic mass with low
signal areas of calcification is seen on T2W images as
well. Encasement of the proximal segment of the
middle cerebral artery (MCA), ACA, the distal part of
the internal carotid artery (ICA) and the basilar trunk
is noted. Invasion to the brain stem from the post-
erior tumoral margin is noted as well (Fig. 7).
Patient 8
A six-year-old girl was admitted with headache,
nausea and vomiting 3 years after surgical treatment
of craniopharyngioma. Physical exam revealed para-
lysis of lateral gaze in the left eye. Brain CT scan
showed a mixed solid and cystic mass with calcifica-
tion in the suprasellar region with extension to the
left temporal lobe and anterior cisterns of the brain
stem. On MRI study, a T1Wand T2W high signal in-
tensity cystic mass is seen in the suprasellar region
with extension to the left parasellar area and encase-
ment of the left ICA and invasion to the left cavern-
ous sinus and both temporal lobes. Compression and
right deviation of the third ventricle are noted as
well. Midline shift to the right is seen as well as supe-
rior displacement at A1 segment of the ACA.

Haghighatkhah et al.
84 Iran J Radiol 2010, 7(2)
Patient 9
A 23-year-old woman presented with headache,
visual loss, nausea and vomiting 6 years after surgical
treatment of craniopharyngioma. Brain MRI study
was performed. A multi cystic mass with low signal
intensity on T1W and high signal intensity on T2W
images is seen in the sellar and suprasellar regions.
Thin rim enhancement of the cystic part and nodular
enhancement of the solid part are also noted after
contrast injection. The mass extends to the right fron-
tal lobe and compressed the optic chiasm. Compres-
sion of the third ventricular floor is also noted. Pre-
vious craniotomy scar is seen in the left parietal re-
gion (Fig. 9).
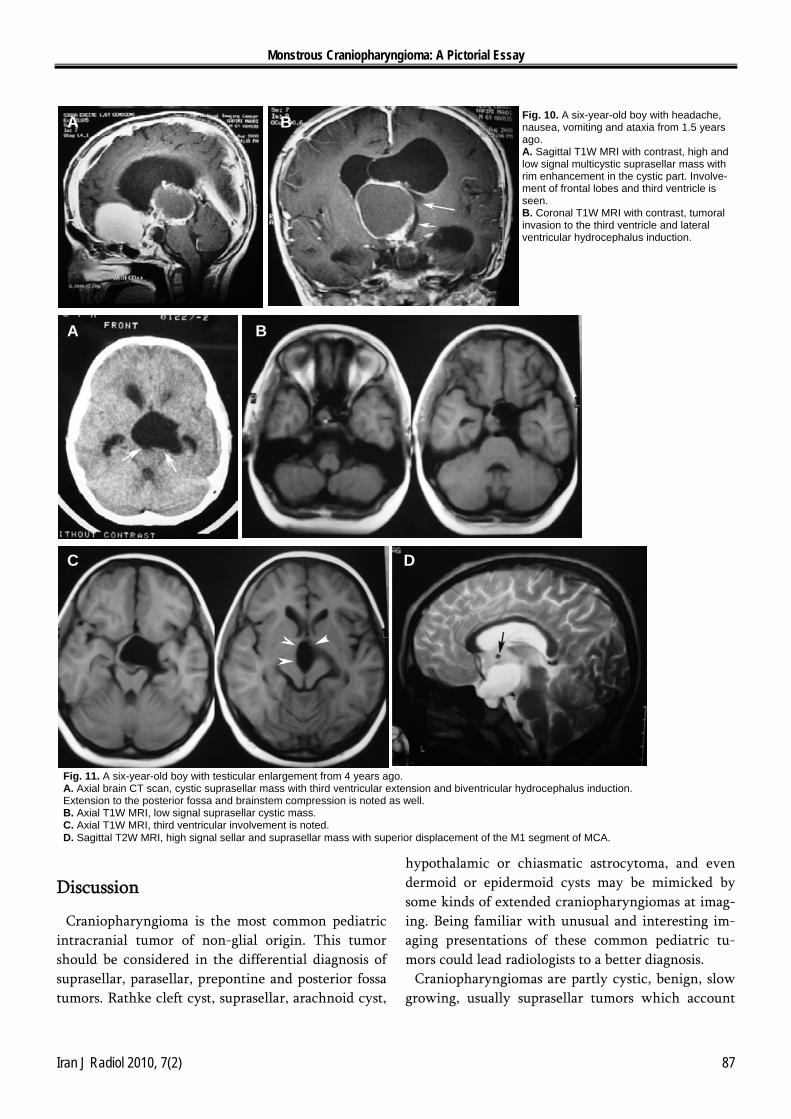
Patient 10
A six-year-old boy was admitted with headache,
Fig. 4. A 12-year-old girl with left eye blindness from 5 months ago. A. Axial brain CT scan, heavily calcified suprasellar mass with extention to both frontal lobes and posterior fossa. B. Axial brain CT scan, large cystic tumoral part in the left frontal lobe with mass effect and midline shift to the right. C. Sagittal T1W MRI, tumoral recurrence 2 years after operation. D. Sagittal T1W MRI with contrast, nodular and rim enhancement is seen in solid and cystic parts.
Fig. 5. A 17-year-old female with headache and epistaxis from one year ago who was admitted 7 years after surgical treatment of craniopharyngioma. A. Axial brain CT scan, heavily calcified suprasellar mass with extension to the right CP angle. B. Axial brain CT scan, tumoral invasion to the posterior aspect of the third ventricle. C. Axial T2W MRI, mixed solid and cystic tumor of suprasella with low signal areas of calcification, exten-sion to the left temporal lobe and anterior aspect of the midbrain. D. Sagittal T1W MRI, high signal tumor with superior displacement of the A1 segment of ACA. Craniotomy defect is seen at the parietal area. E. Sagittal T1W MRI, tumoral invasion to prepontine cistern and compression of the basilar trunk.
A B C D
E
A B
DC

Monstrous Craniopharyngioma: A Pictorial Essay
Iran J Radiol 2010, 7(2) 85
nausea, vomiting and ataxia from 1.5 years ago. Brain
MRI study was performed. An extensive solid and
cystic mass is seen in the anterior, middle and post-
erior cranial fossae. The mass had multi-cystic com-
ponents with high and low signal contents on T1W
images. The high signal cystic part extends to the an-
terior fossa and compresses both frontal lobes and the
optic chiasm. T1W imaging shows a low signal cystic
part extending to the third ventricle with compres-
sion of the foramen of Monro and lateral ventricular
hydrocephalus induction. Reticular and non homo-
geneous enhancement is seen in the solid parts. Right
and left parasellar extension is noted as well. Post-
erior extension to the prepontine and interpeduncu-
Fig. 6. A 15-year-old boy with headache and bitemporal hemianopia from 14 months ago. A. Axial brain CT scan, suprasellar tumoral mass with calcification and invasion to the sphenoidal and posterior ethmoidal sinuses. Extension to posterior fossa is noted as well. B. Axial contrast enhanced brain CT scan, cystic mass with eggshell calcification and extension to frontal lobes. The drainage catheter and right frontal encephalomala-ciais seen. C. Axial T1W MRI with contrast, nonhomogeneous en-hancing mass with invasion to the posterior fossa, both parasellar areas and posterior ethmoidal sinuses.
Fig. 7. A five-year-old girl with visual loss 3 years after surgical treatment of craniopharyngioma. A. Axial brain CT scan, solid and cystic calcified suprasellar mass with extension to the right CP an-gle and compression of the right side of pons. B. Axial brain CT scan, tumoral extension to the third ventricle with biventricular hydrocephalus induc-tion. C. Coronal T1W MRI with contrast, low signal cystic mass with high signal solid parts due to calcifica-tion. Mass effect, midline shift and right lateral ventricular hydrocephalus is evident. D. Sagittal T2W MRI, high signal multicystic mass with low signal areas of calcification. Invasion to the brainstem and encasement of the arteries of the circle of Willis is evident.
D. Axial T1W MRI, tumoral extension to both parasellar areas and encasement of the internal carotid arteries, invasion to both cavernous sinuses is observed. E. Axial T1W MRI with contrast, tumoral invasion to both frontal lobes and compression of anterior aspect of the midbrain.
D E
A B C
A B C
D

Haghighatkhah et al.
86 Iran J Radiol 2010, 7(2)
lar cisterns with basilar trunk compression is pre-
sented (Fig. 10).
Patient 11
A six-year-old boy presented with testicular en-
largement from 4 years ago. Brain CT scan was per-
formed and a hypodense cystic suprasellar mass with
superior extension to the third ventricle is noted.
Thin eggshell calcification is also seen in the walls of
the cystic part. Biventricular hydrocephalus is de-
tected. On MRI study, a T1W low signal cystic mass
with iso signal solid parts is seen in the suprasellar
region with superior extension to the third ventricle
and inferior extension to sella turcica. Encasement of
the left ICA bifurcation and superior displacement at
M1 segment of the MCA is noted. Posterior extension
to the midbrain and basilar trunk compression is seen
as well. Biventricular hydrocephalus is evident on
MRI and CT scan (Fig. 11).
Fig. 8. A six-year-old girl with headache, nausea and vomiting 3 years after surgical treatment of cra-niopharyngioma. A. Axial contrast enhanced brain CT scan, mixed solid and cystic suprasellar mass with calcification and extension to the left temporal lobe. B. Axial T1W MRI, high signal suprasellar mass with extension to the left frontal and temporal lobes. C. Axial T2W MRI, high signal cystic mass with extension to the left temporal lobe. D. Coronal T1W MRI, tumoral extension to the left parasellar region with left ICA encasement and left cavernous sinus invasion.
Fig. 9. A 23-year-old female with headache, visual loss, nausea and vomiting 6 years after surgical treatment of craniophryngioma. A. Coronal T1W MRI with contrast, low signal suprasellar cystic mass with nodular enhancement of the solid part and compression of the third ventricle. B. Sagittal T1W MRI with contrast, tumoral extension to the anterior fossa. C. Axial T2W MRI, high signal cystic tumor with extension to both frontal lobes.
A B
D
A B C
C
Monstrous Craniopharyngioma: A Pictorial Essay
Iran J Radiol 2010, 7(2) 87
Discussion
Craniopharyngioma is the most common pediatric
intracranial tumor of non-glial origin. This tumor
should be considered in the differential diagnosis of
suprasellar, parasellar, prepontine and posterior fossa
tumors. Rathke cleft cyst, suprasellar, arachnoid cyst,
hypothalamic or chiasmatic astrocytoma, and even
dermoid or epidermoid cysts may be mimicked by
some kinds of extended craniopharyngiomas at imag-
ing. Being familiar with unusual and interesting im-
aging presentations of these common pediatric tu-
mors could lead radiologists to a better diagnosis. Craniopharyngiomas are partly cystic, benign, slow
growing, usually suprasellar tumors which account
Fig. 10. A six-year-old boy with headache, nausea, vomiting and ataxia from 1.5 years ago. A. Sagittal T1W MRI with contrast, high and low signal multicystic suprasellar mass with rim enhancement in the cystic part. Involve-ment of frontal lobes and third ventricle is seen. B. Coronal T1W MRI with contrast, tumoral invasion to the third ventricle and lateral ventricular hydrocephalus induction.
Fig. 11. A six-year-old boy with testicular enlargement from 4 years ago. A. Axial brain CT scan, cystic suprasellar mass with third ventricular extension and biventricular hydrocephalus induction. Extension to the posterior fossa and brainstem compression is noted as well. B. Axial T1W MRI, low signal suprasellar cystic mass. C. Axial T1W MRI, third ventricular involvement is noted. D. Sagittal T2W MRI, high signal sellar and suprasellar mass with superior displacement of the M1 segment of MCA.
C D
A B
A B

Haghighatkhah et al.
88 Iran J Radiol 2010, 7(2)
for 5-13% of all intracranial tumors.11 They derive
from Rathke’s pouch, the embryonic infolding of en-
doderm that extends superiorly from the stomodeum
and gives rise in the early fetal development to the
adenohypophysis;7 with manifestation during child-
hood and fourth or fifth decades of adult life. Fre-
quent symptoms of manifestation are visual symp-
toms or endocrine disturbances such as polyuria and
polydipsia due to diabetes insipidus.12 The tumor has
three histologic types: adamantinomatous (pediatric
type), papillary (adult type) and mixed.1
The adamantinomatous type is classically a cystic
tumor with solid components.1,2,5 The papillary type is
predominantly solid, without calcification.1,7 After
surgery and radiation, the 5-year survival rate is more
than 80% in children. Permanent endocrinologic def-
icits are seen in many patients after treatment but
visual disturbances are usually reversible. The recur-
rence rate of the tumor depends on the size of the
tumor, the recurrence rate is approximately 20% for
tumors smaller than 3 cm and 83% for tumors larger
than 5 cm.1
CT and MRI are complementary studies for detec-
tion of extent and characteristics of the tumor.1 On
CT scan, the pediatric type is presented as a predomi-
nantly suprasellar and calcified cystic mass with solid
components in 90% of cases. Extension to sella turci-
ca is seen frequently. The adult type tumors are
usually solid and isodense. Calcifications and intra-
ventricular craniopharyngiomas are rare.
In the papillary subtype, after contrast injection,
enhancement is seen in solid components and the
wall of cystic parts in 90% of cases. Anterior and su-
perior extension of the tumor leads to anterior dislo-
cation of the optic chiasm and superior dislocation of
the A1 segment of the anterior cerebral artery. On
CT scan, the usual extension of the cystic part is to
the anterior and lateral but the solid part extends to
the posterior and lateral.13
MRI is preferred for better determination of the
tumor extent. The pediatric type appears as a predo-
minantly cystic mass with solid components but the
papillary type is predominantly solid.1,7 Calcifications
are better seen in GRE images and may show suscep-
tibility effects. Signal intensity of the cystic part is
variable on T1W images. Blood products, high pro-
tein concentration or cholesterol crystals in the cyst
leads to high signal characteristics of the cystic part
on T1W images. Cysts are hyperintense on T2W and
FLAIR images. Solid components appear isointense
on T1W and heterogeneously iso to hypointense on
T2W images.
A prominent lipid spectrum is seen in MR spectros-
copy around 1PPM because of the cystic contents.
Also variable signal intensities are seen in diffusion
weighted images because of variable cystic contents.
After contrast injection, patterns of enhancement in
solid and cystic tumoral parts are similar to CT scan.13
The location of the tumor is predominantly supra-
sellar in 75%, supra and infrasellar in 12%, and pure-
ly intrasellar in 4% of cases. Encasement or displace-
ment of the vessels forming the circle of Willis is
noted. Lateral displacement of ICAs and superior dis-
location of ACA are also seen. Posterior dislocation
and compression of the basilar trunk is noted as well.
We can categorize the tumoral extension to three
specific subtypes. In type A, the tumors are entirely
within the sella and vascular displacement is not
seen. In type B, the tumor is extended anteriorly be-
tween the optic nerves and pushes the optic chiasm
posteriorly. Elevation of the anterior communicating
artery and the A1 segment of the anterior cerebral
artery are noted as well. In type C, elevation of the
A1 segment of the anterior cerebral artery and ante-
rior communicating artery, with posterior compres-
sion of the basilar trunk is noted. Anterior dislocation
of the optic chiasm with third ventricular compres-
sion and hydrocephalus are seen as well.1
References
1. Wasserman JR, Koenigsberg RA, Batra K, Gange CP Jr. Craniopha-
ryngioma overview. Medscape [serial online] 2008 Jun 11. Available
from: http://emedicine.medscape.corm/article/339424-overview. Ac-
cessed April 28, 2009.
2. Garnett MR, Puget S, Grill J, Sainte-Rose C. Craniopharyngioma.
Orphanet J Rare Dis 2007 Apr;2:18.
3. Tsuda M, Takahashi S, Higano S, Kurihara N, Ikeda H, Sakamoto K.
CT and MR imaging of craniopharyngioma. Eur Radiol 1997;7(4):464-
9.
4. Freeman MP, Kessler RM, Allen JH, Price AC. Craniopharyngioma:
CT and MRI imaging in nine cases. J Comput Assist Tomogr 1987
Sep-Oct;11(5):810-4.
5. Choi SH, Kwon BJ, Na DG, Kim JH, Han MH, Chang KH. Pituitary
adenoma, craniopharyngioma and Rathke cleft cyst involving both
intrasellar and suprasellar regions: differentiation using MRI. Clin
Radiol 2007 May;62(5):453-62.

Monstrous Craniopharyngioma: A Pictorial Essay
Iran J Radiol 2010, 7(2) 89
6. Johnsen DE, Woodruff WW, Allen IS, Cera PJ, Funkhouser GR,
Coleman LL. MR imaging of the sellar and juxtasellar regions. Radio-
graphics 1991 Sep;11(5):727-58.
7. Haaga JR, Dogra VS, Forsting M, Gilkeson RC, Ha HK, Sundaram M.
CT and MRI of the whole body. 5th ed. Philadelphia: Mosby; 2009. p.
124-7.
8. Curran JG, O’connor E. Imaging of craniopharyngioma. Childs Nerv
Syst 2005 Aug;21(8):635-9.
9. Osborn AG. Diagnostic imaging of brain. 1st ed. Salt Lake City: Amir-
sys; 2004. p. 894-7.
10. Karavitaki N, Cudlip S, Adams CB, Wass JA. Craniopharyngiomas.
Endocr Rev 2006 Jun;27(4):371-97.
11. Rossi A, Cama A, Gonsales A, Gandolfo C, Garre ML, Milanaccio C et
al. Neuroimaging of pediatric craniopharyngiomas: a pictorial essay. J
Pediatr Endocrinol Metab 2006 Apr;19 Suppl 1:299-319.
12. Boneville F, Cattin F, Marsot-Dupuch K, Dormont D, Bonneville JF,
Chiras J. T1 signal hyperintensity in the sellar region :spectrum of
findings. Radiographics 2006 Jan-Feb;26(1):93-113.
13. Wasserman JR, Koenigsberg RA, Batra K, Gaange Jr CP. Craniopha-
ryngioma: imaging. Medscape [serial online]. 2008 Jun 11. Available
from: http://www.Medscape.com. Accessed May 4, 2009.