1. introduction 1 - shodhgangashodhganga.inflibnet.ac.in/bitstream/10603/10206/10/10_chapter...
TRANSCRIPT

1. INTRODUCTION 1
1. INTRODUCTION
1.1 MEDICINAL PLANTS: AN OVERVIEW
Medicinal plants contain inherent active ingredients to cure disease or relieve pain. The
use of traditional medicines and medicinal plant in most developing countries as
therapeutic agent for the maintenance of good health has been widely observed. The
world health organization estimated that 80% of the population of developing countries
relies on traditional medicines, mostly herbal plant drugs for their primary health care.
The medicinal property of plant could be based on the anti-oxidant, antimicrobial,
antipyretic effect of the phytochemicals present. Traditionally, herbs have been
considered to be non-toxic and have been used for treating various problems by the
general public and/or traditional medicine doctors worldwide. Although, the literature has
documented several toxicity resulted from the use of herbs on many occasions, still the
potential toxicity of herbs has not been recognized by the general public or by
professional groups of traditional medicine. The use of medicinal plants as raw materials
in the production of drug is gaining popularity.1,2
India perhaps the largest producer of medicinal herbs and is called Botanical Garden of
the World. Medicinal herbs have been in use for thousands of years, in one form or
another, under the indigenous systems of medicine like Ayurveda, Sidha and Unani. On
earth, around 3.6 lakh species of medicinal plants are present, among these 1.4 lakh
species are in India.. A latest survey indicates that about 70000 plants are used in
traditional systems of medicines.3 All over the world, plants were used as main source of
medicines by ancestors. The rise of modern western medicine was initially accompanied
by a decline in the practice of herbalism in all cultures and it was believed that synthetic
chemicals were best medicines to treat illness and cure disease.
The quest for a healthier lifestyle has made people to once again recognize the healing
power of herbs. Even in the west, natural products are now widely available and

1. INTRODUCTION 2
herbalism is again coming into lime light in the world which is becoming healthier and
environmentally conscious. Herbal remedies can work without many of the unpleasant
side effects of modern medicines.
A reversion has been observed towards traditional systems of medicine for better
treatment and care. People all over the world, in future will prefer treatment in the
traditional systems of medicine. The reason for this is that in spite of well-documented
facts regarding the efficacy of modern medicine, certain draw backs have restricted its
future prospects. The disadvantages of modern medicine have led the researchers to look
for alternative systems especially the ancient and traditional medicine.4
1.1.1 Traditional Medicine
The term “traditional medicine” refers to ways of protecting and restoring health that
existed before the arrival of modern medicine. As the term implies, these approaches to
health belong to each country, and have been handed down from generation to
generation. A traditional system requires to meet the needs of the local communities for
many centuries. The traditional system of medicine is prevalent in India since the Vedic
period and as early as the dawn of human civilization. Though it has undergone many
changes in the course of its long history, it still remains the main history of medical relief
to a large section of population of the nation. Traditional medicine has maintained its
popularity in a number of Asian countries such as China, India, Japan and Pakistan.
Medicinal plants are the oldest known health care products. Their importance is still
growing.5
Ayurveda- An Indian system of medicine
Ayurveda ancient sciences of life are believed to be prevalent for the last 5000 years in
India. It is one of the most noted systems of medicine in the world. Ayurveda is based on
the hypothesis that everything in the universe is composed of five basic elements viz.
space, air, energy, liquid and solid. They exist in the human body in confined forms like
vata(space and air), pitta(energy and liquid) and kapha(liquid and solid). Vata, pitta and
kapha together are called tridosha (three pillars of life) .Imbalance in between these will
cause pathological condition.6

1. INTRODUCTION 3
Unani systems of medicine
The roots of this system go deep to the times of the well known Greek philosopher
Hippocrates who is credited with it. Aristotle Golem “Father of natural history” made
valuable contribution to it. This system is based on two theories viz. Hippocratic theory
of four humours and the Pythagorian theory of four proximate qualities. The four
humours are blood, phlegm, yellow bile and black bile while the four qualities are the
states of living human body like hot. cold, moist and dry. They are represented as earth,
water, fire and air. The Unani system of medicine aims at treating the cause of disease
and not its symptoms. For this purpose, thorough history of the patient is recorded in
addition to his pulse, urine and stool examinations. The diseased condition is considered
to be the imbalance between humours and accordingly, treatment is given.6
Homoeopathic system of medicine
In comparison to other traditional systems of medicine, homoeopathy is a newer one and
has been developed in the eighteenth century by Samuel Hahnemann – a German
physician and Chemist. He proposed that the cause of disease itself could be used for its
treatment. He put forth the law of similarities which says that “like cures like”. With this
principle, he showed that cinchona can produce the symptoms of malaria. He complied
all these observations in what is called “The organon of medicine”.
In the homoeopathic system, the treatment is not specified but the choice of drug depends
on symptoms and the clinical condition of the patient. This is based on the concept of
proving and prover. In a healthy person called prover, the symptoms created by different
doses of drug extracts are noted which is called proving and if physical, mental and
emotional changes of prover are specifically considered. Consequently, these symptoms
are composed with a patient with similar symptoms and accordingly, same type of extract
is given for treatment. Various medicinal plants used in Homeopathic system are Arnica,
Belladona, Chamomile, Colchicum, Hyocyamus, Ipecacuhna, Lycopodium, Opium,
Ergot, Nux-vomica etc.6
Siddha system of medicine
The term “Siddha” means achievement and “Siddhars” were saintly personalities, who
attained proficiency in medicine through practice of Bhakti and Yoga. This is the system
of pre-vedic period identified with Dravidian culture and it is largely therapeutic in

1. INTRODUCTION 4
nature. Like Ayurveda, this system believes that all objects in universe are made up of
five basic elements namely earth, water, sky, fire and air. The identification of causative
factors of disease is done through pulse reading, colour of body, study of voice, urine
examination, status of digestive system and examination of tongue.6
Naturopathy and Yoga
Naturopathy is not merely a system of treatment, but also a way of life, which is based on
laws of nature. The attention is particularly paid to eating and living habits, adoption of
purificatory measures, use of hydrotherapy, mud packs, baths, massage etc.
Yoga is a science as well an art of healthy living physically, mentally, morally and
spiritually. Its systematic growth from animal level to the normal, from there to the
divinity ultimately. The eight components of Yoga are restraint, observance of austerity,
physical postures, restraining of sense organs, breathing exercises, contemplation,
meditation and Samadhi.6
1.1.2 Herbal medicine today
Today herbal medicine has just improved ancient secrets and brought them on the market.
Many people turned to herbal medicine because they simply were disappointed with
traditional medicine or surgery. Herbal remedies are still relatively popular today, mainly
due to the fact that they are regarded as harmless because they are natural.
Rather than using a whole plant, pharmacologists identify, isolate, extract, and synthesize
individual components, thus capturing the active principles. In addition to active
ingredients, plants contain minerals, vitamins, volatile oils, glycosides, alkaloids,
bioflavonoid, and other substances that are important in supporting a particular herb's
medicinal properties. These elements also provide an important natural safeguard isolated
or synthesized active compounds can become toxic in relatively small doses; it usually
takes a much greater amount of a whole herb, with all of its components, to reach a toxic
level. Herbs are medicines, however, and they can have powerful effects. They should
not be taken lightly.
The efficacy of many medicinal plants has been validated by scientists abroad, from
Europe to the Orient. Thanks to modern technology, science can now identify some of the
specific properties and interactions of botanical constituents. With this scientific
documentation, we now know why certain herbs are effective against certain conditions.

1. INTRODUCTION 5
However, almost all of the current research validating herbal medicine has been done in
Germany, Japan, China, Taiwan, and Russia. And for the most part, the United States
Food and Drug Administration (FDA), which is responsible for licensing all new drugs
(or any substances for which medicinal properties are claimed) for use in the United
States, does not recognize or accept findings from across the sea. Doctors and
government agencies want to see American scientific studies before recognizing the
effectiveness of a plant as medicine. Yet even though substantial research is being done
in other countries, drug companies and laboratories in the United States so far have not
chosen to put much money or resources into botanical research. The result is that herbal
medicine does not have the same place of importance or level of acceptance in this
country as it does in other countries.7
1.1.3 Approach to drug discovery from plants
There are many approaches to the search for new biologically active principles in higher
plants. One can simply look for new chemical constitution and hope to find a biologist
who is willing to test each substance with whatever pharmacological tests available.
A second approach is simply to collect every readily available plant, prepare extract and
test each extract for one (or) more types of pharmacological activity. This random
collection, broad screening method is a reasonable approach that eventually should
produce useful drugs, but it is contingent as the availability of adequate findings and
appropriate predictable bioassay systems.4
1.1.4 Advantage of herbal medicines
There are a number advantages associated with using herbal medicines as opposed to
pharmaceutical products. Examples include the following:
Reduced risk of side effects: Most herbal medicines are well tolerated by the patient,
with fewer unintended consequences than pharmaceutical drugs. Herbs typically have
fewer side effects than traditional medicine, and may be safer to use over time.
Effectives with chronic conditions: Herbal medicines tend to be more effective for long-
standing health complaints that don't respond well to traditional medicine. One example
is the herbs and alternative remedies used to treat arthritis. Vioxx, a well-known
prescription drug used to treat arthritis, was recalled due to increased risk of
cardiovascular complications. Alternative treatments for arthritis, on the other hand, have

1. INTRODUCTION 6
few side effects. Such treatments include dietary changes like adding simple herbs,
eliminating vegetables from the nightshade family and reducing white sugar
consumption.
Lower cost: Another advantage to herbal medicine is cost. Herbs cost much less than
prescription medications. Research, testing, and marketing add considerably to the cost of
prescription medicines. Herbs tend to be inexpensive compared to drugs.
Widespread availability: Yet another advantage of herbal medicines are their
availability. Herbs are available without a prescription. You can grow some simple herbs,
such as peppermint and chamomile, at home. In some remote parts of the world, herbs
may be the only treatment available to the majority of people.4,7
1.1.5 Comparison of Herbal and Conventional Medicine
Conventional medications have a downside; many can cause harmful side effects and
only serve to lessen the symptoms instead of treat the root problem. Furthermore, many
conventional medicines are based on single compounds that bacteria become resistant to
over time. Herbal remedies, on the other hand, are comprised of complex compounds that
are difficult for bacteria to metabolize and use for colonization. Natural remedies have
the benefit of being non-toxic and devoid of side effects. They are also effective in
treating the sickness as well as the root cause of the condition. Along with these
important advantages, herbal medicines can boost immunity and enhance the body’s
defenses and natural ability to combat the invasion of foreign pathogens.
Many herbs, such as goldenseal and garlic, have natural antibiotic and antiviral properties
as well. Licorice soothes the throat, ginger prevents blood clots and lessens the risk of
heart disease and herbal teas help reduce tension. There are herbs that can address
respiratory, gastrointestinal, neurological and sexual problems as well. In many cases
natural herbal remedies can even help in managing the side effects of aggressive
treatments like chemotherapy. In summary, there is much to gain from the use of natural
remedies. They offer a safe and natural alternative to conventional medicine and are often
times more effective.8
1.1.6 Worldwide herbal trade
People are using herbal medicines from centuries for safety, efficacy, cultural
acceptability and lesser side effects. Plant and plant products have been utilized with

1. INTRODUCTION 7
varying success to cure and prevent diseases throughout history. Written records about
medicinal plants date back at least 5000 years to the Sumerians and ancient records have
suggested earlier use of medicinal plants. Due to side effects of synthetic products, herbal
products are gaining popularity in the world market. In spite of well-practiced knowledge
of herbal medicine and occurrence of a large number of medicinal plants, the share of
India in the global market is not up to the mark. The utilization of herbal drugs is on the
flow and the market is growing step by step .The annual turnover of the Indian herbal
medicinal industry is about Rs. 2,300 crore as against the pharmaceutical industry’s
turnover of Rs. 14,500 crores with a growth rate of 15 percent. The export of medicinal
plants and herbs from India has been quite substantial in the last few years. India is the
second largest producer of castor seeds in the world, producing about 1,25,000 tones per
annum.9
1.1.7 Relationship between man and herbs
Medicinal plants have been a major source of cure of human diseases since time
immemorial. Today, one fourth of the world population depends on traditional medicines.
Despite the introduction of antibiotics since the 1940's, even 80 per cent of the population
today relies on indigenous medicinal plants and the drugs. It is estimated that the global
traditional medicine market is growing at the rate of 7 - 15 per cent annually. The
medicinal plant value is about Rs.5000 crores in India and it is estimated that the country
exports about Rs.550 crore worth of herbal drugs but with the rich and diverse botanical
resources in our country, this is not an impressive export performance considering the
worldwide herbal market worth US 60 billion dollars. It is also necessary to integrate
modern knowledge with traditional knowledge. The drugs and products of the industry
are working on the scientifically defined techniques and explained with modern
biological and chemical definitions and tools, and that alone will give a therapeutically
active herbal original drug available for health care worldwide.9
The ayurvedic drug manufacturers in Kerala with the state government and central
assistance is putting up a Rs.62.5 crore company to set up a world standard QC lab, R&D
facility for the industrial benefit with all the modern equipment for advanced drug
standardization, quality and efficacy. This will also develop own protocols of quality
certification equivalent to other global standards.10

1. INTRODUCTION 8
1.1.8 Herbal medicine for market potential
The global market for herbal medicines currently stands at over $60 billion annually. The
sale of herbal medicines is expected to get higher at 6.4% an average annual growth rate.
Due to the contribution of numerous significant factors, the market of herbal medicines
has grown at an expressive rate worldwide. Some of them are preference of consumers
for natural therapies, growing concern regarding undesirable side effects of modern
medicines and the belief that herbal drugs are free from side effects, since millions of
people all over the world have been using herbal medicines for thousands of years; great
interest in alternative medicines; preference of populations for preventive medicine due
to increasing population age; the belief that herbal medicines might be of effective
benefit in the treatment of certain diseases where conventional therapies and medicines
have proven to be inadequate; tendency towards self-medication; improvement in quality,
proof of efficacy and safety of herbal medicines and high cost of synthetic medicines.
According to World Health Organization, herbal medicines are lucrative globally and
they represent a market value of about US$ 43 billion a year.
According to an estimate in 1991, the herbal medicine market in the European countries
was about $ 6 billion, with Germany accounting for $ 3 billion, France $ 1.6 billion and
Italy $ 0.6 billion while in other countries was 0.8 billion. In 1996, the herbal medicine
market in the European countries was about $ 10 billion, in USA about $ 4 million, in
India about $ 1.0 billion and in other countries was $ 5.0 billion. In 1997, the European
market alone reached about $ 7.0 billion. The German market corresponds to about 50%
of the European market, about $ 3.5 billion. This market is followed by France, $ 1.8
billion; Italy, $ 700 million;
The use of herbal remedies in the U.S. is widespread and increasing dramatically but the
physicians should have a good knowledge base and clear concept about herbal remedies
and should inquire about their use, discuss adverse effects, and monitor and identify
possible herb– drug interactions. There is a clear need for better public and physician
understanding of herbal products through health education, early detection and
management of herbal toxicities, scientific scrutiny of their use, and research on their
safety and effectiveness. Regulatory policies are also needed to protect people from
untoward effects on their health and finances.11

1. INTRODUCTION 9
1.1.9 Crude extract more potent than isolated chemical
Crud extract mixtures of plant are better than pure isolated chemicals. Several
biologically active compounds in a plant work together to produce greater effect then
single chemical on its own. The mixture of chemicals found in herbs can be more potent
than the single purified ingredient so beloved of drugs companies. Chemical partnerships
explain why whole herbs can work better than single purified ingredients. In other words,
the mixture has an effect greater than the sum of its parts. The synergism arises when two
or more factors interact in such a way that outcome is not additive but multiplicative. The
compound impact of the relationship can be so powerful that the result may be a whole
order of magnitude greater than the simple sum of the components. The observation
suggests that synergistic or antagonistic effect of various components of plant material in
its crude natural state may enhance therapeutic effects and reduce side effects, which may
not occur when one or more isolated chemical component are used alone in purified
forms. Synthesizing the bioactive ingredients would inevitably reduce or eliminate that
benefit. Anyway, herbal extract hopefully would delay resistance against diseases, while
bioactive principles can become our therapeutic armamentarium (Fig.1.1).
Figure 1.1: Crude extract more potent than isolated chemical

1. INTRODUCTION 10
Mechanism of synergic effect based on classical pharmacology, molecular biology and
clinical work can be divided into at least following four mechanisms:
1) Synergic multitarget effect: natural products affect not only one target, but several
targets and can cooperate in an agonistic and synergistic way
2) Pharmacokinetic and Physicochemical effect: natural products improve solubility
and /or the reabsorption rate and thereby the bioavailability.
3) Interference with the resistance mechanism of bacteria, natural product antagonizes
the resistance to antibiotics.
4) Elimination and neutralization effect, natural product by itself or after treatment
eliminate or neutralize within a drug preparation or in combination with synthetic
drug preparation adverse events, so that altogether effect improves.12
1.2 INFLAMMATION
Inflammation (Latin, inflammare, to set on fire) is part of the complex biological
response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or
irritants. Inflammation is a protective attempt by the organism to remove the injurious
stimuli and to initiate the healing process. Inflammation is not a synonym for infection,
even in cases where inflammation is caused by infection. Although infection is caused by
a microorganism, inflammation is one of the responses of the organism to the pathogen.
However, inflammation is a stereotyped response, and therefore it is considered as a
mechanism of innate immunity, as compared to adaptive immunity, which is specific for
each pathogen.13
Without inflammation, wounds and infections would never heal. Similarly, progressive
destruction of the tissue would compromise the survival of the organism. However,
chronic inflammation can also lead to a host of diseases, such as hay fever,
atherosclerosis, rheumatoid arthritis, and even cancer (e.g., gallbladder carcinoma). It is
for that reason that inflammation is normally closely regulated by the body.
Inflammation can be classified as either acute or chronic. Acute inflammation is the
initial response of the body to harmful stimuli and is achieved by the increased movement
of plasma and leukocytes (especially granulocytes ) from the blood into the injured
tissues. A cascade of biochemical events propagates and matures the inflammatory
response, involving the local vascular system, the immune system, and various cells

1. INTRODUCTION 11
within the injured tissue. Prolonged inflammation, known as chronic inflammation, leads
to a progressive shift in the type of cells present at the site of inflammation and is
characterized by simultaneous destruction and healing of the tissue from the
inflammatory process13
.
Causes14
Burns
Chemical irritants
Frostbite
Toxins
Infection by pathogens
Physical injury, blunt or penetrating
Immune reactions due to hypersensitivity
Ionizing radiation
Foreign bodies, including splinters, dirt and debris
Trauma
Cardinal signs
Acute inflammation is a short-term process, usually appearing within a few minutes or
hours and ceasing upon the removal of the injurious stimulus.14
It is characterized by five
cardinal signs: 15
The acronym that may be used for this is "PRISH" for Pain, Redness, Immobility (loss of
function), Swelling and Heat.
The traditional names for signs of inflammation come from Latin:
Dolor (pain)
Calor (heat)
Rubor (redness)
Tumor (swelling)
Functio laesa (loss of function)
The first four (classical signs) were described by Celsus (ca 30 BC–38 AD),16
while loss
of function was added later by Galen17
even though the attribution is disputed and the
origination of the fifth sign has also been ascribed to Thomas Sydenham18
and Virchow.
Redness and heat are due to increased blood flow at body core temperature to the

1. INTRODUCTION 12
inflamed site; swelling is caused by accumulation of fluid; pain is due to release of
chemicals that stimulate nerve endings. Loss of function has multiple causes.15
These five signs appear when acute inflammation occurs on the body's surface, whereas
acute inflammation of internal organs may not result in the full set. Pain only happens
where the appropriate sensory nerve endings exist in the inflamed area—e.g., acute
inflammation of the lung (pneumonia) does not cause pain unless the inflammation
involves the parietal pleura, which does have pain-sensitive nerve endings.15
1.2.1 Process of acute inflammation
The process of acute inflammation is initiated by cells already present in all tissues,
mainly resident macrophages, dendritic cells, histiocytes, kupffer cells and mastocytes.
These cells have present on their surfaces certain receptors named pattern recognition
receptors (PRRs), which recognize molecules that are broadly shared by pathogens but
distinguishable from host molecules, collectively referred to as pathogen-associated
molecular patterns (PAMPs). At the onset of an infection, burn, or other injuries, these
cells undergo activation (one of their PRRs recognize a PAMP) and release inflammatory
mediators responsible for the clinical signs of inflammation. Vaso dilation and the
resulting increased blood flow causes the redness (rubor) and increased heat (calor).
Increased permeability of the blood vessels results in an exudation (leakage) of plasma
proteins and fluid into the tissue (edema), which manifests itself as swelling (tumor).
Some of the released mediators such as bradykinin increase the sensitivity to pain
(hyperalgesia, dolor). The mediator molecules also alter the blood vessels to permit the
migration of leukocytes, mainly neutrophils, outside of the blood vessels (extravasation)
into the tissue. The neutrophils migrate along a chemotactic gradient created by the local
cells to reach the site of injury.14
The loss of function (functio laesa) is probably the
result of a neurological reflex in response to pain.
In addition to cell-derived mediators, several acellular biochemical cascade systems
consisting of preformed plasma proteins act in parallel to initiate and propagate the
inflammatory response. These include the complement system activated by bacteria, and
the coagulation and fibrinolysis systems activated by necrosis, e.g. a burn or a trauma.
The acute inflammatory response requires constant stimulation to be sustained.

1. INTRODUCTION 13
Inflammatory mediators have short half lives and are quickly degraded in the tissue.
Hence, acute inflammation ceases once the stimulus has been removed.14
Cyclooxygenase (COX)
COX is an enzyme that is responsible for formation of important biological mediators
called prostanoids,includingprostaglandins, prostacyclin and thromboxane.
Pharmacological inhibition of COX can provide relief from the symptoms of
inflammation and pain. Non-steroidal anti-inflammatory drug, such as aspirin and
ibuprofen, exert effects through inhibition of COX.
COX converts arachidonic acid (AA, an ω-6 PUFA) to prostaglandin H2(PGH2), the
precursor of the series-2 prostanoids. The enzyme contains two active sites:
a heme with peroxidase activity, responsible for the reduction of PGG2 to PGH2, and a
cyclooxygenase site, where arachidonic acid is converted into the hydroperoxy
endoperoxide prostaglandin G2(PGG2). The reaction proceeds through H atom abstraction
from arachidonic acid by a tyrosine radical generated by the peroxidase active site. Two
O2 molecules then react with the arachidonic acid radical, yielding PGG2.
At present, three COX isoenzymes are known: COX-1, COX-2, and COX-3.The COX-
3 is a splice variant of COX-1, which retains intron one and has aframeshift mutation;
thus some prefer the name COX-1b or COX-1 variant(COX-1v).The
main COX inhibitors are the non-steroidal anti-inflammatory drugs (NSAIDs).
The classical COX inhibitors are not selective and inhibit all types of COX. The resulting
inhibition of prostaglandin and thromboxane synthesis has the effect of reduced
inflammation, as well as antipyretic, antithrombotic and analgesic effects.
Selectivity for COX-2 is the main feature of celecoxib, rofecoxib, and other members of
this drug class. Because COX-2 is usually specific to inflamed tissue, there is much less
gastric irritation associated with COX-2 inhibitors, with a decreased risk of peptic
ulceration.
A Natural COX inhibitor which is obtained from natural sources is also generally not
selective and inhibits all types of COX. A large number of studies have revealed that
Medicinal Plants have potent anti-inflammatory actions are called Natural COX inhibitor
and such as mushrooms, like Maitake, able to partially inhibit COX-1 and COX-2.14

1. INTRODUCTION 14
1.2.2 Exudative component
The exudative component involves the movement of plasma fluid, containing important
proteins such as fibrin and immunoglobulins (antibodies), into inflamed tissue. This
movement is achieved via the chemically induced dilation and increased permeability of
blood vessels, which results in a net loss of blood plasma. The increased collection of
fluid into the tissue causes it to swell (edema). This extravasated fluid is funneled by
lymphatics to the regional lymph nodes, flushing bacteria along to start the recognition
and attack phase of the adaptive immune system system.14
1.2.3 Vascular changes
Acute inflammation is characterised by marked vascular changes, including vasodilation,
increased permeability and the slowing of blood flow, which are induced by the actions
of various inflammatory mediators. Vasodilation occurs first at the arteriole level,
progressing to the capillary level, and brings about a net increase in the amount of blood
present, causing the redness and heat of inflammation. Increased permeability of the
vessels results in the movement of plasma into the tissues, with resultant stasis due to the
increase in the concentration of the cells within blood - a condition characterized by
enlarged vessels packed with cells. Stasis allows leukocytes to marginate (move) along
the endothelium, a process critical to their recruitment into the tissues. Normal flowing
blood prevents this, as the shearing force along the periphery of the vessels moves cells in
the blood into the middle of the vessel.15
1.2.4 Plasma cascade systems
The complement system, when activated, results in the increased removal of pathogens
via opsonisation and phagocytosis.
The kinin system generates proteins capable of sustaining vasodilation and other physical
inflammatory effects.
The coagulation system or clotting cascade which forms a protective protein mesh over
sites of injury.
The fibrinolysis system, which acts in opposition to the coagulation system, to
counterbalance clotting and generate several other inflammatory mediators.15

1. INTRODUCTION 15
1.2.5 Cellular component
The cellular component involves leukocytes, which normally reside in blood and must
move into the inflamed tissue via extravasation to aid in inflammation. Some act as
phagocytes, ingesting bacteria, viruses, and cellular debris. Others release enzymatic
granules which damage pathogenic invaders. Leukocytes also release inflammatory
mediators which develop and maintain the inflammatory response. Generally speaking,
acute inflammation is mediated by granulocytes, while chronic inflammation is mediated
by mononuclear cells such as monocytes and lymphocytes.15
1.2.6 Leukocyte extravasation
Various leukocytes are critically involved in the initiation and maintenance of
inflammation. These cells must be able to get to the site of injury from their usual
location in the blood, therefore mechanisms exist to recruit and direct leukocytes to the
appropriate place. The process of leukocyte movement from the blood to the tissues
through the blood vessels is known as extravasation, and can be divided up into a number
of steps: 14-15
Leukocyte localisation and recruitment to the endothelium local to the site of
inflammation – involving margination and adhesion to the endothelial cells:
Recruitment of leukocytes is receptor-mediated. The products of inflammation, such as
histamine, promote the immediate expression of P-selectin on endothelial cell surfaces.
This receptor binds weakly to carbohydrate ligands on leukocyte surfaces and causes
them to "roll" along the endothelial surface as bonds are made and broken. Cytokines
from injured cells induce the expression of E-selectin on endothelial cells, which
functions similarly to P-selectin. Cytokines also induce the expression of integrin ligands
on endothelial cells, which further slow leukocytes down. These weakly bound
leukocytes are free to detach if not activated by chemokines produced in injured tissue.
Activation increases the affinity of bound integrin receptors for ligands on the endothelial
cell surface, firmly binding the leukocytes to the endothelium.
Migration across the endothelium, known as transmigration, via the process of
diapedesis: Chemokine gradients stimulate the adhered leukocytes to move between
endothelial cells and pass the basement membrane into the tissues.

1. INTRODUCTION 16
Movement of leukocytes within the tissue via chemotaxis: Leukocytes reaching the
tissue interstitium bind to extracellular matrix proteins via expressed integrins and CD44
to prevent their loss from the site. Chemoattractants cause the leukocytes to move along a
chemotactic gradient towards the source of inflammation.
1.2.7 Morphologic patterns of inflammation
Specific patterns of acute and chronic inflammation are seen during particular situations
that arise in the body, such as when inflammation occurs on an epithelial surface, or
pyogenic bacteria are involved.
Granulomatous inflammation: Characterised by the formation of granulomas, they are
the result of a limited but diverse number of diseases, which include among others
tuberculosis, leprosy, sarcoidosis, and syphilis.
Fibrinous inflammation: Inflammation resulting in a large increase in vascular
permeability allows fibrin to pass through the blood vessels. If an appropriate
procoagulative stimulus is present, such as cancer cells, a fibrinous exudate is deposited.
This is commonly seen in serous cavities, where the conversion of fibrinous exudate into
a scar can occur between serous membranes, limiting their function.
Purulent inflammation: Inflammation resulting in large amount of pus, which consists
of neutrophils, dead cells, and fluid. Infection by pyogenic bacteria such as staphylococci
is characteristic of this kind of inflammation. Large, localised collections of pus enclosed
by surrounding tissues are called abscesses.
Serous inflammation: Characterised by the copious effusion of non-viscous serous fluid,
commonly produced by mesothelial cells of serous membranes, but may be derived from
blood plasma. Skin blisters exemplify this pattern of inflammation.
Ulcerative inflammation: Inflammation occurring near an epithelium can result in the
necrotic loss of tissue from the surface, exposing lower layers. The subsequent
excavation in the epithelium is known as an ulcer.14
1.2.8 Inflammatory disorders
Inflammatory abnormalities are a large group of disorders which underlie a vast variety
of human diseases. The immune system is often involved with inflammatory disorders,
demonstrated in both allergic reactions and some myopathies, with many immune system
disorders resulting in abnormal inflammation. Non-immune diseases with etiological

1. INTRODUCTION 17
origins in inflammatory processes include cancer, atherosclerosis, and ischaemic heart
disease.
A large variety of proteins are involved in inflammation, and any one of them is open to a
genetic mutation which impairs or otherwise dysregulates the normal function and
expression of that protein.14
Examples of disorders associated with inflammation include:
Acne vulgaris
Asthma
Autoimmune diseases
Coeliac disease
Chronic prostatitis
Glomerulonephritis
Hypersensitivities
Inflammatory bowel diseases
Pelvic inflammatory disease
Reperfusion injury
Rheumatoid arthritis
Sarcoidosis
Transplant rejection
Vasculitis
Interstitial cystitis
1.2.9 Resolution of inflammation
The inflammatory response must be actively terminated when no longer needed to
prevent unnecessary "bystander" damage to tissues.14
Failure to do so results in chronic
inflammation, and cellular destruction. Resolution of inflammation occurs by different
mechanisms in different tissues. Mechanisms which serve to terminate inflammation
include: 14, 19
Short half-life of inflammatory mediators in vivo.
Production and release of Transforming growth factor (TGF) beta from macrophages20-22
Production and release of Interleukin 10 (IL-10)23
Production of anti-inflammatory lipoxins24

1. INTRODUCTION 18
Downregulation of pro-inflammatory molecules, such as leukotrienes
Upregulation of anti-inflammatory molecules such as the Interleukin 1 receptor
antagonist or the soluble tumor necrosis factor receptor (TNFR)
Apoptosis of pro-inflammatory cells25
Desensitization of receptors
Increased survival of cells in regions of inflammation due to their interaction with the
extracellular matrix (ECM)26-27
Downregulation of receptor activity by high concentrations of ligands
Cleavage of chemokines by matrix metalloproteinases (MMPs) might lead to production
of anti-inflammatory factors.26
1.2.10 Exercise as a treatment for inflammation
Regular physical activity is reported to decrease markers of inflammation28-30
although
the correlation is imperfect and seems to reveal differing results contingent upon training
intensity. For instance, while baseline measurements of circulating inflammatory markers
do not seem to differ greatly between healthy trained and untrained adults, long-term
chronic training may help reduce chronic low-grade inflammation.31-33
On the other hand,
levels of inflammatory markers (IL-6) remained elevated longer into the recovery period
following an acute bout of exercise in patients with inflammatory diseases, relative to the
recovery of healthy controls. It may well be that low-intensity training can reduce resting
pro-inflammatory markers (CRP, IL-6), while moderate-intensity training has milder and
less-established anti-inflammatory benefits.34-35
There is a strong relationship between
exhaustive exercise and chronic low-grade inflammation. Marathon running may enhance
IL-6 levels as much as 100 times over normal and increases total leuckocyte count and
neturophil mobilization. As such, individuals pursuing exercise as a means to treat the
other factors behind chronic inflammation may wish to balance their exercise protocol
with bouts of low-intensity training, while striving to avoid chronic over-exertion.36., 37
1.2.11 Medicinal Plants as Anti-Inflammatory Agents
Ananas comosus ( L.) Merr. (Bromeliaceae)
Ananas comosus (L.) Merril (Pineapple) has been used as a medicinal plant in several
native cultures and its major active principle, Bromelain, has been known chemically
since 1876. Bromelain is a general name for a family of sulphydryl proteolytic

1. INTRODUCTION 19
compounds obtained from Ananas comosus L. The primary component of bromelain is a
sulphydryl proteolytic fraction. It also contains peroxidase, acid phosphatase, several
protease inhibitors and originally bound calcium. Eight basic proteolytically active
components have been detected in the stem. Bromelain seems to have both direct as well
as indirect actions involving other enzyme systems exerting its anti-inflammatory effect.
It inhibits the inflammatory pain in rats in a dose dependent manner. It reduces pain and
inflammation associated with surgery, arthritis, trauma or sports injury. Bromelain was
the most potent of nine anti-inflammatory substances tested on experimental rats.
Bromelain interferes with the arachidonic acid cascade there by preventing the formation
of pro-inflammatory eicosanoids. Non-steroidal anti-inflammatory drugs inhibit COX,
which is required for the synthesis of two prostaglandins, resulting in a decrease in both
pro and anti-inflammatory prostaglandins. Bromelain has been shown to inhibit
prostaglandins even though its action is significantly weaker. Bromelain has been shown
to reduce edema, accelerate healing and lowers pain and inflammation after surgery in
clinical trials.38
Boswellia serrata Roxb. (Burseraceae)
Boswellia serrata Roxb has been used traditionally in Indian Ayurvedic medicine and is
well known for its anti-inflammatory activity. The resinous gum of the bark is known as
guggulu in Ayurveda and is also used in modern phytomedicine. It has been reported to
be a powerful anti-inflammatory agent without the ulceration or irritation as observed in
non-steroidal anti-inflammatory drugs. Bosewellia has been shown to possess sedative,
analgesic, anti-inflammatory and anticancer effects. The resin obtained from the plant is
recommended for rheumatoid arthritis, osteoarthritis, fibromyositis and spondylitis.
Patients treated with Bosewellia reported decreases in knee pain, joint swelling and
increases in knee flexion and walking distance. Four pentacyclic triterpene acids
including the bioactive compound β-boswellic acid which interferes with leukotriene
biosynthesis have been isolated from B. serrata. It is a specific and dose dependent
inhibitor of 5- lipoxygenase, 5-eicosatetraenoic acid and leukotriene B4. These chemical
mediators of inflammation are implicated in the pathogenesis of many diseases including
asthma, arthritis, colitis and cancer. Bosewellia inhibits human leukocyte elastase (HLE)
under in vitro conditions. HLE inhibitor medications have been developed for the

1. INTRODUCTION 20
treatment of asthma, emphysema and cystic fibrosis. Bosewellic acids were found to be
more potent inhibitors of human topoisomerases-I and II-α than chemotherapeutic agents
that work largely by inhibition of these enzymes. The mechanism of action of beta
boswellic acid has been recently reported. B. serrata extract can decrease the
glycosaminoglycan degradation which keeps the cartilages in better condition thus
preventing the progression of osteoarthritis.39
Callophyllum inophyllum L. and Mesua ferrea L. (Clusiaceae)
Callophyllum inophyllum L. and Mesua ferrea L. has been commonly used for the
treatment of rheumatism, skin diseases, dysentery and bleeding piles. The whole plant is
medicinal and contains compounds such as xanthones, triterpenes, coumarins and
glucosides. The xanthones of Callophyllum and Mesua have been found to produce
significant anti-inflammatory activity in normal as well as adrenalectomised rats by both
intra-peritoneal and oral routes. Usually the anti-inflammatory agents in clinical use
exhibit analgesic and antipyretic properties along with ulcerogenicity and impairment of
blood clotting as side effects. But the xanthones of C. inophyllum and M. ferrea did not
possess any such properties and thus points to the possibility of developing anti-
inflammatory drugs of future use.40
Calotropis gigantea (L.) R. Br. (Asclepiadaceae)
Calotropis gigantea (L.) R. Br. is an important medicinal plant where all parts of the
plant including the milky secretion have been claimed to possess varied medicinal uses. It
has been claimed to be useful in treating skin diseases and healing of wounds and ulcers.
The methanolic extract of Calotropis gigantea leaves revealed the anti-inflammatory
activity in experimental rats using paw edema test. Anti-inflammatory effects of aqueous
extract of leaves and latex of C. procera were reported earlier.41
Calotropis procera (Ak.) R.Br. (Asclepiadaceae)
Calotropis procera (Ait) R Br. is a well known medicinal plant in the traditional
medicine system of India. It is used in the treatment of skin diseases, rheumatism and
aches. It has been reported to possess antiinflammatory, analgesic and weak antipyretic
activities. The latex was reported to be as potent as standard anti-inflammatory drug
phenylbutazone in inhibiting inflammatory response induced by different inflammatory
agents in acute and chronic models. The anti-inflammatory activity of the latex of C.

1. INTRODUCTION 21
procera and its methanolic extract against various inflammatory mediators as well as on
leucocyte flux induced by carrageenan in rat paw edema model have been reported.41
Camellia sinensis (L.) Kuntze (Theaceae)
Camellia sinensis (L.) Kuntze is one of the most commonly consumed beverages in the
world. The established pharmacological activity of the green tea extracts are attributed to
its high content of polyphenols/catechins, mainly epigallocatechin-3-gallate (EGCG). The
potential effect of green tea in arthritis on collagen type-II-induced arthritis in mice has
been reported. The anti-inflammatory effect of green tea polyphenols was reflected in a
marked inhibition of the inflammatory mediators such as COX 2, interferon–γ and TNF-α
in arthritic joints. Histopathological studies revealed a reduction in biochemical markers
correlated with the marked reduction in inflammation in synovium. Studies have shown
that most of the effects of green tea extracts are mimicked by its constituent polyphenol,
EGCG. Further studies have shown that EGCG inhibited the transcription factor, nuclear
factor-kappa-B (NF-κ B) inconjunction with pro-inflammatory cytokines IL-1β-inducible
nitric oxide synthase (Inos) and COX 2, resulting in reduction of nitric oxide and
prostaglandin E2 (PGE2) in vitro.41
Cannabis sativa L. (Cannabinaceae)
Cannabis sativa L. has been used in various preparations for their medicinal effects
including anti-pyretic, anti-rheumatic, anti-allergic and analgesic purposes. It is possible
that the anti-inflammatory and anti-asthmatic properties of this herb are mediated through
effects on arachidonate metabolism. The constituents of Cannabis are known to stimulate
and inhibit prostaglandin releases by influencing enzymes of the arachidonate pathway.41
Centella asiatica (L.) Urban
It belongs to the family Apiaceae and is commonly found in parts of Asia and the Middle
East. Centella has been used in traditional medicine in Asia for 100 years. In Ayurveda,
Centella is effectively used in the treatment of inflammation, anaemia, asthma, blood
disorders, bronchitis, fever, urinary discharge and splenomegaly. The water extract of the
plant was used to study the anti-inflammatory and analgesic activity in adult male rats.
The extract elicited dose dependent anti-inflammatory activity at 2 mg/kg concentration.
This study revealed that the extract is similar to mefenamic acid and interestingly 10
mg/kg extract showed a significantly higher effect when compared to mefenamic acid.

1. INTRODUCTION 22
These compoundsmay be present in the extract which contributes to the anti-
inflammatory and analgesic property in the study. These findings justify the traditional
use of Centella in the treatment of inflammatory conditions.41
Curcuma longa L. (Zingiberaceae)
Curcuma longa L. is a perennial herb distributed throughout tropical and subtropical
regions of the world. It is widely cultivated in Asiatic countries, mainly in India and
China. As turmeric powder it has been in continuous use for its flavouring, as a spice in
both vegetarian and non-vegetarian food preparations and has digestive properties. There
is a great number of papers in the literature relating the activity of compounds extracted
from C. longa L. being potent inhibitors of inflammation. The activity of curcumin and
other semi synthetic analogues in experimental rats were demonstrated. Studies on anti
inflammatory activities included in vitro, animal and human models. The laboratory
studies have identified a number of different molecules involved in inflammation that are
inhibited by curcumin including phospholipase, lipoxygenase, cyclooxygenase-2,
leukotriens, thromboxane, prostaglandins, nitric oxide, collagenase, elastase,
hyaluronidase, monocyte chemoattractant protein-1 (MCP-1), interferon–inducible
protein, tumour necrosis factor (TNF) and interleukin-12 (IL-12). The anti-inflammatory
activity demonstrated in the experiment may be due to inhibition of a number of different
molecules that play a role in inflammation. In animal studies, oral administration of
curcumin to rats decreased the levels of inflammatory glycoprotein with a reduction in
paw inflammation. Curcumin was also found to be inhibiting the carrageenan induced
paw edema in mice and rats with an ED 50 dose 48 and 100.2 mg/kg respectively.41
Euphorbia heterophylla L. (Euphorbiaceae)
Euphorbia heterophylla is a local medicinal plant commonly known as ‘spurge weed’. It
is used in ethnomedicine for the treatment of constipation, bronchitis and asthma [94]. It
grows in semi humid places especially in cassava, cow pea and soyabean plantations.
Phytochemical studies have revealed the presence of saponins, diterpenes and
phorbolesters in the extracts. The anti-inflammatory activity of the aqueous and
methanolic extract of Euphorbia heterophylla were evaluated by carrageenin induced rat
paw edema test. The aqueous extract of Euphorbia showed significant anti-inflammatory
activity (P<0.001) comparable to the reference drug. But the methanolic extract did not

1. INTRODUCTION 23
show any appreciable anti-inflammatory activity. These studies were in agreement with
the earlier investigations suggesting the presence of a flavanoid, quercetin, which is a
known anti-inflammatory agent. The significant level of anti inflammatory activity of the
aqueous extract could be attributed to high amount of flavanoids present in the extract.
This study justifies the traditional use of Euphorbia in the treatment of inflammatory
disease conditions such as asthma. 41
Gastrodia elata Blume (Orchidaceae)
Gastrodia elata Blume is a very important traditional herbal medicine used to treat head
ache, migraine, dizziness, epilepsy, rheumatism, neuralgia, paralysis and other disorders.
The anti-inflammatory and analgesic activities of these phenolic extracts were studied
using animal models. They suggested that these phenolic compounds inhibited COX
activity and silica induced reactive oxygen species (ROS) generation in a dose-dependent
manner. The phenolic compounds of Gastrodia elata are anti-inflammatory, which could
be related to inhibition of COX activity and to anti-oxidant activity. Consideration of the
structure-activity relationship of these compounds of G. elata on the anti-inflammatory
action revealed that both C-4 hydroxy and C-3 methoxy radicals of benzyl aldehyde play
an important role in anti-inflammatory activities. 41
Harpagophytum procumbens (Burch.) DC (Pedaliaceae)
Harpagophytum procumbens (Burch.) DC is commonly known as Devil’s claw and is a
native of South Africa. The root tubers of the plant are used in herbal preparations. Leung
and Foster reported three iridoid glycosides viz. harpagoside, harpagide and procumbide
and are responsible for the anti-inflammatory and analgesic actions. These glycosides
effectively reduced Osteoarthritis (OA) pain and was comparable with that of the
analgesic/ cartilage protective drug, Diacerhein. H. procumbens at the rate of 600-120
mg/day was helpful in reducing low back pain. The anti-inflammatory and analgesic
effect of the aqueous extract of H. procumbens has been reported recently. 41
Kalanchoe crenata Andr. (Crassulaceae)
Klanchoe crenata Andr. is commonly known as “never die” or “dog’s liver”. It has been
traditionally used for the treatment of ear ache, small pox, head ache, inflammation, pain,
asthma, palpitations, convulsion and general debility. The anti-inflammatory property of
the leaf extract of K. crenata was scientifically validated. They reported the presence of

1. INTRODUCTION 24
sterols, flavanoids and saponins in the different extracts which were responsible for the
acute and chronic anti-inflammatory activity against various phlogistic agents. They act
by inhibition of COX and therefore inhibit the production of gastric prostaglandins which
in turn leads to a reduction in the gastric mucus and an increase in mucosal permeability.
This can be attributed to the inhibition of COX. Hence, it was concluded from this study
that the flavanoids in the n-butanol fraction was responsible for its pharmacological
activities. 41
Mangifera indica L. (Anacardiaceae)
Mangifera indica L. aqueous extract, known as Vimang in Cuba, is used to improve the
quality of life in patients suffering from elevated stress. Mangifera indica bark aqueous
extract. Analgesia was determined using acetic acid induced abdominal constriction and
formalin induced licking. Antiinflammatory effects were studied using carrageenin and
formalin inducededema. They reported polyphenols in the extract which might be
responsible for the effect. Edema formation was significantly inhibited both in
carrageenin and formalin models. 41
Plumeria accuminata W.T. Aiton (Apocyanaceae)
Plumeria acuminata W.T. Aiton belongs to the family Apocynaceae and is widely
distributed in Southern parts of India. In traditional medicine system different parts of the
plant have been used in a variety of diseases. The milky juice is employed for the
treatment of inflammation and rheumatism. The leaves are reported to have anti-
inflammatory and rubefacient in rheumatism and have strong purgative effect. The
methanol extract of Plumeria acuminata exhibited significant anti-inflammatory activity
on the tested experimental models in both acute and chronic inflammation models. The
Methanolic extract produced significant (P<0.001) anti-inflammatory activity and the
results were comparable to that of indomethacin as a standard anti-inflammatory drug.
Their studies indicated that the extract acted in later phases probably involving
arachidonic acid metabolites which produce an edema dependent on neutrophil
mobilization. 41
Ricinus communis L. (Euphorbiaceae)
Ricinus communis Linn. is a small tree distributed throughout the tropics and warm
temperate regions of the world. In Indian traditional system of medicine different parts of

1. INTRODUCTION 25
this plant has been used to cure inflammation and liver disorders. The anti-inflammatory
activity of the methanolic extract of Ricinus communis Linn. root was reported by the
methanolic extract at a dose of 250 mg/kg p.o exhibited significant (p<0.001) anti-
inflammatory activity in carrageenin induced rat paw edema model and a higher dose of
500 mg/kg p.o also\ exhibited significant (p<0.001) activity in cotton pellet granuloma
model in Wistar albino rats. Flavanoids have been reported to have anti-inflammatory
and antiarthritic activity. The anti-inflammatory activity of Ricinus can be attributed to
the presence of phytochemicals such as flavanoids, alkaloids and tannins in the plant
extract. 41
Salix alba L. (Salicaceae)
Salix alba L. is commonly known as the Willow tree and its bark contains heavy
concentrations of salicin, a glycoside, which is the precursor of aspirin. Salicin is
responsible for the anti-inflammatory and analgesic actions. The consumption of herbal
combination containing 100 mg willow bark for two months improved functioning via
pain relief in OA. A trial study revealed that 1360 mg of willow bark extract per day
(delivering 240 mg of salicin) for two weeks to be effective in treating pain associated
with knee and hip. A four week trial found that willow extract containing 240 mg of
salicin was effective in reducing exacerbations of low back pain. 42
Sida cordifolia L. (Malvaceae)
Sida cordifolia Linn is an extensively used herbal ingredient in the Ayurvedic system of
medicine in the Indian subcontinent. The antiinflammatory and analgesic activities of the
water extract of the plant in animal models were reported. Phytochemical analyses from
time to time have revealed the presence of ephedrine, vasicinol, vascicinone and N-
methyl tryptophan. Chloroform, methanol, ethyl acetate and butanol extracts also showed
significant activity in experimental models. In addition another chemical constituent (5' –
Hydroxymethyl - 1'-(1,2,3,9-tetrahydro-pyrrolo[2,1-b] quinazolin -1- yl)-heptan-1-one)
was reported141 from the aerial parts of Sida cordifolia. The bioactivity thus reported
was due to the inhibitory effect of the compound by the inhibition of COX enzyme
leading to the inhibition of prostaglandin synthesis. 41

1. INTRODUCTION 26
Silybum marianum (L.) Gaertn. (Asteraceae)
Silybum marianum (L.) Gaertn. is an important medicinal plant commonly known as
‘Milk thistle’ or ‘St. Mary’s Thistle’. The anti-inflammatory activity of this plant has
been reported earlier. The plant extract was reported to contain an important bioactive
principle, sylimarin, which belongs to the flavanolignan group and possess anticancer,
antiinflammatory, antioxidant and immunomodulatory effects. 43
Spilanthes acmella Murr. (Asteraceae)
Spilanthes acmella Murr. is an indigenous herb growing as an annual throughout the
tropics. The whole plant is claimed to possess medicinal properties. The flowers are
chewed to relieve tooth ache and the crushed plant is used in rheumatism. The presence
of flavanoids in the aqueous extract which is responsible for the significant anti-
inflammatory and analgesic property of the plant. The extract produced dose dependent
and significant inhibition of prostaglandins which are involved in the late phase of acute
inflammation and pain perception. 44
Tripterygium wilfordii Hook F (Celastraceae)
Tripterygium wilfordii Hook F is a perennial vine like plant that grows in China and
Thaiwan. The root of the plant is medicinal and is used for the treatment of inflammatory
diseases like rheumatoid arthritis, asthma, nephritis etc for centuries ago. The ethanolic
and ethyl acetate extract of the plant is used in the treatment of rheumatoid arthritis. The
anti-inflammatory effect of T. wilfordii was believed to be due to the presence of
triptolide, the active ingredient. 45
Uncaria tomentosa (Willd.) DC. and U. guianensis J.F. Gmel (Rubiaceae)
Uncaria tomentosa (Willd.) DC. and U. guianensis DC commonly known as Cat’s claw
is a Peruvian vine with medicinal properties that are well documented in alternative
medicine literature. The anti-inflammatory activity of Cat’s claw extract was reported
earlier.In Peruvian medicinal system, the extract of both species has been used
interchangeably to treat inflammatory and non-inflammatory conditions. The chemical
composition of U. tomentosa and U. guianensis vary and accordingly the anti-
inflammatory effects are independent of one another. The anti-inflammatory activity of
U. tomentosa is mainly due to the active constituent, pentacyclic oxindole alkaloid.46

1. INTRODUCTION 27
Zingiber officinale Roscoe (Zingiberaceae)
Zingiber officinale Rosc. is one of the most common constituents of diets world wide and
is reported to possess antioxidant, anti-inflammatory, antiseptic anti-inflammatory,
analgesic and carminative properties. In folk medicine it has been used against pain,
inflammation, arthritis, urinary infections and gastrointestinal disorders. Ayurveda
supports the use of ginger to treat inflammatory and rheumatic disorders. Ginger oil
contains a mixture of constituents like monoterpenes and sesquiterpenes which were
reported to have anti-inflammatory and analgesic activities. The anti-inflammatory
activity of the ginger essential oil was determined by pleuricy test using carrageenan (200
μg /cavity) in experimental mice. Ginger essential oil and indomethacin in 200 and 500
mg/kg was significant in proving anti-inflammatory activity. The experimental data
suggested that ginger essential oil does not have influence on cells’ recruitment different
to that observed for other essential oils. Gingerol has been reported to have anti-
inflammatory actions, which include suppression of both COX metabolites of arachidonic
acid . The anti-inflammatory activity shown by ginger essential oil could be owing to the
inhibition of prostaglandin release and hence ginger may act in a way similar to other
nonsteroidal anti-inflammatory drugs which interfere with prostaglandin biosynthesis.47
1.3 TOPICAL DRUG DELIVERY SYSTEM
Topical preparations are used for the localized effects at the site of their application by
virtue of drug penetration into the underlying layers of skin or mucous membranes. The
main advantage of topical delivery system is to bypass first pass metabolism. Avoidance
of the risks and inconveniences of intravenous therapy and of the varied conditions of
absorption, like pH changes, presence of enzymes, gastric emptying time are other
advantage of topical preparations. Semi-solid formulation in all their diversity dominate
the system for topical delivery, but foams, spray, medicated powders, solution, and even
medicated adhesive systems are in use. The topical drug delivery system is generally used
where the others system of drug administration fails or it is mainly used in pain
management, contraception, and urinary incontinence48.
Topical delivery includes two basic types of product:
External topicals that are spread, sprayed, or otherwise dispersed on to cutaneous tissues
to cover the affected area.

1. INTRODUCTION 28
Internal topicals that are applied to the mucous membrane orally, vaginally or
on anorectal tissues for local activity49
.
For the most part topical preparations are used for the localized effects at the site of their
application by virtue of drug penetration into the underlying layers of skin or mucous
membranes. Although some unintended drug absorption may occur, it is sub therapeutics
quantities and generally of minor concern50
.
1.3.1 Advantages of Topical Drug Delivery Systems: 51-52
Avoidance of first pass metabolism.
Convenient and easy to apply.
Avoidance of the risks and inconveniences of intravenous therapy and of the varied
conditions of absorption, like pH changes, presence of enzymes, gastric emptying time
etc.
Achievement of efficacy with lower total daily dosage of drug by continuous drug input.
Avoids fluctuation in drug levels, inter- and intrapatient variations.
Ability to easily terminate the medications, when needed.
A relatively large area of application in comparison with buccal or nasal cavity
Ability to deliver drug more selectively to a specific site.
Avoidance of gastro-intestinal incompatibility.
Providing utilization of drugs with short biological half-life, narrow therapeutic window.
Improving physiological and pharmacological response.
Improve patient compliance.
Provide suitability for self-medication.
Disadvantages of Topical Drug Delivery Systems: 53-54
Skin irritation of contact dermatitis may occur due to the drug and/or excipients.
Poor permeability of some drugs through the skin.
Possibility of allergenic reactions.
Can be used only for drugs which require very small plasma concentration for action
Enzyme in epidermis may denature the drugs
Drugs of larger particle size not easy to absorb through the skin
1.3.2 Classification of Topical Drug Delivery Systems: 54
Classification of Topical Drug Delivery Systems based on physical state

1. INTRODUCTION 29
(A) Solid:
Powder
Aerosol
Plaster
(B)Liquid:
Lotion
Liniment
Solution
Emulsion
Suspension
Aerosol
1.3.3 Skin
Delivery of drugs to the skin is an effective and targeted therapy for local dermatological
disorders. This route of drug delivery has gained popularity because it avoids first-pass
effects, gastro-intestinal (GI) irritation, and metabolic degradation associated with oral
administration. Topical formulations provide a suitable delivery system for drugs because
they are less greasy and can be easily removed from the skin. Nowadays the extensive
research has been considered that topical route is possible site for the systemic, localized
delivery of drug.55
For the topical drug delivery, the main barrier is skin. To understand the concept of
topical drug delivery system, it is important to review the structural and biochemical
features of human skin and those characteristics which contribute to the barrier function
and the rate of drug access into the body via skin.
Anatomy and physiology of skin
Human skin is, on average, 0.5 mm to 2 mm and composed of four main layers: the
stratum corneum, viable epidermis, dermis and subcutaneous tissue (Fig.1.2).The thick
(10-20mm) surface layer, the stratum corneum is highly hydrophobic and contains 10-15
layers of interdigitated corneocytes, which are constantly shed and renewed. Its
organization can be the “brick and mortar” model, in which extracellular lipid accounts
(c) Semi-solid:
Ointment
Cream
Paste
Gel
Jelly
Suppository

1. INTRODUCTION 30
for 10% of the dry weight of this layer, and the 90% is intracellular protein (mainly
keratin).56,57
The stratum corneum lacks phospholipids, but is enriched in ceramides and neutral lipids
(cholesterol, fatty acids, cholesteryl esters) that are arranged in a bilayer format and form
so called ‘lipid channels’. Barrier lipids are tightly controlled and any impairment to the
skin results in active synthetic processes to restore them. The skin’s barrier function
appears to depend on the specific ratio of various lipids.
Because of its highly organized structure the stratum corneum is permeability barrier to
external materials, and is regarded as the rate- limiting factor in the penetration of
therapeutic agents through the skin. The ability of various agents to interact with the
intercellular lipid therefore dictates the degree to which absorption is enhanced.
Figure 1.2: Structure of skin
Epidermis:
The viable epidermis consists of multiple layers of keratinoctes at various stages of
differentiation. The basal layer contains actively dividing cells, which migrate upwards to
successively form the spinous, granular and clear layers. As part of this process, the cells
gradually lose their nuclei and undergo changes in composition. The role of the viable
epidermis in skin barrier function is mainly related to the intercellular lipid channels and

1. INTRODUCTION 31
to several partitioning phenomena. Depending on their solubility, drugs can partition
from layer to layer after diffusing through the stratum corneum. Several other cells (e.g.
melanocytes, langerhans cells, dendritic T cells, and epidermotropic lymphoctes) are also
scattered throughout the viable epidermis, which also contains a variety of active
catabolic enzymes (e.g. esterases, phosphatases, proteases nucleotidases and lipases.
Dermis and hypodermis
The dermis is largely a layer that is rich in blood vessels, lymphatic vessels and nerve
endings. An extensive network of dermal capillaries connects to the systemic circulation,
with considerable horizontal branching from the arterioles and venules in the papillary
dermis to form plexuses and to supply capillaries to hair follicles and glands. Dermal
lymphatic vessels help drain excess extra cellular fluid and clear antigenic materials.
The elasticity of the dermis is attributed to a network of protein fibers, including collagen
(type 1 and 3) and elastin, which are embedded in an amorphous glycosaminoglycan
ground substance. The dermis also contains scattered fibroblasts, macrophages, mast cells
and leukocytes. Hair follicles, sebaceous glands and sweat glands are found in the dermis
and subcutis, and might serve as additional specific, albeit fairly limited pathways for
drug absorption.58
1.3.4 Mechanism of topical delivery
When a drug system is applied topically, the drug diffuses out of its vehicle onto the
surface tissues of the skin. There are three potential portals of entry: through the follicular
region, through the sweat ducts, or through the unbroken stratum corneum between these
appendages. There is little convincing evidence that eccrine sweat glands play any
significant role in cutaneous permeability. Material may enter the ducts, and even the
glands, but there appears to be no penetration from these areas to the dermis.
For substances absorbed by the transepidermal route, penetration is fairly rapid, although
slower than intestinal tract absorption, and is almost always accompanied by some degree
of pilosebeceous penetration as well. For substances that are absorbed through both
pathways, the transepidermal route is the principal portal of entry because of the total,
relatively small, absorbing surface offered by the pilosebeceous units. The epidermis
presents a surface area 100 to 1000 times greater than the other routes of absorption. The
appendages, sweat glands, and hair follicles are scattered throughout the skin in varying

1. INTRODUCTION 32
numbers, but are comparatively sparse; their total cross-sectional area is probably
between 0.1 and 1.0% of the skin area.
Once a substance passes through the stratum corneum, there is apparently no significant
further hindrance to penetration of the remaining epidermal layers and corneum; there is
a ready entry into the circulation via the capillaries. The concentration gradient
essentially ends in the dermal layer at the beginning of the circulation. The systemic
circulation acts as a reservoir or “sinks” for the drug. Once in the general circulation, the
drug is diluted and distributed rapidly with little systemic buildup.(Fig.1.2 )
Diffusion through the horny layer is a passive process. There is little evidence to support
specialized active transport systems for cells of the stratum corneum. The passive process
is affected only by the substance being absorbed, by the medium in which the substance
is dispersed, and by ambient conditions. On the other hand, percutaneous absorption is a
more complicated process, of which epidermal diffusion is the first phase, and clearance
from the dermis the second. The latter depends on effective blood flow, interstitial fluid
movement, lymphatics, and perhaps other factors that combine with dermal
constituents.59
1.3.5 Physical chemistry of percutaneous absorption
There has been little evidence to suggest that there are any active processes involved in
skin permeation therefore the underlining transport process is controlled by simple
passive diffusion. Fick’s laws of diffusion can be used to analyze permeation data and
can be used predicatively. Fick’s first law is used to describe steady state diffusion and
can be define as:-
J = DKΔC / h …….. (1)
Where J is the flux per unit area, D is the diffusion coefficient in the skin, K is the skin
vehicle partition coefficient, ΔC is the concentration difference across the skin, and h is
the diffusional path length.
Under normal circumstances the applied concentration (CAPP) is very much larger than
the concentration under the skin and equation 1 is often simplified to:
J = Kp* CAPP ………. (2)

1. INTRODUCTION 33
Where Kp is a permeability coefficient (= KD/h) and is a heterogeneous rate constant
having the units cm/h. As will become apparent, it is often difficult to separate K and D
and their calculated magnitude will depend on ‘h’ that cannot be accurately estimated as
it is the tortuosity of the intracellular channels, which is imprecise58
.
1.3.6 Drug absorption
Percutaneous absorption of drugs from topical formulations involves the release of the
drug from the formulation and permeation through skin to reach the target tissue. The
release of the drug from topical preparation depends on the physicochemical properties of
the vehicle and the drug employed. In order to enhance drug release and skin permeation,
methods such as the selection of a suitable vehicle, co-administration of a chemical
enhancer, and iontophoresis have been studied 55
.
There are many traditional valuable dermatological systems available which apply
topically, for example- semisolid preparation (e.g. cream, ointment), and liquid
preparations, etc. which have a considerable problem in the delivery of medicament
through the skin, is impermeability, low bioavailability, and only few percentage of the
active material reaches to the target site.
This can be improved by developing novel dermatological formulation which is much
more efficient and effective than traditional topical system. Nowadays different carrier
systems has been extensively investigated for the topical delivery of drugs, such as
liposomes, niosomes, transfersomes, ethosomes, solid lipid nanoparticles and
microemulsion etc.
1.3.7 Physicochemical criteria for topical formulation
Stability of the active ingredients
Stability of the adjuvant
Rheological properties- consistency, extrudability
Loss of water and other volatile components
Phase changes- homogeneity, phase separation
Particle size and particles size distribution
Apparent pH
Particulate contamination.59
1.3.8 Ideal properties of topical formulation

1. INTRODUCTION 34
Achieves a concentration in the target tissue that is sufficient to produce desired
pharmacological response
Preferably non toxic
Leaves the skin in an inactive form (as a metabolite)60
1.3.9 Vesicular approaches for topical delivery system59
Various vesicular systems are used to increase drug transport across the skin. They are as
follows:
1.3.10 Formulation approaches
Penetration enhancement with special formulation approaches is mainly based on the
usage of colloidal carriers. Submicron sized particles are intended to transport entrapped
active molecules into the skin. Such carriers include liposomes, nanoemulsions, and
solid-lipid nanoparticles (Fig.1.3). Most reports cite a localizing effect whereby the
carriers accumulate in stratum corneum or other upper skin layers. Generally, these
colloidal carriers are not expected to penetrate into viable skin. However, the
effectiveness of these carriers is still under debate. 60-61
Figure 1.3: Vesicular approaches for topical delivery system
Liposomes
Liposomes are made up of amphiphlic molecules (phospholipids and mixture of lipids
containing phospholipids) capable of self-organization properties. These molecules are
able to form a lipidic bilayer and this bilayer encapsulates a small internal aqueous
volume. Hydrophilic molecules can be encapsulated in the internal aqueous volume
where as amphiphlic molecules can be incorporated in the bilayer. Liposomes are formed

1. INTRODUCTION 35
when thin lipid films or lipid cake are hydrated and stacks of liquid crystalline bilayers
become fluid and swell. The hydrated lipid sheets detach during agitation and self-close
to form large multilamellar vesicles (LMV) which prevents interaction of water with the
hydrocarbon core of the bilayer at the edges, once these particles have formed, reducing
the size of the particle requires energy input in the form of sonic energy (Sonication) or
mechanical energy (extrusion). Properties of lipid formulations can vary depending on
the composition (cationic, anionic, neutral lipid species).
Niosomes
Niosomes are non-ionic surfactant based multilamellar or unilamellar vesicles in which
an aqueous solution of solute is entirely enclosed by a membrane resulted from the
organization of surfactant macromolecules as bilayer.
Pharmacosomes
Pharmacosomes are colloidal dispersions of drugs covalently bound to lipids and may
exist as ultra fine vesicular, micellar or hexagonal aggregate depending on the chemical
structure of the drug-lipid complex. The development of vesicular pharmacosomes is
based on surface and bulk interactions of lipids with water. Any drug possessing an
active hydrogen atom (-COOH,-OH,-NH2, etc) can be esterified to the lipid with or
without spacer chain, the limitation of liposomes and niosomes can be overcome by
pharmacosome approach.
Ethosomes
Ethosomal system is a vesicular system composed mainly of phospholipids, alcohol
(ethanol and isopropyl alcohol) in relatively high concentration, sometime glycols
(polyols) and water. Ethosomes contain high concentration of ethanol that is responsible
for their better skin permeation ability. Ethosomal system is vesicular in nature,
depending on the ratio of components and the chemical structure of the phospholipids can
be comprised of very small entities (nm).
Hydrogels in topical delivery
Hydrogels are three dimensional, water-swollen structure composed of mainly
hydrophilic homopolymers or copolymers. They are rendered insoluble due to cross-
linking by chemical bonds, or other cohesion forces such as ionic interaction, hydrogen
bonding, or hydrophobic interaction. Hydrogels are elastic solids because they exist in a

1. INTRODUCTION 36
reference configuration to which the system returns even after being deformed for a very
long time.
Transfersome
A transfersome is an artificial vesicle designed to be like a cell vesicle, and used to
deliver drugs or genetic material into a cell. A basic transfersome is composed of one
natural amphipath (such as phosphatidylcholine) that tends to self-aggregate into vesicles.
The latter are then supplemented by at least one bilayer softener (e.g. a biocompatible
surfactant). The vesicle-like Transfersome thus normally possesses an aqueous core
surrounded by a complex, very fluid and adaptable lipid bilayer. In its basic organization
is broadly similar to a simple lipid vesicle (a so-called liposome), a Transfersome differs
from the latter by its more flexible and permeable, "softened" bilayer membrane.
Out of this mentioned delivery system, the present work emphasize on potentiality of
ethosomes as smart drug delivery system for treatment of inflammation. Smart Delivery
Systems that are now a day’s famous for topical application are summarized in
(Table1.1).
1.3.11 Ethosomes
In the early 1980s, Mezei and his group described liposomes as the first topical lipid
vesicular system for enhanced drug delivery to the skin. Since then, many works have
shown that lipid vesicular systems are able to increase the accumulation of various
molecules in the SC or other upper skin layers. Drug delivery from such vesicles results
in the formation of a drug reservoir in the horny layer of the skin and is generally
characterized by a lack of penetration into the deeper layers of the skin. This behavior is
useful both for local treatment of skin disorders and for cosmetic formulations. Specific
drug accumulation at the site of action and decreased systemic drug absorption can
impart increased efficiency as well as decreased side effects for a compound applied
topically. Early works by Mezei and coworkers reported that application of triamcinolone
acetonide encapsulated within liposomes to depilated rabbit skin in vivo resulted in a
fourfold increase in the amount of drug accumulated in the epidermis, as compared to
application of the same drug concentration in an ointment base. More recently, Touitou’s
group studied the delivery of dyphylline incorporated in unilamellar liposomes from
polyethylene glycol (PEG),carbopol gel, a PEG enhancer base and water. Conversely,

1. INTRODUCTION 37
when caffeine delivered from small unilamellar liposomes, was found mostly localized
into the skin. By using quantitative autoradiography, it was also found that the
concentration of the drug was greatest in the epidermis, lowest in the dermis, and
relatively high in the appendages. As discussed above, conventional liposomal systems
were demonstrated to be effective at delivering active agents to the upper layers of the
skin. More recently, novel lipid vesicular systems that are capable of penetrating to the
deep layers of the skin and delivering the active agents transdermally have been invented
by Prof. Elka Touitou from the Faculty of Medicine, Hebrew University in Jerusalem,
Israel in1996 as additional novel lipid carriers composed of ethanol, phospholipid, and
water termed as Ethosomes.63
Table 1.1: Smart delivery system
Ethosomes are soft, malleable, tiny bubble like lipid vesicles composed mainly of
phospholipids, ethanol (relatively high concentration) and water. These “soft vesicles”
S.No Systems Example Delivers
1. Emulsions Microemulsions, liquid crystals,
multipleemulsion, nanoemulsions,
pickering emulsions
Carotenoids, vitaminA
palmitate, free radical
scavengers, nitrocellulose
and antimicrobials.
2. Particulate
delivery
systems
Microparticulates,porous polymeric
systems, nanoparticulates,
cyclodextrin, melanosponge
Vegetable oil, tocopherols,
retinal, tocopherols,
genetically engineered
melanin.
3. Vesicle
delivery
systems
Ethosomes, liposomes, photosomes,
niosomes siliconevesicles,matrices,
multi-walled-delivery systems,
phytosome, marinosomes
ultrasomes, asymmetric-oxygen
carrier system (AOCS) liposomes
Photo-reactivating enzyme
extracted from a marine
plant, Anacystis nidulans
catechin, quercetin,
glycyrrhetinicacid,
endonuclease enzyme.
4. Other
delivery
systems
Iontophoresis, cosmetic patches. Vitamin C, E.

1. INTRODUCTION 38
represents smart vesicular carrier for enhanced delivery to/through skin. All components
of the Ethosomal systems are considered as being safe for pharmaceutical and cosmetic
use. Ethosomal systems were found to be significantly superior at delivering drugs
through the skin in terms of both quantity and depth when compared to liposomes and to
many commercial transdermal and dermal delivery systems. Ethosomes are sophisticated
vesicular delivery carriers that are capable of delivering various chemical applications.
Visualization by dynamic light scattering showed that Ethosomes could be unilamellar or
multilamellar through to the core. These novel delivery systems contain soft phospholipid
vesicles in the presence of high concentrations of ethanol. Ethosomal systems are
sophisticated conceptually, but characterized by simplicity in their preparation, safety and
efficiency - a rare combination that can expand their applications. 63-64
Mechanism of ethosomes
The enhanced delivery of actives using ethosomes over liposomes can be ascribed to an
interaction between ethosomes and skin. It is thought that the first part of the mechanism
is due to the’ ethanol effect’, whereby intercalation of the ethanol into intercellular lipids
increasing lipid fluidity and decreases the density of the lipid multilayer. This is followed
by the ‘ethosomes effect’, which includes inter lipid penetration and permeation by the
opening of new pathways due to the malleability and fusion of ethosomes with skin
lipids, resulting in the release of the drug in deep layers of the skin, shown in
Fig.1.4&1.5.65
Composition
The ethosomes are vesicular carrier comprise of hydroalcoholic or
hydro/alcoholic/glycolic phospholipid in which the concentration of alcohols or their
combination is relatively high. Typically, ethosomes may contain phospholipids with
various chemical structures like phosphatidylcholine (PC), hydrogenated PC,
phosphatidic acid (PA), phosphatidylserine (PS), phosphatidylethanolamine (PE),
phosphatidylglycerol (PPG), phosphatidylinositol (PI), hydrogenated PC, alcohol
(ethanol or isopropyl alcohol), water and propylene glycol (or other glycols). Such a
composition enables delivery of high concentration of active ingredients through skin.
Drug delivery can be modulated by altering alcohol: water or alcohol-polyol: water ratio.

1. INTRODUCTION 39
Figure 1.4: Drug penetration through Ethosomes
Figure 1.5: Mechanism of action of Ethosomes

1. INTRODUCTION 40
Some preferred phospholipids are soya phospholipids such as Phospholipon 90 (PL-90).
It is usually employed in a range of 0.5-10% w/w. The concentration of alcohol in the
final product may range from 20 to 50%. The concentration of the non-aqueous phase
(alcohol and glycol combination) may range 22 to 70 % .
66-67
Properties
The size of Ethosomes vesicles can be modulated from tens of nanometers to microns.
Delivery can be targeted for local delivery or for systemic use.
Ethosome allows it to carry a wide variety of molecules with various physico-chemical
properties hydrophobic, hydrophilic and amphiphilic.
Reduced doses and toxicity.
High patient compliance.
Enhancement of a product's life cycle.
Significant superiority compared to other drug delivery system.
Science behind ethosome formation
Closed lipid vesicles can be prepared from lipid multi-lamellae by strong pertrubation
that is by mechanical or chemical energy, introduced by pressure, homogenisation,
agitation, osmotic shock, with increasing lipid bilayer elasticity the energy required for
vesiculation decreases. Lipid in solvent (eg water) that contains a co-solvent (eg ethanol)
typically have rather complex (lyotropic phase diagram).The generalized phase diagram
of such system exhibits normal and inverse micellar or cubic or hexagonal phases,
seperated by central phase region in which lamellar or or vesicular phase prevail. All
such phases are sensetive to isothermal composition changes but only latter kind of
agregates-structure is practically meaningful for the colloidal mediated transdermal drug
delivery. 68
Parameters effecting bilayer formation
Large free energy difference between the aqueous and hydrophobic environment
promotes the bilayer structure in order to achieve lowest free energy level.
Driving force for bilayer configuration is the hydrophobic interaction coupled with the
amphiphilic nature of the phospholipid molecule.
Supermolecular self-assemblages mediated through specific molecular geometry.

1. INTRODUCTION 41
Ternary phase diagram
A ternary phase diagram of phosphotidylcholine, ethanol, and water reveals a complex.
In pure ethanolic solution an isotropic micellar phase is found. Addition of little water
prompts micellar elongation and crowding. Solvent content between lipid lamellae is
higher in presence of ethanol, notwithstanding the fact that alcohol replaces some water
in vicinity of phospholipid head group. The reason are the lateral and transverse
expansion of lipid bilayers caused by greater mobility of polar lipid heads, whole lipid
molecule, and bilayer segments in a hydro- alcoholic solvent mixture..This states that
ethanol increases lipid bilayer fluidity and flexibility. 68
Figure 1.6: Ternary phase diagram; L: fluid lamellar phase; I: isotropic (micellar) phase
Advantages of ethosomes
Advantages of ethosomal delivery system in comparison to other novel transdermal &
dermal delivery systems .65-73
As compared to liposomes, ethosomes are easy to prepare, store, high entrapment,
deeper permeability and enhanced delivery of active constituents
Various application in Pharmaceutical, Veterinary, Cosmetic field reported and further
developments are going on.
Ethosomes composition is safe and the components are approved for pharmaceutical and
cosmetic use.
Vesicles without use of additional surfactants to which many consumers are allergic. As
compared to others which requires lot of inputs.
Water
Ethanol SoyPC
L
I+L
L
LL
LL
LL
LL
LL
LL
LL
0.0
1 0.0
1
1.0 0.0

1. INTRODUCTION 42
Low risk profile- The technology has no large-scale drug development risk since the
toxicological profiles of the ethosomal components are well documented in the
scientific literature.
The ethosomes administered in semisolid form (gel or cream), producing high patient
compliance is high. In contrast, Iontophoresis and Phonophoresis are relatively
complicated to use that affect patient compliance.
High market attractiveness for products with proprietary technology. Relatively simple
to manufacture with no complicated technical investments required for production
of Ethosomes. Hence easy to scale up.
The ethosomal system is passive, non-invasive and is available for immediate
commercialization.
Ethosomes enhances permea tion of active constituents through skin
for transdermal and dermal delivery.
Comparative studies of existing dermal and transdermal drug delivery systems with the
Ethosome technology proved a significant superiority for ethosome over the other
technologies in terms of efficiency and lack of irritancy.
Ethosomes are platform for the delivery of large and diverse group
of drugs (peptides, protein molecules), active herbal constituents.
Ethosomes have been reported to deliver many synthetic drug for example Salbutamol
Sulfates,66
Minoxidil,75
Cannabidol,76
Acyclovir,77
AntiHIVAgents,78
zidovudine,Lamivudin
e,Trihexiphenidyl.hydrochloride79
,Insulin80
,Azelaic.acid81
,Erythromycin,82
Bacitracin,83
D
NA,84
Diclofenac,85
peptides86
. All mentioned drugs delivered through ethosomes posses
improved dermal deposition, improved intracellular delivery, bioavailability and reduced
possible side effects.
1.3.12 Topical Gel
Topical drug administration is a localized drug delivery system anywhere in the body
through ophthalmic, rectal, vaginal and skin as topical routes. Skin is one of the most
readily accessible organs on human body for topical administration and is main route of
topical drug delivery system. The skin of an average adult body covers a surface area
approximately 2m2
and receives about one third of the blood circulating through the
body. An average human skin surface is known to contain, on the average 40-70 hair

1. INTRODUCTION 43
follicles and 200-300 sweat ducts on every square centimeter of the skin. Although skin
has been divided histologically into the stratum corneum, the living epidermis and the
dermis, collectively it can be considered a laminate of barrier, permeation of this laminate
can occur by diffusion via:
Transcellular penetration (across the cells)
Intracellular penetration (between the cells)
Transappendageal penetration (via hair follicles, sweat and sebum glands).
A myriad of medicated product are applied to the skin or readily accessible mucous
membrane that in some way either augment or restore a fundamental function of a skin or
pharmacologically modulate an action in the underlined tissues. Such products are
referred as topical or dermatological product.87
Rational Approach to Topical Formulations
Topical formulation can be used to manipulate the barrier function of the skin, for
example, topical antibiotics and antibacterials help a damaged barrier to ward off
infection, sun screening agents and the horny layer protect the viable tissues from U.V.
radiation and emollient preparations restore pliability to a desiccated horny layer. For
skin appendage treatment, for example, antiperspirants, exfolients and depilatories are to
be delivered to the skin appendages. Delivery of drugs for systematic treatment, for
example, transdermal therapeutic systems provide systemic therapy for motion sickness,
angina and hypertension. Gels are becoming more popular due to ease of application and
better percutaneous absorption. The term “Gel” was introduced in the late 1800 to name
some semisolid material according to pharmacological, rather then molecular criteria.88-90
The U.S.P. defines gels as a semisolid system consisting of dispersion made up of either
small inorganic particle or large organic molecule enclosing and interpenetrated by
liquid. The inorganic particles form a three-dimensional “house of cards” structure. Gels
consist of two-phase system in which inorganic particles are not dissolved but merely
dispersed throughout the continuous phase and large organic particles are dissolved in the
continuous phase, randomly coiled in the flexible chains.
Classification
Gels are classified mainly by two methods based on:
a) Nature of colloid phase

1. INTRODUCTION 44
Inorganic gels
Organic gels
b) Based on nature of solvent
Aqueous gels
Non aqueous gels
Gel forming substances
Polymers are used to give the structural network, which is essential for the preparation of
gels. Gel forming polymers are classified as follows:
Natural polymer
Proteins: Collagen, Gelatin
Polysaccharides: Agar, Alginate acid, Sodium or Potassium carageenan, Tragacanth,
Pectin, Guar Gum, Cassia tora, Xanthan, Gellum Gum
Semisynthetic polymers
Cellulose derivatives: Carboxymethyl cellulose, Methylcellulose, Hydroxypropyl
cellulose, Hydroxy propyl (methyl cellulose), Hydroxyethyl cellulose.
Synthetic polymers
Carbomer: Carbopol 940, Carbopol 934
Poloxamer
Polyacrylamide
Polyvinyl alcohol
Polyethylene and its co-polymers
Inorganic substances
Aluminium hydroxide
Besitonite
Surfactants
Cebrotearyl alcohol
Brij – 96
Advantages
The topical administration of drug in order to achieve optimal cutaneous and
percutaneous drug delivery has recently gain an importance because of various
advantages:
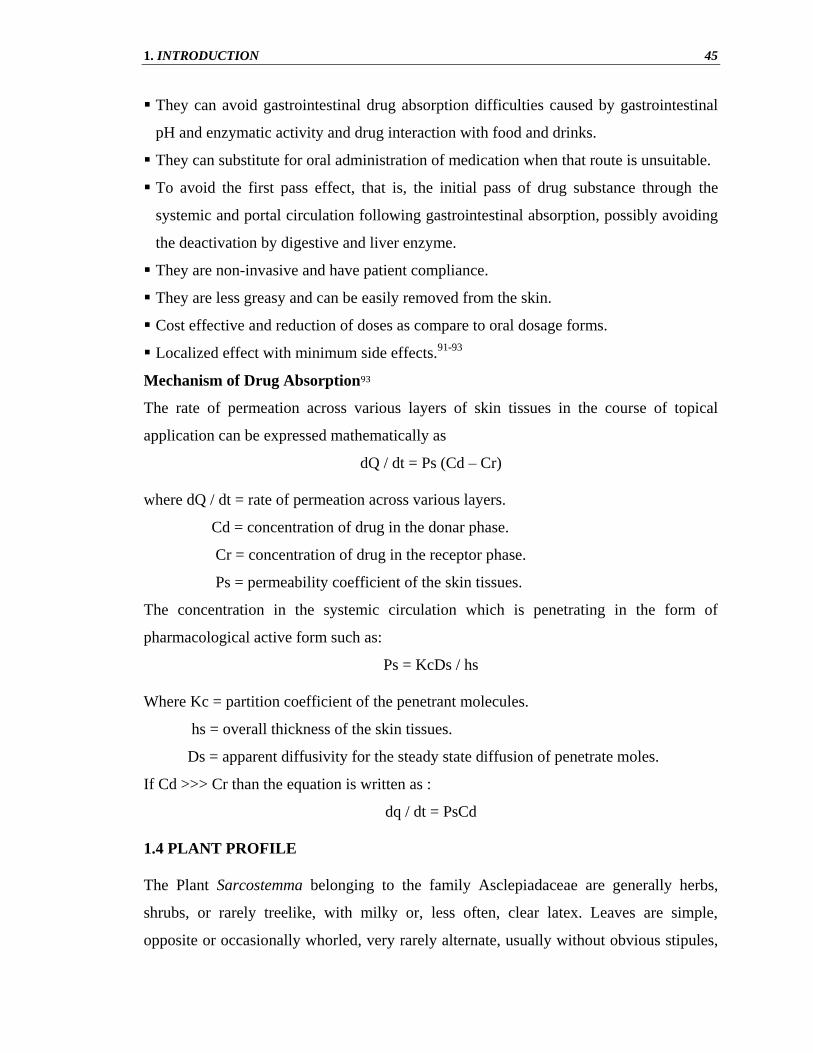
1. INTRODUCTION 45
They can avoid gastrointestinal drug absorption difficulties caused by gastrointestinal
pH and enzymatic activity and drug interaction with food and drinks.
They can substitute for oral administration of medication when that route is unsuitable.
To avoid the first pass effect, that is, the initial pass of drug substance through the
systemic and portal circulation following gastrointestinal absorption, possibly avoiding
the deactivation by digestive and liver enzyme.
They are non-invasive and have patient compliance.
They are less greasy and can be easily removed from the skin.
Cost effective and reduction of doses as compare to oral dosage forms.
Localized effect with minimum side effects.91-93
Mechanism of Drug Absorption93
The rate of permeation across various layers of skin tissues in the course of topical
application can be expressed mathematically as
dQ / dt = Ps (Cd – Cr)
where dQ / dt = rate of permeation across various layers.
Cd = concentration of drug in the donar phase.
Cr = concentration of drug in the receptor phase.
Ps = permeability coefficient of the skin tissues.
The concentration in the systemic circulation which is penetrating in the form of
pharmacological active form such as:
Ps = KcDs / hs
Where Kc = partition coefficient of the penetrant molecules.
hs = overall thickness of the skin tissues.
Ds = apparent diffusivity for the steady state diffusion of penetrate moles.
If Cd >>> Cr than the equation is written as :
dq / dt = PsCd
1.4 PLANT PROFILE
The Plant Sarcostemma belonging to the family Asclepiadaceae are generally herbs,
shrubs, or rarely treelike, with milky or, less often, clear latex. Leaves are simple,
opposite or occasionally whorled, very rarely alternate, usually without obvious stipules,

1. INTRODUCTION 46
margin nearly always entire. Inflorescences terminal, axillary, or extra-axillary, cymose,
often condensed and umbel-like, occasionally a racemelike bostrychium. Flowers are
bisexual, 5-merous, actinomorphic. Sepals joined at base only, often with 5 or more basal
glands in the sinuses. Corolla sympetalous, reflexed to urceolate or salverform; lobes
valvate or overlapping in bud to right or left. Corona usually present, inserted on corolla,
stamens, or both. Stamens five, usually inserted at base of corolla tube and adhering to
stigma head to form gynostegium; filaments usually connate to form a tube enclosing
ovaries; anthers 4-celled (Periplocoideae and Secamonoideae) or 2-celled
(Asclepiadoideae), often with a membranous apical appendage; pollen tetrads contained
loosely on a spatulate translator with a basal corpusculum (Periplocoideae), or pollen
united into waxy pollinia, each attached through a caudicle (stalk) to the retinaculum
(gland) between adjacent anthers to form a pollinarium, pollinia 2 (Asclepiadoideae) or 4
(Secamonoideae) per pollinarium. Ovaries two, free, superior; ovules numerous. Styles
connate; stigma head fleshy. Fruit of one or two follicles. Seeds numerous, strongly
compressed, with a coma (a prominent basal tuft of silky hairs). Chromosome number x =
(8–)11 (or 12). Some 250 genera and over 2000 species: widespread in tropical and
subtropical regions, especially in Africa and southern South America, with a moderate
representation in northern and southeastern Asia; 44 genera (four endemic) and 270
species (153 endemic) in China.
Some authorities include this family in the Apocynaceae. Genera 1–6 are sometimes
placed in a separate family, the Periplocaceae, here regarded as a subfamily,
Periplocoideae. Genera 7–10 belong to the Secamonoideae and the remaining genera to
the Asclepiadoideae. Many Chinese taxa are known only from dried material, sometimes
not well preserved, and it is likely that the study of living or spirit-preserved material
could lead to a reassessment of the taxonomy of some of these endemic taxa.
All plant parts, especially the seeds and latex, are often poisonous. They contain various
alkaloids and glycosides, many of which are used in medicine and as insecticides. A few
succulent species (e.g., Stapelia gigantia N. E. Brown, Orbea pulchella (Masson) L. C.
Leach, and O. variegata (Linnaeus) Haworth are grown by specialist collectors in
China.94

1. INTRODUCTION 47
1.4.1 Sarcostemma
Sarcostemma is a genus of at least 35 species of plants in family Asclepiadaceae. These
are known generally as climbing milkweeds or caustic bushes. They are found across
Africa and tropical Asia, in Australia, and in parts of North America. These plants are
perennial flowering shrubs with trailing vines or lianas. They are often adapted to heat
and/or desert conditions. Leaves reduced to scales, short lived so plant is often leafless
and photosynthesize in the tissues of the green stems. The soft stems are filled with milky
white latex that is poisonous and caustic in some species. The flowers have a ring of thick
tissue at the base which extends into hollow spherical appendages within the flower
corolla.
Taxonomy of this group is controversial. Sarcostemma are widely distributed throughout
the sub-tropical and tropical old World in Africa, India and Malaysia. Several species in
this group are listed as invasive weeds and best cultivated in pots with a climbing frame,
where they can be kept under control. The milky sap is toxic and Sarcostemma australe
(Caustic Vine) blisters skin on contact. Some species may contain substance of medicinal
value.95
1.4.2 Species of the Sacrastemma include:
Sarcostemma acidum
Sarcostemma angustissima
Sarcostemma australe - caustic vine
Sarcostemma brevipedicellatum
Sarcostemma cynanchoides
Sarcostemma clausum - white twine vine
Sarcostemma decorsei
Sarcostemma esculentum
Sarcostemma hirtellum - hairy milkweed
Sarcostemma membranaceum
Sarcostemma mulanjense
Sarcostemma socotranum
Sarcostemma viminale Rapunzel plant.

1. INTRODUCTION 48
Funastrum (Sarcostemma) cynanchoides (Climbing Milkweed): Widely-distributed
across the Southern USA from Florida to California, commonly twining through shrubs,
fences and other supports. The greenish-white to pink petals are fringed with white hairs
but the stems and lanceolate to heart-shaped leaves are smooth. Flowers are followed by
pairs of pods full of seeds with silken parachutes. This plant is attractive to bees,
butterflies and birds but may be an invasive weed in some areas. .
Funastrum (Sarcostemma) hirtellum Schlechter 1914 (Hairy Milkweed): A widespread
vining plant of the lower desert in South-Western USA and North-Western Mexico. The
white petals are fringed with white hairs and the twining stems and sparse lanceolate
leaves are pubescent. May be an invasive weed, swamping other vegetation.
Sarcostemma vanlessenii Lavranos 1974: : This species from Kenya and N. Tanzania
has narrow stems up to an eighth of an inch in diameter. In a sunny location, clusters of
small pinkish to brownish flowers are produced freely during the summer.
Sarcostemma viminale R. Brown 1810: A robust species distributed acrosss Tropical and
Southern Africa. The leafless, photosynthetic stems up to a quarter of an inch in diameter
tend to explore and scramble through their surroundings, rooting as they go, but can be
confined to the footprint of a plant pot with a climbing frame and some creative basket
weaving. The cream-coloured flowers are sweetly scented. May be an invasive weed.
Sarcostemma brevistigma: A leafless East Indian vine plant with a weak stem that
derives support from climbing, twining, or creeping along a surface; its sour milky juice
formerly used to make an intoxicating drink. The herb is highly used by the rural and
tribal people in curing various disorders (fig.1.7).96

1. INTRODUCTION 49
Sarcostemma cynanchoides Sarcostemma hirtellum
Sarcostemma vanlessenii Sarcostemma viminale
Sarcostemma acidum Sarcostemma acidum
Figure 1.7: Species of the Sacrastemma

1. INTRODUCTION 50
1.4.3 Sarcostemma brevistigma Wight & Arnott
Asclepias acida Roxburgh, Fl. Ind. ed. 1832, 2: 31. 1832;
Sarcostemma acidum (Roxburgh) Voigt, Hort. Suburb. Calcutt. 542. 1845,. belonging to
family Asclepiadaceae. Stem 2-5 mm diameter, glabrous, joints 10-20 cm long.,leaves
reduced to scales, shor lived so plant is often leafless, Leafless trailing or twining jointed
shrubs with pendulous branches.,Flowers in sessile many flowered terminal umbels;
pedicles 6-8 mm long, slender, pubescent, bracts minute, lanceolate.,Calyx divided to the
base or nearly so, with glands inside, segments 1.25 mm long, ovate-oblong, subacute,
with membranous margins.,Corolla campanulate, pale greenish white, divided nearly to
the base, lobes 5 mm long, ovate oblong, subacute, outer corona crenately 10-lobed on
the margin, lobes of the inner corona thick, fleshy, obtuse, longer than the staminl column
almost concealing the anther. Stamina column very short, pollen-masses waxy,
compressed, clavate, slightly curved, attached by a very short caudicle to the pollen
carriers. Style-apex very shortly conical or blunt. Follicles 10-12.5 by 0.8 cm, lanceolate,
tapering to both ends, straight, slightly diverging when two together. Seeds 5 by 3 mm,
ovate, flattened, coma 2 cm long.
S. brevistigma leafless East Indian vine plant with a weak stem that derives support from
climbing, twining, or creeping along a surface; its sour milky juice formerly used to make
an intoxicating drink.The herb is highly used by the rural and tribal people in curing
various disorders.
On the basis of well designed open ended questions tool a study performed in central
region of Madhya Pradesh, India and enumerates various traditional and ethnomedicinal
utility of the plant. It has been concluded that somlata herb(comman name) was used in
various diseases such as asthma, swelling, fever and cold, dyspepsia, inflammation
infection and gastric problem etc.
Common Name: Somavalli, haoma, soma.
Synonyms :
Bengal : Soma, Somlata
Bombay : Lama, Soma
Canarese : Brahmi, Hambukalli, Somaballi, Somalate, vasukanti
English : Moon Creeper, moon plant, Sour Creeper

1. INTRODUCTION 51
Gujerati : Somvel
Hindi : Somlata
Koya : Kadujemudu
Malayalam : Somam, somavallari, Somavalli, Vayastha
Marathi : Ransher, Ransheryel, Somyel
Mundari : Kulatoa
Porebunder : Chirodi Sandhiavelm,Thoravel
Sanskrit : Chandravallari, Dhanurlata, Dvijapriya, gulmavalli, Indulekha, Mahagulma,
Padmakashtha, Soma, Somakshiri, Somalata, Somhara, Somavalli, Somavallika,
Yajnaga, Yajnashreshtha, Yajnavalli
Sind : Thorinjal
Sinhalese : Muwakiriya
Tamil : Kodikkalli, Somam
Telugu :Kondapala, Padmakashtamu, Pullajemudu, Pollatige, Somlata,
Tigejemudu, Pullangi tiga
Uriya : Borohwi, Notasiju, Somolota
Geographical source : Some 250 genera and over 2000 species: of Asclepiadaceae
widespread in tropical and subtropical regions, especially in Africa and southern South
America, with a moderate representation in northern and southeastern Asia; 44 genera
(four endemic) and 270 species (153 endemic) in China.
S. bevistigma distributed in various parts of India it is found in dry rocky places in Bihar,
Bengal, Konkan, Deccan, Tamil Nadu, Maharashtra, Kerala, Chota Nagpur, Burma, N.
Circars, and Carnatic.97,98
Sarcostemma acidum as an Indian Soma :
Vedic literature supports that Soma was a sacred plant, the juice of which (Soma-Rasa)
was considered as the divine drink offered to Gods, contemplated with medicinal
efficacy, used as natural restorative for health that makes the consumer awakened and
alert. As a matter of fact, the Rig Veda describes how the marvelous drink was prepared:
the dried Soma plants were moistened with water to make them swell up again and
pounded with pestles. After being filtered through a fine woollen cloth, the tawny yellow
inebriating juice was imbibed by the Vedic priests in their sacrificial rites. The effects, as

1. INTRODUCTION 52
these emerge from the poetic imagery of the hymns, were clearly what we would now
call hallucinogenic or psychedelic.
Soma is known to most readers as the stimulant, euphoriant and hallucinogen in Aldous
Huxley's novel Brave New World. Few people know that the plant soma actually exists
and has been used as a narcotic since the time of India's earliest civilizations. In Ancient
Indian mythology Soma, the brother of Indra, was the giver of health, courage, long life,
a sense of immortality, and almost every other virtue known. As a narcotic, soma is
thought to have originated in the Hindu Kush mountain range of northeast Afghanistan.
Nor is there evidence that Sarcostemma has psychoactive properties, particularly of the
kind implied in such Vedic hymns as one that speaks of the priestly imbiber of the divine
Soma having the power of flight beyond the limits of heaven and earth and feeling strong
enough to pick up the earth itself and move it about wherever he desired. An modern
Hindu tantric practices in the southern state of Kerala, however, Soma is a different
quantity. It is described in the book “Agni by Frits Stall” that the botanical name of Soma
is `Sarcostemma brevistigma`. It is a creeper(vine) that is commonly found in the
Western Ghats of South India. The stem is used to make the Somarasa for many yagas in
Kerala. The King of Kollengode, an erstwhile principality in Kerala, is obliged to supply
the soma stems for yagas.
Sarcostemma brevistigma is used in India today under the name soma, as are several
other plants including Ephedra species. It may be that all of these are surrogates, or it is
quite possible that Sarcostemma bievistigma is the plant soma of antiquity. A thorough
chemical analysis of the latter to establish the presence of an intoxicating narcotic is in
order. It is known that the dried stem is an emetic in Indian medicine, but knowledge
about fresh milky latex is required Certainly the herb is worthy of more investigation than
has been conducted to date. In a volume entitled Medicinal, Economic, and Useful Plants
of India by Sudhir Kumar Das, the foreword notes that the "therapeutic uses of plant
materials have been quoted from records of the findings made through the ages by Hindu
Ayurvedic Pharmacists." In this compendium of ancient sources, Sarcostemma
brevistigma is listed with the following note: "Herb. Plant juice is intoxicating and blood
purifying." Such evidence is only circumstantial, but most intriguing.99

1. INTRODUCTION 53
1.4.4 Active Constituents
Phytochemical Studies have revealed the presence of Bergenin, Brevine, Brevinine,
Sarcogenin, Sarcobiose and Flavonids (Obeai et al 1985). The aerial Parts of
Sarcostemma acidum has shown various Pregnane glycoside which are diglycosides and
triglycosides. Some important pregnane glycosides are:- Sarcogenin (triglycoside),
Brevobiose (disaccharide), Sarcobiose (nonreducing disaccharide), Tigmobiose (non
reducing disaccharide), Brevine (triglycoside), Brevinine (Pregnane ester diglycoside)
Brevine: Brevine is a pregnane ester triglycoside isolated from the dried twigs of
Sarcostemma brevistigma. Its chemical and spectroscopic properties were consistent with
the structure 11-O-benzoyl-sarcogenin-3-O-α-L-diginopyranosyl (1 → 4)-O-α-L-
diginopyranosyl(1 → 4)-O-α-L-diginopyranoside.
Sarcobiose: It is a nonreducing disaccharide, isolated from dried twig of Sarcostemma
acidum. Its structure has been established as 3,4-anhydro-2,6-dideoxy-β-D-lyxo-
hexopyranosyl 6-deoxy-3-O-methyl-β-D-allo-pyranoside.
Figure 1.8: Chemical structure of Brevine Figure 1.9: Chemical structure Sarcobiose
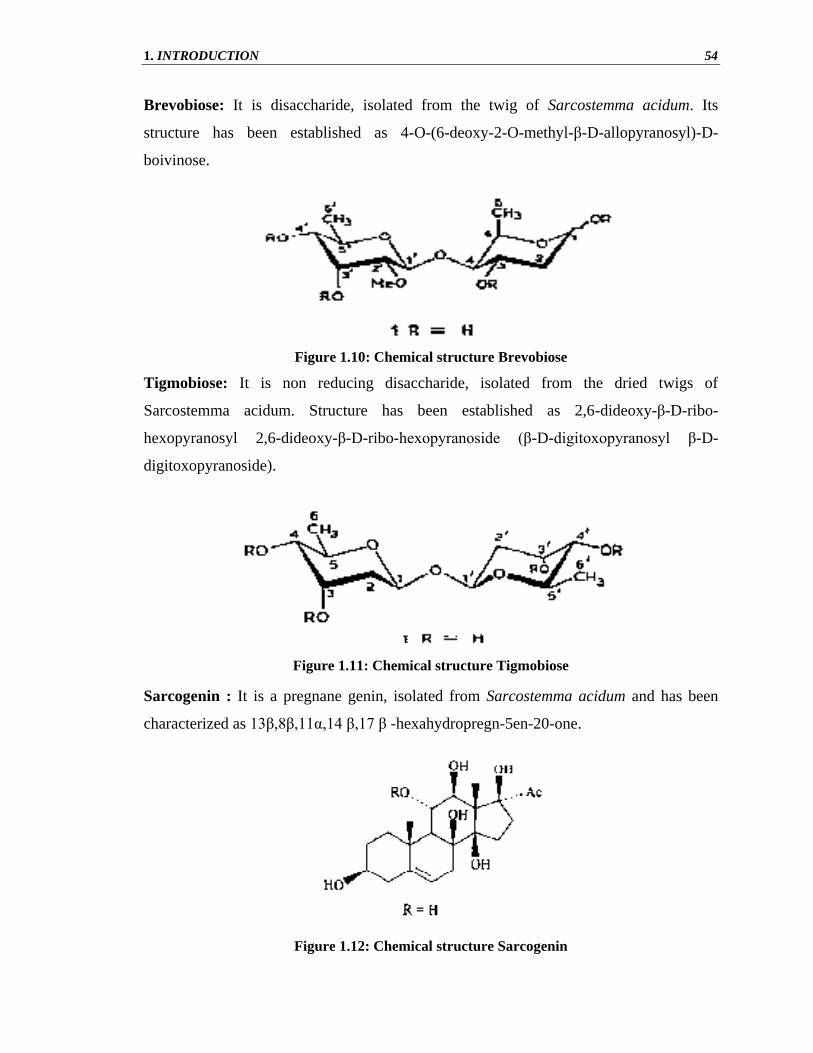
1. INTRODUCTION 54
Brevobiose: It is disaccharide, isolated from the twig of Sarcostemma acidum. Its
structure has been established as 4-O-(6-deoxy-2-O-methyl-β-D-allopyranosyl)-D-
boivinose.
Figure 1.10: Chemical structure Brevobiose
Tigmobiose: It is non reducing disaccharide, isolated from the dried twigs of
Sarcostemma acidum. Structure has been established as 2,6-dideoxy-β-D-ribo-
hexopyranosyl 2,6-dideoxy-β-D-ribo-hexopyranoside (β-D-digitoxopyranosyl β-D-
digitoxopyranoside).
Figure 1.11: Chemical structure Tigmobiose
Sarcogenin : It is a pregnane genin, isolated from Sarcostemma acidum and has been
characterized as 13β,8β,11α,14 β,17 β -hexahydropregn-5en-20-one.
Figure 1.12: Chemical structure Sarcogenin

1. INTRODUCTION 55
Brevinine: It is a Pregnane ester diglycoside, isolated from the dried twigs of
Sarcostemma breoisrigma and has been characterized as 11-O-benzoyl-sarcogenin-3-O-
α-L-diginopyranosyl(1→4)-α-L-diginopyranoside.
Its chemical and spectroscopic data are consistent with structure -
Figure 1.13: Chemical structure Brevinine
Bergenin :It is trihydroxybenzoic acid glycoside. It is the C-glycoside of 4-O-methyl
gallic acid. It possesses an O-demethylated derivative called norbergenin. These are
chemical compounds and drugs of Ayurveda.Chemical Structure of Bergenin is-
(2R,3S,4S,4aR,10bS)-3,4,8,10-tetrahydroxy-2-(hydroxymethyl)-9-methoxy-3,4,4a,10b-
tetrahydro-2H-pyrano[3,2-c]isochromen-6-one.
Bergenin have various activity like Anti-inflammatory (T.Swarnalakshmi et al.1984),
Fever reducer, Obesity and Hepatoprotective activity (Xuan QIN et al 2010). It decongest
the airways and stimulates the bronchial secretion.It liquefies the mucus and enhances
expectoration.It strengthens immunity system against all type of cold. But still research is
necessary for Sarcostemma acidum herbal plant.
Figure 1.14: Chemical structure Bergenin
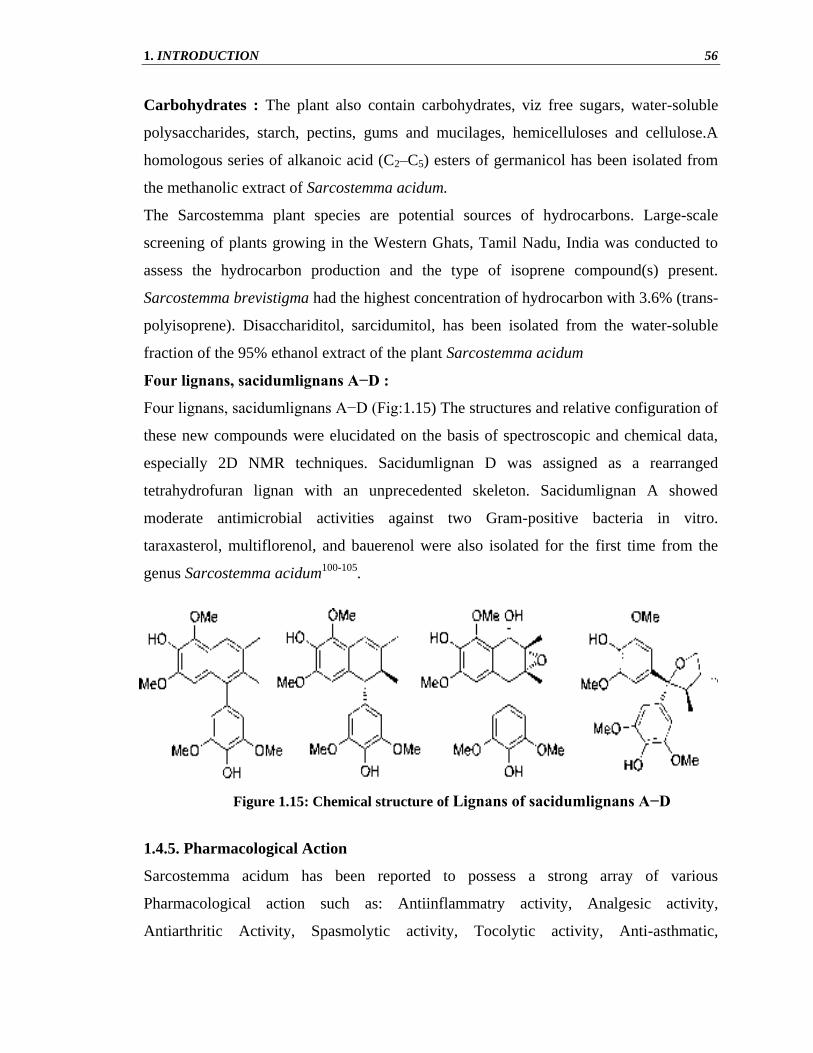
1. INTRODUCTION 56
Carbohydrates : The plant also contain carbohydrates, viz free sugars, water-soluble
polysaccharides, starch, pectins, gums and mucilages, hemicelluloses and cellulose.A
homologous series of alkanoic acid (C2–C5) esters of germanicol has been isolated from
the methanolic extract of Sarcostemma acidum.
The Sarcostemma plant species are potential sources of hydrocarbons. Large-scale
screening of plants growing in the Western Ghats, Tamil Nadu, India was conducted to
assess the hydrocarbon production and the type of isoprene compound(s) present.
Sarcostemma brevistigma had the highest concentration of hydrocarbon with 3.6% (trans-
polyisoprene). Disacchariditol, sarcidumitol, has been isolated from the water-soluble
fraction of the 95% ethanol extract of the plant Sarcostemma acidum
Four lignans, sacidumlignans A−D :
Four lignans, sacidumlignans A−D (Fig:1.15) The structures and relative configuration of
these new compounds were elucidated on the basis of spectroscopic and chemical data,
especially 2D NMR techniques. Sacidumlignan D was assigned as a rearranged
tetrahydrofuran lignan with an unprecedented skeleton. Sacidumlignan A showed
moderate antimicrobial activities against two Gram-positive bacteria in vitro.
taraxasterol, multiflorenol, and bauerenol were also isolated for the first time from the
genus Sarcostemma acidum100-105
.
1.4.5. Pharmacological Action
Sarcostemma acidum has been reported to possess a strong array of various
Pharmacological action such as: Antiinflammatry activity, Analgesic activity,
Antiarthritic Activity, Spasmolytic activity, Tocolytic activity, Anti-asthmatic,
Figure 1.15: Chemical structure of Lignans of sacidumlignans A−D

1. INTRODUCTION 57
Antiallergic activity,Bronchospasmolytic activity, Hepatoprotective activity,
Spermatogenesis, Larvicidal acivity, Immunity, C.N.S. depression, Antimicrobial
activity, Anti-Syphilitic and Anthelmintic Activity and Antioxidant Properties.106-121
1.4.6 Ethnomedical Uses of S. brevistigma
Source of hydrocarbons
Plant species are potential sources of hydrocarbons. Sarcostemma brevistigma may be
use as a source of biomass fuel. (Augustus et al. 2002) estimate the potential hydrocarbon
in selected species of Western Ghats, Tamil Nadu, which show that Sarcostemma
brevistigma has the highest concentration of hydrocarbon of 3.6%. While species such as
Tylophora asthmatica, Euphorbia tirucalli, Cryptostegia grandiflora, Ficus ealstica and
Euphorbia antisyphylitica contained more than 2%. The gross heat value of hydrocarbon
fraction in Sarcostemma brevistigma is 8733 Cal/g, which is comparable to fuel oil
calorific value. This study showed the significant importance of this plant in light of the
decline in global supplies of hydrocarbons, which has led to a search for alternate sources
of fuels.122
Use in inflammation
S. brevistigma is used in the treatment of swelling and inflammation condition. The
boiling water of S. brevistigma use to cure swelling. This ethnobotanical studies were
carried out by Y.S.patel et al. in Tapkeshwari hill of Bhuj Taluka (Kachchh district,
India) by collect information on the use of medicinal plants by local communities.
In The Treatment of Arthritis
S. brevistigma is used in the treatment of Arthritis. Whole part of plant crushed and made
to powdered given with water in case of asthma. Samir K Shah et. al. investigated the
antiarthritic activity stem of Sarcostemma brevistigma in experimental animals.123
In The Treatment of Preterm Labour
Sarcostemma brevistigma exhibits uterine relaxant activity, by interfering with the
extracellular Ca 2+
(P Suresh Kumar et al. 2006). This tocolytic activity of S.brevistigma
used in treatment of preterm labour. The major cause of perinatal morbidity and
mortality, is preterm labour. During term, oxytocin (OT) and prostaglandins act on the
uterus, and induce contractions, that result in preterm labour. OT binds to the specific
receptors, and increases the intracellular Ca 2+
level through release of Ca 2+
from both

1. INTRODUCTION 58
sarcoplasmic reticulum via inositol-1, 4, 5-triphosphate (IP3) pathway, and extracellular
fluid through voltage operated calcium channels. Preterm labour has been conventionally
treated with calcium channel blockers, OT antagonists, b 2-agonists, magnesium sulphate,
and prostaglandin synthetase inhibitors. However, these drugs are sometimes inadequate,
and have adverse effects like tachycardia, increased cardiac output, pulmonary edema,
hyperglycemia, cardiac depression, and inhibition of neuromuscular transmission.110
Asthma
According to folklore, this plant extract is used for the treatment of asthma. 124
Cough, chronic and acute bronchitis
S. brevistigma have bronchospasmolytic activity because it inhibited the contractions
induced by acetylcholine and histamine on animal. And for bronchospsmolytic activety it
have antitusive properties and used in cough, congestion of the upper respiratory tract,
asthma, chronic and acute bronchitis. Its antiinflammetory property also help to relief
pain in dry cough condition.125-126
Used in treatment of Cold
According to folklore of Tribals of Sriharikota Island, Andhra Pradesh it is used to relief
from cold,10-15 ml of fresh stem juice slightly warmed administered orally to children
for 4-5 days to get relief from cold.
Cataract
According to folklore of Tribals of Sriharikota Island, Andhra Pradesh, Latex of
S.brevistigma dropped into eyes in case of early stages of cataract (Suklamu).127
In preparation of male contraceptive pills
In medieval Persia various herbs were used for male contraception, Sarcostemma acidum
(Asclepiadaceae) is one of that drugs. However, the compound isolated from Gossypium,
as well as other cotton seeds and okra (gossypol) has been abandoned as for contraceptive
use because it was found to cause permanent infertility in ten to twenty percent of users.
Multiple male hormonal contraceptive protocols have been developed. One is a
combination protocol, involving injections of Depo-Provera to prevent spermatogenesis,
combined with the topical application of testosterone gel to provide hormonal support.
Sarcostemma acidum has property of preventing spermatogenesis.115

1. INTRODUCTION 59
Rejuvenation
S. brevistigma strengthens the immunity system against all types of cold. It is used in
general debility, mental disorders, to rejuvenate the mind and senses, and have attributed
mood-enhancing properties to help alleviate stress, depression and insomnia. Combined
with healthy diet, regular exercise, and lifestyle measures such as meditation, S.
brevistigma helps to promote mental and emotional wellness.Quantum adaptogen
complex containing S. bevistigma have been used for thousands of years for that
purpose.122
Burning micturation
C.Sudharkar Reddy et al. Studied in traditional medicinal plants in Seshachalam hills
Andhra Pradesh, India and giving the ethno medicinal use of sarcostemma acidum that it
is use during burning maturation (A teaspoonful of plant powder administered with two
cups of toddy). 127
Milky juice is anti-syphilitic and anthelmintic
Some articles state that milky juice of S. brevistigma is used as a anti-syphilitic and
anthelmintic however farther scientific study is necessary.128-129
Root have been used in snack bite and rabies
A.S.Wabale et al. studied on the basis of aquestionnaire prepared containing the
information about the tribals, their living style, source of income, ethnomedicinal uses of
plant species and their style of treatment with references of tribal vaidyas of Kalsubai and
Ratangad and concluded that S. brevistigmma was used externally as a ethnomedicinal
plants in the treatment of dog and different animal bites. There is need for further
scientific research.130
Dyspesia and other gastric problem
Powder part is given twice a day with cow milk or Luke water as remedy for gastric
problems.131
1.4.7 Marketed Product
Various marketed product are available of sarcostema acidum for treatment of different
diseases which are shown in Table.1.2 and fig.1.16. 132-141

1. INTRODUCTION 60
Table 1.2: Marketed products containing Sarcostemma acidum herb
S.No Marketed
Product
Ethnomedical Uses
1. Coughend, Cofdar
Syrup and Quote
Capsule
All types of cough (dry, productive, gasp) and is also a
stimulant of bronchial secretions.. .
It decongests the airways, stimulates the bronchial secretions.
It is good as a complementary therapy in acute and chronic
bronchitis and in asthma therapy.
2. Sewanti Stressnil Used to treat mental stress, depression, and insomnia.
3. Koflin Syrup Cough of allergic, infective or asthmatic origin, Cough
associated with gastro-esophageal reflux, Cough caused by
dusts, Cough of TB, Bronchial asthma
5. Asthalab Tablet
For Smokers cough, allergic, seasonal cough, and spasmodic
cough.
7. Kashin Syrup It also provides quick and long lasting relief from coughs and
sore throat. .
It provides bronchodilator activity and offers an antimicrobial
and anti-inflammatory action on the respiratory system.
8. Ecasma Tablet Used in Bronchitis, Laryngitis, Respiratory tract infection,
Nasal congestion, Cough and Asthma
9. Spasma Syrup Used in cough of allergic, infective or asthmatic origin,
cough associated with gastro-esophageal reflux, cough
caused by dusts, cough of TB, bronchial asthma.
10. Shankof Syrup Productive Cough & Non Productive Cough .Bronchitis.
Asthma, Whooping Cough, Lung Infection, Dry Cough,
Wheezing.
12. Vikas Amrit It is very effective in reducing overweight and obesity
13. Nakas Syrup For asthmatic cough it reduces mucosal irritation in the
respiratory tract in non productive cough

1. INTRODUCTION 61
(a) (b) (c) (d)
(e) (f) (g)
Figure 1.16: Marketed product containing S.acidum herb
(a),Coughend Syrup,(b)Stressnil Syrup,(c) Kflin Syrup,(d) Quantum adaptogen complex capsule,
(e) Asthaleb tablet, (f) Vikas Amrit capsule, (g) soma complex.

1. INTRODUCTION 62
1.4.7 Conservation and Cultivation Practices
The need for conservation of Sarcostemma acidum medicinal plants
The use of medicinal plants as raw materials in the production of new drugs is ever
increasing because of their potentials in combating the problem of drug resistance in
micro-organisms. Demand for medicinal plants is increasing in both developing and
developed countries. Research on medicinal plants is one of the leading areas of research
globally. However, there is a need to pay closer attention to the issue of conservation of
medicinal plants.
Somlata (Sarcostemma acidum) belonging to the family Asclepiadacea grown in India,
Europe and US is an underutilized crop. The herb is highly used by the rural and tribal
people in curing various disorders such as asthma, swelling, fever and cold, dyspepsia,
inflammatory infection, gastric problems and as rejuvenating .There is a great need to
conserve these medicinal plants because they contain highly bioactive components which
can be developed into pharmacologically active agents. The plant is widely used in the
treatment of various diseases and disorders, so there is need for necessary conservation
of this plant.
Reasons to become endangered species
1. The use of S.acidum is reducing day by day because people decline to walk long
distances to collect them and also lack of knowledge.
2. Rising number of human and animal population which causes pressure on plant
survival. Human agricultural activities result in clearing of natural habitats for
farming and grazing, trees are felled for timber, charcoal and other commercial
uses and lands are used in a way that are not sustainable.
3. Popularity of Sarcostemma brevistigma has decreased now.
4. Due to modernization and destruction of natural habitat.
5. Due to biotic interference
6. Fungal growth on the plant which deplete the species.
Need of bioactivity-safety evaluation of Sarcostemma acidum
Sarcostemma brevistigma Wight (family Asclepiadaceae) grows throughout India and
other tropical regions of the world. It is found to be active as anti-rheumatic, anti-allergy,
anti-emetic and branchodilator. Phytochemical studies reveal the presence of bergenin,
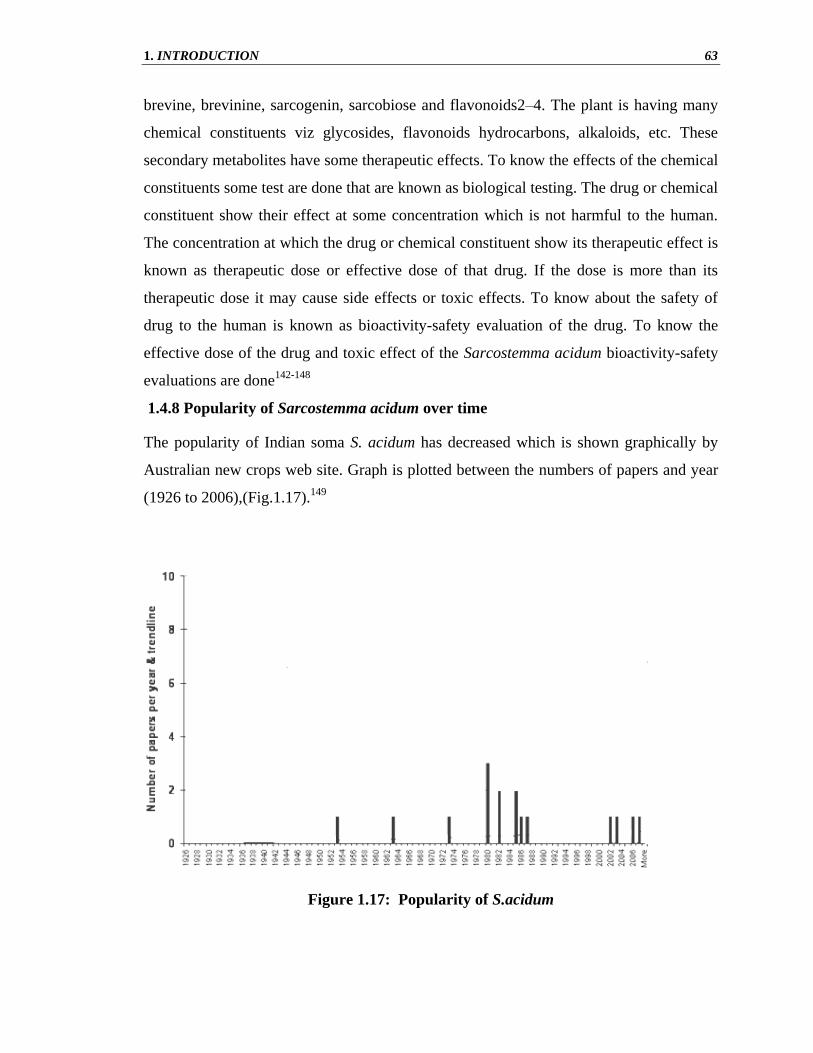
1. INTRODUCTION 63
brevine, brevinine, sarcogenin, sarcobiose and flavonoids2–4. The plant is having many
chemical constituents viz glycosides, flavonoids hydrocarbons, alkaloids, etc. These
secondary metabolites have some therapeutic effects. To know the effects of the chemical
constituents some test are done that are known as biological testing. The drug or chemical
constituent show their effect at some concentration which is not harmful to the human.
The concentration at which the drug or chemical constituent show its therapeutic effect is
known as therapeutic dose or effective dose of that drug. If the dose is more than its
therapeutic dose it may cause side effects or toxic effects. To know about the safety of
drug to the human is known as bioactivity-safety evaluation of the drug. To know the
effective dose of the drug and toxic effect of the Sarcostemma acidum bioactivity-safety
evaluations are done142-148
1.4.8 Popularity of Sarcostemma acidum over time
The popularity of Indian soma S. acidum has decreased which is shown graphically by
Australian new crops web site. Graph is plotted between the numbers of papers and year
(1926 to 2006),(Fig.1.17).149
Figure 1.17: Popularity of S.acidum

1. INTRODUCTION 64
1.4.9 Cultivation Practices
Humanities rely on a diverse range of cultivated species. It is often stated that only a few
staple crops produce the majority of the food supply. Several countries in the world have
a rich heritage of herbal drugs, very few can put claim for their procurement only from
cultivated species. It is recently that some of these drugs have been subjected to
systematic cultivation based on modern scientific information (Getinet et al., 1996). Our
reliance on wild sources of crude drugs and the lack of information of sound cultivation
technology have resulted in gradual depletion of raw materials from wild sources.
The wealth of India is stored in the enormous natural flora which has been gifted to her.
Endowed with diversity of agro-climatic conditions, India is virtually herbarium of the
world. India possesses all types of climatic conditions varying from north to south.
Because of vast area and variety of agro-climates, a large number of medicinal and
aromatic plants are found growing wildly and has been considered as “Botanical Garden
of the World” and this botanical wealth constitutes more than 2200 species of medicinal
and essential oil containing plants. (Kokate et al., 2005).
Cultivation is frequently advocated as a measure to take pressure of wild stocks
especially for species collected in large quantities for trade. It can be commercially
attractive to companies because they have greater control over quality and supply.
Various factors influence the feasibility of cultivation. The best way to provide the plant
material needed for medicine is to cultivate the plants. Cultivation of medicinal plants is
one of the major mechanisms by which conservation, sustainable harvesting as well as
utilization can be drawn simultaneously. With the increasing demand of natural resources
in the world, cultivation of medicinal plants will be more profitable than cultivating
conventional cash crops. Thus, it becomes essential to generate the knowledge of
agronomics and make the same available to the farmers with agricultural technologies
(Verma et al., 2007).
Protein, carbohydrates, vitamins and fats are the main constituents of our diet. Oil is an
important source of fat and is important in human diet. Beside this, oil plays a vital role
in maintaining the agricultural economy of the country. The necessity for providing more
oil and fat to the human society has been the incentive for intensive cultivation of crops.
Scientists are working in this field to search out natural sources of oil crop’s containing

1. INTRODUCTION 65
various drugs of medicinal importance. Their sole aim has been to have better yield.
Later, as a result of more and more appreciation of oil in our daily food, they have
unavoidable place in man’s economy. As a matter of facts, the interest in production of
oil crops has increased tremendously in recent years (Kumar, 1992).
The general cultivation practices of S. acidum are given below (Table 1.3)150-154
: (as per
Dwivedi 2010)
Table 1.3: Cultivation practices of S. acidum
S/No. Parameters Requirements
1. Method of propagation Stem cutting
2. Size of stem cutting 4-6 inch
3. Nature of soil Loamy –sandy
4. Irrigation Very less amount of water is required
5. Light range Partially
6. pH range 5-8
7. Water range Dry
8. Temperature Moderate to low
9. Bloom time Early Summer
10 Fertilizers Generally fertilizers are not required
11. Phyto-hormones Addition of IAA and GA3 will
increase the aerial growth of the plant
Addition of Ethylene will promote the
more number of flowers
12. Pesticides Generally malathion or other anti-
fungal agents may be spread to avoid
the growth of fungus in the plant.
13. Weedicides Normally not required