10#year(outcome(of(lmsten4ng(( (management(of(restenosis · 10#year(outcome(of(lmsten4ng((&...
TRANSCRIPT

10-‐year Outcome of LM Sten4ng &
Management of Restenosis
I Sheiban
Director Interventional Cardiology Pederzoli Hospital
Peshiera del Garda ( Verona ) / Italy
E-mail: [email protected] [email protected]
Background • Unprotected Le1 Main disease is burdened by relevant risk of death and MI
( up to 10-‐15% of pts presenBng both with ACS or stable presentaBon
• CABG has represented the standard of care for these paBents for many years, offering if performed with LIMA gra1s rates of patency up to 90% at ten years, but very inferior if performed with SVG vein gra1s.
• In the last 12 years PCI for LM disease has become widely used offering a feasible alternaBve
• The 5-‐year follow up data from the Syntax trial and others : similar rates of MACE in paBents treated with PCI vs. CABG for ULM leading to significant change in ESC guidelines for paBents with ULM
• EvaluaBon of long term outcome of PCI vs. CABG is mandatory, but no data have been reported from observaBonal registries on 10 year outcome of PCI on ULM .

• DiparBmento di Scienze Mediche, Divisione di Cardiologia, CiWà
della Salute e della Scienza, Turin, Italy, • Pederzoli Hospital , Peschiera del Garda , Italy • Division of Cardiology, Brighton, UK • ScienBfic InsBtute S. Raffaele, Milan, Italy, • Department of Cardiology, InsBtut Cardiovasculaire Paris Stud, • Hôpital Privé Jacques CarBer, Générale de Santé, Massy, France, • Cardiovascular InsBtute, Hospital Clínico San Carlos, Madrid,
Spain; • Servicio de Cardiología, Hospital Marqués de Valdecilla,
Santander, Cantabria, Spain (JDLT) • Divisione di Cardiologia, Ospedale Mauriziano, Turin, • Divisione di Cardiologia , Ospedale Di Rivoli , Tutrin , Italy
326 consecuBve paBents were enrolled in 10 Centers Index Procedure for ULM disease performed prior to 2004 with DES

q All paBents treated with PCI on ULM in our Centers with at least 10 years follow up were enrolled.
Methods
q For each paBent the following data were recorded : • burden of cardiovascular risk factors, indicaBon for PCI,
ejecBon fracBon • site of the lesion (osBal, mid, distal), of kind of technique
for bifurcaBon (provisional vs. two-‐stents strategies), of kind of stent and its diameter
• angiographic features on non-‐ULM stenosis, site of vessel and of lesion
q for a subgroup of paBents Syntax Score was evaluated by two different operators at each center.
• Primary End-‐point Re-‐PCI on ULM at 10 years • Secondary End-‐point MACE (Major Adverse Cardiac Events) and its
single components (cardiac and not cardiac death, myocardial infarcBon, re-‐PCI not on ULM and Stent Thrombosis)
Registry Endpoint
338 consecuBve paBents treated with PCI for LM disease with DES before 2004 10 paBents lost to FU 6 paBents alive , excluded for incomplete clinical data 326 paBents with completed follow Up (96%), included in the Registry 256 paBents without re-‐PTCA on LM ( 79%) 70 paBents with re-‐PTCA on LM ( 21%)
Study PopulaBon

Overall population
(326)
Patients with rePTCA on LM at 10 years (70, 21%)
Patients without rePTCA on LM at 10 years (256, 79%)
P
Age (years) 65±9 66±10 65±9 0.45 Female gender (%) 37 (28) 18 (25) 19 (51) 0.67 Hypertension (%) 231(71) 53 (77) 178 (71) 0.69 Hyperlipidemia (%) 231 (71) 49 (71) 182 (73) 0.83 Diabetes mellitus
- Non insulin dependent
- Insulin dependent
96 (32)
29 (12)
24 (35)
8 (13)
72 (28)
21 (11)
0.44
Smoker habit, both previous and current (%)
128 (39) 26 (37) 102 (43) 0.88
Previous Percutaneous Coronary Intervention (PCI)
103 (31) 22 (32)
81 (33) 0.53
Previous surgical revascularization
102 (38) 28 (41) 74 (29) 0.05
Creatinine at admission (md/dl)
1.11±0.54 1.21±0.82 0.91±0.45 0.07
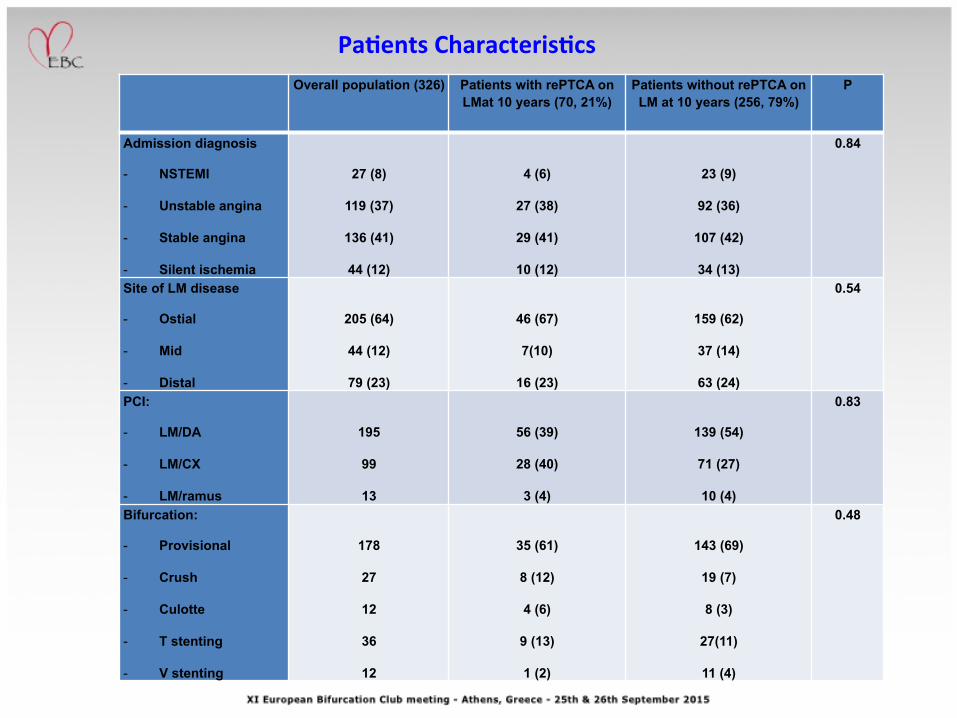
PaBents CharacterisBcs
Overall population (326) Patients with rePTCA on LMat 10 years (70, 21%)
Patients without rePTCA on LM at 10 years (256, 79%)
P
Admission diagnosis
- NSTEMI
- Unstable angina
- Stable angina
- Silent ischemia
27 (8)
119 (37)
136 (41)
44 (12)
4 (6)
27 (38)
29 (41)
10 (12)
23 (9)
92 (36)
107 (42)
34 (13)
0.84
Site of LM disease
- Ostial
- Mid
- Distal
205 (64)
44 (12)
79 (23)
46 (67)
7(10)
16 (23)
159 (62)
37 (14)
63 (24)
0.54
PCI:
- LM/DA
- LM/CX
- LM/ramus
195
99
13
56 (39)
28 (40)
3 (4)
139 (54)
71 (27)
10 (4)
0.83
Bifurcation:
- Provisional
- Crush
- Culotte
- T stenting
- V stenting
178
27
12
36
12
35 (61)
8 (12)
4 (6)
9 (13)
1 (2)
143 (69)
19 (7)
8 (3)
27(11)
11 (4)
0.48
PaBents CharacterisBcs

Temporal trend for rePTCA on LM.
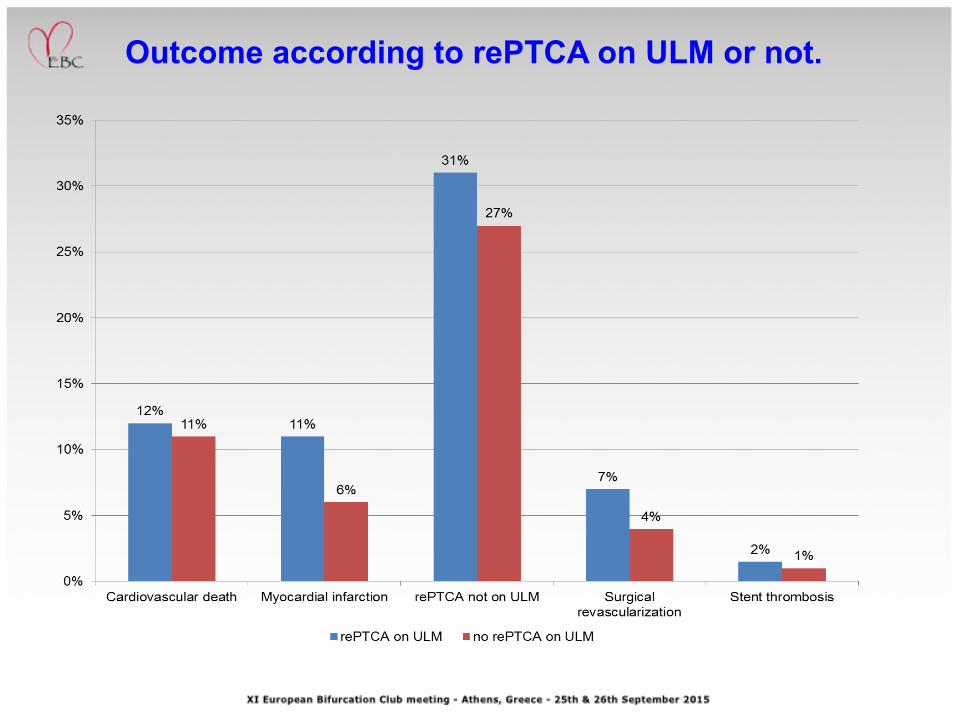
Outcome according to rePTCA on ULM or not.
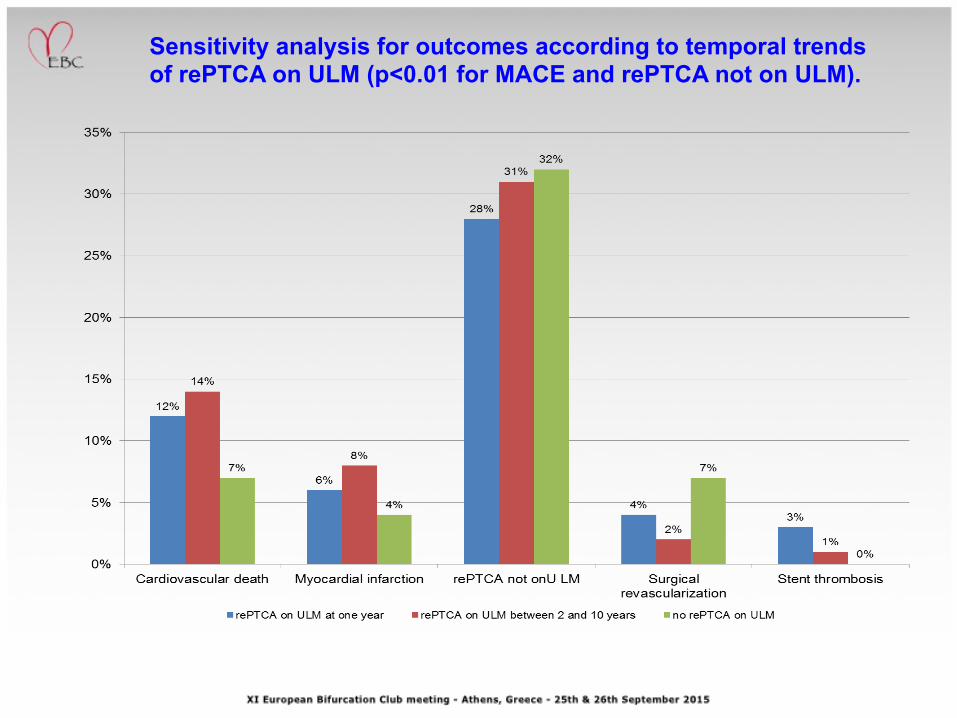
Sensitivity analysis for outcomes according to temporal trends of rePTCA on ULM (p<0.01 for MACE and rePTCA not on ULM).

Freedom from MACE according to isolated (green) vs. not isolated (blu) ULM disease (p for rank <0.01)

Freedom from rePTCA not on left main according to isolated (green) vs. not isolated (blu) ULM disease (p for rank <0.001)
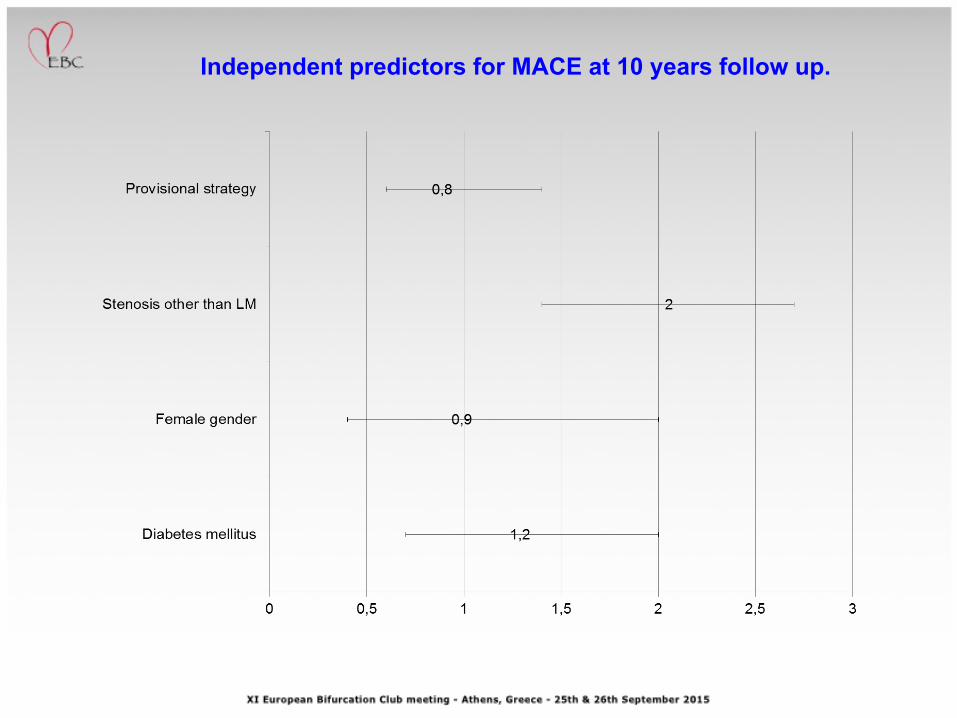
Independent predictors for MACE at 10 years follow up.

Sensitivity analysis for outcomes according to Syntax score (p<0.01 for MACE and rePTCA not on ULM).
What about 2 stents vs. provisional for patients with true bifurcation? Before and after propensity score for type C lesions, lesion of ostial Cx and DA.

Two stents strategy: incidence of acute myocardial infarction and TLR (p not significant)
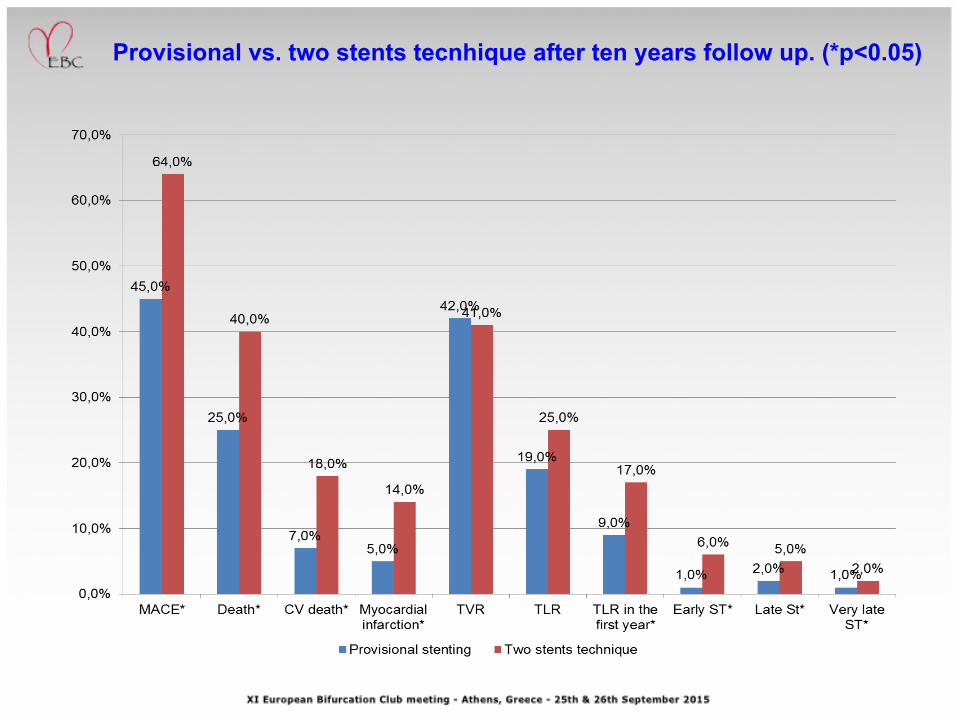
Provisional vs. two stents tecnhique after ten years follow up. (*p<0.05)
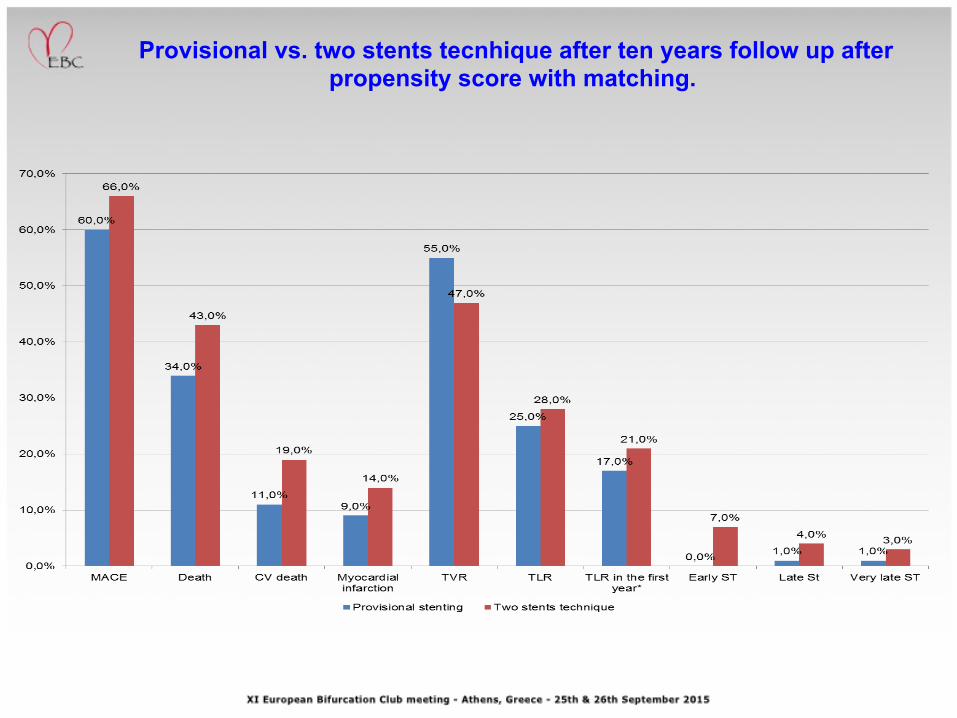
Provisional vs. two stents tecnhique after ten years follow up after propensity score with matching.

Long term freedom from MACE betwenn provisional (green) vs. two stents strategy after propensity matching (p for log-rank 0.67)

Long term freedom from TLR between provisional (green) vs. two stents strategy after propensity matching (p for log-rank 0.67)
Management of In-‐Stent Restenosis
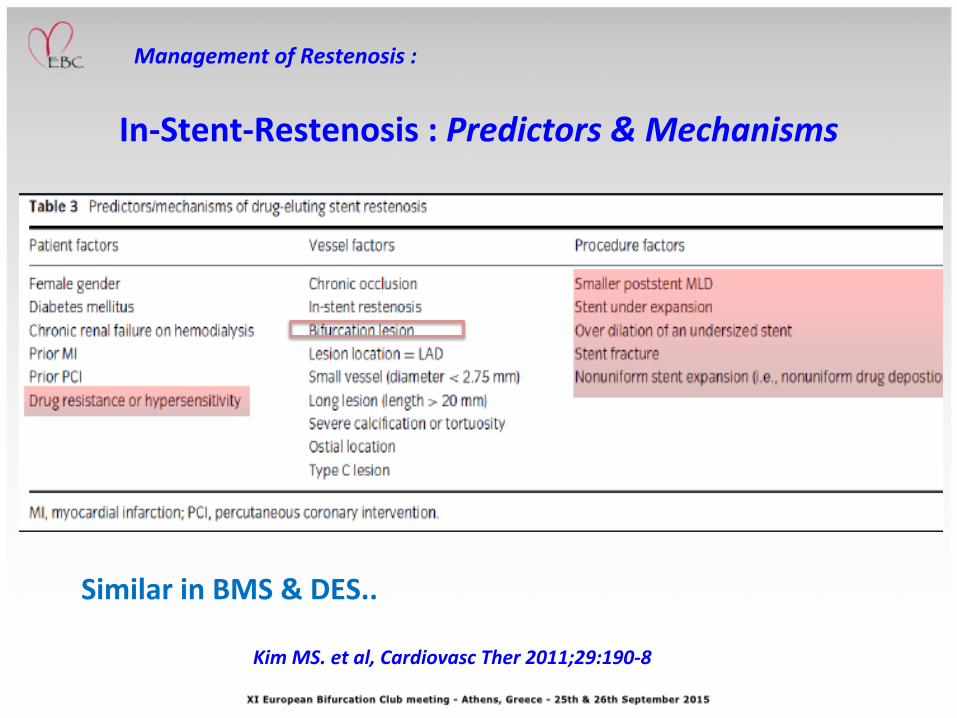
In-‐Stent-‐Restenosis : Predictors & Mechanisms
Kim MS. et al, Cardiovasc Ther 2011;29:190-‐8
Similar in BMS & DES..
Management of Restenosis :

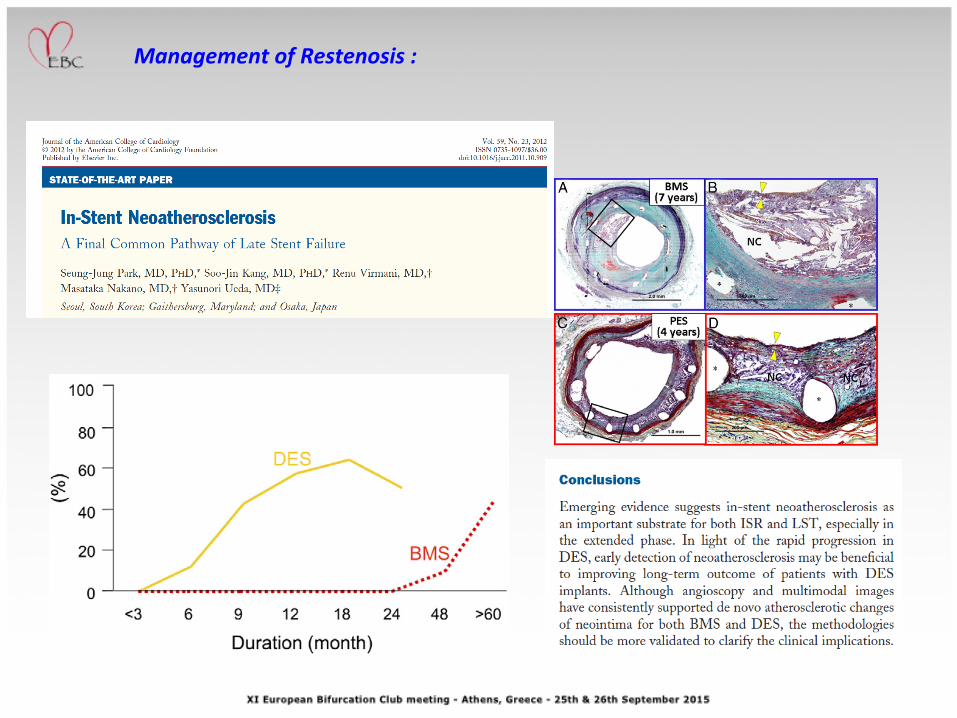
Mechanisms of DES Restenosis
• Biological factors Drug resistance HypersensiBvity Neoatherosclerosis •Mechanical factors Non uniform stent strut distribuBon Stent fractures Polymer peeling Non uniform drug deposiBon
•Technical factors Incomplete stent expansion Stent gaps or “misses” (uncovered lesion segments) Barotrauma to unstented segments
Management of Restenosis :
Management of Restenosis :

Restenosis : Stent underexpansion
Management of Restenosis :
In-‐Stent-‐Restenosis Treatment Op4ons Ø POBA Ø Cuong Balloon Ø Scoring Balloon Ø Laser, RotablaBon Ø DEB Ø DES (same vs. different) Ø VBT Ø CABG
Management of Restenosis :

DES vs. POBA : RIBS II: 150 paBents with BMS-‐restenosis: SES vs. POBA
Alfonso F. et al, JACC 2006;56:2152-‐60
Management of Restenosis :
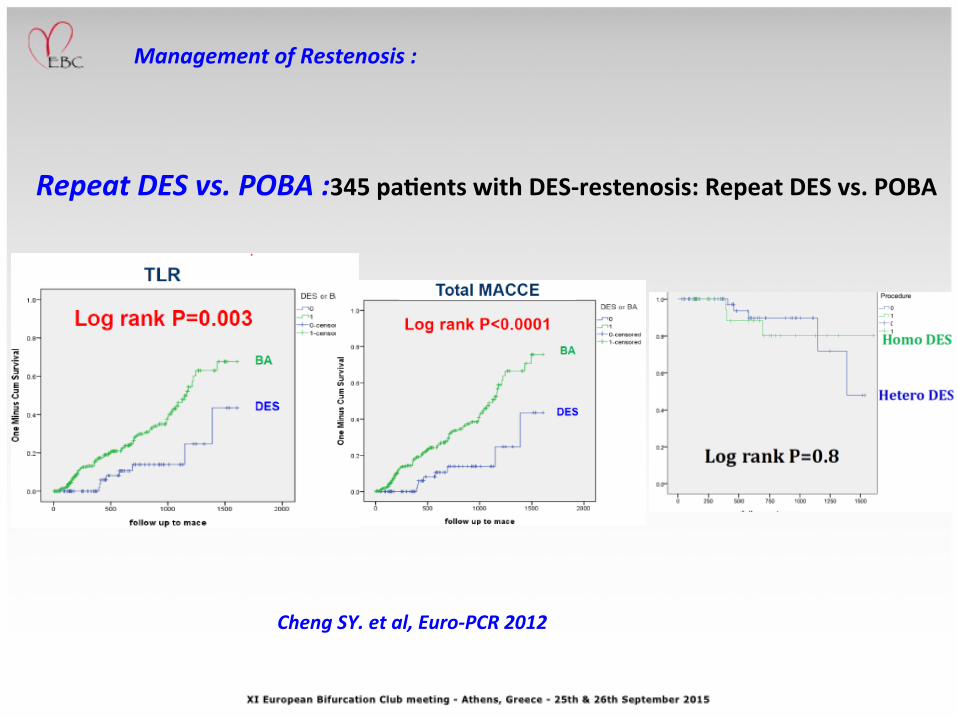
Repeat DES vs. POBA :345 paBents with DES-‐restenosis: Repeat DES vs. POBA
Cheng SY. et al, Euro-‐PCR 2012
Management of Restenosis :
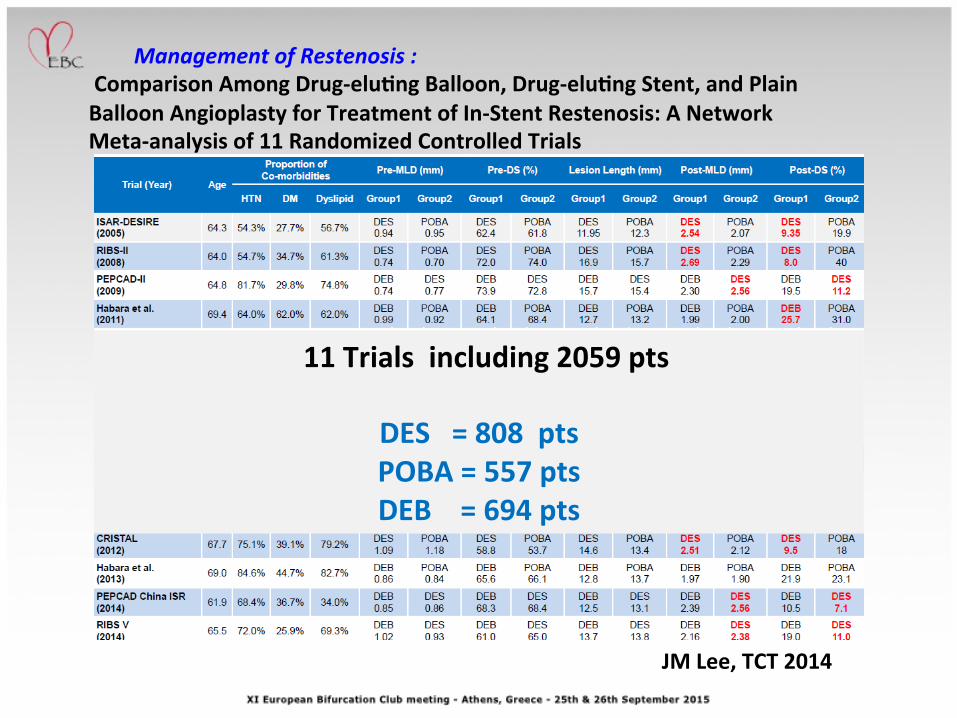
Comparison Among Drug-‐eluBng Balloon, Drug-‐eluBng Stent, and Plain Balloon Angioplasty for Treatment of In-‐Stent Restenosis: A Network Meta-‐analysis of 11 Randomized Controlled Trials
Management of Restenosis :
JM Lee, TCT 2014
11 Trials including 2059 pts
DES = 808 pts POBA = 557 pts DEB = 694 pts

Target Lesions RevascularizaBon
Management of Restenosis :
JM Lee, TCT 2014

MACE
JM Lee, TCT 2014
Management of Restenosis :

In-‐ BVS Restenosis
• Total paBents recieving BVS = 101
• In-‐BVS Restenosis = 6 (6%)
• Managment : • CABG = 1 • DES = 5
Management of Restenosis :
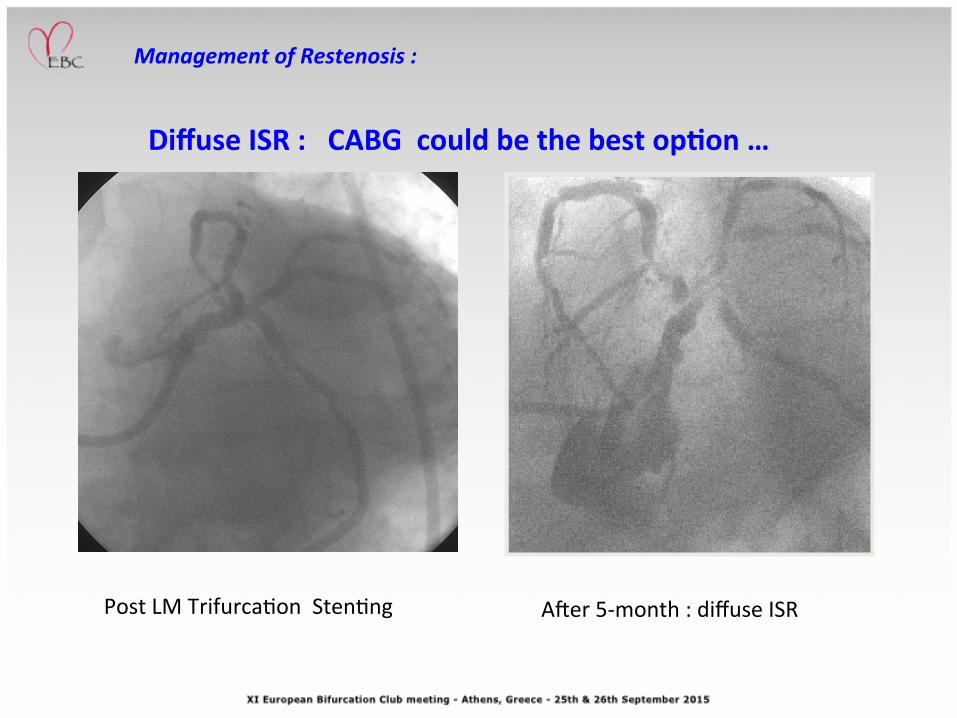
Diffuse ISR : CABG could be the best opBon …
Post LM Trifurca8on Sten8ng A;er 5-‐month : diffuse ISR
Management of Restenosis :


Procedural aspects of PCI : Specific PCI devices
Management of Restenosis :

Ø Despite use of first generaBon stents, PCI on ULM is safe and efficacy is long lasBng over Bme (10 yrs) with low rates of recurrent events due to index-‐revascularizaBon.
Ø Progression of atheroscleroBc lesions on other coronary vessels ( and not LM itself) represents the only independent predicBve factor for prognosis following index procedure .
Ø Despite many limitaBons (observaBonal with mainly a descripBve aim, use of first generaBon stents), the concept of the PCI on ULM and of its feasibility is the most useful finding.
Ø In-‐stent Restenosis , when occurs , can be safely and effecBvely managed with DES and DCB
Final Remarks