11 monday, may 24, 2010 beyond pills: when the most common depression therapies don’t work
Post on 19-Dec-2015
214 views
TRANSCRIPT

11
Monday, May 24, 2010
BEYOND PILLS:
When the Most Common Depression Therapies Don’t Work

Agenda
Is Remission of Depressive Symptoms a Realistic Goal?Linda Carpenter, MDAssociate Professor, Department of Psychiatry and Human Behavior, Brown University; Chief, Mood Disorders Program, Butler Hospital
Understanding How TMS Therapy WorksMark Demitrack, MDPsychiatrist and Chief Medical OfficerNeuronetics, Inc.
View from the Clinic: Finding a Direct Route to Getting Patients WellDemonstration: NeuroStar® Transcranial Magnetic Stimulation Therapy SystemKarl Lanocha, MDThe TMS Center of New EnglandPortsmouth, NH
A Battle on Two Fronts: My Struggle with DepressionCatherine Hogan, depression patient and advocate
Q&A
2

Is Remission ofDepressive Symptoms a Realistic
Goal?
Linda Carpenter, M.D.
3

4
Depression: What We Know
• Nearly 15 million American adults experience a major depressive disorder (MDD) episode in any given year
• More common in women
– 10-12 million women have MDD each year
• Men less likely to seek treatment
– 6 million men each year develop MDD
• No racial, ethnic, or socioeconomic boundaries
– Life events and environmental factors can trigger an episode or prevent recovery
– Similar to heart disease: genes and biology raise underlying risk
Kessler RC, et al. Archives of General Psychiatry. 2005;62(6):617-627.
Mark – we used this picture before – do you have anything else that works?
The Tangled Web of Depression
• Depression is an independent factor impacting a range of medical conditions and increasing risk of death and hospitalization:– All cause mortality1
– Acute stroke2
– Diabetes3
– Myocardial infarction4
– Cardiovascular disease5
– Congestive heart failure6
– HIV7
1. Murphy, JM, et al Arch Gen Psychiatry. 1987. 44(5)473-480; 2. Everson, SA, et. al. Arch Intern Med. 1998; 158(10): 1133-1138; 3. Lustman, PT, et.al. Diabetes Care. 2000: 23(7): 934-942; 4. Frasure-Smith, N, et. al. JAMA. 1993; 270(15): 1819-1825; 5. Penninx, BW, et. al. Arch Gen Psych. 2001; 58(3): 221-227. 6. Vaccarino, V, et. al J. Am Coll Cardiol. 2001; 38(1): 199-205. 7. Ickovics, JR, et. JAMA. 2001: 285(11): 1466-1474.
5

6
The Impact of Depression
• Of the 30,000 people in the U.S. who commit suicide each year, 60 percent have depression
• Increased risk of substance abuse/dependence
• Increased medical co-morbidities
• Strain on interpersonal relationships
• Estimated U.S. economic burden: $83.1 billion in 2000
• World Health Organization reported that MDD is projected to become the second leading cause of disability worldwide by 2020
Carney RM, Freedland KE. Biological Psychiatry. 2003;54(3):241-247.

One Step Forward, One Step Back
• Less stigma & increased awareness by physicians and public
• Antidepressant use has increased steadily in the U.S. in recent years
• Newer medications have fewer severe side effects and better safety profiles – But efficacy continues to be
questioned
• Despite major advances nearly one-third of patients do not experience substantial relief
7

8
The Goals of Treatment
• Acute phase: remission of depression symptoms
– Complete symptom resolution is the goal
• Maintenance phase: Continued response to the treatment over time
– elimination of residual symptoms
– restoration of prior level of functioning
– prevention of recurrence or relapse
Can we realistically get all patients to remission?

Challenge for Remission – Treatment-Resistant Depression
• Roughly 70 percent of people do not achieve an adequate response to their first trial of antidepressant medication
• Four million patients (30 percent) do not achieve adequate response to treatment and/or do not tolerate medication side effects after multiple treatment attempts with different medications
– Considered to be treatment-resistant depression (TRD)
9

1010
1. Nemeroff CB. Depress Anxiety. 1996/1997;4(4):169-181; 2. Oquendo MA et al. J Clin Psychiatry. 2003;64(7):825-833; 3. Oquendo MA et al. Am J Psychiatry. 1999;156(2):190-194. 4.Kessler RC, et al. JAMA. 2003;289(23):3095-3105.
Adequate Dosage Adequate Duration
Poor Tolerability
Nonadherence Safety Issues
Lack of Efficacy
Comorbidities
Factors contributing to inadequate treatment include:
Many Obstacles to “Adequate” Treatment of Depression1-3
Despite treatment ▬ 4 million remain depressed4
.

1111
STAR*D: Achieving Remission Is Difficult Despite Adequate Treatment
2830
20
14
21
16
7
0
10
20
30
40
50
HA
MD
-17
Re
mis
sio
n R
ate
s (
%)
Initial Treatment
Mono Aug Mono Aug Mono Comb Mono
Augmentation/Combination
Monotherapy
Level 11
(n=3671)Level 22,3
(n=1439)Level 34,5
(n=390)Level 46
(n=123)
Treatment-Resistance Continuum
1. Trivedi MH et al. Am J Psychiatry. 2006;163(1):28-40; 2. Trivedi MH et al. N Engl J Med. 2006;354(12):1243-1252; 3. Rush AJ et al. N Engl J Med. 2006;354(12):1231-1242; 4. Nierenberg AA et al. Am J Psychiatry. 2006;163(9):1519-1530; 5. Fava M et al. Am J Psychiatry. 2006;163(7):1161-1172; 6. McGrath PJ et al. Am J Psychiatry. 2006;163(9):1531-1541.

1212
17 17
22
8
42
35
24
0
10
20
30
40
50
STAR*D: Discontinuation Rates Increase With Increasing Treatment Resistance
Level 11 Level 22,3 Level 34,5 Level 46
Dis
con
tin
uat
ion
Rat
e (%
)
Adverse events were the most common reason for treatment discontinuation
Augmentation/Combination
Monotherapy
1. Trivedi MH et al. Am J Psychiatry. 2006;163(1):28-40; 2. Trivedi MH et al. N Engl J Med. 2006;354(12):1243-1252; 3. Rush AJ et al. N Engl J Med. 2006;354(12):1231-1242; 4. Nierenberg AA et al. Am J Psychiatry. 2006;163(9):1519-1530; 5. Fava M et al. Am J Psychiatry. 2006;163(7):1161-1172; 6. McGrath PJ et al. Am J Psychiatry. 2006;163(9):1531-1541.

Consequences of of TRD
• Significantly more inpatient hospitalizations, outpatient office visits, and psychotropic medications1,2,3
• Average annual costs ranged from between 2 times greater1 and 6 times greater3 compared to treatment-responsive patients
• Costs >$42K versus only $6.5K for treatment-responsive patients3
• Significantly greater work loss costs (disability and absenteeism) than treatment-responsive patients1
• Increased direct costs of non-remitters include increased medical utilization for non-psychiatric conditions1,2
1.Corey-Lisle PK, et. Al. J. Clin Psych (2002) 63 (8), 717-726. 2..Corey-Lisle PK, et. Al APA 2002. 3. Crown, WH, et. All J. Clin;. Psych. (2002). 63 (11), 963-971.
13

Strategies for Managing TRD
• Current options for treating resistant depression include:– Increasing medication dose or switching to another
antidepressant
– Adding another drug to augment the current medication treatment
– Adding or switching to psychotherapy and/or non-pharmacologic options
14

15
Where Do We Go From Here?
• Available antidepressant medications are effective for a significant number of MDD patients
• However, approximately one-third of MDD patients don’t adequately benefit from, or can’t tolerate, the available antidepressant medications
• Various combinations and augmentation strategies are frequently utilized to treat resistant MDD
– Some evidence-based
– Most empirical

Understanding How TMS Therapy Works
Mark Demitrack, M.D.
16

17
Beyond Pills – What are our Options?
• Lifestyle modifications: Exercise, nutrition, environment manipulations
• Psychotherapy
• Biomedical devices
– Electroconvulsive Therapy (ECT)
– Vagus Nerve Stimulation (VNS)
– Transcranial Magnetic Stimulation (TMS) Therapy

18
Electroconvulsive Therapy (ECT)
• Introduced in 1930s
• Most effective depression treatment
• Works by inducing whole brain “seizure” pattern of neural activation through application of direct electrical current to scalp
• Modern ECT is controlled and painless with anesthesia
• Common adverse events: temporary confusion and memory loss
• Long-term cognitive dysfunction possible
Sackeim HA, et al. Neuropsychopharmacology. 2007;32(1):244-254.

19
Vagus Nerve Stimulation (VNS)
• Approved by FDA in 2005 as adjunct to antidepressant medications
• Electrodes implanted on vagus nerve, pulse generator in chest wall
– Indirect stimulation of the brain
• Evidence of efficacy from non-randomized trial
• Invasive procedure required (surgery) with risks from anesthesia
• MRI contraindication

2020
Transcranial Magnetic Stimulation (TMS)
• Application of electromagnetic induction described by Michael Faraday in 1839– Faraday’s Law: a time-varying
magnetic field induces an electric current that runs perpendicular to the time-varying motion of the magnetic field1,2
• Clinical application: Pulsed magnetic fields can induce electrical currents in brain tissues and neurons3
1. Faraday M. In: Experimental Research in Electricity. Vol 1. London Quaritch; 1839:1-15; 2. Barker AT. J Clin Neurophysiol. 1991;8(1):26-37; 3. Barker AT et al. Lancet. 1985;11(8437):1106-1107.

2121
Effect of TMS on the Brain
Acute Effects– Induces electric current
– Depolarizes neurons in superficial cortex
– Leads to local and trans-synaptic changes in brain activity
Example:
Left prefrontal TMS
23 depressed individuals
Activation demonstrated at site of stimulation and also at synaptically connected cortical and subcortical regions
Li X et al. Biol Psychiatry. 2004;55(9):882-890; Teneback CC et al. J Neuropsychiatry Clin Neurosci. 1999;11(4):426-435; Epstein CM et al. Neurology. 1990;40(4):666-670.

22
NeuroStar TMS Therapy: Clinical Development Program
1. O’Reardon JP et al. Biol Psychiatry. 2007;62(11):1208-1216; 2. Janicak PG et al. J Clin Psychiatry. 2008;69(2):222-232; 3. Avery DH et al. J Clin Psychiatry. 2008;69(3):441-451; 4. Lisanby SH et al. Neuropsychopharm, 2009;34(1):522-534; 5. Data on file: Study 103. Neuronetics, Inc: Malvern, PA; 2008.
Maintenance ofEffect Study2,4,5
‘103’
Open-LabelCrossover Study 2,3,4
‘102’
Randomized, Controlled Study1,2,4
‘101’
Not Improved
Improved
Improved

23
P=.007P=.0006 P=.0041
NeuroStar Produced Significant Improvements in Depressive Symptoms
MADRS Total Score(Baseline to Endpoint Change)1
HAMD-24 Total Score(Baseline to Endpoint Change)2
** P<.01.LOCF analysis of evaluable study population.1. Lisanby SH et al. Neuropsychopharmacology. 2009;34(2):522-534; 2. Data on file. Neuronetics, Inc: Malvern, PA; 2008.
NeuroStar TMS Therapy (n=88)
Sham (n=76)
**** **
Baseline Week 2 Week 4 Week 6
0
-2
-4
-6
-8C
han
ge
Fro
m B
asel
ine
**** **P=.0018
P=.0006 P=.0063
Baseline Week 2 Week 4 Week 6
0
-2
-4
-6
-8
Ch
ang
e F
rom
Bas
elin
e

24
0.52
0
0.2
0.4
0.6
0.8
1
0.31
0
0.2
0.4
0.6
0.8
1
N=164 N=12,564
Sta
nd
ard
ize
d
Eff
ec
t S
ize
(H
AM
D-1
7)
1. Data on file. Neuronetics, Inc: Malvern, PA; 2008.2. Turner EH et al. N Engl J Med. 2008;358(3):252-260.
Sta
nd
ard
ize
d
Eff
ec
t S
ize
(H
AM
D-1
7)
Analysis of Effect Size: NeuroStar vs Antidepressant Medications
[95% CI 0.21–0.83]
[95% CI 0.26–0.36]
NeuroStar TMS Therapy1
Antidepressant Medication2
25
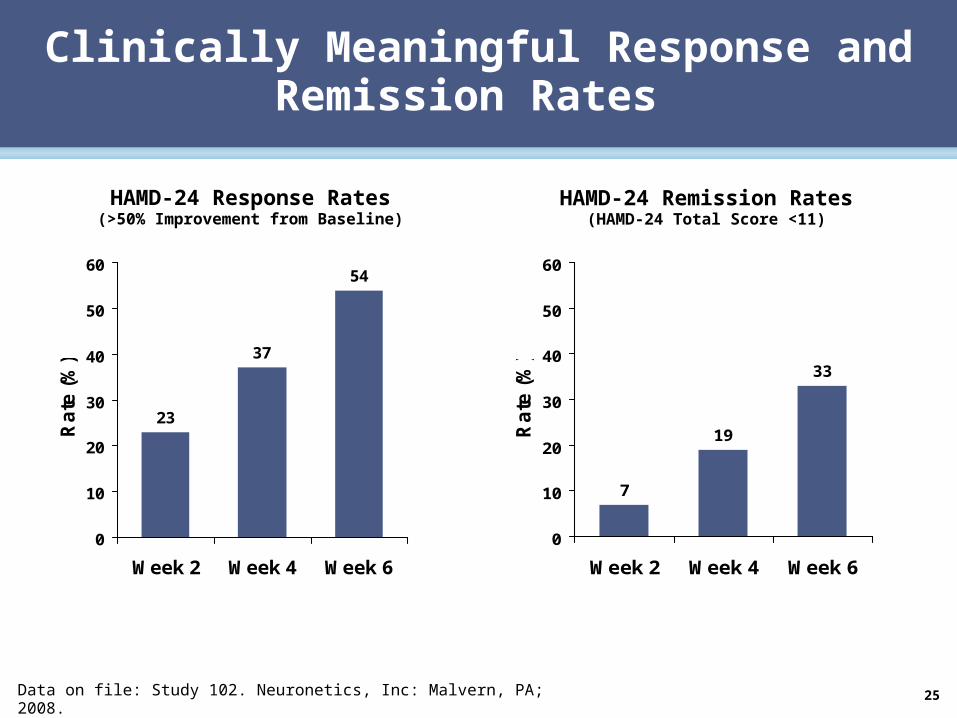
23
37
54
0
10
20
30
40
50
60
Week 2 Week 4 Week 6
Ra
te (
%)
Clinically Meaningful Response and Remission Rates
7
19
33
0
10
20
30
40
50
60
Week 2 Week 4 Week 6
Ra
te (
%)
HAMD-24 Response Rates(>50% Improvement from Baseline)
HAMD-24 Remission Rates(HAMD-24 Total Score <11)
Data on file: Study 102. Neuronetics, Inc: Malvern, PA; 2008.
26
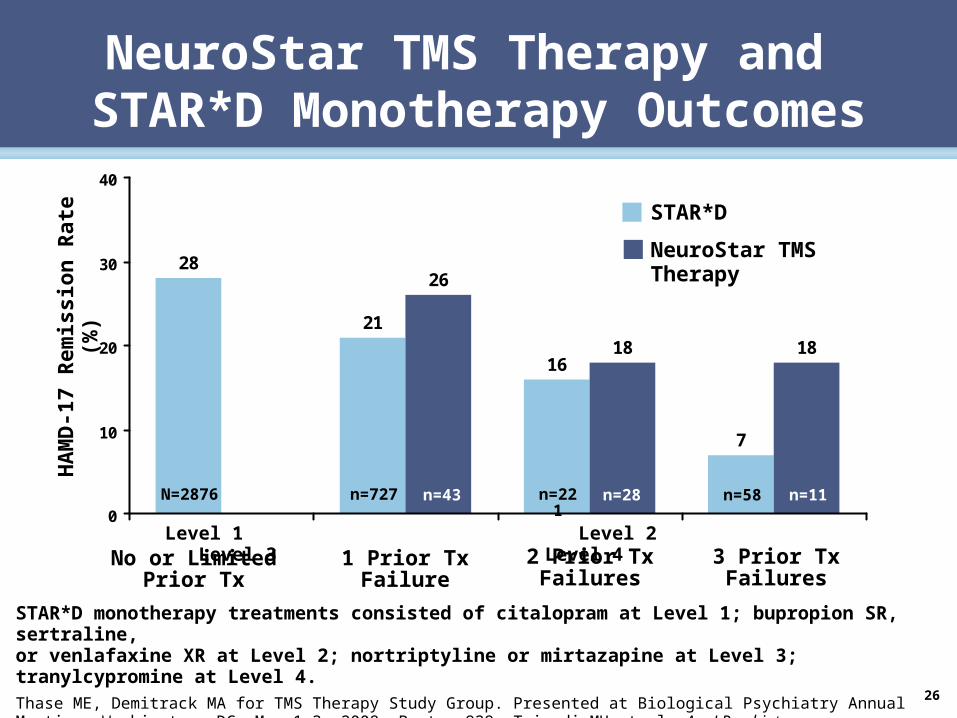
STAR*D monotherapy treatments consisted of citalopram at Level 1; bupropion SR, sertraline, or venlafaxine XR at Level 2; nortriptyline or mirtazapine at Level 3; tranylcypromine at Level 4.Thase ME, Demitrack MA for TMS Therapy Study Group. Presented at Biological Psychiatry Annual Meeting. Washington, DC: May 1-3, 2008. Poster 929; Trivedi MH et al. Am J Psychiatry, 2006;163(1):28-40; Rush AJ et al. N Engl J Med, 2006;354(12):1231-1242; Fava M et al. Am J Psychiatry. 2006;163(7):1161-1172; McGrath PJ et al. Am J Psychiatry. 2006;163(9):1531-1541.
28
21
16
7
26
18 18
0
10
20
30
40
HA
MD
-17
Rem
issi
on
Rat
e (%
)
N=2876 n=11n=58n=28n=221n=43n=727
STAR*D
NeuroStar TMS Therapy
No or Limited Prior Tx
1 Prior Tx Failure
2 Prior Tx Failures
3 Prior Tx Failures
Level 1 Level 2 Level 3 Level 4
NeuroStar TMS Therapy and STAR*D Monotherapy Outcomes
27
• NeuroStar TMS Therapy was offered to patients from acute efficacy and open-label studies
• 6 months of open-label medication monotherapy
• Worsening of symptoms, based on protocol-defined criteria, mandated periodic reintroduction of TMS
Data on file: Study 103. Neuronetics, Inc: Malvern, PA; 2008.
6-Month Long-Term Follow-Up Study: Study Design

28
6-Month Long-Term Follow-Up Study: Results
• ~50% experienced symptom breakthrough and required NeuroStar TMS Therapy retreatment
• Patients previously treated with NeuroStar TMS Therapy had <10% relapse rate at the end of 6 months
Data on file: Study 103. Neuronetics, Inc: Malvern, PA; 2008.

29
NeuroStar TMS Therapy:Safety Overview
• No seizures
• No systemic side effects such as weight gain, sexual dysfunction, nausea, dry mouth, or sedation
• No adverse effect on cognition
• Most common adverse events were headache and scalp discomfort during active treatment
• <5% of patients discontinued due to adverse events
More than 10,000 active treatments performed across all studies
Janicak PG et al. J Clin Psychiatry. 2008;69(2):222-232. NeuroStar TMS Therapy (n=155)
Sham (n=146)
Prestudy 1 2 3 4 5 6 7 8 9 Week

30
No Evidence of Emergent Suicidal Ideation With NeuroStar TMS Therapy
* Shift Score indicates the percent of subjects who experienced a change in HAMD Item 3 score from 0 or 1 at baseline to 3 or 4 at later point in time.
• HA
MD
Ite
m 3
Su
icid
al I
dea
tio
n• S
hif
t S
core
(%
)*
•0.0
•0.5
•1.0
•1.5
•2.0
•2.5
•3.0
•3.5
•4.0
•Baseline •Week 2 •Week 4 •Week 6
•NeuroStar TMS Therapy (n=155)
•Sham TMS (n=146)
O’Reardon JP et al. Biol Psychiatry. 2007;62(11):1208-1216; Avery DH et al. J Clin Psychiatry. 2008;69(3):441-451; Janicak PG et al. J Clinical Psychiatry. 2008;69(2):222-232.
•No adverse effect on cognitive function•Tested across several cognitive function outcome measures•No evidence of emergent suicidal ideation
Summary of NeuroStar TMS Therapy Clinical Evidence
31
• Efficacy established in largest multi-site, randomized, sham-controlled TMS clinical trial conducted to date:
– Primary outcome (MADRS): 22.1% reduction in MADRS total score with active NeuroStar TMS vs 9.1% on sham
– Clinically meaningful effect size = 0.52
• In open label extension study, 1 in 2 patients reached response, 1 in 3 patients achieved remission
• In a 6 month, open-label follow up study that allowed TMS reintroduction if needed, <10% of patients experienced relapse of illness
• Safety and tolerability shown to be excellent

32
Where Does TMS Therapy Fit in the MDD Treatment Landscape?
Kessler RC et al. Arch Gen Psychiatry. 2005;62(6):617-627; Kessler RC et al. JAMA. 2003;289(23):3095-3105; Herrmann RC. Am J Psychiatry. 1995;152(6):869-875.
SSRISNRINDRI
TMS
Primary Care• Initial Diagnosis
• Early Treatment Attempts
Psychiatry• Improved Diagnosis
• Improved Dosing
• Psychotherapy
• New Treatment Options
Combination & Augmentation– Atypical Antipsychotics– Mood Stabilizers
MAOI & TCA
ECT
10M
8M
6M
4M
2M
0 1 2 3 4 5 6 7 8
Failed Treatment Attempts in Current Episode
Nu
mb
er o
f M
DD
Pat
ien
ts
VNS
Treatment-Resistance Continuum

TMS Research by the National Institute of Mental Health
Linda Carpenter, M.D.
33

Independent Research on TMS
• Neuronetics provided NeuroStar devices, but was not involved in study design or implementation
• Tested whether daily left prefrontal rTMS safely and effectively treats MDD– Focus on masking sham conditions
• Well-designed study
– Prospective, multi-site, randomized, active sham-controlled (1:1 randomization)
– 3 weeks of daily weekday treatment followed by continued blinded treatment for up to another 3 weeks in improvers
– Evaluated 199 antidepressant drug-free patients with unipolar, non-psychotic, major depressive disorder
34George et al. Arch Gen Psychiatry 2010; 67(3):507-516.
Confirm # of patients - maybe only 190 actually studied
Confirm # of patients - maybe only 190 actually studied

NIMH Study Findings
• Patients, treaters, and raters effectively masked
• Minimal adverse effects did not differ between active and sham treatment arms
– 88% retention rate (90% sham; 86% active)
• Significant effect of treatment on proportion of remitters (14% active rTMS, 5% sham) (P=0.02)
• Odds of attaining remission 4.2 times greater with active rTMS than sham
– 95% confidence interval, 1.32 – 13.24
• Most remitters had low antidepressant treatment resistance
• Almost 30% of patients remitted in the open-label follow-up
• Conclusion:
Daily left prefrontal rTMS as monotherapy produced statistically significant and clinically meaningful
antidepressant therapeutic effects greater than sham
George et al. Arch Gen Psychiatry 2010; 67(3):507-516.35

NIMH Study Takeaways
• Conducted completely independent of industry
– Used the NeuroStar TMS Therapy system which is the only FDA-cleared device available for the treatment of depression
• Met its a priori primary outcome measure – remission (p=0.02)
• Effect size of treatment benefit is large
– Patients in the active TMS arm had a 4.2 times greater odds of achieving remission
• Included patients with a broad range of treatment resistance
– Patients with one to four prior antidepressant treatment failures were enrolled
36

View from the Clinic:Finding a Direct Route to
Getting Patients Well
Karl Lanocha, M.D.
37

A Turning Point for My Practice and My Patients
• Changed my practice
• Remarkable success – Even in patients disabled
by depression for years
• Provide TMS therapy exclusively
38
Mark - can we insert some kind of visual to imply a turning point…
Slide is essentially showing how TMS changed the way he practices
What Patients Ask Me
• Will TMS allow me to stop taking medications?
– Simplifies treatment regimen if it does not completely eliminate meds
• Will it bring permanent relief from depression?
– Achieved remission in more than half of patients; infrequently need maintenance therapy
• Is this painful?
– It’s a ‘unique’ experience; never had a pt unable to finish course of treatment; get used to it very quickly; fall asleep after 3-4 tx; oldest patient is 87 who takes a nap;
• How much will this cost?
• Will it change my personality?
39
I’ve included the answers that Lanocha will give, but in presentation, will just list questions, not sub-bullets
I’ve included the answers that Lanocha will give, but in presentation, will just list questions, not sub-bullets
Most people are fascinated and want to learn how their brain works

40
Psychotherapy Remains Vital Component of Treatment
• Incorporated into treatment sessions
– Can target behaviors and interpersonal dynamics
• Cognitive-Behavioral Therapy (CBT)
– Focuses on changing negative or irrational thoughts and associated behaviors
– Most validated form of psychotherapy for MDD
• Interpersonal Therapy (IPT)
– Addresses interpersonal issues, relationships
Mark – we used this picture before – do you have anything else that works?

41
How We Decide if TMS is an Option
• Choice of treatment after an initial treatment “failure” depends on many factors, including:– Nature of depressive symptoms
– History of responses to past medication trials
– Medication tolerability
– Side effect profile
– Concurrent medical conditions
– Medication cost
– Likelihood of adherence
– Patient choice
– Physician comfort with managing the treatment
42
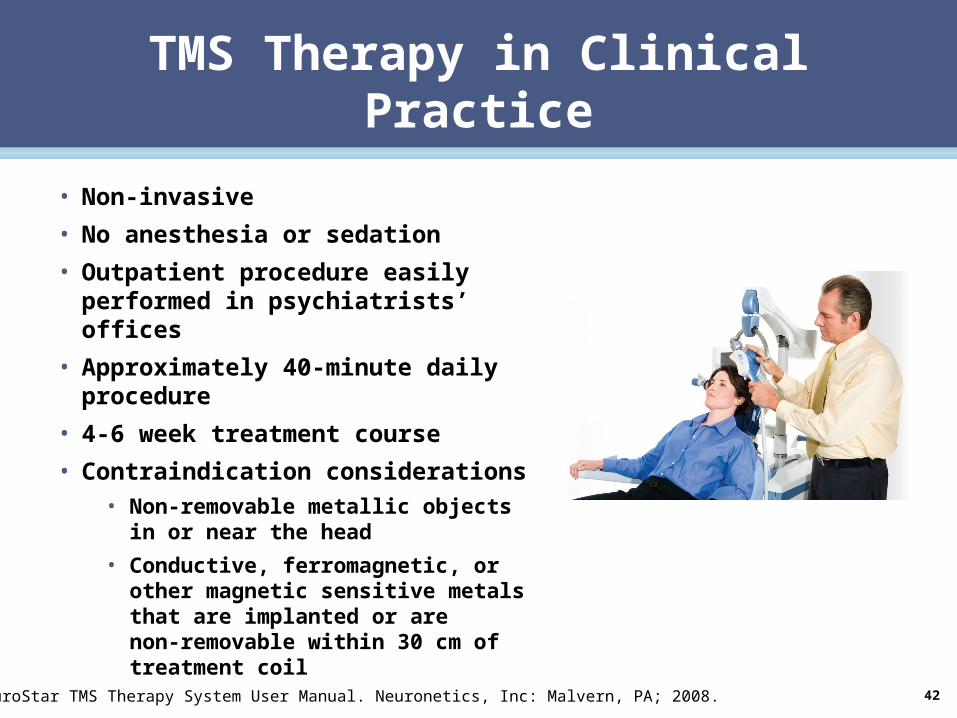
TMS Therapy in Clinical Practice
• Non-invasive
• No anesthesia or sedation
• Outpatient procedure easily performed in psychiatrists’ offices
• Approximately 40-minute daily procedure
• 4-6 week treatment course
• Contraindication considerations• Non-removable metallic objects in or
near the head
• Conductive, ferromagnetic, or other magnetic sensitive metals that are implanted or are non-removable within 30 cm of treatment coil
NeuroStar TMS Therapy System User Manual. Neuronetics, Inc: Malvern, PA; 2008.

Quality of Life and Economic Benefits
• NeuroStar TMS shows improvements in standard measures of functional status and quality of life
• When NeuroStar TMS is compared to current standard of care using complex combination antidepressant medications– TMS results in decreased # days lost due to illness, and
increased work productivity,
– TMS results in a net cost savings relative to current pharmaceutical standard of care
43
Simpson, KN, Welch, MJ, Kozel, FA, et al. Adv in Therapy 2009; 29(3):346-368; Neuronetics, Inc, data on file.

44
timePulseTrain
(10 pulses/sec)
1 sec
TreatmentSession
4 sec 26 sec
~ 40 min
SingleMagnetic
Pulsetime
.2 msec
• Pulse Train: group of electromagnetic pulses followed by non-pulse interval
• Stimulation Time: duration of pulse train, measured in seconds
• Interval: time period between pulse trains, measured in seconds
Key TMS Therapy Terms

45
Understanding Motor Threshold (MT)
• Location: position on motor cortex that stimulates thumb
• Level: minimum stimulation that induces observable motor response in 50% of applied pulses
• % MT: pulse output used for treatment, relative to MT level

46
TMS Therapy Treatment Parameters
• Treatment sessions– 37.5 minutes
• Treatment course– 5x/week for 4 to 6 weeks
– Then taper over 3 weeks
• Treatment magnetic field strength = 120% of MT
• Treatment parameters– Stimulation time = 4 seconds
– Pulses per second = 10
– Interval = 26 seconds
– Number of pulses = 3000
NeuroStar TMS Therapy System User Manual. Neuronetics, Inc: Malvern, PA; 2008.
4747
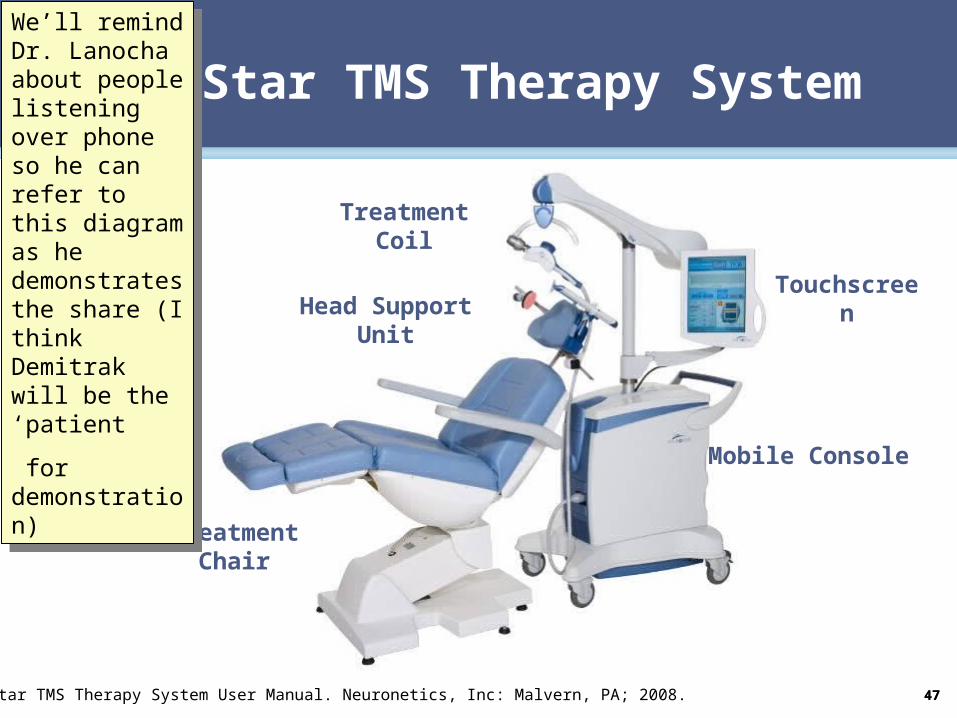
NeuroStar TMS Therapy System
Treatment Coil
Head Support Unit
Treatment Chair
Mobile Console
Touchscreen
NeuroStar TMS Therapy System User Manual. Neuronetics, Inc: Malvern, PA; 2008.
We’ll remind Dr. Lanocha about people listening over phone so he can refer to this diagram as he demonstrates the share (I think Demitrak will be the ‘patient
for demonstration)
We’ll remind Dr. Lanocha about people listening over phone so he can refer to this diagram as he demonstrates the share (I think Demitrak will be the ‘patient
for demonstration)

A Battle on Two Fronts: My Struggle with Depression
Catherine Hogan
48

49
Q&A