1455 wilson
TRANSCRIPT



When does Primary become Secondary Injury?
On scene ED NCCU
Secondary brain injury occurs after the primary mechanisms of injury have run their course (Gennarelli & Graham, 2005)
Secondary brain injuries often result from complications of the primary mechanism of injury and may occur anywhere from hours to days after the initial injury (Dawodu, 2007)

So at best
Neurocritical Care will only save neurons that have not died

NCCU Has 3 functions
Maintain Airway Good Nursing Care Weaning from Ventilator


A S S O O N A S W E G E T I N V O L V E D W E C A N
E A S I L Y D O H A R M

utter clusterfxxx /
abject harm
perfect care
/ good outcome
The Spectrum of Neuro Critical Care
The goodperfectionist
The bad perfectionist Nature
Where most of us practice
{

BUT WE MUST STOP SECONDARY INJURY….
Like Hypotension?


BUT WE MUST STOP SECONDARY INJURY….
Like ICP?



HYPERVENTILATION1982 Good 2002 Bad

C O O L I N G

J U G U L A R V E N O U S S A T U R A T I O N
Who regularly does this?

B R A I N O X Y G E N A T I O N

B R A I N O X Y G E N A T I O N

So we await….

S T E R O I D S
2004 Bad1985 Good

N E U R O P R O T E C T A N T S … .

N T E R V E N T I O N S T H A T D O H E L P
e.g. Dialysis
….But these are not NCCU specific

N T E R V E N T I O N S T H A T D O H E L P
e.g. Antibiotics
….Probably don’t need ITU

The Time to Save neurons is BEFORE Neurocritical care
Once there… In the spontaneously breathing patient…

than NOB THERAPYIs all this really better
VentilationArt Line
Central LineVasopressors
ICPLicox
Microdialysis TPN
Tracheostomy

Neurocritical care is no better than


W H A T H A P P E N S I F
S H O W S D E C O M P R E S S I O N B A D ?

Neurocritical care improves outcome in severe traumatic brain injury
Martin SmithConsultant & Honorary Professor in Neurocritical CareThe National Hospital for Neurology & NeurosurgeryUniversity College London Hospitals

Diringer et al, Crit Care Med 2001; 29: 635-40
• notbeinginaneuroICUisassociatedwithanincreaseinhospital
mortalityafterintracerebralhaemorrhage
(OR,3.4;95%CI,1.65–7.6)

Observational studies comparing outcomes between neurological critical care units and alternative models of care
Kramer & Zygun, Curr Opin Care 2014; 20: 174-81
Mortality Favourable outcome
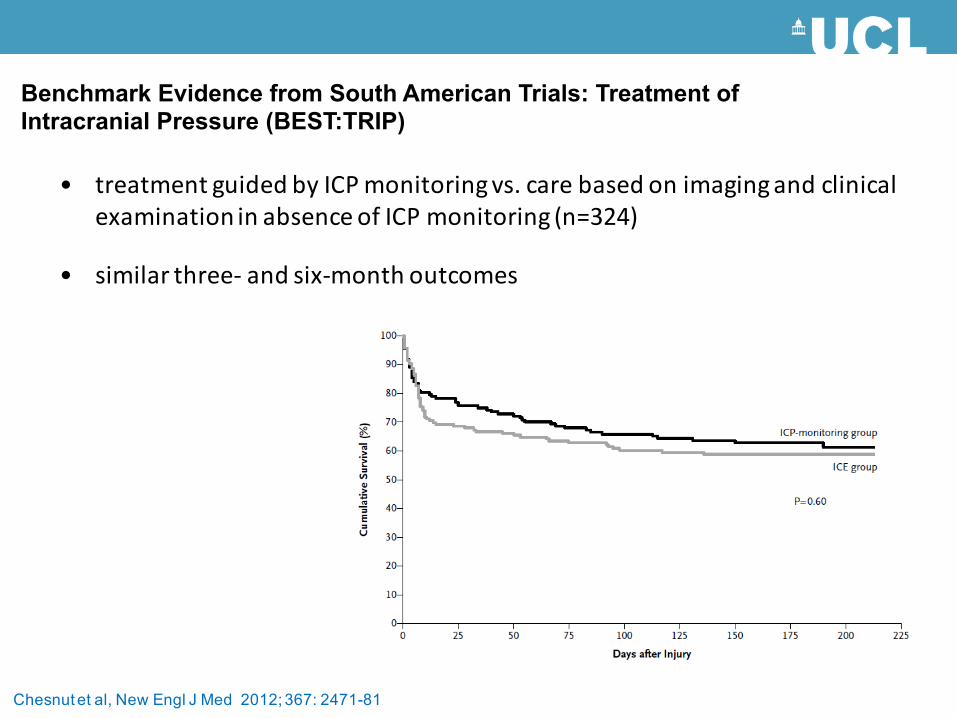
• treatmentguidedbyICPmonitoringvs.carebasedonimagingandclinical
examinationinabsenceofICPmonitoring(n=324)
• similarthree- andsix-monthoutcomes
Benchmark Evidence from South American Trials: Treatment of Intracranial Pressure (BEST:TRIP)
Chesnut et al, New Engl J Med 2012; 367: 2471-81

• moderatehypothermiaoneofthemosteffectiveneuroprotectivestrategiesinpreclinicalstudies
- translatedintohumans
Targetedtemperaturemanagement
Andrews et al, New Engl J Med 2015; 373: 2403-12
• Eurotherm3235trialrandomized387patientsfrom47centersin18countries
– TTM(32-35˚C)asacomponent ofICPmanagementofintracranialhypertension(ICP>20mmHg) resistanttoinitialICP-loweringtherapies
• recruitmentsuspendedearlybecauseofsafetyconcernsinthehypothermiagroup
– worsefunctionaloutcomes (odds ratio1.53,95%CI1.02-2.30)
– highermortalityrates(hazardratio1.45,95%CI1.01-2.10)

Andrews et al, New Engl J Med 2015; 373: 2403-12

• complexandmultifactorial
• severalcomponentsofkeyimportance
– reductioninsubstratedeliverybelowcriticalthresholds
– failingcellularmetabolism
− inabilitytoutilizedeliveredoxygen&glucose
− profoundmetaboliccrisis
• cerebralischaemia/hypoxia
– tissueburdenrelatedtoclinicaloutcome
Pathophysiologyoftraumaticbraininjury
• secondaryinsultsadverselyaffecttheinjuredbrain
– associatedwithworseoutcomes
– prevention/rapidtreatmentassociatedwithimprovedoutcomes
Pathophysiologyoftraumaticbraininjury

– hypoxia
– hypotension
– hyper- andhypocarbia
– hyper- andhypoglycaemia
– hyperthermia
– intracranialhypertension
– seizures
Secondaryinsults

McHugh et al, J Neurotrauma 2007; 24: 287-93
• IMPACTstudydatabase
− mergedcohortof7phaseIIIRCTswith>9000patients
• singleepisodeofhypoxiaorhypotensionstronglyassociatedwithworse
outcome
- hypoxiaOR2.1(95%CI1.7-2.6)
- hypotension OR2.7(95%CI2.1-3.4)
SystolicBP<90mmHgorPaO2
<8.0kPamustbeavoidedor
rapidlycorrectedafterTBI

• ABGtargets
– PaO2 >13.0kPa
– PaCO2 4.5- 5.0kPa
• CVStargets
– MAP>90mmHg
– volumeresuscitation
– vasopressors/inotropes
• glucose5.0- 10.0mmol/l
• coretemperature<37oC
• ICP<20cmH20
• CPP50-70mmHg
Brain Trauma Foundation, J Neurotrauma 2007; 24: S1-S106
Consensusguidelines

Brain Trauma Foundation, J Neurotrauma 2007; 24: S1-S106
Consensusguidelines
• guidelinesareatool,notagoal
• goalisindividualised,targeted
treatment
• treatmentguidedbymonitor-derived
physiologicalvariables
• ABGtargets
– PaO2 >13.0kPa
– PaCO2 4.5- 5.0kPa
• CVStargets
– MAP>90mmHg
– volumeresuscitation
– vasopressors/inotropes
• glucose5.0- 10.0mmol/l
• coretemperature<37oC
• ICP<20cmH20
• CPP50-70mmHg

• multimodalmonitoringallowsdeliveryoftailoredtreatmentregimens– identifyphysiological/pathophysiologicalphenotype
– guidetargetedtherapy
– assesseffectsoftherapy
– guidedecisionsaboutintensityanddurationoftherapy
– improvedpatientoutcomes
• confidencetowithholdpotentiallydangeroustherapyinthosewithoutevidenceofbrainischaemiaormetabolicdisturbance
Individualizedtherapy


ICP-directedmanagement
• greatlyelevatedICPisfatal– abilitytocontrolitislimited
• oversimplifiedconceptssurroundingmanipulationofICPandtheassociationwithoutcome– thresholdsforinitiatingmedicalandsurgicalmanagement
– cerebralperfusionoftennotcompromisedevenifICPis>20mmHg
– outcomeeffectsofcurrenttreatmentprobablysmallerthanwethink
– alltreatmentshavesideeffects
• severeTBIisanoverwhelmingandcomplexprocess
– involvesneurones,gliaandvasculature
– raisedICPcompressescerebralveinscreatingaself-regeneratingcycleofevenhigherpressure

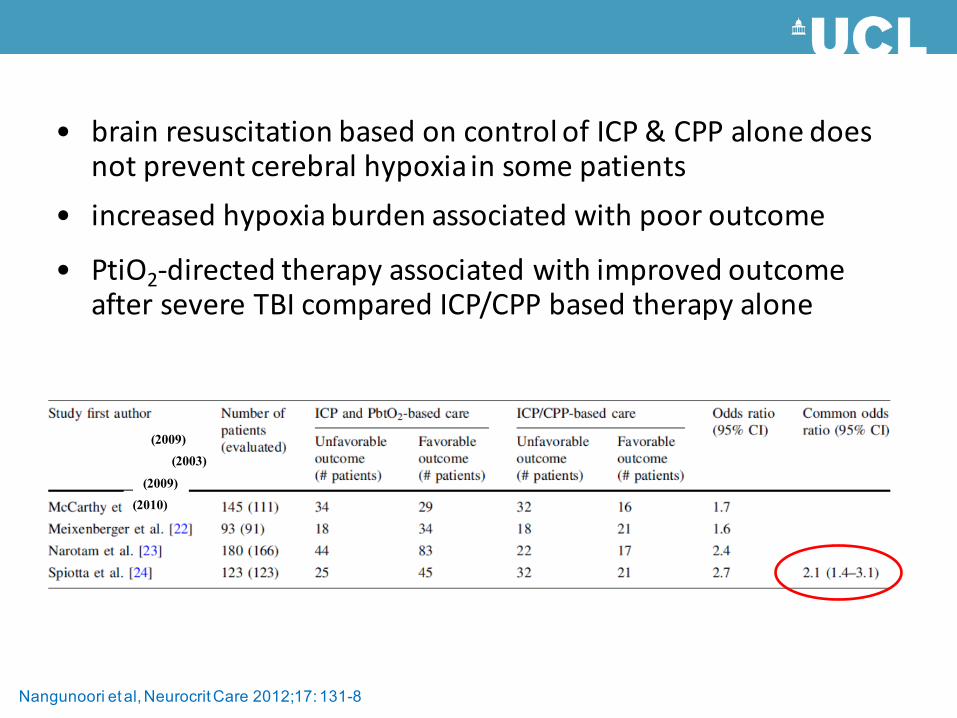
Nangunoori et al, Neurocrit Care 2012;17: 131-8
• brainresuscitationbasedoncontrolofICP&CPPalonedoesnotpreventcerebralhypoxiainsomepatients
• increasedhypoxiaburdenassociatedwithpooroutcome
Nangunoori et al, Neurocrit Care 2012;17: 131-8
(2009)(2003)
(2009)(2010)
• brainresuscitationbasedoncontrolofICP&CPPalonedoesnotpreventcerebralhypoxiainsomepatients
• increasedhypoxiaburdenassociatedwithpooroutcome
• PtiO2-directedtherapyassociatedwithimprovedoutcomeaftersevereTBIcomparedICP/CPPbasedtherapyalone

Marenko et al, J Clin Neurosci 2016; 26: 8-13
• optimalCPPis�92.5mmHgwithan
autoregulatoryrange
between80–100mmHg
• maintenanceofCPP
withinBTFguidelines
(50–70mmHg)would
leavethispatientatrisk
ofon-goingischemia

• braintissuedestructioncausedbyacuteinjuryisworsenedbyon-goinginsults- early,aggressiveinterventiontominimizesecondaryinsultsimprovesthe
outcometrajectoryinmanypatients
- minimizingsecondinsultswillminimizeresidualdisability
CriticalcaremanagementofsevereTBI
• getallthelittlethingsrightallthetime- neurocriticalcareisasmuchaboutmeticuloussystemicphysiological
optimizationasitisaboutspecificbrain-directedtherapies
• keepitsimple- thesix‘Ns’– normoxia
– normocapnia
– normovolaemia
– normotension
– normoglycaemia
– normothermia
– normonatraemia
– normomagnesaemia
CriticalcaremanagementofsevereTBI

• getallthelittlethingsrightallthetime- neurocriticalcareisasmuchaboutmeticuloussystemicphysiological
optimizationasitisaboutspecificbrain-directedtherapies
• optimisecerebralhaemodynamics andoxygention
– blindadherencetoguidelinesrisksdeliveringpotentiallyharmful
treatmentthatisofnobenefit
– individualizeICPandCPP-guidedtherapy
– multimodalphysiologicalmonitoring
CriticalcaremanagementofsevereTBI

• systemicorgansmayfail- sympatheticsurgeandneuroinflammatoryresponsescancause
neurogenicpulmonaryoedema,stresscardiomyopathyandageneralendocrinopathy
- complicationsofbrain-directedtreatment
CriticalcaremanagementofsevereTBI

• systemicorgansmayfail- sympatheticsurgeandneuroinflammatoryresponsescancause
neurogenicpulmonaryoedema,stresscardiomyopathyandageneralendocrinopathy
- complicationsofbrain-directedtreatment
• complexinteractionbetweenbrainandsystemicphysiology
- optimizesystemicandintracranialvariables
- physiologicalneuroprotection
CriticalcaremanagementofsevereTBI

English et al, Neurocrit Care 2013; 18: 131-142

English et al, Neurocrit Care 2013; 18: 131-142

• burdenofneuronallossdirectlyrelatedtoclinicaloutcomes
– minimizesecondaryischaemicbraininjury
• clinicalguidelinesareausefulstartingpoint
• individualizedtreatmentregimens
• neurocritical caredoesimproveoutcomesafterTBI
Summary

THANK YOU!

SOCIETY FOR NEUROSCIENCE IN ANESTHESIOLOGY AND CRITICAL CARE
SNACC 44th Annual MeetingOctober 20-21, 2016Chicago
www.snacc.org