1 overview of scientific issues j. craig rowlands, ph.d. nutrition programs and labeling staff...
TRANSCRIPT

1
Overview of Scientific Issues
J. Craig Rowlands, Ph.D.Nutrition Programs and Labeling Staff
Center for Food Safety and Applied Nutrition

2
Overview of Scientific Issues
Background Summary of Scientific Evidence Submitted Petitioners’ Conclusions FDA’s Evaluation of the Evidence Questions Meeting Objectives

3
Petitioners
Weider Nutrition International, Inc. (petitioner A)
Rotta Pharmaceutical, Inc. (petitioner B)

4
Weider Nutrition International, Inc. (petitioner A)
Glucosamine may reduce the risk of: Osteoarthritis Joint degeneration Cartilage deterioration
Chondroitin sulfate may reduce the risk of: Osteoarthritis Joint degeneration Cartilage deterioration
Glucosamine and chondroitin sulfate may reduce the risk of:
Osteoarthritis Joint degeneration Cartilage deterioration

5
Rotta Pharmaceutical, Inc. (petitioner B)
Crystalline glucosamine sulfate may reduce the risk of osteoarthritis

6
Health Claims
Health claims are about a substance –disease relationship Risk reduction in healthy populations, NOT Disease treatment or mitigation (i.e.,
drugs)

7
Substance(s)
Glucosamine Glycoprotein, endogenous substance Derived from marine exoskeletons or produced
synthetically Sold as the sulfate sodium chloride (sulfate) salt,
hydrochloride (HCL) salt and N-acetyl-glucosamine
Chondroitin sulfate Glucosaminoglycans (GAGs), large molecule made
of glucuronic acid and galactosamine Manufactured from natural sources, such as shark
and bovine cartilage

8
Disease
Osteoarthritis (Stedman's Medical Dictionary 27th Edition) Arthritis characterized by erosion of articular
cartilage, either primary or secondary to trauma or other conditions, which becomes soft, frayed, and thinned with eburnation* of subchondral bone and outgrowths of marginal osteophytes
*Eburnation=A change in exposed subchondral bone in degenerative joint diseasein which it is converted into a dense substance with a smooth surface like ivory.

9
Osteoarthritis
Risk Factors Genetic predisposition, trauma,
anatomic/postural abnormalities, obesity
No biomarkers that are valid modifiable risk factors/surrogate endpoints for OA Osteoarthritis Initiative (NIH) Biochemical Markers (e,g., cartilage or bone
metabolism)

10
Scientific Evidence
Scientific evidence summarized in petitions included: In vitro mechanistic studies Animal studies Human clinical studies in OA patients

11
In Vitro Mechanistic Data
Human and animal primary cell cultures, established cell culture models and tissue/organ cultures
Glucosamine and/or chondroitin sulfate reported to affect Inflammation Cartilage degradation Immune responses Production of proteoglycans

12
Animal Studies
Glucosamine Reduce kaolin- and adjuvant-induced tibio-tarsal
arthritis in rats Reduce cartilage degradation in rabbits
(±chondroitin sulfate) Enhance the rate of new articular cartilage
proteoglycan synthesis in mice
Chondroitin sulfate Prevent articular cartilage degradation induced
by: Chymopapain in rabbits Freund’s adjuvant in mice Surgery in rabbits
13
Human Clinical Studies
In OA patients, glucosamine and chondroitin sulfate Reported to improve symptoms of pain and
functionality Compared with the non-steroidal anti-inflammatory
drugs (NSAIDs)
Reported to improve joint degeneration and cartilage deterioration
Radiographic evidence: joint space narrowing Biochemical evidence: synovium, serum, urine:
bone/cartilage metabolism

14
Petitioners’ Conclusions
Human clinical intervention studies in OA patients support OA risk reduction in healthy populations
Joint degeneration and cartilage deterioration are valid modifiable risk factors/surrogate endpoints for OA
Animal and in vitro models of OA are relevant to OA risk reduction in humans

15
FDA’s Evaluation of the Evidence
Several issues identified Relevance of OA treatment studies to OA risk
reduction in healthy populations
Validity of joint degeneration and cartilage deterioration as modifiable risk factors/surrogate endpoints for OA
Relevance of animal and in vitro models of OA to humans

16
Disease Risk Reduction
Reduction in incidence of disease Intervention and observational studies
in healthy people demonstrating that a substance reduces the incidence of OA

17
Human Studies in Petitions
ALL of the human clinical intervention studies were conducted in OA patients
NO intervention or observational studies in healthy people demonstrating OA risk reduction

18
Disease Risk Reduction
Beneficial changes in valid modifiable risk factor/surrogate endpoint for disease Intervention and observational studies in
healthy humans demonstrating that intake of a substance produces beneficial changes in valid modifiable risk factors/surrogate endpoints for OA

19
Valid Modifiable Risk Factors/Surrogate Endpoints
A valid modifiable risk factor/surrogate endpoint for disease meets ALL 3 of the following conditions:
Associated with disease Mediates the relationship between intake in healthy people
and disease Expression is modified by intake of a substance in healthy
people
Diseaseor HealthRelated
Condition
HealthyPeopleSubstance
Walnuts LDL-Cholesterol CHD
12
ValidModifiable
Risk Factors/Surr. Endpts

20
Valid Modifiable Risk Factors/Surrogate Endpoints for OA?
Are joint degeneration and cartilage deterioration associated with OA? Yes, associated with OA
OAPatients
HealthyPeople
Joint degenerationCartilage deterioration
12
ValidModifiable
Risk Factors/Surr. Endpts

21
Does joint degeneration and cartilage deterioration mediate the relationship between intake of a substance in healthy people and OA?
Is there evidence that changes in joint degeneration or cartilage deterioration predict clinical outcome for OA?
No intervention studies with ANY substance in healthy individuals that measured BOTH joint degeneration or cartilage deterioration AND OA incidence
OAPatients
HealthyPeople
?OA
PatientsHealthyPeople
Substance
12
Valid Modifiable Risk Factors/Surrogate Endpoints for OA?
ValidModifiable
Risk Factors/Surr. Endpts

22
Are joint degeneration and cartilage deterioration modified by intake of a substance in healthy people? ALL of the evidence provided was in OA patients
OAPatients
HealthyPeople
Substance
?12
Valid Modifiable Risk Factors/Surrogate Endpoints for OA?
ValidModifiable
Risk Factors/Surr. Endpts
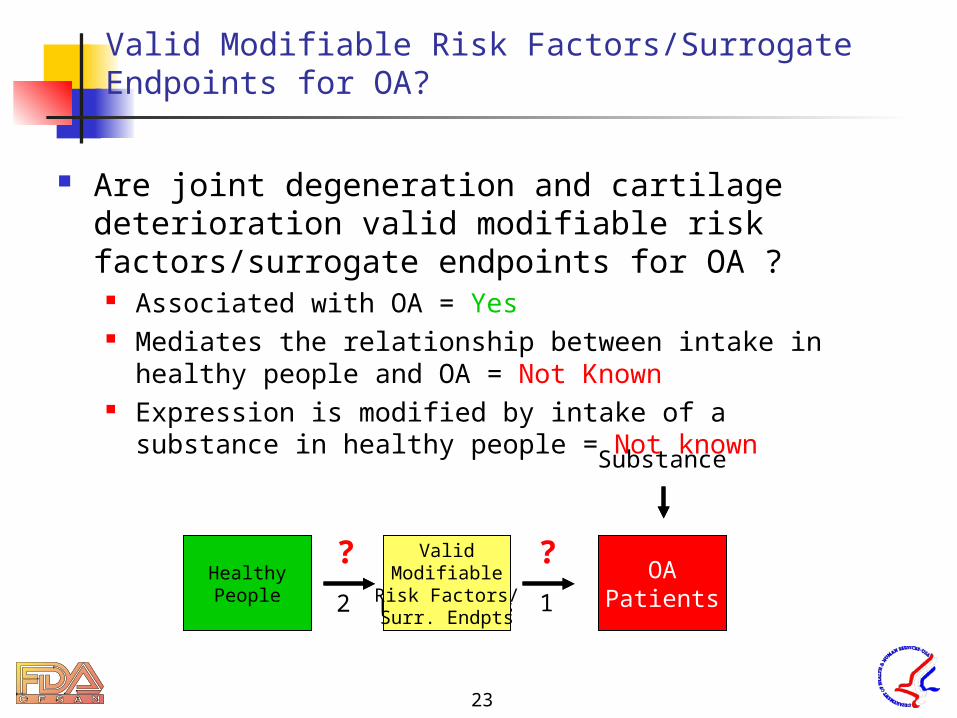
23
Are joint degeneration and cartilage deterioration valid modifiable risk factors/surrogate endpoints for OA ?
Associated with OA = Yes Mediates the relationship between intake in healthy
people and OA = Not Known Expression is modified by intake of a substance in
healthy people = Not known
OAPatients
ValidatedModifiable
Risk Factors
HealthyPeople
?OA
Patients
ValidModifiable
Risk Factors/Surr. Endpts
HealthyPeople
?
Substance
12
Valid Modifiable Risk Factors/Surrogate Endpoints for OA?

24
Animal and in vitro models of OA
Do animal and in vitro models of OA mimic human OA? Animals have a different physiology In vitro models are conducted in an artificial
environment Etiology of OA in humans is poorly understood
Example: non-steroidal anti-inflammatory drugs (NSAIDs) inhibit OA in rodents but not humans*
*Otterness, I.G., Larsen, D., and Lombardino, J.G. An analysis of piroxicam in rodent models of arthritis. Agents Actions 1982; 12:308-312.

25
Questions
Is: (1a) joint degeneration; (1b) cartilage deterioration, a state of health leading to disease, i.e., a modifiable risk factor/surrogate endpoint for OA risk reduction? What are the strengths and limitations of the scientific evidence on this issue ?
Are joint degeneration and cartilage deterioration valid modifiable risk factors/ surrogate endpoints for OA?

26
Questions
If we assume that: (2a) joint degeneration; (2b) cartilage deterioration, is a modifiable risk factor/surrogate endpoint for OA risk reduction and we assume that research demonstrates that a dietary substance treats, mitigates or slows joint degeneration in patients diagnosed with OA, is it scientifically valid to use such research to suggest a reduced risk of OA in the general healthy population (i.e., individuals without OA) from consumption of the dietary substance ?
Is it scientifically valid to use human OA treatment studies to suggest a reduced risk of OA in the general healthy population?

27
Questions
(3) If human data are absent, can the results from animal and in vitro models of OA demonstrate risk reduction of OA in humans?
(a) To the extent that animal or in vitro models of OA may be useful, what animal models, types of evidence, and endpoints should be used to assess risk reduction of OA in humans?
(b) If limited human data are available, what data should be based on human studies and what data could be based on animal and in vitro studies to determine whether the overall data are useful in assessing a reduced risk of OA in humans?
Are the results from animal and in vitro models of OA relevant for demonstrating OA risk reduction in humans?

28
Meeting Objectives
About the science needed to demonstrate risk reduction NOT disease treatment or mitigation
About osteoarthritis NOT glucosamine and chondroitin sulfate
Etiology of OA Valid modifiable risk factors/surrogate endpoints for OA Relevant models of OA
Recommendation of FAC can apply to other substance–OA relationships