1.11 asymptomatic arsine nephrotoxixity.a case report
DESCRIPTION
Arsine GasTRANSCRIPT

192 SA MEDIESE TYD KRIF 4 Augustu 1979
Asymptomatic Arsine ephrotoxicit)
A Case Report
H. LEVY, J. R. LEWI D.T. H. R. SCH EIDER, F. J. MIL TE
SUMMARYA completely asymptomatic patient wi:h arsine nephro
toxicity is described. The light and electron microscopicappearances of the kidney biopsy specimen are docu
mented. The pathogenesis of the lesions, the usual
manifestations of arsine exposure, and how these dif
fered from those seen in our patient, are discussed.
S. Afr. med. J.. 56. 192 (1979).
Arsine is one of the most toxic gases known to manand causes cough with pyrexia. haemolysis, jaundice.gastro-intestinal di turbances and haematuria or haemoglobinuria. The prognosis depends on the degree of kidneydamage and is directly related to the recovery of renalfunction. Anuria is usually fatal. unle s exchange transfusion. haemodialysis or peritoneal dialysi is instituted.Mild presentations have been recorded in the literature.but all were of sufficient severity to attract medical attention. Blood transfu ions are given for anaemia and urinei alkalinized.
Our patient was totally asymptomatic and would haveescaped detection had arsine not been incriminated in theillnesses and deaths of others in his work environment.
CASE REPORTThe patient is a 37-year-old man who works as an analystat a platinum metal refinery on the East Rand. On 28February 197 he received small samples of an aluminium/platinum group metal alloy which he crushed with a standard hammer and buckboard method. Further sampleswere handled in a similar manner on 7 March 1978. and.in the intervening period. the first set of samples sub equently joined by (he o(her samples was left in his office.These samples were later shown to be evolving arsine gaon standing in ambient air.
Approximately 2 weeks before our patient presented. aworker in the refinery had died as a result of arsinepoi oning. He had al 0 been handling the aluminiumpla(inum group metal allav. After the death of the worker.personnel were informed of the possibility of arsine
OeparrmcnI of Mcdicine. nivcrsirv of the Witwatersrandand Johannesburg General Hospital. Johannesburg
11. LE\')'. R,.,' .. ~I.Jl. 13.( 11 .. IlIterll11. H. SCII1'\EIDEH..\I.B. (lI.B. F.e.p. (S ..~.I. .\/edical RegistrarF. .I. \IlL:'-JE. F.CP. (s ..~.l. ~l.n .. Sellior Physiciall. Rellal Ullit
School of Palhology. Soulh African Instilule for MedicalResearch and ni\'ersity of IheWitwaiersrand, Johannesburg
.I. H. LE\\T\'. ~l.U. U.CH .. F.F. PATH .. Sellior PathologistI). T. NL\'J'\'. ~I.R. n.CH .. Regivtmr
Dote received: 5 January 1979.
exposure and everyone in the refinery and laboratory wasexamined.
On 12 March 197 , the patient presented for examination. ystematic questioning revealed that he was fit,having been passed as normal for an insurance examinationin 1971 and by the Phthisis Board in September 1977. Hehad no burning on micturition, no urgency, and no frequency. There wa no hesitancy on passing urine and hiSstream wa good. There had been no period of oliguriaor anuria. Careful questioning failed to reveal any previous ymptoms of urinary tract abnormality or anyother cause of haematuria or proteinuria. He is a blooddonor. and after having given 5 I units he wa.· told hehad become Australia antigen-positive. He had not beenill and had never been jaundiced. He had had no gastrointestinal symptom during the preceding year. Examinationon the same day revealed an alert. completely normalmiddle-aged man. His blood pressure was 110 80 mmHg.
rine testing showed moderate haematuria. and mildproteinuria was revealed with dipsticks, although he hadbeen completely well during the intervening period. Ophthalmoscopic examination was negative. There was norenal angle tenderness or renal artery bruit. A radiograph of the chest and an ECG were normal.
On admission to the Chamber of Mines Hospital, thehaemoglobin concentration was 14.2 g/dl. and there wasno evidence of haemolysis. The ESR was 14 mm/h. Theserum electrolyte level was normal, the serum urea levelwas 9,8 mmoJ/l, and the serum creatinine level was 132.6fJ.mol/1. The results of a midstream urine examinationand 24-h urine collections are shown in Tables I and JIrespectively. The cercarial indirect fluorescent antibody testwas negative. TO arsenic was found in the specimen ofhair submitted for examination.
An excretory urogram performed on 11 April 1978 wasnormal. with an excellent nephrogram phase. The kidneysexcreted the contrast medium simultaneously.
On admission to the Johannesburg General Hospital on17 April 1978 the full blood count was normal. the ESRwas 5 mm/h and the liver function tests were negative. Theerum electrolyte level wa normal, the erum urea level
wa elevated (8,5 mmol/I), and the serum creatinine levelwas normal (123,8 fJ.molll). The midstream urine examination and the 24-h urine collections showed a total proteinof 0, I g/l. The Addis count was normal. no casts wereeen (Table 11). and Au tralia antigen wa ab ent. Serum
immunoglobulin and complement level were normal,and nephritic factor was present in trace amounts.
The renal biopsy specimen obtained on 20 April 1978con isted of cortical tissue in which the main pathologicalchange were een in the proximal tubules. The lining epithelial cells were swollen and many of the nuclei containedprominent nucleoli.
4 August 197Y SA MI:DICAL JOURNAL
TABLE I. MIDSTREAM URINE EXAMINATION
193
Leucocyte count (/ml)
Erythrocyte count (/ml)
pHProtein
Glucose
BloodCulture
23 March 1978
2000
130006
traceStaphylococcus
epidermis
and diphtheroids
<100oo/ml
12 Apnl 1978
10001000
6trace
+,No 9rowth
20 Apnl 1978
100025000
6
No 9rowth
5 May 1978
100010000
6trace
Not done
TABLE 11. 24·HOUR URINE COLLECTIONS
Volume (ml)
Urine urea (mmol/I)Urine creatinine (jJ.mol/l)
Serum urea (mmol/I)Serum creatinine (J1.mol/l)Creatinine clearance (ml/min)
Urea clearanceAddis count
29 March 1978
1220
3209724
9,8132,662
56 10 of normalNot done
5 Apnl 1978
1 710
88407,8
132,6
85
Not done
19 Apnl 1978
1900
2929724
8,5
123,8104
73'1- of normal1 900 000 erythrocytes
and leucocytes
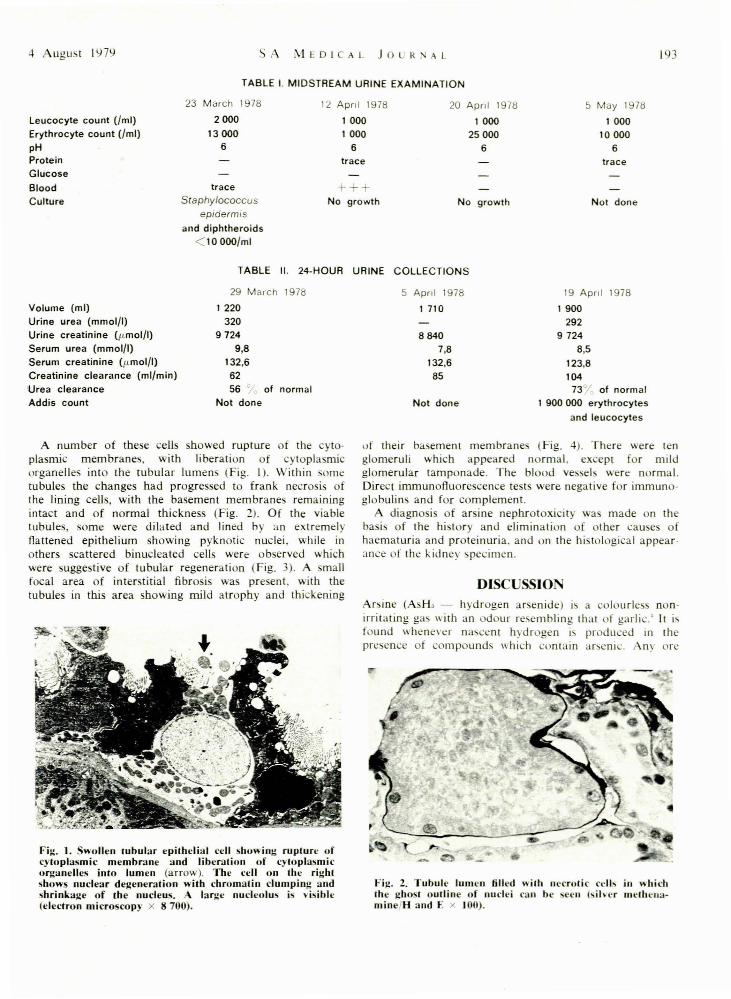
A number of these cells showed rupture of the cyto-plasmic membranes, with liberation of ytoplasmiorganelles into the tubular lumens (Fig. I). Within sometubules the changes had progressed to frank necrosis ofthe lining cells, with the basement membranes remainingintact and of normal thicknes (Fig. 2). Of the viabletubules, some were dilated and lined by an extremelyflattened epithelium showing pyknotic nuclei, while inothers scattered binucleated cells were observed whichwere suggestive of tubular regeneration (Fig. 3). A smallfocal area of interstitial fibrosi wa present, with thetubules in this area showing mild atrophy and thickening
Fig. 1. Swollen /Ubular epithelial cell showing rupture ofcytoplasmic membrane and liberation of cytoplasmicorganelles into lumen (arrow). The cell on the rightshows nuclear degeneration with chromatin clumping andshrinkage of the nucleus. A large nucleolus is \'isible(electron microscopy x 8 700).
uf their ba emem membrane (Fig. 4). There were lenglomeruli which appeared normal. except for mildglomerular tamponade. The blood vessels were normal.Direct immunofluorescence tests were negative for immunoglobulins and for complement.
A diagno i of arsine nephrotoxicity wa made on theba is of the history and elimination of other eau e ofhaematuria and proteinuria. and on the histological appear·ance of the kidney pecimen.
DISCUSSIOArsine (A H:. - hydrogen arsenide) is a colourles nonirritating ga with an odour resembling that of garlic.' It ifound whenever na~cem hydrogen i~ produced ID thepre ence of compounds which contain arsenic. ny ore
Fig. 2. Tubule lumen filled with necrotic ccll~ in whichIhe gho I outline of nuclei can be seen I ilver melhcn3minefH and E x lOO).

194 SA MEDTESE TVDSKRIF 4 Augustus 1979
Fig. 3. Binucleatcd epithelial cells suggestive of regeneration (arrows) and dilated tubules lined by a flatlenedepithelium (silvcr methenamine/H and E x 40).
Fig. 4. Interstitial fibrosis with tbe tubules showing mildatrophy and thickened basemcUl membranes (H and Ex-lO).
contaminated with arsenic will liberate arsine when treatedwith acid.'" During recent years, the commonest methodof arsine generation has been a reaction between arsenicand aluminium, with the subsequent release of hydrogenin the presence of water to permit the formation of arsine.'ItS properties became known in 1815 when Gehlen, aMunich chemist, sniffed some and was ill within an hour,with vomiting and fever. and died 9 days later:"
The first cases in South Africa were reported in 1958in workers shovelling zinc ash into boiling sulphuric acid.'It is one of the most toxic gases known to man and hasbeen incorporated into lewisite, a war gas. Arsine enters thebody through inhalation. There is usually a 2 - 24-hourdelay before symptoms occur. Initially. headache, malai e.weakness. dizziness and dyspnoea. accompanied by gastrointestinal disturbance or abdominal pain, nausea andvomiting, occur."'·' Arsine combines with haemoglobin,and haemolysis, which can be total, results.'·,·, The arsenichaemoglobin complex is filtered by the glomeruli. Dark redurine is passed 4 - 6 hours later. Oliguria or anuria mayresult from either a direct toxic effect of inhibition ofrenal tubular cell respiration or hypoxia. secondary to thehaemolytic anaemia or sludging of renal circulation.' ormassive precipitation of the arsenic-haemoglobin-haptoglo-
bin complex in the tubular lumen.' ecrotic renal tubulescontaining haemoglobin casts are characteristically observedat autopsy.
Jaundice is seen 24 - 48 hours after exposure and abronze tint of the skin has been described. Transversewhite striae of the finger nails (Mees' stripes) have beenobserved 2 - 3 weeks after exposure.'" Encephalopathy and,later, peripheral neuropathy may occur.' Marrow depressionhas also been described·'"
The prognosis of any patient depends on the degree ofkidney damage and is directly related to urine output.When anuria develops death is inevitable, unless heroicmeasures such as complete exchange transfusion, haemodialysis or peritoneal dialysis are instituted.'"
Sequential renal biopsies were performed by Muehrckeand Pirani' who demonstrated extensive tubular damagefollowed by rapid regeneration of tubular cells. In theproximal tubule. these cells have a modified and apparentlyfunctionally defective structure. The glomerular basementmembrane is thickened and diffuse interstitial fibrosis,which becomes focal, develops, and profound nephronatrophy occurs. Alteration in renal function may persistowing to basement membrane thickening' and may continue for prolonged periods after recovery from arsineinduced renal failure.' The renal biopsy specimen in ourpatient was suggestive of an episode of tubular necrosisfollowed by tubular regeneration with tubular obstructionand glomerular tamponade, and is consistent with previously reported biopsy findings.
Severe tubular damage has been described in arsinepoisoning in the absence of extensive haemoglobinuria, andis independent of haemolysis.'
Massive haemolysis with minimal impairment of renalfunction was described by Jenkins eT al.' Uldall eT al:described 2 patients who were mildly affected with cystitis.haematuria and jaundice and who recovered spontaneouslywith only transient renal impairment. Our patient is uniquein that he was totally asymptomatic at all times, and thecondition would have remained undetected had a specimenof urine not been examined.
Arsine exposure occurs despite precautions, and recentattempts at using geothermal and fossil fuel energy sourceshigh in arsenic content may increase the incidence of exposure.' For prevention, strict industrial surveillance forthe presence of arsine is necessary.
We believe that asymptomatic exposure to arsine mayoccur, and recommend that persons who are at risk intheir occupations regularly have their urine examined forarsenic and have routine urine and blood tests for detection of renal damage.
We should like to thank Dr R. Enslin, Chamber of MinesHospital. for referring the patient.
REFERE CES
J. Editorial (1974): Lancet. 1. 1433.2. Comad. M. E.. Mazey. R. M. and Reed. J. E. (1976): Ala. J. med.
Se; .. 13. 65.3. Fowler. B. A. and Weissberg. J. B. (1974): ew Eng!. J. Med .. 191.
1171.4. Muehrcke. R. C. and Pi rani. C. L. (1968): Ann. intern. Med .. 68.
53.5. Uldall. P. R .. Khan. H. A.• Ennis. J. E. et tll. (1970): Brit. J. industr.
Med .. 27. 372.6. Greig. H. B. W .. Bradlow. B. A.. Hard'on. C. et al. (1958): S. AIr.
med. 1.. 32. 101.7. Wilkinson. S. P .. McHugb, P .. Horsiey. S. et al. (1975): Brit. med. J.,
3. 559.8. Jenkins, G. C., Ind, J. E., Kazanuis. G. et al. (1965): Tbid., 1, 7 .