1 influenza virus cdc website 2002
Post on 22-Dec-2015
218 views
TRANSCRIPT

1
INFLUENZA VIRUS
INFLUENZA VIRUSCDC WEBSITEhttp://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm
2002
2
‘FLU’
• True influenza– influenza virus A or influenza virus B (or
influenza virus C infections - much milder)
• Febrile respiratory disease with systemic symptoms caused by a variety of other organisms often called ‘flu’

3
South Carolina 1996-1997 DHEC bulletin
http://www.state.sc.us/dhec/LAB/labbu017.htm
no virus
influenza A
influenza B
CULTURE RESULTS
malathia influenzae per le stelle

4
1918-19 Spanish flu 500,000 US20,000,000 world
1957-58 Asian flu 70,000 US
1968-69 Hong Kongflu
34,000 US
THE IMPACT OF INFLUENZAPANDEMICS
Deaths:

5
THE IMPACT OF INFLUENZA
• 1972-1994 (19 influenza seasons)
– >20,000 US deaths in 11 seasons
– >40,000 US deaths in 6 of these
– many more hospitalizations (~110,000 per year)
6
THE IMPACT OF INFLUENZA
• recently some increase in morbidity and mortality - possible factors?– more elderly people– CF patients live longer– more high risk neonates– more immunosuppressed patients
7
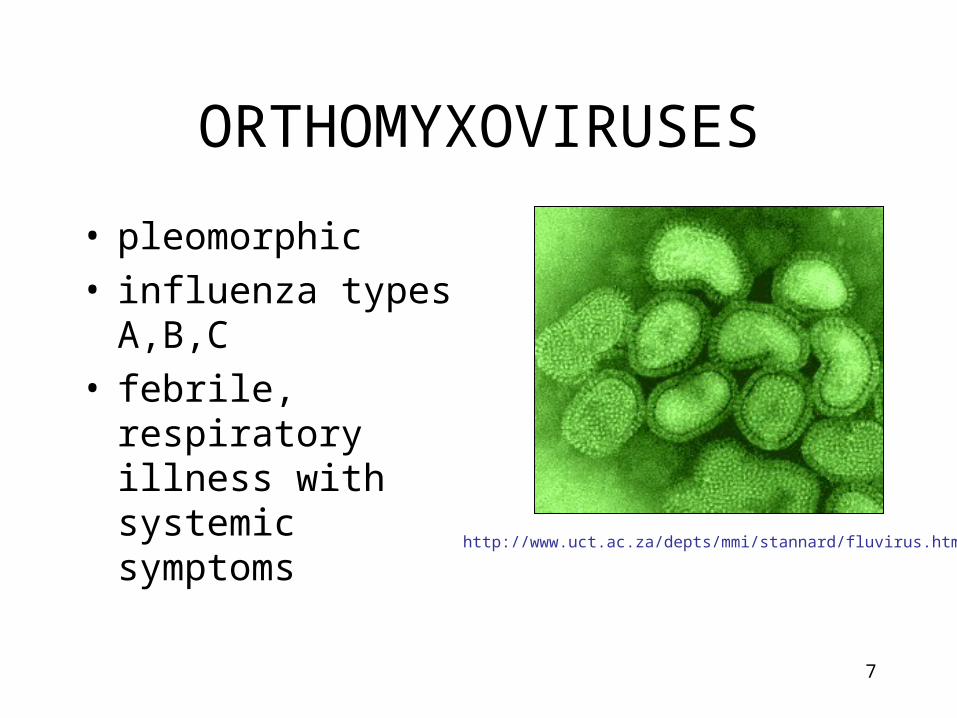
ORTHOMYXOVIRUSES
http://www.uct.ac.za/depts/mmi/stannard/fluvirus.html
• pleomorphic• influenza types A,B,C• febrile, respiratory
illness with systemic symptoms

8
ORTHOMYXOVIRUSES
M1 protein
helical nucleocapsid (RNA plus NP protein)
HA - hemagglutinin
polymerase complex
lipid bilayer membrane
NA - neuraminidase
type A, B, C : NP, M1 protein sub-types: HA or NA protein

9
TRANSMISSION
• AEROSOL– 100,000 TO
1,000,000 VIRIONS PER DROPLET
• 18-72 HR INCUBATION
• SHEDDING

10
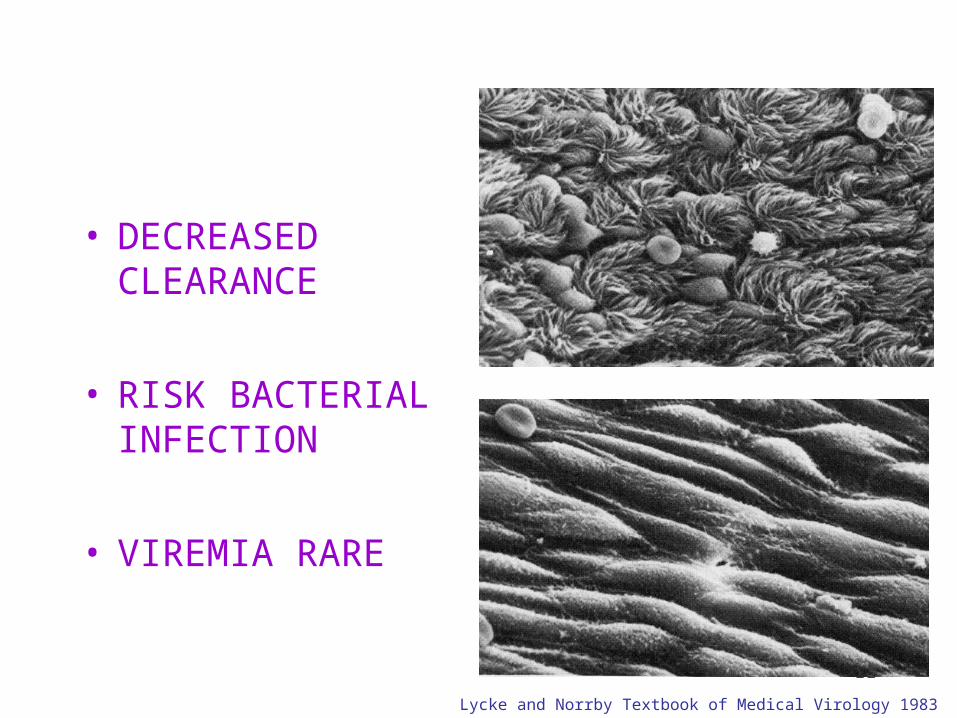
NORMAL TRACHEAL MUCOSA
3 DAYS POST-INFECTION 7 DAYS POST-INFECTION
Lycke and Norrby Textbook of Medical Virology 1983
11
• DECREASED CLEARANCE
• RISK BACTERIAL INFECTION
• VIREMIA RARE
Lycke and Norrby Textbook of Medical Virology 1983

12
RECOVERY
• INTERFERON - SIDE EFFECTS INCLUDE:– FEVER, MYALGIA, FATIGUE, MALAISE
• CELL-MEDIATED IMMUNE RESPONSE
• TISSUE REPAIR– CAN TAKE SOME TIME

13
An immunological diversion
INTERFERON

14
INTERFERON
timecourse of virus production will vary from virus to virus

15
INTERFERON
16
INTERFERON
antiviral stateantiviral state
antiviral state
antiviral state

17
INTERFERON
antiviral stateantiviral state
antiviral state
antiviral state
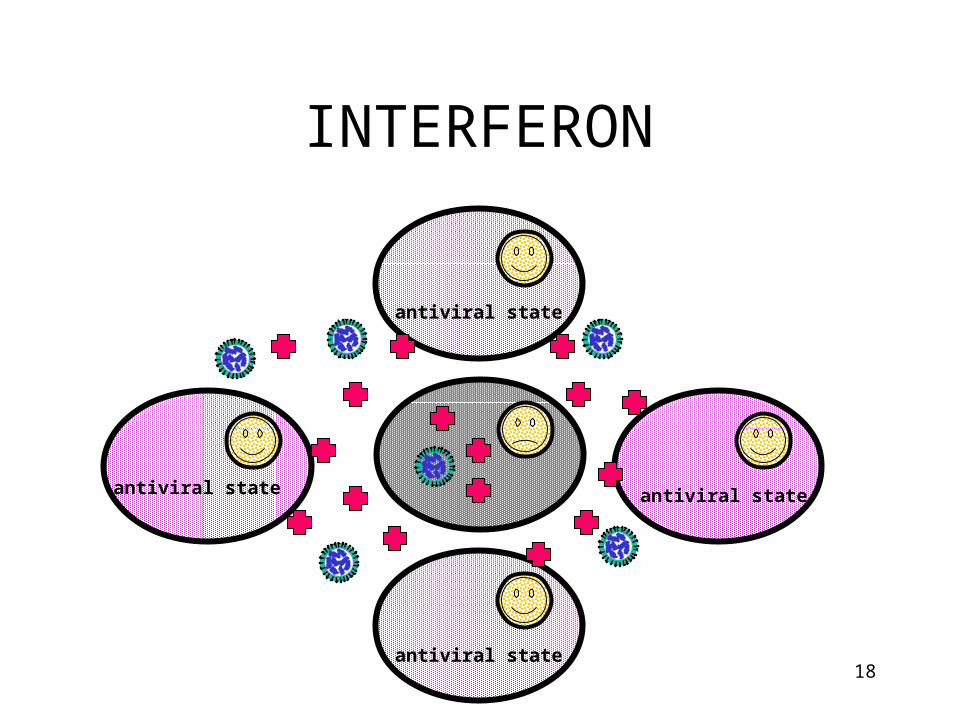
18
INTERFERON
antiviral stateantiviral state
antiviral state
antiviral state

19
INTERFERONTHE VIRUSES ARE COMING!
http://www.paulreverehouse.org/midnight.html
PAUL REVEREhttp://www.mfa.org/collections/one_hour/6.htm
20
TYPES OF INTERFERON
• TYPE I•Interferon-alpha (leukocyte interferon, about 20 related proteins)
- leukocytes, etc•Interferon-beta (fibroblast interferon)
- fibroblasts, epithelial cells, etc•TYPE II
•Interferon-gamma (immune interferon)
- certain activated T-cells, NK cells

21
INDUCTION OF INTERFERON
•interferon-alpha and interferon-beta
- viral infection (especially RNA viruses), double stranded RNA, certain bacterial components
- strong anti-viral properties•interferon-gamma
- antigens, mitogenic stimulation lymphocytes

22
INTERFERON
• induce various proteins in target cells
• many consequences, not all fully understood

23
INTERFERON-ALPHA AND INTERFERON-BETA

24
interferon-alpha, interferon-beta
interferon receptor
induction of 2’5’oligo A synthase
induction of aprotein kinase
2’5’oligo A
induction of ribonuclease L
activated ribonuclease L
ATP
ds RNA ds RNA
activatedprotein kinase
activated2’5’oligo A synthase
ATP
2’5’oligo A
mRNA degraded
phosphorylated initiation factor (eIF-2)
inhibition of protein synthesis

25
interferons
• only made when needed

26
OTHER EFFECTS OF INTERFERONS
• ALL TYPES– INCREASE MHC I EXPRESSION
• CYTOTOXIC T-CELLS
– ACTIVATE NK CELLS• CAN KILL VIRALLY INFECTED CELLS

27
OTHER EFFECTS OF INTERFERONS
• INTERFERON-GAMMA– INCREASES MHC II EXPRESSION ON APC
• HELPER T-CELLS
– INCREASES ANTIVIRAL POTENTIAL OF MACROPHAGES
• INTRINSIC• EXTRINSIC
28
THERAPEUTIC USES OF INTERFERONS
• ANTI-VIRAL – e.g. interferon-alpha is currently approved for certain cases
of acute and chronic HCV and chronic HBV
• MACROPHAGE ACTIVATION– interferon-gamma has been tried for e.g. lepromatous
leprosy, leishmaniasis, toxoplasmosis
• ANTI-TUMOR– have been used in e.g. melanoma, Kaposi’s sarcoma, CML
• MULTIPLE SCLEROSIS– interferon-beta
29
Viral response to host immune system
Viruses may :
block interferon binding
inhibit function of interferon-induced proteins
inhibit NK function
interfere with MHC I or MHC II expression
block complement activation
inhibit apoptosis
etc!

30
SIDE EFFECTS OF INTERFERONS
• FEVER
• MALAISE
• FATIGUE
• MUSCLE PAINS

31
BACK TO INFLUENZA

32
PROTECTION AGAINST RE-INFECTION
• IgG and IgA– IgG less efficient but lasts longer
• antibodies to both HA and NA important– antibody to HA more important (can
neutralize)

33
SYMPTOMS
• FEVER
• HEADACHE
• MYALGIA
• COUGH
• RHINITIS
• OCULAR SYMPTOMS

34
CLINICAL FINDINGS
• SEVERITY– VERY YOUNG– ELDERLY– IMMUNO-
COMPROMISED– HEART OR LUNG
DISEASE

35
PULMONARY COMPLICATIONS
• CROUP (YOUNG CHILDREN)• PRIMARY INFLUENZA VIRUS
PNEUMONIA• SECONDARY BACTERIAL
INFECTION– Streptococcus pneumoniae– Staphlyococcus aureus– Hemophilus influenzae

36
NON-PULMONARY COMPLICATIONS
• myositis (rare, > in children, > with type B)• cardiac complications• recent studies report encephalopathy
– studies of patients <21 yrs in Michigan - 8 cases seen last season
• liver and CNS– Reye syndrome
• peripheral nervous system– Guillian-Barré syndrome

37
Reye’s syndrome
• liver - fatty deposits• brain - edema• vomiting, lethargy, coma• risk factors
– youth– certain viral infections (influenza, chicken
pox)– aspirin

38
NON-PULMONARY COMPLICATIONS
• myositis (rare, > in children, > in type B)
• cardiac complications
• encephalopathy
• liver and CNS– Reye’s syndrome
• peripheral nervous system– Guillian-Barré syndrome

39
Guillian-Barré syndrome
• 1976/77 swine flu vaccine– 35,000,000 doses
• 354 cases of GBS• 28 GBS-associated deaths
• recent vaccines much lower risk
40
MORTALITY
• MAJOR CAUSES OF INFLUENZA VIRUS- ASSOCIATED DEATH– BACTERIAL PNEUMONIA– CARDIAC FAILURE
• 90% OF DEATHS IN THOSE OVER 65 YEARS OF AGE

41
DIAGNOSIS
• ISOLATION– NOSE, THROAT SWAB– TISSUE CULTURE OR EGGS
• SEROLOGY
• RAPID TESTS
• provisional - clinical picture + outbreak
42
S S
S S
S S
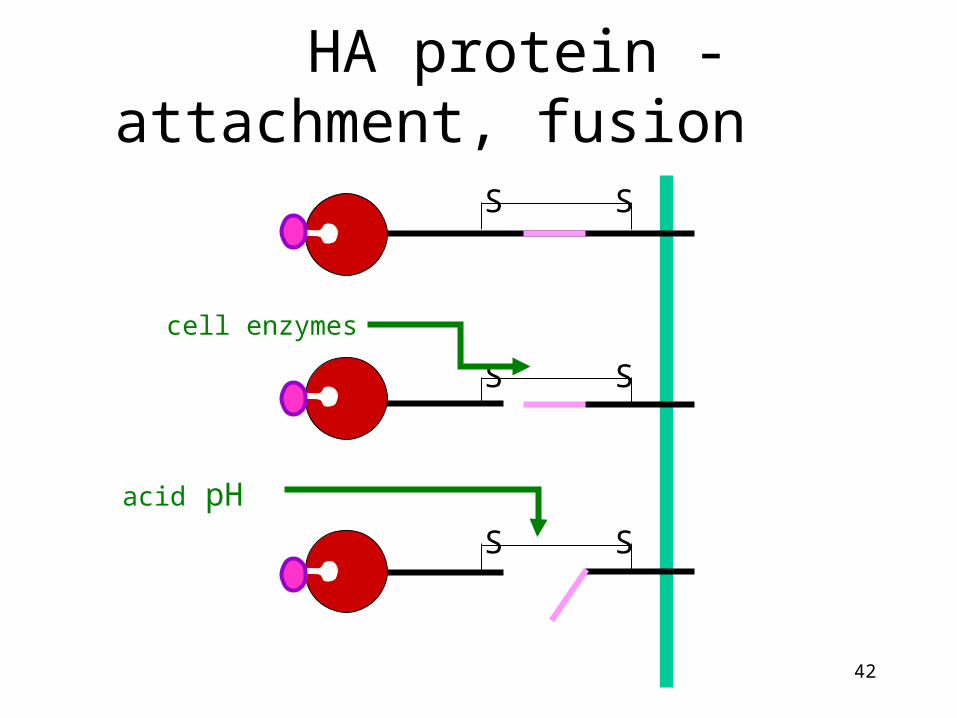
cell enzymes
acid pH
HA protein - attachment, fusion

43
NA protein - neuraminidase
44
ANTIGENIC DRIFT
• HA and NA accumulate mutations– RNA virus
• immune response no longer protects fully
• sporadic outbreaks, limited epidemics

45
ANTIGENIC SHIFT
• “new” HA or NA proteins
• pre-existing antibodies do not protect
• may get pandemics

46
INFLUENZA A PANDEMICS
Ryan et al., in Sherris Medical Microbiology
47
where do “new” HA and NA come from?
• 13 types HA• 9 types NA
– all circulate in birds
• pigs– avian and human

48
where do “new” HA and NA come from?

49
why do we not have influenza B pandemics?
• so far no shifts have been recorded
• no animal reservoir known

50
SURVEILLANCE
CDC/Katherine Lord

51
actual percentage of deaths
(CDC MMWR 2003 / Vol. 52 / No. RR-8)

520
10
2030
4050
6070
8090
100
99/00 00/01 01/02 02/03
H1N1
H3N2
B

53
VACCINE
• ‘BEST GUESS’ OF MAIN ANTIGENIC TYPES– CURRENTLY
• type A - H1N1• type A - H3N2• type B• each year choose which variant of each
subtype is the best to use for optimal protection

54
VACCINE
• inactivated• egg grown• sub-unit vaccine for children
• reassortant live vaccine approved 2003– for healthy persons (those not at risk for
complications from influenza infection) ages 5-49 years

55
CDC

56
RECOMMENDATIONSPersons at High Risk for Influenza-Related Complications
· 65 years
· residents of nursing homes and other chronic-care facilities
· adults/children who have chronic pulmonary or cardiovascular disorders, including asthma
· adults/children who have required regular medical follow-up or hospitalization during the last year because of chronic metabolic diseases (including diabetes mellitus), renal dysfunction, hemoglobinopathies, or immunosuppression (including immunosuppression caused by medications)
57
RECOMMENDATIONSPersons at High Risk for Influenza-Related Complications · children and teenagers (6 mths to 18 yrs) receiving long-term aspirin therapy - might be at risk for developing Reye syndrome after influenza
· women who will be in the 2nd or 3rd trimester of pregnancy during the influenza season.

58
RECOMMENDATIONSPersons aged 50-64 years
increased prevalence of high-risk conditions
from public health point of view, easier to target by age than by high-risk condition (which may not have been
discovered)

59
RECOMMENDATIONS
Persons Who Can Transmit Influenza to Those at High Risk
Persons who are clinically or subclinically infected can transmit influenza virus to persons at high risk for complications from influenza.

60
RECOMMENDATIONS · physicians, nurses, and other personnel in both hospital and outpatient-care settings
· employees of nursing homes and chronic-care facilities who have contact with patients or residents
· employees of assisted living and other residences for persons in high-risk groups
· persons who provide home care to persons in high-risk groups
· household members (including children) of persons in high-risk groups.

61
RECOMMENDATIONS
Children from 0-23 mths are at increased risk for hospitalization from influenza, vaccination is encouraged for their household contacts and out-of-home caretakers, particularly for contacts of children aged 0–5 months because influenza vaccines have not been approved for use among children aged <6 months.

62
RECOMMENDATIONS
• others, including travellers and the general population may wish to be vaccinated

63
PREVENTION - DRUGS
• RIMANTADINE (M2)• type A only
• AMANTADINE (M2)• type A only
• ZANAMIVIR (NA)• types A and B, not yet approved for prevention
• OSELTAMIVIR (NA)• types A and B

64
TREATMENT - DRUGS
• RIMANTADINE (M2)• type A only, needs to be given early
• AMANTADINE (M2)• type A only, needs to be given early
• ZANAMIVIR (NA)• types A and B, needs to be given early
• OSELTAMIVIR (NA)• types A and B, needs to be given early

65
NA protein - neuraminidase
.. ..
. . ...
..
....
..
..

66
OTHER TREATMENT
• REST, LIQUIDS, ANTI-FEBRILE AGENTS (NO ASPIRIN FOR AGES 6MTHS-18YRS)
• BE AWARE OF COMPLICATIONS AND TREAT APPROPRIATELY

67
TYPE A
++++
yes
yes
yes
shift, drift
yes
sensitive
sensitive
2
severity of illness
animal reservoir
human pandemics
human epidemics
antigenic changes
segmented genome
amantadine, rimantidine
zanamivir
surface glycoproteins
TYPE B
++
no
no
yes
drift
yes
no effect
sensitive
2
TYPE C
+
no
no
no (sporadic)
drift
yes
no effect
(1)

68
END

69
live vaccine development
adapted from
Treanor JJ Infect. Med. 15:714

70