10.3 pid - epi
TRANSCRIPT
8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 1/9
PELVICINFLAMMATORY
DISEASE
Fernandez Torres Victor Universidad nacional del centro del peru

8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 2/9
PELVIC INFLAMMATORY DISEASE
infection of the uterus, fallopian tubes, andadjacent pelvic structures that is not associatedwith surgery or pregnancy
8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 3/9
Etiology and Pathogenesis
2 stages of PID:
-acquisition of a vaginal or cervical infection
-direct ascent of micro-organisms from the
vagina and cervix
ORGANISMS MOST COMMONLY ISOLATED :
• Neisseria gonorrhoeae and Chlamydia trachomatis• Gardnerella vaginalis, Mycoplasma hominis, Ureaplasma
urealyticum, herpes simplex virus-2 (HSV-2), Trichomonas
vaginalis, cytomegalovirus, Haemophilus influenzae, Streptococcus
agalactiae

8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 4/9
Risk factors
young age
multiple sexual partners
certain methods of contraception
previous history of chlamydia or another
sexually transmitted infection delayed and decreased access to care
8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 5/9
Symptoms
lower abdominal pain
abnormal vaginal discharge
abnormal uterine bleeding
dysuria dyspareunia
nausea
vomiting
fever
Gonococcal PID - dramatic symptoms of fever and
peritoneal irritation
8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 6/9
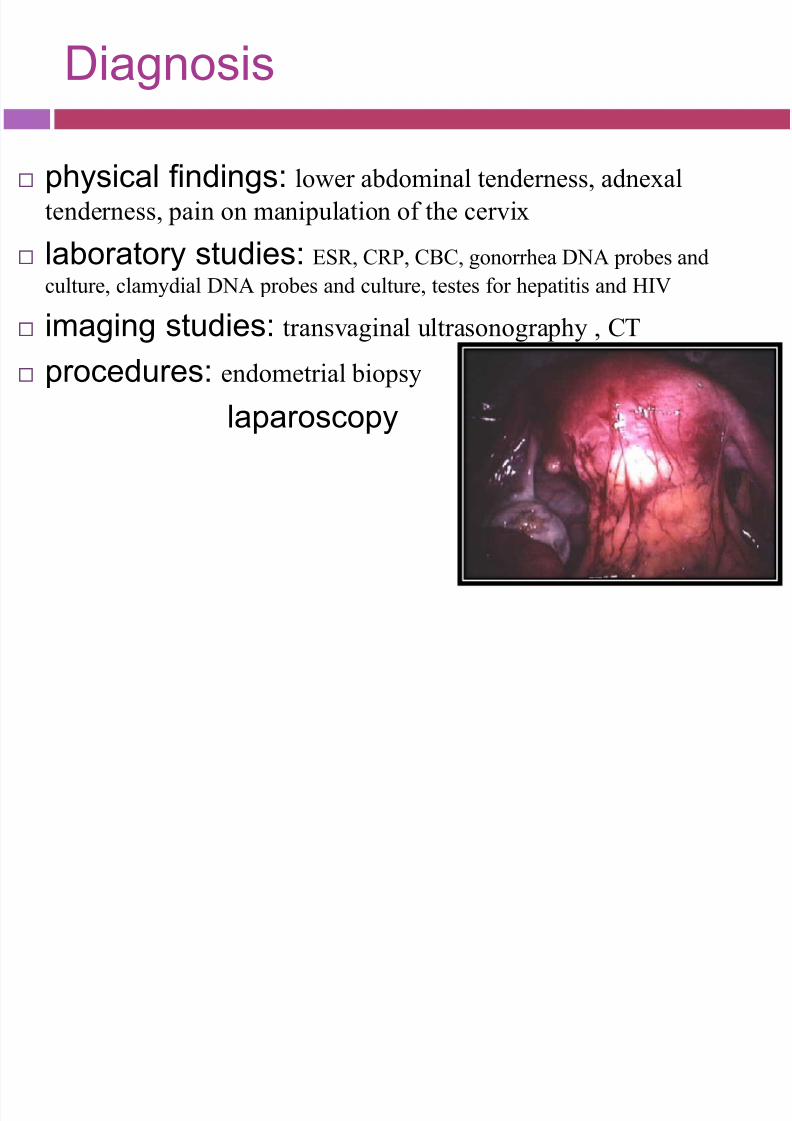
Diagnosis
physical findings: lower abdominal tenderness, adnexal
tenderness, pain on manipulation of the cervix
laboratory studies: ESR, CRP, CBC, gonorrhea DNA probes and
culture, clamydial DNA probes and culture, testes for hepatitis and HIV
imaging studies: transvaginal ultrasonography , CT
procedures: endometrial biopsy
laparoscopy
8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 7/9
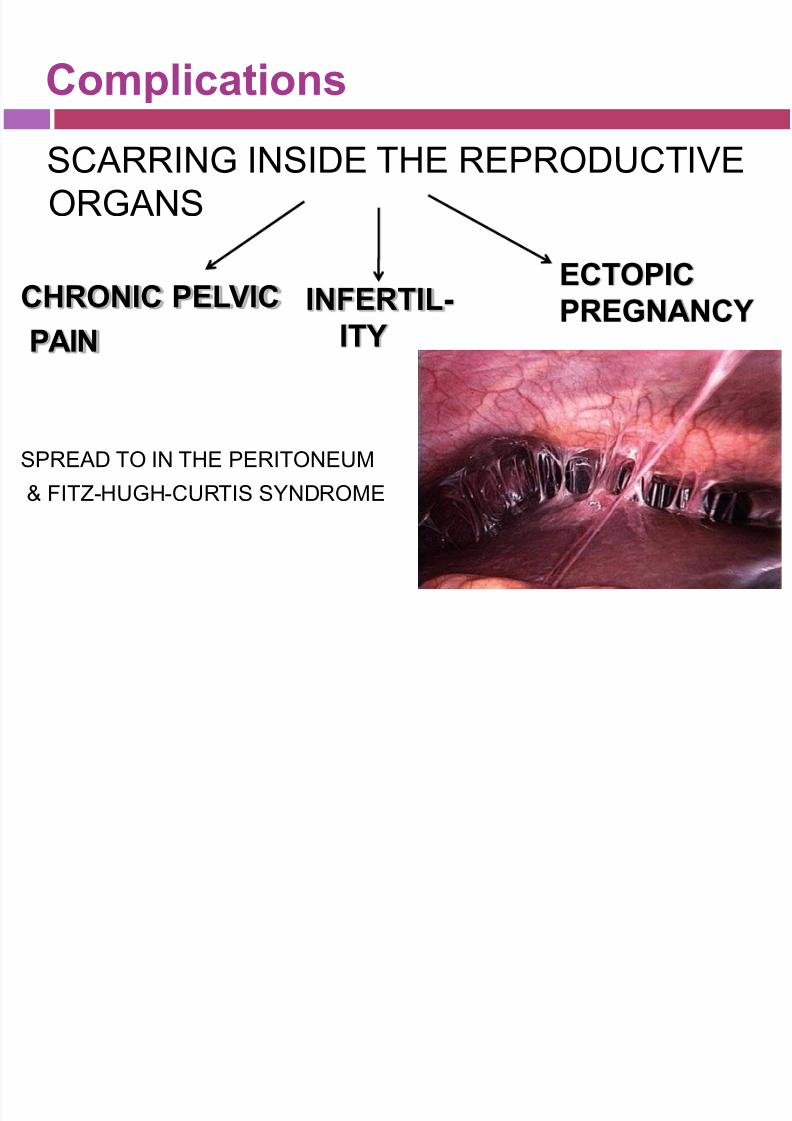
Complications
SCARRING INSIDE THE REPRODUCTIVE
ORGANS
CHRONIC PELVIC
PAIN
SPREAD TO IN THE PERITONEUM
& FITZ-HUGH-CURTIS SYNDROME
INFERTIL-
ITY
ECTOPICPREGNANCY
8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 8/9
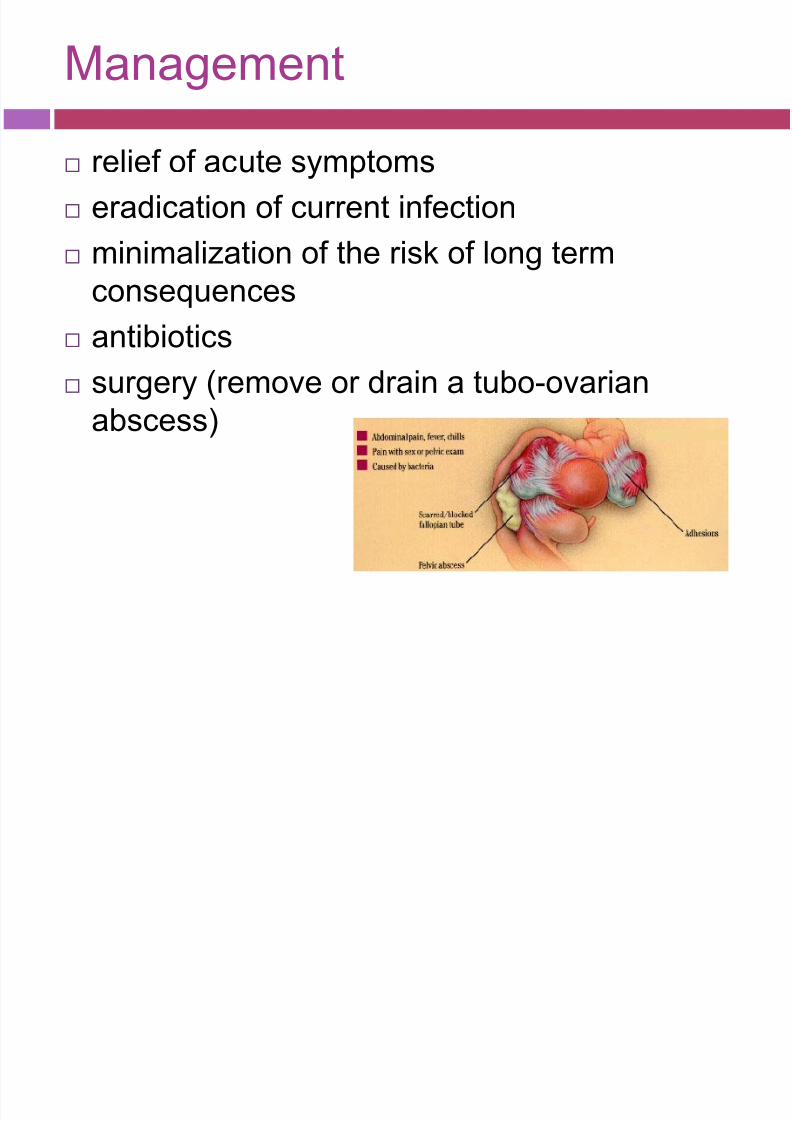
Management
relief of acute symptoms
eradication of current infection
minimalization of the risk of long term
consequences
antibiotics
surgery (remove or drain a tubo-ovarian
abscess)

8/13/2019 10.3 PID - EPI
http://slidepdf.com/reader/full/103-pid-epi 9/9
Antibiotics
Inpatient treatment
Regimen A: Administer cefoxitin 2 g IV q6h orcefotetan 2 g IV q12h plus doxycycline 100 mgPO/IV q12h.. Continue this regimen for 24hours after the patient remains clinicallyimproved, and then start doxycycline 100 mgPO bid for a total of 14 days. Administerdoxycycline PO when possible because of
pain associated with infusion. Bioavailability issimilar with PO and IV administrations. If tubo-ovarian abscess is present, use clindamycin ormetronidazole with doxycycline for moreeffective anaerobic coverage.
Regimen B: Administer clindamycin 900 mg IVq8h plus gentamicin 2 mg/kg loading dose IVfollowed by a maintenance dose of 1.5 mg/kgq8h. IV therapy may be discontinued 24 hours
after the patient improves clinically, and POtherapy of 100 mg bid of doxycycline shouldbe continued for a total of 14 days. If tubo-ovarian abscess is present, use clindamycin ormetronidazole with doxycycline for moreeffective anaerobic coverage.
Outpatient treatmentRegimen A: Administer ceftriaxone 250 mg IM
once as a single dose plus doxycycline 100 mg
PO bid for 14 days, with or without
metronidazole 500 mg PO bid for 14 days.
Metronidazole can be added if there is
evidence or suspicion for vaginitis or
gynecologic instrumentation in the past 2-3weeks.
Regimen B: Administer cefoxitin 2 g IM once
as a single dose and probenecid 1 g PO
concurrently in a single dose or other single
dose parenteral third-generation cephalosporin
(ceftizoxime or cefotaxime) plus doxycycline
100 mg PO bid for 14 days with or without
metronidazole 500 mg PO bid for 14 days.
Metronidazole can be added if there is
evidence or suspicion of vaginitis or
gynecological instrumentation in the past 2-3
weeks.