(1800 patients x rays analysis) - · pdf file10 < ta - gt < 15 patellar tilt > 20 ......
TRANSCRIPT
La PATELLA Lyon 2012 “ALRM”
1987

La PATELLA Lyon 2012 “ALRM”
25 years
later…
La PATELLA Lyon 2012 “ALRM”
1987 Findings (1800 patients X Rays analysis)
4 Instability factors (Statistical Threshold)
• Trochlear Dysplasia 96%
• Patella Alta > 1.2
• Excessive TT-TG > 20 mm
• Excessive Patellar Tilt > 20°

La PATELLA Lyon 2012 “ALRM”
1987 Findings
Systematic use of true lateral view
3/ Trochlear depth
1/ Crossing Sign
2/ Bump : “la saillie”
1987

La PATELLA Lyon 2012 “ALRM”
1987 Trochlear Dysplasia classification
The first classification
Normal
Dysplasia

La PATELLA Lyon 2012 “ALRM”
1987 Findings
Patella Alta> 1.2 30% in dislocation population
VMO Dysplasia
J. Caton 1977
Tibial Landmark
G. Deschamps 1982
Patella Landmark
+ =
C&D Index AT/AP

La PATELLA Lyon 2012 “ALRM”
1987 Findings Systematic use of CT Scan
Alignment – torsion measurements
TT-TG > 20 mm 56 % Dislocation population
1978 Goutallier & Bernageau TT-TG on axial view
1987
1987

La PATELLA Lyon 2012 “ALRM”
1987 Findings
Patellar Tilt > 20° 83% in dislocation population
VMO Dysplasia
Systematic use of CT Scan
Alignment – torsion measurements
1987

La PATELLA Lyon 2012 “ALRM”
Instability
factors Knee side
Proposed
procedure
Trochlear
dysplasia Type I, II, III ????
Patellar height Index AT / AP Distalization
Index = 1
TT-TG > 20 mm Medialization
10 < TA - GT < 15
Patellar Tilt > 20° VMO Plasty
1987 ”menu à la carte” for patella dislocation

La PATELLA Lyon 2012 “ALRM”
What were the results… Elvire Servien, Rev Chir Orthop Reparatrice Appar Mot. 2004
All Patients Distalization Medialization Distalization +
Medialization
Préop TT-TG and post op 10 mm <TT-TG<15 mm
0
5
10
15
20
25
Isolated distalization Leads to Automatic medialization of 4 mm

La PATELLA Lyon 2012 “ALRM”
What were the results… Elvire Servien,
Rev Chir Orthop Reparatrice Appar Mot. 2004
Good correlation between the planned TT-TG & the post op TT-TG
No patellar tendon shortening after TT Osteotomy (immediate
mobilisation)

La PATELLA Lyon 2012 “ALRM”

La PATELLA Lyon 2012 “ALRM”
WHAT REMAINS ?
WHICH UPDATE ?
WHICH CHANGES ?

La PATELLA Lyon 2012 “ALRM”
WORLDWIDE WORK 41 Countries…

La PATELLA Lyon 2012 “ALRM”
2012
Patellar Instability

Clinical Evaluation “some particular features”
• Torsional anomalies
• Foot angle
• Pelvis and back position
CT scan for Femoral & Tibial rotation measurement

Clinical Evaluation “some particular features”
Apprehension sign
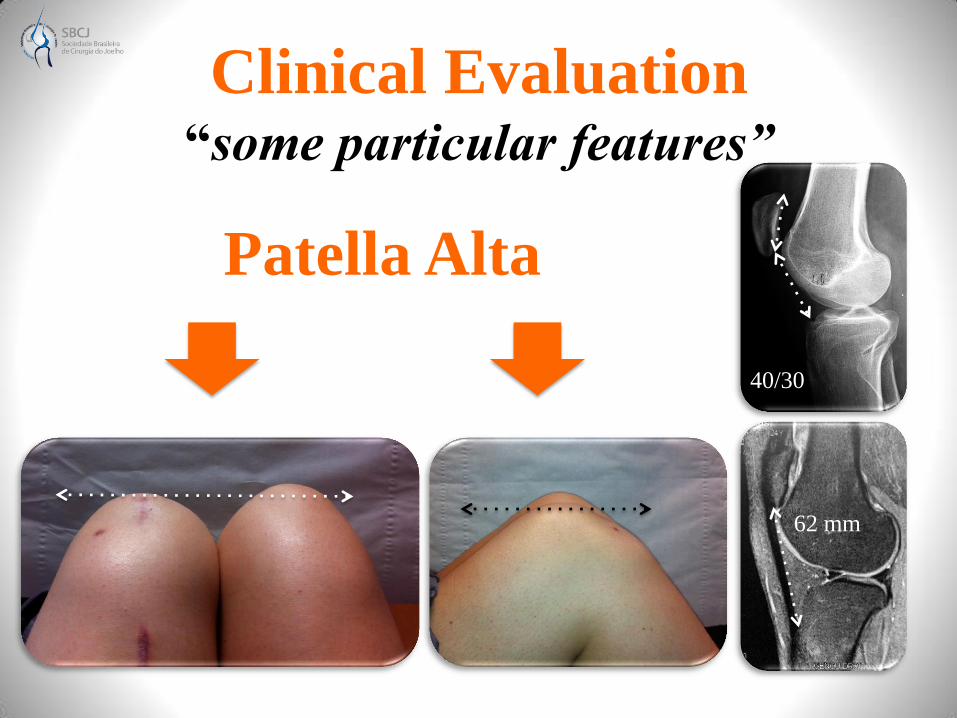
Clinical Evaluation “some particular features”
Patella Alta
40/30
62 mm
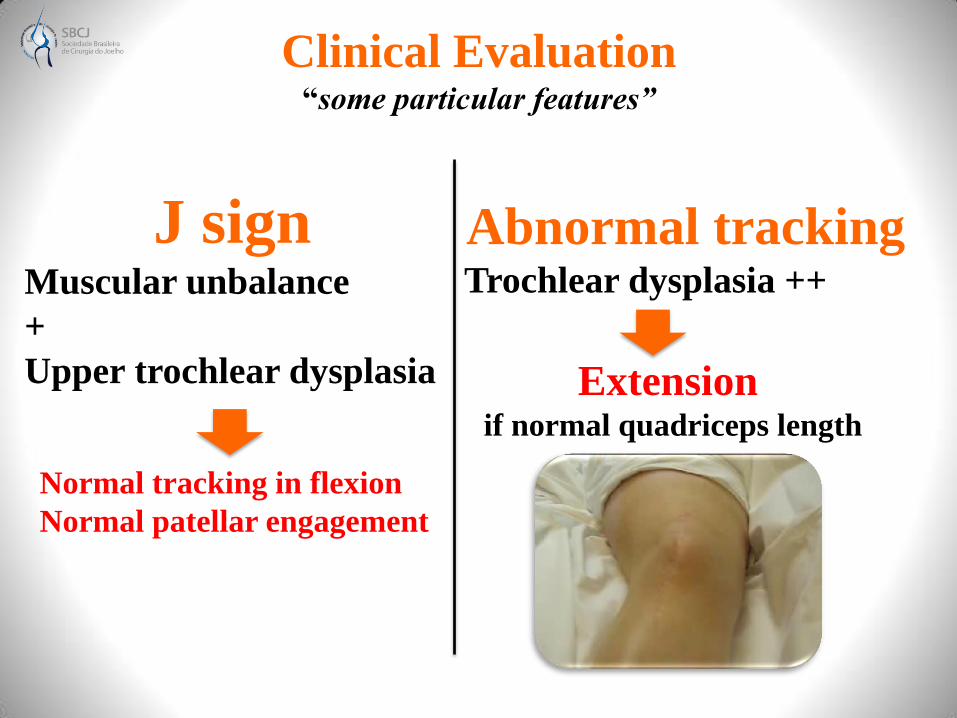
Clinical Evaluation “some particular features”
J sign Muscular unbalance
+
Upper trochlear dysplasia
Abnormal tracking Trochlear dysplasia ++
Extension if normal quadriceps length
Normal tracking in flexion
Normal patellar engagement
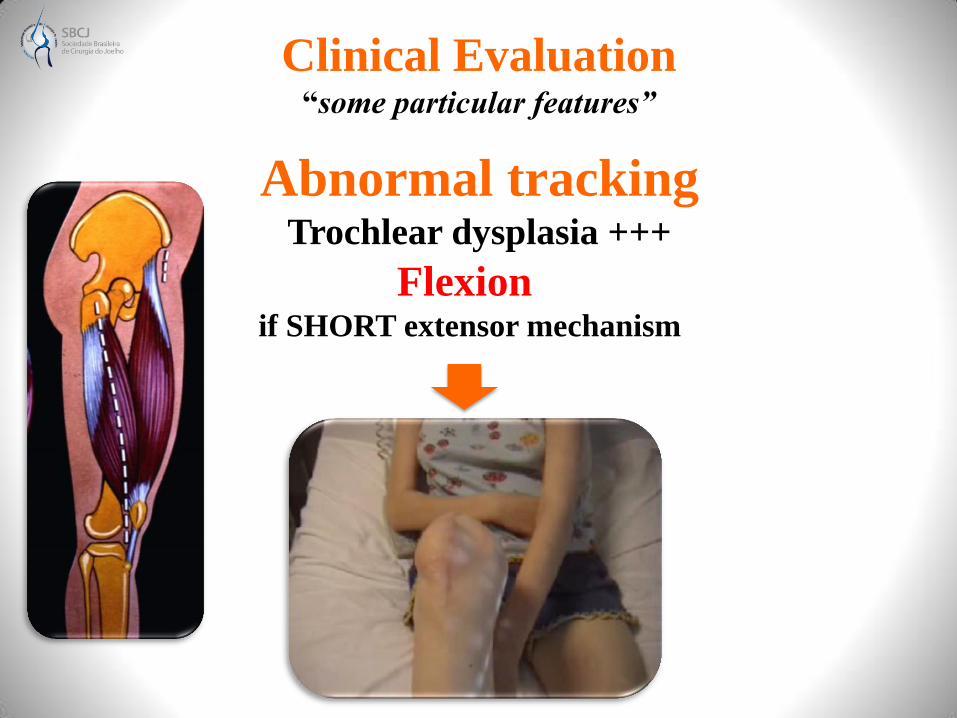
Clinical Evaluation “some particular features”
Abnormal tracking Trochlear dysplasia +++
Flexion if SHORT extensor mechanism
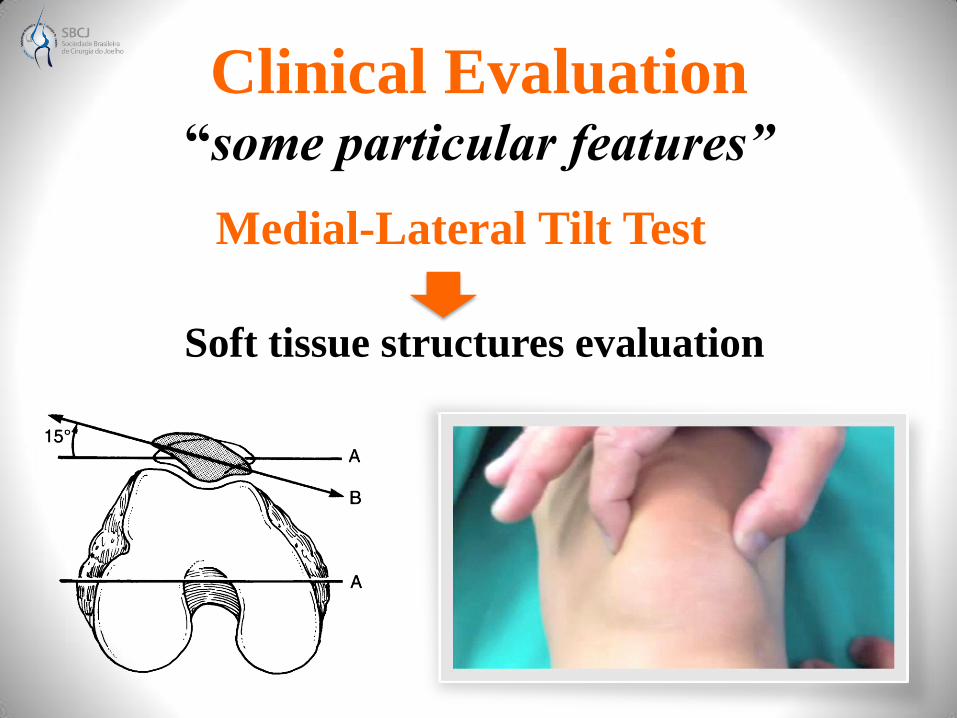
Clinical Evaluation “some particular features”
Medial-Lateral Tilt Test
Soft tissue structures evaluation

Clinical Evaluation “some particular features”
Quadrant Test “Patellar mobility”
Medial structures resistance
MPFL competency
Extension Flexion Patella engages the trochlea
Gives a reference point
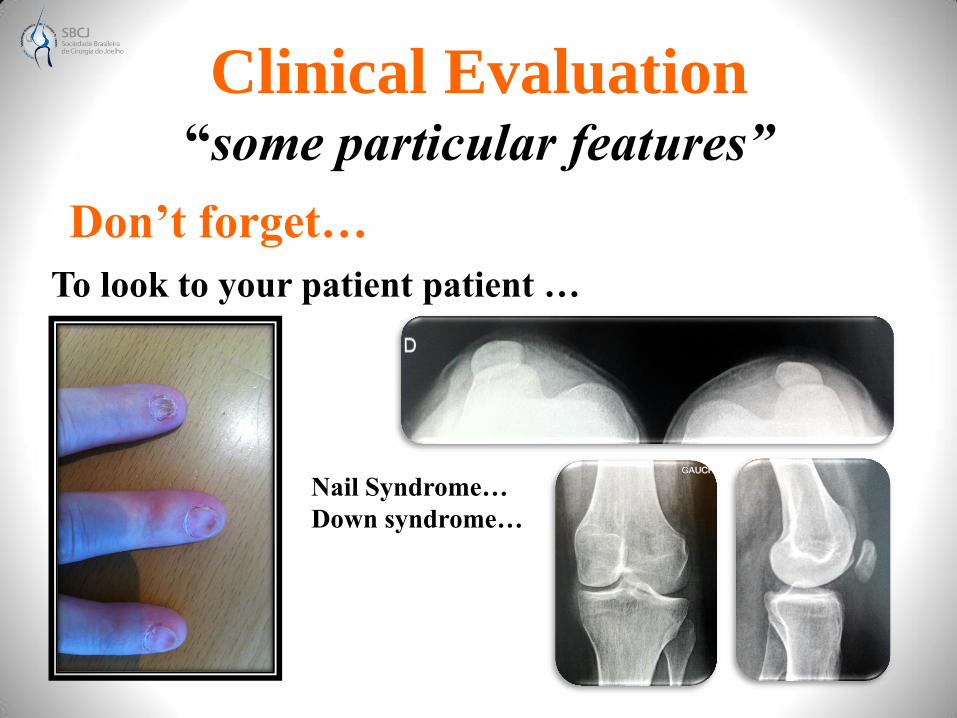
Clinical Evaluation “some particular features”
Don’t forget…
To look to your patient patient …
Nail Syndrome…
Down syndrome…

La PATELLA Lyon 2012 “ALRM”
Trochlear Dysplasia Classification
4 types (2 new landmarks)
Inter and intra observer reliability +++
La PATELLA Lyon 2012 “ALRM”
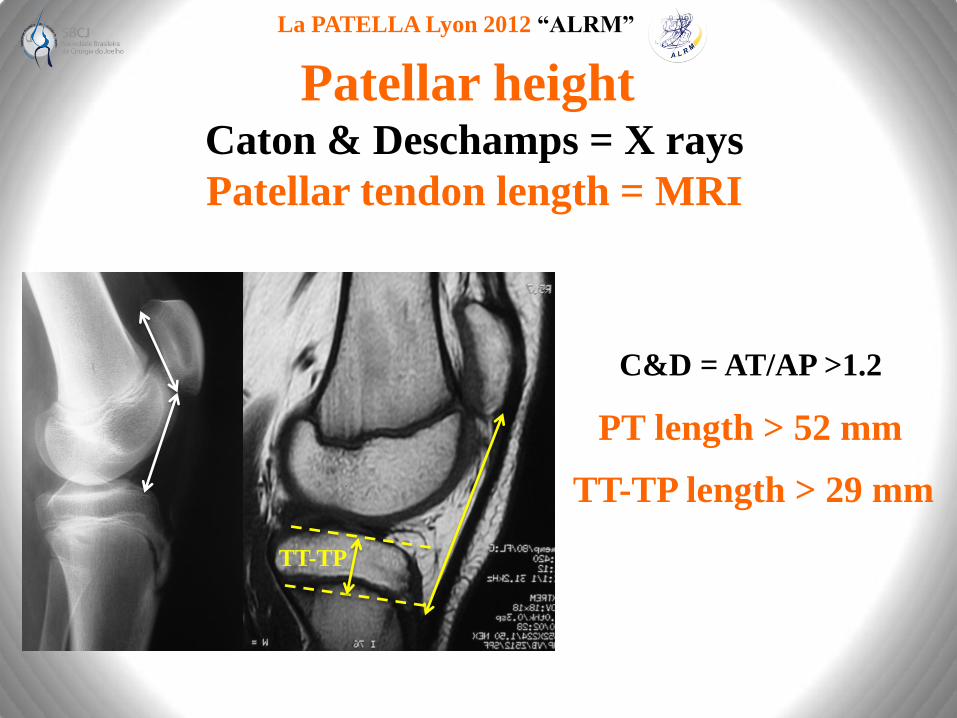
Patellar height Caton & Deschamps = X rays
Patellar tendon length = MRI
C&D = AT/AP >1.2
PT length > 52 mm
TT-TP length > 29 mm
TT-TP
La PATELLA Lyon 2012 “ALRM”
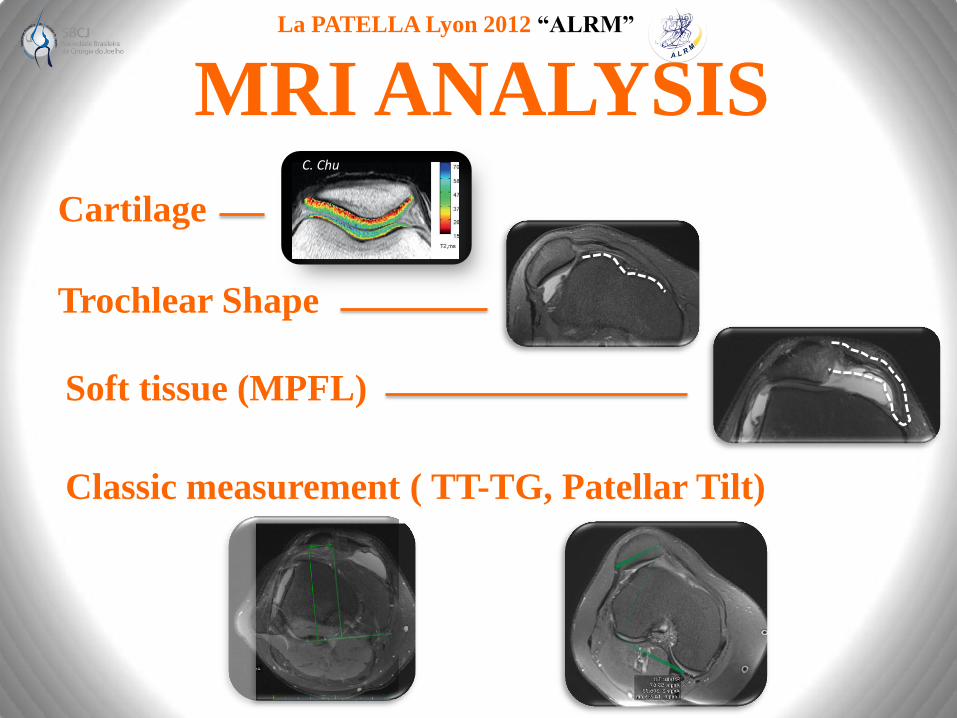
MRI ANALYSIS
Cartilage
Trochlear Shape
Soft tissue (MPFL)
Classic measurement ( TT-TG, Patellar Tilt)
C. Chu
La PATELLA Lyon 2012 “ALRM”
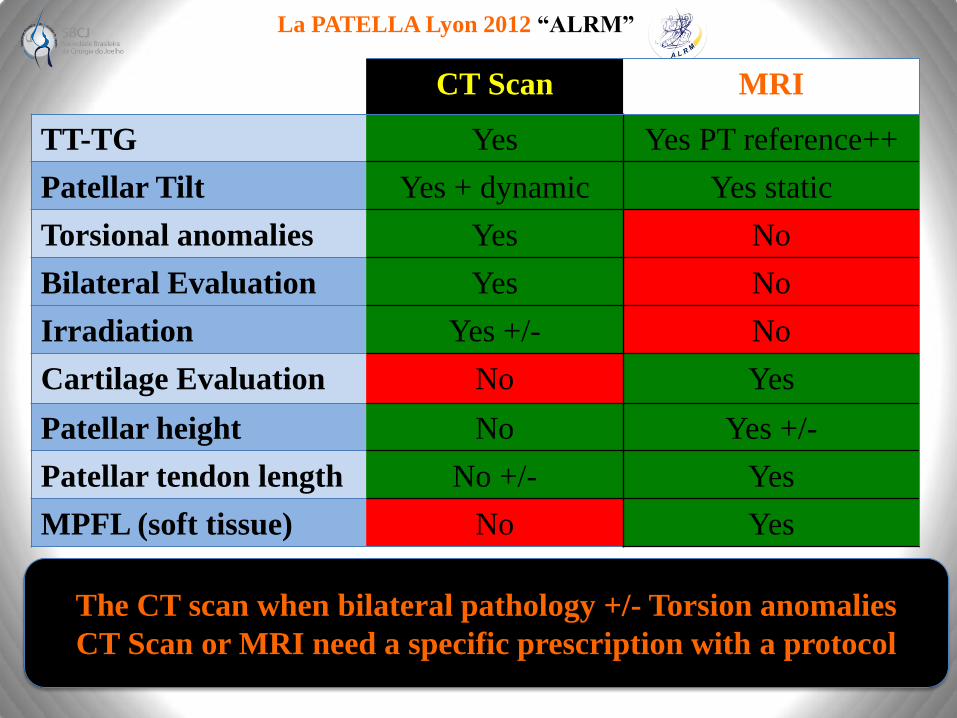
CT Scan MRI
TT-TG Yes Yes PT reference++
Patellar Tilt Yes + dynamic Yes static
Torsional anomalies Yes No
Bilateral Evaluation Yes No
Irradiation Yes +/- No
Cartilage Evaluation No Yes
Patellar height No Yes +/-
Patellar tendon length No +/- Yes
MPFL (soft tissue) No Yes
The CT scan when bilateral pathology +/- Torsion anomalies
CT Scan or MRI need a specific prescription with a protocol

La PATELLA Lyon 2012 “ALRM”
1987 Instability factors ?
Trochlear dysplasia :
Patella Alta :
TT - TG:
Patellar Tilt :
YES
YES
YES
YES
Resulting factor of all the others
2012 Instability factors = 3
NO

La PATELLA Lyon 2012 “ALRM”
2012 Surgical Algorithm …
VMO Plasty + LR
for the Patellar Tilt
MPFL isolated or combined
Lateral release if : Medial Tilt test negative
“Possible option”
All cases

La PATELLA Lyon 2012 “ALRM”
MPFL has to be reconstruct
Restore “torn anatomy”
Primary restraint
Always torn or no competent after the first dislocation
Positioning rules : Fluoroscopy: lateral views+++
Indication for isolated:
C&D < 1.2
Avoid femoral malpositioning
Avoid hypercorrection and fixed patella
Graft: for primary surgery preserve extensor mechanism

La PATELLA Lyon 2012 “ALRM”
TT osteotomy
Correct “abnormal alignment”
Procedure rules :
Prior to MPFL recontrsuction
No over correction
CT or MRI mandatory : objective measurement
Medialization 10 mm < TT-TG <15 mm
2
1

La PATELLA Lyon 2012 “ALRM”
Distalization index C&D = 1
TT osteotomy
Correct “abnormal height”
Procedure rules :
Adapted to trochlear shape
Prior to MPFL reconstruction
La PATELLA Lyon 2012 “ALRM”
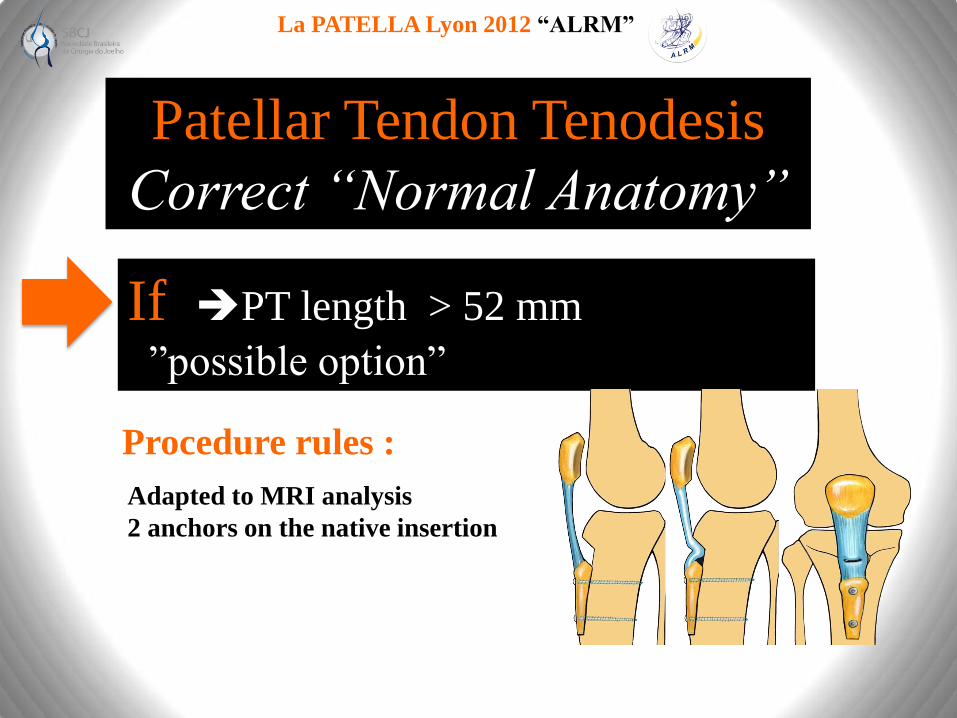
If PT length > 52 mm
“”possible option”
Patellar Tendon Tenodesis
Correct “Normal Anatomy”
Procedure rules :
Adapted to MRI analysis
2 anchors on the native insertion

La PATELLA Lyon 2012 “ALRM”
Proximal realignment + prominence removal Dysplasia Type B or D
Abnormal patellar tracking
1987
2012
Deepening Trochleoplasty
Restore“Normal Anatomy”
La PATELLA Lyon 2012 “ALRM”
2012
Patellofemoral
Arthritis

La PATELLA Lyon 2012 “ALRM”
Key Questions to the patient
PreviousTrauma Type of surgery
Infection
Mobilisation
Patella dislocation +++ Surgery ?
Operating report, X rays…
Swelling knee Hemarthrosis
Chondrocalcinosis XR

La PATELLA Lyon 2012 “ALRM”
Note : Control population 3 % Patellar instability pop. 96 %
Anti Maquet effect
Predisposing factors
Trochlear dysplasia 78 %

La PATELLA Lyon 2012 “ALRM”
Isolated PF OA Aetiologies ...
Chondrocalcinosis 9 %
“Primary arthritis”
No orthopedic history
49 %
“Instability arthritis”
Dislocation history
33 %
Post - trauma 9 %

La PATELLA Lyon 2012 “ALRM”
Patelloplasty Patella Magna - Post traumatic
Osteophyte resection, global remodelling

La PATELLA Lyon 2012 “ALRM”
Natural History Isolated patellofemoral arthritis
18 years
Slow evolution
Well tolerated
La PATELLA Lyon 2012 “ALRM”
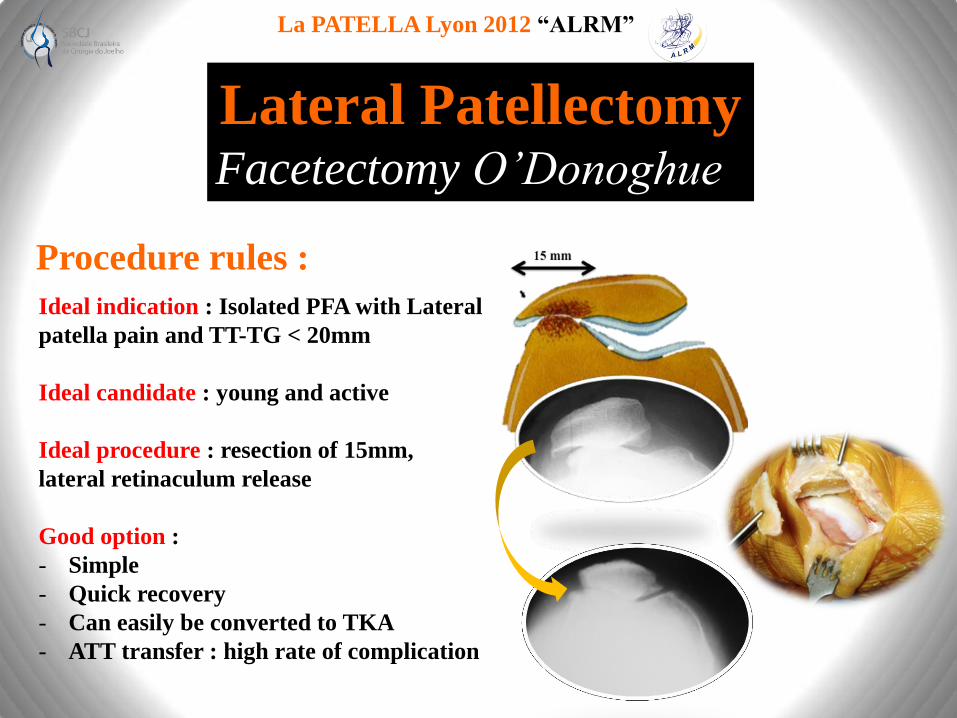
Lateral Patellectomy Facetectomy O’Donoghue
Procedure rules :
Ideal indication : Isolated PFA with Lateral
patella pain and TT-TG < 20mm
Ideal candidate : young and active
Ideal procedure : resection of 15mm,
lateral retinaculum release
Good option :
- Simple
- Quick recovery
- Can easily be converted to TKA
- ATT transfer : high rate of complication
La PATELLA Lyon 2012 “ALRM”
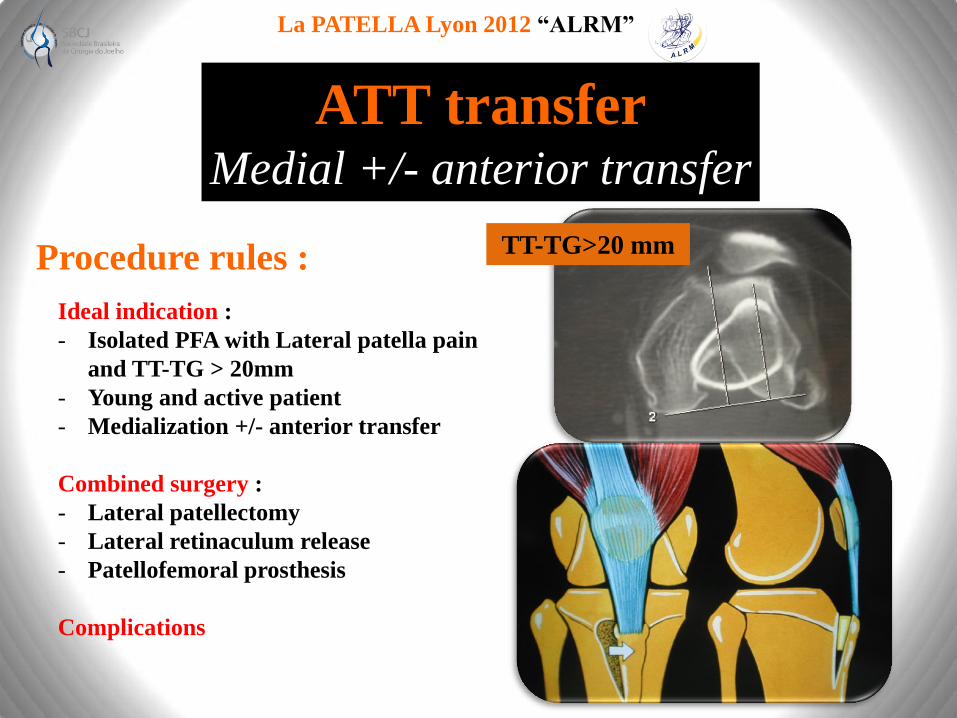
ATT transfer Medial +/- anterior transfer
Ideal indication :
- Isolated PFA with Lateral patella pain
and TT-TG > 20mm
- Young and active patient
- Medialization +/- anterior transfer
Combined surgery :
- Lateral patellectomy
- Lateral retinaculum release
- Patellofemoral prosthesis
Complications
TT-TG>20 mm Procedure rules :

La PATELLA Lyon 2012 “ALRM”
Patellofemoral arthroplasty indications
Procedure rules :
Ideal indication :
- Younger patient
- Active patient
- “Instability osteoarthritis” +++
- Normal femorotibial compartment
Different designs :
- Resurfacing
- Anatomic ++
La PATELLA Lyon 2012 “ALRM”
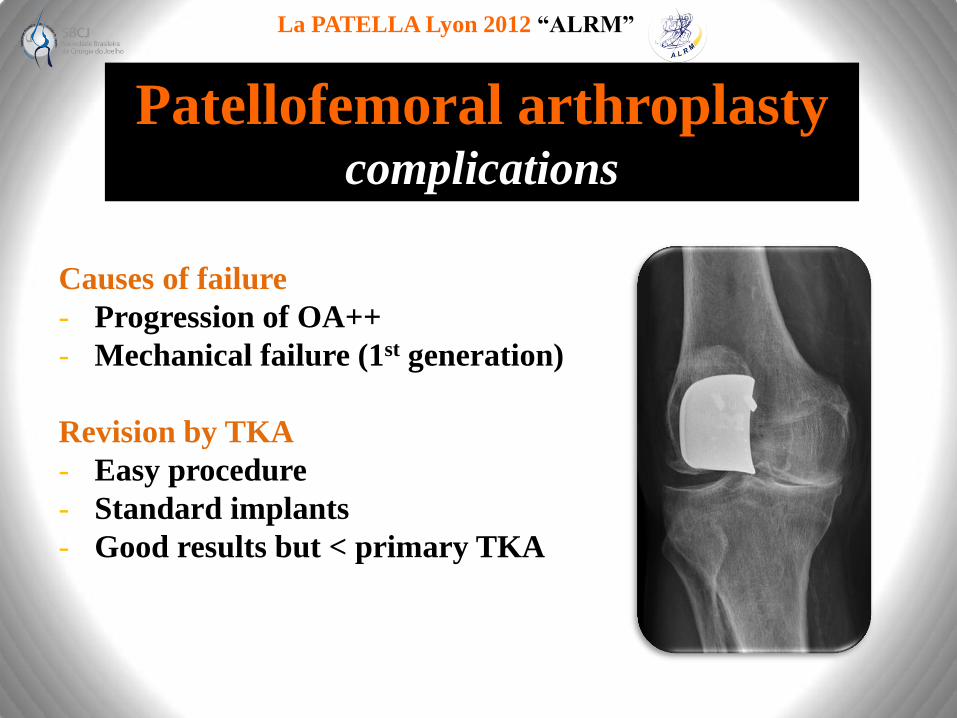
Patellofemoral arthroplasty complications
Causes of failure
- Progression of OA++
- Mechanical failure (1st generation)
Revision by TKA
- Easy procedure
- Standard implants
- Good results but < primary TKA
La PATELLA Lyon 2012 “ALRM”
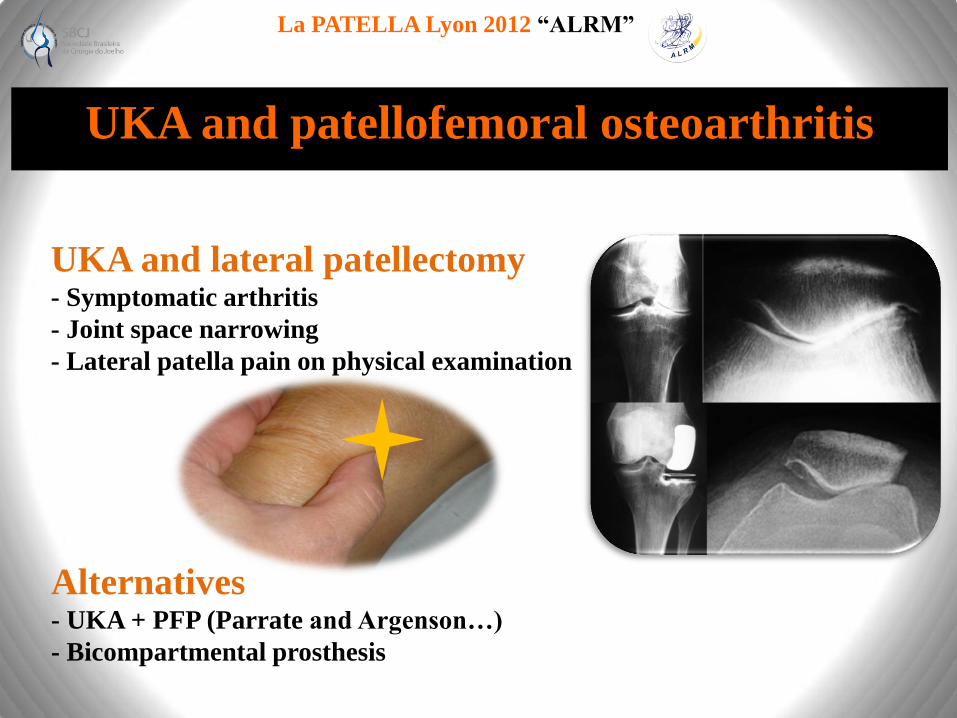
UKA and patellofemoral osteoarthritis
UKA and lateral patellectomy - Symptomatic arthritis
- Joint space narrowing
- Lateral patella pain on physical examination
Alternatives - UKA + PFP (Parrate and Argenson…)
- Bicompartmental prosthesis
La PATELLA Lyon 2012 “ALRM”
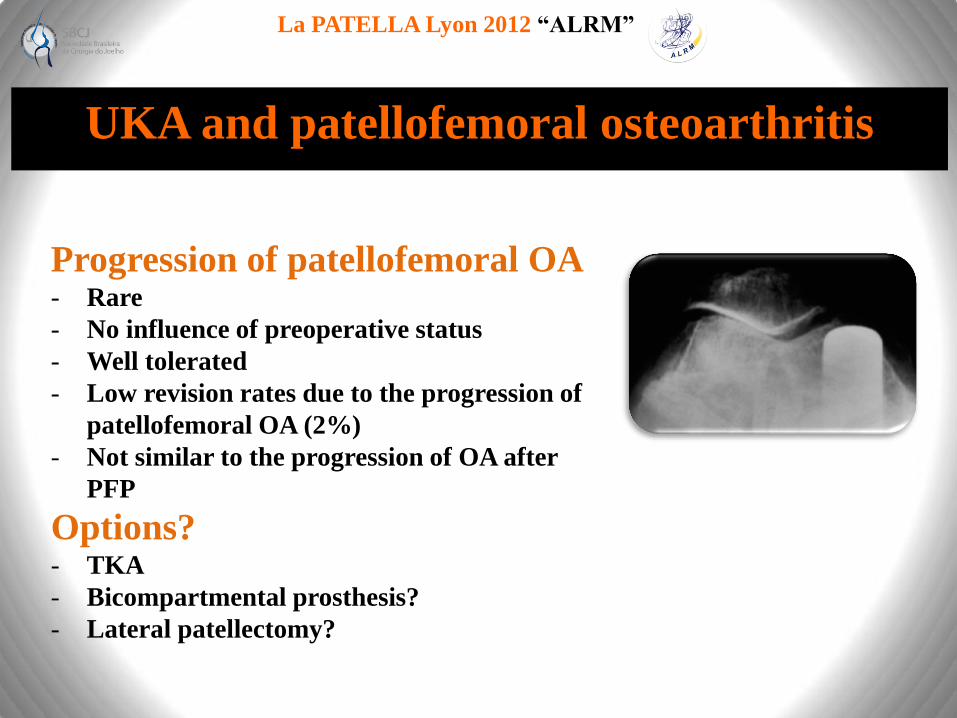
UKA and patellofemoral osteoarthritis
Progression of patellofemoral OA - Rare
- No influence of preoperative status
- Well tolerated
- Low revision rates due to the progression of
patellofemoral OA (2%)
- Not similar to the progression of OA after
PFP
Options? - TKA
- Bicompartmental prosthesis?
- Lateral patellectomy?

La PATELLA Lyon 2012 “ALRM”
2012 Extensor Mechanism
La PATELLA Lyon 2012 “ALRM”
Stretching & Cycling
“Plat du jour”
Anterior knee pain
1987

Anterior Knee
Pain
2012
FONCTIONNAL
STRUCTURAL
ANATOMICAL
NEUROLOGIC

La PATELLA Lyon 2012 “ALRM”
X-Rays & MRI
“Le Menu s’il vous plait?”
Anterior knee pain
2012
Structural problems
La PATELLA Lyon 2012 “ALRM”
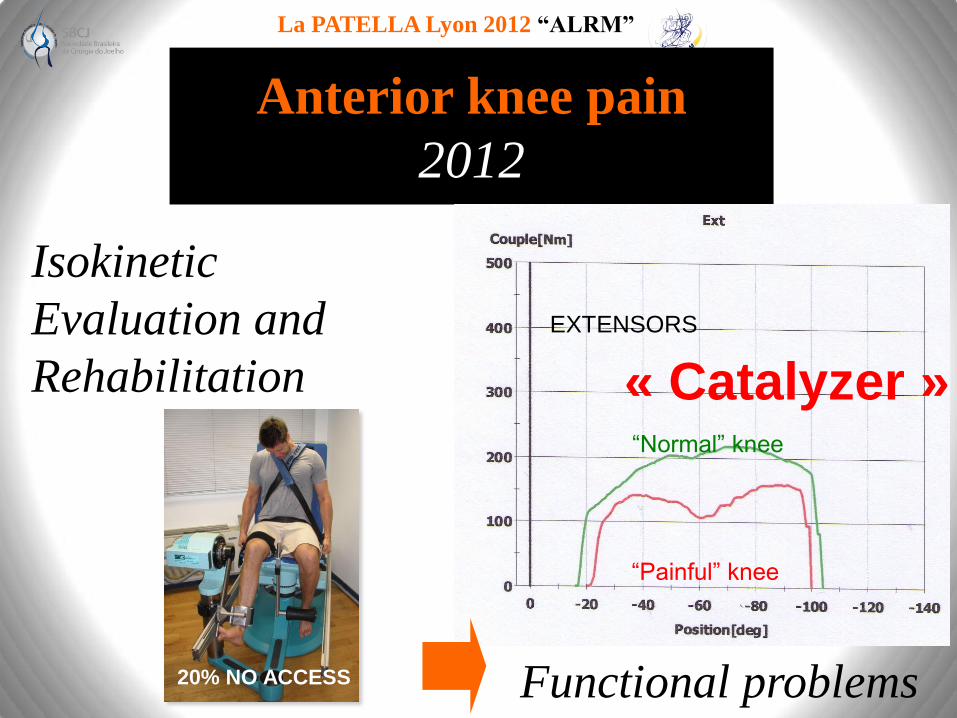
Anterior knee pain
2012
Functional problems
EXTENSORS
“Normal” knee
“Painful” knee
20% NO ACCESS
Isokinetic
Evaluation and
Rehabilitation « Catalyzer »

La PATELLA Lyon 2012 “ALRM”
New medical
treatment in 2012 Platelet Rich Plasma
Under US control
After failed classical treatment
- Analgesics, NSAIs, cryotherapy…
- Eccentric strengthening (Stanish)
- Repeat the procedure!
Patellar tendinosis
La PATELLA Lyon 2012 “ALRM”
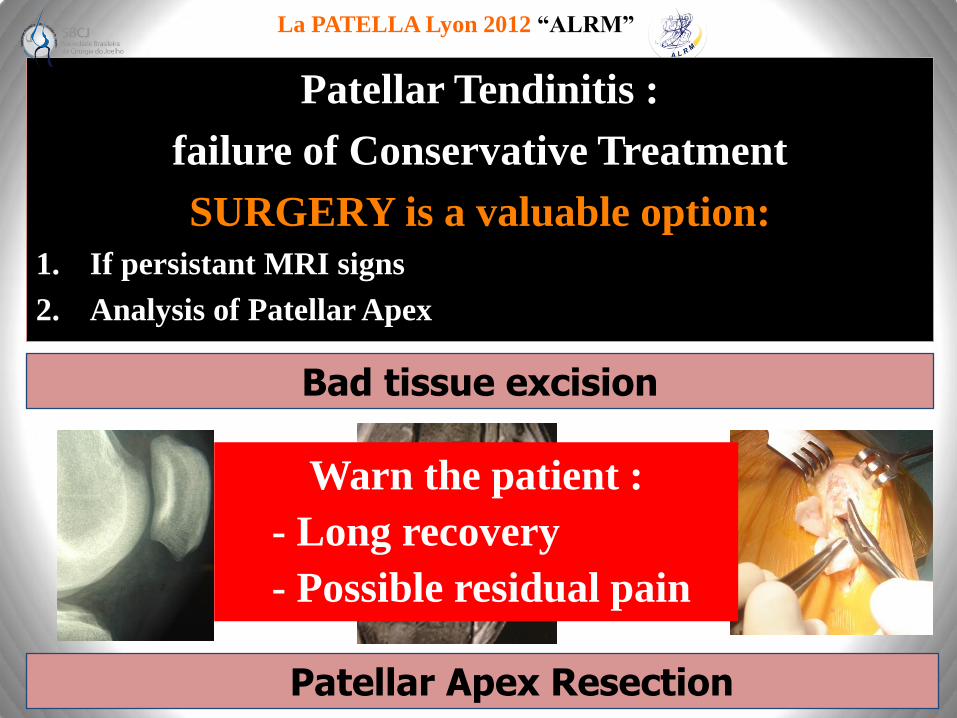
Bad tissue excision
Patellar Tendinitis :
failure of Conservative Treatment
SURGERY is a valuable option:
1. If persistant MRI signs
2. Analysis of Patellar Apex
Patellar Apex Resection
Warn the patient :
- Long recovery
- Possible residual pain

La PATELLA Lyon 2012 “ALRM”
New surgical
treatment in 2012
In case of failure
Patellar tendinosis
Arthroscopic debridement
Safe and efficient (but >6 months+++)
- No nerve complication (Open 50%)+++

La PATELLA Lyon 2012 “ALRM”
CONCLUSION

La PATELLA Lyon 2012 “ALRM”
Enjoy this delicious “menu à la carte” from Lyon
with international flavours …
Have a nice trip back… you are always welcome to LYON
The LSKS ‘s Team …
La PATELLA Lyon 2012 “ALRM”
Next ….”Rendez-vous”
16 -18
Octobre
2014

3 Dates … With
October 16 -18
2014
June 7 -11
2015
May 4 -7
2016