1 practical aspects of assessing msi status: what tests to order and how to interpret them by henry...
TRANSCRIPT

1
PRACTICAL ASPECTS OF ASSESSING MSI STATUS: WHAT TESTS TO ORDER AND HOW TO
INTERPRET THEMby
HENRY T. LYNCH, M.D.JANE F. LYNCH, B.S.N.
CARRIE SNYDER, R.N, M.S.N.Creighton UniversitySchool of MedicineOmaha, Nebraska

2
Magnitude of the ProblemAnnual worldwide incidence of CRC is 1,023,152*:
• Lynch syndrome (LS) accounts for 2-5% (20,460-51,160 cases).
• < 1% (10,230 cases) constitute FAP.
• 20% (204,630 cases) are familial (2 or more first- degree relatives with CRC.
*International Agency for Research on Cancer. Globocan 2002. Available at: http://www-dep.iarc.fr/.

3
Magnitude of the Problem
Question: Why are these figures of such significant public health impact?
Answer: Each hereditary cancer comes from a family that could benefit immensely from genetic counseling.
DNA testing, surveillance, and highly-targeted management are the key!
4
J Clin Oncol25:3534-3542, 2007.

5
Who Should Be Tested?1. Pedigree consistent with hereditary colorectal cancer (CRC) syndrome;
2. Known germline mutation predisposing to
cancer;
3. Patients at acceptable high cancer risk status;
4. Presence of cancer syndrome stigmata (phenotype): e.g., polyposis in FAP;
5. Genetic counseling, risks/benefits understood;
6. Consent given;
7. Results: full explanation of surveillance/management advice.

6
Who Should Be Tested?Referral to medical geneticist/center of hereditary cancer expertise:
1. When physician lacks expertise, referral should be made to a cancer genetics center.
2. Key medical/genetic/genealogic findings made available to referral center.
3. Patient/family acceptance.
4. Candidate for DNA testing accepts, is tested, and results are fully explained in genetic counseling setting.

7
Could this behereditary
Colon Cancer

8
HETEROGENEITY
LYNCH SYNDROME

9
Cardinal Features of Lynch Syndrome• Family pedigree shows autosomal dominant inheritance pattern for syndrome cancers.
• Earlier average age of CRC onset than in the general population: - Lynch syndrome: 45 years;- general population: 63 years.
• Accelerated carcinogenesis, i.e., shorter time for a tiny adenoma to develop into a carcinoma:
- Lynch syndrome: 2-3 years;- general population: 8-10 years.
• High risk of additional CRCs:25-30% of patients who have surgery for a LS-associated CRC will have asecond primary CRC within 10 years, if surgery was < a subtotal colectomy.
• Increased risk for certain extracolonic malignancies:
- endometrium (40-60% lifetime risk for ♀ carriers); - ovary (12% lifetime risk for ♀ carriers); - stomach (higher risk in families from Orient); - small bowel;

10
Cardinal Features of Lynch Syndrome• Increased risk for certain extracolonic malignancies (continued):
- hepatobiliary tract;
- pancreas;- upper uroepithelial tract (transitional cell carcinoma of the ureter and renal
pelvis);
- brain (in Turcot’s syndrome variant of LS);- sebaceous adenomas, sebaceous carcinomas, multiple keratoacanthomas
(in Muir-Torre syndrome variant of LS).
• Differentiating pathology features of LS CRCs:
- more often poorly differentiated;
- excess of mucoid and signet-cell features;
- Crohn’s-like reaction;
- significant excess of infiltrating lymphocytes within the tumor.
• Increased survival from CRC.
• Sine qua non for diagnosis is identification of germline mutation in MMR gene (most commonly MLH1, MSH2, MSH6) segregating in the family.

11
Sporadic
Lynch Syndrome
Familial
Hereditary
FAP; AFAPMixed Polyposis SyndromeAshkenazi I1307KCHEK2 (HBCC)MYHTGFBR1
PJSFJPCDBRRS
= as yet undiscovered hereditary cancer variants
HamartomatousPolyposisSyndromes
AC-1 without MMR(Familial CRC of syndrome “X”)

12
Genetic Heterogeneity in HNPCC
HNPCC is associated with germline HNPCC is associated with germline mutations in any one of at least five genesmutations in any one of at least five genes
Chr 2Chr 2Chr 3Chr 3
Chr 7Chr 7
MSH2MSH2
PMS1PMS1
MLH1MLH1PMS2PMS2
MSH6MSH6

13
Lynch Syndrome: Genotypic Heterogeneity
Clinical cancer phenotypes differ with each of the MMR mutations:
1. MSH2 has extracolonic cancer types and Muir-Torre syndrome
2. MLH1 may have CRC expression.
3. MSH6 may be more “benign” with CRC but endometrial cancer.
14
PMS2 Mutations, Phenotype, and Penetrance*
PMS2 mutations contribute significantly to LS.
Penetrance for monoallelic mutation carriers appears to be lower than that for other MMR genes.
*Senter et al. Gastroenterology135:419-428,2008.
15

16
Valle et al. Science 321:1361-1365, 2008.

17
Expression of TGFBR1 in CRC
Valle et al.* hypothesize that TGFBR1 is a notable candidate for a gene that, when mutated, causes predisposition to CRC.
It also acts as a modifier of other genes, resulting in a predisposition.
*Science 321:1361-1365, 2008

18
Molecular Genetics and Lynch Syndrome
15% of all CRCs show MSI: Most not caused by Lynch syndrome.
Acquired silencing (epigenetic inactivation)
of MLH1 gene by methylation of promoter.
Immunohistochemistry (IHC) useful for
identifying protein loss (MSH2, MLH1).
19
Molecular Diagnosis of LS: Toward a Consensus
If tumor is MSI-positive, IHC is then done to direct mutational testing to a specific MMR gene, which MSI alone cannot do.*
If tumor is MSS, must weigh low probability of an informative IHC test and cost of performing it.**
*Engel et al. Int J Cancer 118:115-122, 2006.
**Lynch et al. J Natl Cancer Inst 99:261-263, 2007.
20
Molecular Diagnosis of LS: Toward a Consensus
MSI alone should not be used as a sole basis for selecting patients for mutational testing for LS given the modest but real fraction of patients with MSI-negative tumors in which mutations were found.
**Lynch et al. J Natl Cancer Inst 99:261-263, 2007.

21
BRAF V600E mutation and LS
BRAF V600E mutation can sort this out since when detected it excludes LS and contributes to improved cost-effectiveness of genetic testing for LS.
*Clin Gastroenterol Hepatol 6:206-214, 2008.

22
Clinical Relevance of MMR Deficiency*
Methods to identify MMR-deficient CRC in LS:
1) MSI;
2) IHC;
3) MLH1 promoter hypermethylation testing;
4) germline mutation analysis.
*Pal et al. Cancer 113:733-742, 2008.
23
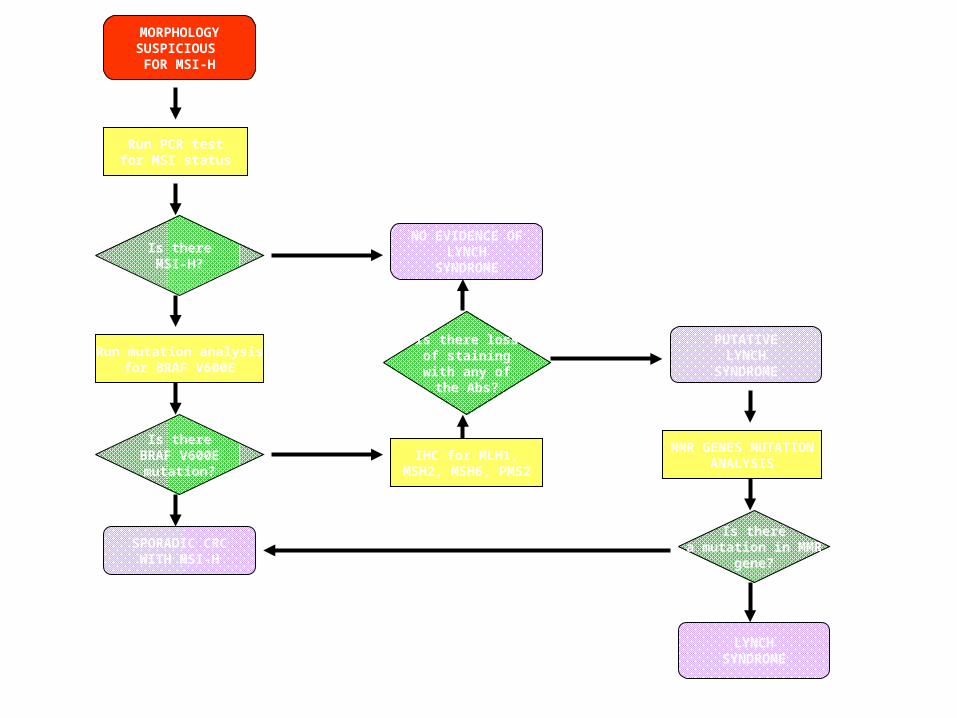
MORPHOLOGYSUSPICIOUS
FOR MSI-H
Run PCR testfor MSI status
Is thereMSI-H?
Run mutation analysisfor BRAF V600E
Is thereBRAF V600E
mutation?
SPORADIC CRCWITH MSI-H
NO EVIDENCE OFLYNCH
SYNDROME
Is there lossof stainingwith any ofthe Abs?
IHC for MLH1,MSH2, MSH6, PMS2
PUTATIVELYNCH
SYNDROME
MMR GENES MUTATIONANALYSIS
Is therea mutation in MMR
gene?
LYNCHSYNDROME
YES
YES
NO
NO
NO
YES
YES
NO
Gatalica Z, Torlakovic E. Fam Cancer 2008;7:15-26

24Lynch syndrome (LS) and Mismatch Repair (MMR) Genes:
What Are the Risks?
A new era for genetic counseling evolved thanks to the cloning of MSH2, MLH1 and MSH6.
Prior to MMR mutation discovery we had to rely solely on an individual’s family history.
Now we can determine lifetime risks for CRC and extra colonic cancers by MMR testing.
25
Do Molecular Genetic Changes in CRC Impact Treatment?

26
Early Evidence of 5-FU Resistence in Lynch Syndrome
Carethers et al.* developed paradigms showing MMR proficiency and the in vitro response to 5-FU.
*J Clin Invest 98:199-206, 1996.
Gastroenterology 117:123-131, 1999.
Gastroenterology 126:394-401, 2004.

27
Efficacy of 5-FU Adjuvant Chemotherapy and MMR Status
These investigators* studied the survival influence of 5-FU in patients with MSI-H tumors.
Results:
Their findings showed that there is improved survival in patients with non-MSI-H tumors after 5-FU-based chemotherapy that does not extend to patients with MSI-H. The MSI status of a patient’s CRC may indicate differences in 5-FU-based chemotherapy.
These findings are consistent with in vitro studies
*Carethers et al. Gastroenterology 126:394-401, 2004.

28
Efficacy of 5-FU Adjuvant Chemotherapy and MMR Status
Ribic et al.* investigated 5-FU-based chemotherapy which benefited patients with stage II and stage III CRC.
They note that CRCs with MSI-H have clinical and pathologic features that distinguish them from MSS tumors. They investigated the usefulness of MSI status as a predictor of the benefit of adjuvant chemotherapy with 5-FU in stage II and stage III CRC.
*N Engl J Med 349:247-257, 2003.

29
Efficacy of 5-FU Adjuvant Chemotherapy and MMR Status
Their study* showed that of 570 tissue specimens, 95 (16.7%) showed MSI-H.
Among 287 patients who did not receive adjuvant chemotherapy, those with MSI-H tumors had a better 5-year rate of overall survival than patients with MSS or MSI-L tumors (hazard ratio for death, 0.31, 95% CI: 0.14-0.72; p = 0.04).
*Ribic et al. N Engl J Med 349:247-257, 2003.

30
K-Ras Mutation in CRC*
Recent clinical data showed that the efficacy of cetuximab and panitumumab is confined to patients whose tumors have K-ras wild-type.
Conclusion:
K-ras mutation analysis considered a new standard of care in the selection of patients for epidermal growth factor receptor (EFGR)-targeted therapy.
*Ramos & Caturla. Cancer & Chemotherapy Reviews 3:194-203, 2008.
31
MSI Status as a Predictor of Benefit from 5-FU-based Adjuvant Chemotherapy in CRC
Conclusion:
5-FU-based adjuvant chemotherapy benefitted patients with stage II or III CRC with microsatellite stable (MSS) tumors, tumors with low MSI frequency (MSI-L), but not MSI-H tumors.
*N Engl J Med 349:247-257, 2003.

32
Genetic Testing and Cancer Control in Lynch Syndrome
The Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group* constructed a chain of evidence linking genetic testing for LS in patients with newly dx CRC with improved health outcomes in their relatives.
Does it work?
*Genet Med 11:35-41, 2009.

33 Evaluation of Genomic Applications in Practice and
Prevention (EGAPP) of Lynch Syndrome*
Testing of all individuals with newly diagnosed CRC proposed as a strategy to reduce CRC morbidity and mortality in relatives of Lynch syndrome (LS) affected.
Assessing patients who have newly Dx CRC with a series of genetic tests (MSI, IHC, MMR) could lead to the identification of LS. Relatives of patients with LS could then be offered genetic testing.
*Genetics in Medicine 11:35-41, 2009.

34
Genetic Testing and Cancer Control in Lynch Syndrome*
Testing of newly dx (with CRC) proband with a series of genetic tests could lead to the identification of LS.
Relatives of proband with LS could then be offered genetic testing and where indicated CRC and endometrial cancer (EC) surveillance with expectation of improved health outcome.
*EGAPP Working Group. Genet Med 11:35-41, 2009.

35
Genetic Testing and Cancer Control in Lynch Syndrome
Clinical Validity:
Accounting for specific technologies and numbers of markers used, the EWG identified adequate evidence to describe the clinical sensitivity and specificity of selected testing strategies:
Most cost effective approach for LS screening is MSI testing for all CRC, followed by MMR (MSH2 and MLH1) testing when CRC is found to be MSI-H.
*EGAPP Working Group. Genet Med 11:35-41, 2009.

36
Genetic Testing and Cancer Control in Lynch Syndrome*
Screening for MSI is cost effective for patients with newly dx CRC, because mutation identification in MSI-H cases offers an opportunity to provide predictive testing for at-risk relatives. .
Such testing enables targeted management for mutation carriers, with population level screening measures for non-carriers.
*EGAPP Working Group. Genet Med 11:35-41, 2009.

37 Evaluation of Genomic Applications in Practice and
Prevention (EGAPP) of Lynch Syndrome*
Conclusion:
E W G concluded that there was moderate certainty that such a testing strategy would provide moderate population benefit.
*Genetics in Medicine 11:35-41, 2009.

38
Biochemical Basis of MSI*
Boland et al. state that the dx of LS is becoming more complex as more and more is learned about the disease; one, therefore, needs to understand how the DNA MMR proteins function and what makes them malfunction to arrive at an optimal appreciation of how to interpret diagnostic studies such as MSI and IHC of the DNA MMR proteins.
*Boland et al. Fam Cancer 7:41-52, 2008.
39
Biochemical Basis of MSI*
Conclusion:
Understanding the role of DNA MMR system in regulation of the cell cycle and the response to DNA damage helps illuminate the differences in natural history and response to chemotherapeutic agents seen in LS.
*Boland et al. Fam Cancer 7:41-52, 2008.

40
Family Information Service (FIS)
Cost-effective and highly efficient way of educating and counseling all available family members from a geographic catchment area during a single setting.
Makes best use of physician’s time and effort, has group therapy potential and patients welcome it.

41

42