1 quality improvement series session 6- culture and systems windy stevenson [email protected] cindy...
Post on 19-Dec-2015
214 views
TRANSCRIPT


2
Today’s AgendaToday’s Agenda

3
RecapRecap
Problem: The DCH ambulatory clinic problem lists are incomplete and inaccurate.
Drivers:1. Improve patient care2. Improve provider efficiency (reduce chart review)
Lessons Learned:• We have to narrow our scope• Just saying we fix the system is woefully inadequate• Everything is more complex than we expect• Random audits of an ill defined product are not helpful• We are still limited by our access to data

4
Last time we met…Last time we met…
1. Capture data regarding types of patients or types of problems not well documented in the clinic
2. Explore data capacity to compare the # of patients with asthma on a bill to the # of patients with asthma on a problem list

5
Start somewhere, anywhere…Start somewhere, anywhere…
Institutional or leadership priorities– Clinical– Fiscal
Safety risk Most annoying (therefore most motivation to fix?) Most easily solved Most easily measured Most meaningful to customers
So, Why do we feel stuck???

6
Changing behaviorBy changing motivation By making the right thing
the easy thing
Culture change
Convince every provider that this is important so that he/she REMEMBERS to change behavior
Systems change leading to eventual culture change
Reconfigure the system so it doesn’t matter in the beginning if it is important to providers
This works in a system with immediate feedback
(treats or shock collar)
This works when there is no natural consequence
(fence)
Let’s say your dog keeps running into the street

7
Challenges (ie barriers)Challenges (ie barriers)
Time Culture
– Ownership
Definition of accuracy Lack of natural error identification Lack of natural rewards Need for manual audits

8
Project Focus OptionsProject Focus Options
Asthma ADHD Failed ASQ Obesity
Pros Clinic focusEPIC momentumPublic reporting
Common dxNational focus
Direct clinical impactClear trigger
EPIC momentumEase of IDLess complex than asthma
Cons Triggers less clear than obesity
No EPIC interestIs trigger clear (order for stim?)
No EPIC interest Lack of passion? Downstream impact?

9
Purpose: Capture discrete data during office visit of asthma managementWhere should this show: Rows should display within the visit navigator when an asthma ICD-9 problem is added to the problem list • Does pt have active daytime symptoms ? Y/N• How frequent are daytime symptoms ? < or equal to 2 times/week, > or equal to 2 times per week, daily, always • Does the patient have active nighttime symptoms ? Y/N• How frequent are the nighttime symptoms ? < or equal to 2 times/month, > or equal to 2 times/month, >1 per
week, frequent• What is the asthma classification? Mild intermittent, mild persistent, moderate persistent, severe persistent • Level of control: well controlled, not well controlled, very poorly controlled, not assessed• Today’s ACT Score ________ (free text)• Today’s Track Score ________ (free text)• Asthma action Plan: completed, reviewed, not appropriate• Stepwise approach used to identify treatment option or to adjust therapy based on asthma control? Yes, no• If this patient has persistent mild, moderate or severe asthma have they received prescription for an inhaled
corticosteroid or an acceptable alternative? Y/N• If this patient has persistent mild, moderate or severe asthma and have not received a prescription for an inhaled
corticosteroid or acceptable alternative document reason why.• Influenza vaccine given: yes, no• Influenza recommended but not given due to: contraindicated, too ill, younger than 6 months old patient,
declined by parent/guardian, not available, already had the vaccine for this influenza season• Spirometry completed today ? Yes, No• Hospitalized since last visit ? No, acute care admission, critical care admission• ER encounter since last visit? No Yes
New Docflowsheet Requests for Asthma Metrics

10
Obesity and Meaningful UseObesity and Meaningful Use
The percentage of patients 2‐17 years of age who had an outpatient visit with a PCP and who had evidence of BMI percentile documentation, counseling for nutrition and counseling for physical activity during the measurement year.
11
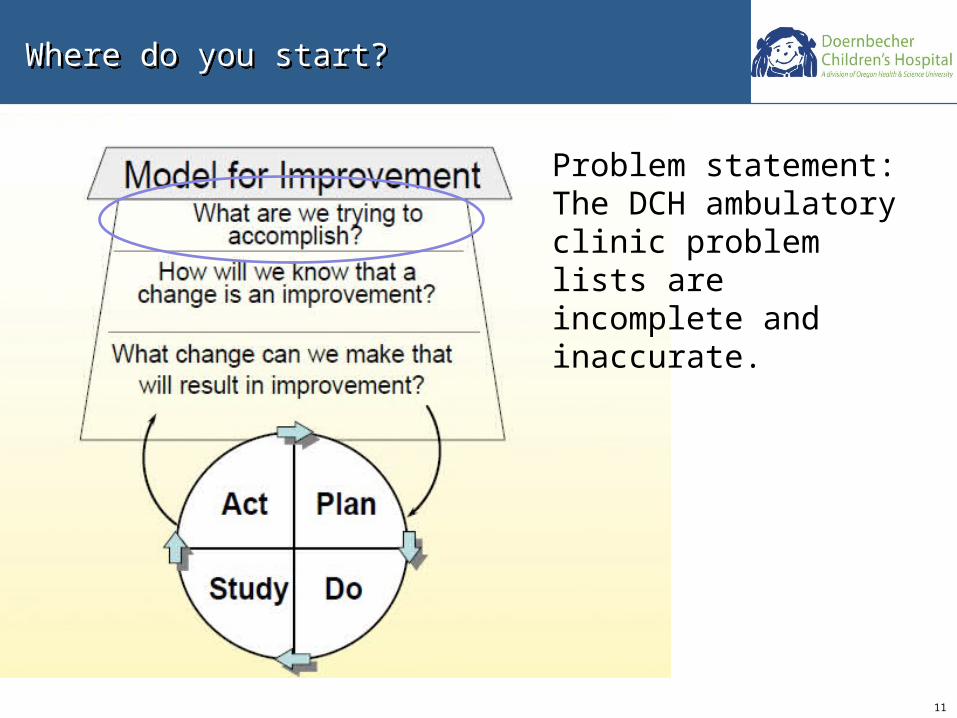
Where do you start? Where do you start?
Problem statement: The DCH ambulatory clinic problem lists are incomplete and inaccurate.

12
How do you create a SMART aim? How do you create a SMART aim?
Specific we are intentional and focused Measurable we can prove we’ve had an impact Actionable there are no known insurmountable barriers Realistic it’s within our scope Timely we’ll do it within a time frame

13
Take Home Points (review)Take Home Points (review)
Real (sustainable) change comes from changing systems, not changing within systems
Be specific about what you want to accomplish, and why; be intentional
Focus on patients
Start before you think you are ready; don’t get paralyzed