1 mlab 2401: clinical chemistry quality control, quality assessment and statistics
TRANSCRIPT

1
MLAB 2401: Clinical Chemistry
Quality Control, Quality Assessment and Statistics

2
Quality Assurance/Assessment (QA)
An all inclusive / comprehensive system monitoring the accuracy of test results where all steps before, during and after the testing process are considered. Includes pre-analytic, analytic and post analytic factors
Essentials include commitment to quality, facilities, resources, competent staff, and reliable procedures, methods and instrumentation
Provides a structure for achieving lab and hospital quality goals

3
Quality Control (QC)
QC systems monitor the analytical process; detect and minimize errors during the analysis and prevent reporting of erroneous test results.
It uses statistical analysis of test system data Requires following published rules
Westgard Rules

Types of QC
Internal Daily Establishment of
reference ranges Validation of a new
reagent lot and/or shipment
Following instrument repair
External Proficiency testing
Determination of laboratory testing performance by means of intralaboratory comparisons
CAP, CLIA, The Joint Commission requirement
Must be integrated within routine workload and analyzed by personnel who are running the tests.
Ongoing evaluation of results to correct for unacceptable results
Used to access employee competency
4

Pre-Analytical & Analytical Causes of Error
5

Post- Analytical Causes of Error
Incorrect reference values Physician not notified of a panic or critical
value Incorrect interpretation of lab results by
physician Incorrect data entry of lab result
6

7
Introduction to Statistical Analysis
When evaluating laboratory results, how do we determine what is normal or acceptable? In other words: What is “normal” or “OK”?
When does a laboratory test result become “weird” or “abnormal” ? When do we become uncomfortable with a result?
At some point we have to draw a “line in the sand” … on this side of the line you’re normal … on the other side of the line you’re abnormal. Where and how do we “draw the line” ?
Answer: Statistics are used to determine the lines of ‘normal’ and ‘acceptable’.
8
Statistical Concepts
Statistics is a (science of )branch of mathematics that collects, analyzes, summarizes and presents information about “observations.”
In the clinical lab, these “observations” are usually numerical test results
A statistical analysis of lab test data can help us to define Reference ranges for patient’s (normal and abnormal) Acceptable ranges for control specimens ( “in” and “out” of
control)

Measures of Central Tendency
Mean (x̄? ) - the mathematical average of a group of numbers, determined by adding a group of numbers (events) and dividing the result by the number of events
Median - determined as the ‘middle’ of a group of numbers that have been arranged in sequential order. That is to say, there are an equal number of numbers on either side of the ‘middle’ number. In an odd # of observations, it is the middle observation. In an even # of observations, average the two middle values.
Mode - the number that appears most frequently in a group of numbers. There can be more than mode, or none at all.
9
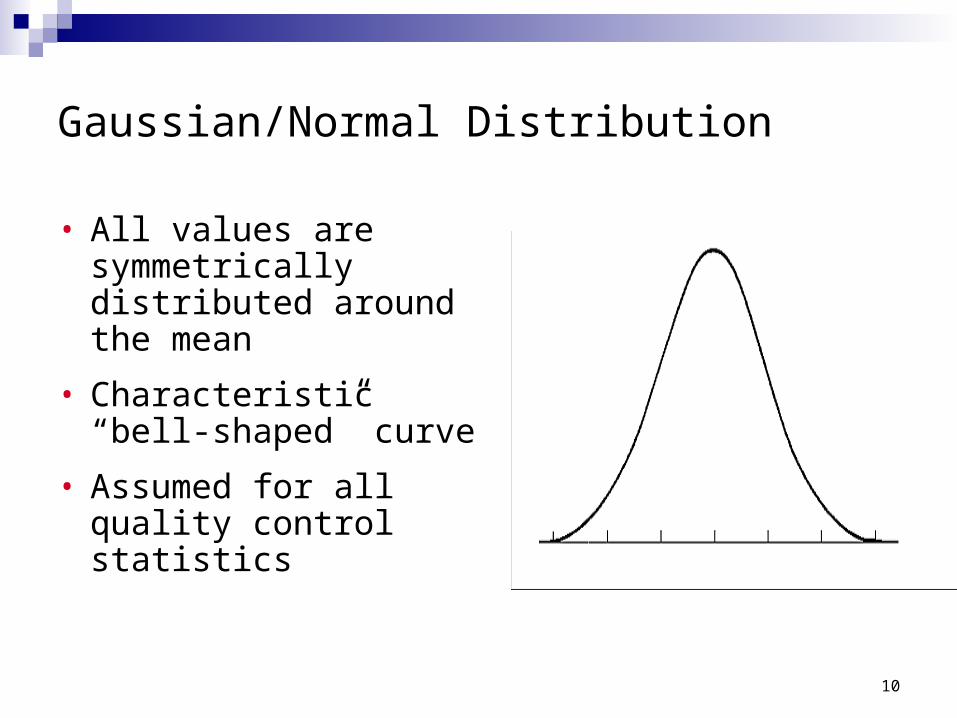
Gaussian/Normal Distribution
• All values are symmetrically distributed around the mean
• Characteristic “bell-shaped” curve
• Assumed for all quality control statistics
10

11

Accuracy and Precision
The degree of fluctuation in the measurements is indicative of the precision of the assay. Precision-refers to the ability to get the same (but not
necessarily ‘true’) result time after time.
The closeness of measurements to the true value is indicative of the accuracy of the assay. Accuracy - An accurate result is one that is the ‘true’
result.
12

Precise and AccuratePrecise and Accurate

Systematic Error
Random Error
Systematic error
Systematic change in the test system resulting in a displacement of the mean from the original value
Systematic error of an analytic system is predictable and causes shifts or trends on control charts that are consistently low or high
15

Causes of Systematic Error
Change in reagent or calibrator lot numbers Wrong calibrator values Improperly prepared reagents Deterioration of reagents or calibrators Inappropriate storage of reagents or calibrators Variation in sample or reagent volumes due to pipettor
misalignments Variation in temperature or reaction chambers Deterioration of photometric light source Variation in procedure between technologists
16

Random Error
Imprecision of the test system causing a scatter or spread of control values around the mean
17
Causes of Random Error
Air bubbles in reagent Improperly mix̄ed reagents Reagent lines, sampling, or reagent syringes Improperly fitting pipette tips Clogged or imprecise pipetter Fluctuations in power supply
18

Bias
Bias – the amount by which an analysis varies from the correct result.Ex̄ample, If the Ex̄pected Value is 50 units,
and the result of an analysis is 47, the bias is 3 units.
19
20
Statistical Formulas
Standard Deviation (SD) Is a mathematical ex̄pression of the dispersion of a
group of data around a mean.
SDx x
n
2
1

21
SDx x
n
2
1
x
Standard Deviation :
n = the number of observations (how many numerical values )
Σ = the sum of … in this case, the sum of
= the mean value
X = the value of each individual observation
The Standard Deviation is an expression of dispersion … the greater the SD, the more spread out the observations are
x x2

Standard Deviation and Probability
For a set of data with a normal distribution, a value will fall within a range of: +/- 1 SD 68.2 % of the
time +/- 2 SD 95.5% of the
time +/- 3 SD 99.7% of the
time
22

23
Statistical Formulas Coefficient of Variation (CV)
Indicates what percentage of the mean is represented by the standard deviation
Reliable means for comparing the precision or SD at different units or concentration levels
Ex̄pressed as a percentage
CV% =
Standard deviation X 100
mean
24
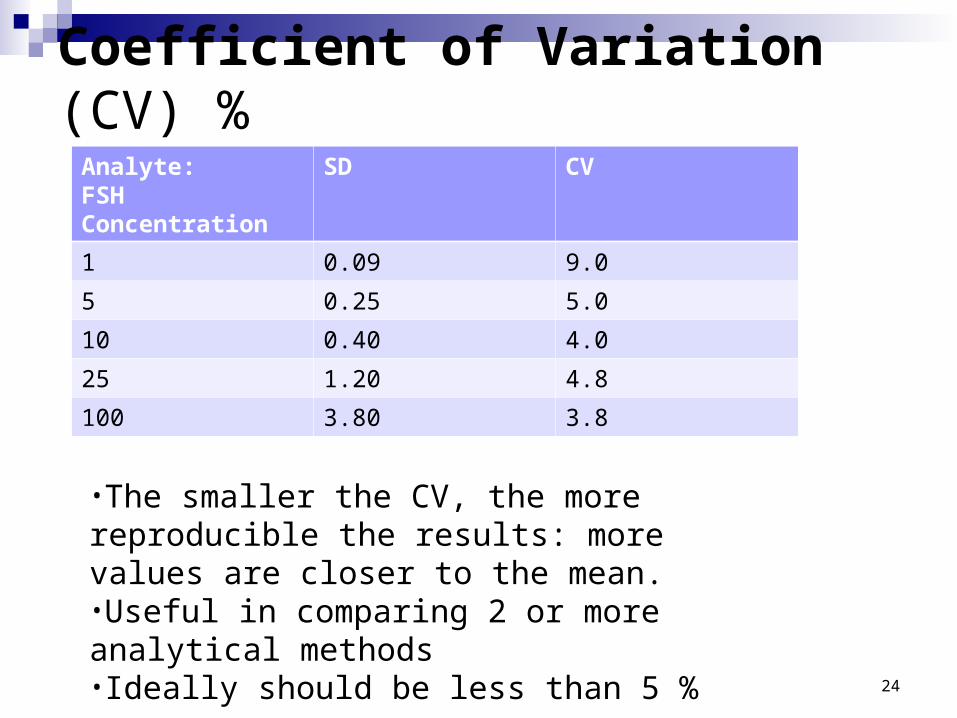
Coefficient of Variation (CV) %
Analyte:FSH Concentration
SD CV
1 0.09 9.0
5 0.25 5.0
10 0.40 4.0
25 1.20 4.8
100 3.80 3.8
•The smaller the CV, the more reproducible the results: more values are closer to the mean.•Useful in comparing 2 or more analytical methods•Ideally should be less than 5 %

Establishment of a QC System
Two or three levels of control material used A control is a material or preparation used to monitor
the stability of the test system within predetermined limits
Measure of precision and reproducibility
Purpose: verify the analytic measurement range of instrument for a specific analyte
25

Establishment of a QC System
Control material matrix̄ should resemble actual specimens tested Lyophilized/liquid Assayed
Mean calculated by the manufacturer Must verify in the laboratory
Unassayed Less ex̄pensive Must perform data analysis in house
26

27
Establishment of a QC system Collecting data
Run assay on control sample & manually enter control results on chart
One chart for each analyte and for each level of control

28
Establishment of a QC system Collecting data
Many modern chemistry analyzers have computer program that maintains the QC log.
i.e Dade Dimension
29
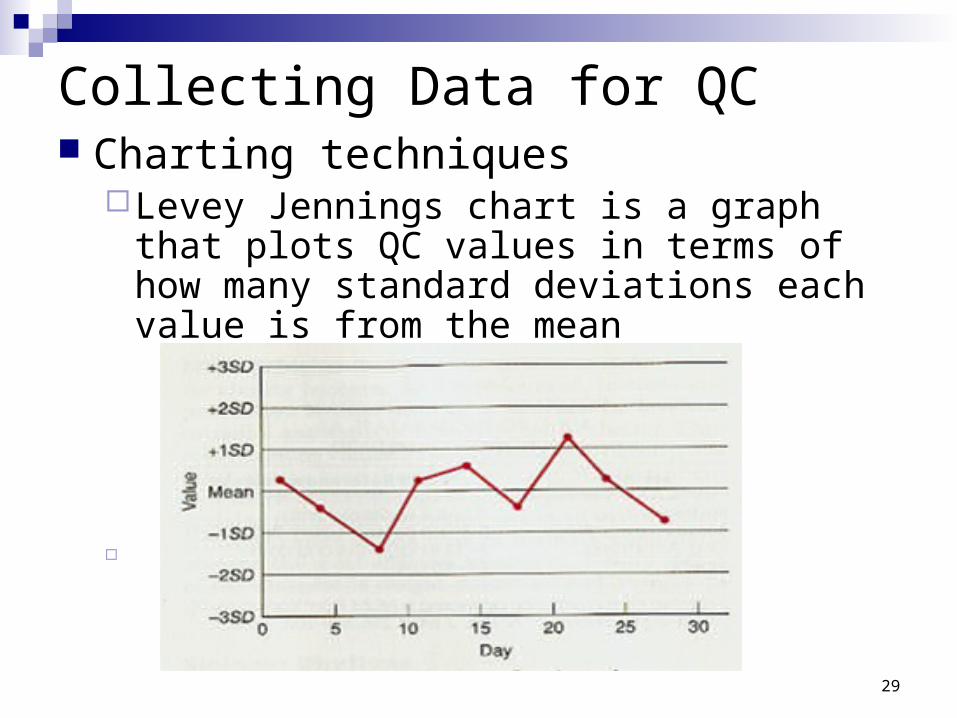
Collecting Data for QC Charting techniques
Levey Jennings chart is a graph that plots QC values in terms of how many standard deviations each value is from the mean

30
Use of Standard Deviation
Once you have determined the standard deviation, must use the information to evaluate current/ future analysis.
Most labs make use of ± 2 SD or 95% confidence limit. To put this into a workable form, you must establish the range of the ± 2 SDs

31
So, how do we determine the range of acceptable results ?
Scenario Mean of group of control values = 104 mg/dL Standard Deviation = ± 5 mg/dL Determine the Range of ± 2SD; (which will allow you
to evaluate acceptability of performance of the control on subsequent days.)
Is a control value of 100 mg/dL acceptable?

Shifts and Trends
ShiftQC data results are distributed on one side of
the mean for 6-7 consecutive days
TrendConsistent increase or decrease of QC data
points over a period of 6-7 days
32

33
But what if your control specimen is “out of control?”
“Out of control” means that there is too much dispersion in your result compared with the rest of the results
This suggests that something is wrong with the process that generated that observation
Patient test results cannot be reported to physicians when Patient test results cannot be reported to physicians when there is something wrong with the testing process that is there is something wrong with the testing process that is generating inaccurate reportsgenerating inaccurate reports
Remember … No information is better than wrong Remember … No information is better than wrong informationinformation

Westgard System
34
Is 1control> 2 SD?
12S
No
Yes
No NoNo NoYes
No
Violation
randomindicates
error
Violation
randomindicates
error
indicates
errorsystematic
Violationindicates
errorsystematic
Violation
Rejectrun
ReportResults
Is 1control> 3 SD?
13S
Are 2controls> 2 SDon sameside ofmean?
22S
Is SD
controls
betweendifference
any 2
> 4?
R4S
Are 4
controls> +/- 1 SD?
consecutive
42S
Acceptrun
Acceptrun
Are 10
controlsconsecutive
on sameside ofmean?
10X
ReportResults
Rejectrun Reject
run
Rejectrun
Rejectrun
indicates
errorsystematic
Violation
Yes Yes
Yes
Yes
Testremaining
rules
Testremaining
rulesTest
remainingrules
Testremaining
rules

35
But what if your control specimen is “out of control?”
Corrective methods
Things that can go Wrong Corrective Action
Instrument malfunction Identify malfunction and fix̄
Reagents: preparation, contamination, volume
New reagents
Tech error Identify error and repeat test
Control specimen is old or prepared improperly
Use new control

QC terms
AMR= Analytical Measurement Range Range of analyte values that a method can directly measure on
the specimen without any dilution, concentration or other pretreatment
CRR= Clinical Reportable Range Range of analyte values that a method can report as a
quantitative result, allowing for specimen dilution, concentration, or other pretreatment used to ex̄pand the direct AMR.
36
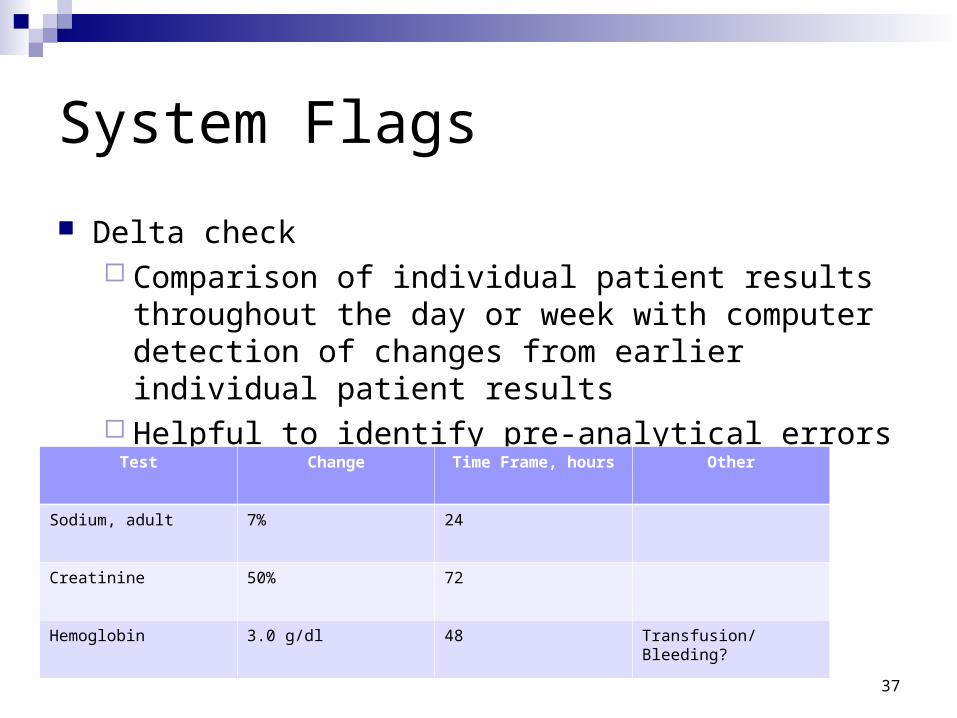
System Flags
Delta check Comparison of individual patient results throughout
the day or week with computer detection of changes from earlier individual patient results
Helpful to identify pre-analytical errors
37
Test Change Time Frame, hours Other
Sodium, adult 7% 24
Creatinine 50% 72
Hemoglobin 3.0 g/dl 48 Transfusion/ Bleeding?

38
Establishment of Reference Ranges
Reference ranges – the ‘normals’ The normal or ex̄pected value for patients. Are defined as being within +2 Standard
Deviations from the mean A large sampling of clinical normal
representatives.
Each lab must establish its own reference ranges based on local population

39
Establishment of Reference Ranges
Factors affecting reference ranges:
Age Sex̄ Diet Medications Physical activity Pregnancy Personal habits (smoking, alcohol) Geographic location (altitude) Body weight Laboratory instrumentation (methodologies) Laboratory reagents
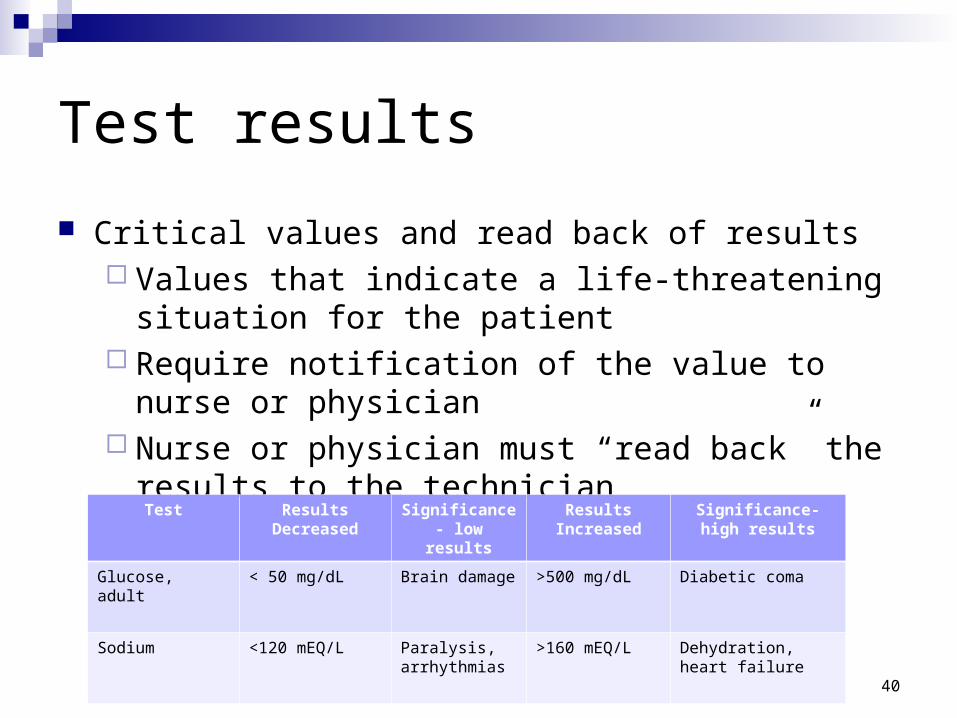
Test results
Critical values and read back of results Values that indicate a life-threatening situation for the
patient Require notification of the value to nurse or physician Nurse or physician must “read back” the results to the
technician
40
Test Results Decreased
Significance- low results
Results Increased
Significance- high results
Glucose, adult < 50 mg/dL Brain damage >500 mg/dL Diabetic coma
Sodium <120 mEQ/L Paralysis, arrhythmias
>160 mEQ/L Dehydration, heart failure
References
Astles, J. R., Stang, H., & Alspach, T. (2013, September). CLIA requirements for proficiency testing: the basics for laboratory professionals. MLO, 45(9), 8-15.
Bishop, M., Fody, E., & Schoeff, l. (2010). Clinical Chemistry: Techniques, principles, Correlations. Baltimore: Wolters Kluwer Lippincott Williams & Wilkins.
Sunheimer, R., & Graves, L. (2010). Clinical Laboratory Chemistry. Upper Saddle River: Pearson .
41