1 neonatal swallowing and feeding lamya al-abdulkarim, ph.d., ccc-slp, mass. license, nomas...
TRANSCRIPT

1
Neonatal Swallowing and Feeding
Lamya Al-Abdulkarim, Ph.D., CCC-SLP, Mass. License, NOMASDepartment of Rehabilitation
College of Medical Applied SciencesKing Saud University
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
2
Learners objectives
Identify issues related to swallowing function
Determine underlying factors/etiology
Differentially identify feeding and swallowing problems
Determine if F/U evaluations/tests are needed
Develop and/or implement treatment/intervention strategies to improve or alter the factors that may influence a neonate’s swallowing and feeding disorder
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

3
Background and Overview
The care giving model for preterm infants has evolved into a holistic framework integrating medical as well as early developmental interventions to support the neurobehavioral and physiologic organization of the neonate.
Any patient represents an interrelated system
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

4
Anatomy and physiology of the oral mechanism:
Pediatrics
• Emergence of primitive oral reflexes:
• Gag reflex: 32 weeks
• Rooting reaction: mouth opening at 32 weeks
• Transverse tongue reflex: 28 weeks
• Phasic bite: 28 weeks
• Non-nutritive suck: in utero
• Nutritive suck: immature pattern, mature pattern
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
5
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
Mouth narrow and small
When open mouth: tongue up against alv. ridge (normal) secondary to developing oral structure
Compressed oropharyngeal structures which is a natural protection from aspir.
Cheeks right against teeth. Sucking pads to keep mouth stable (no buckle cavity)

6
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

7
Developmental Subsystems in Neonates
• Autonomic
• Motor
• State (Als, 1984)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

8
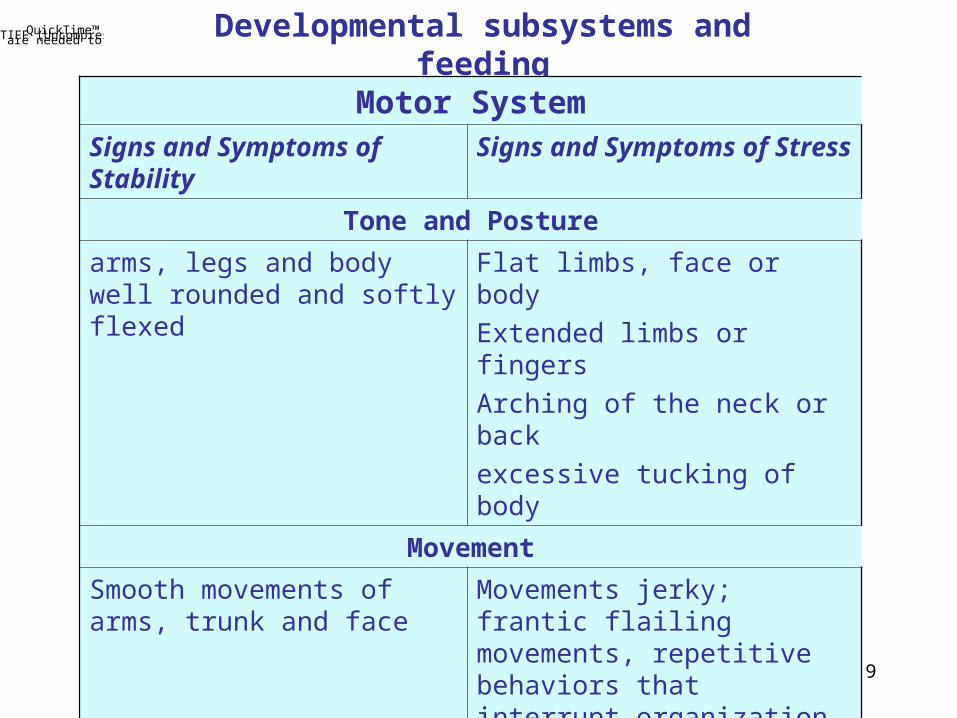
Developmental subsystems and feeding(Als, 1986, Browne, et al., 1990)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
Autonomic System
Signs and Symptoms of Stability Signs and Symptoms of Stress
Color
Pink over the entire body Pale, red, dusky or mottled color changes on part or whole body
Respiratory pattern/Breathing
Regular
40 - 60 breaths/minute
Uneven intervals, > 60 or < 40 breaths/minute; pauses > 2 sec.’s;
Gasps, yawns, coughs
Visceral Signs
Stable digestion with appropriate burping; regular elimination of abdominal wastes
Regurgitation, hiccups, gagging, excessive drooling, diarrhea, gases
9
Developmental subsystems and feedingQuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
Motor SystemSigns and Symptoms of Stability Signs and Symptoms of Stress
Tone and Posture
arms, legs and body well rounded and softly flexed
Flat limbs, face or body
Extended limbs or fingers
Arching of the neck or back
excessive tucking of body
Movement
Smooth movements of arms, trunk and face
Movements jerky; frantic flailing movements, repetitive behaviors that interrupt organization and stability
Self-regulatory behaviors
Holding hands to face
Mouthing/sucking on hands
Adjusting posture
Not successful at

10
Developmental subsystems and feedingQuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
State System
Signs and Symptoms of Stability Signs and Symptoms of Stress
Sleep or fully awake is clearly defined
Smooth transition
Appropriate state for the situation
Stable, predictable cycles (e.g. schedule)
Control and not overwhelmed by stimuli
States not easily defined
Rapid changes
Inappropriateness of state to time
Unpredictable cycles
Overwhelmed by stimuli
Sleep states: Robust deep sleepy; light sleep; drowsy; alert; actively aroused; highly aroused

11
Developmental subsystems and feeding
Clinical Goal: improving feeding skills by helping the infant regulate the organization of all the subsystems (e.g. Browne and Ross, 2001)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

12
• A sensori-motor coordination of:• suck- swallow - breathe (S-S-B)• Interaction of the jaw, tongue, soft palate, pharynx, larynx and esophagus (e.g. Miller, 1982)
• burst (a short pause)• Typical pattern: >15 reps of S- S-B between two bursts• Ultrasound studies showed that most infants older than 37 weeks pma mature to 1:1:1 ratio (BuLock, 1990)
• Mature pattern:• by 6 - 12 weeks in infants born at 32 - 34 weeks pma• by 2 weeks born at 34 - 36 weeks pma (Gryboski, 1969)
• term infants: continuous improvement within first month (Qureshi, et.al.,
2002)• Correlation between PMA and feeding skills (e.g. sucking, breathing, volume, alertness) (Medoff-Cooper, et.al, 2000, Gewolb, 2001)
• Heart rate: 120 - 180 bpm; Respiratory rate 40 - 60; oxygen saturation above %90.• A developmental indicator of maturation (e.g. Gewolb, et.al., 2001;
Hanlong, et.al., 1997)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture. Feeding in Neonates
13
Non-nutritive sucking
Sucking on pacifier or gloved finger *: fast rhythm with 5-10 sucks/burst
Benefits:-regulating (respirations, GI peristalsis, oxygen saturation, heart rate)
(Sehgal, 1990; Woodson and Hamilton, 1988)
behavioral state changes during feeding
- alert states (McCain, 1995) length of stay
- improved transitions
- better bottle feeding (Pinelli & Symington, 2001)
* Please note hand hygiene protocol
Types of Sucking FunctionsQuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

14
Nutritive Sucking
Sucking for feeding: suck-swallow-breathe pattern; suctioning and expression
Stages of development (Palmer, 2003):
a. Obligatory: no transition from NNS; 15 - 25 bursts; does not stop to breathe;
caregiver must intervene
b. Alternating: longer sucking bursts with desaturation; shorter bursts with
stable saturations; state of alertness to complete feeding
c. Intermittent: brief breathing rests (2 - 3 sucks); stronger suction; integration
of sucking and expression; longer sucks, volume; alert state
d. Coordinated: mature suck pattern (20- 30 sucks/burst); integration of
sucking-breathing (suck-swallow-breath); alert state during feeding;
usually after transitioning to home
e. Integrated: social interaction during feeding; full coordination of suck-
swallow-breath; demanding prior to feeding
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.

15
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.Assessment-Intervention Pathways for Oral Feeding in Neonates
Initial Screening using a tool based on Saudi neonates
(c.f. hearing screening)
Referrals for a diagnostic evaluation by a specialist depending on the need area(s) of the neonate (e.g. to Neuro,GI, ENT, OT, PT,SLP)
Dx of feeding disorderand/or other subsystems
Positive
F/U with family
Negative
Intervention: Medical,Behavioral, Feeding
Reassessment and F/U
Discharge (identify emerging disabilities

16
Feeding Disorders in NeonatesQuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
� � The transition to full nipple feeding is an important criterion for discharge from the NICU.
At risk neonates for feeding and swallowing disorders
Infants born prematurely Infants born following an intrauterine event or a difficult deliveryInfants with cardiac issuesInfants with congenital anomaliesInfants with diabetic mothers (IDMs)Infants with acquired medical conditionsExtended stay in the NICU
(Hawdon, et.al., 2000, Hay, et.al., 1999, Rogers, et.al., 1998, Singer, et.al., 1992)

17
Assessment of Feeding Skills in Neonates and Preterm Infants
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
I. Infant’s background history (pre-, peri- and postnatal Hx for at risk &/or etiological factors that could impact feeding skills)
II. Observation of an infant’s neurobehavioral output and self-regulation skills
III. Establish an infant’s baseline before initiating feeding
1. Alertness, controlled stability2. Holding3. Establish stability with Non-nutritive sucking (NNS):
pacifier 5 - 10 sucks/burst; Rate: fast

18
Assessment of Feeding Skills in Neonates and Preterm Infants
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
IV. Assessment of sucking patternNutritive suck
Three sucking patterns (Palmer, 2001)
√ Normal: Sucking , swallowing and breathing are coordinated indicating self-regulation
√ Disorganized √ Dysfunctional
Look for signs/symptoms of stress during feeding across the developmental subsystems:
Changes in color, state of alertness, breathing and swallowing
Check respiratory status during and after feeding

19
QuickTime™ and aDV/DVCPRO - NTSC decompressor
are needed to see this picture.
20
QuickTime™ and aYUV420 codec decompressor
are needed to see this picture.
21
Assessment of Feeding Skills in Neonates and Preterm Infants
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
Predictors of sucking abilities- At term: duration of oxygen use- Postnatal age when nipple feeding began
3 months adjustedNumber of days of intubationGestational age at birth
(Blaymore Bier, et.al.,
1993)
Breast feed vs. Bottle feed:Breastfeeding is variable: s/s could be due to infant’s adaptabilityLabored breathing with nasal flaring is a reliable clinical sign of disorganized sucking at the breastHowever, oral-motor patterns during reflexive sucking are independent of type of feedingFor assessment, use the most familiar feed for the infant 20 decreased adaptability by premies (Palmer, 2002)

22
Team: MD, RN, Family, SLP/PT/OT
Individualized, developmentally supportive approach to nipple feeding:
1) Observation of behavioral cues for infant stability or stress
2) Response to an infant’s cues to help her regain and maintain coordination
3) Parent education and training in feeding their infant
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.The Intervention Model for Nipple Feeding

23
Develop a feeding plan for continuity Feed only after resting/sleep
If an infant has an open-mouth posture indicating a mouth breather, try a pacifier to see if she is comfortable
Provide appropriate oral experiences: (Ross, 2003) -Positioning w/ hands to face- provide nurturing experiences during gavage feeding- introduce appropriate smells, tastes- allow rooting to a finger or pacifier to maintain sucking abilities and association between oral and GI systems- avoid oral stimulation when infant is sleep- place milk on fingers to hand to mouth association (discuss with pulmonologist)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.Intervention strategies
General guidelines

24
Modifying variables that affect sucking and feeding
Imposed breaks: regulate sucks by allowing 3 to 5 sucks then pause and remove nipple Bolus size: first two minutes is the best time an infant would take most during oral feed. What is left could be given by
gavage. Flow rate:
- slow the flow to support organization of suck/swallow/breathe and burst rhythm- tipping of bottle: out of central tongue groove/ removal of bottle- nipple selection: material, shape, size, flow rate
(Ross, 2003)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.Intervention strategies

25
Support to the neonate during feeding based on her needs: - jaw - cheeks - position: upright, midline, swaddle, next to caregiver (Ross, 2003),
no flexion (re. GER: 60% of premies,Tsou,et.al., 1998)
- regulating feeds - holding rather than stroking or patting; rocking could be overwhelming - Self-regulation: hands to mouth, bracing feet, NNS, state
Support timing and pacing of feeding schedule
Oral feeding: - mean ~34 - 36 weeks - When moved to fully interval gavage (Lau, 2003)
Important: infant’s abilities to tolerate nipple feeding should be the indicator to readiness to feed not gestational age (e.g.Hanlon, et.al., 1997;Meyer-
Palmer, 1993)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.Intervention strategies

26
Breast feeding: - according to needs and strength of an infant- positive oral experience- benefits: prolonged sleep, better transition, weight gain
Skin to skin care: - during gavage feeding for positive associations w/ feedings
Light/Noise
Miminize moving infant w/ limited energy before feeding (Ross, 2003)
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.Intervention strategies
27
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture. Specific Intervention strategies
For the disorganized feeder w/ reflexive suck < 3months
Feeding: - maintenance of respiration- timing of nipple presentation- consistent regulation of suck/swallow/breathe
Environment: - midline position - holding - environmental sensory input - promoting rhythmic sucking
- grading of intra-oral sensation
For the dysfunctional feeder w/ reflexive suck < 3months
- jaw support- cheek support- peri-oral stimulation- facilitation of central tongue groove
(Palmer, 2001)

28
From the NICU to home:
- Date of discharge impacts cost of care and infant-family relationship.- Identified challenges by parents (Thoyre, 2001):
Safety during feedingDetermine adequate calorie intakeWhen to advance feeding plans
- Observations of the nurse- Educate about and help to recognize the stability or stress behaviors- Intervention strategies contingent upon an infant’s cues to help their baby feed - Nurse observes and monitors the infant and the parents during non-feeding and then feeding tasks (bottle/breast)- Team approach
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture. Family support

29
QuickTime™ and aTIFF (Uncompressed) decompressorare needed to see this picture.
-Transition to home:
- Weight gain (LBW= Avg. 35gm/day; ELBW= Avg. 18.7gm/day)(Deloian, 1999)
-Charting to help parents (e.g. feeding schedules, calorie intake, , or plateau of self-regulation skills, new cues/symptoms, etc.)
- F/U with family
- Referral to early intervention &/or related medical and rehab. clinics if needed and if emergence of disabilities observed

30
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.