2006 coding guidelines and policy update -
TRANSCRIPT

20
06
Codin
gG
uid
elin
esa
ndP
olicy
Update
Com
pendiu
m
w
ww
.am
erih
ealth
.com
Important Note:
The medical policies referenced in this document apply to all HMO, POS, and PPO products of AmeriHealth, including its affiliates, as well as to traditional indemnity products to the extent the applicable covered services are underwritten by AmeriHealth or its affiliates. This document was developed to assist AmeriHealth in administering the provisions of its benefits programs and does not constitute medical advice. Professional providers are responsible for providing medical advice and treatment. Even though this document may conclude that a particular service or item is medically necessary, such conclusion is NOT based upon the terms of a particular member’s benefit plan. Members must refer to their specific benefit program for the terms, conditions, limitations and exclusions of coverage. Please note that the Policy Bulletins which are referenced herein describe the status of a specific topic at the time the Policy Bulletin was created. Policy Bulletins are updated biennially and when new medical evidence becomes available, therefore, they are subject to change. Please be aware that the actual Policy Bulletins which are discussed herein are used as a guide only. Coverage decisions are made on a case-by-case basis by applying Policy Bulletin criteria to the member’s medical history, condition, and proposed course of treatment as well as the member’s benefit program. Providers should review Policy Bulletins with Members as treatment options are discussed, as the Policy Bulletins are designed to be used by our professional staff in making coverage determinations and can be highly technical. Information contained in this document and the actual Policy Bulletin does not constitute an offer of coverage, medical advice, or guarantee of payment. Please note that, if there is a conflict between the Policy Bulletin and a member’s benefit program, the terms of the benefit program will govern.Please note that providers who opted out of the class action settlement may not be entitled to certain claim payment policy changes. Therefore, any payments made pursuant to such policy changes to providers who opted out of the class action settlement are subject to retroactive adjustments.
2006CodinGGUidelinesAndPoliCyUPdAte
CoMPendiUMwww.amerihealth.com
Table of CoNTeNTs
View full Policies online Full descriptions of these policies are available online: www.amerihealth.com/medpolicy.
Introduction..........................................3 About the Coding Guidelines and
Policy Update (CGPU) Compendium ....3 What are the Primary Reasons that
AmeriHealth Develops Claim Payment and Medical Policies? ...........3
Physician Volunteers Needed to Assist in Developing Medical Policies ................................................3
Medical.Policies.Covered:.According.to.Certain.Criteria.....................................5
Medical.Policies.Not.Covered:.Considered.Experimental/Investigational.................21
Claim.Payment.Policies........................27
2006.Articles........................................31 ICD-9 CM Diagnosis Codes
Change for Routine Gynecological Exams ...............................................32
Billing for Neonatal Hearing Screening Should be Directed to Facility ..........................................32
Anesthesia Claims Update ................32 Gardasil® Approved by the FDA .....32 Clarifications to the Intensity
Modulated Radiation Therapy Policy ................................................33
Class.Action.Settlement.Update...........35 Enhancements to Claim Payment
Policy, Processing and Payment Disclosure, and an Appeals Process for Class Action Settlement Providers ...........................................36
Assistant Surgery Modifiers 80, 81, 82 ...........................................36
Co-Surgery Modifier 62 ...................37
Medical.Code.Updates.........................39 CPT® Codes ....................................40 HCPCS Codes .................................62 ICD-9 CM Codes ............................90
AmeriHealth HMO, Inc. • QCC Insurance Company, d/b/a AmeriHealth Insurance Company • AmeriHealth Insurance Company of New Jersey
�
GR A P HIC COMMUNICATIONS
I N T E R N AT I O N A L U N I O N
UNION LABEL® 526-M

www.amerihealth.com/providers/communications �
AbouttheCodingGuidelinesandPolicyUpdate(CGPU)Compendium
Over the past year, AmeriHealth has published four Coding Guidelines and Policy Update (CGPU) newsletters.
This 2006 Coding Guidelines and Policy Update Compendium is a collection of relevant policy summaries that have been published in CGPU during the past year. We are not able to reproduce all of the CGPU summaries in the Compendium because some policies have undergone updates and revisions since their initial publication in CGPU; however, these updated policies will appear in future issues of CGPU. We encourage you to visit www.amerihealth.com/providers for expanded, up-to-date versions of each policy.
In addition to the descriptions of policies previously published in the CGPU, the Compendium has also expanded the normal CGPU parameters to include articles on coding and policy, plus a section detailing new, revised, and deleted CPT®*, HCPCS, and ICD-9 CM codes.
This Compendium contains information that you can immediately adopt within your practice to simplify your information retrieval and claims submission processes.
*Current Procedural Terminology (CPT®) is a copyright of the American Medical Association (AMA). All Rights Reserved. No fee schedules, basic units, relative values, or related listings are included in the CPT. The AMA assumes no liability for the data contained herein. Applicable FARS/DFARS restrictions apply to government use. CPT® is a trademark of the AMA.
WhatArethePrimaryReasonsThatAmeriHealthDevelopsClaimPaymentandMedicalPolicies?
Some of the primary reasons that AmeriHealth develops claim payment and medical policy are to:
• Comply with legislation (e.g., federal, state, and local legislative mandates).
• Correspond to national or local Medicare Carrier Coverage Policy.
• Allow consistent interpretation and application of benefits.
• Respond to requests for new, emerging technology or changes in existing technology.
• Ensure a relevant and timely scheduled review of existing policies.
• Provide claims submission policies and procedures.
PhysicianVolunteersNeededtoAssistinDevelopingMedicalPolicies
AmeriHealth is currently recruiting physicians to join our Policy Committee Advisory Panel. This panel is responsible for evaluating the scientific evidence and local standards of care addressed in our medical policies.
Medical policies are research-based documents that allow AmeriHealth to evaluate the medical necessity of services, devices, biologics, and procedures for its members. In addition, medical policies provide guidelines for obtaining benefits and reimbursement in accordance with a member’s plan. As a volunteer consultant on the Policy Committee Advisory Panel, you will evaluate proposed medical policies based on your area(s) of expertise. As such, your contributions will significantly impact the care of patients in your region.
At this time, AmeriHealth is seeking physician consultants in the following specialties:
• Neurosurgery• Orthopedics• Urology• Vascular Surgery• Physical Medicine and Rehabilitation• Rheumatology• Cardiology• Gastroenterology• Pain Medicine
INTRODUCTION
Visit www.amerihealth.com/medpolicy to get the most current, in-depth and up-to-date information on policies affecting health care in your region. Review and accept the terms & conditions, and you can quickly and easily search all active policies. Bookmark this site and check back regularly for the latest information and updates.
The 2006 CGPU Compendium can be found at www.amerihealth.com/providers/communications. You can also check the website to find specific billing codes, in-depth descriptions of services, or other policy-related data.
43034txtAH.indd 3 2/19/07 2:43:02 PM

�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
To qualify as a member of the Policy Committee Advisory Panel, you must:
• Maintain board certification for each specialty or subspecialty for which you wish to consult.
• Maintain an active clinical practice in each specialty or subspecialty for which you wish to consult.
• Understand and agree to adhere to our confidentiality statement.
• Maintain a high ethical standard, evidenced by the absence of any AmeriHealth investigation into personal or group claims practices.
• Complete and sign a Conflict of Interest Statement and Confidentiality Agreement prior to becoming a member of the advisory panel.
If you meet the above criteria and have an interest in sharing your expertise as a member of the Policy Committee Advisory Panel, please submit your curriculum vitae to:
Gerald W. Peden, M.D., M.A.Senior Medical DirectorClaim Payment Policy DepartmentAmeriHealth1901 Market StreetPhiladelphia, PA 19103-1480
ViewFullPoliciesonline
Full descriptions of these policies are available online at: www.amerihealth.com/medpolicy.
43034txtAH.indd 4 2/19/07 2:43:02 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
Medical Policies covered: according to certain criteria
www.amerihealth.com
Table of ConTenTs
www.amerihealth.com/providers/communications �
Ambulatory Blood Pressure Monitoring (ABPM) (07.02.09) ................................................................6
Blepharoplasty with or without a Brow Lift/Repair of Blepharoptosis (11.05.02c) .................................................6
Bone Growth Stimulators (05.00.09c) ...................................7
High-Frequency Chest Wall Oscillation Devices (05.00.14c) ................................................................9
Home Phototherapy for Neonatal Jaundice (07.06.02) ........9
Hospital Beds and Accessories (05.00.56a) .........................10
Islet Cell Transplantation (11.04.01) ..................................12
Maze Procedure (11.02.20a) ...............................................12
Medical Evaluation and Management for Attention-Deficit Hyperactivity Disorder ADHD) (07.03.03b) ............................................................13
Negative Pressure Wound Therapy (NPWT) Pump (05.00.38a) ................................................................13
Outpatient Speech Therapy (10.06.01a) ............................15
Reduction Mammaplasty (11.08.02c) ..................................17
The BOSTON® Scleral Lens (07.13.11) ........................... 18
Trigger Point Injections (11.14.02c) ................................... 19
43034txtAH.indd 5 2/19/07 2:43:02 PM

6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
Medical Policies Covered: According to certAin criteriA
AmbulatoryBloodPressureMonitoring(ABPM)(07.02.09)covered: According to certAin criteriA
Ambulatory blood pressure monitoring (ABPM) involves the use of a noninvasive device that measures blood pressure in 24-hour cycles. The device consists of a portable sphygmomanometer attached to a recording device. The information it provides can help a physician determine whether an individual is truly hypertensive or is exhibiting white coat hypertension (WCH).
The ABPM device is fitted to and removed from the individual by a trained technician. The sphygmomanometer inflates at predetermined times, generally every 30 minutes, and the blood pressure recorded at each inflation is stored. The individual performs normal activities while wearing the monitor. Automated ABPM is considered more accurate than individual self-monitoring. Therefore, it is generally thought that readings obtained at frequent intervals throughout the day and night would help the physician better manage the individual’s care. These stored 24-hour measurements are later interpreted at the physician’s office. A clinician is required to interpret the collected data by uploading it onto a computer where device-specific programs are used to categorize and analyze the measurements.
ABPM is considered medically necessary for individuals who meet the definition criteria of WCH and have no evidence of end-organ damage. ABPM is covered for individuals requiring 24-hour monitoring of their blood pressure to confirm the diagnosis.
Physician interpretation is medically necessary and required for reimbursement. Therefore, ABPM utilizing a system such as magnetic tape and/or computer disk, for 24 hours or longer, with recording only or scanning analysis with report only (no mention of physician interpretation), is not eligible for separate reimbursement when billed alone or in conjunction with another service.
When a primary care physician (PCP) is contracted to provide medically necessary and preventive care services on a monthly capitation basis, this service is included in the monthly capitation payment.
Originally published in Winter 2006 CGPU.
BlepharoplastywithorwithoutaBrowlift/RepairofBlepharoptosis(11.05.02c)covered: According to certAin criteriA
Blepharoptosis is the condition of droopiness of the upper eyelid due to underlying eye muscle dysfunction (e.g., levator muscle or Muller’s muscle). Surgical repair of this condition, including repair of the eye muscle, is performed in conjunction with the blepharoplasty procedure.
A blepharoplasty procedure includes the removal of redundant skin of the upper and/or lower eyelids and the removal of protruding periorbital fat. This procedure can be performed for either cosmetic or reconstructive purposes. When performed for cosmetic reasons, the surgery reshapes eye-related structures in order to improve appearance and self-esteem; when provided as part of a reconstructive procedure, the surgery reshapes eye-related structures in order to improve functional ability. Blepharoplasty can be performed alone or in conjunction with other procedures such as a brow lift.
Under most circumstances, a blepharoplasty with or without a brow lift and/or repair of blepharoptosis is a cosmetic service and a benefit contract exclusion. However, each of these procedures is medically necessary when performed as functional or reconstructive surgeries in certain clinical situations.
BlepharoplastyBlepharoplasty is medically necessary when performed to correct:
• Prosthetic difficulties in an anophthalmic (without an eye) socket.
• Disorders of visual impairment caused by redundant skin of the eyelid or eyebrow that include, but are not limited to:
- Visual impairment due to dermatochalasis, blepharochalasis, or ptosis of the eyelid.
- Symptomatic, redundant skin that is resting on the upper lashes.
- Chronic, symptomatic dermatitis of pretarsal skin caused by redundant upper eyelid skin.
Lower eyelid blepharoplasty is generally not medically indicated to treat conditions that cause visual field
43034txtAH.indd 6 2/19/07 2:43:02 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �
obstruction because the lower eyelids are not usually associated with visual impairment. In the absence of visual impairment, lower eyelid blepharoplasty is considered a cosmetic service and, therefore, not covered.
Requests for lower eyelid blepharoplasty are considered on an individual basis when documentation (including the individual’s chief complaint and preoperative photographs) demonstrates that the procedure is medically necessary for reconstructive reasons.
Blepharoptosis RepairBlepharoptosis repair is medically necessary when performed as functional/reconstructive surgery to correct a visual impairment due to drooping or displacement of the upper eyelid.
Brow Ptosis RepairBrow ptosis repair is medically necessary when performed as functional/reconstructive surgery to correct either of the following:
• Visual impairment due to droop or displacement of the brow.
• Brow malposition that would prevent adequate correction of dermatochalasis, blepharochalasis, or blepharoptosis.
Documentation RequirementsAll requests for any of the procedures listed above require a letter of medical necessity that describes the individual’s chief complaints and that justifies the need for surgery to correct the functional impairment. Additionally, when blepharoplasty is to be performed as a functional/reconstructive surgery to correct visual impairment, the following additional documentation is required:
• Preoperative color photographs that include a view of the individual: in forward gaze, looking up, and looking down, and that demonstrate one or more of the following:
- The upper eyelid margin is within 2.5 mm (one-fourth of the diameter of the visible iris) of the corneal light reflex (margin-to-reflex distance [MRD] less than 2.5 mm) with the individual in primary gaze.
- The upper eyelid skin rests on the eyelashes.
- The upper eyelid indicates the presence of dermatitis.
- The upper eyelid position contributes to difficulty tolerating a prosthesis in an anophthalmic socket.
- The brow position is below the superior orbital rim.
• A written interpretation of the results of both the taped and untaped automated visual field studies must be submitted and must demonstrate one of the following:
- The upper visual field has improved by at least eight degrees or 20 percent with the eyelid taped as compared with the visual field obtained without taping (two sets of visual fields are required).
- Visual field obstruction by the eyelid limits the upper visual field to within 30 degrees of fixation.
If both a blepharoplasty and a brow ptosis repair are planned, the need for both must be documented. This requires photographs showing the affect of the drooping, redundant skin; the skin resting on the upper eyelid; the presence of dermatitis; or the actual presence of blepharoptosis.
Originally published in Fall 2006 CGPU.
BoneGrowthstimulators(05.00.09c)covered: According to certAin criteriA
Noninvasive bone growth stimulators consist of an external power supply and externally applied coils or a transducer that generate a weak electrical current through the site where bone growth is desired. Noninvasive devices use pulsed electromagnetic fields (PEMFs), capacitative coupling, or combined magnetic fields technology to generate the current. Ultrasonic bone growth stimulators are noninvasive devices that accelerate fracture healing by emitting low-intensity, pulsed ultrasound signals on the skin surface over the fracture site. Ultrasonic bone growth stimulators are used in conjunction with cast immobilization.
Electrical bone growth stimulators are used for nonunion fracture(s) of long bone, which is defined by Medicare to include the following: the clavicle, humerus, radius, ulna, metacarpal, femur, tibia, fibula, malleolus, and metatarsal. Studies of bone growth stimulators in the treatment of fresh fractures (less than seven days) and in delayed union and nonunion fractures of both long and short bone indicate
43034txtAH.indd 7 2/19/07 2:43:02 PM

�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
that insufficient scientific evidence exists to demonstrate the effectiveness of electrical bone growth stimulators in fresh and delayed union fractures. In addition, the safety and effectiveness of electrical bone growth stimulators in individuals under the age of 17 has not been established in clinical trials.
Electrical bone growth stimulators (noninvasive/invasive) are considered medically necessary and, therefore, covered for individuals 17 years of age or older when one of the following conditions is present:
• A fracture secondary to congenital pseudarthrosis (755.8).
• A nonunion fracture (733.82) of a long bone (includes the following: the clavicle, humerus, radius, ulna, metacarpal, femur, tibia, fibula, malleolus, metatarsal).
- Nonunion fracture is defined as the point at which healing has stopped (three months or greater from the initial fracture) and further healing (as evidenced by serial radiographic documentation) has ceased.
• A failed joint fusion.
- Post-surgical joint fusion failure is defined as radiologic documentation of nonunion nine months or more after surgical fixation of the fracture.
Electrical bone growth stimulators (noninvasive/invasive) are considered medically necessary and, therefore, covered following spinal surgery (V45.4) when one of the following criteria is met:
• A failed spinal fusion when the surgery was performed a minimum of nine months from the last surgery.
• A multilevel spinal fusion surgery (e.g., L3-L5, L4-S1, etc.).
• Revisional spinal fusion surgery due to a previously failed spinal fusion at the same level.
Unless any exclusion criteria exists, low-intensity ultrasonic bone growth stimulators (noninvasive) are considered medically necessary and, therefore, covered for any of the following:
• Fresh (less than seven days), closed or Grade l open, tibial diaphysis fracture (823.20, 823.30) when used as an adjunct to closed reduction and cast immobilization.
• Fresh, closed fracture of the distal radius (Colles fracture [813.41, 813.42]) when used as an adjunct to closed reduction and cast immobilization.
• Nonunion fractures (733.82) of the clavicle, scapula, humerus, radius, ulna, carpal, metacarpal, phalanges (fingers or toes), femur, patella, tibia, fibula, malleolus, talus, calcaneus, cuboid, navicular, cuneiform, tarsal, metatarsal, rib(s), sternum, and pelvis.
- Nonunion fracture is defined as the point at which healing has stopped (three months or greater from the initial fracture) and further healing (as evidenced by serial radiographic documentation) has ceased.
If one or more of the following exclusion criteria exist, low-intensity ultrasonic bone growth stimulators are considered experimental/investigational and, therefore, not covered because the safety and/or efficacy of this device for these conditions cannot be established by review of the available published literature:
• For a fracture of the skull or vertebrae.
• For a fracture that is tumor-related.
• For concurrent use with any other noninvasive osteogenic stimulator.
• In individuals under the age of 17.
• For a fresh fracture other than one of the tibial diaphysis or distal radius.
• For a delayed union fracture (a recent fracture [three months or less from the initial fracture], where healing has not advanced at the “average” rate for the location and type of fracture).
For all other indications, electrical bone growth stimulators and low-intensity ultrasonic bone growth stimulators are considered experimental/investigational and, therefore, not covered because the safety and/or efficacy of these devices cannot be established by review of the available published literature. Examples of other indications include, but are not limited to: individuals under the age of 17, fresh fractures (except ultrasonic stimulator use for fractures of the tibial diaphysis or distal radius), and delayed union fractures.
Originally published in Fall 2006 CGPU.
43034txtAH.indd 8 2/19/07 2:43:02 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �
High-FrequencyChestWalloscillationDevices(05.00.14c)covered: According to certAin criteriA
A high-frequency chest wall oscillation device is designed to enhance the mobilization of bronchial secretions. The device is an inflatable vest that is connected by two tubes to a small air-pulse generator. Oscillating positive air pressure causes the vest to inflate and deflate up to 25 times a minute, creating a vibratory motion that aids in the mobilization of secretions. The action of the device creates mini-coughs that dislodge mucus from the bronchial walls, thus increasing mobilization of the mucus toward the central airways. The oscillating action also thins the secretions and makes them easier to remove by coughing or suctioning. High-frequency chest wall oscillation devices can be used for individuals who have cystic fibrosis or bronchiectasis and require chest physiotherapy, manual chest percussion, postural drainage, and device-assisted coughing to help them clear their lungs.
A four- to six-week trial of a high-frequency chest wall oscillation device is considered medically necessary and, therefore, covered for the treatment of individuals with a documented history that confirms a failure of standard treatments (e.g., manual chest percussion, postural drainage) to adequately mobilize retained bronchial secretions and one of the following diagnoses:
• Cystic fibrosis.
• Bronchiectasis, confirmed by computed tomography (CT) scan, and documentation of one of the following:
- Daily productive cough for at least six continuous months.
- Frequent (i.e., more than two per year) exacerbations of respiratory infection requiring antibiotic therapy.
Continued coverage of the device after the trial is considered medically necessary and, therefore, covered when the effectiveness of the device has been demonstrated by:
• Documentation that the device has been used daily or as prescribed.
• Documentation of increased expectoration of mucus.
If the trial of the device is successful and the individual wishes to continue using the device, continued authorization for the device must be obtained. The ordering physician must provide a letter of medical necessity to the Company stating compliance with the above requirements.
High-frequency chest wall oscillation devices for any diagnosis other than cystic fibrosis or bronchiectasis are considered not medically necessary and, therefore, not covered because the available published literature does not support the use of this device for the treatment of any other diagnosis.
Originally published in Fall 2006 CGPU.
HomePhototherapyforNeonatalJaundice(07.06.02)covered: According to certAin criteriA
Phototherapy is often used to treat neonatal jaundice and involves the continuous application of ultraviolet light via a lamp or a fiberoptic system to a newborn for a prescribed period of time. The fiberoptic system consists of a pad of woven fibers that transport light from a light source to the baby. This covered fiberoptic pad is placed directly against the baby to bathe the skin in light. Phototherapy uses blue wavelengths of light to convert the bilirubin to less toxic water-soluble photoisomers, which are then excreted in bile and urine. Phototherapy can be administered in a hospital or home setting (home phototherapy). It is important to note that the use of phototherapy in the home setting is contraindicated in the presence of risk factors.
Home phototherapy devices do not consistently provide the same degree of irradiance as those available in the hospital. Due to the questionable efficiency of home phototherapy for neonatal jaundice, the American Academy of Pediatrics states that home phototherapy is considered inappropriate for infants with higher bilirubin concentrations.
Home phototherapy is considered medically necessary for full-term newborns who are diagnosed with neonatal jaundice and have none of the risk factors, major or minor, that have been identified by the American Academy of Pediatrics.*
The following are major risk factors that have been identified by the American Academy of Pediatrics for the development of severe hyperbilirubinemia in infants of 35 weeks or more gestation:
• Predischarge total serum bilirubin (TSB) or transcutaneous bilirubin (TcB) level in the high-risk zone.
• Jaundice observed within the first 24 hours.
43034txtAH.indd 9 2/19/07 2:43:03 PM

10Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
• Blood group incompatibility with positive direct antiglobulin test, other known hemolytic disease (e.g., glucose-6-phosphate-dehydrogenase [G6PD] deficiency), elevated end tidal carbon monoxide (ETCOc).
• Gestational age 35-36 weeks.
• Previous sibling received phototherapy.
• Cephalohematoma or significant bruising.
• Exclusive breastfeeding, particularly if nursing is not going well and weight loss is excessive.
• East Asian race.
The following are minor risk factors identified by the American Academy of Pediatrics for the development of severe hyperbilirubinemia in infants of 35 weeks or more gestation:
• Predischarge TSB or TcB level in the high intermediate-risk zone
• Gestational age 37-38 weeks
• Jaundice observed before discharge
• Previous sibling with jaundice
• Macrosomic infant of a diabetic mother
• Maternal age of 25 years or more
• Male gender
*Reproduced with permission from Pediatrics, Vol. 114, Pages 297-316, Copyright © 2004 by the American Academy of Pediatrics (AAP).
Originally published in Winter 2006 CGPU.
HospitalBedsandAccessories(05.00.56a)covered: According to certAin criteriA
A hospital bed is a bed with head and leg elevation and height adjustment features that are used to assist individuals who require adjustment or repositioning to alleviate pain, prevent contractures, prevent respiratory infections, and to allow individuals to transfer to and from bed with increased independence.
Hospital bed accessories are additions to a bed that are not provided as part of the original bed. Accessories that may be needed for the essential functioning of the hospital bed in
relation to the individual’s condition include trapeze bars, bed cradles, or side rails.
Medically NecessaryFixed-height Hospital Beds
A fixed-height hospital bed (E0250, E0251, E0290, E0291) is medically necessary when the individual meets one or more of the following medical necessity criteria:
• The individual has a medical condition that requires positioning of the body in ways that are not feasible in an ordinary bed. The elevation of the head/upper body of less than 30 degrees does not usually require the use of a hospital bed.
• The individual requires head elevation of more than 30 degrees most of the time due to congestive heart failure (CHF), problems with aspiration, or chronic pulmonary disease. Pillows or wedges must have been considered and ruled out.
• The individual requires positioning of the body in ways that are not feasible in an ordinary bed to alleviate pain.
• The individual requires traction equipment, which can only be attached to a hospital bed.
Variable-height Hospital Beds
A variable-height hospital bed (E0255, E0256, E0292, E0293) is medically necessary for individuals with severely debilitating diseases and conditions (including, but not limited to severe cardiac conditions, spinal cord injuries, amyotrophic lateral sclerosis [ALS], and multiple sclerosis) when all of the following apply:
• The individual meets one or more of the medical necessity criteria for a fixed-height hospital bed.
• The individual requires a bed height that cannot be attained with a fixed hospital bed and that allows them to be transferred to a chair, wheelchair, or standing position.
Semi-Electric Hospital Beds
A semi-electric hospital bed (E0260, E0261, E0294, E0295) is medically necessary when the individual meets one or more of the medical necessity criteria for a fixed-height hospital bed and both of the following criteria:
• The individual’s condition requires that their body position be changed frequently and/or that their body
43034txtAH.indd 10 2/19/07 2:43:03 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 11
position may be changed immediately when necessary (i.e., no delay can be tolerated).
• The individual is able to operate the controls and cause the adjustments. Exceptions to this requirement can be made in cases of spinal cord injury (SCI) and brain injury.
Heavy-duty Hospital Beds
A heavy-duty hospital bed (E0301, E0303) is medically necessary when the individual meets one or more of the medical necessity criteria for a fixed-height hospital bed and when the individual’s weight exceeds 350 pounds but is less than 600 pounds.
Extra-heavy-duty Hospital Beds
An extra-heavy-duty hospital bed (E0302, E0304) is medically necessary when the individual meets one or more of the medical necessity criteria for a fixed-height hospital bed and when the individual’s weight exceeds 600 pounds.
Pediatric Hospital Beds
A pediatric hospital bed is medically necessary when the individual meets all of the medical necessity criteria for one of the hospital beds specified above.
Not Medically NecessaryTotal Electric Hospital Beds
A total electric hospital bed (E0265, E0266, E0296, E0297) is considered not medically necessary and, therefore, not covered because the electric height adjustment feature does not aid in the treatment of the individual’s condition.
Institutional Hospital Beds
An institutional hospital bed (E0270) is considered not medically necessary and, therefore, not covered because it is deemed inappropriate for home use. These beds include oscillating beds, circulating beds, and Stryker frame beds.
Hospital Bed AccessoriesMedically Necessary
The following hospital bed accessories are considered medically necessary when the individual meets the medical
necessity requirement for the specified bed and meets the additional criteria as indicated below:
• Bed cradle (E0280): When the individual has a medical condition that requires the prevention of contact with bed coverings (i.e., burns, diabetic ulcers, gout).
• Trapeze equipment (E0910, E0940): When the individual requires this device to do any one of the following:
- Sit up because of a respiratory condition.
- Change body position for other medical reasons.
- Get in or out of bed.
• Heavy-duty trapeze equipment (E0911, E0912): When the individual meets both of the following criteria:
- The individual meets the criteria for regular trapeze equipment.
- The individual weighs more than 250 pounds.
• Side rails (E0305, E0310): When the individual’s condition requires that they have bed side rails and the rails are a part of or an accessory to the hospital bed.
Not Medically Necessary
The following hospital bed accessory is considered not medically necessary:
• Trapeze bars (E0910, E0911) will be considered not medically necessary and, therefore, not covered when they are used on an ordinary bed.
Not Primarily Medical In Nature (Benefit Exclusion)
• Safety enclosures (E0316) (nylon netting that encloses the top and sides of a hospital bed) are considered benefit exclusions and, therefore, not covered as these devices are not primarily medical in nature. Additionally, these devices have safety concerns associated with them. For Medicare members, safety enclosures are considered not medically necessary, and, therefore, not covered; these devices have safety concerns associated with them.
• A bed board (E0273, E0315) (a device placed under a mattress to make the mattress firmer) is considered a benefit exclusion and, therefore, not covered because its use is not primarily medical in nature.
• An over bed table (E0274, E0315) is considered a benefit exclusion and, therefore, not covered because its use is not primarily medical in nature.
Originally published in Fall 2006 CGPU.
43034txtAH.indd 11 2/19/07 2:43:03 PM

12Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
isletCellTransplantation(11.04.01)covered: According to certAin criteriA
Islet cell transplant tissue comes from either the patient (autologous transplant) or from a cadaveric donor (allogeneic transplant). Islet cell transplantation may benefit an individual who does not have a functioning pancreas. Currently only individuals with either chronic pancreatitis or type 1 diabetes mellitus have been the subject of clinical investigations.
Autologous islet transplantation is a technique to prevent the serious morbidity of surgical induced diabetes due to the removal of the individual’s pancreas. Although the pancreatectomy and transplant can be performed on two different days, the transplant is generally performed during the pancreatectomy procedure. During the pancreatectomy, a suspension is created by mixing plasma and the isolated islet cells collected from the individual’s own resected pancreatic specimen. This suspension is then injected into the portal vein of the liver, where the cells function as a free graft. There is no risk of rejection because, unlike allogeneic organ/tissue transplants, the individual’s own islet cells are used in the procedure.
Autologous islet cell transplantation is considered medically necessary and, therefore, covered as an adjunct to a total or near-total pancreatectomy in individuals with chronic pancreatitis.
Autologous islet cell transplantation is considered experimental/investigational for all other indications because the safety and/or efficacy of this service cannot be established by review of the available published literature. Therefore, this service is not covered.
Allogeneic islet cell transplantation is considered experimental/investigational for all indications because the safety and/or efficacy of this service can not be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Winter 2006 CGPU.
MazeProcedure(11.02.20a)covered: According to certAin criteriA
The Maze procedure is a surgical procedure intended to restore normal heart rhythm in individuals afflicted with atrial fibrillation or atrial flutter that does not respond to medical therapy. It can be performed alone or in conjunction with other cardiac surgeries for restoring the normal electrical impulses of the heart. The procedure is done under general anesthesia while the individual is on cardiopulmonary bypass (a machine that performs the functions of the heart and lungs during the surgery). Access to the heart is obtained through a sternal incision. The cardiothoracic surgeon then makes several incisions in the right and left atria of the heart to create a pathway (maze) for the electrical impulses to flow, thus restoring the normal rhythm of the heart. These incisions create a direction for the impulse to flow from the sinoatrial (SA) node to the atrioventricular (AV) node and block the re-entry of impulses that result in atrial fibrillation or atrial flutter.
Results may not be evident immediately due to cardiac swelling, and some individuals may experience temporary fibrillation up to three months following the procedure. The fibrillation normally stops after the heart has had time to heal completely.
The Maze procedure is considered medically necessary and, therefore, covered for the treatment of atrial fibrillation or atrial flutter in individuals with any of the following clinical indications:
• Resistance to drug therapy.
• Intolerance of drug therapy.
• Atrial fibrillation or atrial flutter for more than six months with an enlarged left atrium.
• High risk for thromboembolism (i.e., previous thromboembolism or long-standing atrial fibrillation with mitral valve disease).
Originally published in Spring 2006 CGPU.
43034txtAH.indd 12 2/19/07 2:43:03 PM
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 1�
MedicalevaluationandManagementforAttention-DeficitHyperactivityDisorder(ADHD)(07.03.03b)covered: According to certAin criteriA
Evaluation
All of the following are considered medically necessary and, therefore, covered for the medical evaluation of attention-deficit hyperactivity disorder (ADHD):
• A complete physical examination within the last 12 months (including blood tests such as lead levels and quantitative plasma amino acid assays to detect phenylketonuria).
• A comprehensive medical history.
• Interviews with the parents and child to establish problem pattern of behavior and parent-child and child-peer conflicts.
Neuropsychological testing for the evaluation of a previously diagnosed ADHD is considered not medically necessary and, therefore, not covered. It should only be performed if there is a suspicion of a neurological deficit that requires additional evaluation.
Management
Pharmacological therapy in the management of ADHD may be covered under the prescription plan when the member has a pharmacy benefit.
Not Medically Necessary
Nontraditional treatments for ADHD such as, but not limited to, the following, have not shown positive health outcomes and are, therefore, considered not medically necessary and are not covered:
• Elimination diets (e.g., Feingold diet).
• Nutritional supplements (e.g., megadoses of vitamins).
• Antifungal therapy.
• Electroencephalogram (EEG) biofeedback.
• Antimotion sickness medication.
• Spinal manipulation.
Physical, occupational, and/or speech therapy is considered not medically necessary and, therefore, not covered in the treatment of ADHD, unless the individual has a neurological or physical deficit that requires such therapy.
Experimental/InvestigationalNontraditional treatments for ADHD lack validation and scientific support and are, therefore, considered experimental/investigational and are not covered. Examples of nontraditional treatments for ADHD include:
• Sensory integration therapy.
• Optometric vision training (orthoptic/pleoptic).
• Interactive metronome training (a computerized version of keeping the beat, which provides auditory feedback).
• Chiropractic therapy.
Originally published in Summer 2006 CGPU.
NegativePressureWoundTherapy(NPWT)Pump(05.00.38a)covered: According to certAin criteriA
Negative pressure wound therapy (NPWT), also known as vacuum-assisted closure, is the application of controlled negative pressure (vacuum pressure) to a wound using an electrical pump. The NPWT vacuum pressure pump is used to apply from 25 mm to greater than 200 mm Hg of pressure to a wound, either continuously or intermittently.
Medical NecessityA NPWT pump and the supplies necessary for its use are considered medically necessary and, therefore, covered for chronic nonhealing wounds (of at least 30 days duration) as specified below when all of the following applicable conditions are met:
• For chronic nonhealing ulcers or wounds, all of the following program measures should apply or be considered and ruled out by an eligible health care professional prior to the application of a NPWT pump:
- Any wound-specific therapeutic measures.
- Documentation in the individual’s medical record of the evaluation, wound measurements (length, depth, and width), and general care performed and documented by a health care professional.
- Wound assessments are performed and documented at least weekly (e.g., size [length, depth, and width], color, exudate type and amount, odor, evidence of healing, sinus tracking or tunneling, pain, type of dressing used).
43034txtAH.indd 13 2/19/07 2:43:04 PM

1�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
- Application of dressings to maintain a moist wound environment.
- Debridement of necrotic tissue (if present) by a health care professional.
- Evaluation of and provision for adequate nutritional status.
• The following wound-specific therapeutic measures (if applicable) must be applied or considered and ruled out by an eligible health care professional prior to the application of a NPWT pump for the following specific types of ulcers and wounds:
- For Stage III or IV pressure ulcers:
º The individual has been appropriately turned and positioned.
º The individual has used a group 2 or 3 support surface for pressure ulcers on the posterior trunk or pelvis. (A group 2 or 3 support surface is not required if the ulcer is not on the trunk or pelvis. For more information on support surfaces, refer to the policy addressing this topic.)
º The individual’s moisture and incontinence have been appropriately managed.
- For neuropathic (e.g., diabetic) ulcers:
º The individual has been on a comprehensive diabetic management program.
º The individual has experienced reduced pressure on a foot ulcer as a result of using the appropriate modalities (such as, but not limited to, the following: total contact casts; removable cast walkers; half shoes; saline wet-to-dry dressings; debridement of all necrotic, callus, and fibrous tissue; crutches).
- For venous insufficiency ulcers:
º The individual has had compression bandages and/or garments consistently applied.
º The individual has applied leg elevation.
º The individual has applied ambulation.
• For complications of surgical, subacute, or traumatic wounds (e.g., postoperative flap, dehiscence, skin graft failure, traumatic amputation, gunshot wounds, or burns) when accelerated granulation tissue formation
cannot be achieved by topical wound treatments and is a medical necessity as demonstrated by documentation of conditions such as, but not limited to, any of the following:
- The presence of excessive wound drainage.
- Large wounds not amenable to primary closure.
- Conditions that slow healing times (e.g., diabetes).
- Infection.
- The wound is a chronic and nonhealing wound of at least 30 days duration.
Initial NPWT pump treatments may begin during an inpatient stay for wounds encountered in the inpatient setting. Treatment with the NPWT pump beyond the inpatient stay may continue (upon discharge) in the home setting, subject to meeting the above medical necessity criteria.
Continued CoverageFor continuing coverage of up to four months, an eligible health care professional must:
• Directly assess the wound(s) being treated with the NPWT pump device and document findings.
• Supervise or directly perform the NPWT pump dressing changes and document findings.
• Document changes in the ulcer’s dimensions and characteristics (e.g., size [length, depth, and width], color, exudate type and amount, odor, and evidence of healing) at least weekly.
For continued coverage beyond four months, continued documentation demonstrating wound healing is required and will be evaluated by a Company medical director.
Not Medically NecessaryTreatment with an NPWT pump and supplies is considered not medically necessary and, therefore, not covered when:
• Adequate wound healing has occurred.
• Any measurable degree of wound healing has failed to occur over the prior month.
• Cancer is present in the wound.
• The equipment or supplies are no longer being used for
43034txtAH.indd 14 2/19/07 2:43:04 PM
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 1�
the individual, regardless of whether it is a result of the health care professional’s orders.
• The eligible health care professional fails to perform and document the following on a weekly basis:
- Direct assessment of the wound(s) being treated with the NPWT pump.
- Supervision or directly performing the ulcer/wound dressing changes.
- Changes in the ulcer’s dimensions (length, depth, and width) at least weekly.
• Necrotic tissue with eschar is present if debridement has not been attempted.
• There is a fistula to an organ or body cavity within the vicinity of the wound.
• Untreated osteomyelitis exists within the vicinity of the wound.
Supplies for NPWTAn individual is eligible for a maximum of 15 wound care sets (A6550) per wound per month, unless there is documentation that the wound size requires more than one wound care set for each dressing change. An individual is eligible for a maximum of 10 canisters (A7000) per month, unless there is documentation evidencing a large volume of drainage (90 ml of exudate/day).
An NPWT pump (E2402) must be capable of accommodating more than one wound dressing set for multiple wounds on an individual. Therefore, more than one E2402 billed per individual for the same time period will be denied as not medically necessary.
Originally published in Fall 2006 CGPU.
outpatientspeechTherapy(10.06.01a)covered: According to certAin criteriA
Speech pathology services are services that are deemed necessary for the diagnosis of speech and language disorders. Speech therapy is the medically prescribed treatment of speech and language disorders due to disease, surgery, injury, congenital anomalies, speech language delay, or previous therapeutic processes that result in communication disabilities and/or swallowing disorders.
Medical Necessity CriteriaSpeech pathology evaluation and services related to the speech therapy process that are within the scope of the member’s benefit contract are considered medically necessary and, therefore, are covered when all of the following criteria are met:
• The evaluation is prescribed by a physician and performed by a speech/language pathologist who is licensed in the state where the services are being performed and who is certified by the American Speech-Language-Hearing Association (ASHA).
• The services must be of such a complex nature that they can only be performed by a speech/language pathologist.
• The medical condition must be such that there is a reasonable expectation that the services will bring about a significant improvement within a reasonable time frame, regardless of whether the individual has a coexisting disorder.
• The services are provided in accordance with an ongoing plan of care specific to the diagnosis.
- The plan of care should be updated at least weekly, or more frequently as the treatment progresses, and as goals change or are met. Upon request, documentation must be available that shows measurable progress toward meeting the short- and long-term goals outlined in the plan of care.
• The therapy is performed for a communication disorder that is a result of at least one of the following:
- Disease (e.g., Parkinson’s disease that results in increased difficulty in swallowing and speaking).
- Surgery (e.g., surgical removal of a malignant growth on the head or neck).
- Injury (e.g., automobile accident that results in a subdural hematoma influencing the speech center and causing neurogenic stuttering or aphasia following a cerebrovascular accident [CVA]).
- Congenital anomalies (e.g., inborn defect of the skull, cleft lip, or cleft palate).
- Speech-language delay that is developmental in nature.
or
• The therapy is performed for a swallowing disorder (dysphagia) that results from a condition such as,
43034txtAH.indd 15 2/19/07 2:43:04 PM

16Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
but not limited to, a CVA regardless of whether a communication disorder also exists.
Speech therapy performed for reasons other than those listed above is considered not medically necessary and, therefore not covered except as required by law.
Conditions that do not Meet Medical Necessity CriteriaConditions or situations that do not meet medical necessity criteria for speech pathology evaluation and services related to the speech therapy process include, but are not limited to:
• Psychological speech delay.
• Behavior problems (e.g., impulsive behavior).
• Except as required by law, mental retardation, autism, attention disorders, or pervasive developmental disorders (PDDs) in the absence of a documented communication co-morbidity that is amenable to speech therapy with a reasonable expectation of achieving sustainable, measurable improvement in a reasonable time frame.
- Social communication disorder is not considered a medically necessary co-morbidity.
• Stammering and stuttering with the following exception:
- Speech therapy is considered medically necessary and, therefore, covered for neurogenic stuttering caused by acquired brain damage.
• Programs that are primarily educational in nature or that support an academic program.
• Speech therapy for the maintenance of a chronic condition when the therapeutic goals of a treatment plan have been achieved, no additional functional improvement is apparent or expected to occur, and the provision of services for a condition ceases to be of therapeutic value.
- Maintenance therapy is defined as a continuation of care and management of the individual when the therapeutic goals of a treatment plan have been achieved, no additional functional improvement is apparent or expected to occur, and the provision of services for a condition ceases to be of therapeutic value. This includes maintenance services that seek to prevent disease, promote health, and prolong and enhance the quality of life.
• Services that otherwise would not require the skills of a qualified speech/language pathologist, such as treatments that maintain function by using routines and repetitions.
- Examples of these services include, but are not limited to, word drills for developmental articulation errors, computer-based programs (e.g., Fast Forward), and procedures that may be performed by the individual, family, and/or caregivers.
Duplicate TherapyWhen individuals are receiving both occupational and speech therapy, the therapies must provide different treatments with separate treatment plans and goals in order for each to be covered and be separately reimbursed. Otherwise, the therapy is considered duplicate therapy and coverage and reimbursement is only available for one therapy.
Benefit Limitations Limitations, frequency, and annual maximums may be applied and vary by product or by group. Individual member benefits must be verified, as speech therapy benefits vary by product and group.
Speech Therapy Services Provided in Conjunction with Speech Generating Devices, Electronic Speech Aids, and Computer-Based Programs Speech generating devices including computer-based programs:
Speech therapy provided in association with a speech generating device, including a computer-based program, is considered medically necessary and, therefore, covered when the device is considered medically necessary consistent with the applicable medical policy.
Electronic speech aids and other electronic devices for speech:
Electronic speech aids/devices are considered medically necessary and, therefore, covered only when an individual has had a laryngectomy or has a nonfunctional larynx consistent with the applicable medical policy. There are several electronic speech aids/devices approved by the U.S. Food and Drug Administration (FDA) for use with speech therapy. Speech therapy provided in association with an approved electronic speech aid/device is considered medically necessary and, therefore, covered in accordance with the terms defined in the applicable medical policy.
43034txtAH.indd 16 2/19/07 2:43:04 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 1�
Electronic speech devices that are designed to improve fluency problems (such as stuttering) rather than aid in communication disabilities are considered experimental/investigational because the efficacy of these devices cannot be established by review of the available published literature. Therefore, these devices are not covered. Examples of these types of electronic devices include, but are not limited to:
• SpeechEasy ( Janus Development Group, Inc., Greenville, N.C.).
• FluencyMaster (National Medical Equipment, Inc., New Hyde Park, N.Y.).
Originally published in Summer 2006 CGPU.
ReductionMammaplasty(11.08.02c)covered: According to certAin criteriA
Reduction mammaplasty is a surgical procedure that excises a portion of the breast, including the skin and underlying glandular tissue to reduce the size, shape, and weight of mammary tissue. In some selected cases (e.g., when the breasts are not too large and the skin has good elasticity), liposuction can be utilized. However, in most cases, only fat, not glandular breast tissue, can be successfully removed by liposuction.
For all products except Medicare Advantage, the following criteria are applicable:
Reduction mammaplasty is considered medically necessary and, therefore, covered when all of the following medical necessity criteria are met:
• An individual has macromastia (enlargement of the breasts) or gigantomastia.
• Clinical symptoms of breast, neck, back, or shoulder pain, or painful shoulder grooving are present for a minimum six-week period and have not responded to conservative measures (e.g., support bra, exercises, heat/cold treatment, non-steroidal anti-inflammatory drugs (NSAIDs)/muscle relaxants).
• The individual meets the minimum specimen weight of breast tissue to be removed based on the individual’s body surface area (BSA).
- Simplified formula for calculation of body surface area: BSA (in m2) = [height (cm)] 0.718 X [weight (kg)] 0.427 X 0.007449
• Any individual 40 years of age or older is required to have a mammogram which is negative for cancer within the year prior to the planned surgery.
When a request is made for reduction mammaplasty, photographs documenting breast size are required.
For Medicare Advantage Members only, the following criteria are applicable:
Reduction mammaplasty is considered reconstructive surgery and medically necessary for symptomatic individuals with macromastia when all of the following criteria are met:
• The individual has significant symptoms that interfere with normal daily activities, including at least one of the following:
- Symptomatic neck, back, or shoulder pain not related to other causes (e.g., poor posture, acute strains, poor lifting techniques).
- Significant breast pain.
- Brachial plexus irritation.
- Clinical, nonseasonal submammary intertrigo.
º Medicare requires that hypertrophy of breast (611.1) be reported as the primary diagnosis, with one of the following clinical conditions reported as a secondary diagnosis:
□ Other specified erythematous condition (695.89).
□ Pain in joint, shoulder region (719.41).
□ Cervicalgia (723.1).
□ Unspecified musculoskeletal disorders and symptoms referable to neck (723.9).
□ Pain in thoracic spine (724.1).
□ Unspecified backache (724.5).
□ Unspecified osteoporosis (733.00).
□ Senile osteoporosis (733.01).
□ Kyphosis (acquired) (postural) (737.10).
• The amount of breast tissue anticipated to be removed is at least 350 grams per breast.
43034txtAH.indd 17 2/19/07 2:43:05 PM

1�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
• Conservative treatment has failed. Examples of conservative treatment include, but are not limited to:
- Appropriate support bra.
- Conservative analgesia (NSAIDs).
- In individuals where obesity is a documented risk factor, a legitimate, medically-based attempt to reduce and maintain weight (e.g., diet, exercise).
- Appropriate medical management of intertrigo.
Requests for reduction mammaplasty that do not meet medical necessity criteria are considered cosmetic, and therefore are not covered.
Originally published in Fall 2006 CGPU.
TheBosToN®sclerallens(07.13.11)covered: According to certAin criteriA
A contact lens that covers the cornea and the adjacent portion of the white of the eye (sclera) is called a scleral contact lens and is sometimes referred to as a corneal liquid bandage.
The BOSTON® Scleral Lens (BSL), which is more specifically termed the BOSTON® Equalens II, is the only rigid gas-permeable scleral contact lens that is commercially available in the U.S. and that can be post-fabricated for the treatment of persistent corneal epithelial defects (PED). Currently, it is only post-fabricated and distributed by the Boston Foundation for Sight in Needham, Mass. The BSL, unlike a traditional rigid gas-permeable contact lens, is a specially designed, fluid-ventilated, gas-permeable scleral contact lens. It is designed to maintain a bubble-free reservoir of oxygenated aqueous fluid over the corneal surface at a neutral hydrostatic pressure. Due to the fact that air bubbles are avoided, the fluid reservoir functions as a liquid corneal bandage that offers unique therapeutic benefits for the management of severe ocular surface disease, in addition to its traditional role of masking irregular corneal astigmatism.
Although limited, compelling evidence exists that shows that the BSL is effective in alleviating pain and photophobia and improves the vision of patients with PED. In the majority of studies, the most frequent specific indication for the BSL was Stevens-Johnson syndrome. The BSL has also been shown to be effective in preventing the recurrence of PED in anesthetic corneas.
The BSL is considered medically necessary and, therefore, covered to alleviate pain and photophobia for PED that have been documented as disabling and that have symptoms that are not significantly relieved with medical treatment. The BSL is also considered medically necessary and, therefore, covered to improve visual acuity in individuals for whom surgery is either undesirable and/or contraindicated due to any of the following conditions:
• Stevens-Johnson disease (a syndrome of systemic, as well as more severe, mucocutaneous lesions that results in corneal opacities, perforations, and/or blindness).
• Conditions that result from a chemical and/or traumatic injury.
• Postradiotherapy complications.
• Recurrent corneal erosion.
• Congenital and/or postsurgical lid defect(s).
• Ocular cicatricial pemphigoid.
• Exposure keratitis.
• Toxic epidermal necrolysis.
• Lacrimal and/or meibomian gland obliteration or deficiency.
• Superior limbal keratoconjunctivitis.
• Sjögren syndrome.
• Inflammatory corneal degeneration.
• Neurotrophic corneal disease (e.g., corneal denervation that is related to acoustic neuroma surgery, trigeminal ganglion obliteration, diabetes mellitus, herpetic syndrome, congenital dysautonomia [Reily-Day syndrome]).
• Corneal edema.
Originally published in Winter 2006 CGPU.
43034txtAH.indd 18 2/19/07 2:43:05 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 1�
TriggerPointinjections(11.14.02c)covered: According to certAin criteriA
Trigger point injection is one of many modalities utilized in the management of chronic pain. Myofascial trigger points are self-sustaining hyperirritative foci that may occur in any skeletal muscle in response to strain produced by acute or chronic overload.
Trigger point injections are considered medically necessary and, therefore, covered when performed for myofascial pain syndrome (MPS) when at least one of the following situations is present:
• Noninvasive medical management (e.g., analgesics, passive physical therapy, ultrasound therapy, range-of- motion, and/or active exercises) is unsuccessful.
• Joint movement is mechanically blocked, as when the coccygeus muscle is involved.
Trigger point injections are appropriate when administered to any of the following body regions:
• Head.
• Cervical spine.
• Left upper extremities, including shoulder.
• Right upper extremities, including shoulder.
• Left lower extremities, including hip.
• Right lower extremities, including hip.
• Thoracic spine (including the trapezius and scapular areas).
• Lumbosacral spine.
When a given region is injected, it is considered one injection service, regardless of the number of injections administered within that region.
• It is expected that this procedure would not be performed on more than three body regions on a given date of service.
• Trigger point injections for a specific body region should not be performed more frequently than once a month.
- Requests for more frequent injections require additional documentation of medical necessity.
Medications listed in the coding table are eligible for separate reimbursement when used for trigger point injections that meet the medical necessity criteria listed in this policy.
• Additional reimbursement will not be made for the injection of water, saline, or local anesthetics.
Dry needling of trigger points is considered medically necessary and, therefore, covered. The medical necessity criteria for dry needling of trigger points are the same as those for trigger point injections.
Originally published in Fall 2006 CGPU.
43034txtAH.indd 19 2/19/07 2:43:05 PM

20Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
43034txtAH.indd 20 2/19/07 2:43:05 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com
Table of ConTenTs
www.amerihealth.com/providers/communications 21
Medical Policies not covered: considered eXPeriMental/
investigational
Computer-Assisted Musculoskeletal Surgical Navigational Orthopedic Procedure (11.14.17) ...................22
Cryoablation of Neuromas (11.15.21) ................................. 22
Dual-Energy X-ray Absorptiometry (DEXA) Body Composition Study (09.00.20a) ...........................................22
Infrared Heating Pad Systems (07.00.18a) ..........................22
Intraperitoneal Hyperthermic Chemotherapy (IPHC) (11.00.13) ............................................................................23
Ocular Photoscreening (07.13.12) .......................................23
Prolotherapy (11.14.15b) ......................................................24
Scintimammography (09.00.39) ...........................................24
Subfascial Endoscopic Perforator Surgery (SEPS) (11.02.23) ...............................................................24
Surgical Ventricular Restoration (SVR) (11.02.24) .............24
Thermography (07.02.13a) .................................................25
43034txtAH.indd 21 2/19/07 2:43:05 PM

22Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
Computer-AssistedMusculoskeletalsurgicalNavigationalorthopedicProcedure(11.14.17)not covered: considered experimentAl/investigAtionAl
Computer-assisted navigational orthopedic procedures use navigational systems during musculoskeletal surgery to provide additional information and to further integrate preoperative planning with how the surgery is being performed. Navigational systems are typically used to improve the placement and positioning of a prosthetic and/or surgical instrument during the procedure. Computer-assisted navigational orthopedic procedures can also be used as an adjunct to fixation of pelvic, acetabular, or femoral fractures and as an adjunct to hip or knee arthroplasty procedures.
A computer-assisted musculoskeletal surgical navigational orthopedic procedure is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Summer 2006 CGPU.
CryoablationofNeuromas(11.15.21)not covered: considered experimentAl/investigAtionAl
Cryoanalgesia, also known as cryosurgery, cryolysis, cryoneurolysis, and cryoablation, uses extremely low temperatures to produce a reversible nerve block similar to that delivered by local anesthesia. No randomized or controlled studies have tested cryoanalgesia specifically for pain control of neuromas.
Cryoablation of neuromas is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Summer 2006 CGPU.
Dual-energyX-rayAbsorptiometry(DeXA)BodyCompositionstudy(09.00.20a)not covered: considered experimentAl/investigAtionAl
A full-body DEXA is a noninvasive method for assessing body fat and composition. It can also be combined with an additional measurement of total body water and contribute to a body composition assessment that is based on a four-compartment mode: bone, fat, dry fat-free soft tissue, and water.
DEXA body composition study is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Spring 2006 CGPU.
infraredHeatingPadsystems(07.00.18a)not covered: considered experimentAl/investigAtionAl
Monochromatic infrared energy (MIRE), applied via an infrared heating pad system, has been used to treat various conditions related to circulation and pain. An infrared heating pad system consists of a pad or pads containing mechanisms that generate infrared, or near-infrared, light (e.g., luminous gallium aluminum arsenide diodes) and a power source. The pads are placed on the skin for 30 to 45 minutes, three times weekly, as a treatment program for diabetic neuropathy, ischemic ulcers, and/or musculoskeletal conditions such as back, foot, or myofascial pain. No randomized, controlled studies have been conducted to assess the efficacy of the technique or its long-term effects.
Treatment of wounds, diabetic neuropathy, and/or musculoskeletal conditions with infrared heating pad systems is considered experimental/investigational because the safety and/or efficacy of the service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Spring 2006 CGPU.
Medical Policies Not Covered: considered experimentAl/investigAtionAl
43034txtAH.indd 22 2/19/07 2:43:05 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 2�
intraperitonealHyperthermicChemotherapy(iPHC)(11.00.13)not covered: considered experimentAl/investigAtionAl
Intraperitoneal hyperthermic chemotherapy (IPHC) is a procedure that includes a combination of cytoreductive surgery (debulking or macroscopically removing all visible tumors) with heated chemotherapy delivered intraperitoneally immediately following the surgery. The extent of this surgery plays a significant role in treatment because of the limited 1-3 mm penetration of cytostatic drugs into the peritoneal tissue. The goal of IPHC is to eliminate microscopic metastases that are too small to be identified and removed during cytoreductive surgery. It is theorized that heated chemotherapy increases cytotoxicity and will enhance penetration of chemotherapy into the tumor. In addition, hyperthermia itself has a cytotoxic effect on tumor tissue.
IPHC has been explored in a number of studies over the past 20 years. The majority of research evidence includes phase II trials and case series. There are few phase III trials. Also, the populations studied included only a small number of individuals with various locations of primary cancer, different stages of peritoneal carcinomatosis and varying degrees of success with cytoreductive surgery. Additional research is needed to further define the criteria used to select which individuals should receive hyperthermia, and to identify the most effective drug combination for peritoneal administration. In addition, some of the technical aspects of the procedure such as the optimal temperature of the chemotherapeutic agents, the length of time for the IPHC perfusion, and the efficacy and safety of open and closed chemoperfusion need to be determined and standardized.
IPHC in conjunction with cytoreductive surgery is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Winter 2006 CGPU.
ocularPhotoscreening(07.13.12)not covered: considered experimentAl/investigAtionAl
Ocular photoscreening has been investigated as an alternative screening method to detect the risk factors for amblyopia, which include strabismus (a misalignment of the eyes in any direction), media opacities (e.g., cataracts) and refractive errors (e.g., myopia, hyperopia, astigmatism, presbyopia). It is based on the principle of photorefraction, in which the refractive state of the eye is assessed via the pattern of light that is reflected through the pupil.
Ocular photoscreening involves the use of a camera or video system that is equipped for photoscreening. By using this equipment, images of the pupillary reflexes (autonomic reflex constrictions caused by light) and red reflex (a circular red light reflected from the retina of the eye) are obtained. The images can then be analyzed based on the position of the corneal light reflex, as well as the overall reflection of light from the fundus, which provides information on the child’s fixation pattern and the presence or absence of strabismus. Ocular photoscreening is performed in a darkened room and requires little cooperation from the child, other than fixating on a target for the duration of the photoscreening process. The photographs can then be analyzed by the evaluator or sent to a central laboratory for analysis by an ophthalmologist or specially-trained personnel. Test results are typically graded as pass, fail, or repeat photoscreening.
Ocular photoscreening is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by review of the current available published literature. Therefore, this service is not covered.
Originally published in Winter 2006 CGPU.
43034txtAH.indd 23 2/19/07 2:43:06 PM

2�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
Prolotherapy(11.14.15b)not covered: considered experimentAl/investigAtionAl
Prolotherapy consists of a series of intraligamentous and intratendinous injections of sclerosing agents that alleviate chronic pain by inducing the proliferation of new cells. There are three classes of proliferant solutions used in prolotherapy: chemical irritants (e.g., phenol), osmotic shock agents (e.g., hypertonic dextrose and glycerin), and chemotactic agents (e.g., morrhuate sodium, a fatty acid derivative of cod liver oil). Prolotherapy should not be confused with trigger point injections, which relieve pain by infusing anesthetics and/or anti-inflammatory agents into affected areas.
Prolotherapy is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by review of the available published literature. Therefore, this service is not covered.
Reporting prolotherapy using the trigger point injection CPT® procedure code or any other code is a misrepresentation of the actual service rendered. These services are subject to post-payment review and audit procedures.
Originally published in Fall 2006 CGPU.
scintimammography(09.00.39)not covered: considered experimentAl/investigAtionAl
Scintimammography, also known as mammoscintigraphy, has been proposed primarily as an adjunct to standard film mammography using radiopharmaceutical agents (radioactive tracer [e.g., technetium-99m sestamibi]) to provide tumor-specific imaging of the breast. Scintimammography has also been proposed for the detection of axillary lymph node metastases in individuals with breast carcinoma; however, it has not been fully investigated for this purpose. There is insufficient data comparing the use of scintimammography for decision-making regarding nodal dissection versus standard nodal dissection. Although scintimammography is currently being performed, the published medical literature does not support its efficacy in differentiating malignancies when compared with using surgical biopsy.
Scintimammography is considered experimental/investigational because the safety and/or efficacy of this
service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Summer 2006 CGPU.
subfascialendoscopicPerforatorsurgery(sePs)(11.02.23)not covered: considered experimentAl/investigAtionAl
Subfascial endoscopic perforator surgery (SEPS) is performed as a minimally invasive way to treat individuals with chronic venous insufficiency of the lower extremities. Guided by ultrasound scanning, small incisions are made into the skin that is unaffected by severe chronic venous insufficiency. Using endoscopic techniques, the perforating veins are clipped or divided by endoscopic scissors.
SEPS is considered experimental/investigational because the efficacy of this procedure cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Summer 2006 CGPU.
surgicalVentricularRestoration(sVR)(11.02.24)not covered: considered experimentAl/investigAtionAl
Surgical ventricular restoration (SVR) is a procedure that is designed to restore or remodel the left ventricle to its normal spherical shape and size in individuals who have akinetic (non-moving) segments of the heart. This condition may be secondary to either dilated cardiomyopathy or postinfarction left ventricular aneurysm. The SVR procedure is most commonly performed after coronary artery bypass grafting (CABG) and may also proceed or be followed by procedures such as mitral valve repair or replacement, endocardectomy, and cryoablation for the treatment of ventricular tachycardia.
The SVR procedure may also be referred to as ventricular remodeling or surgical anterior ventricular endocardial restoration (SAVER).
SVR is considered experimental/investigational because the safety and/or efficacy of this service cannot be established by a review of the available published literature. Therefore, this service is not covered.
Originally published in Winter 2006 CGPU.
43034txtAH.indd 24 2/19/07 2:43:06 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 2�
Thermography(07.02.13a)not covered: considered experimentAl/investigAtionAl
Thermography is the measurement of self-emanating infrared radiation that reveals temperature variations at the surface of the body. The thermographic device senses body temperature and demonstrates areas of differing heat emission by producing brightly colored patterns on a liquid crystal display. Each color represents a specific temperature level. Interpretation of these color patterns according to designated anatomic distribution is thought to aid in diagnosing a vast array of disease, such as, but not limited to, breast cancer, Raynaud’s phenomenon, headache, and reflex sympathetic dystrophy.
The American College of Radiology, the American Medical Association, and the American Academy of Neurology have all issued documents that do not recommend or endorse thermography as a diagnostic technology.
Thermography is considered experimental/investigational because the safety and/or efficacy of the service cannot be established by review of the available published literature. Therefore, this service is not covered.
Originally published in Spring 2006 CGPU.
43034txtAH.indd 25 2/19/07 2:43:06 PM

26Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
43034txtAH.indd 26 2/19/07 2:43:06 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com
Table of ConTenTs
www.amerihealth.com/providers/communications 2�
claiM PayMent Policies
Associated Services Performed in Conjunction with Dental Services Considered Eligible for Reimbursement When Certain Criteria are Met (00.01.18a) ....................................................................28
Modifiers LT/RT: Left Side/Right Side Procedures (03.00.10) ...........................................................28
Work Hardening and Work Conditioning is Not Covered Under Most of the Company’s Products (10.05.02) ..............................................................29
43034txtAH.indd 27 2/19/07 2:43:06 PM

2�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
Claim Payment PoliciesAssociatedservicesPerformedinConjunctionwithDentalservicesConsideredeligibleforReimbursementWhenCertainCriteriaareMet(00.01.18a)
Dental services include procedures and/or surgery that relate to the teeth, jaw, and/or mouth (e.g., routine cleanings, fillings).
The Company covers and considers for reimbursement charges that are associated with noncovered dental procedures or surgery, including anesthesia, when any of the following conditions are met:
• The individual has a comorbid condition that would potentially increase the risk of the procedure being performed.
• The individual is severely disabled.
• The individual is a child.
• The individual’s admission to the Ambulatory Surgery Center (ASC), Short Procedure Unit (SPU), or hospital setting is appropriate/necessary to ensure and safeguard the individual’s health.
This policy applies to services that are performed in the following settings: ASC, SPU, hospital outpatient, or inpatient.
This policy applies whether or not the dental service is eligible under the medical benefits.
For information on dental services that are covered under the medical benefits, refer to the individual and/or group benefit contract.
Originally published in Spring 2006 CGPU.
ModifierslT/RT:leftside/RightsideProcedures(03.00.10)
Modifiers LT/RT are used to indicate the side of the body on which a service or procedure is performed. Modifiers LT/RT do not indicate a bilateral service and should not be used to report a service or procedure that is performed bilaterally. Modifier 50 should be used to report bilateral services or procedures.
The Company has established the following guidelines for the appropriate reporting of Modifiers LT/RT with the appropriate procedure codes:
• Modifiers LT/RT should be used to identify procedures that can be performed on contralateral anatomic sites (e.g., bones, joints), paired organs (e.g., ears, eyes, nasal passages, kidneys, lungs, ovaries), or extremities (e.g., arms, legs).
• Modifiers LT/RT should be used to indicate that the procedure is performed on only one side of the body.
It is inappropriate to use Modifiers LT/RT to identify bilateral services or procedures because a more appropriate modifier exists.
To report a bilateral service or procedure, the appropriate procedure code and/or modifier should be used.
Multiple surgery reduction logic will be applied when appropriate.
Additional reporting requirements for Modifiers LT/RT:
• The medical records must clearly support the appropriate use of Modifiers LT/RT.
• Medical records, notes, and/or other documentation should not be attached to the claim unless specifically required and/or requested by the Company.
• Claims submitted with Modifiers LT/RT are subject to post-reimbursement clinical review and potential retractions for inappropriate use.
Originally published in Spring 2006 CGPU.
43034txtAH.indd 28 2/19/07 2:43:07 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 2�
WorkHardeningandWorkConditioningisNotCoveredUnderMostoftheCompany’sProducts(10.05.02)
Work hardening services address physical, functional, behavioral and vocational needs of the worker by utilizing real or simulated work activities. Additionally, work hardening includes education (e.g., body mechanics, work pacing, safety and injury prevention). A work hardening program begins at four hours per day and builds to eight hours per day over the course of the program, usually four weeks. Work hardening requires a specific return-to-work goal. Work hardening services relate directly to specific work skills and do not provide any diagnostic or therapeutic rehabilitation benefit for the individual.
Work conditioning (including reconditioning) utilizes physical conditioning and functional activities related to work. These services bridge a gap between acute outpatient therapy and a structured work hardening program or return to work. Work conditioning/re-conditioning may or may not include an education component. Work conditioning/ re-conditioning is typically four hours/day or less and there is no specific return to work goal required.
Work hardening and work conditioning are benefit contract exclusions for some of the Company’s products. If the group benefit contract does not provide a specific exclusion for work hardening, the service is considered not medically necessary as it is considered vocational in nature and does not provide any diagnostic or therapeutic benefit of a medical nature for the individual.
Originally published in Summer 2006 CGPU.
43034txtAH.indd 29 2/19/07 2:43:07 PM

�0Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
43034txtAH.indd 30 2/19/07 2:43:07 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com
Table of ConTenTs
www.amerihealth.com/providers/communications �1
2006 articles
ICD-9 CM Diagnosis Codes Change for Routine Gynecological Exams ...........................................................32
Billing for Neonatal Hearing Screening Should be Directed to Facility ..........................................................32
Anesthesia Claims Update ...................................................32
Gardasil® Approved by the FDA ......................................... 32
Clarifications to the Intensity Modulated Radiation Therapy Policy .....................................................33
43034txtAH.indd 31 2/19/07 2:43:07 PM

�2Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
iCD-9CMDiagnosisCodesChangeforRoutineGynecologicalexams
Effective January 1, 2006, capitated PCPs who bill for routine gynecological exams should report diagnosis code V72.31 with the applicable preventive evaluation and management (E&M) Current Procedural Terminology (CPT®) codes 99384-99387 and 99394-99397 or Healthcare Common Procedure Coding System (HCPCS) codes S0610 and S0612 for reimbursement consideration.
Routine gynecological exams that are reported with ICD-9 CM code V72.32 for CPT codes 99384-99387 and 99394-99397 are no longer eligible for additional payment outside of the standard capitation amount. HCPCS codes S0610 and S0612 may still be reported with ICD-9 CM code V72.32 when appropriate. For reference, the diagnosis code narratives are as follows:
• V72.31: Routine gynecological examination.
• V72.32: Encounter for Papanicolaou cervical smear to confirm findings of a recent normal smear following initial abnormal smear.
Important reminder: As previously communicated, effective October 1, 2004, we require all practitioners to report diagnosis codes to the highest degree of specificity, according to the ICD-9 CM Coding Manual.
If you have questions, please call Provider Services or your Network Coordinator.
This article originally appeared in the January 2006 Partners in Health Update.
BillingforNeonatalHearingscreeningshouldbeDirectedtoFacility
AmeriHealth has recently received inquiries from members who received bills for hearing screenings provided to their newborns before discharge from a facility.
Please be advised that newborn hearing screenings are covered services and included within the facility’s payment for the delivery and are not eligible for separate billing to AmeriHealth or to the member. In the event that a provider has a contract or arrangement with a facility to provide these screenings, the provider must look to that facility for payment and not to AmeriHealth or to our members.
Please call Provider Services or your Network Coordinator with any questions.
This article originally appeared in the March 2006 Partners in Health Update.
AnesthesiaClaimsUpdate
Effective August 1, 2006, as part of the standard claims adjudication process, ClaimCheck clinical relationship logic will be applied to claims reported with anesthesia services. ClaimCheck is the code relationship editing tool that is integrated into the claims adjudication process for professional claims processing.
For information regarding ClaimCheck clinical relationship logic, please refer to the Clear Claim Connection tool which is available through the NaviNetSM Portal. You may also refer to the user guide that was mailed to you in December 2005.
This article originally appeared in the July 2006 Partners in Health Update.
Gardasil®ApprovedbytheFDA
In June, the U.S. Food and Drug Administration (FDA) approved the biologic license application for Gardasil® (Quadrivalent Human Papillomavirus [Types 6, 11, 16, 18] Recombinant Vaccine). Gardasil® is a new vaccine indicated for females ages 9 to 26 for the prevention of the following conditions caused by HPV types 6, 11, 16, and 18:
• Cervical cancer
• Genital warts
And the following precancerous or dysplastic lesions:
• Cervical adenocarcinoma in situ (AIS)
• Cervical intraepithelial neoplasia (CIN) grade 1, grade 2, and grade 3
• Vulvar intraepithelial neoplasia (VIN) grade 2 and grade 3
• Vaginal intraepithelial neoplasia (VaIN) grade 2 and grade 3
Coverage StatementGardasil® (Quadrivalent Human Papillomavirus [Types 6, 11, 16, 18] Recombinant Vaccine) is considered medically necessary and, therefore, covered as a three-dose regimen
2006 Articles
43034txtAH.indd 32 2/19/07 2:43:07 PM

www.amerihealth.com/providers/communications 33
for use in females ages 9 to 26 for the prevention of cervical
cancer; genital warts; AIS; CIN grade 1, 2, and 3; VIN grade
2 and 3; and VaIN grade 2 and 3 for those members who
have an immunization benefi t.
Th is article originally appeared in the October 2006 Partners in
Health Update.
Clarifications to the Intensity Modulated Radiation Therapy PolicyEff ective December 6, 2006, we will amend the criteria for
medical policy #09.00.17b – Intensity Modulated Radiation
Th erapy (IMRT). Th e annual review of this policy led to the
addition of the following coverage limitations based on the
current literature on this topic.
Coverage Limitations
Th e following CPT® codes are not to be reported when the
services are performed as part of developing an IMRT plan
that is reported using CPT code 77301, even if the services
are performed on diff erent dates, as reimbursement for the
following codes is already included in CPT code 77301.
Reimbursement for MRI guidance for placement of radiation
therapy fi elds is already included in CPT code 77301 and
should not be separately reported, regardless of the date of
service.
To review the full version of this policy, go to
www.amerihealth.com/medpolicy.
Th is article originally appeared in the November 2006 Partners
in Health Update.
76370 Computerized axial tomographic guidance for placement of radiation therapy fi elds
76376 3D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality; not requiring image post-processing on an independent workstation
76377 3D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality; requiring image post-processing on an independent workstation
77280 Th erapeutic radiology simulation-aided fi eld setting, simple
77285 Th erapeutic radiology simulation-aided fi eld setting; intermediate
77290 Th erapeutic radiology simulation-aided fi eld setting; complex
77295 Th erapeutic radiology simulation-aided fi eld setting; three-dimensional simulation
77305 Teletherapy, isodose plan (whether hand or computer calculated); simple (one or two parallel opposed unmodifi ed ports directed to a single area of interest)
77310 Teletherapy, isodose plan (whether hand or computer calculated); intermediate (three or more treatment ports directed to a single area of interest)
77315 Teletherapy, isodose plan (whether hand or computer calculated); complex (mantle or inverted Y, tangential ports, the use of wedges, compensators, complex blocking, rotational beam, or special beam considerations)
77321 Special teletherapy port plan, particles, hemibody, total body
77331 Special dosimetry (e.g., TLD, microdosimetry) (specify), only when prescribed by the treating physician
77336 Continuing medical physics consultation, including assessment of treatment parameters, quality assurance of dose delivery, and review of patient treatment documentation in support of the radiation oncologist, reported per week of therapy
77370 Special medical radiation physics consultation

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
43034txtAH.indd 34 2/19/07 2:43:07 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com
Table of ConTenTs
www.amerihealth.com/providers/communications ��
class action settleMent uPdate
Enhancements to Claim Payment Policy, Processing and Payment Disclosure, and an Appeals Process for Class Action Settlement Providers .................................36
Assistant Surgery Modifiers 80, 81, 82 ................................36
Co-Surgery Modifier 62 ......................................................37
43034txtAH.indd 35 2/19/07 2:43:07 PM

�6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
Class Action Settlement Update: enhancementstoClaimPaymentPolicy,ProcessingandPaymentDisclosure,andanAppealsProcessforClassActionsettlementProviders
The class action settlements involving New Jersey and Delaware providers [of Gregg, et al. v. Independence Blue Cross, et al., Good v. Independence Blue Cross, et al., and Pennsylvania Orthopaedic Society v. Independence Blue Cross, et al.] include the following enhancements for providers who agreed to the settlement:
• Improving disclosure to Settlement Providers, including standard fee schedules, changes to schedules, and medical and payment policies that may affect payment/reimbursement of services, which will be made available online via NaviNetSM, our secure provider portal.
• Changing claims processing for Settlement Providers on the following: selected modifiers (25, 50, 51, 59, 62, 66, 80, 81, 82, RT, LT), multiple surgical procedures, radiological guidance during a procedure, and certain Current Procedural Terminology (CPT®) code-level designations (e.g., Modifier 51 Exempt, Separate Procedure, Add-on Codes).
• Introducing a two-level formal claims appeal process for Settlement Providers in AmeriHealth’s Delaware subsidiary. AmeriHealth New Jersey providers will continue to have access to the existing provider claims appeal process.
Certain of these enhancements are currently available. Others will be announced as they become available.
This article originally appeared in the January 2006 Partners in Health Update.
AssistantsurgeryModifiers80,81,82
AmeriHealth has enhanced its processing system to apply the Centers for Medicare & Medicaid Services (CMS) payment methodology for modifiers that represent assistant surgery [Assistant Surgeon 80; Minimum Assistant Surgeon 81; Assistant Surgeon (when qualified resident surgeon not available) 82] as outlined in the Medicare Physician Fee Schedule Database on the CMS website.*
Assistant surgery Modifiers 80, 81, and 82 are used to denote surgical procedures that require both a primary and an assistant surgeon because of the complexity and/or time requirement of the surgery. An assistant surgeon is a surgeon
who actively assists and supports a primary surgeon during a surgical procedure. Both primary and assistant surgeons should report the same procedure code. The assistant surgeon should append the most appropriate assistant surgery modifier based on the narrative.
The table below identifies and describes the intended processing outcome that is associated with each indicator. However, reimbursement consideration for services that are reported with Modifiers 80, 81, and/or 82 are also contingent upon eligibility, benefits, exclusions, precertification/referral requirements, provider contracts, and/or applicable policies. Payment for these procedures is based on 20 percent of the fee schedule allowance for the surgical service. Please note that assistant surgical services that are performed in conjunction with other surgical services may be subject to multiple surgery reduction guidelines.
CMS utilizes a payment methodology for these types of services by applying assistant surgery payment indicators to procedure codes that, when submitted in combination with Modifiers 80, 81, and/or 82, will allow or restrict payment consideration:
CMS Indicator and Description
Outcome for the Code/Modifier 80, 81, and/or 82 Combination
(0) Assistant surgery payment is inappropriate unless documentation supports medical necessity.
Ineligible for assistant surgery; additional consideration determined on an appeal basis only.
(1) Assistant surgery payment is inappropriate.
Ineligible for assistant surgery reimbursement consideration.
(2) Assistant surgery payment is appropriate.
Eligible for assistant surgery reimbursement consideration.
(9) Concept does not apply. Invalid procedure/modifier code combination.
Medical records, operative reports, and/or other supporting documentation should not be appended to the claim or submitted to the Company unless specifically requested by the Company.
*The following is a link to the Medicare website: www.cms.gov. These sites are maintained by organizations over which AmeriHealth exercises no control and,
43034txtAH.indd 36 2/19/07 2:43:08 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
accordingly, AmeriHealth expressly disclaims any responsibility for the content, the accuracy of the information, and/or quality of the products or services provided by or advertised in these third-party sites. Certain services/treatments referred to in other sites may not be covered under specif ic benefit plans. Please refer to benefit contracts for complete details of the terms, limitations, and exclusions of coverage.
This article originally appeared in the January 2006 Partners in Health Update.
Co-surgeryModifier62
AmeriHealth has enhanced its processing system to apply the Centers for Medicare & Medicaid Services (CMS) payment methodology for Co-surgery Modifier 62 as outlined in the Medicare Physician Fee Schedule Database on the CMS website.*
Co-surgery Modifier 62 is used to denote when two surgeons act as primary surgeons during the same operative procedure or session for the same individual because of the complexity of the procedure and/or the patient’s condition. The co-surgeons are typically of different specialties and perform consecutive or overlapping parts of the same procedure or simultaneous procedures during the same session with one of the following exceptions for co-surgeons of the same specialty:
• Each surgeon must perform a distinct part of the surgical procedure that requires the distinct skills of each surgeon.
• Each surgeon performs the same procedure(s) simultaneously for different regions/organs (e.g., bilateral lung reduction, bilateral knee replacements). In such cases, the operative report must reflect the necessity of two primary surgeons with the same skills.
Each of the two surgeons should submit the same procedure code that represents the entire surgical procedure appended with Modifier 62.
The table below identifies and describes the final processing outcome that is associated with each indicator; however, reimbursement consideration for services that are reported with Modifier 62 are also contingent upon eligibility, benefits, exclusions, precertification/referral requirements, provider contracts, and applicable policies.
Payment for these procedures is based on 62.5 percent of the fee schedule allowance for the service. Please note that co-surgery services that are performed in conjunction with other co-surgery services are subject to multiple surgery reduction guidelines.
CMS utilizes a payment methodology for these types of services by applying co-surgery payment indicators to procedure codes that, when submitted in combination with Modifier 62, will allow or restrict payment consideration:
CMS Indicator and Description
Outcome for the Code/Modifier 62
(0) Co-surgery payment is inappropriate.
Ineligible for co-surgery reimbursement consideration.
(1) Co-surgery payment is inappropriate unless supporting documentation establishes medical necessity.
Ineligible for co-surgery; additional consideration determined on an appeal basis only.
(2) Co-surgery payment is appropriate.
Eligible for co-surgery reimbursement consideration.
(9) Concept does not apply.
Invalid procedure/modifier code combination.
It is inappropriate to report Modifier 62 when one surgeon acts as an assistant to the primary surgeon or when more than two surgeons act as primary surgeons during the same operative session.
Medical records, operative reports, and/or other supporting documentation should not be appended to the claim or submitted to the Company unless specifically requested by the Company.
*The following is a link to the Medicare website: www.cms.gov. These sites are maintained by organizations over which AmeriHealth exercises no control and, accordingly, AmeriHealth expressly disclaims any responsibility for the content, the accuracy of the information, and/or quality of the products or services provided by or advertised in these third-party sites. Certain services/treatments referred to in other sites may not be covered under specif ic benefit plans. Please refer to benefit contracts for complete details of the terms, limitations, and exclusions of coverage.
This article originally appeared in the January 2006 Partners in Health Update.
43034txtAH.indd 37 2/19/07 2:43:08 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
43034txtAH.indd 38 2/19/07 2:43:08 PM

C o d i n g g u i d e l i n e s a n d P o l i C y u P d a t e C o m P e n d i u m
www.amerihealth.com
Table of ConTenTs
www.amerihealth.com/providers/communications 39
Medical code updates
CPT®* Codes .......................................................................40
HCPCS Codes .....................................................................62
ICD-9 CM Codes ...............................................................90
As part of the medical/claim payment policy process, the AmeriHealth Procedure Code Review Unit supports medical code activities. It establishes and maintains the development and documentation of coverage positions for ICD-9 CM, CPT, and HCPCS medical codes across all lines of business and all processing systems.
The following pages detail the new/revised ICD-9 CM, CPT, and HCPCS code updates effective as follows, unless otherwise specified:
ICD-9 CM: Additions and Revisions have an effective date of 10/1/2006. Deletions have a delete date of 10/1/2006.
CPT: Additions and Revisions have an effective date of 1/1/2007. Deletions have a delete date of 1/1/2007.
HCPCS: Additions and Revisions have an effective date of 10/1/2006 or 1/1/2007. Deletions have a delete date of 1/1/2007.
Please note that the listing of a code in this Compendium does not necessarily guarantee coverage or reimbursement for a procedure.
*Current Procedural Terminology (CPT®) is a copyright of the American Medical Association (AMA). All Rights Reserved. No fee schedules, basic units, relative values, or related listings are included in the CPT. The AMA assumes no liability for the data contained herein. Applicable FARS/DFARS restrictions apply to government use. CPT® is a trademark of the AMA.

�0Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A 0062� Anesthesiaforproceduresonthethoracicspineandcord,viaananteriortransthoracicapproach;notutilizing1-lungventilation
1/1/200�
A 00626 Anesthesiaforproceduresonthethoracicspineandcord,viaananteriortransthoracicapproach;utilizing1-lungventilation
1/1/200�
A 1�002 Surgicalpreparationorcreationofrecipientsitebyexcisionofopenwounds,burneschar,orscar(includingsubcutaneoustissues),orincisionalreleaseofscarcontracture,trunk,arms,legs;first100sqcmor1%ofbodyareaofinfantsandchildren
1/1/200�
A 1�00� Surgicalpreparationorcreationofrecipientsitebyexcisionofopenwounds,burneschar,orscar(includingsubcutaneoustissues),orincisionalreleaseofscarcontracture,trunk,arms,legs;eachadditional100sqcmoreachadditional1%ofbodyareaofinfantsandchildren(Listseparatelyinadditiontothecodefortheprimaryprocedure)
1/1/200�
A 1�00� Surgicalpreparationorcreationofrecipientsitebyexcisionofopenwounds,burneschar,orscar(includingsubcutaneoustissues),orincisionalreleaseofscarcontracture,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feetand/ormultipledigits;first100sqcmor1%ofbodyareaofinfantsandchildren
1/1/200�
A 1�00� Surgicalpreparationorcreationofrecipientsitebyexcisionofopenwounds,burneschar,orscar(includingsubcutaneoustissues),orincisionalreleaseofscarcontracture,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feetand/ormultipledigits;eachadditional100sqcmor1%ofbodyareaofinfantsandchildren(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 1���1 Foreheadflapwithpreservationofvascularpedicle(e.g.,axialpatternflap,paramedianforeheadflap)
1/1/200�
A 1���0 Excision,excessiveskinandsubcutaneoustissue(includeslipectomy);abdomen,infraumbilicalpanniculectomy
1/1/200�
A 1���� Excision,excessiveskinandsubcutaneoustissue(includeslipectomy),abdomen(e.g.,abdominoplasty)(includesumbilicaltranspositionandfascialplication)(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 1��11 Mohsmicrographictechnique,includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andhistopathologicpreparationincludingroutinestain(s)(e.g.,hematoxylinandeosin,toluidineblue),head,neck,hands,feet,genitalia,oranylocationwithsurgerydirectlyinvolvingmuscle,cartilage,bone,tendon,majornerves,orvessels;firststageupto�tissueblocks
1/1/200�
CPTCoDes
43034txtAH.indd 40 2/19/07 2:43:09 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �1
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A 1��12 Mohsmicrographictechnique,includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andhistopathologicpreparationincludingroutinestain(s)(e.g.,hematoxylinandeosin,toluidineblue),head,neck,hands,feet,genitalia,oranylocationwithsurgerydirectlyinvolvingmuscle,cartilage,bone,tendon,majornerves,orvessels;eachadditionalstageafterthefirststage,upto�tissueblocks(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 1��1� Mohsmicrographictechnique,includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andhistopathologicpreparationincludingroutinestain(s)(e.g.,hematoxylinandeosin,toluidineblue),ofthetrunk,arms,orlegs;firststage,upto�tissueblocks
1/1/200�
A 1��1� Mohsmicrographictechnique,includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andhistopathologicpreparationincludingroutinestain(s)(e.g.,hematoxylinandeosin,toluidineblue),ofthetrunk,arms,orlegs;eachadditionalstageafterthefirststage,upto�tissueblocks(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 1��1� Mohsmicrographictechnique,includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andhistopathologicpreparationincludingroutinestain(s)(e.g.,hematoxylinandeosin,toluidineblue),eachadditionalblockafterthefirst�tissueblocks,anystage(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 1�10� Ablation,cryosurgical,offibroadenoma,includingultrasoundguidance,eachfibroadenoma
1/1/200�
A 1��00 Mastectomyforgynecomastia 1/1/200�
A 1��01 Mastectomy,partial(e.g.,lumpectomy,tylectomy,quadrantectomy,segmentectomy);
1/1/200�
A 1��02 Mastectomy,partial(e.g.,lumpectomy,tylectomy,quadrantectomy,segmentectomy);withaxillarylymphadenectomy
1/1/200�
A 1��0� Mastectomy,simple,complete 1/1/200�
A 1��0� Mastectomy,subcutaneous 1/1/200�
A 1��0� Mastectomy,radical,includingpectoralmuscle,axillarylymphnodes
1/1/200�
A 1��06 Mastectomy,radical,includingpectoralmuscles,axillaryandinternalmammarylymphnodes(Urbantypeoperation)
1/1/200�
A 1��0� Mastectomy,modifiedradical,includingaxillarylymphnodes,withorwithoutpectoralisminormuscle,butexcludingpectoralismajormuscle
1/1/200�
A 22�26 Percutaneousintradiscalelectrothermalannuloplasty,unilateralorbilateralincludingfluoroscopicguidance;singlelevel
1/1/200�
CPTCoDes
43034txtAH.indd 41 2/19/07 2:43:09 PM

�2Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A 22�2� Percutaneousintradiscalelectrothermalannuloplasty,unilateralorbilateralincludingfluoroscopicguidance;oneormoreadditionallevels(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 22��� Totaldiscarthroplasty(artificialdisc),anteriorapproach,includingdiscectomytoprepareinterspace(otherthanfordecompression),lumbar,singleinterspace
1/1/200�
A 22�62 Revisionincludingreplacementoftotaldiscarthroplasty(artificialdisc)anteriorapproach,lumbar,singleinterspace
1/1/200�
A 22�6� Removaloftotaldiscarthroplasty(artificialdisc),anteriorapproach,lumbar,singleinterspace
1/1/200�
A 2�10� Excisionoftendon,forearmand/orwrist,flexororextensor,each
1/1/200�
A 2�606 Percutaneousskeletalfixationofdistalradialfractureorepiphysealseparation
1/1/200�
A 2�60� Opentreatmentofdistalradialextra-articularfractureorepiphysealseparation,withinternalfixation
1/1/200�
A 2�60� Opentreatmentofdistalradialintra-articularfractureorepiphysealseparation;withinternalfixationof2fragments
1/1/200�
A 2�60� Opentreatmentofdistalradialintra-articularfractureorepiphysealseparation;withinternalfixationof�ormorefragments
1/1/200�
A 2��2� Neurectomy,hamstringmuscle 1/1/200�
A 2��26 Neurectomy,popliteal(gastrocnemius) 1/1/200�
A 2�0�� Neurectomy,intrinsicmusculatureoffeet 1/1/200�
A �2��� Ablationtherapyforreductionoreradicationofoneormorepulmonarytumor(s)includingpleuraorchestwallwheninvolvedbytumorextension,percutaneous,radiofrequency,unilateral
1/1/200�
A ��202 Insertionofepicardialelectrode(s);openincision(e.g.,thoracotomy,mediansternotomy,subxiphoidapproach)
1/1/200�
A ��20� Insertionofepicardialelectrode(s);endoscopicapproach(e.g.,thoracoscopy,pericardioscopy)
1/1/200�
A ��2�� Operativetissueablationandreconstructionofatria,limited(e.g.,modifiedmazeprocedure)
1/1/200�
A ��2�� Operativetissueablationandreconstructionofatria,extensive(e.g.,mazeprocedure);withoutcardiopulmonarybypass
1/1/200�
A ��2�6 Operativetissueablationandreconstructionofatria,extensive(e.g.,mazeprocedure);withcardiopulmonarybypass
1/1/200�
A ��26� Endoscopy,surgical;operativetissueablationandreconstructionofatria,limited(e.g.,modifiedmazeprocedure),withoutcardiopulmonarybypass
1/1/200�
A ��266 Endoscopy,surgical;operativetissueablationandreconstructionofatria,extensive(e.g.,mazeprocedure),withoutcardiopulmonarybypass
1/1/200�
A ��6�� Closureofmultipleventricularseptaldefects; 1/1/200�
A ��6�6 Closureofmultipleventricularseptaldefects;withpulmonaryvalvotomyorinfundibularresection(acyanotic)
1/1/200�
A ��6�� Closureofmultipleventricularseptaldefects;withremovalofpulmonaryarteryband,withorwithoutgusset
1/1/200�
CPTCoDes
43034txtAH.indd 42 2/19/07 2:43:09 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A ���2� Repairofisolatedpartialanomalouspulmonaryvenousreturn(e.g.,ScimitarSyndrome)
1/1/200�
A ���26 Repairofpulmonaryvenousstenosis 1/1/200�
A ���02 Thromboendarterectomy,includingpatchgraft,ifperformed;superficialfemoralartery
1/1/200�
A ���0� Thromboendarterectomy,includingpatchgraft,ifperformed;poplitealartery
1/1/200�
A ���0� Thromboendarterectomy,includingpatchgraft,ifperformed;tibioperonealtrunkartery
1/1/200�
A ���0� Thromboendarterectomy,includingpatchgraft,ifperformed;tibialorperonealartery,initialvessel
1/1/200�
A ���06 Thromboendarterectomy,includingpatchgraft,ifperformed;eachadditionaltibialorperonealartery(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ����� Bypassgraft,withvein;aortoiliac 1/1/200�
A ����� Bypassgraft,withvein;aortobi-iliac 1/1/200�
A ����� Bypassgraft,withvein;aortofemoral 1/1/200�
A ����0 Bypassgraft,withvein;aortobifemoral 1/1/200�
A ��6�� Bypassgraft,withotherthanvein;aortoiliac 1/1/200�
A ��6�� Bypassgraft,withotherthanvein;aortobi-iliac 1/1/200�
A ����� Revision,femoralanastomosisofsyntheticarterialbypassgraftingroin,open;withnonautogenouspatchgraft(e.g.,Dacron,ePTFE,bovinepericardium)
1/1/200�
A ����� Revision,femoralanastomosisofsyntheticarterialbypassgraftingroin,open;withautogenousveinpatchgraft
1/1/200�
A ��210 Uterinefibroidembolization(UFE,embolizationoftheuterinearteriestotreatuterinefibroids,leiomyomata),percutaneousapproachinclusiveofvascularaccess,vesselselection,embolization,andallradiologicalsupervisionandinterpretation,intraproceduralroadmapping,andimagingnecessarytocompletetheprocedure
1/1/200�
A ��6�� Laparoscopy,surgical;implantationorreplacementofgastricneurostimulatorelectrodes,antrum
1/1/200�
A ��6�� Laparoscopy,surgical;revisionorremovalofgastricneurostimulatorelectrodes,antrum
1/1/200�
A ����1 Implantationorreplacementofgastricneurostimulatorelectrodes,antrum,open
1/1/200�
A ����2 Revisionorremovalofgastricneurostimulatorelectrodes,antrum,open
1/1/200�
A ��1�� Colectomy,total,abdominal,withproctectomy;withileoanalanastomosis,includesloopileostomy,andrectalmucosectomy,whenperformed
1/1/200�
A ��1�� Colectomy,total,abdominal,withproctectomy;withileoanalanastomosis,creationofilealreservoir(SorJ),includesloopileostomy,andrectalmucosectomy,whenperformed
1/1/200�
A ���1� Anastomosis,choledochalcyst,withoutexcision 1/1/200�
A ��10� Resectionordebridementofpancreasandperipancreatictissueforacutenecrotizingpancreatitis
1/1/200�
A ����� Pancreaticojejunostomy,side-to-sideanastomosis(Puestow-typeoperation)
1/1/200�
CPTCoDes
43034txtAH.indd 43 2/19/07 2:43:10 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A ���2� Laparoscopy,surgical;withinsertionofintraperitonealcannulaorcatheter,permanent
1/1/200�
A ���2� Laparoscopy,surgical;withrevisionofpreviouslyplacedintraperitonealcannulaorcatheter,withremovalofintraluminalobstructivematerialifperformed
1/1/200�
A ���26 Laparoscopy,surgical;withomentopexy(omentaltackingprocedure)(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ���02 Removalofperitonealforeignbodyfromperitonealcavity 1/1/200�
A ����� Insertionofsubcutaneousextensiontointraperitonealcannulaorcatheterwithremotechestexitsite(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ����6 Delayedcreationofexitsitefromembeddedsubcutaneoussegmentofintraperitonealcannulaorcatheter
1/1/200�
A ���6� Explorationofepididymis,withorwithoutbiopsy 1/1/200�
A ����� Transperinealplacementofneedlesorcathetersintoprostateforinterstitialradioelementapplication,withorwithoutcystoscopy
1/1/200�
A ����6 Placementofinterstitialdevice(s)forradiationtherapyguidance(e.g.,fiducialmarkers,dosimeter),prostate(vianeedle,anyapproach),singleormultiple
1/1/200�
A �6��2 Hymenotomy,simpleincision 1/1/200�
A ��2�6 Revision(includingremoval)prostheticvaginalgraft;openabdominalapproach
1/1/200�
A ����� Dilationandcurettageofcervicalstump 1/1/200�
A ����1 Laparoscopy,surgical,supracervicalhysterectomy,foruterus2�0gorless;
1/1/200�
A ����2 Laparoscopy,surgical,supracervicalhysterectomy,foruterus2�0gorless;withremovaloftube(s)and/orovary(s)
1/1/200�
A ����� Laparoscopy,surgical,supracervicalhysterectomy,foruterusgreaterthan2�0g;
1/1/200�
A ����� Laparoscopy,surgical,supracervicalhysterectomy,foruterusgreaterthan2�0g;withremovaloftube(s)and/orovary(s)
1/1/200�
A ����� Laparoscopysurgical,withradicalhysterectomy,withbilateraltotalpelviclymphadenectomyandpara-aorticlymphnodesampling(biopsy),withremovaloftube(s)andovary(s),ifperformed
1/1/200�
A ����� Resection(tumordebulking)ofrecurrentovarian,tubal,primaryperitoneal,uterinemalignancy(intra-abdominal,retroperitonealtumors),withomentectomy,ifperformed;
1/1/200�
A ����� Resection(tumordebulking)ofrecurrentovarian,tubal,primaryperitoneal,uterinemalignancy(intra-abdominal,retroperitonealtumors),withomentectomy,ifperformed;withpelviclymphadenectomyandlimitedpara-aorticlymphadenectomy
1/1/200�
A 6��10 Nerverepair;withsyntheticconduitorveinallograft(e.g.,nervetube),eachnerve
1/1/200�
A 6��11 Nerverepair;withautogenousveingraft(includesharvestofveingraft),eachnerve
1/1/200�
A 6���6 Biopsyofextraocularmuscle 1/1/200�
CPTCoDes
43034txtAH.indd 44 2/19/07 2:43:10 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A �0��� Magneticresonanceimaging,brain,functionalMRI;includingtestselectionandadministrationofrepetitivebodypartmovementand/orvisualstimulation,notrequiringphysicianorpsychologistadministration
1/1/200�
A �0��� Magneticresonanceimaging,brain,functionalMRI;requiringphysicianorpsychologistadministrationofentireneurofunctionaltesting
1/1/200�
A �22�1 Radiologicalsupervisionandinterpretation,percutaneousvertebroplastyorvertebralaugmentationincludingcavitycreation,pervertebralbody;underfluoroscopicguidance
1/1/200�
A �22�2 Radiologicalsupervisionandinterpretation,percutaneousvertebroplastyorvertebralaugmentationincludingcavitycreation,pervertebralbody;underCTguidance
1/1/200�
A �6��6 Ultrasound,transplantedkidney,realtimeandduplexDopplerwithimagedocumentation
1/1/200�
A �6�1� Ultrasound,pregnantuterus,realtimewithimagedocumentation,firsttrimesterfetalnuchaltranslucencymeasurement,transabdominalortransvaginalapproach;singleorfirstgestation
1/1/200�
A �6�1� Ultrasound,pregnantuterus,realtimewithimagedocumentation,firsttrimesterfetalnuchaltranslucencymeasurement,transabdominalortransvaginalapproach;eachadditionalgestation(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A �6��� Ultrasonicguidance,intraoperative 1/1/200�
A ��001 Fluoroscopicguidanceforcentralvenousaccessdeviceplacement,replacement(catheteronlyorcomplete),orremoval(includesfluoroscopicguidanceforvascularaccessandcathetermanipulation,anynecessarycontrastinjectionsthroughaccesssiteorcatheterwithrelatedvenographyradiologicsupervisionandinterpretation,andradiographicdocumentationoffinalcatheterposition)(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ��002 Fluoroscopicguidanceforneedleplacement(e.g.,biopsy,aspiration,injection,localizationdevice)
1/1/200�
A ��00� Fluoroscopicguidanceandlocalizationofneedleorcathetertipforspineorparaspinousdiagnosticortherapeuticinjectionprocedures(epidural,transforaminalepidural,subarachnoid,paravertebralfacetjoint,paravertebralfacetjointnerveorsacroiliacjoint),includingneurolyticagentdestruction
1/1/200�
A ��011 Computedtomographyguidanceforstereotacticlocalization
1/1/200�
A ��012 Computedtomographyguidanceforneedleplacement(e.g.,biopsy,aspiration,injection,localizationdevice),radiologicalsupervisionandinterpretation
1/1/200�
A ��01� Computedtomographyguidancefor,andmonitoringof,parenchymaltissueablation
1/1/200�
A ��01� Computedtomographyguidanceforplacementofradiationtherapyfields
1/1/200�
A ��021 Magneticresonanceguidanceforneedleplacement(e.g.,forbiopsy,needleaspiration,injection,orplacementoflocalizationdevice)radiologicalsupervisionandinterpretation
1/1/200�
CPTCoDes
43034txtAH.indd 45 2/19/07 2:43:11 PM

�6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A ��022 Magneticresonanceguidancefor,andmonitoringof,parenchymaltissueablation
1/1/200�
A ��0�1 Stereotacticlocalizationguidanceforbreastbiopsyorneedleplacement(e.g.,forwirelocalizationorforinjection),eachlesion,radiologicalsupervisionandinterpretation
1/1/200�
A ��0�2 Mammographicguidanceforneedleplacement,breast(e.g.,forwirelocalizationorforinjection),eachlesion,radiologicalsupervisionandinterpretation
1/1/200�
A ��0�1 Computer-aideddetection(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretation,withorwithoutdigitizationoffilmradiographicimages;diagnosticmammography(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ��0�2 Computer-aideddetection(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretation,withorwithoutdigitizationoffilmradiographicimages;screeningmammography(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ��0�� Mammaryductogramorgalactogram,singleduct,radiologicalsupervisionandinterpretation
1/1/200�
A ��0�� Mammaryductogramorgalactogram,multipleducts,radiologicalsupervisionandinterpretation
1/1/200�
A ��0�� Mammography;unilateral 1/1/200�
A ��0�6 Mammography;bilateral 1/1/200�
A ��0�� Screeningmammography,bilateral(2-viewfilmstudyofeachbreast)
1/1/200�
A ��0�� Magneticresonanceimaging,breast,withoutand/orwithcontrastmaterial(s);unilateral
1/1/200�
A ��0�� Magneticresonanceimaging,breast,withoutand/orwithcontrastmaterial(s);bilateral
1/1/200�
A ��0�1 Manualapplicationofstressperformedbyphysicianforjointradiography,includingcontralateraljointifindicated
1/1/200�
A ��0�2 Boneagestudies 1/1/200�
A ��0�� Bonelengthstudies(orthoroentgenogram,scanogram) 1/1/200�
A ��0�� Radiologicexamination,osseoussurvey;limited(e.g.,formetastases)
1/1/200�
A ��0�� Radiologicexamination,osseoussurvey;complete(axialandappendicularskeleton)
1/1/200�
A ��0�6 Radiologicexamination,osseoussurvey,infant 1/1/200�
A ��0�� Jointsurvey,singleview,2ormorejoints(specify) 1/1/200�
A ��0�� Computedtomography,bonemineraldensitystudy,1ormoresites;axialskeleton(e.g.,hips,pelvis,spine)
1/1/200�
A ��0�� Computedtomography,bonemineraldensitystudy,1ormoresites;appendicularskeleton(peripheral)(e.g.,radius,wrist,heel)
1/1/200�
A ��0�0 Dual-energyX-rayabsorptiometry(DXA),bonedensitystudy,1ormoresites;axialskeleton(e.g.,hips,pelvis,spine)
1/1/200�
CPTCoDes
43034txtAH.indd 46 2/19/07 2:43:11 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A ��0�1 Dual-energyX-rayabsorptiometry(DXA),bonedensitystudy,1ormoresites;appendicularskeleton(peripheral)(e.g.,radius,wrist,heel)
1/1/200�
A ��0�2 Dual-energyX-rayabsorptiometry(DXA),bonedensitystudy,1ormoresites;vertebralfractureassessment
1/1/200�
A ��0�� Radiographicabsorptiometry(e.g.,photodensitometry,radiogrammetry),1ormoresites
1/1/200�
A ��0�� Magneticresonance(e.g.,proton)imaging,bonemarrowbloodsupply
1/1/200�
A ����1 Radiationtreatmentdelivery,stereotacticradiosurgery(SRS),completecourseoftreatmentofcerebrallesion(s)consistingof1session;multi-sourceCobalt60based
1/1/200�
A ����2 Radiationtreatmentdelivery,stereotacticradiosurgery(SRS),completecourseoftreatmentofcerebrallesion(s)consistingof1session;linearacceleratorbased
1/1/200�
A ����� Stereotacticbodyradiationtherapy,treatmentdelivery,perfractionto1ormorelesions,includingimageguidance,entirecoursenottoexceed�fractions
1/1/200�
A ����� Stereotacticbodyradiationtherapy,treatmentmanagement,pertreatmentcourse,tooneormorelesions,includingimageguidance,entirecoursenottoexceed�fractions
1/1/200�
A �210� Alfa-fetoprotein(AFP);AFP-L�fractionisoformandtotalAFP(includingratio)
1/1/200�
A ��6�� Lipoprotein-associatedphospholipaseA2,(Lp-PLA2) 1/1/200�
A ���1� Moleculardiagnostics;RNAstabilization 1/1/200�
A �6��� Antibody;WestNilevirus,IgM 1/1/200�
A �6��� Antibody;WestNilevirus 1/1/200�
A ���0� Infectiousagentantigendetectionbyenzymeimmunoassaytechnique,qualitativeorsemiquantitative,multiplestepmethod;Aspergillus
1/1/200�
A ����� Infectiousagentdetectionbynucleicacid(DNAorRNA);enterovirus,amplifiedprobetechnique
1/1/200�
A ��6�0 Infectiousagentdetectionbynucleicacid(DNAorRNA);Staphylococcusaureus,amplifiedprobetechnique
1/1/200�
A ��6�1 Infectiousagentdetectionbynucleicacid(DNAorRNA);Staphylococcusaureus,methicillinresistant,amplifiedprobetechnique
1/1/200�
A ��6�� Infectiousagentdetectionbynucleicacid(DNAorRNA);Staphylococcus,groupB,amplifiedprobetechnique
1/1/200�
A ���0� Infectiousagentantigendetectionbyimmunoassaywithdirectopticalobservation;Trichomonasvaginalis
1/1/200�
A �1111 Gastrointestinaltractimaging,intraluminal(e.g.,capsuleendoscopy),esophaguswithphysicianinterpretationandreport
1/1/200�
A �202� Computerizedcornealtopography,unilateralorbilateral,withinterpretationandreport
1/1/200�
A �26�0 Diagnosticanalysiswithprogrammingofauditorybrainstemimplant,perhour
1/1/200�
A ��002 Ventilationassistandmanagement,initiationofpressureorvolumepresetventilatorsforassistedorcontrolledbreathing;hospitalinpatient/observation,initialday
1/1/200�
CPTCoDes
43034txtAH.indd 47 2/19/07 2:43:12 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A ��00� Ventilationassistandmanagement,initiationofpressureorvolumepresetventilatorsforassistedorcontrolledbreathing;hospitalinpatient/observation,eachsubsequentday
1/1/200�
A ��00� Ventilationassistandmanagement,initiationofpressureorvolumepresetventilatorsforassistedorcontrolledbreathing;nursingfacility,perday
1/1/200�
A ��00� Homeventilatormanagementcareplanoversightofapatient(patientnotpresent)inhome,domiciliaryorresthome(e.g.,assistedliving)requiringreviewofstatus,reviewoflaboratoriesandotherstudiesandrevisionofordersandrespiratorycareplan(asappropriate),withinacalendarmonth,�0minutesormore.
1/1/200�
A ��610 Intrapulmonarysurfactantadministrationbyaphysicianthroughendotrachealtube
1/1/200�
A ��6�� Continuousinhalationtreatmentwithaerosolmedicationforacuteairwayobstruction;firsthour
1/1/200�
A ��6�� Continuousinhalationtreatmentwithaerosolmedicationforacuteairwayobstruction;eachadditionalhour(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A ����� Pediatrichomeapneamonitoringeventrecordingincludingrespiratoryrate,patternandheartrateper�0-dayperiodoftime;includesmonitorattachment,downloadofdata,physicianreview,interpretation,andpreparationofareport
1/1/200�
A ����� Pediatrichomeapneamonitoringeventrecordingincludingrespiratoryrate,patternandheartrateper�0-dayperiodoftime;monitorattachmentonly(includeshook-up,initiationofrecordinganddisconnection)
1/1/200�
A ����6 Pediatrichomeapneamonitoringeventrecordingincludingrespiratoryrate,patternandheartrateper�0-dayperiodoftime;monitoring,downloadofinformation,receiptoftransmission(s)andanalysesbycomputeronly
1/1/200�
A ����� Pediatrichomeapneamonitoringeventrecordingincludingrespiratoryrate,patternandheartrateper�0-dayperiodoftime;physicianreview,interpretationandpreparationofreportonly
1/1/200�
A ��012 Nitricoxideexpiredgasdetermination 1/1/200�
A �6020 Neurofunctionaltestingselectionandadministrationduringnoninvasiveimagingfunctionalbrainmapping,withtestadministeredentirelybyaphysicianorpsychologist,withreviewoftestresultsandreports
1/1/200�
A �60�0 Medicalgeneticsandgeneticcounselingservices,each�0minutesface-to-facewithpatient/family
1/1/200�
A �6�0� Wholebodyintegumentaryphotography,formonitoringofhighriskpatientswithdysplasticnevussyndromeorahistoryofdysplasticnevi,orpatientswithapersonalorfamilialhistoryofmelanoma
1/1/200�
A ���6� Anticoagulantmanagementforanoutpatienttakingwarfarin,physicianreviewandinterpretationofInternationalNormalizedRatio(INR)testing,patientinstructions,dosageadjustment(asneeded),andorderingofadditionaltests;initial�0daysoftherapy(mustincludeaminimumof�INRmeasurements)
1/1/200�
CPTCoDes
43034txtAH.indd 48 2/19/07 2:43:12 PM
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A ���6� Anticoagulantmanagementforanoutpatienttakingwarfarin,physicianreviewandinterpretationofInternationalNormalizedRatio(INR)testing,patientinstructions,dosageadjustment(asneeded),andorderingofadditionaltests;eachsubsequent�0daysoftherapy(mustincludeaminimumof�INRmeasurements)
1/1/200�
A 0162T Electronicanalysisandprogramming,reprogrammingofgastricneurostimulator(i.e.,morbidobesity)
1/1/200�
A 016�T Totaldiscarthroplasty(artificialdisc),anteriorapproach,includingdiscectomytoprepareinterspace(otherthanfordecompression),lumbar,eachadditionalinterspace
1/1/200�
A 016�T Removaloftotaldiscarthroplasty,anteriorapproach,lumbar,eachadditionalinterspace
1/1/200�
A 016�T Revisionoftotaldiscarthroplasty,anteriorapproach,lumbar,eachadditionalinterspace
1/1/200�
A 0166T Transmyocardialtranscatheterclosureofventricularseptaldefect,withimplant;withoutcardiopulmonarybypass
1/1/200�
A 016�T Transmyocardialtranscatheterclosureofventricularseptaldefect,withimplant;withcardiopulmonarybypass
1/1/200�
A 016�T Rhinophototherapy,intranasalapplicationofultravioletandvisiblelight,bilateral
1/1/200�
A 016�T Stereotacticplacementofinfusioncatheter(s)inthebrainfordeliveryoftherapeuticagent(s),includingcomputerizedstereotacticplanningandburrhole(s)
1/1/200�
A 01�0T Repairofanorectalfistulawithplug(e.g.,porcinesmallintestinesubmucosa[SIS])
1/1/200�
A 01�1T Insertionofposteriorspinousprocessdistractiondevice(includingnecessaryremovalofboneorligamentforinsertionandimagingguidance),lumbar;singlelevel
1/1/200�
A 01�2T Insertionofposteriorspinousprocessdistractiondevice(includingnecessaryremovalofboneorligamentforinsertionandimagingguidance),lumbar;eachadditionallevel(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 01��T Monitoringofintraocularpressureduringvitrectomysurgery(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 01��T Computeraideddetection(CAD)(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretationandreport,withorwithoutdigitizationoffilmradiographicimages,chestradiograph(s),performedconcurrentwithprimaryinterpretation(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
A 01��T Computeraideddetection(CAD)(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretationandreport,withorwithoutdigitizationoffilmradiographicimages,chestradiograph(s),performedremotefromprimaryinterpretation
1/1/200�
A 01�6T Transluminaldilationofaqueousoutflowcanal;withoutretentionofdeviceorstent
1/1/200�
A 01��T Transluminaldilationofaqueousoutflowcanal;withretentionofdeviceorstent
1/1/200�
CPTCoDes
43034txtAH.indd 49 2/19/07 2:43:13 PM

�0Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D 01��� Regionalintravenousadministrationoflocalanestheticagentorothermedication(upperorlowerextremity)
1/1/200�
D 1�000 Surgicalpreparationorcreationofrecipientsitebyexcisionofopenwounds,burneschar,orscar(includingsubcutaneoustissues),orincisionalreleaseofscarcontracture;first100sqcmoronepercentofbodyareaofinfantsandchildren
1/1/200�
D 1�001 Surgicalpreparationorcreationofrecipientsitebyexcisionofopenwounds,burneschar,orscar(includingsubcutaneoustissues),orincisionalreleaseofscarcontracture;eachadditional100sqcmoreachadditionalonepercentofbodyareaofinfantsandchildren(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
D 1���1 Excision,excessiveskinandsubcutaneoustissue(includeslipectomy);abdomen,(e.g.,abdominoplasty)
1/1/200�
D 1��0� Chemosurgery(Mohsmicrographictechnique),includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andcompletehistopathologicpreparationincludingthefirstroutinestain(e.g.,hematoxylinandeosin,toluidineblue);firststage,freshtissuetechnique,upto�specimens
1/1/200�
D 1��0� Chemosurgery(Mohsmicrographictechnique),includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andcompletehistopathologicpreparationincludingthefirstroutinestain(e.g.,hematoxylinandeosin,toluidineblue);secondstage,fixedorfreshtissue,upto�specimens
1/1/200�
D 1��06 Chemosurgery(Mohsmicrographictechnique),includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andcompletehistopathologicpreparationincludingthefirstroutinestain(e.g.,hematoxylinandeosin,toluidineblue);thirdstage,fixedorfreshtissue,upto�specimens
1/1/200�
D 1��0� Chemosurgery(Mohsmicrographictechnique),includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andcompletehistopathologicpreparationincludingthefirstroutinestain(e.g.,hematoxylinandeosin,toluidineblue);additionalstage(s),upto�specimens,eachstage
1/1/200�
D 1��10 Chemosurgery(Mohsmicrographictechnique),includingremovalofallgrosstumor,surgicalexcisionoftissuespecimens,mapping,colorcodingofspecimens,microscopicexaminationofspecimensbythesurgeon,andcompletehistopathologicpreparationincludingthefirstroutinestain(e.g.,hematoxylinandeosin,toluidineblue);eachadditionalspecimen,afterthefirst�specimens;fixedorfreshtissue,anystage(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
D 1�1�0 Mastectomyforgynecomastia 1/1/200�
D 1�160 Mastectomy,partial(e.g.,lumpectomy,tylectomy,quadrantectomy,segmentectomy);
1/1/200�
CPTCoDes
43034txtAH.indd 50 2/19/07 2:43:13 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �1
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D 1�162 Mastectomy,partial(e.g.,lumpectomy,tylectomy,quadrantectomy,segmentectomy);withaxillarylymphadenectomy
1/1/200�
D 1�1�0 Mastectomy,simple,complete 1/1/200�
D 1�1�2 Mastectomy,subcutaneous 1/1/200�
D 1�200 Mastectomy,radical,includingpectoralmuscle,axillarylymphnodes
1/1/200�
D 1�220 Mastectomy,radical,includingpectoralmuscles,axillaryandinternalmammarylymphnodes(Urbantypeoperation)
1/1/200�
D 1�2�0 Mastectomy,modifiedradical,includingaxillarylymphnodes,withorwithoutpectoralisminormuscle,butexcludingpectoralismajormuscle
1/1/200�
D 21�00 Closedtreatmentofskullfracturewithoutoperation 1/1/200�
D 2�611 Percutaneousskeletalfixationofdistalradialfracture(e.g.,CollesorSmithtype)orepiphysealseparation,withorwithoutfractureofulnarstyloid,requiringmanipulation,withorwithoutexternalfixation
1/1/200�
D 2�620 Opentreatmentofdistalradialfracture(e.g.,CollesorSmithtype)orepiphysealseparation,withorwithoutfractureofulnarstyloid,withorwithoutinternalorexternalfixation
1/1/200�
D 26�0� Reconstructionoftendonpulley,eachtendon;withtendonprosthesis(separateprocedure)
1/1/200�
D 2��1� Neurectomy,hamstringmuscle 1/1/200�
D 2��20 Neurectomy,popliteal(gastrocnemius) 1/1/200�
D 2�0�0 Neurectomy,intrinsicmusculatureoffeet 1/1/200�
D �1�00 Catheterization,transglottic(separateprocedure) 1/1/200�
D �1�0� Instillationofcontrastmaterialforlaryngographyorbronchography,withoutcatheterization
1/1/200�
D �1�10 Catheterizationforbronchography,withorwithoutinstillationofcontrastmaterial
1/1/200�
D ��200 Insertionofpermanentpacemakerwithepicardialelectrode(s);bythoracotomy
1/1/200�
D ��201 Insertionofpermanentpacemakerwithepicardialelectrode(s);byxiphoidapproach
1/1/200�
D ��2�� Insertionofepicardialsingleordualchamberpacingcardioverterdefibrillatorelectrodesbythoracotomy;
1/1/200�
D ��2�6 Insertionofepicardialsingleordualchamberpacingcardioverterdefibrillatorelectrodesbythoracotomy;withinsertionofpulsegenerator
1/1/200�
D ��2�� Operativeincisionsandreconstructionofatriafortreatmentofatrialfibrillationoratrialflutter(e.g.,mazeprocedure)
1/1/200�
D ����1 Thromboendarterectomy,withorwithoutpatchgraft;femoraland/orpopliteal,and/ortibioperoneal
1/1/200�
D ���0� Bypassgraft,withvein;subclavian-carotid 1/1/200�
D ����1 Bypassgraft,withvein;aortoiliacorbiiliac 1/1/200�
D ����6 Bypassgraft,withvein;aortofemoralorbifemoral 1/1/200�
D ��6�1 Bypassgraft,withotherthanvein;aortoiliacorbiiliac 1/1/200�
CPTCoDes
43034txtAH.indd 51 2/19/07 2:43:13 PM
�2Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D ��1�2 Colectomy,total,abdominal,withoutproctectomy;withrectalmucosectomy,ileonalanastomosis,withorwithoutloopileostomy
1/1/200�
D ��1�� Colectomy,total,abdominal,withoutproctectomy;withrectalmucosectomy,ileonalanastomosis,creationofilealreservoir(SorJ),withorwithoutloopileostomy
1/1/200�
D ���16 Anastomosis,choledochalcyst,withoutexcision 1/1/200�
D ��00� Resectionordebridementofpancreasandperipancreatictissueforacutenecrotizingpancreatitis
1/1/200�
D ��1�0 Pancreaticojejunostomy,side-to-sideanastomosis(Puestow-typeoperation)
1/1/200�
D ��0�� Removalofperitonealforeignbodyfromperitonealcavity 1/1/200�
D ��1�2 Circumcision,usingclamporotherdevice;exceptnewborns
1/1/200�
D ���20 Explorationofepididymis,withorwithoutbiopsy 1/1/200�
D ����� Transperinealplacementofneedlesorcathetersintoprostateforinterstitialradioelementapplication,withorwithoutcystoscopy
1/1/200�
D �6�20 Hymenotomy,simpleincision 1/1/200�
D ���20 Dilationandcurettageofcervicalstump 1/1/200�
D 6���0 Biopsyofextraocularmuscle 1/1/200�
D ����� Fluoroscopicguidanceforcentralvenousaccessdeviceplacement,replacement(catheteronlyorcomplete),orremoval(includesfluoroscopicguidanceforvascularaccessandcathetermanipulation,anynecessarycontrastinjectionsthroughaccesssiteorcatheterwithrelatedvenographyradiologicsupervisionandinterpretation,andradiographicdocumentationoffinalcatheterposition)(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
D �600� Fluoroscopicguidanceforneedleplacement(e.g.,biopsy,aspiration,injection,localizationdevice)
1/1/200�
D �600� Fluoroscopicguidanceandlocalizationofneedleorcathetertipforspineorparaspinousdiagnosticortherapeuticinjectionprocedures(epidural,transforaminalepidural,subarachnoid,paravertebralfacetjoint,paravertebralfacetjointnerveorsacroiliacjoint),includingneurolyticagentdestruction
1/1/200�
D �6006 Manualapplicationofstressperformedbyphysicianforjointradiography,includingcontralateraljointifindicated
1/1/200�
D �6012 Radiologicalsupervisionandinterpretation,percutaneousvertebroplastyorvertebralaugmentationincludingcavitycreation,pervertebralbody;underfluoroscopicguidance
1/1/200�
D �601� Radiologicalsupervisionandinterpretation,percutaneousvertebroplastyorvertebralaugmentationincludingcavitycreation,pervertebralbody;underCTguidance
1/1/200�
D �6020 Boneagestudies 1/1/200�
D �60�0 Bonelengthstudies(orthoroentgenogram,scanogram) 1/1/200�
D �6061 Radiologicexamination,osseoussurvey;limited(e.g.,formetastases)
1/1/200�
D �6062 Radiologicexamination,osseoussurvey;complete(axialandappendicularskeleton)
1/1/200�
CPTCoDes
43034txtAH.indd 52 2/19/07 2:43:14 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D �606� Radiologicexamination,osseoussurvey;infant 1/1/200�
D �6066 Jointsurvey,singleview,twoormorejoints(specify) 1/1/200�
D �60�0 Computedtomography,bonemineraldensitystudy,oneormoresites;axialskeleton(e.g.,hips,pelvis,spine)
1/1/200�
D �60�1 Computedtomography,bonemineraldensitystudy,oneormoresites;appendicularskeleton(peripheral)(e.g.,radius,wrist,heel)
1/1/200�
D �60�� Dualenergyx-rayabsorptiometry(DXA),bonedensitystudy,oneormoresites;axialskeleton(e.g.,hips,pelvis,spine)
1/1/200�
D �60�6 Dualenergyx-rayabsorptiometry(DXA),bonedensitystudy,oneormoresites;appendicularskeleton(peripheral)(e.g.,radius,wrist,heel)
1/1/200�
D �60�� Dualenergyx-rayabsorptiometry(DXA),bonedensitystudy,oneormoresites;vertebralfractureassessment
1/1/200�
D �60�� Radiographicabsorptiometry(e.g.,photodensitometry,radiogrammetry),oneormoresites
1/1/200�
D �60�2 Computeraideddetection(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretation,withorwithoutdigitizationoffilmradiographicimages;diagnosticmammography(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
D �60�� Computeraideddetection(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretation,withorwithoutdigitizationoffilmradiographicimages;screeningmammography(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
D �60�6 Mammaryductogramorgalactogram,singleduct,radiologicalsupervisionandinterpretation
1/1/200�
D �60�� Mammaryductogramorgalactogram,multipleducts,radiologicalsupervisionandinterpretation
1/1/200�
D �60�0 Mammography,unilateral 1/1/200�
D �60�1 Mammography,bilateral 1/1/200�
D �60�2 Screeningmammography,bilateral(twoviewfilmstudyofeachbreast)
1/1/200�
D �60�� Magneticresonanceimaging,breast,withoutand/orwithcontrastmaterial(s);unilateral
1/1/200�
D �60�� Magneticresonanceimaging,breast,withoutand/orwithcontrastmaterial(s);bilateral
1/1/200�
D �60�� Stereotacticlocalizationguidanceforbreastbiopsyorneedleplacement(e.g.,forwirelocalizationorforinjection),eachlesion,radiologicalsupervisionandinterpretation
1/1/200�
D �60�6 Mammographicguidanceforneedleplacement,breast(e.g.,forwirelocalizationorforinjection),eachlesion,radiologicalsupervisionandinterpretation
1/1/200�
D �6��� Computedtomographyguidanceforstereotacticlocalization
1/1/200�
D �6�60 Computedtomographyguidanceforneedleplacement(e.g.,biopsy,aspiration,injection,localizationdevice),radiologicalsupervisionandinterpretation
1/1/200�
CPTCoDes
43034txtAH.indd 53 2/19/07 2:43:14 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D �6�62 Computedtomographyguidancefor,andmonitoringof,visceraltissueablation
1/1/200�
D �6��0 Computedtomographyguidanceforplacementofradiationtherapyfields
1/1/200�
D �6��� Magneticresonanceguidanceforneedleplacement(e.g.,forbiopsy,needleaspiration,injection,orplacementoflocalizationdevice)radiologicalsupervisionandinterpretation
1/1/200�
D �6��� Magneticresonanceguidancefor,andmonitoringof,visceraltissueablation
1/1/200�
D �6�00 Magneticresonance(e.g.,proton)imaging,bonemarrowbloodsupply
1/1/200�
D �6��� Ultrasound,transplantedkidney,B-scanand/orrealtimewithimagedocumentation,withorwithoutduplexDopplerstudy
1/1/200�
D �6��6 Ultrasonicguidance,intraoperative 1/1/200�
D ���0� Kidneyimaging;withfunctionstudy(i.e.,imagingrenogram)
1/1/200�
D ���1� Kidneyvascularflowonly 1/1/200�
D ���60 Testicularimaging; 1/1/200�
D �1060 Gastricsalineloadtest 1/1/200�
D �2��� Lombardtest 1/1/200�
D ��6�6 Ventilationassistandmanagement,initiationofpressureorvolumepresetventilatorsforassistedorcontrolledbreathing;firstday
1/1/200�
D ��6�� Ventilationassistandmanagement,initiationofpressureorvolumepresetventilatorsforassistedorcontrolledbreathing;subsequentdays
1/1/200�
D ��0�� Provocativetesting(e.g.,Rankletest) 1/1/200�
D 00��T Wholebodyintegumentaryphotography,atrequestofaphysician,formonitoringofhighriskpatients;withdysplasticnevussyndromeorfamilialmelanoma
1/1/200�
D 00��T Wholebodyintegumentaryphotography,atrequestofaphysician,formonitoringofhighriskpatients;withhistoryofdysplasticneviorpersonalhistoryofmelanoma
1/1/200�
D 00�2T Stereotacticbodyradiationtherapy,treatmentdelivery,oneormoretreatmentareas,perday
1/1/200�
D 00��T Stereotacticbodyradiationtherapy,treatmentmanagement,perday
1/1/200�
D 00�1T Totaldiscarthroplasty(artificialdisc),anteriorapproach,includingdiscectomytoprepareinterspace(otherthanfordecompression);singleinterspace,lumbar
1/1/200�
D 00��T Removaloftotaldiscarthroplasty,anteriorapproach;singleinterspace,lumbar
1/1/200�
D 00��T Revisionoftotaldiscarthroplasty,anteriorapproach;singleinterspace,lumbar
1/1/200�
D 0120T Ablation,cryosurgical,offibroadenoma,includingultrasoundguidance,eachfibroadenoma
1/1/200�
CPTCoDes
43034txtAH.indd 54 2/19/07 2:43:15 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D 01�2T Computeraideddetection(computeralgorithmanalysisofdigitalimagedataforlesiondetection)withfurtherphysicianreviewforinterpretation,withorwithoutdigitizationoffilmradiographicimages;chestradiograph(s)(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�100 Split-thicknessautograft,trunk,arms,legs;first100sqcmorless,or1%ofbodyareaofinfantsandchildren(except1�0�0)
1/1/200�
R 1�101 Split-thicknessautograft,trunk,arms,legs;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�110 Epidermalautograft,trunk,arms,legs;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1�111 Epidermalautograft,trunk,arms,legs;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�11� Epidermalautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1�116 Epidermalautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�120 Split-thicknessautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;first100sqcmorless,or1%ofbodyareaofinfantsandchildren(except1�0�0)
1/1/200�
R 1�121 Split-thicknessautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�1�0 Dermalautograft,trunk,arms,legs;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1�1�1 Dermalautograft,trunk,arms,legs;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�1�� Dermalautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1�1�6 Dermalautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsorchildrenorpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�1�2 Tissueculturedepidermalautograft,trunk,arms,legs;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
CPTCoDes
43034txtAH.indd 55 2/19/07 2:43:15 PM
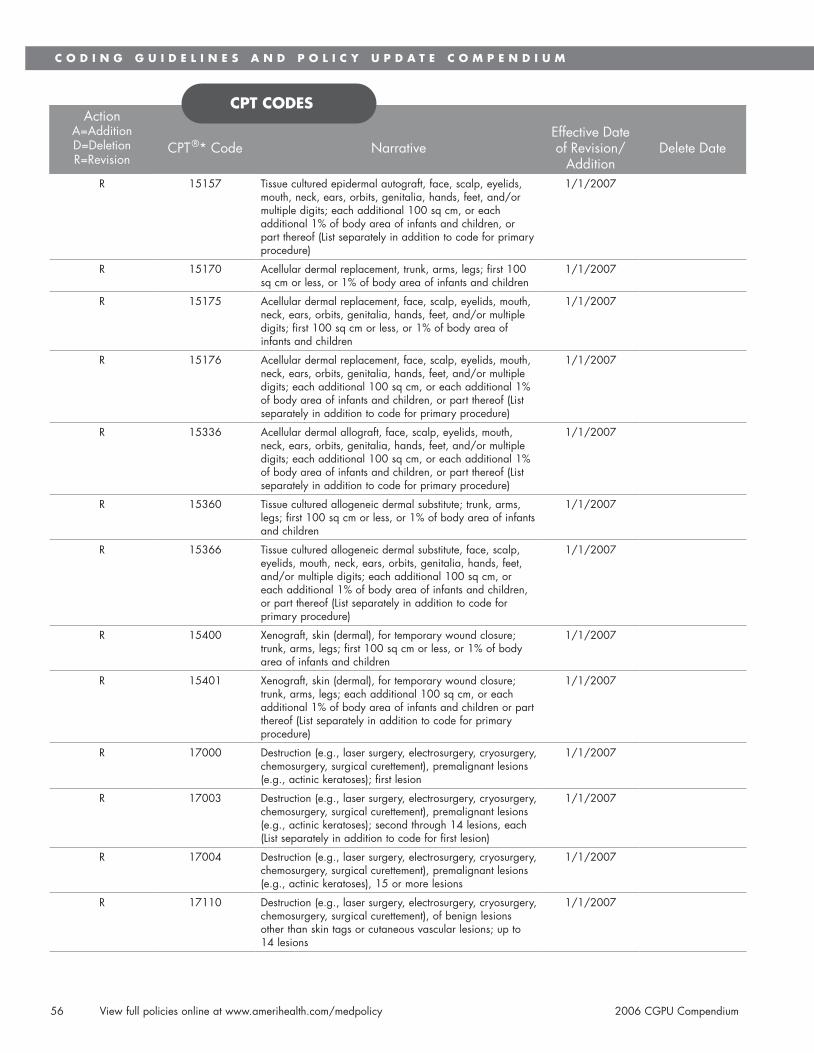
�6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R 1�1�� Tissueculturedepidermalautograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�1�0 Acellulardermalreplacement,trunk,arms,legs;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1�1�� Acellulardermalreplacement,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1�1�6 Acellulardermalreplacement,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1���6 Acellulardermalallograft,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1��60 Tissueculturedallogeneicdermalsubstitute;trunk,arms,legs;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1��66 Tissueculturedallogeneicdermalsubstitute,face,scalp,eyelids,mouth,neck,ears,orbits,genitalia,hands,feet,and/ormultipledigits;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildren,orpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1��00 Xenograft,skin(dermal),fortemporarywoundclosure;trunk,arms,legs;first100sqcmorless,or1%ofbodyareaofinfantsandchildren
1/1/200�
R 1��01 Xenograft,skin(dermal),fortemporarywoundclosure;trunk,arms,legs;eachadditional100sqcm,oreachadditional1%ofbodyareaofinfantsandchildrenorpartthereof(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 1�000 Destruction(e.g.,lasersurgery,electrosurgery,cryosurgery,chemosurgery,surgicalcurettement),premalignantlesions(e.g.,actinickeratoses);firstlesion
1/1/200�
R 1�00� Destruction(e.g.,lasersurgery,electrosurgery,cryosurgery,chemosurgery,surgicalcurettement),premalignantlesions(e.g.,actinickeratoses);secondthrough1�lesions,each(Listseparatelyinadditiontocodeforfirstlesion)
1/1/200�
R 1�00� Destruction(e.g.,lasersurgery,electrosurgery,cryosurgery,chemosurgery,surgicalcurettement),premalignantlesions(e.g.,actinickeratoses),1�ormorelesions
1/1/200�
R 1�110 Destruction(e.g.,lasersurgery,electrosurgery,cryosurgery,chemosurgery,surgicalcurettement),ofbenignlesionsotherthanskintagsorcutaneousvascularlesions;upto1�lesions
1/1/200�
CPTCoDes
43034txtAH.indd 56 2/19/07 2:43:16 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R 1�111 Destruction(e.g.,lasersurgery,electrosurgery,cryosurgery,chemosurgery,surgicalcurettement),ofbenignlesionsotherthanskintagsorcutaneousvascularlesions;1�ormorelesions
1/1/200�
R 1��61 Breastreconstructionwithlatissimusdorsiflapwithoutprostheticimplant
1/1/200�
R 2�600 Closedtreatmentofdistalradialfracture(e.g.,CollesorSmithtype)orepiphysealseparation,includesclosedtreatmentoffractureofulnarstyloid,whenperformed;withoutmanipulation
1/1/200�
R 2�60� Closedtreatmentofdistalradialfracture(e.g.,CollesorSmithtype)orepiphysealseparation,includesclosedtreatmentoffractureofulnarstyloid,whenperformed;withmanipulation
1/1/200�
R 261�0 Excisionoftendon,palm,flexororextensor,single,eachtendon
1/1/200�
R 261�0 Excisionoftendon,finger,flexororextensor,eachtendon 1/1/200�
R ��6�1 Closureofsingleventricularseptaldefect,withorwithoutpatch;
1/1/200�
R ��6�� Closureofsingleventricularseptaldefect,withorwithoutpatch;withpulmonaryvalvotomyorinfundibularresection(acyanotic)
1/1/200�
R ��6�� Closureofsingleventricularseptaldefect,withorwithoutpatch;withremovalofpulmonaryarteryband,withorwithoutgusset
1/1/200�
R ���01 Thromboendarterectomy,includingpatchgraft,ifperformed;carotid,vertebral,subclavian,byneckincision
1/1/200�
R ���11 Thromboendarterectomy,includingpatchgraft,ifperformed;subclavian,innominate,bythoracicincision
1/1/200�
R ���21 Thromboendarterectomy,includingpatchgraft,ifperformed;axillary-brachial
1/1/200�
R ����1 Thromboendarterectomy,includingpatchgraft,ifperformed;abdominalaorta
1/1/200�
R ����1 Thromboendarterectomy,includingpatchgraft,ifperformed;mesenteric,celiac,orrenal
1/1/200�
R ����1 Thromboendarterectomy,includingpatchgraft,ifperformed;iliac
1/1/200�
R ����� Thromboendarterectomy,includingpatchgraft,ifperformed;iliofemoral
1/1/200�
R ���61 Thromboendarterectomy,includingpatchgraft,ifperformed;combinedaortoiliac
1/1/200�
R ���6� Thromboendarterectomy,includingpatchgraft,ifperformed;combinedaortoiliofemoral
1/1/200�
R ����1 Thromboendarterectomy,includingpatchgraft,ifperformed;commonfemoral
1/1/200�
R ����2 Thromboendarterectomy,includingpatchgraft,ifperformed;deep(profunda)femoral
1/1/200�
R ���01 Bypassgraft,withvein;commoncarotid-ipsilateralinternalcarotid
1/1/200�
R ���06 Bypassgraft,withvein;carotid-subclavianorsubclavian-carotid
1/1/200�
CPTCoDes
43034txtAH.indd 57 2/19/07 2:43:16 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R ���0� Bypassgraft,withvein;carotid-contralateralcarotid 1/1/200�
R ��601 Bypassgraft,withotherthanvein;commoncarotid-ipsilateralinternalcarotid
1/1/200�
R ��211 Laparoscopy,surgical;colectomy,totalabdominal,withproctectomy,withileoanalanastomosis,creationofilealreservoir(SorJ),withlookileostomy,includesrectalmucosectomy,whenperformed
1/1/200�
R �1�20 Bladderinstillationofanticarcinogenicagent(includingretentiontime)
1/1/200�
R �220� Cystourethroscopy,withbiopsy(s) 1/1/200�
R ��1�0 Circumcision,usingclamporotherdevicewithregionaldorsalpenileorringblock;neonate(2�daysofageorless)
1/1/200�
R ��160 Circumcision,surgicalexcisionotherthanclamp,device,ordorsalslit;neonate(2�daysofageorless)
1/1/200�
R ��161 Circumcision,surgicalexcisionotherthanclamp,device,ordorsalslit;olderthan2�daysofage
1/1/200�
R ����0 Resection(initial)ofovarian,tubalorprimaryperitonealmalignancywithbilateralsalpingo-oophorectomyandomentectomy;
1/1/200�
R ����1 Resection(initial)ofovarian,tubalorprimaryperitonealmalignancywithbilateralsalpingo-oophorectomyandomentectomy;withtotalabdominalhysterectomy,pelvicandlimitedpara-aorticlymphadenectomy
1/1/200�
R ����2 Resection(initial)ofovarian,tubalorprimaryperitonealmalignancywithbilateralsalpingo-oophorectomyandomentectomy;withradicaldissectionfordebulking(i.e.,radicalexcisionordestruction,intra-abdominalorretroperitonealtumors)
1/1/200�
R 6110� Twistdrillhole(s)forsubdural,intracerebral,orventricularpuncture;forimplantingventricularcatheter,pressurerecordingdevice,orotherintracerebralmonitoringdevice
1/1/200�
R 61210 Burrhole(s);forimplantingventricularcatheter,reservoir,EEGelectrode(s),pressurerecordingdevice,orothercerebralmonitoringdevice(separateprocedure)
1/1/200�
R 6���0 Insertionorreplacementofperipheralorgastricneurostimulatorpulsegeneratororreceiver,directorinductivecoupling
1/1/200�
R 6���� Revisionorremovalofperipheralorgastricneurostimulatorpulsegeneratororreceiver
1/1/200�
R �0��0 Magneticresonance(e.g.,proton)imaging,orbit,face,and/orneck;withoutcontrastmaterial(s)
1/1/200�
R �0��2 Magneticresonance(e.g.,proton)imaging,orbit,face,and/orneck;withcontrastmaterial(s)
1/1/200�
R �0��� Magneticresonance(e.g.,proton)imaging,orbit,face,and/orneck;withoutcontrastmaterial(s),followedbycontrastmaterial(s)andfurthersequences
1/1/200�
R �12�� Computedtomographicangiography,chest(noncoronary)withoutcontrastmaterial(s),followedbycontrastmaterial(s)andfurthersections,includingimagepostprocessing
1/1/200�
R �6��6 Ultrasound,softtissuesofheadandneck(e.g.,thyroid,parathyroid,parotid),realtimewithimagedocumentation
1/1/200�
CPTCoDes
43034txtAH.indd 58 2/19/07 2:43:17 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R �660� Ultrasound,chest,(includesmediastinum)realtimewithimagedocumentation
1/1/200�
R �66�� Ultrasound,breast(s)(unilateralorbilateral),realtimewithimagedocumentation
1/1/200�
R �6�00 Ultrasound,abdominal,realtimewithimagedocumentation;complete
1/1/200�
R �6�0� Ultrasound,abdominal,realtimewithimagedocumentation;limited(e.g.,singleorgan,quadrant,follow-up)
1/1/200�
R �6��0 Ultrasound,retroperitoneal(e.g.,renal,aorta,nodes),realtimewithimagedocumentation;complete
1/1/200�
R �6��� Ultrasound,retroperitoneal(e.g.,renal,aorta,nodes),realtimewithimagedocumentation;limited
1/1/200�
R �6��6 Ultrasound,pelvic(nonobstetric),realtimewithimagedocumentation;complete
1/1/200�
R �6��� Ultrasound,pelvic(nonobstetric),realtimewithimagedocumentation;limitedorfollow-up(e.g.,forfollicles)
1/1/200�
R �6��0 Ultrasound,extremity,nonvascular,realtimewithimagedocumentation
1/1/200�
R �6��0 Ultrasoundguidancefor,andmonitoringof,parenchymaltissueablation
1/1/200�
R ���00 Kidneyimagingmorphology; 1/1/200�
R ���0� Kidneyimagingmorphology;withvascularflowandfunction,singlestudywithoutpharmacologicalintervention.
1/1/200�
R ���0� Kidneyimagingmorphology;withvascularflowandfunction,singlestudy,withpharmacologicalintervention(e.g.,angiotensinconvertingenzymeinhibitorand/ordiuretic)
1/1/200�
R ���0� Kidneyimagingmorphology;withvascularflowandfunction,multiplestudies,withandwithoutpharmacologicalintervention(e.g.,angiotensinconvertingenzymeinhibitorand/ordiuretic)
1/1/200�
R ���10 Kidneyimagingmorphology;tomographic(SPECT) 1/1/200�
R ����0 Urinarybladderresidualstudy(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R ���61 Testicularimaging;withvascularflow 1/1/200�
R ��0�� Culture,bacterial;withisolationandpresumptiveidentificationofeachisolate,urine
1/1/200�
R ��106 Cytopathology,fluids,washingsorbrushings,exceptcervicalorvaginal;simplefiltermethodwithinterpretation
1/1/200�
R ��10� Cytopathology,fluids,washingsorbrushings,exceptcervicalorvaginal;smearsandsimplefilterpreparationwithinterpretation
1/1/200�
R ��060 Crystalidentificationbylightmicroscopywithorwithoutpolarizinglensanalysis,tissueoranybodyfluid(excepturine)
1/1/200�
R �06�� Influenzavirusvaccine,splitvirus,preservativefree,whenadministeredtochildren6-��monthsofage,forintramuscularuse
1/1/200�
R �06�6 Influenzavirusvaccine,splitvirus,preservativefree,whenadministeredtochildren�yearsandolderforintramuscularuse
1/1/200�
CPTCoDes
43034txtAH.indd 59 2/19/07 2:43:17 PM

60Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R �06�� Influenzavirusvaccine,splitvirus,whenadministeredtochildren6-��monthsofage,forintramuscularuse
1/1/200�
R �06�� Influenzavirusvaccine,splitvirus,whenadministeredtochildren�yearsofageandolder,forintramuscularuse
1/1/200�
R �066� Pneumococcalconjugatevaccine,polyvalent,whenadministeredtochildrenyoungerthan�years,forintramuscularuse
1/1/200�
R �0�00 Diphtheria,tetanustoxoids,andacellularpertussisvaccine(DTaP)whenadministeredtoyoungerthanchildren�years,forintramuscularuse
1/1/200�
R �0�02 Diphtheria,andtetanustoxoids(DT)adsorbed,preservativefree,whenadministeredtoyoungerthanchildren�years,forintramuscularuse
1/1/200�
R �0�1� Tetanusanddiphtheriatoxoids(Td)adsorbed,preservativefreewhenadministeredtochildren�yearsorolder,forintramuscularuse
1/1/200�
R �0�1� Tetanus,diphtheriatoxoidsandacellularpertussisvaccine(Tdap),whenadministeredtochildren�yearsorolder,forintramuscularuse
1/1/200�
R �0�1� Tetanusanddiphtheriatoxoids(Td)adsorbedwhenadministeredtochildren�yearsorolder,forintramuscularuse
1/1/200�
R �0��2 Pneumococcalpolysaccharidevaccine,2�-valent,adultorimmunosuppressedpatientdosage,whenadministeredtochildren2yearsorolder,forsubcutaneousorintramuscularuse
1/1/200�
R ��620 Pulmonarystresstesting;simple(e.g.,6minutewalktest,prolongedexercisetestforbronchospasmwithpre-andpost-spirometryandoximetry)
1/1/200�
R ��2�1 Inpatientconsultationforaneworestablishedpatientwhichrequiresthesethreekeycomponents:aproblemfocusedhistory;aproblemfocusedexamination;andstraightforwardmedicaldecisionmaking
1/1/200�
R ��2�2 Inpatientconsultationforaneworestablishedpatientwhichrequiresthesethreekeycomponents:anexpandedproblemfocusedhistory;anexpandedproblemfocusedexamination;andastraightforwardmedicaldecisionmaking
1/1/200�
R ��2�� Inpatientconsultationforaneworestablishedpatientwhichrequiresthesethreekeycomponents:adetailedhistory;adetailedexamination;andmedicaldecisionoflowcomplexity
1/1/200�
R ��2�� Inpatientconsultationforaneworestablishedpatientwhichrequiresthesethreekeycomponents:acomprehensivehistory;acomprehensiveexamination;andmedicaldecisionmakingofmoderatecomplexity
1/1/200�
R ��2�� Inpatientconsultationforaneworestablishedpatientwhichrequiresthesethreekeycomponents:acomprehensivehistory;acomprehensiveexamination;andmedicaldecisionmakingofhighcomplexity
1/1/200�
R 0062T Percutaneousintradiscalannuloplasty,anymethodexceptelectrothermal,unilateralorbilateralincludingfluoroscopicguidance;singlelevel
1/1/200�
CPTCoDes
43034txtAH.indd 60 2/19/07 2:43:18 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 61
ActionA=AdditionD=DeletionR=Revision
CPT®*Code NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R 006�T Percutaneousintradiscalannuloplasty,anymethodexceptelectrothermal,unilateralorbilateralincludingfluoroscopicguidance;oneormoreadditionallevels(Listseparatelyinadditionto0062Tforprimaryprocedure)
1/1/200�
R 006�T Acousticheartsoundrecordingandcomputeranalysis;withinterpretationandreport
1/1/200�
R 006�T Acousticheartsoundrecordingandcomputeranalysis;only
1/1/200�
R 00�0T Acousticheartsoundrecordingandcomputeranalysis;interpretationandreportonly
1/1/200�
R 00��T Spermevaluation,Hyaluronanspermbindingtest 1/1/200�
R 00�0T Totaldiscarthroplasty(artificialdisc),anteriorapproach,includingdiscectomytoprepareinterspace(otherthanfordecompression)cervical;singleinterspace
1/1/200�
R 00�2T Totaldiscarthroplasty(artificialdisc),anteriorapproach,includingdiscectomytoprepareinterspace(otherthanfordecompression)cervical;eachadditionalinterspace(Listseparatelyinadditiontothecodeforprimaryprocedure)
1/1/200�
R 00��T Removaloftotaldiscarthroplasty,anteriorapproachcervical;singleinterspace
1/1/200�
R 00��T Removaloftotaldiscarthroplasty,anteriorapproachcervical;eachadditionalinnerspace(Listseparatelyinadditiontocodeforprimaryprocedure)
1/1/200�
R 00�6T Revisionoftotaldiscarthroplasty,anteriorapproachcervical;singleinterspace
1/1/200�
R 00��T Revisionoftotaldiscarthroplasty,anteriorapproachcervical;eachadditionalinterspace
1/1/200�
CPTCoDes
43034txtAH.indd 61 2/19/07 2:43:18 PM

62Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A C�2�1 Injection,decitabine,per1mg 10/1/2006
A C��2� Insertionofimplantsintothesoftpalate;minimumofthreeimplants
10/1/2006
A K0��� Portablegaseousoxygensystem,rental:homecompressorusedtofillportableoxygencylinders,includesportablecontainers,regulator,flowmeter,humidifier,cannulaormaskandtubing
10/1/2006
A K0�00 Poweroperatedvehicle,group1standard,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�01 Poweroperatedvehicle,group1heavyduty,patientweightcapacity,�01to��0lbs
10/1/2006
A K0�02 Poweroperatedvehicle,group1veryheavyduty,patientweightcapacity��1to600pounds
10/1/2006
A K0�06 Poweroperatedvehicle,group2standard,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�0� Poweroperatedvehicle,group2heavyduty,patientweightcapacity�01to��0pounds
10/1/2006
A K0�0� Poweroperatedvehicle,group2veryheavyduty,patientweightcapacity��1to600pounds
10/1/2006
A K0�12 Poweroperatedvehicle,nototherwiseclassified 10/1/2006
A K0�1� Powerwheelchair,group1standard,portable,sling/solidseatandback,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�1� Powerwheelchair,group1standard,portable,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�1� Powerwheelchair,group1standard,sling/solidseatandback,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�16 Powerwheelchair,group1standard,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�20 Powerwheelchair,group2standard,portable,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�21 Powerwheelchair,group2standard,portable,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�22 Powerwheelchair,group2standard,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�2� Powerwheelchair,group2standard,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�2� Powerwheelchair,group2heavyduty,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0�2� Powerwheelchair,group2heavyduty,captain’schair,patientweightcapacity�01to��0pounds
10/1/2006
A K0�26 Powerwheelchair,group2veryheavyduty,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
A K0�2� Powerwheelchair,group2veryheavyduty,captain’schair,patientweightcapacity��1to600pounds
10/1/2006
HCPCsCoDes
43034txtAH.indd 62 2/19/07 2:43:18 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 6�
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A K0�2� Powerwheelchair,group2extraheavyduty,sling/solidseat/back,patientweightcapacity601poundsormore
10/1/2006
A K0�2� Powerwheelchair,group2extraheavyduty,captain’schair,patientweightcapacity601poundsormore
10/1/2006
A K0��0 Powerwheelchair,group2standard,seatelevator,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��1 Powerwheelchair,group2standard,seatelevator,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group2standard,singlepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��6 Powerwheelchair,group2standard,singlepoweroption,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group2heavyduty,singlepoweroption,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��� Powerwheelchair,group2heavyduty,singlepoweroption,captain’schair,patientweightcapacity�01to��0pounds
10/1/2006
A K0��� Powerwheelchair,group2veryheavyduty,singlepoweroption,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
A K0��0 Powerwheelchair,group2extraheavyduty,singlepoweroptionsling/solidseat/back,patientweightcapacity601poundsormore
10/1/2006
A K0��1 Powerwheelchair,group2standard,multiplepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��2 Powerwheelchair,group2standard,multiplepoweroption,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group2heavyduty,multiplepoweroption,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��� Powerwheelchair,group�standard,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group�standard,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��0 Powerwheelchair,group�heavyduty,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��1 Powerwheelchair,group�heavyduty,captain’schair,patientweightcapacity�01to��0pounds
10/1/2006
A K0��2 Powerwheelchair,group�veryheavyduty,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
A K0��� Powerwheelchair,group�veryheavyduty,captain’schair,patientweightcapacity,��1to600pounds
10/1/2006
A K0��� Powerwheelchair,group�extraheavyduty,sling/solidseat/back,patientweightcapacity601poundsormore
10/1/2006
HCPCsCoDes
43034txtAH.indd 63 2/19/07 2:43:19 PM

6�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A K0��� Powerwheelchair,group�extraheavyduty,captain’schair,patientweightcapacity601poundsormore
10/1/2006
A K0��6 Powerwheelchair,group�standard,singlepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group�standard,singlepoweroption,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group�heavyduty,singlepoweroption,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��� Powerwheelchair,group�heavyduty,singlepoweroption,captain’schair,patientweightcapacity�01to��0pounds
10/1/2006
A K0�60 Powerwheelchair,group�veryheavyduty,singlepoweroption,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
A K0�61 Powerwheelchair,group�standard,multiplepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�62 Powerwheelchair,group�heavyduty,multiplepoweroption,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0�6� Powerwheelchair,group�veryheavyduty,multiplepoweroption,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
A K0�6� Powerwheelchair,group�extraheavyduty,multiplepoweroption,sling/solidseat/back,patientweightcapacity601poundsormore
10/1/2006
A K0�6� Powerwheelchair,group�standard,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0�6� Powerwheelchair,group�standard,captainschair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��0 Powerwheelchair,group�heavyduty,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��1 Powerwheelchair,group�veryheavyduty,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
A K0��� Powerwheelchair,group�standard,singlepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group�standard,singlepoweroption,captain’schair,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group�heavyduty,singlepoweroption,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��0 Powerwheelchair,group�veryheavyduty,singlepoweroption,sling/solidseat/back,patientweightcapacity��1to600pounds
10/1/2006
HCPCsCoDes
43034txtAH.indd 64 2/19/07 2:43:19 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 6�
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A K0��� Powerwheelchair,group�standard,multiplepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding�00pounds
10/1/2006
A K0��� Powerwheelchair,group�standard,multiplepoweroption,captain’schair,weightcapacityuptoandincluding�00pounds
10/1/2006
A K0��6 Powerwheelchair,group�heavyduty,multiplepoweroption,sling/solidseat/back,patientweightcapacity�01to��0pounds
10/1/2006
A K0��0 Powerwheelchair,group�pediatric,singlepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding12�pounds
10/1/2006
A K0��1 Powerwheelchair,group�pediatric,multiplepoweroption,sling/solidseat/back,patientweightcapacityuptoandincluding12�pounds
10/1/2006
A K0��� Powerwheelchair,nototherwiseclassified 10/1/2006
A K0��� Powermobilitydevise,notcodedbySADMERCordoesnotmeetcriteria
10/1/2006
A S01�� Injection,alglucosidaseALFA,20mg 10/1/2006
A S2�2� Hipcoredecompression 10/1/2006
A A��61 Surgicaldressingholder,non-reusable,each 1/1/200�
A A��6� Surgicaldressingholder,reusable,each 1/1/200�
A A���� Couplinggelorpaste,forusewithultrasounddevice,peroz
1/1/200�
A A�600 Sleeveforintermittentlimbcompressiondevice,replacementonly,each
1/1/200�
A A�601 Lithiumionbatteryfornon-prostheticuse,replacement 1/1/200�
A A�000 Helmet,protective,soft,prefabricated,includesallcomponentsandaccessories
1/1/200�
A A�001 Helmet,protective,hard,prefabricated,includesallcomponentsandaccessories
1/1/200�
A A�002 Helmet,protective,soft,customfabricated,includesallcomponentsandaccessories
1/1/200�
A A�00� Helmet,protective,hard,customfabricated,includesallcomponentsandaccessories
1/1/200�
A A�00� Hoftinterfaceforhelmet,replacementonly 1/1/200�
A A�2�� Monitoringfeature/device,stand-aloneorintegrated,anytype,includesallaccessories,componentsandelectronics,nototherwiseclassified
1/1/200�
A A��2� IodineI-12�,sodiumiodidesolution,therapeutic,permillicurie
1/1/200�
A A��6� TechnetiumTc-��marcitumomab,diagnostic,perstudydose,upto��millicuries
1/1/200�
A C1�21 Interspinousprocessdistractiondevice(implantable) 1/1/200�
A C�2�2 Injection,idursulfase,1mg 1/1/200�
A C�2�� Injection,ranibizumab,0.�mg 1/1/200�
A C�2�� Injection,alglucosidasealfa,10mg 1/1/200�
HCPCsCoDes
43034txtAH.indd 65 2/19/07 2:43:20 PM

66Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A C�2�� Injection,panitumumab,10mg 1/1/200�
A C���0 Microporouscollagentubeofnon-humanorigin,percentimeterlength
1/1/200�
A C���1 Acellulardermaltissuematrixofnon-humanorigin,persquarecentimeter(donotreportC���1inconjunctionwithJ����)
1/1/200�
A D01�� Oralevaluationforapatientunderthreeyearsofageandcounselingwithprimarycaregiver
1/1/200�
A D02�� Bitewings-threefilms 1/1/200�
A D0�60 ConebeamCT-craniofacialdatacapture 1/1/200�
A D0�62 Conebeam-two-dimensionalimagereconstructionusingexistingdata,includesmultipleimages
1/1/200�
A D0�6� Conebeam-three-dimensionalimagereconstructionusingexistingdata,includesmultipleimages
1/1/200�
A D0��6 Accessionofbrushbiopsysample,microscopicexamination,preparationandtransmissionofwrittenreport
1/1/200�
A D1206 Topicalfluoridevarnish;therapeuticapplicationformoderatetohighcariesriskpatients
1/1/200�
A D1��� Removaloffixedspacemaintainer 1/1/200�
A D�2�0 Anatomicalcrownexposure-fourormorecontiguousteethperquadrant
1/1/200�
A D�2�1 Anatomicalcrownexposure-onetothreeteethperquadrant
1/1/200�
A D6012 Surgicalplacementofinterimimplantbodyfortransitionalprosthesis:endostealimplant
1/1/200�
A D60�1 Replacementofsemi-precisionorprecisionattachment(maleorfemalecomponent)ofimplant/abutmentsupportedprosthesis,perattachment
1/1/200�
A D60�2 Recementimplant/abutmentsupportedcrown 1/1/200�
A D60�� Recementimplant/abutmentsupportedfixedpartialdenture
1/1/200�
A D�2�2 Surgicalplacement:temporaryanchoragedevice[screwretainedplate]requiringsurgicalflap
1/1/200�
A D�2�� Surgicalplacement:temporaryanchoragedevicerequiringsurgicalflap
1/1/200�
A D�2�� Surgicalplacement:temporaryanchoragedevicewithoutsurgicalflap
1/1/200�
A D���1 Sinusaugmentationwithboneorbonesubstitutes 1/1/200�
A D���� Intraoralplacementofafixationdevicenotinconjunctionwithafracture
1/1/200�
A D�6�� Rebondingorrecementing;and/orrepair,asrequired,offixedretainers
1/1/200�
A D�120 Fixedpartialdenturesectioning 1/1/200�
A D�612 Therapeuticparenteraldrugs,twoormoreadministrations,differentmedications
1/1/200�
A E06�6 Intermittentlimbcompressiondevice(includesallaccessories),nototherwisespecified
1/1/200�
HCPCsCoDes
43034txtAH.indd 66 2/19/07 2:43:20 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 6�
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A E0��6 Continuouspassivemotionexercisedeviceforuseotherthanknee
1/1/200�
A E2��� Powerwheelchairaccessory,handorchincontrolinterface,mini-proportional,compact,orshortthrowremotejoystickortouchpad,proportional,includingallrelatedelectronicsandfixedmountinghardware
1/1/200�
A E2��� Powerwheelchairaccessory,handorchincontrolinterface,standardremotejoystick(notincludingcontroller),proportional,includingallrelatedelectronicsandfixedmountinghardware,replacementonly
1/1/200�
A E2��� Powerwheelchairaccessory,non-expandablecontroller,includingallrelatedelectronicsandmountinghardware,replacementonly
1/1/200�
A E2��6 Powerwheelchairaccessory,expandablecontroller,includingallrelatedelectronicsandmountinghardware,replacementonly
1/1/200�
A E2��� Powerwheelchairaccessory,expandablecontroller,includingallrelatedelectronicsandmountinghardware,upgradeprovidedatinitialissue
1/1/200�
A E2��1 Powerwheelchairaccessory,pneumaticdrivewheeltire,anysize,replacementonly,each
1/1/200�
A E2��2 Powerwheelchairaccessory,tubeforpneumaticdrivewheeltire,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,insertforpneumaticdrivewheeltire(removable),anytype,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,pneumaticcastertire,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,tubeforpneumaticcastertire,anysize,replacementonly,each
1/1/200�
A E2��6 Powerwheelchairaccessory,foamfilleddrivewheeltire,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,foamfilledcastertire,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,foamdrivewheeltire,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,foamcastertire,anysize,replacementonly,each
1/1/200�
A E2��0 Powerwheelchairaccessory,solid(rubber/plastic)drivewheeltire,anysize,replacementonly,each
1/1/200�
A E2��1 Powerwheelchairaccessory,solid(rubber/plastic)castertire(removable),anysize,replacementonly,each
1/1/200�
A E2��2 Powerwheelchairaccessory,solid(rubber/plastic)castertirewithintegratedwheel,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,valveforpneumatictiretube,anytype,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,drivewheelexcludestire,anysize,replacementonly,each
1/1/200�
A E2��� Powerwheelchairaccessory,casterwheelexcludestire,anysize,replacementonly,each
1/1/200�
HCPCsCoDes
43034txtAH.indd 67 2/19/07 2:43:21 PM
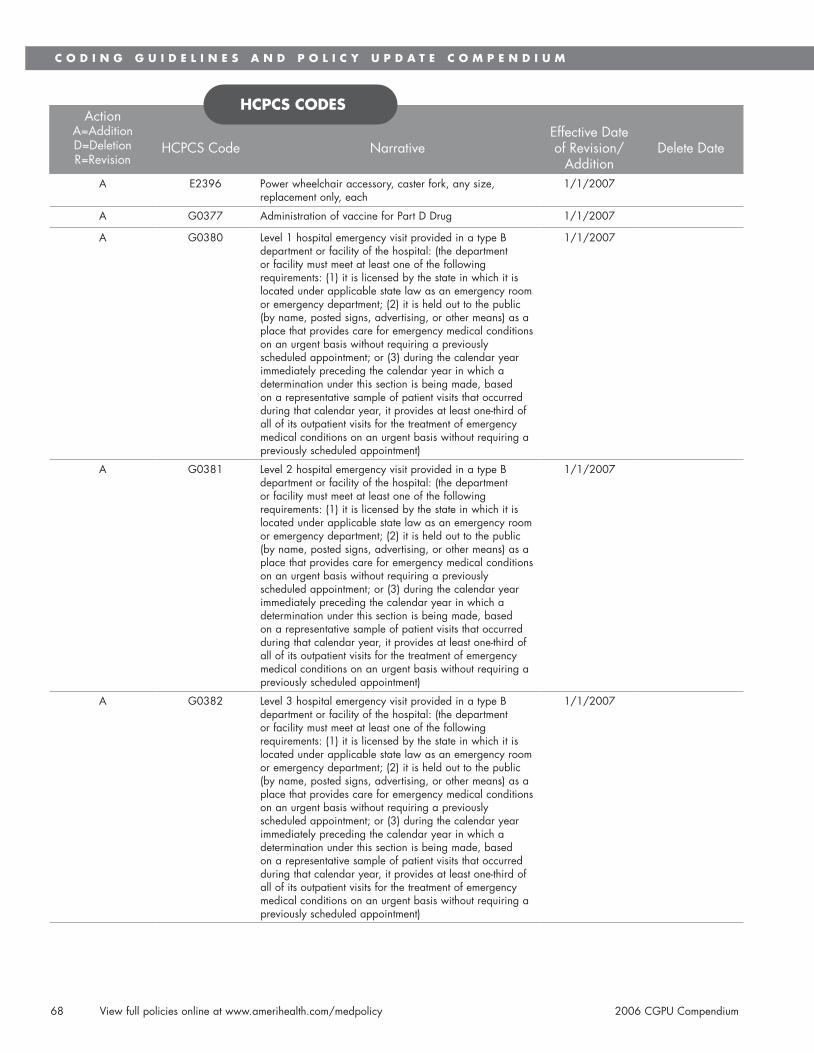
6�Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A E2��6 Powerwheelchairaccessory,casterfork,anysize,replacementonly,each
1/1/200�
A G0��� AdministrationofvaccineforPartDDrug 1/1/200�
A G0��0 Level1hospitalemergencyvisitprovidedinatypeBdepartmentorfacilityofthehospital:(thedepartmentorfacilitymustmeetatleastoneofthefollowingrequirements:(1)itislicensedbythestateinwhichitislocatedunderapplicablestatelawasanemergencyroomoremergencydepartment;(2)itisheldouttothepublic(byname,postedsigns,advertising,orothermeans)asaplacethatprovidescareforemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment;or(�)duringthecalendaryearimmediatelyprecedingthecalendaryearinwhichadeterminationunderthissectionisbeingmade,basedonarepresentativesampleofpatientvisitsthatoccurredduringthatcalendaryear,itprovidesatleastone-thirdofallofitsoutpatientvisitsforthetreatmentofemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment)
1/1/200�
A G0��1 Level2hospitalemergencyvisitprovidedinatypeBdepartmentorfacilityofthehospital:(thedepartmentorfacilitymustmeetatleastoneofthefollowingrequirements:(1)itislicensedbythestateinwhichitislocatedunderapplicablestatelawasanemergencyroomoremergencydepartment;(2)itisheldouttothepublic(byname,postedsigns,advertising,orothermeans)asaplacethatprovidescareforemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment;or(�)duringthecalendaryearimmediatelyprecedingthecalendaryearinwhichadeterminationunderthissectionisbeingmade,basedonarepresentativesampleofpatientvisitsthatoccurredduringthatcalendaryear,itprovidesatleastone-thirdofallofitsoutpatientvisitsforthetreatmentofemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment)
1/1/200�
A G0��2 Level�hospitalemergencyvisitprovidedinatypeBdepartmentorfacilityofthehospital:(thedepartmentorfacilitymustmeetatleastoneofthefollowingrequirements:(1)itislicensedbythestateinwhichitislocatedunderapplicablestatelawasanemergencyroomoremergencydepartment;(2)itisheldouttothepublic(byname,postedsigns,advertising,orothermeans)asaplacethatprovidescareforemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment;or(�)duringthecalendaryearimmediatelyprecedingthecalendaryearinwhichadeterminationunderthissectionisbeingmade,basedonarepresentativesampleofpatientvisitsthatoccurredduringthatcalendaryear,itprovidesatleastone-thirdofallofitsoutpatientvisitsforthetreatmentofemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment)
1/1/200�
HCPCsCoDes
43034txtAH.indd 68 2/19/07 2:43:21 PM
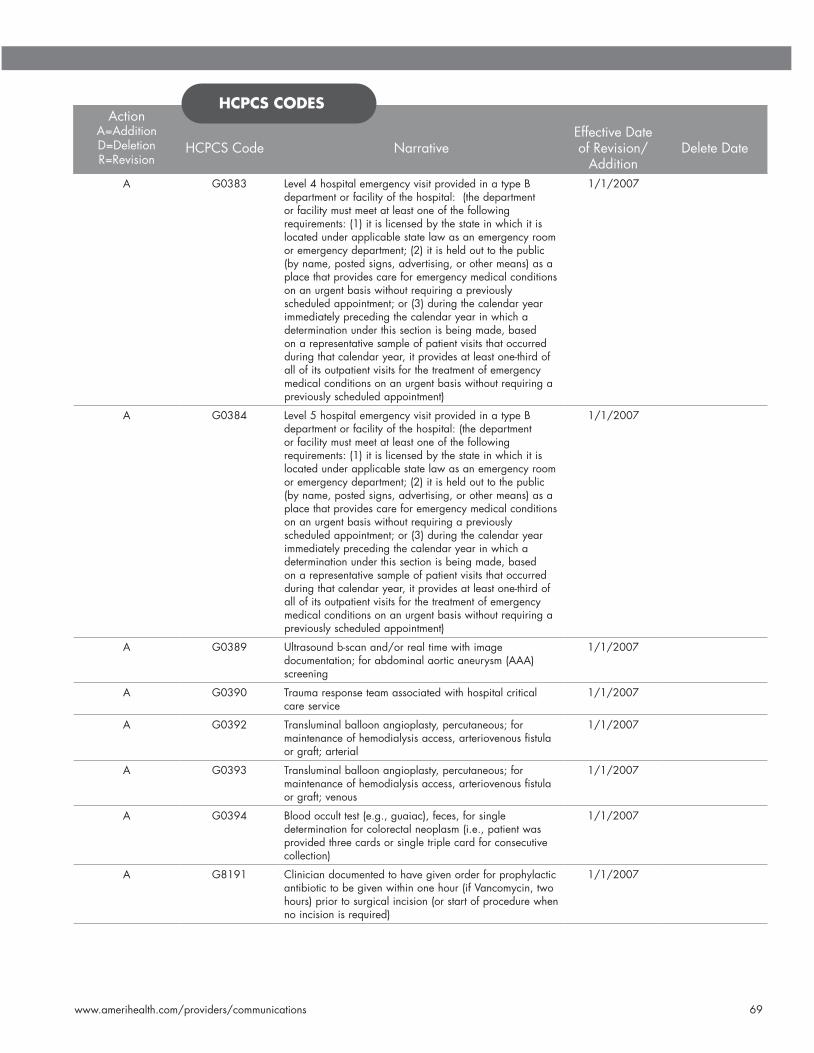
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications 6�
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G0��� Level�hospitalemergencyvisitprovidedinatypeBdepartmentorfacilityofthehospital:(thedepartmentorfacilitymustmeetatleastoneofthefollowingrequirements:(1)itislicensedbythestateinwhichitislocatedunderapplicablestatelawasanemergencyroomoremergencydepartment;(2)itisheldouttothepublic(byname,postedsigns,advertising,orothermeans)asaplacethatprovidescareforemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment;or(�)duringthecalendaryearimmediatelyprecedingthecalendaryearinwhichadeterminationunderthissectionisbeingmade,basedonarepresentativesampleofpatientvisitsthatoccurredduringthatcalendaryear,itprovidesatleastone-thirdofallofitsoutpatientvisitsforthetreatmentofemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment)
1/1/200�
A G0��� Level�hospitalemergencyvisitprovidedinatypeBdepartmentorfacilityofthehospital:(thedepartmentorfacilitymustmeetatleastoneofthefollowingrequirements:(1)itislicensedbythestateinwhichitislocatedunderapplicablestatelawasanemergencyroomoremergencydepartment;(2)itisheldouttothepublic(byname,postedsigns,advertising,orothermeans)asaplacethatprovidescareforemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment;or(�)duringthecalendaryearimmediatelyprecedingthecalendaryearinwhichadeterminationunderthissectionisbeingmade,basedonarepresentativesampleofpatientvisitsthatoccurredduringthatcalendaryear,itprovidesatleastone-thirdofallofitsoutpatientvisitsforthetreatmentofemergencymedicalconditionsonanurgentbasiswithoutrequiringapreviouslyscheduledappointment)
1/1/200�
A G0��� Ultrasoundb-scanand/orrealtimewithimagedocumentation;forabdominalaorticaneurysm(AAA)screening
1/1/200�
A G0��0 Traumaresponseteamassociatedwithhospitalcriticalcareservice
1/1/200�
A G0��2 Transluminalballoonangioplasty,percutaneous;formaintenanceofhemodialysisaccess,arteriovenousfistulaorgraft;arterial
1/1/200�
A G0��� Transluminalballoonangioplasty,percutaneous;formaintenanceofhemodialysisaccess,arteriovenousfistulaorgraft;venous
1/1/200�
A G0��� Bloodocculttest(e.g.,guaiac),feces,forsingledeterminationforcolorectalneoplasm(i.e.,patientwasprovidedthreecardsorsingletriplecardforconsecutivecollection)
1/1/200�
A G�1�1 Cliniciandocumentedtohavegivenorderforprophylacticantibiotictobegivenwithinonehour(ifVancomycin,twohours)priortosurgicalincision(orstartofprocedurewhennoincisionisrequired)
1/1/200�
HCPCsCoDes
43034txtAH.indd 69 2/19/07 2:43:21 PM

�0Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�1�2 Cliniciandocumentedtohavegiventheprophylacticantibioticwithinonehour(ifVancomycin,twohours)priortothesurgicalincision(orstartofprocedurewhennoincisionisrequired)
1/1/200�
A G�1�� Cliniciandidnotdocumentthatanorderforprophylacticantibiotictobegivenwithinonehour(ifVancomycin,twohours)priortosurgicalincision(orstartofprocedurewhennoincisionisrequired)wasgiven
1/1/200�
A G�1�� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforprophylacticantibiotic
1/1/200�
A G�1�� Cliniciandocumentedtohavegiventheprophylacticantibioticwithinonehour(ifVancomycin,twohours)priortothesurgicalincision(orstartofprocedurewhennoincisionisrequired)
1/1/200�
A G�1�6 Cliniciandidnotdocumentaprophylacticantibioticwasadministeredwithinonehour(ifVancomycin,twohours)priortosurgicalincision(orstartofprocedurewhennoincisionisrequired)
1/1/200�
A G�1�� Patientdocumentedtohaveorderforprophylacticantibiotictobegivenwithinonehour(ifVancomycin,twohours)priortosurgicalincision(orstartofprocedurewhennoincisionisrequired)
1/1/200�
A G�1�� PatientdocumentedtohaveorderforCefazolinorCefuroximeforantimicrobialprophylaxis
1/1/200�
A G�1�� CliniciandocumentedtohavegivenCefazolinorCefuroximeforantimicrobialprophylaxis
1/1/200�
A G�200 OrderforCefazolinorCefuroximeforantimicrobialprophylaxisnotdocumented
1/1/200�
A G�201 PatientwasnotaneligiblecandidateforCefazolinorCefuroximeforantimicrobialprophylaxis
1/1/200�
A G�202 Cliniciandocumentedanorderwasgiventodiscontinueprophylacticantibioticswithin2�hoursofsurgicalendtime
1/1/200�
A G�20� Cliniciandocumentedthatprophylacticantibioticswerediscontinuedwithin2�hoursofsurgicalendtime
1/1/200�
A G�20� Cliniciandidnotdocumentanorderwasgiventodiscontinueprophylacticantibioticswithin2�hoursofsurgicalendtime
1/1/200�
A G�20� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforprophylacticantibioticdiscontinuationwithin2�hoursofsurgicalendtime
1/1/200�
A G�206 Cliniciandocumentedthatprophylacticantibioticwasgiven
1/1/200�
A G�20� Cliniciandocumentedanorderwasgiventodiscontinueprophylacticantibioticswithin��hoursofsurgicalendtime
1/1/200�
A G�20� Cliniciandocumentedthatprophylacticantibioticswerediscontinuedwithin��hoursofsurgicalendtime
1/1/200�
A G�20� Cliniciandidnotdocumentanorderwasgiventodiscontinueprophylacticantibioticswithin��hoursofsurgicalendtime
1/1/200�
HCPCsCoDes
43034txtAH.indd 70 2/19/07 2:43:22 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �1
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�210 Cliniciandocumentedpatientwasnotaneligiblecandidatefordiscontinuationofprophylacticantibioticdiscontinuationwithin��hoursofsurgicalendtime
1/1/200�
A G�211 Cliniciandocumentedthatprophylacticantibioticwasgiven
1/1/200�
A G�212 Cliniciandocumentedanorderwasgivenforappropriatevenousthromboembolism(VTE)prophylaxistobegivenwithin2�hrspriortoincisiontimeor2�hoursaftersurgeryendtime
1/1/200�
A G�21� CliniciandocumentedtohavegivenVTEprophylaxiswithin2�hrspriortoincisiontimeor2�hoursaftersurgeryendtime
1/1/200�
A G�21� Cliniciandidnotdocumentanorderwasgivenforappropriatevenousthromboembolism(VTE)prophylaxistobegivenwithin2�hrspriortoincisiontimeor2�hoursaftersurgeryendtime
1/1/200�
A G�21� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforvenousthromboembolism(VTE)prophylaxistobegivenwithin2�hourspriortoincisiontimeor2�hoursaftersurgeryendtime
1/1/200�
A G�216 PatientdocumentedtohavereceivedDVTprophylaxisbyendofhospitaldaytwo
1/1/200�
A G�21� PatientnotdocumentedtohavereceivedDVTprophylaxisbyendofhospitalday2
1/1/200�
A G�21� PatientwasnotaneligiblecandidateforDVTprophylaxisbyendofhospitalday2,includingphysiciandocumentationthatpatientisambulatory
1/1/200�
A G�21� PatientdocumentedtohavereceivedDVTprophylaxisbyendofhospitalday2
1/1/200�
A G�220 PatientnotdocumentedtohavereceivedDVTprophylaxisbyendofhospitalday2
1/1/200�
A G�221 CliniciandocumentedthatpatientwasnotaneligiblecandidateforDVTprophylaxisbytheendofhospitalday2,includingphysiciandocumentationthatpatientisambulatory
1/1/200�
A G�222 Patientdocumentedtohavebeenprescribedantiplatelettherapyatdischarge
1/1/200�
A G�22� Patientnotdocumentedtohavereceivedprescriptionforantiplatelettherapyatdischarge
1/1/200�
A G�22� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforantiplatelettherapyatdischarge,includingidentificationfrommedicalrecordthatpatientisonanticoagulationtherapy
1/1/200�
A G�22� Patientdocumentedtohavebeenprescribedananticoagulantatdischarge
1/1/200�
A G�226 Patientnotdocumentedtohavereceivedprescriptionforanticoagulanttherapyatdischarge
1/1/200�
A G�22� Patientnotdocumentedtohavepermanent,persistent,orparoxysmalatrialfibrillation
1/1/200�
A G�22� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforanticoagulanttherapyatdischarge
1/1/200�
A G�22� PatientdocumentedtohavebeenadministeredorconsideredforT-PA
1/1/200�
HCPCsCoDes
43034txtAH.indd 71 2/19/07 2:43:22 PM

�2Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�2�0 PatientnoteligibleforT-PAadministration,ischemicstrokesymptomonsetofmorethan�hours
1/1/200�
A G�2�1 PatientnotdocumentedtohavereceivedT-PAornotdocumentedtohavebeenconsideredacandidateforT-PAadministration
1/1/200�
A G�2�2 Patientdocumentedtohavereceiveddysphagiascreeningpriortotakinganyfoods,fluidsormedicationbymouth
1/1/200�
A G�2�� Patientnotdocumentedtohavereceiveddysphagiascreening
1/1/200�
A G�2�� Patientnotreceivingorineligibletoreceivefood,fluidsormedicationbymouth,ordocumentationofNPO(nothingbymouth)order
1/1/200�
A G�2�6 Cliniciandocumentedthatpatientwasnotaneligiblecandidatefordysphagiascreeningpriortotakinganyfoods,fluidsormedicationbymouth
1/1/200�
A G�2�� Patientdocumentedtohavereceivedorderforrehabilitationservicesordocumentationofconsiderationforrehabilitationservices
1/1/200�
A G�2�� Patientnotdocumentedtohavereceivedorderfororconsiderationforrehabilitationservices
1/1/200�
A G�2�� Internalcarotidstenosispatientbelow�0%,referencetomeasurementsofdistalinternalcarotiddiameterasthedenominatorforstenosismeasurementnotnecessary
1/1/200�
A G�2�0 Internalcarotidstenosispatientinthe�0-��%range,andnodocumentationofreferencetomeasurementsofdistalinternalcarotiddiameterasthedenominatorforstenosismeasurement
1/1/200�
A G�2�1 Cliniciandocumentedthatpatientwhosefinalreportofthecarotidimagingstudyperformed(neckMRA,neckCTA,neckduplexultrasound,carotidangiogram),withcharacterizationofaninternalcarotidstenosisinthe�0-��%range,wasnotaneligiblecandidateforreferencetomeasurementsofdistalinternalcarotiddiameterasthedenominatorforstenosismeasurement
1/1/200�
A G�2�2 PatientdocumentedtohavereceivedCTorMRIwithpresenceorabsenceofhemorrhage,masslesionandacuteinfarctiondocumentedinthefinalreport
1/1/200�
A G�2�� PatientnotdocumentedtohavereceivedCTorMRIandthepresenceorabsenceofhemorrhage,masslesionandacuteinfarctionnotdocumentedinthefinalreport
1/1/200�
A G�2�� Cliniciandocumentedpresenceorabsencealarmsymptoms
1/1/200�
A G�2�6 Patientwasnotaneligiblecandidateformedicalhistoryreviewwithassessmentofneworchangingmoles
1/1/200�
A G�2�� Patientwithalarmsymptom(s)documentedtohavehadupperendoscopyperformedorreferralforupperendoscopy
1/1/200�
A G�2�� Patientwithatleastonealarmsymptomnotdocumentedtohavehadupperendoscopyorreferralforupperendoscopy
1/1/200�
A G�2�� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforupperendoscopy
1/1/200�
HCPCsCoDes
43034txtAH.indd 72 2/19/07 2:43:23 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�2�0 PatientwithsuspicionofBarrett’sesophagusinendoscopyreportanddocumentedtohavereceivedanesophagealbiopsy
1/1/200�
A G�2�1 PatientnotdocumentedtohavereceivedanesophagealbiopsywhensuspicionofBarrett’sesophagusisindicatedintheendoscopyreport
1/1/200�
A G�2�2 Cliniciandocumentedthatpatientwasnotaneligiblecandidateforesophagealbiopsy
1/1/200�
A G�2�� Patientdocumentedtohavereceivedanorderforabariumswallowtest
1/1/200�
A G�2�� Patientwithnodocumentationorderforbariumswallowtest
1/1/200�
A G�2�� Cliniciandocumentationthatpatientwasaneligiblecandidateforbariumswallowtest
1/1/200�
A G�2�6 Cliniciandocumentedreconciliationofdischargemedicationswithcurrentmedicationlistinmedicalrecord
1/1/200�
A G�2�� Clinicianhasnotdocumentedreconciliationofdischargemedicationswithcurrentmedicationlistinmedicalrecord
1/1/200�
A G�2�� Patientwasnotaneligiblecandidatefordischargemedicationsreview
1/1/200�
A G�2�� Patientdocumentedtohavesurrogatedecisionmakeroradvancecareplaninmedicalrecord
1/1/200�
A G�260 Patientnotdocumentedtohavesurrogatedecisionmakeroradvancecareplaninmedicalrecord
1/1/200�
A G�261 Cliniciandocumentedthatpatientwasnotaneligiblecandidateforsurrogatedecisionmakeroradvancecareplan
1/1/200�
A G�262 Patientdocumentedtohavebeenassessedforpresenceorabsenceofurinaryincontinence
1/1/200�
A G�26� Patientnotdocumentedtohavebeenassessedforpresenceorabsenceofurinaryincontinence
1/1/200�
A G�26� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforanassessmentofthepresenceorabsenceofurinaryincontinence
1/1/200�
A G�26� Patientdocumentedtohavereceivedcharacterizationofurinaryincontinence
1/1/200�
A G�266 Patientnotdocumentedtohavereceivedcharacterizationofurinaryincontinence
1/1/200�
A G�26� Patientdocumentedtohavereceivedaplanofcareforurinaryincontinence
1/1/200�
A G�26� Patientnotdocumentedtohavereceivedplanofcareforurinaryincontinence
1/1/200�
A G�26� Clinicianhasnotprovidedcareforthepatientfortherequiredtimetodevelopplanofcareforurinaryincontinence
1/1/200�
A G�2�0 Patientdocumentedtohavereceivedscreeningforfallrisk(2ormorefallsinthepastyearoranyfallwithinjuryinthepastyear)
1/1/200�
A G�2�1 Patientwithnodocumentationofscreeningforfallrisks(2ormorefallsinthepastyearoranyfallwithinjuryinthepastyear)
1/1/200�
HCPCsCoDes
43034txtAH.indd 73 2/19/07 2:43:23 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�2�2 Cliniciandocumentationthatpatientwasnotaneligiblecandidateforfallriskscreening
1/1/200�
A G�2�� Clinicianhasnotprovidedcareforthepatientfortherequiredtimetoscreenforfallrisk
1/1/200�
A G�2�� Clinicianhasnotdocumentedpresenceorabsenceofalarmsymptoms
1/1/200�
A G�2�� Patientdocumentedtohavemedicalhistorytakenwhichincludedassessmentofneworchangingmoles
1/1/200�
A G�2�6 Patientnotdocumentedtohavereceivedmedicalhistorywithassessmentofneworchangingmoles
1/1/200�
A G�2�� Patientwasnotaneligiblecandidateformedicalhistoryreviewwithassessmentofneworchangingmoles
1/1/200�
A G�2�� Patientdocumentedtohavereceivedcompletephysicalskinexam
1/1/200�
A G�2�� Patientnotdocumentedtohavereceivedacompletephysicalskinexam
1/1/200�
A G�2�0 Patientwasnotaneligiblecandidateforcompletephysicalskinexamduringthereportingyear
1/1/200�
A G�2�1 Patientdocumentedtohavereceivedcounselingtoperformaself-examination
1/1/200�
A G�2�2 Patientnotdocumentedtohavereceivedcounselingtoperformaself-examination
1/1/200�
A G�2�� Patientwasnotaneligiblecandidateforcounselingtoperformself-examination
1/1/200�
A G�2�� Patientdocumentedtohavereceivedaprescriptionforpharmacologictherapyforosteoporosis
1/1/200�
A G�2�� Patientnotdocumentedtohavereceivedpharmacologictherapy
1/1/200�
A G�2�6 Cliniciandocumentedthatpatientwasnotaneligiblecandidateforpharmacologictherapy
1/1/200�
A G�2�� Clinicianhasnotprovidedcareforthepatientfortherequiredtimeforthepharmacologictherapymeasure
1/1/200�
A G�2�� PatientdocumentedtohavereceivedcalciumandvitaminDorcounselingonbothcalciumandvitaminDuse,andexercise
1/1/200�
A G�2�� PatientwithnodocumentationofcalciumandvitaminDuseorcounselingregardingbothcalciumandvitaminDuse,orexercise
1/1/200�
A G�2�0 CliniciandocumentationthatpatientwasnotaneligiblecandidateforcalciumandvitaminD,andexerciseduringthereportingyear
1/1/200�
A G�2�1 Clinicianhasnotprovidedcareforthepatientfortherequiredtimeforthecalcium,vitaminD,andexercisemeasure
1/1/200�
A G�2�2 COPDpatientwithspirometryresultsdocumented 1/1/200�
A G�2�� COPDpatientwithoutspirometryresultsdocumented 1/1/200�
A G�2�� COPDpatientwasnoteligibleforspirometryresults 1/1/200�
A G�2�� COPDpatientdocumentedtohavereceivedinhaledbronchodilatortherapy
1/1/200�
HCPCsCoDes
43034txtAH.indd 74 2/19/07 2:43:24 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�2�6 COPDpatientnotdocumentedtohaveinhaledbronchodilatortherapyprescribed
1/1/200�
A G�2�� COPDpatientwasnoteligibleforinhaledbronchodilatortherapy
1/1/200�
A G�2�� Patientdocumentedtohavereceivedopticnerveheadevaluation
1/1/200�
A G�2�� Patientnotdocumentedtohavereceivedopticnerveheadevaluation
1/1/200�
A G��00 Cliniciandocumentedthatpatientwasnotaneligiblecandidateforopticnerveheadevaluationduringthereportingyear
1/1/200�
A G��01 Clinicianhasnotprovidedcarefortheprimaryopen-angleglaucomapatientfortherequiredtimeforopticnerveheadevaluationmeasure
1/1/200�
A G��02 Patientdocumentedtohaveaspecifictargetintraocularpressurerangegoal
1/1/200�
A G��0� Patientnotdocumentedtohaveaspecifictargetintraocularpressurerangegoal
1/1/200�
A G��0� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforaspecifictargetintraocularpressurerangegoal
1/1/200�
A G��0� Clinicianhasnotprovidedcarefortheprimaryopen-angleglaucomapatientfortherequiredtimefortreatmentrangegoaldocumentationmeasurement
1/1/200�
A G��06 Primaryopen-angleglaucomapatientwithintraocularpressureabovethetargetrangegoaldocumentedtohavereceivedplanofcare
1/1/200�
A G��0� Primaryopen-angleglaucomapatientwithintraocularpressureatorbelowgoal,noplanofcarenecessary
1/1/200�
A G��0� Primaryopen-angleglaucomapatientwithintraocularpressureabovethetargetrangegoal,andnotdocumentedtohavereceivedplanofcareduringthereportingyear
1/1/200�
A G��0� Patientdocumentedtohavebeenprescribed/recommendedantioxidantvitaminormineralsupplement
1/1/200�
A G��10 Patientnotdocumentedtohavebeenprescribed/recommendedatleastoneantioxidantvitaminormineralsupplementduringthereportingyear
1/1/200�
A G��11 Cliniciandocumentationthatpatientwasnotaneligiblecandidateforantioxidantvitaminormineralsupplementduringthereportingyear
1/1/200�
A G��12 Clinicianhasnotprovidedcarefortheage-relatedmaculardegenerationpatientfortherequiredtimeforantioxidantsupplementprescription/recommendedmeasure
1/1/200�
A G��1� Patientdocumentedtohavereceivedmacularexam,includingdocumentationofthepresenceorabsenceofmacularthickeningorhemorrhageandthelevelofmaculardegenerationseverity
1/1/200�
A G��1� Patientnotdocumentedtohavereceivedmacularexamwithdocumentationofpresenceorabsenceofmacularthickeningorhemorrhageandnodocumentationoflevelofmaculardegenerationseverity
1/1/200�
HCPCsCoDes
43034txtAH.indd 75 2/19/07 2:43:24 PM

�6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G��1� Cliniciandocumentationthatpatientwasnotaneligiblecandidateformacularexaminationduringthereportingyear
1/1/200�
A G��16 Clinicianhasnotprovidedcarefortheage-relatedmaculardegenerationpatientfortherequiredtimeformacularexaminationmeasurement
1/1/200�
A G��1� Patientdocumentedtohavevisualfunctionalstatusassessed
1/1/200�
A G��1� Patientdocumentednottohavevisualfunctionalstatusassessed
1/1/200�
A G��1� Cliniciandocumentedthatpatientwasnotaneligiblecandidateforassessmentofvisualfunctionalstatus
1/1/200�
A G��20 Clinicianhasnotprovidedcareforthecataractpatientfortherequiredtimeforassessmentofvisualfunctionalstatusmeasurement
1/1/200�
A G��21 Patientdocumentedtohavehadpre-surgicalaxiallength,cornealpowermeasurementandmethodofintraocularlenspowercalculation
1/1/200�
A G��22 Patientnotdocumentedtohavehadpre-surgicalaxiallength,cornealpowermeasurementandmethodofintraocularlenspowercalculation
1/1/200�
A G��2� Cliniciandocumentationthatpatientwasnotaneligiblecandidateforpre-surgicalaxiallength,cornealpowermeasurementandmethodofintraocularlenspowercalculation
1/1/200�
A G��2� Clinicianhasnotprovidedcareforthecataractpatientfortherequiredtimeforpre-surgicalmeasurementandintraocularlenspowercalculationmeasure
1/1/200�
A G��2� Patientdocumentedtohavereceivedfundusevaluationwithinsixmonthspriortocataractsurgery
1/1/200�
A G��26 Patientnotdocumentedtohavereceivedfundusevaluationwithinsixmonthspriortocataractsurgery
1/1/200�
A G��2� Patientwasnotaneligiblecandidateforpre-surgicalfundusevaluation
1/1/200�
A G��2� Clinicianhasnotprovidedcareforthecataractpatientfortherequiredtimeforfundusevaluationmeasurement
1/1/200�
A G��2� Patientdocumentedtohavereceiveddilatedmacularorfundusexamwithlevelofseverityofretinopathyandthepresenceorabsenceofmacularedemadocumented
1/1/200�
A G���0 Patientnotdocumentedtohavereceiveddilatedmacularorfundusexamwithlevelofseverityofretinopathyandthepresenceorabsenceofmacularedemanotdocumented
1/1/200�
A G���1 Cliniciandocumentationthatpatientwasnotaneligiblecandidatefordilatedmacularorfundusexamduringthereportingyear
1/1/200�
A G���2 Clinicianhasnotprovidedcareforthediabeticretinopathypatientfortherequiredtimeformacularedemaandretinopathymeasurement
1/1/200�
A G���� Patientdocumentedtohavehadfindingsofmacularorfundusexamcommunicatedtothephysicianmanagingthediabetescare
1/1/200�
HCPCsCoDes
43034txtAH.indd 76 2/19/07 2:43:25 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G���� Documentationoffindingsofmacularorfundusexamnotcommunicatedtothephysicianmanagingthepatient’songoingdiabetescare
1/1/200�
A G���� Cliniciandocumentationthatpatientwasnotaneligiblecandidateforthefindingsoftheirmacularorfundusexambeingcommunicatedtothephysicianmanagingtheirdiabetescareduringthereportingyear
1/1/200�
A G���6 Clinicianhasnotprovidedcareforthediabeticretinopathypatientfortherequiredtimeforphysiciancommunicationmeasurement
1/1/200�
A G���� Cliniciandocumentedthatcommunicationwassenttothephysicianmanagingongoingcareofpatientthatafractureoccurredandthatthepatientwasorshouldbetestedortreatedforosteoporosis
1/1/200�
A G���� Clinicianhasnotdocumentedthatcommunicationwassenttothephysicianmanagingongoingcareofpatientthatafractureoccurredandthatthepatientwasorshouldbetestedortreatedforosteoporosis
1/1/200�
A G���� Patientwasnotaneligiblecandidateforcommunicationwiththephysicianmanagingthepatient’songoingcarethatafractureoccurredandthatthepatientwasorshouldbetestedortreatedforosteoporosis
1/1/200�
A G���0 PatientdocumentedtohavehadcentralDEXAperformedandresultsdocumentedorcentralDEXAorderedorpharmacologictherapyprescribed
1/1/200�
A G���1 PatientnotdocumentedtohavehadcentralDEXAmeasurementorpharmacologictherapy
1/1/200�
A G���2 CliniciandocumentedthatpatientwasnotaneligiblecandidateforcentralDEXAmeasurementorprescribingpharmacologic
1/1/200�
A G���� ClinicianhasnotprovidedcareforthepatientfortherequiredtimeforcentralDEXAmeasurementorpharmacologicaltherapymeasure
1/1/200�
A G���� PatientdocumentedtohavehadcentralDEXAorderedorperformedandresultsdocumentedorpharmacologicaltherapyprescribed
1/1/200�
A G���� PatientnotdocumentedtohavehadcentralDEXAmeasurementorderedorperformedorpharmacologictherapy
1/1/200�
A G���6 CliniciandocumentedthatpatientwasnotaneligiblecandidateforcentralDEXAmeasurementorpharmacologictherapy
1/1/200�
A G���� ClinicianhasnotprovidedcareforthepatientfortherequiredtimeforcentralDEXAmeasurementorpharmacologicaltherapymeasure
1/1/200�
A G�1�1 Oncology;diseasestatus;invasivefemalebreastcancer(doesnotincludeductalcarcinomainsitu);adenocarcinomaaspredominantcelltype;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�2 Oncology;diseasestatus;prostatecancer,limitedtoadenocarcinoma;hormone-refractory/androgen-independent(e.g.,risingPSAonanti-androgentherapyorpost-orchiectomy);clinicalmetastases(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
HCPCsCoDes
43034txtAH.indd 77 2/19/07 2:43:25 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A G�1�� Oncology;diseasestatus;prostatecancer,limitedtoadenocarcinoma;hormone-responsive;clinicalmetastasesorM1atdiagnosis(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�� Oncology;diseasestatus;non-Hodgkin’slymphoma,anycellularclassification;stageI,IIatdiagnosis,notrelapsed,notrefractory(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�� Oncology;diseasestatus;non-Hodgkin’slymphoma,anycellularclassification;stageIII,IV,notrelapsed,notrefractory(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�6 Oncology;diseasestatus;non-Hodgkin’slymphoma,transformedfromoriginalcellulardiagnosistoasecondcellularclassification(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�� Oncology;diseasestatus;non-Hodgkin’slymphoma,anycellularclassification;relapsed/refractory(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�� Oncology;diseasestatus;non-Hodgkin’slymphoma,anycellularclassification;diagnosticevaluation,stagenotdetermined,evaluationofpossiblerelapseornon-responsetotherapy,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A G�1�� Oncology;diseasestatus;chronicmyelogenousleukemia,limitedtoPhiladelphiachromosomepositiveand/orBCR-ABLpositive;extentofdiseaseunknown,staginginprogress,notlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
A H00�� Alcoholand/ordrugscreening 1/1/200�
A H00�0 Alcoholand/ordrugservices,briefintervention,per1�minutes
1/1/200�
A J012� Injection,abatacept,10mg 1/1/200�
A J0��� Injection,anadulafungin,1mg 1/1/200�
A J0�6� Injection,apomorphinehydrochloride,1mg 1/1/200�
A J0��� Injection,busulfan,1mg 1/1/200�
A J0��� Injection,decitabine,1mg 1/1/200�
A J1�2� Injection,enfuvirtide,1mg 1/1/200�
A J1��� Injection,galsulfase,1mg 1/1/200�
A J1�62 Injection,immuneglobulin,subcutaneous,100mg 1/1/200�
A J1��0 Injection,ibandronatesodium,1mg 1/1/200�
A J21�0 Injection,mecasermin,1mg 1/1/200�
A J22�� Injection,micafunginsodium,1mg 1/1/200�
A J2�1� Injection,naltrexone,depotform,1mg 1/1/200�
A J�2�� Injection,tigecycline,1mg 1/1/200�
A J���� Injection,hyaluronidase,recombinant,1uspunit 1/1/200�
HCPCsCoDes
43034txtAH.indd 78 2/19/07 2:43:25 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A J�1�� Injection,VonWillebrandfactorcomplex,human,ristocetincofactor,perIU
1/1/200�
A J��11 Fluocinoloneacetonide,intravitrealimplant 1/1/200�
A J��1� Hyaluronan(sodiumhyaluronate)orderivative,intra-articularinjection,perinjection
1/1/200�
A J���� Dermal(substitute)tissueofnon-humanorigin,withorwithoutotherbioengineeredorprocessedelements,withoutmetabolicallyactiveelements,persquarecentimeter
1/1/200�
A J���6 Dermal(substitute)tissueofhumanorigin,injectable,withorwithoutotherbioengineeredorprocessedelements,butwithoutmetabolicallyactiveelements,1cc
1/1/200�
A J�60� Levalbuterol,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,0.�mg
1/1/200�
A J�60� Albuterol,inhalationsolution,compoundedproduct,administeredthroughDME,unitdose,1mgconcentratedform,1mg
1/1/200�
A J�610 Albuterol,inhalationsolution,compoundedproduct,administeredthroughDME,unitdose,1mgconcentratedform,1mg
1/1/200�
A J�61� Levalbuterol,inhalationsolution,compoundedproduct,administeredthroughDME,unitdose,0.�mg
1/1/200�
A J�6�� Budesonide,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,per0.2�milligram
1/1/200�
A J�6�� Ipratropiumbromide,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
A J�6�� SoetharineHCL,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
A J�6�0 IsoetharineHCL,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
A J�6�� IsoproterenolHCL,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
A J�660 IsoproterenolHCL,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
A J�66� Metaproterenolsulfate,inhalationsolution,compoundedproduct,concentratedform,per10milligrams
1/1/200�
A J�6�0 Metaproterenolsulfate,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,per10milligrams
1/1/200�
A J�6�� Tobramycin,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,per�00milligrams
1/1/200�
A J�6�0 Nabilone,oral,1mg 1/1/200�
A J�261 Injection,nelarabine,�0mg 1/1/200�
A L1001 Cervicalthoraciclumbarsacralorthosis,immobilizer,infantsize,each
1/1/200�
HCPCsCoDes
43034txtAH.indd 79 2/19/07 2:43:26 PM

�0Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A L��06 Wristhandfingerorthosis,includesoneormorenontorsionjoint(s),elasticbands,turnbuckles,mayincludesoftinterfacematerial,straps,customfabricated,includesfittingandadjustment
1/1/200�
A L��0� Wristhandfingerorthosis,rigidwithoutjoints,mayincludesoftinterfacematerial;straps,customfabricated,includesfittingandadjustment
1/1/200�
A L��1� Wristhandorthosis,includesoneormorenontorsionjoint(s),elasticbands,turnbuckles,mayincludesoftinterface,straps,prefabricated,includesfittingandadjustment
1/1/200�
A L���� Additiontolowerextremityprosthesis,heavydutyfeature,footonly,(forpatientweightgreaterthan�00lbs)
1/1/200�
A L���� Additiontolowerextremityprosthesis,heavydutyfeature,kneeonly,(forpatientweightgreaterthan�00lbs)
1/1/200�
A L6611 Additiontoupperextremityprosthesis,externalpowered,additionalswitch,anytype
1/1/200�
A L662� Upperextremityaddition,flexion/extensionandrotationwristunit
1/1/200�
A L66�� Upperextremityaddition,heavydutyfeature,anyelbow 1/1/200�
A L6�0� Terminaldevice,passivehand/mitt,anymaterial,anysize 1/1/200�
A L6�0� Terminaldevice,sport/recreational/workattachment,anymaterial,anysize
1/1/200�
A L6�06 Terminaldevice,hook,mechanical,voluntaryopening,anymaterial,anysize,linedorunlined
1/1/200�
A L6�0� Terminaldevice,hook,mechanical,voluntaryclosing,anymaterial,anysize,linedorunlined
1/1/200�
A L6�0� Terminaldevice,hand,mechanical,voluntaryopening,anymaterial,anysize
1/1/200�
A L6�0� Terminaldevice,hand,mechanical,voluntaryclosing,anymaterial,anysize
1/1/200�
A L�00� Electrichand,switchormyoelectriccontrolled,adult 1/1/200�
A L�00� Electrichand,switchormyoelectric,controlled,pediatric 1/1/200�
A L�00� Electrichook,switchormyoelectriccontrolled,adult 1/1/200�
A L�6�0 Auditoryosseointegrateddevice,includesallinternalandexternalcomponents
1/1/200�
A L�6�1 Auditoryosseointegrateddevice,externalsoundprocessor,replacement
1/1/200�
A L�6�� Externalrechargingsystemforbattery(external)forusewithimplantableneurostimulator
1/1/200�
A Q�0�1 Injection,epoetinalfa,100units(forESRDondialysis) 1/1/200�
A Q�0�2 Drugorbiological,nototherwiseclassified,partBdrugcompetitiveacquisitionprogram(cap)
1/1/200�
A Q�0�� Hyaluronanorderivative,HyalganorSupartz,forintra-articularinjection,perdose
1/1/200�
A Q�0�� Hyaluronanorderivative,Synvisc,forintra-articularinjection,perdose
1/1/200�
A Q�0�� Hyaluronanorderivative,Euflexxa,forintra-articularinjection,perdose
1/1/200�
HCPCsCoDes
43034txtAH.indd 80 2/19/07 2:43:26 PM
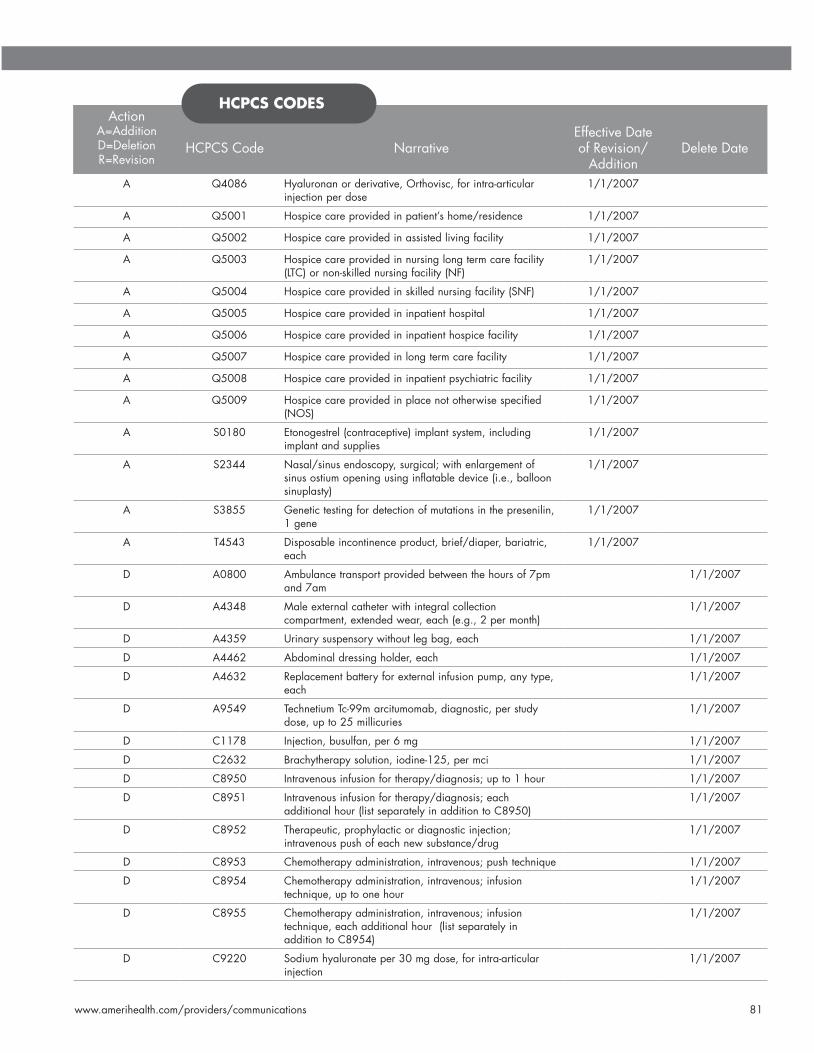
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �1
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
A Q�0�6 Hyaluronanorderivative,Orthovisc,forintra-articularinjectionperdose
1/1/200�
A Q�001 Hospicecareprovidedinpatient’shome/residence 1/1/200�
A Q�002 Hospicecareprovidedinassistedlivingfacility 1/1/200�
A Q�00� Hospicecareprovidedinnursinglongtermcarefacility(LTC)ornon-skillednursingfacility(NF)
1/1/200�
A Q�00� Hospicecareprovidedinskillednursingfacility(SNF) 1/1/200�
A Q�00� Hospicecareprovidedininpatienthospital 1/1/200�
A Q�006 Hospicecareprovidedininpatienthospicefacility 1/1/200�
A Q�00� Hospicecareprovidedinlongtermcarefacility 1/1/200�
A Q�00� Hospicecareprovidedininpatientpsychiatricfacility 1/1/200�
A Q�00� Hospicecareprovidedinplacenototherwisespecified(NOS)
1/1/200�
A S01�0 Etonogestrel(contraceptive)implantsystem,includingimplantandsupplies
1/1/200�
A S2��� Nasal/sinusendoscopy,surgical;withenlargementofsinusostiumopeningusinginflatabledevice(i.e.,balloonsinuplasty)
1/1/200�
A S���� Genetictestingfordetectionofmutationsinthepresenilin,1gene
1/1/200�
A T���� Disposableincontinenceproduct,brief/diaper,bariatric,each
1/1/200�
D A0�00 Ambulancetransportprovidedbetweenthehoursof�pmand�am
1/1/200�
D A���� Maleexternalcatheterwithintegralcollectioncompartment,extendedwear,each(e.g.,2permonth)
1/1/200�
D A���� Urinarysuspensorywithoutlegbag,each 1/1/200�
D A��62 Abdominaldressingholder,each 1/1/200�
D A�6�2 Replacementbatteryforexternalinfusionpump,anytype,each
1/1/200�
D A���� TechnetiumTc-��marcitumomab,diagnostic,perstudydose,upto2�millicuries
1/1/200�
D C11�� Injection,busulfan,per6mg 1/1/200�
D C26�2 Brachytherapysolution,iodine-12�,permci 1/1/200�
D C���0 Intravenousinfusionfortherapy/diagnosis;upto1hour 1/1/200�
D C���1 Intravenousinfusionfortherapy/diagnosis;eachadditionalhour(listseparatelyinadditiontoC���0)
1/1/200�
D C���2 Therapeutic,prophylacticordiagnosticinjection;intravenouspushofeachnewsubstance/drug
1/1/200�
D C���� Chemotherapyadministration,intravenous;pushtechnique 1/1/200�
D C���� Chemotherapyadministration,intravenous;infusiontechnique,uptoonehour
1/1/200�
D C���� Chemotherapyadministration,intravenous;infusiontechnique,eachadditionalhour(listseparatelyinadditiontoC����)
1/1/200�
D C�220 Sodiumhyaluronateper�0mgdose,forintra-articularinjection
1/1/200�
HCPCsCoDes
43034txtAH.indd 81 2/19/07 2:43:27 PM

�2Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D C�221 Acellulardermaltissuematrix,per16sq.cm. 1/1/200�
D C�222 Decellularizedsofttissuescaffold,per1cc 1/1/200�
D C�22� Injection,galsulfase,per�mg 1/1/200�
D C�22� Injection,fluocinoloneacetonideintravitrealimplant,per0.��mg
1/1/200�
D C�22� Injection,micafunginsodium,per1mg 1/1/200�
D C�22� Injection,tigecycline,per1mg 1/1/200�
D C�22� Injection,ibandronatesodium,per1mg 1/1/200�
D C�2�0 Injection,abatacept,per10mg 1/1/200�
D C�2�1 Injection,decitabine,per1mg 1/1/200�
D D1201 Topicalapplicationoffluoride(includingprophylaxis)-child 1/1/200�
D D120� Topicalapplicationoffluoride(includingprophylaxis)-adult 1/1/200�
D D6��1 Castpostaspartofbridgeretainer 1/1/200�
D E016� Commodechair,mobile,withfixedarms 1/1/200�
D E0166 Commodechair,mobile,withdetachablearms 1/1/200�
D E01�0 Pressurepad,alternatingwithpump 1/1/200�
D E0�01 Helmetwithfaceguardandsoftinterfacematerial,prefabricated
1/1/200�
D E0��� Wedgecushion,wheelchair 1/1/200�
D E0��� Casterwithafork 1/1/200�
D E0��� Casterwithoutfork 1/1/200�
D E0��� Pneumatictirewithwheel 1/1/200�
D E2�20 Powerwheelchairaccessory,handorchincontrolinterface,remotejoystickortouchpad,proportional,includingallrelatedelectronics,andfixedmountinghardware
1/1/200�
D G010� Colorectalcancerscreening;fecal-occultbloodtest,1-�simultaneousdeterminations
1/1/200�
D G02�� Multi-sourcephotonstereotacticradiosurgery,deliveryincludingcollimatorchangesandcustomplugging,completecourseoftreatment,alllesions
1/1/200�
D G�12� Oncology;diseasestatus;limitedtomultiplemyeloma,systemicdisease;smoldering,stageI(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
D J2�12 Injection,sodiumchloride,0.�%,per2ml 1/1/200�
D J�1�� Injection,VonWillebrandfactorcomplex,human,IU 1/1/200�
D J��1� Sodiumhyaluronate,per20to2�mgdoseforintra-articularinjection
1/1/200�
D J��20 HylanG-F20,16mg,forintra-articularinjection 1/1/200�
D J���0 Dermal(substitute)tissueofhumanorigin,injectable,withorwithoutotherbioengineeredorprocessedelements,butwithoutmetabolizedactiveelements,per10mg
1/1/200�
D K00�0 Rearwheeltireforpowerwheelchair,anysize,each 1/1/200�
D K00�1 Rearwheeltiretubeotherthanzeropressureforpowerwheelchair,anysize,each
1/1/200�
D K00�2 Rearwheelassemblyforpowerwheelchair,complete,each
1/1/200�
HCPCsCoDes
43034txtAH.indd 82 2/19/07 2:43:27 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D K00�� Rearwheel,zeropressuretiretube(flatfreeinsert)forpowerwheelchair,anysize,each
1/1/200�
D K00�� Wheeltireforpowerbase,anysize,each 1/1/200�
D K00�� Wheeltiretubeotherthanzeropressureforeachbase,anysize,each
1/1/200�
D K00�6 Wheelassemblyforpowerbase,complete,each 1/1/200�
D K00�� Wheelzeropressuretiretube(flatfreeinsert)forpowerbase,anysize,each
1/1/200�
D K00�� Frontcasterforpowerwheelchair 1/1/200�
D L0100 Cranialorthosis(helmet),withorwithoutsoftinterface,moldedtopatientmodel
1/1/200�
D L0110 Cranialorthosis(helmet),withorwithoutsoft-interface,non-molded
1/1/200�
D L��02 Wristhandfingerorthosis,externalpowered,compressedgas,custom-fabricated
1/1/200�
D L��1� Wristhandorthosis,wristextensioncock-up,prefabricated,includesfitting/adjustment
1/1/200�
D L6�00 Terminaldevice,hook,Dorrance,orequal,model#� 1/1/200�
D L6�0� Terminaldevice,hook,Dorrance,orequal,model#� 1/1/200�
D L6�10 Terminaldevice,hook,Dorrance,orequal,model#�X 1/1/200�
D L6�1� Terminaldevice,hook,Dorrance,orequal,model#�XA 1/1/200�
D L6�20 Terminaldevice,hook,Dorrance,orequal,model#6 1/1/200�
D L6�2� Terminaldevice,hook,Dorrance,orequal,model#� 1/1/200�
D L6��0 Terminaldevice,hook,Dorrance,orequal,model#�LO 1/1/200�
D L6��� Terminaldevice,hook,Dorrance,orequal,model#� 1/1/200�
D L6��0 Terminaldevice,hook,Dorrance,orequal,model#�X 1/1/200�
D L6��� Terminaldevice,hook,Dorrance,orequal,model#��X 1/1/200�
D L6��0 Terminaldevice,hook,Dorrance,orequal,model#10P 1/1/200�
D L6��� Terminaldevice,hook,Dorrance,orequal,model#10X 1/1/200�
D L6�6� Terminaldevice,hook,Dorrance,orequal,model#12P 1/1/200�
D L6��0 Terminaldevice,hook,Dorrance,orequal,model#��X 1/1/200�
D L6��� Terminaldevice,hook,Dorrance,orequal,model#��� 1/1/200�
D L6��0 Terminaldevice,hook,Dorrance,orequal,model#ss��� 1/1/200�
D L6��0 Terminaldevice,hook,Accuhook,orequal 1/1/200�
D L6��� Terminaldevice,hook,2load,orequal 1/1/200�
D L6�00 Terminaldevice,hook,APRLVC,orequal 1/1/200�
D L6�06 Terminaldevice,hook,TRSGrip,GripIII,VC,orequal 1/1/200�
D L6�0� Terminaldevice,hook,GripI,GripII,VC,orequal 1/1/200�
D L6�0� Terminaldevice,hook,TRSAdept,infantorchild,VC,orequal
1/1/200�
D L6�0� Terminaldevice,hook,TRSSuperSport,passive 1/1/200�
D L6�2� Terminaldevice,hand,Dorrance,VO 1/1/200�
D L6��0 Terminaldevice,hand,APRL,VC 1/1/200�
D L6��� Terminaldevice,hand,Sierra,VO 1/1/200�
D L6��0 Terminaldevice,hand,BeckerImperial 1/1/200�
HCPCsCoDes
43034txtAH.indd 83 2/19/07 2:43:28 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
D L6��� Terminaldevice,hand,BeckerLockGrip 1/1/200�
D L6��0 Terminaldevice,hand,BeckerPlylite 1/1/200�
D L6��� Terminaldevice,hand,Robin-Aids,VO 1/1/200�
D L6�60 Terminaldevice,hand,Robin-Aids,VOsoft 1/1/200�
D L6�6� Terminaldevice,hand,passivehand 1/1/200�
D L6�6� Terminaldevice,hand,Detroitinfanthand(mechanical) 1/1/200�
D L6�6� Terminaldevice,hand,passiveinfanthand,(Steeper,Hosmerorequal)
1/1/200�
D L6��0 Terminaldevice,hand,childmitt 1/1/200�
D L6��2 Terminaldevice,hand,NYUchildhand 1/1/200�
D L6��� Terminaldevice,hand,mechanicalinfanthand,steeperorequal
1/1/200�
D L6��� Terminaldevice,hand,Bock,VC 1/1/200�
D L6��0 Terminaldevice,hand,Bock,VO 1/1/200�
D L�010 Electronichand,OttoBock,Steeperorequal,switchcontrolled
1/1/200�
D L�01� Electronichand,SystemTeknik,VarietyVillageorequal,switchcontrolled
1/1/200�
D L�020 Electronicgreifer,OttoBockorequal,switchcontrolled 1/1/200�
D L�02� Electronichand,OttoBockorequal,myoelectronicallycontrolled
1/1/200�
D L�0�0 Electronichand,SystemTeknik,VarietyVillageorequal,myoelectronicallycontrolled
1/1/200�
D L�0�� ElectronicGreifer,OttoBockorequal,myoelectronicallycontrolled
1/1/200�
D S2262 Abortionformaternalindication,2�weeksorgreater 1/1/200�
D S�0�6 Intravaginalculture(IVC),caserate 1/1/200�
R S0�16 DiseaseManagementProgram,follow-up/reassessment 10/1/2006
R A�216 Sterilewater,salineand/ordextrose,diluent/flush,10ml 1/1/200�
R A��06 Disposabledrugdeliverysystem,flowrateoflessthan�0mlperhour
1/1/200�
R A��26 Maleexternalcatheterwithintegralcollectionchamber,anytype,each
1/1/200�
R A���� Ostomydeodorant,withorwithoutlubricant,foruseinostomypouch,perfluidounce
1/1/200�
R A���� Conductivegelorpaste,forusewithelectricaldevice(e.g.,TENS,NMES),peroz
1/1/200�
R A�10� Urinarysuspensory;withorwithoutlegbag,withorwithouttube,each
1/1/200�
R D0120 Periodicoralevaluation-establishedpatient 1/1/200�
R D0��0 Accessionofexfoliativecytologicsmears,microscopicexamination,thepreparationandtransmissionofwrittenreport
1/1/200�
R D2��2 Postandcoreinadditiontocrown,indirectlyfabricated 1/1/200�
R D2��� Eachadditionalindirectlyfabricatedpost-sametooth 1/1/200�
HCPCsCoDes
43034txtAH.indd 84 2/19/07 2:43:29 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R D6��0 Postandcoreinadditiontofixedpartialdentureretainer,indirectlyfabricated
1/1/200�
R D6��6 Eachadditionalindirectlyfabricatedpost-sametooth 1/1/200�
R D��10 Alveoloplastyinconjunctionwithextractions-fourormoreteethortoothspaces,perquadrant
1/1/200�
R D��20 Alveoloplastynotinconjunctionwithextractions-fourormoreteethortoothspaces,perquadrant
1/1/200�
R D���� Osteotomy-segmentedorsubapical 1/1/200�
R D���0 Osseous,osteoperiosteal,orcartilagegraftofthemandibleormaxilla-autogenousornonautogenous,byreport
1/1/200�
R D��10 Consultation-diagnosticserviceprovidedbydentistorphysicianotherthanrequestingdentistorphysician
1/1/200�
R D�610 Therapeuticparenteraldrug,singleadministration 1/1/200�
R E016� Commodechair,mobileorstationary,withfixedarms 1/1/200�
R E016� Commodechair,mobileorstationary,withdetachablearms
1/1/200�
R E016� Pailorpanforusewithcommodechair,replacementonly 1/1/200�
R E01�1 Poweredpressurereducingmattressoverlay/pad,alternating,withpump,includesheavyduty
1/1/200�
R E01�2 Pumpforalternatingpressurepad,forreplacementonly 1/1/200�
R E01�0 Positioningcushion/pillow/wedge,anyshapeorsize,includesallcomponentsandaccessories
1/1/200�
R E0�20 Transcutaneouselectricalnervestimulation(TENS)device,twolead,localizedstimulation
1/1/200�
R E0��0 Transcutaneouselectricalnervestimulation(TENS)device,fourormoreleads,formultiplenervestimulation
1/1/200�
R E0�6� Manualwheelchairaccessory,handrimwithprojections,anytype,each
1/1/200�
R E220� Armtrough,withorwithouthandsupport,each 1/1/200�
R G010� Prostatecancerscreening;prostatespecificantigentest(PSA)
1/1/200�
R G0��2 Servicesforintravenousinfusionofimmunoglobulinpriortoadministration(thisserviceistobebilledinconjunctionwithadministrationofimmunoglobulin)
1/1/200�
R G�06� Oncology;diseasestatus;limitedtonon-smallcelllungcancer;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�0�0 Oncology;diseasestatus;smallcelllungcancer,limitedtosmallcellandcombinedsmallcell/non-small;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�0�� Oncology;diseasestatus;prostatecancer,limitedtoadenocarcinoma;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
HCPCsCoDes
43034txtAH.indd 85 2/19/07 2:43:29 PM

�6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R G�0�� Oncology;diseasestatus;coloncancer,limitedtoinvasivecancer;adenocarcinomaaspredominantcelltype;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�0�� Oncology;diseasestatus;rectalcancer,limitedtoinvasivecancer;adenocarcinomaaspredominantcelltype;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�0�� Oncology;diseasestatus;esophagealcancer,limitedtoadenocarcinomaorsquamouscellcarcinomaaspredominantcelltype;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�10� Oncology;diseasestatus;gastriccancer,limitedtoadenocarcinomaaspredominantcelltype;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�10� Oncology;diseasestatus;pancreaticcancer,limitedtoadenocarcinoma;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�112 Oncology;diseasestatus;headandneckcancer,limitedtocancersoforalcavity,pharynxandlarynxwithsquamouscellaspredominantcelltype;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�11� Oncology;diseasestatus;ovariancancer,limitedtoepithelialcancer;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R G�1�0 Oncology;diseasestatus;limitedtomultiplemyeloma,systemicdisease;extentofdiseaseunknown,staginginprogress,ornotlisted(foruseinaMedicare-approveddemonstrationproject)
1/1/200�
R J�611 Albuterol,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,concentratedform,1mg
1/1/200�
R J�612 Levalbuterol,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,concentratedform,0.�mg
1/1/200�
R J�61� Albuterol,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdose,1mg
1/1/200�
R J�61� Levalbuterol,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdose,0.�mg
1/1/200�
R J�620 Albuterol,upto2.�mgandipratropiumbromide,upto0.�mg,FDA-approvedfinalproduct,non-compounded,administeredthroughDME
1/1/200�
R J�622 Beclomethasone,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�62� Betamethasone,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
HCPCsCoDes
43034txtAH.indd 86 2/19/07 2:43:30 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R J�626 Budesonide,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdoseform,upto0.�mg
1/1/200�
R J�62� Budesonide,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,upto0.�mg
1/1/200�
R J�62� Bitolterolmesylate,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�62� Bitolterolmesylate,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�� Budesonide,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,concentratedform,per0.2�milligram
1/1/200�
R J�6�� Atropine,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�6 Atropine,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�� Dexamethasone,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�� Dexamethasone,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�0 Formoterol,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,12micrograms
1/1/200�
R J�6�1 Flunisolide,inhalationsolution,compoundedproduct,administeredthroughDME,unitdose,permilligram
1/1/200�
R J�6�2 Glycopyrrolate,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�� Glycopyrrolate,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�� Ipratropiumbromide,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�� IsoetharineHCL,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�� IsoetharineHCL,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�� IsoproterenolHCL,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�� IsoproterenolHCL,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�66� Metaproterenolsulfate,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,concentratedform,per10milligrams
1/1/200�
HCPCsCoDes
43034txtAH.indd 87 2/19/07 2:43:30 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R J�66� Metaproterenolsulfate,inhalationsolution,FDA-approvedfinalproduct,non-compounded,administeredthroughDME,unitdoseform,per10milligrams
1/1/200�
R J�6�0 Terbutalinesulfate,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�1 Terbutalinesulfate,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R J�6�2 Tobramycin,inhalationsolution,FDA-approvedfinalproduct,non-compounded,unitdoseform,administeredthroughDME,per�00milligrams
1/1/200�
R J�6�� Triamcinolone,inhalationsolution,compoundedproduct,administeredthroughDME,concentratedform,permilligram
1/1/200�
R J�6�� Triamcinolone,inhalationsolution,compoundedproduct,administeredthroughDME,unitdoseform,permilligram
1/1/200�
R L06�1 Lumbar-sacralorthosis,sagittalcontrol,withrigidanteriorandposteriorpanels,posteriorextendsfromsacrococcygealjunctiontoT-�vertebra,producesintracavitarypressuretoreduceloadontheintervertebraldiscs,includesstraps,pendulousabdomendesign,closures,mayincludepadding,shoulderstraps,pendulousabdomendesign,prefabricated,includesfittingandadjustment
1/1/200�
R L���� Additiontoendoskeletalknee-shinsystem,hydraulicfluidstanceextension,dampeningfeature,withorwithoutadjustability
1/1/200�
R L���� Additiontolowerextremityprosthesis,heavydutyfeature,otherthanfootorknee,(forpatientweightgreaterthan�00lbs)
1/1/200�
R L6�0� Additiontoterminaldevice,modifierwristunit 1/1/200�
R L6�10 Additiontoterminaldevice,Pinchertool,OttoBockorequalprecisionpinchdevice
1/1/200�
R L6��1 Automaticgraspfeature,additiontoupperlimbelectricprostheticterminaldevice
1/1/200�
R L6��� Replacementsocket,aboveelbow/elbowdisarticulation,moldedtopatientmodel,forusewithorwithoutexternalpower
1/1/200�
R L�0�0 Prehensileactuator,Hosmerorequalswitchcontrolled 1/1/200�
R L�0�� Electrichook,child,Michiganorequalswitchormyoelectriccontrolled,pediatric
1/1/200�
R L�61� Cochleardevice/system,includesallinternalandexternalcomponents
1/1/200�
R L�6�� Externalrechargingsystemforimplantedbattery(internal)forusewithimplantableneurostimulator,replacementonly
1/1/200�
R P�011 Blood,splitunit 1/1/200�
R S10�0 Cranialremoldingorthosis,pediatric,rigid,withsoftinterfacematerial,customfabricated,includesfittingandadjustment(s)
1/1/200�
R S2260 Inducedabortion,1�to2�weeks,anysurgicalmethod 1/1/200�
HCPCsCoDes
43034txtAH.indd 88 2/19/07 2:43:30 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR=Revision
HCPCSCode NarrativeEffectiveDateofRevision/
AdditionDeleteDate
R S226� Inducedabortionforfetalindication,2�to2�weeks 1/1/200�
R S2266 Inducedabortionforfetalindication,2�to�1weeks 1/1/200�
R S226� Inducedabortionforfetalindication,�2weeksorgreater 1/1/200�
R T�001 Positioningseatforpersonswithspecialorthopedicneeds,foruseinvehicles
1/1/200�
HCPCsCoDes
43034txtAH.indd 89 2/19/07 2:43:31 PM

�0Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A V1�.�1 Familyhistory,colonicpolyps 10/1/2006
A V1�.�� Familyhistory,otherdigestivedisorders 10/1/2006
A V26.�� Testingofmaleforgeneticdiseasecarrierstatus 10/1/2006
A V26.�� Encounterfortestingofmalepartnerofhabitualaborter 10/1/2006
A V26.�� Othergenetictestingofmale 10/1/2006
A V��.�6 Bariatricsurgerystatus 10/1/2006
A V��.�0 Encounterforchangeorremovalofnonsurgicalwounddressing 10/1/2006
A V��.�1 Encounterforchangeorremovalofsurgicalwounddressing 10/1/2006
A V��.�2 Encounterforremovalofsutures 10/1/2006
A V�2.11 Encounterforhearingexaminationfollowingfailedhearingscreening 10/1/2006
A V�2.1� Otherexaminationofearsandhearing 10/1/2006
A V�2.�1 Screeningforgeneticdiseasecarrierstatus 10/1/2006
A V�2.�� Othergeneticscreening 10/1/2006
A V��.�1 Bodymassindex,pediatric,lessthan�thpercentileforage 10/1/2006
A V��.�2 Bodymassindex,pediatric,�thpercentiletolessthan��thpercentileforage 10/1/2006
A V��.�� Bodymassindex,pediatric,��thpercentiletolessthan��thpercentileforage 10/1/2006
A V��.�� Bodymassindex,pediatric,greaterthanorequalto��thpercentileforage 10/1/2006
A V�6.0 Estrogenreceptorpositivestatus[ER+] 10/1/2006
A V�6.1 Estrogenreceptornegativestatus[ER-] 10/1/2006
A 0�2.2 Postvaricellamyelitis 10/1/2006
A 0��.1� Herpeszostermyelitis 10/1/2006
A 0��.�� Herpessimplexmyelitis 10/1/2006
A 2��.�1 Essentialthrombocythemia 10/1/2006
A 2��.�2 Lowgrademyelodysplasticsyndromelesions 10/1/2006
A 2��.�� Highgrademyelodysplasticsyndromelesions 10/1/2006
A 2��.�� Myelodysplasticsyndromewith�qdeletion 10/1/2006
A 2��.�� Myelodysplasticsyndrome,unspecified 10/1/2006
A 2��.�6 Myelofibrosiswithmyeloidmetaplasia 10/1/2006
A 2��.�� Otherlymphaticandhematopoietictissues 10/1/2006
A 2��.�0 Amyloidosis,unspecified 10/1/2006
A 2��.�1 FamilialMediterraneanfever 10/1/2006
A 2��.�� Otheramyloidosis 10/1/2006
A 2��.01 Constitutionalredbloodcellaplasia 10/1/2006
A 2��.0� Otherconstitutionalaplasticanemia 10/1/2006
A 2��.1 Pancytopenia 10/1/2006
A 2��.2 Myelophthisis 10/1/2006
A 2��.00 Neutropenia,unspecified 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 90 2/19/07 2:43:31 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications �1
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A 2��.01 Congenitalneutropenia 10/1/2006
A 2��.02 Cyclicneutropenia 10/1/2006
A 2��.0� Druginducedneutropenia 10/1/2006
A 2��.0� Neutropeniaduetoinfection 10/1/2006
A 2��.0� Otherneutropenia 10/1/2006
A 2��.� Hemophagocyticsyndromes 10/1/2006
A 2��.�0 Leukocytopenia,unspecified 10/1/2006
A 2��.�1 Lymphocytopenia 10/1/2006
A 2��.�� Otherdecreasedwhitebloodcellcount 10/1/2006
A 2��.60 Leukocytosis,unspecified 10/1/2006
A 2��.61 Lymphocytosis(symptomatic) 10/1/2006
A 2��.62 Leukemoidreaction 10/1/2006
A 2��.6� Monocytosis(symptomatic) 10/1/2006
A 2��.6� Plasmacytosis 10/1/2006
A 2��.6� Basophilia 10/1/2006
A 2��.6� Otherelevatedwhitebloodcellcount 10/1/2006
A 2��.�� Neutropenicsplenomegaly 10/1/2006
A 2��.�� Myelofibrosis 10/1/2006
A �2�.01 Encephalitisandencephalomyelitisinviraldiseasesclassifiedelsewhere 10/1/2006
A �2�.02 Myelitisinviraldiseasesclassifiedelsewhere 10/1/2006
A �2�.�1 Otherencephalitisandencephalomyelitisduetoinfectionclassifiedelsewhere 10/1/2006
A �2�.�2 Othermyelitisduetoinfectionclassifiedelsewhere 10/1/2006
A �2�.�1 Encephalitisandencephalomyelitisfollowingimmunizationprocedures 10/1/2006
A �2�.�2 Myelitisfollowingimmunizationprocedures 10/1/2006
A �2�.61 Infectiousacutedisseminatedencephalomyelitis(ADEM) 10/1/2006
A �2�.62 Otherpostinfectiousencephalitisandencephalomyelitis 10/1/2006
A �2�.6� Postinfectiousmyelitis 10/1/2006
A �2�.�1 Toxicencephalitisandencephalomyelitis 10/1/2006
A �2�.�2 Toxicmyelitis 10/1/2006
A �2�.�1 Othercausesofencephalitisandencephalomyelitis 10/1/2006
A �2�.�2 Othercausesofmyelitis 10/1/2006
A ��1.�� Mildcognitiveimpairment,sostated 10/1/2006
A ���.�1 Athetoidcerebralpalsy 10/1/2006
A ���.�2 Acutedystoniaduetodrugs 10/1/2006
A ���.�� Otheracquiredtorsiondystonia 10/1/2006
A ���.�� Subacutedyskinesiaduetodrugs 10/1/2006
A ���.�� Restlesslegssyndrome(RLS) 10/1/2006
A ���.0 Centralpainsyndrome 10/1/2006
A ���.11 Acutepainduetotrauma 10/1/2006
A ���.12 Acutepost-thoracotomypain 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 91 2/19/07 2:43:32 PM

�2Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A ���.1� Otheracutepostoperativepain 10/1/2006
A ���.1� Otheracutepain 10/1/2006
A ���.21 Chronicpainduetotrauma 10/1/2006
A ���.22 Chronicpost-thoracotomypain 10/1/2006
A ���.2� Otherchronicpostoperativepain 10/1/2006
A ���.2� Otherchronicpain 10/1/2006
A ���.� Neoplasmrelatedpain(acute)(chronic) 10/1/2006
A ���.� Chronicpainsyndrome 10/1/2006
A ��1.20 Acute(transverse)myelitisnos 10/1/2006
A ��1.21 Acute(transverse)myelitisinconditionsclassifiedelsewhere 10/1/2006
A ��1.22 Idiopathictransversemyelitis 10/1/2006
A ���.�� Opticnervehypoplasia 10/1/2006
A ���.60 Inflammation(infection)ofpostproceduralbleb,unspecified 10/1/2006
A ���.61 Inflammation(infection)ofpostproceduralbleb,stage1 10/1/2006
A ���.62 Inflammation(infection)ofpostproceduralbleb,stage2 10/1/2006
A ���.6� Inflammation(infection)ofpostproceduralbleb,stage� 10/1/2006
A ���.1� Sensorineuralhearingloss,unilateral 10/1/2006
A ���.16 Sensorineuralhearingloss,asymmetrical 10/1/2006
A �2�.�� Takotsubosyndrome 10/1/2006
A ���.11 Nasalmucositis(ulcerative) 10/1/2006
A ���.1� Otherdiseaseofnasalcavityandsinuses 10/1/2006
A �1�.� Transfusionrelatedacutelunginjury(TRALI) 10/1/2006
A �1�.11 Acutebronchospasm 10/1/2006
A �1�.1� Otherdiseasesoftracheaandbronchus 10/1/2006
A �21.�1 Crackedtooth 10/1/2006
A �21.�� Otherspecificdiseasesofhardtissuesofteeth 10/1/2006
A �2�.00 Acutegingivitis,plaqueinduced 10/1/2006
A �2�.01 Acutegingivitis,non-plaqueinduced 10/1/2006
A �2�.10 Chronicgingivitis,plaqueinduced 10/1/2006
A �2�.11 Chronicgingivitis,non-plaqueinduced 10/1/2006
A �2�.�0 Aggressiveperiodontitis,unspecified 10/1/2006
A �2�.�1 Aggressiveperiodontitis,localized 10/1/2006
A �2�.�2 Aggressiveperiodontitis,generalized 10/1/2006
A �2�.�� Acuteperiodontitis 10/1/2006
A �2�.�0 Chronicperiodontitis,unspecified 10/1/2006
A �2�.�1 Chronicperiodontitis,localized 10/1/2006
A �2�.�2 Chronicperiodontitis,generalized 10/1/2006
A �2�.60 Unspecifiedunsatisfactoryrestorationoftooth 10/1/2006
A �2�.61 Openrestorationmargins 10/1/2006
A �2�.62 Unrepairableoverhangingofdentalrestorativematerials 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 92 2/19/07 2:43:32 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A �2�.6� Fractureddentalrestorativematerialwithoutlossofmaterial 10/1/2006
A �2�.6� Fractureddentalrestorativematerialwithlossofmaterial 10/1/2006
A �2�.6� Contourofexistingrestorationoftoothbiologicallyincompatiblewithoralhealth 10/1/2006
A �2�.66 Allergytoexistingdentalrestorativematerial 10/1/2006
A �2�.6� Pooraestheticsofexistingrestoration 10/1/2006
A �2�.6� Otherunsatisfactoryrestorationofexistingtooth 10/1/2006
A �26.61 Perforationofrootcanalspace 10/1/2006
A �26.62 Endodonticoverfill 10/1/2006
A �26.6� Endodonticunderfill 10/1/2006
A �26.6� Otherperiradicularpathologyassociatedwithpreviousendodontictreatment 10/1/2006
A �2�.00 Stomatitisandmucositis,unspecified 10/1/2006
A �2�.01 Mucositis(ulcerative)duetoantineoplastictherapy 10/1/2006
A �2�.02 Mucositis(ulcerative)duetootherdrugs 10/1/2006
A �2�.0� Otherstomatitisandmucositis(ulcerative) 10/1/2006
A ��� Gastrointestinalmucositis(ulcerative) 10/1/2006
A 60�.20 Torsionoftestis,unspecified 10/1/2006
A 60�.21 Extravaginaltorsionofspermaticcord 10/1/2006
A 60�.22 Intravaginaltorsionofspermaticcord 10/1/2006
A 60�.2� Torsionofappendixtestis 10/1/2006
A 60�.2� Torsionofappendixepididymis 10/1/2006
A 616.�1 Mucositis(ulcerative)ofcervix,vagina,andvulva 10/1/2006
A 616.�� Otherinflammatorydiseaseofcervix,vaginaandvulva 10/1/2006
A 61�.�� Cervicalstumpprolapse 10/1/2006
A 62�.2� Otherfemalegenitalmutilationstatus 10/1/2006
A 62�.�1 Habitualaborterwithoutcurrentpregnancy 10/1/2006
A 62�.�� Otherspecifieddisordersoffemalegenitalorgans 10/1/2006
A 6��.00Tobaccousedisordercomplicatingpregnancy,childbirth,orthepuerperium,unspecifiedastoepisodeofcareornotapplicable
10/1/2006
A 6��.01Tobaccousedisordercomplicatingpregnancy,childbirth,orthepuerperium,delivered,withorwithoutmentionofantepartumcondition
10/1/2006
A 6��.02Tobaccousedisordercomplicatingpregnancy,childbirth,orthepuerperium,delivered,withmentionofpostpartumcomplication
10/1/2006
A 6��.0� Tobaccousedisordercomplicatingpregnancy,childbirth,orthepuerperium,antepartumconditionorcomplication 10/1/2006
A 6��.0� Tobaccousedisordercomplicatingpregnancy,childbirth,orthepuerperium,postpartumconditionorcomplication 10/1/2006
A 6��.10Obesitycomplicatingpregnancy,childbirth,orthepuerperium,unspecifiedastoepisodeofcareornotapplicable
10/1/2006
iCD-9CMCoDes
43034txtAH.indd 93 2/19/07 2:43:33 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A 6��.11Obesitycomplicatingpregnancy,childbirth,orthepuerperium,delivered,withorwithoutmentionofantepartumcondition
10/1/2006
A 6��.12Obesitycomplicatingpregnancy,childbirth,orthepuerperium,delivered,withmentionofpostpartumcomplication
10/1/2006
A 6��.1� Obesitycomplicatingpregnancy,childbirth,orthepuerperium,antepartumconditionorcomplication 10/1/2006
A 6��.1� Obesitycomplicatingpregnancy,childbirth,orthepuerperium,postpartumconditionorcomplication 10/1/2006
A 6��.20Bariatricsurgerystatuscomplicatingpregnancy,childbirth,orthepuerperium,unspecifiedastoepisodeofcareornotapplicable
10/1/2006
A 6��.21Bariatricsurgerystatuscomplicatingpregnancy,childbirth,orthepuerperium,delivered,withorwithoutmentionofantepartumcondition
10/1/2006
A 6��.22Bariatricsurgerystatuscomplicatingpregnancy,childbirth,orthepuerperium,delivered,withmentionofpostpartumcomplication
10/1/2006
A 6��.2� Bariatricsurgerystatuscomplicatingpregnancy,childbirth,orthepuerperium,antepartumconditionorcomplication 10/1/2006
A 6��.2� Bariatricsurgerystatuscomplicatingpregnancy,childbirth,orthepuerperium,postpartumconditionorcomplication 10/1/2006
A 6��.�0Coagulationdefectscomplicatingpregnancy,childbirth,orthepuerperium,unspecifiedastoepisodeofcareornotapplicable
10/1/2006
A 6��.�1Coagulationdefectscomplicatingpregnancy,childbirth,orthepuerperium,delivered,withorwithoutmentionofantepartumcondition
10/1/2006
A 6��.�2Coagulationdefectscomplicatingpregnancy,childbirth,orthepuerperium,delivered,withmentionofpostpartumcomplication
10/1/2006
A 6��.�� Coagulationdefectscomplicatingpregnancy,childbirth,orthepuerperium,antepartumconditionorcomplication 10/1/2006
A 6��.�� Coagulationdefectscomplicatingpregnancy,childbirth,orthepuerperium,postpartumconditionorcomplication 10/1/2006
A 6��.�0Epilepsycomplicatingpregnancy,childbirth,orthepuerperium,unspecifiedastoepisodeofcareornotapplicable
10/1/2006
A 6��.�1Epilepsycomplicatingpregnancy,childbirth,orthepuerperium,delivered,withorwithoutmentionofantepartumcondition
10/1/2006
A 6��.�2Epilepsycomplicatingpregnancy,childbirth,orthepuerperium,delivered,withmentionofpostpartumcomplication
10/1/2006
A 6��.�� Epilepsycomplicatingpregnancy,childbirth,orthepuerperium,antepartumconditionorcomplication 10/1/2006
A 6��.�� Epilepsycomplicatingpregnancy,childbirth,orthepuerperium,postpartumconditionorcomplication 10/1/2006
A 6��.�0 Spottingcomplicatingpregnancy,unspecifiedastoepisodeofcareornotapplicable 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 94 2/19/07 2:43:33 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A 6��.�1 Spottingcomplicatingpregnancy,delivered,withorwithoutmentionofantepartumcondition 10/1/2006
A 6��.�� Spottingcomplicatingpregnancy,antepartumconditionorcomplication 10/1/2006
A 6��.60 Uterinesizedatediscrepancy,unspecifiedastoepisodeofcareornotapplicable 10/1/2006
A 6��.61 Uterinesizedatediscrepancy,delivered,withorwithoutmentionofantepartumcondition 10/1/2006
A 6��.62 Uterinesizedatediscrepancy,delivered,withmentionofpostpartumcomplication 10/1/2006
A 6��.6� Uterinesizedatediscrepancy,antepartumconditionorcomplication 10/1/2006
A 6��.6� Uterinesizedatediscrepancy,postpartumconditionorcomplication 10/1/2006
A �2�.�1 Nontraumaticcompartmentsyndromeofupperextremity 10/1/2006
A �2�.�2 Nontraumaticcompartmentsyndromeoflowerextremity 10/1/2006
A �2�.�� Nontraumaticcompartmentsyndromeofabdomen 10/1/2006
A �2�.�� Nontraumaticcompartmentsyndromeofothersites 10/1/2006
A ��1.� Majorosseousdefects 10/1/2006
A �6�.� Hypoxic-ischemicencephalopathy(HIE) 10/1/2006
A ��0.�� Respiratoryarrestofnewborn 10/1/2006
A ��0.�� Hypoxemiaofnewborn 10/1/2006
A ���.�1 Otheracidosisofnewborn 10/1/2006
A ���.�� Otherneonatalendocrineandmetabolicdisturbances 10/1/2006
A ���.�� Cardiacarrestofnewborn 10/1/2006
A ��0.�2 Complexfebrileconvulsions 10/1/2006
A ��0.�6 Generalizedpain 10/1/2006
A ��0.�� Alteredmentalstatus 10/1/2006
A ���.�1 Postnasaldrip 10/1/2006
A ���.�� Othersymptomsinvolvingheadandneck 10/1/2006
A ���.6� Urinaryhesitancy 10/1/2006
A ���.6� Strainingonurination 10/1/2006
A ���.�1 Imagetestinconclusiveduetoexcessbodyfat 10/1/2006
A ���.�� Othernonspecificabnormalfindingsonradiologicalandotherexaminationsofbodystructure 10/1/2006
A ���.06 Papanicolaousmearofcervixwithcytologicevidenceofmalignancy 10/1/2006
A ���.�1 Elevatedcarcinoembryonicantigen[CEA] 10/1/2006
A ���.�2 Elevatedcancerantigen12�[CA12�] 10/1/2006
A ���.�� Otherabnormaltumormarkers 10/1/2006
A ���.�0 Compartmentsyndrome,unspecified 10/1/2006
A ���.�1 Traumaticcompartmentsyndromeofupperextremity 10/1/2006
A ���.�2 Traumaticcompartmentsyndromeoflowerextremity 10/1/2006
A ���.�� Traumaticcompartmentsyndromeofabdomen 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 95 2/19/07 2:43:34 PM

�6Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
A ���.�� Traumaticcompartmentsyndromeofothersites 10/1/2006
A ���.20 Unspecifiedadverseeffectofunspecifieddrug,medicinalandbiologicalsubstance 10/1/2006
A ���.21 Arthusphenomenon 10/1/2006
A ���.22 Unspecifiedadverseeffectofanesthesia 10/1/2006
A ���.2� Unspecifiedadverseeffectofinsulin 10/1/2006
A ���.2� Otherdrugallergy 10/1/2006
A ���.2� Unspecifiedadverseeffectofotherdrug,medicinalandbiologicalsubstance 10/1/2006
D V1�.� Familyhistoryofdigestivedisorders 10/1/2006
D V��.� Attentiontodressingsandsutures 10/1/2006
D V�2.1 Examinationofearsandhearing 10/1/2006
D 2��.� Neoplasmofuncertainbehaviorofotherlymphaticandhematopoietictissues 10/1/2006
D 2��.� Amyloidosis 10/1/2006
D 2��.0 Constitutionalaplasticanemia 10/1/2006
D 2��.0 Aplasticanemiaandotherbonemarrowfailuresyndromes 10/1/2006
D �2�.0 Encephalitis,myelitis,andencephalomyelitisinviraldiseasesclassifiedelsewhere 10/1/2006
D �2�.� Otherencephalitisduetoinfectionclassifiedelsewhere 10/1/2006
D �2�.� Encephalitis,myelitis,andencephalomyelitisfollowingimmunizationprocedures 10/1/2006
D �2�.6 Postinfectiousencephalitis,myelitis,andencephalomyelitis 10/1/2006
D �2�.� Toxicencephalitis,myelitis,andencephalomyelitis 10/1/2006
D �2�.� Othercausesofencephalitis,myelitis,andencephalomyelitis 10/1/2006
D ���.� Acquiredtorsiondystonia 10/1/2006
D ���.1 Otherdiseasesofnasalcavityandsinuses 10/1/2006
D �1�.1 Otherdiseasesoftracheaandbronchus,notelsewhereclassified 10/1/2006
D �21.� Otherspecifieddiseasesofhardtissuesofteeth 10/1/2006
D �2�.0 Acutegingivitis 10/1/2006
D �2�.1 Chronicgingivitis 10/1/2006
D �2�.� Aggressiveandacuteperiodontitis 10/1/2006
D �2�.� Chronicperiodontitis 10/1/2006
D �2�.0 Stomatitisandmucositis(ulcerative) 10/1/2006
D 60�.2 Torsionoftestis 10/1/2006
D 616.� Otherspecifiedinflammatorydiseaseofcervix,vagina,andvulva 10/1/2006
D 62�.� Otherspecifieddisorderoffemalegenitalorgans 10/1/2006
D ���.� Otherneonatalendocrineandmetabolicdisturbances 10/1/2006
D ���.� Othersymptomsinvolvingheadandneck 10/1/2006
D ���.� Nonspecificabnormalfindingsonradiologicalandotherexaminationofothersiteofbody 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 96 2/19/07 2:43:35 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
D ���.2 Otherandunspecifiedadverseeffectofdrug,medicinalandbiologicalsubstance 10/1/2006
R 2��.10 Hyperaldosteronism,unspecified 10/1/2006
R 2��.2� Anemiaofotherchronicdisease 10/1/2006
R �2�.1 Encephalitis,myelitis,andencephalomyelitisinrickettsialdiseasesclassifiedelsewhere 10/1/2006
R �2�.2 Encephalitis,myelitis,andencephalomyelitisinprotozoaldiseasesclassifiedelsewhere 10/1/2006
R �2�.� Unspecifiedcauseofencephalitis,myelitis,andencephalomyelitis 10/1/2006
R ���.6 Genetictorsiondystonia 10/1/2006
R ���.�0Localization-related(focal)(partial)epilepsyandepilepticsyndromeswithcomplexpartialseizureswithoutmentionofintractableepilepsy
10/1/2006
R ���.�1Localization-related(focal)(partial)epilepsyandepilepticsyndromeswithcomplexpartialseizureswithintractableepilepsy
10/1/2006
R ���.�0Localization-related(focal)(partial)epilepsyandepilepticsyndromeswithsimplepartialseizureswithoutmentionofintractableepilepsy
10/1/2006
R ���.�1Localization-related(focal)(partial)epilepsyandepilepticsyndromeswithsimplepartialseizureswithintractableepilepsy
10/1/2006
R ���.�0 Otherformsofepilepsyandrecurrentseizureswithoutmentionofintractableepilepsy 10/1/2006
R ���.�1 Otherformsofepilepsyandrecurrentseizures,withintractableepilepsy 10/1/2006
R ���.11 Sensoryhearingloss,bilateral 10/1/2006
R ���.12 Neuralhearingloss,bilateral 10/1/2006
R ���.1� Centralhearingloss,bilateral 10/1/2006
R ���.1� Sensorineuralhearinglossofcombinedtypes,bilateral 10/1/2006
R �0�.00Hypertensivechronickidneydisease,malignant,withchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.10 Hypertensivechronickidneydisease,benign,withchronickidneydiseasestageVorendstagerenaldisease 10/1/2006
R �0�.�0Hypertensivechronickidneydisease,unspecified,withchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.�1 Hypertensivechronickidneydisease,unspecified,withchronickidneydiseasestageVorendstagerenaldisease 10/1/2006
R �0�.00Hypertensiveheartandchronickidneydisease,malignant,withoutheartfailureandwithchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.01Hypertensiveheartandchronickidneydisease,malignant,withheartfailureandwithchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.02Hypertensiveheartandchronickidneydisease,malignant,withoutheartfailureandwithchronickidneydiseasestageVorendstagerenaldisease
10/1/2006
iCD-9CMCoDes
43034txtAH.indd 97 2/19/07 2:43:35 PM

��Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
R �0�.0�Hypertensiveheartandchronickidneydisease,malignant,withheartfailureandwithchronickidneydiseasestageVorendstagerenaldisease
10/1/2006
R �0�.10Hypertensiveheartandchronickidneydisease,benign,withoutheartfailureandwithchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.11Hypertensiveheartandchronickidneydisease,benign,withheartfailureandwithchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.12Hypertensiveheartandchronickidneydisease,benign,withoutheartfailureandwithchronickidneydiseasestageVorendstagerenaldisease
10/1/2006
R �0�.1�Hypertensiveheartandchronickidneydisease,benign,withheartfailureandwithchronickidneydiseasestageVorendstagerenaldisease
10/1/2006
R �0�.�0Hypertensiveheartandchronickidneydisease,unspecified,withoutheartfailureandwithchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.�1Hypertensiveheartandchronickidneydisease,unspecified,withheartfailureandwithchronickidneydiseasestageIthroughstageIV,orunspecified
10/1/2006
R �0�.�2Hypertensiveheartandchronickidneydisease,unspecified,withoutheartfailureandwithchronickidneydiseasestageVorendstagerenaldisease
10/1/2006
R �0�.��Hypertensiveheartandchronickidneydisease,unspecified,withheartfailureandwithchronickidneydiseasestageVorendstagerenaldisease
10/1/2006
R �2�.21 Malocclusion,angle’sclassI 10/1/2006
R �2�.22 Malocclusion,angle’sclassII 10/1/2006
R �2�.2� Malocclusion,angle’sclassIII 10/1/2006
R �2�.�� Rotationoftooth/teeth 10/1/2006
R 600.00 Hypertrophy(benign)ofprostatewithouturinaryobstructionandotherlowerurinarytractsymptoms(LUTS) 10/1/2006
R 600.01 Hypertrophy(benign)ofprostatewithurinaryobstructionandotherlowerurinarytractsymptoms(LUTS) 10/1/2006
R 600.20 Benignlocalizedhyperplasiaofprostatewithouturinaryobstructionandotherlowerurinarytractsymptoms(LUTS) 10/1/2006
R 600.21 Benignlocalizedhyperplasiaofprostatewithurinaryobstructionandotherlowerurinarytractsymptoms(LUTS) 10/1/2006
R 600.�0 Hyperplasiaofprostate,unspecified,withouturinaryobstructionandotherlowerurinarysymptoms(LUTS) 10/1/2006
R 600.�1 Hyperplasiaofprostate,unspecified,withurinaryobstructionandotherlowerurinarysymptoms(LUTS) 10/1/2006
R �6�.� Fetaldistressfirstnotedduringlaboranddelivery,inliveborninfant 10/1/2006
R ��0.�1 Febrileconvulsions(simple),unspecified 10/1/2006
R ��0.�� Excessivecryingofchild,adolescent,oradult 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 98 2/19/07 2:43:36 PM

C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
www.amerihealth.com/providers/communications ��
ActionA=AdditionD=DeletionR-Revision
ICD-�CMCode Narrative
EffectiveDateof
Revision/Addition
DeleteDate
R ���.6� Tooth(broken)(fractured)(duetotrauma),withoutmentionofcomplication 10/1/2006
R ���.�� Tooth(broken)(fractured)(duetotrauma),complicated 10/1/2006
R ���.�1 Sepsis 10/1/2006
R ���.�2 Severesepsis 10/1/2006
R ���.�� Systemicinflammatoryresponsesyndromeduetononinfectiousprocesswithoutacuteorgandysfunction 10/1/2006
R ���.�� Systemicinflammatoryresponsesyndromeduetononinfectiousprocesswithacuteorgandysfunction 10/1/2006
R V26.�1 Testingoffemaleforgeneticdiseasecarrierstatus 10/1/2006
R V26.�2 Othergenetictestingoffemale 10/1/2006
iCD-9CMCoDes
43034txtAH.indd 99 2/19/07 2:43:36 PM

100Viewfullpoliciesonlineatwww.amerihealth.com/medpolicy 2006CGPUCompendium
C o D i N G G U i D e l i N e s A N D P o l i C y U P D A T e C o M P e N D i U M
NOTES
43034txtAH.indd 100 2/19/07 2:43:36 PM