2006 job analysis of medication assistants - national council of
TRANSCRIPT
NCSBN reSearCh Brief
Volume 27 | March 2007
2006 Job Analysis
of Medication
Assistants


Report of Findings from the
2006 Job Analysis of Medication Assistants
Anne Wendt, PhD, RN, CAE
National Council of State Boards of Nursing, Inc. (NCSBN®)

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
iv
Mission Statement
The National Council of State Boards of Nursing, composed of member boards, provides leadership to advance regulatory excellence for public protection.
Copyright © 2007 National Council of State Boards of Nursing, inc. (NCSBN®)
all rights reserved. The NCSBN logo, NCLeX®, NCLeX-rN® and NCLeX-PN® are registered trademarks of NCSBN and this document may not be used, reproduced or disseminated to any third party without written permission from NCSBN.
Permission is granted to boards of nursing to use or reproduce all or parts of this document for licensure related purposes only. Nonprofit education programs have permission to use or reproduce all or parts of this document for educational purposes only. Use or reproduction of this document for commercial or for-profit use is strictly prohibited. any authorized reproduc-tion of this document shall display the notice: “Copyright by the National Council of State Boards of Nursing, inc. all rights reserved.” Or, if a portion of the document is reproduced or incorporated in other materials, such written materials shall in-clude the following credit: “Portions copyright by the National Council of State Boards of Nursing, inc. all rights reserved.” address inquiries in writing to NCSBN Permissions, 111 e. Wacker Drive, Suite 2900, Chicago, iL 60601-4277.
Suggested citation:
National Council of State Boards of Nursing. (2007). Report of findings from the 2006 job analysis of medication assis-tants. (Research Brief Vol. 27). Chicago: author.
Printed in the United States of america
ISBN# 0-9779066-4-7
2006 Job AnAlysis of MedicAtion AssistAnts

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
vtAble of contents
TABlE oF CoNTENTS
List of Tables vList of Figures viAcknowledgments viiExecutive Summary 1I. Background of Study 6II. Methodology 7
Panel of Subject Matter Experts (SMEs) 7Questionnaire Development 7Survey Process 7
Mailing 8
Representativeness 8
Confidentiality 8
Return Rates 8Summary 9
III. Demographics, Experiences and Practice Environments of Participants 10Age and Gender 10NCSBN Geographic Area 10Ethnicity 10Years of Experience 10MA Preparation 12
Training Received 12
Specific Medication Assistant Training 12
Training Hours 12
Additional Requirements 12
Training Programs 13
Certification Program/Course 13
Enrollment in Nursing Programs 13
Type of Program Enrollment 13
Continuing Education 13
Annual Continuing Education Requirement 13Work Settings and Shifts 14
Medication Assistant Work Settings 14
Shifts Worked 14
Hours Employed and Hours Worked Per Week 14Clients 14
Client Ages 14
Client Conditions 14
Administering Medication 14Summary 18
IV. Activity Performance Findings 19Activity Performance Characteristics 19
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
vi tAble of contents
Reliability of the Instrument 19
Validation of Findings 19
Representativeness of Activity Statements 19
Overview of Methods 19
Applicability of Activities to Practice Setting 24
Frequency of Activity Performance 24
Importance of Activity Performance 24Subgroup Analyses 24
Years of Experience Subgroup Analysis 24
Work Setting Subgroup Analysis 25
NCSBN Geographic Area Subgroup Analysis 25Conclusion 25V. References 26Appendix A: External Job Analysis Methodology Experts 27Appendix B: 2006 Medication Assistant Subject Matter Experts 28Appendix C: 2006 Medication Assistant Survey Instrument 32Appendix D: Mailing Correspondences 39Appendix E: Activities Sorted by Percent Not Applicable 43Appendix F: Activities Sorted by Mean Frequency 46Appendix G: Activities Sorted by Mean Importance 49Appendix H. Subgroup Analysis: Mean Importance by Years of Experience 52Appendix I. Subgroup Analysis: Mean Importance by Work Setting 56Appendix J. Subgroup Analysis: Mean Importance by NCSBN Geographic Area 60
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
vii
lIST oF TABlES
Table 1. Representativeness 8
Table 2. Jurisdictions Included in NCSBN Geographic Areas 10
Table 3. Years of Experience 11
Table 4. Training Received 12
Table 5. Additional Requirements 13
Table 6. Training Program Completed 13
Table 7. Certification Program/Course Completed 14
Table 8. Formal Nursing Education Program Enrollment 14
Table 9. Type of Program Enrollment 14
Table 10. Annual Continuing Education Requirement 14
Table 11. Medication Assistant Work Setting 17
Table 12. Response Validation Sorted by Activity Number 20
Table 13. Activities Sorted in Survey Order 21
Table 14. Years of Experience Groups 25
Table 15. Work Setting Groups 25
Table 16. NCSBN Geographic Area Groups 25
list of tAbles

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
viii
lIST oF FIguRES
list of figures
Figure 1. NCSBN Geographic Area Representation 10Figure 2. Ethnicity 11Figure 3. Years of Experience 11Figure 4. Specific Medication Assistant Training Required 12Figure 5. Training Hours 12Figure 6. Required Continuing Education 13Figure 7. Hours Worked Per Shift 15Figure 8. Hours Employed to Work Per Week 15Figure 9. Average Hours Worked Per Week 15Figure 10. Client Ages 16Figure 11. Client Conditions 16Figure 12. Clients Administered Medication Per Shift 17

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
ix
ACkNoWlEDgmENTS
This study would not have been possible without the support of a large number of medication assistants from all parts of the United States. The time and attention they gave to completing the survey is greatly appreciated; the information they provided has increased our understanding of the work performed by medication assistants. In addition, the author gratefully acknowledges the assistance of Michelle Eich and Chelsea Ives in the preparation of this document, which was essential to the completion of this study.
A.W.
AcknowledgMents

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
1
Background of StudyThe National Council of State Boards of Nursing (NCSBN®) is responsible for assisting its members, the boards of nursing in the U.S. and four territories, in their mission of public protection through safe nursing practice. Care provided by medication assistants (MAs) impacts client safety directly and influences the quality of care provided by licensed nurses. As nursing practice changes, the activities performed by those assisting nurses may change. Periodic job analyses provide a means of identifying the activities delegated to and performed by MAs.
This 2006 research is the first time NCSBN has per-formed an MA job analysis. However, NCSBN has performed job analyses for registered nurses (RNs), licensed practical/vocational nurses (LPN/VNs) and nursing assistants for many years. Results of MA job analyses may be used by boards of nursing as they regulate the practice of MAs or the nurses overseeing them, by educational programs as they plan curriculums for nurses and their assistants, and by entities involved in the assessment of MA competencies.
One of the most important uses for a job analysis is to provide validity evidence to support an as-sessment or examination. The Joint Standards for Educational and Psychological Testing (APA, AERA and NCME, 1999) state:
Standard 14.10 When evidence of validity on test content is presented, the rationale for defining and describing a specific job content domain in a particular way (e.g., tasks, knowledge, skills, abilities or other personal characteristics) should be stated clearly.
Standard 14.14 The content domain to be covered by a credentialing test should be defined clearly and justified in terms of importance of the content for the credential-worthy perfor-mance in an occupation or profession. A rationale should be provided to support
a claim that the knowledge or skills being assessed are required for credential-worthy performance in an occupation and are consis-tent with the purpose for which the licensing or certification program was instituted.
Indeed, it has been stated that a practice analy-sis should address those competencies that are needed to practice safely and effectively in order to protect the public (CLEAR, 2004).
methodologyA nonexperimental, descriptive study was conduct-ed to explore the activities performed by MAs as well as the frequency and importance of perform-ing the activities in the provision of safe client care.
Panel of subject Matter experts (sMes)
A panel of 14 nurses and MAs was assembled to assist with the job analysis. Panel members all supervised (or personally performed) the work of MAs and represented all NCSBN geographic areas and all major nursing specialties.
The panel of subject matter experts (SMEs) used activity logs, job descriptions, policy and procedure manuals, medication assistant curriculum, job analy-ses, and state nurse practice acts, as well as their own intimate knowledge of MA work to create a list of 104 activities performed by MAs. The activity list was cre-ated within the framework developed by the panel of SMEs.
Questionnaire development
An adequate assessment of MA work requires infor-mation about the frequency of activity performance and the importance of each activity in relation to client safety and well-being. Data related to the fre-quency with which activities are performed and the importance of activity performance were collected from practicing MAs.
The Medication Assistant (MA) Practice Analysis Study contained four sections. Section One asked questions about the MAs’ work environment includ-ing setting, hours worked, and types and numbers
ExECuTIvE SummARy
National Council of State Boards of Nursing, Inc. (NCSBN) | 2006
executive suMMAry

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
2
of clients for whom care was provided. Section Two covered educational preparation and certifications achieved. The 104 MA activities were arranged in random order in Section Three. Section Four allowed the writing of comments and suggestions by the respondent.
survey Process
A random sample of 7,000 MAs was generated from lists supplied to NCSBN by various state agencies. A five-stage, first-class mailing process was used to engage potential participants in the study. All po-tential participants were promised confidentiality with regard to their participation and their respons-es. The study protocol was reviewed and approved by NCSBN’s executive director for compliance with organizational guidelines for research studies involving human subjects.
In March 2006, 7,000 surveys were sent to a mail-ing house to be distributed to MAs across the country. Prior to mailing inside the continental U.S., the mailing house checked the addresses using a program that accesses the National Change of Address (NCOA) database. This pro-gram identified 619 invalid addresses, mostly due to persons moving without providing a change of address. From the 6,381 remaining mailings, an additional 651 surveys were returned due to incorrect addresses. Surveys were returned by 1,433 respondents for an adjusted return rate of 25.0%.
A count of valid responses for the remaining 1,433 scanned surveys was conducted. Analysis was con-ducted on all ratings. Valid responses were counted for all ratings and 50% completion was established as the cut-off. A total of 145 records were removed based on this cut-off. Therefore, the analyzable surveys have valid responses for at least 50% of all ratings. Analyzable surveys were returned by 1,288 respondents for an analyzable return rate of 22.5%.
DemographicsA total of 1,288 MAs responded to the survey. The majority of respondents reported being female (91.9%). Overall, the average age of respondent MAs was 43 years (SD 12.46 years).
The majority of respondent MAs reported their ethnicity as White/Non-Hispanic (64.6%) while 0.4% were Asian Indian, 20.4% were African American and 6.9% were Hispanic.
Of the respondent MAs, 20.8% had one year or less of total experience, 38.1% had two to five years of experience, 19.5% had 6 to 10 years of experience, 9.3% had 11 to 15 years of experience, and 12.2% had over 15 years of experience.
On average, respondents reported approximately seven years of MA experience. About half (49.8%) of responding MAs indicated receiving MA training from their employer. They also frequently reported being prepared through courses offered by their community or junior college (25.4%) and training offered by technical or vocational schools (23.6%). The majority of MA respondents (89.4%) reported being required to complete specific medication as-sistant training. On average, respondents reported that 50 hours of classroom training and 31 hours of clinical training were required. Approximately 77.1% of respondents indicated that being a certified nurs-ing aide/assistant was an additional requirement to become an MA while 67.6% indicated that receipt of a high school diploma/GED was required.
When asked about training completed, MAs were most likely to have completed medication training (35.9%), dialysis technician training (34.1%) and home health aide training (31.6%). MAs were least likely to have completed training as an advanced or skilled nurse assistant (CNA Advanced) (1.2%).
When asked about certifications earned, MAs were most likely to have earned dialysis technician (81.1%), basic nurse assistant (CNA) (66.6%) and first aid (61.6%) certifications. MAs were least likely to have earned CNA Advanced (0.5%) certifications.
Approximately 9.0% of the MA respondents reported current enrollment in nursing education programs. Of the respondents enrolled, 46.7% were enrolled in LPN/VN programs, and 38.7% were enrolled in RN programs (24.0% of these were in associate degree programs). Approximately 10.5% reported that they had applied to but were not currently enrolled in a nursing education program.
When asked whether continuing education was required, a majority (76.2%) of MA respondents
executive suMMAry
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�
reported “yes.” On average, respondents reported a requirement of 11 hours of continuing education contact hours.
work settings
Medication Assistant Employment SettingsMA respondents most frequently reported employ-ment in long-term care facilities (56.1%), assisted living facilities (32.5%) and rehabilitation facilities (11.1%). The least frequently reported practice set-tings were day care (adult or child) (1.6%), schools (2.6%) and correctional facilities (2.6%).
Shifts WorkedThe majority of the MA respondents (53.6%) report-ed working 8 hours per shift.
Hours Employed and WorkedApproximately 49.3% of MAs actually reported being employed to work 40 hours or more per week as a MA. However, 40.7% reported working 40 hours or more per week as a MA.
Client Ages And TypesMAs were asked to indicate all of the age groups and types of clients that they cared for in their roles as MAs. MAs were most likely to care for clients aged 65 to 85 years (77.6%), clients over the age of 85 (57.2%) and clients aged 31 to 64 years (40.0%). MAs provided care most for clients with behavioral/emotional conditions (66.9%), clients with stable chronic conditions (59.9%) and clients at the “end of life” (52.0%). MAs were asked the number of clients they administered medication to during a typical shift. MAs administered medication to an average of 28 clients per shift.
Activity Performance Findings
overview of Methods
The 2006 MA Survey asked respondents to provide frequency and importance ratings for each of the 104 activity statements on the survey. In addition, respondents were asked to indicate if an activity was not applicable to his or her work setting by marking the “NA Not Applicable” response.
Applicability of Activities to Practice setting
Respondents indicated an activity was not ap-plicable to his or her work setting by marking the “NA Not Applicable” response. The activities ranged from 1.43% not applicable (more than 1% of the respondents reported that the activity was not performed within their work settings or al-most 99% of respondents do perform the activity) to 89.10% (nearly 9 out of 10 of the respondents reported the activity was not applicable within their work setting or only 10% of respondents do perform the activity).
frequency of Activity Performance
Respondents were asked to rate the frequency of per-formance of all activities that were applicable to their work settings. They reported how frequently they per-formed the activity in a typical shift using a five-point scale: “0 Less than 1 Time” to “4 times or more.” Frequency of performance for all activities ranged from an average of 0.26 times in a typical shift to 3.87 times in a typical shift.
importance of Activity Performance
Respondents were asked to rank the importance of performing each MA activity considering “safety and/or improving functioning and health status of the client.” Importance ratings were recorded using a four-point scale: “1 Not Important” to “4 Extremely Important.” Importance of perfor-mance for all activities ranged from 2.96 to 3.96 on the four-point scale.
subgroup Analyses
To ensure practice was consistent across cer-tain parameters, analyses were conducted to determine if MA practice activities were viewed similarly by respondents regardless of years of experience, work setting and geographic location. Mean importance ratings for all activity statements were calculated based on 24 subgroups. These subgroups were derived from responses to three demographic questions related to years of experi-ence, work setting and NCSBN geographic area. In summary, average importance ratings were calcu-lated according to years of experience, work setting and geographic area.
executive suMMAry

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
4
ConclusionA nonexperimental, descriptive study was per-formed to explore the importance and frequency of activities performed by MAs. More than 1,400 MAs responded. In general, importance ratings were comparable across work settings, years of experi-ence and geographic location. Results of this study can be used to describe MA practice across a variety of work settings. In addition, the results of the study can be used to identify core MA activities.
executive suMMAry
Report of Findings from the
2006 Job Analysis of Medication Assistants
National Council of State Boards of Nursing, Inc. (NCSBN®)

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
6
The National Council of State Boards of Nursing (NCSBN®) is responsible for assisting its members, the boards of nursing in the U.S. and member board ter-ritories, in their mission of public protection through safe nursing practice. Care provided by medication assistants (MAs) impacts client safety directly and influences the quality of care provided by licensed nurses. As nursing practice itself changes, the activities performed by those assisting nurses may change. Periodic job analyses provide a means of identifying the activities performed and/or delegated to MAs.
This 2006 research is the first MA job analysis per-formed by NCSBN. However, NCSBN has been performing job analyses for registered nurses (RNs), licensed practical/vocational nurses (LPN/VNs) and nursing assistants for many years. The results of MA job analyses may be used by boards of nursing as they regulate the practice of MAs or the nurses overseeing them, by educational programs as they plan curriculums for nurses and their assistants, and by entities involved in the assessment of MA competencies.
One of the most important uses for a job analy-sis is to provide validity evidence to support an assessment or examination. The Joint Standards for Educational and Psychological Testing (AERA, APA and NCME, 1999) states:
Standard 14.10 When evidence of validity on test content is presented, the rationale for defining and describing a specific job content domain in a particular way (e.g., tasks, knowledge, skills, abilities or other personal characteristics) should be stated clearly.
Standard 14.14 The content domain to be covered by a credentialing test should be defined clearly and justified in terms of importance of the content for the credential-worthy performance in an occupation or profession. A rationale should be provided to support a claim that the knowledge or skills being assessed are required for credential-worthy performance in an occupation and are consis-tent with the purpose for which the licensing or certification program was instituted.
Indeed, it has been stated that a practice analysis should address those competencies that are needed to practice safely and effectively in order to protect the public (CLEAR, 2004).
bAckground
BACkgRouND oF STuDy

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
7
A nonexperimental, descriptive study was conduct-ed to explore the activities performed by MAs as well as the frequency and importance of performing the activities in the provision of safe client care.
In order to ensure that the methodology that was used for the 2006 Medication Assistant Job Analysis met and/or exceeded industry standards, an independent External Job Analysis Panel of Methodology Experts reviewed and approved the general methodology. See Appendix A for the list of External Job Analysis Methodology Experts and their qualifications.
Panel of Subject matter Experts (SmEs)A panel of 14 nurses and MAs was assembled to assist with the job analysis. Panel members all supervised (or personally performed) the work of MAs and represented all geographic areas of the country and all major nursing specialties and prac-tice settings for MAs. Refer to Appendix B for a listing of panel members and their qualifications.
The subject matter experts (SMEs) were asked to submit daily activity logs for at least three MAs whom they supervise. In addition, the SMEs sub-mitted MA curriculum, policies and procedures, job descriptions, evaluation forms and orientation manuals. All of these documents, as well as activ-ity statements from other job analyses, state nurse practice acts, and a draft of NCSBN’s Medication Assistant Certified Curriculum were available for the panel to use as source documents. The panel used the activity logs, source documents and their own intimate knowledge of MA work to create a list of 104 activities performed by MAs in various practice settings.
Additionally, the SMEs developed a draft content category structure that would assist them as they developed the activity list.
The panel members worked to create a list of nursing activities performed within each content category. Each MA activity was reviewed for applicability to MA practice and the safety of the client. Care was
taken to create the MA activities at approximately the same level of conceptual specificity, to avoid redundancy within and between categories, and to ensure that the activity statements were clear, understandable and observable. In addition, the panel took care to ensure that the list of activities was comprehensive in order to ensure that there was no artificial restriction in the range of activities. The SMEs also considered the number of activities so as not to create an overwhelming burden for the responding MA. Appendix C contains a copy of the survey form.
Questionnaire DevelopmentAn adequate assessment of MA work requires information about the frequency of activity perfor-mance and importance of each activity in relation to client safety and well-being. Data related to the fre-quency with which activities are performed and the importance of activity performance were collected from practicing MAs.
The questionnaire form and 104 activity statements were reviewed by NCSBN’s Practice, Regulation and Education Committee. Then the survey form was pi-loted and revisions made as needed.
The Medication Assistant (MA) Practice Analysis Study contained four sections. Section One asked questions about the MA’s work environment includ-ing setting, hours worked, and types and numbers of clients for whom care was provided. Section Two covered educational preparation and certifications achieved. The 104 MA activities were arranged in random order in Section Three. Section Four al-lowed the writing of comments and suggestions by respondents. Appendix C contains a copy of the 2006 MA survey.
Survey ProcessA random sample of the names and addresses of 7,000 MAs was generated from lists supplied to NCSBN by various state agencies. A five-stage, first-class mailing process was used to engage potential participants in the study. All potential participants
mEThoDology
Methodology

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
� Methodology
were promised confidentiality with regard to their participation and their responses. The study protocol was reviewed and approved by NCSBN’s executive director for compliance with organizational guide-lines for research studies involving human subjects.
Mailing
Prior to the mailing of the survey, an announcement postcard was mailed to the respondents telling them to expect a survey in a few days and that the survey was very important. This announcement was followed by the first-class mailing of the sur-vey, which included a cover letter that described the scope and purpose of the study. One week later, a reminder postcard was sent. A second re-minder postcard was sent to nonresponders two weeks later. After three weeks a third postcard was mailed. A second survey was sent to any participants who requested one. See Appendix D for copies of the announcement postcard, cover letter and reminder postcards.
representativeness
It became clear that not all jurisdictions could be represented in the sample either because the jurisdiction does not regulate the practice of MAs or because the jurisdiction does not maintain a registry of MAs with addresses that could be disclosed to NCSBN. After contacting several agencies in each jurisdiction, only 13 jurisdictions met the criteria. Only those 13 jurisdictions were included in the sample.
The intention was to mail a survey to a sample of 7,000 MAs such that each of the 13 jurisdictions had equal representation or roughly 538 people for each jurisdiction. The rationale for using equal representation across jurisdictions was to assess whether there is a common practice across jurisdic-tions. Although the intention was to equally weight the jurisdictions, some jurisdictions had fewer than 538 MAs with complete addresses and current cer-tification. As a result, some jurisdictions contributed fewer than the desired number of participants and others contributed slightly more to keep the sample at the targeted 7,000. See Table 1.
As expected, the jurisdictions that comprised smaller percentages of the sample represented smaller per-centages of the cohort that responded. Conversely, several jurisdictions that were well represented in the sample were surprisingly underrepresented in the cohort that responded (i.e., Kentucky, Nebraska and Washington). The reason for the difference in response tendencies across jurisdictions is unclear, however, the difference may be related to the cur-rency of the addresses in the registries.
confidentiality
All potential participants were promised confiden-tiality with regard to their participation and their responses. Preassigned code numbers were used to facilitate cost-effective follow-up mailings. The files that contained mailing information were kept separate from the data files. The study protocol was reviewed and approved by NCSBN’s executive director for compliance with organizational guidelines for research studies involving human subjects.
return rates
In March 2006, 7,000 surveys were sent to a mail-ing house to be distributed to MAs in the identified jurisdictions. Prior to mailing inside the continen-tal U.S., the mailing house checked the addresses
Table 1. Representativeness
StateEqual
Representation %Estimated
Population %Sample % Survey %
IN 7.7 3.5 9.5 14.5
KS 7.7 8.6 9.3 9.9
KY 7.7 6.6 8.5 3.6
MD 7.7 20.8 8.8 6.7
NC 7.7 0.1 0.7 1.6
ND 7.7 1.6 9.8 15.1
NE 7.7 19.2 9.8 0.2
NH 7.7 0.1 1.0 1.5
NJ 7.7 1.7 9.7 11.2
NM 7.7 0.3 4.2 7.2
OR 7.7 1.4 10.0 14.2
TX 7.7 9.5 9.9 12.1
WA 7.7 26.6 8.8 2.2
The adjusted response rate was 22.5%.

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
9
using a program that accesses the National Change of Address (NCOA) database. This pro-gram identified 619 invalid addresses, mostly due to persons moving without providing a change of address. From the 6,381 remaining mailings, an additional 651 surveys were returned due to incorrect addresses. Surveys were returned by 1,433 respondents for an adjusted return rate of 25%. The data set was then analyzed to ensure it met quality assurance criteria.
A count of valid responses for the 1,433 scanned surveys was conducted. Analysis was conducted on all responses. Valid responses were counted for all ratings and 50% completion was established as the cut-off. At total of 145 records were removed based on this cut-off. Therefore, the analyzable surveys have valid responses for at least 50% of all 208 ratings. Analyzable surveys were returned by 1,288 respon-dents for an analyzable response rate of 22.5%.
SummaryA panel of SMEs met and created a list of MA activi-ties. A data collection instrument was created and sent to 7,000 MAs. A 22.5% response rate of analyzable surveys was obtained. This job analysis contains the responses of 1,288 MAs.
Methodology

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
10 study PArticiPAnts
A total of 1,288 MAs responded to the survey. This section reports on the demographic information from those 1,288 respondents.
Age and genderThe majority of respondent MAs reported being female (91.9%). Overall, the average age of respondent MAs was 43 years (SD 12.46 years). The reported ages of respondent MAs ranged from 16 to 79 years old.
NCSBN geographic AreaRespondents were asked the state/territory in which they were currently practicing. Responses were grouped into the four areas of NCSBN’s member boards. Area II had the largest representation with 38.4% of the responding MAs. Area III had the low-est percentage of representation. There were 23 respondents who did not answer this question. See Figure 1. Note that Table 2 lists the NCSBN member jurisdictions in each NCSBN geographic area when the survey was conducted.
EthnicityThe majority of respondent MAs reported their ethnicity as White/Non-Hispanic (64.6%) while 0.4% were Asian Indian, 20.4% were African American and 6.9% were Hispanic. There were 55 respondents who did not answer this question. See Figure 2.
years of ExperienceRespondents reported an average of approxi-mately 7 years of MA experience. Figure 3 presents the distribution of years of experience. Of the respondent MAs, 20.8% had 1 year or less of total experience, 38.1% had 2 to 5 years of experience, 19.5% had 6 to 10 years of experience, 9.3% had 11 to 15 years of experience, and 12.2% had more than 15 years of experience. See Table 3.
DEmogRAPhICS, ExPERIENCES AND PRACTICE ENvIRoNmENTS oF PARTICIPANTS
Figure 1. NCSBN geographic Area Representation
-
Table 2. Jurisdictions Included in NCSBN geographic Areas
Area I Area II Area III Area Iv
Alaska Illinois Alabama Connecticut
American Samoa
Indiana Arkansas Delaware
Arizona Iowa Florida District of Columbia
California Kansas Georgia Maine
Colorado Michigan Kentucky Maryland
Guam Minnesota Louisiana Massachusetts
Hawaii Missouri Mississippi New Hampshire
Idaho Nebraska North Carolina
New Jersey
Montana North Dakota
Oklahoma New York
Nevada Ohio South Carolina
Pennsylvania
New Mexico South Dakota
Tennessee Puerto Rico
NorthernMariana Islands
West Virginia
Texas Rhode Island
Oregon Wisconsin Virginia Vermont
Utah Virgin Islands
Washington
Wyoming

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
11
Figure 2. Ethnicity
-
Table 3. years of Experience
Range Frequency Percent (%)
1 Year or Less 251 20.8
2 to 5 Years 461 38.1
6 to 10 Years 236 19.5
11 to 15 Years 113 9.3
More than 15 Years 148 12.2
Figure 3. years of Experience
study PArticiPAnts
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
12
mA Preparation
training received
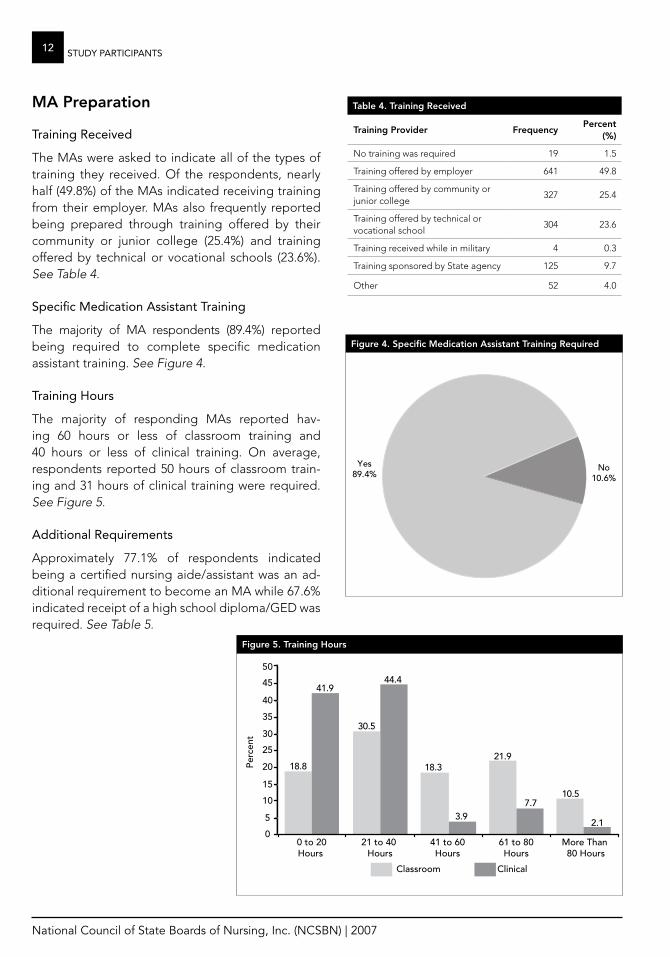
The MAs were asked to indicate all of the types of training they received. Of the respondents, nearly half (49.8%) of the MAs indicated receiving training from their employer. MAs also frequently reported being prepared through training offered by their community or junior college (25.4%) and training offered by technical or vocational schools (23.6%). See Table 4.
specific Medication Assistant training
The majority of MA respondents (89.4%) reported being required to complete specific medication assistant training. See Figure 4.
training hours
The majority of responding MAs reported hav-ing 60 hours or less of classroom training and 40 hours or less of clinical training. On average, respondents reported 50 hours of classroom train-ing and 31 hours of clinical training were required. See Figure 5.
Additional requirements
Approximately 77.1% of respondents indicated being a certified nursing aide/assistant was an ad-ditional requirement to become an MA while 67.6% indicated receipt of a high school diploma/GED was required. See Table 5.
Figure 4. Specific medication Assistant Training Required
No10.6%
Yes89.4%
No23.8%
Yes76.2%
Table 4. Training Received
Training Provider FrequencyPercent
(%)
No training was required 19 1.5
Training offered by employer 641 49.8
Training offered by community or junior college
327 25.4
Training offered by technical or vocational school
304 23.6
Training received while in military 4 0.3
Training sponsored by State agency 125 9.7
Other 52 4.0
Figure 5. Training hours
study PArticiPAnts

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
1�study PArticiPAnts
Figure 6. Required Continuing Education
No10.6%
Yes89.4%
No23.8%
Yes76.2%
training Programs
MAs were most likely to have completed medica-tion (35.9%), dialysis technician (34.1%) and home health aide (31.6%) training programs. MAs were least likely to have completed training as advanced or skilled nurse assistants (CNA Advanced) (1.2%). See Table 6.
certification Program/course
MAs were asked to indicate all of the certification programs/courses that they had completed. They were most likely to have completed certification courses for dialysis technician (81.1%), basic nurse assistant (CNA) (66.6%) and first aid (61.6%). MAs were least likely to have earned CNA Advanced (0.5%) certifications. See Table 7.
enrollment in nursing Programs
Of the MA respondents, 9.0% reported current enrollment in nursing education programs. Ap-proximately 10.5% reported that they had applied to but were not currently enrolled in a nursing education program. See Table 8.
type of Program enrollment
Of the respondents enrolled, 46.7% were enrolled in LPN/VN programs and 38.7% were enrolled in RN programs (24.0% of these were in associate degree programs). See Table 9.
continuing education
When asked whether continuing education was required, a majority (76.2%) of MA respondents reported “yes.” See Figure 6.
Annual continuing education requirement
As shown in Table 10, the majority of respondents reported a requirement between 1 and 8 hours of continuing education per year. On average, respondents reported an annual requirement of 11 hours of continuing education contact hours.
Table 5. Additional Requirements
Requirement Frequency Percent (%)
High School Diploma/GED 871 67.6
Certified Nurse Aide/Assistant 993 77.1
Assessment Test 261 9.2
Home Health Aide 119 20.3
Other 98 7.6
*Respondents were asked to select all that apply
Table 6. Training Program Completed
Program Frequency Percent (%)
Medication 462 35.9
Dialysis Technician 439 34.1
Home Health Aide 407 31.6
Geriatric Care 399 31.0
First Aid 396 30.7
Phlebotomy 371 28.8
Basic Nurse Assistant (CNA) 357 27.7
Wound Care 258 20.0
Psychiatric/Mental Health Aide 233 18.1
Pharmacy Technician 227 17.6
Basic Life Support (CPR) 192 14.9
Feeding Assistant 187 14.5
Restorative Care 131 10.2
Alzheimer’s Care 52 4.0
Other 34 2.6
Intravenous Therapy 33 2.6
Hospice Care 31 2.4
Advanced or Skilled Nurse Assistant (CNA Advanced)
16 1.2
*Respondents were asked to select all that apply

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
14
Work Settings and Shifts
Medication Assistant work settings
MA respondents most frequently reported employ-ment in long-term care facilities (56.1%), assisted living facilities (32.5%) and rehabilitation facilities (11.1%). The least frequently reported work settings were day care (adult or child) (1.6%), schools (2.6%) and correctional facilities (2.6%). See Table 11.
shifts worked
The majority of the MA respondents (53.6%) reported working 8 hours per shift as shown in Figure 7.
hours employed and hours worked Per week
Respondents worked an average of 28.89 hours each week. Approximately 49.3% of MAs reported that they were employed to work 40 hours or more per week as an MA. However, 40.7% of the respondents reported that they actually worked 40 hours or more per week as an MA. See Figures 8 and 9.
Clients
client Ages
MAs were asked to indicate all of the age groups of clients that they cared for in their roles as MAs. As seen in Figure 10, MAs were most likely to care for cli-ents aged 65 to 85 years (77.6%), clients over the age of 85 (57.2%) and clients aged 31 to 64 years (40.0%).
client conditions
MAs were asked to indicate all of the types of “medical conditions” of the clients for whom they provided care. MAs provided care most for clients with behavioral/emotional conditions (66.9%), clients with stable chronic conditions (59.9%) and clients at the “end of life” (52.0%) as shown in Figure 11.
Administering Medication
MAs were asked the number of clients they administered medication to during a typical shift. See Figure 12. MAs administered medication to an average of 28 clients per shift.
study PArticiPAnts
Table 8. Formal Nursing Education Program Enrollment
Response Frequency Percent (%)
No 1,012 80.5
Applied but not currently enrolled 132 10.5
Yes 113 9.0
Table 9. Type of Program Enrollment
Program Frequency Percent (%)
LPN/VN 70 46.7
RN-Associate Degree Program 36 24.0
RN-Diploma 4 2.7
RN-Bachelor’s Degree Program 18 12.0
Other 22 14.7
Table 10. Annual Continuing Education Requirement
Range Frequency Percent (%)
0 Hours 9 1.0
1 to 8 Hours 490 54.7
9 to 12 Hours 212 23.7
More than 12 Hours 185 20.6
Table 7. Certification Program/Course Completed
Program Frequency Percent (%)
Dialysis Technician 1,045 81.1
Basic Nurse Assistant (CNA) 858 66.6
First Aid 793 61.6
Basic Life Support (CPR) 472 36.6
Home Health Aide 437 33.9
Psychiatric/Mental Health Aide 226 17.5
Geriatric Care 204 15.8
Medication 203 15.8
Phlebotomy 147 11.4
Pharmacy Technician 111 8.6
Wound Care 67 5.2
Restorative Care 59 4.6
Feeding Assistant 52 4.0
Alzheimer’s Care 50 3.9
Other 45 3.5
Intravenous Therapy 33 2.6
Hospice Care 28 2.2
Advanced or Skilled Nurse Assistant (CNA Advanced)
7 0.5
*Respondents were asked to select all that apply

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
15study PArticiPAnts
Figure 7. hours Worked Per Shift
Figure 8. hours Employed to Work Per Week
*Respondents were asked to select all that applied
*Respondents were asked to select all that applied
Figure 9. Average hours Worked Per Week
*Respondents were asked to select all that applied
*Respondents were asked to select all that applied

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
16 study PArticiPAnts
Figure 10. Client Ages
*Respondents were asked to select all that applied
*Respondents were asked to select all that applied
Figure 11. Client Conditions*Respondents were asked to select all that applied
*Respondents were asked to select all that applied

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
17study PArticiPAnts
Table 11. medication Assistant Work Setting
Setting Frequency Percent (%)
Long-Term Care Facility 723 56.1
Assisted Living Facility 419 32.5
Rehabilitation Facility 143 11.1
Developmental Disabilities Facility 113 8.8
Residential Facility 106 8.2
Home Health 95 7.4
Psychiatric or Mental Health Facility 82 6.4
Hospice 73 5.7
Group Home 69 5.4
Hospital 38 3.0
Community-Based or Ambulatory Care Facility/Organization 37 2.9
Correctional Facility 34 2.6
Schools 33 2.6
Daycare (Adult or Child) 20 1.6
Other 63 4.9
Figure 12. Clients Administered medication Per Shift
*Respondents were asked to select all that applied
*Respondents were asked to select all that applied

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
1� study PArticiPAnts
SummaryThe majority of MAs responding to the 2006 Medi-cation Assistant Practice Analysis Survey were female averaging 43 years of age. Most of the MAs were trained for their current work by their employers or received training from their commu-nity or junior college. Most of the MAs who had earned medication certification had also earned a dialysis technician certification. About 9.0% of MA respondents were enrolled in a nursing education program. An additional 10.5% of MA respondents had applied to a nursing education program but were not enrolled. The majority of MAs were required to complete some continuing education on an annual basis.
The majority of responding MAs were employed in long-term care facilities and assisted living facilities. They were most likely to care for older clients with behavioral/emotional conditions, clients with stable chronic conditions and clients at “end of life.” Most respondents worked 8-hour shifts and reported working an average of 28.9 hours per week. MAs administered medication to an average of 28 clients per shift.
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
19Activity PerforMAnce
ACTIvITy PERFoRmANCE FINDINgS
Findings relative to the activities performed by MAs are presented in this section of the report. The meth-ods used to collect and analyze findings related to frequency and importance of MA activity perfor-mance will be discussed. A validation of the survey findings by the SME panel will also be provided.
Activity Performance CharacteristicsThis section contains the rating responses of the 1,288 respondent MAs ranging from less than one to more than 35 years of experience, and who are practicing as MAs. Findings relative to the activities performed by MAs are presented in this section of the report. The methods used to collect and analyze activity findings related to frequency and importance of MA activity per-formance will be discussed. A validation of the survey instrument by the SME panel will also be provided.
reliability of the instrument
To evaluate the instrument, a statistic known as coefficient alpha was calculated. This estimate is affected by the number of questions and the num-ber of respondents. Higher values (e.g., greater than 0.90) reflect lower error, with a maximum theoretical value of 1.0. For this survey, the importance ratings had a reliability estimate of 0.98, which suggested limited error (Hopkins, K.D., Stanley, J.C., Hopkins, B.R. 1990).
validation of findings
The SME panel was asked to rate the 104 activity state-ments using the frequency and importance scales. The results of their ratings were averaged for each activity statement. Table 12 shows the five activities that received the lowest and highest activity ratings by the SMEs and the mean frequency and importance ratings by MA respondents. The activities that were predicted by the SMEs to be performed most fre-quently were activities that the respondents rated as being performed most frequently. The activities that were predicted by SMEs to be most important were activities that the respondents rated as most
important. This congruence between expert ratings and respondent ratings helps to provide validation for activity statements and respondent ratings.
representativeness of Activity statements
The participants were asked whether the activities on their questionnaire represented what they actu-ally performed in their positions. A majority (79.5%) indicated that the activities were representative of their current practice. This finding indicates that the survey was perceived by respondents as being a sufficient or reasonable representation of their work. This information is important for establishing the content validity of the survey. In addition, the respondents were asked to list any activity state-ments that were “missing.” These comments were reviewed by NCSBN nursing content staff. In general, the “missing” activities were already included in the lists of activity statements. Examples of “missing” activities noted by several respondents included “Fax orders” and “Suppositories-rectal/vaginal.” Activity statements “Take telephone or-ders for medications” and “Take (receive) written orders for medication” could include “Fax orders.” Similarly, activity statements “Administer a medica-tion by rectal route” and “Administer a medication by vaginal route” includes “Suppositories-rectal/vaginal.” These finding further helped to establish the content validity of the survey instrument.
overview of Methods
The 2006 MA survey asked respondents to provide frequency and importance ratings for each of the 104 activity statements on the survey. The scale of frequency ranged from “0 Less Than 1 Time” to “4 Times or More.” Importance was rated on a scale of “1 Not Important” to “4 Extremely Important.” Respondents were asked to provide the ratings based on a typical shift. Activities sorted in the order they appeared on the 2006 MA Survey can be found in Table 13.

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
20 Activity PerforMAnce
Table 12. Response validation Sorted by Activity Number
Activity # SmE low Frequency ActivitiesRespondent mean
Frequency
t7 Perform Cardiopulmonary Resuscitation (CPR) 0.26
t8 Initiate emergency care for a client who is choking 0.45
t38 Report violation of client rights within required time frame 1.10
t42Report unsafe practice by a health care worker (e.g., improper care, substance abuse, medication theft)
0.80
t65 Administer an emergency medication (e.g., epinephrine Epi-penTM) 0.68
Activity # SmE high Frequency ActivitiesRespondent mean
Frequency
t48 Adhere to basic authorized job duties 3.60
t49 Identify if a medication or route is appropriate to administer 3.25
t95 Follow safety policies/procedures used to prevent incidents and accidents 3.62
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
3.87
t99 Follow facility/agency procedures to verify client identity (e.g., client name bands, allergy bands) 3.55
Activity # SmE low Importance ActivitiesRespondent mean
Importance
t9 Assist with admission, transfer, and/or discharge of client 2.98
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
2.96
t31 Take verbal order for medication 3.03
t32 Take telephone orders for medication 2.97
t68 Administer medication by intradermal route (e.g., PPD test) 3.00
Activity # SmE high Importance ActivitiesRespondent mean
Importance
t46 Maintain confidentiality 3.93
t78Use the six “rights” when administering medication (right drug, right dose, right client, right time, right route, right documentation)
3.96
t79 Checks medications three times before giving 3.93
t88 Review medication orders for completeness (dose, time, route, frequency, name of medication) 3.90
t101 Recognize life threatening emergencies 3.89

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
21
Table 13. Activities Sorted in Survey order
ID #
Activity Statement
Frequency Importance
% NA mean mean
t1 Use effective time management skills 6.49 3.64 3.62
t2 Assist client with activities of daily living (ADLs) (e.g., bathing, feeding, hygiene, toileting)
15.19 2.97 3.44
t3 Assist client with self-administration of medication 24.11 2.78 3.43
t4 Perform capillary blood glucose testing 43.15 2.54 3.45
t5 Provide non-invasive treatments (e.g., basic first aid and continuous passive motion [CPM] machine)
44.70 1.78 3.02
t6 Measure client vital signs (e.g., temperature, pulse, respiration, and blood pressure)
5.99 3.04 3.67
t7 Perform Cardiopulmonary Resuscitation (CPR) 34.26 0.26 3.60
t8 Initiate emergency care for a client who is choking 20.18 0.45 3.72
t9 Assist with admission, transfer, and/or discharge of client 37.76 1.64 2.98
t10 Use cost effective measures when providing client care (e.g., supplies) 29.52 2.68 3.09
t11 Use restraints according to agency policy 55.74 1.70 2.97
t12 Identify signs and/or symptoms of high or low blood sugar 12.23 2.22 3.78
t13 Report signs and/or symptoms of high or low blood sugar 10.22 2.18 3.81
t14 Administer oxygen as ordered 29.60 2.26 3.61
t15 Check oxygen saturation percentage using pulse oximetry 34.77 2.43 3.51
t16 Maintain the supply of medication 11.74 3.06 3.75
t17 Take client’s apical pulse 14.82 2.56 3.57
t18 Respond to signs and/or symptoms of high or low blood sugar 15.04 2.09 3.74
t19 Reinforce client teaching using an established plan of care 29.98 2.53 3.29
t20 Participate in interdisciplinary client care conferences 56.55 1.71 2.99
t21 Notify appropriate personnel of change in client’s condition 7.08 2.68 3.77
t22 Communicate effectively with family, parent, or guardian regarding health care status of client
33.39 2.29 3.46
t23 Give or receive report (e.g., communication log, shift report) 10.66 2.56 3.66
t24 Document client information in accordance with agency policy and procedure 12.25 3.22 3.70
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
58.64 1.81 2.96
t26 Documents adverse effects/ side effects of client’s medication 15.31 2.24 3.76
t27 Send medication orders to pharmacy 26.36 2.46 3.57
t28 Document client’s medication administration according to facility/agency policy 6.64 3.44 3.87
t29 Document medication errors according to facility/agency policy 12.22 1.05 3.81
t30Use resources to review medication information (e.g., drug book, pharmacist, nurse, information technology)
7.60 2.49 3.70
t31 Take verbal orders for medication 74.68 1.42 3.03
t32 Take telephone orders for medication 81.96 1.13 2.97
t33 Take (receive) written orders for medication 59.41 2.21 3.38
t34 Transcribe orders 70.79 2.01 3.18
t35 Review medication record for order changes 22.44 2.88 3.73
t36Use knowledge of medical terminology to interpret symbols, common abbre-viations, and terminology used in administration of medications
9.18 3.29 3.76
t37 Recognize client’s right to refuse medication/treatment 4.45 2.49 3.70
Activity PerforMAnce

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
22 Activity PerforMAnce
Table 13. Activities Sorted in Survey order
ID #
Activity Statement
Frequency Importance
% NA mean mean
t38 Report violation of client rights within required time frame 16.51 1.10 3.72
t39 Act/serve as an advocate for the client 33.11 2.16 3.48
t40 Promote client self-advocacy 31.75 2.09 3.43
t41 Provide culturally sensitive care 22.90 2.34 3.49
t42Report unsafe practice by a health care worker (e.g., improper care, substance abuse, medication theft)
14.95 0.80 3.84
t43 Report client abuse, neglect, injury 13.14 0.81 3.88
t44 Complete incident/accident report according to facility/agency policy 17.82 1.09 3.69
t45 Identify ethical issues affecting staff or client 24.56 1.08 3.42
t46 Maintain confidentiality 1.52 3.56 3.93
t47 Provide for client’s privacy 1.78 3.63 3.87
t48 Adhere to basic authorized job duties 4.08 3.60 3.73
t49 Identify if a medication or route is appropriate to administer 6.41 3.25 3.87
t50 Follow agency policy related to HIPAA or FERPA rules 4.94 3.56 3.85
t51 Count controlled substances 12.37 2.73 3.89
t52 Report medication errors according to facility/agency policy 7.42 1.04 3.85
t53 Recognize limitations within scope of practice 10.01 2.63 3.68
t54 Position a client for medication administration 8.71 3.25 3.73
t55 Observe client’s responses to medication 3.79 3.38 3.81
t56 Report client’s responses to medication 4.04 2.88 3.78
t57 Observe client for adverse effects/side effects of medications 4.65 3.05 3.84
t58Respond to client’s adverse reaction to medication according to facility/agency policy
8.06 1.91 3.80
t59 Withhold medication if necessary 10.45 1.75 3.71
t60 Administer PRN medications 9.33 3.07 3.66
t61 Administer medications by gastric tube (g-tube) 68.35 1.88 3.31
t62 Administer medications by nasogastric (NG) tube 89.10 0.85 3.05
t63 Administer medications by jejunostomy (j-tube) 84.83 1.28 3.12
t64 Administer a subcutaneous medication 72.97 1.96 3.26
t65 Administer an emergency medication (e.g., glucagon, epinephrine (Epi-pen™) 77.55 0.68 3.22
t66 Administer a medication by rectal route 29.86 1.27 3.38
t67 Administer a medication by vaginal route 50.08 0.90 3.26
t68 Administer a medication by intradermal route (e.g., PPD test) 87.78 0.97 3.00
t69 Administer medication by sublingual route 28.97 1.43 3.53
t70 Administer medication by transdermal route (e.g., patch) 19.74 2.14 3.61
t71 Administer medication by a metered dose inhaler 23.18 2.53 3.59
t72 Administer medication by nebulizer 33.52 2.30 3.55
t73 Administer ear medications 16.61 1.58 3.54
t74 Administer eye medications 7.78 2.85 3.64
t75 Administer nasal medication 12.48 2.26 3.58
t76 Administer oral medication 4.35 3.60 3.80
t77 Administer topical medication 12.17 2.63 3.60

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
2�Activity PerforMAnce
Table 13. Activities Sorted in Survey order
ID #
Activity Statement
Frequency Importance
% NA mean mean
t78Use the six “rights” when administering medications (right drug, right dose, right client, right time, right route, right documentation)
2.83 3.78 3.96
t79 Checks medications three times before giving 2.57 3.71 3.93
t80 Observe client swallowing oral medications 2.99 3.72 3.93
t81 Follow medication direction and warning labels 2.92 3.73 3.93
t82 Administer medications prepared by self, not others 9.39 3.63 3.89
t83 Identify expiration date prior to administration of medication 5.16 3.47 3.85
t84 Mix insulin from two different vials for client 88.09 1.29 3.17
t85 Administer medication to coincide with lab tests 49.96 2.07 3.53
t86 Prepare medication for administration (e.g., crushing, mixing with food or water) 9.07 3.35 3.77
t87 Provide adequate liquids when administering medication 4.49 3.68 3.83
t88Review medication orders for completeness (dose, time, route, frequency, name of medication)
4.33 3.65 3.90
t89 Review possible adverse effects/ side effects of medications 5.04 3.08 3.79
t90Dispose of client’s unused or expired medications according to facility/agency policy
23.88 2.35 3.69
t91 Properly store medications 3.83 3.56 3.85
t92 Maintain security of medication storage areas 3.86 3.64 3.89
t93Maintain security of controlled substances according to legal statutes and facility/agency policy
8.33 3.62 3.91
t94 Maintain clean technique 2.34 3.74 3.87
t95 Follow safety policies/procedures used to prevent incidents and accidents 1.68 3.62 3.87
t96 Monitor for and report client care safety hazards 5.76 2.92 3.77
t97Check for client allergies (e.g., latex, food/medications/vaccines/ environmental factors)
7.51 3.17 3.83
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
1.50 3.87 3.94
t99Follow facility/agency procedures to verify client identity (e.g., client’s name bands, allergy bands)
9.44 3.55 3.87
t100 Access poison control agency when necessary 34.12 0.90 3.69
t101 Recognize life threatening emergencies 6.55 1.68 3.89
t102 Maintain equipment for client care 12.89 2.87 3.71
t103 Maintain clean work environment 1.43 3.62 3.80
t104 Date appropriate medication when first used (e.g., insulin, eye drops) 11.02 2.89 3.80

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
24 Activity PerforMAnce
Applicability of Activities to Practice setting
Respondents indicated an activity was not applicable to or not performed in their work setting by marking the “NA Not Applicable” response. The activities ranged from 1.43% not performed (just over 1.0% of the respondents reported that the activity was not performed within their work settings) to 89.10% (nearly 9 out of 10 of the respondents reported the activity was not performed within their work setting). The activities that were performed by fewest respondents were “Administer medications by nasogastric (NG) tube” (89.10% not performed) and “Mix insulin from two different vials for client” (88.08% not performed). The activities that were performed by the most respondents were “Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment (PPE)” (1.50% not performed) and “Maintain clean work environment” (1.43% not performed). Activities sorted by percent not appli-cable can be found in Appendix E.
frequency of Activity Performance
Respondents were asked to rate the frequency of performance of all activities that were applicable to their work settings. They reported how frequently they performed the activity in a typical shift on a five point scale: “0 Less Than 1 Time” to “4 Times or More.” Frequency of performance for all activities ranged from an average of 3.87 times in a typical shift to 0.26 times in a typical shift. Those activities which received the lowest total group mean frequency ratings were “Perform Cardiopulmonary Resuscitation (CPR)”(0.26) and “Initiate emergency care for a client who is choking” (0.45). Those activities which received the highest total group mean frequency ratings were “Use six ‘rights’ when administering medi-cations (right drug, right dose, right client, right time, right route, right documentation)” (3.78) and “Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])” (3.87). Activities sorted by mean frequency rating can be found in Appendix F.
importance of Activity Performance
Respondents were asked to rank the importance of performing each nursing activity considering “safety and/or improving functioning and health status of my client.” Importance ratings were recorded using a four-point scale: “1 Not Important” to “4 Extremely Important.” Importance of perfor-mance for all activities ranged from 2.96 to 3.96 on the four-point scale. Those activities with the lowest importance rating were “Participate in performance improvement/quality assurance activity (e.g., col-lecting data, serving on performance improvement committee” (2.96) and “Use restraints according to agency policy” (2.97). Those activities with the highest importance rating were “Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equip-ment [PPE])” (3.94) and “Use the six ‘rights’ when administering medications (right drug, right dose, right client, right time, right route, right documentation” (3.96). Activities sorted by mean importance rating can be found in Appendix G.
Subgroup AnalysesTo ensure practice was consistent across certain parameters, analyses were conducted to deter-mine if practice (activities) was viewed similarly by respondents regardless of years of experience, work setting and location. Importance ratings for all activity statements were calculated based on 24 demographic subgroups. These subgroups were derived from responses to three demographic questions. Average importance ratings were calculated according to years of experience, work setting and geographic region.
years of experience subgroup Analysis
Respondent importance ratings were divided into five subgroups based on responses to Section 1, Question 3 which queried respondents’ years of MA experience. See Table 14. Subgroup averages were calculated for all activity statements. In general, the mean importance ratings were similar across years of experience. Mean importance data for subgroup analyses by years of experience can be found in Appendix H.

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
25
work setting subgroup Analysis
Importance ratings for all activity statements were calculated for the 15 work setting type response options listed for Section 1, Question 2 of the MA survey instrument. The settings that comprised the 15 subgroups can be found in Table 15 below. The importance ratings for most of the activity state-ments were similar for the various work settings. Mean importance data for subgroup analyses by work setting can be found in Appendix I.
ncsbn geographic Area subgroup Analysis
Importance ratings for all activity statements were calculated for the four geographic areas of the NCSBN member board jurisdictions as shown in Tables 2 and 16. Mean importance rat-ings of the activity statements were quite consistent based on NCSBN’s four geo-graphic areas. Mean importance data for subgroup analyses by NCSBN geographic region can be found in Appendix J.
CoNCluSIoNA nonexperimental, descriptive study was con-ducted to explore the importance and frequency of activities performed by MAs. More than 1,400 MAs responded. In general, importance ratings were comparable across work settings, years of experi-ence and geographic location. Results of this study can be used to determine MA practice across a va-riety of work settings. In addition, the results of the study can be used to identify core MA activities.
Table 14. years of Experience groups
1 1 Year or Less
2 2 to 5 Years
3 6 to 10 Years
4 11 to 15 Years
5 More than 15 Years
Table 15. Work Setting groups
group Name Abbreviation
Assisted Living Facility Ast Liv Fac
Community-based or Ambulatory Care Facility / Organization
Com-Amb Care
Correctional Facility Corr Fac
Daycare (adult or child) Day Care
Developmental Disabilities Facility Dev Dis Fac
Group Home Grp Hme
Home Health Hme Hlth
Hospice Hspc
Hospital Hsptl
Long-Term Care Facility LTC
Psychiatric or Mental Health Facility Psych Hlth Fac
Rehabilitation Facility Rehab
Residential Facility ResdFac
Schools Sch
Other (Please specify) Oth
Table 16. NCSBN geographic Area groups
1 Area I
2 Area II
3 Area III
4 Area IV
Activity PerforMAnce

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
26 references
REFERENCESAmerican Psychological Association, American Educational Research Association, National Council on Measurement in Education (1999). The Joint Standards for Educational and Psychological Testing, Wash-ington, DC, APA.
CLEAR. (2004) Development, Administration, Scoring and Reporting of Credentialing Examinations: Recommendations for Board Members Second Edition (2004) by The Council on Licensure, Enforcement and Regulation, Lexington, KY.
Hopkins, K.D., Stanley, J.C., Hopkins, B.R. (1990). Educational and psychological measurement and evalu-ation, 17th edition. New Jersey: Prentice Hall.
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
27APPendix A
Barbara Showers, PhD, is the director of Wisconsin’s Department of Regulation and Licens-ing’s Office of Education and Examination. She is nationally recognized as an expert in licensure test-ing and has substantial experience with regard to the defensibility of licensure tests.
Richard Smith, PhD, is the editor of the Journal of Applied Measurement and a well-published scholar who specializes in testing and measurement. He has supervised the development of licensing examinations and is very knowledgeable regarding practice analyses and issues regarding connecting test content to practice.
Jim Fidler, PhD, is the director of testing and competency assurance for the American Medical Technologists. He has more than 15 years of experience working with certification testing and supervises the development of several certification examinations.
gene kramer, PhD, is the director of testing for the American Dental Association. In this capacity, he is responsible for the practice analyses that provide the basis for their national licensing examinations. Dr. Kramer has managed these practice analyses and other psychometric analyses for more than 20 years.
matthew Schulz, PhD, worked for American College Testing for many years in several psycho-metric roles. He is knowledgeable about common practices and industry standards with regard to job analyses and practice analyses. He is also familiar with the NCLEX® Examination as he was NCSBN’s director of testing in the 1980s.
APPENDIx A: ExTERNAl JoB ANAlySIS mEThoDology ExPERTS

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
2� APPendix b
Panel members
Name Jurisdiction Setting Specialty
Mary Calkins, PhD, RN* Wyoming Nursing Regulation Nephrology
Chuck Cumiskey, BSN, RN, MBA Washington Nursing Regulation Health Care Policy
Roxann Hofer, LPN Montana Assisted Living Geriatrics
Patricia Latona, MSN, RN New Mexico School NursingPediatrics/Medically Fragile Student Population
Judi Murphy, RN, CDDN New MexicoSchool Nursing/Developmental Disabilities
Developmental Disabilities
Barb Goosic, RN** Nebraska Long-Term Care Geriatrics
Janet Mai, RN Kansas Long-Term Care Staff Education
Gena Munoz, CMA Kansas Long-Term Care Geriatrics
Mary Stassi, RN Missouri Long-Term Care Geriatrics, Geriatric Education
Gail Mallow, MSN, RN** North Dakota Long-Term Care Geriatrics
Angela Cobb, RN North Carolina Public Health/Correctional Facility Correctional Nursing
Martha Holloway, MSHA, BS, RN Alabama School Nursing Pediatric Community Health
Lepaine Sharp-McHenry, RN, MS, FACDONA*
Arkansas Long-Term Care/Nursing RegulationGeriatrics, Mental Health
Deborah Churchey, RN Maryland Community/Home Health Developmental Disabilities
Josephine Seinkiewicz, MSN, RN New Jersey Home Care/Assisted Living Home Care
Margaret Walker, MA, RN New York Nursing Education LPN Education
* Practice Regulation and Education Committee Liaison
** Available by telephone conference call
APPENDIx B: 2006 mEDICATIoN ASSISTANT SuBJECT mATTER ExPERTS

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
29
Area Iliaison: Mary calkins, Phd, rn Professional Nursing Development Coordinator
Cheyenne Regional Medical Center
Board: Wyoming State Board of Nursing
Setting: Nursing Regulation
Dr. Mary Calkins has been a nurse for more than 30 years, first earning an associate degree in nursing in 1975, followed by a BSN in 1989, an MSN in 1993 and a PhD in 1996. She has 17 years of experience as a staff nurse in medical-surgical, pediatrics, dialysis and critical care. She has taught both undergraduate and graduate nursing at the University of Nebraska in Scottsbluff and the University of Wyoming. She was the Wyoming Board of Nursing’s compliance consultant, investigating complaints for two years before accepting the position of assis-tant executive director and practice and education consultant with the Wyoming Board of Nursing. Dr. Calkins’ research has included self-determinism and health-promoting behavior in select sections of the population. Dr. Calkins has been active with NCSBN by holding positions on the Item Review Sub-Committee; Practice, Education and Regulation Committee; and Nominations Committee.
Member: chuck cumiskey, bsn, rn, MbA Nurse Practice and Policy Manager for
Health Professions Quality Assurance
Department of Health
Washington State
Board: Washington State, Nursing Care Quality Assurance Commission
Setting: Nursing Regulation
Cumiskey has 23 years experience in nursing. He is the nurse prac-tice and policy manager for Health Professions Quality Assurance in the Washington State Department of Health and is the leader of the Consumer Safety and Medication Assistance Taskforce in Washington State. Cumiskey has diverse experience in nursing, including working as a major in the U.S. Army, and he has held several management positions. He is a major in the U.S. Army Reserve, a member of the Northwest Organization of Nurse Executives and a member of South Puget Sound Club of Rotary International.
Member: roxann hofer, lPn Health Care Manager
Riverside Senior Living
Board: Montana State Board of Nursing
Setting: Assisted Living
Hofer has 10 years in nursing and is the health care manager at Riverside Senior Living. She has several years of experience training qualified CNAs for MAs. She worked as an LPN in Wisconsin and Mon-tana, and developed a medication aide program with best practice as a top priority. She also supervises medication aides and ensures that they receive ongoing training. Hofer recently received state cer-tification through Montana to be an instructor for medication aide training.
Member: Patricia latona, Msn, rn Special Education Nurse/
Department of Integrated Instructional Services
Alamogordo Public Schools
Board: New Mexico Board of Nursing
Setting: School Nursing
Latona has 34 years of experience in nursing. She is a special education nurse in Alamogordo Public Schools. Latona has worked with medica-tion assistants as a school nurse and in the U.S. Army Nurse Corps. She has a diverse background including school nursing, critical care nursing and burn nursing. She has been published twice in school nursing texts on the subject of burns. Latona has held a variety of positions including director and charge nurse. She has supervised medication administra-tion at various levels and settings. Her background is in the training and integration of paraprofessionals into the health care field. Latona also has multiple experiences in teaching nurses and paraprofessional staff. She is a member of the National Association of Diabetic Educa-tors, American Association of Critical Care Nurses and the National School Nurse Organization.
Member: Judi Murphy, rn Health Care Director
ARCA
Board: New Mexico Board of Nursing
Setting: School Nursing/Developmental Disabilities
Murphy has 38 years in nursing, which includes participating in pro-gram writing, teaching and supervision for CMAs. She is currently Health Care Director at ARCA, a not-for-profit organization providing residential and vocational services to people with developmental dis-abilities. She is a member of New Mexico Board of Nursing’s CMA advisory committee since its beginning in 1991. She has experience in nursing management, nursing education and legal consulting. Mur-phy holds certification as a developmental disabilities nurse, and is active in the New Mexico Developmental Disabilities Nursing Associa-tion. She is a member of several task forces on the developmentally disabled and CMA programs in New Mexico including developmental disabilities and schools. Murphy has also written CMA programs for developmental disabilities programs.
Area IIMember: barb goosic, rn, c Director of Nursing
Franklin Health Care Center
Board: Nebraska Department of Health and Human Services
Regulation and Licensure
Setting: Long-Term Care and Assisted Living
Goosic has seven years of nursing experience and is the director of nursing at Franklin Health Care Center. She is a certified gerontologi-cal nurse, and currently teaches and supervises medication assistants in both long-term care and assisted living settings. Goosic has held a variety of positions in different facilities, including staff nurse, assistant director of nursing and charge nurse. Additionally, she is an EMS mem-ber, CPR instructor for Red Cross and ENCARE presenter.
APPendix b

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�0 APPendix b
Member: Janet Mai, bsn, rn Director of Staff Development
St. Joseph Village
Board: Kansas State Board of Nursing
Setting: Long-Term Care
Mai has 25 years of nursing experience with a diverse nursing back-ground, including medical-surgical, public health, home health, hospice and long-term care. She has developed and presented in-services for long-term care and hospital-based organizations. Mai has also taught CNA, CMA, HHA and medication aide updates for local area facilities.
Member: gena Munoz, cMA Certified Medication Assistant
St. Joseph Village
Board: Kansas Board of Nursing
Setting: Long-Term Care
Munoz has three years of experience as an MA. She has specialty cer-tification in restorative aid and as a phlebotomy technician. She was given the CNA for Excellence award through the Kansas Association of Homes and Services for the Aging (KAHSA). Munoz is respon-sible for administering medications and treatments. She functions as residential coordinator facilitating staff and family meetings.
Member: Mary stassi, rn, c Health Occupations Coordinator
St. Charles Community College (SCC)
Board: Missouri Board of Nursing
Setting: Long-Term Care
Stassi has 25 years of nursing experience including curriculum development. She is a certified nursing assistant and certified medica-tion technician instructor/examiner. Stassi provides education on state and federal guidelines for health care personnel. She also has certifica-tion as a gerontological nurse by the American Nurses Credentialing Center (ANCC). Stassi is experienced in acute care, long-term care, women’s health and nursing management. She held an adjunct faculty position teaching pharmacology at SCC and she plans, coordinates and oversees preprofessional health programs and professional de-velopment programs at SCC. She is a primary writer for the Missouri CNA, CMT and Home Health Aide curriculum and state exams; a co-writer for Missouri LPN IV Therapy Curriculum; an active textbook author for Elsevier Science; and a national speaker on issues related to long-term care. Additionally, Stassi served as a board member and past president of the Long-Term Care Educators Association as well as a committee member for the Missouri SBN IV Therapy Task Force.
Member: gail Mallow, Msn, rn Staff Development Coordinator
Hi-Acres Manor Nursing Center
Board: North Dakota Board of Nursing
Setting: Long-Term Care
Mallow has 34 years in nursing and is currently staff development co-ordinator at Hi-Acres Manor Nursing Center. She is experienced in a variety of nurse settings and specialties including nursing education, where she taught certified nurse assistant and medication assistant classes. Mallow has served on many committees to further excellence in nursing. She has worked on several publications related to nurs-ing education, research and learning texts, and is a well-established speaker. Mallow is a member of Sigma Theta Tau and received the Excellence in Teaching Award from the Presentation College Nursing Honor Society.
Area IIIMember: Angela cobb, rn Nurse Education Director
North Carolina Department of Corrections
Board: North Carolina Board of Nursing
Setting: Public Health/Correctional Facility
Cobb has 23 years of nursing experience and is currently the nurse education director at the North Carolina Department of Corrections. Cobb worked in a variety of staff positions in hospital and long-term care settings, including assistant director of nursing and staff develop-ment. She is current advisory member for and served on the Curriculum Committee for the North Carolina Board of Nursing Medication Aide pilot project. She was also pilot project site administrator and instructor at correctional facilities and assisted living facilities.
Member: Martha holloway, bs, MshA, rn Education Administrator
Alabama State Department of Education
Board: Alabama Board of Nursing
Setting: School Nursing
Holloway has 36 years of nursing experience and is currently education administrator/state school nurse consultant at the Division of Instruc-tion, Alabama State Department of Education. She contributed to the Alabama Board of Nursing’s medication curriculum for school person-nel and has worked in many positions related to school nursing and the health care of children. Holloway is a member of the National Associa-tion of State School Nurse Consultants, National Association of School Nurses, Alabama Association of School Nurses, American School Health Association and the Sigma Theta Tau Nursing Honor Society. She is the former treasurer of the Alabama Association of School Nurs-es and is active in Chi Eta Phi Nursing Sorority. She received the Nurse Practice Award for the Mobile County Nursing Society in 1998. Hol-loway was appointed to numerous state committees and task forces related to nursing and health care, and has worked in the training and development of medication curriculum for the State Department of Education in conjunction with the Alabama Board of Nursing.

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�1
liaison: lepaine sharp-Mchenry, rn, Ms FACDONA
Independent Long-Term Care Nursing Consultant
Board: Arkansas Board of Nursing
Setting: Long-Term Care/Nursing Regulation
Sharp-McHenry has worked in various clinical and management po-sitions in long-term care, acute care and psychiatric mental health settings. She has been responsible for financial, personnel, educa-tion, material and clinical management in each of these settings. She has developed and presented educational training programs for administrators, managers, nurses and allied health profession-als. She has co-authored numerous articles on geriatric care in the long-term care setting and served as an expert panel member in the development of clinical practice guidelines for residents in long-term care facilities. Sharp-McHenry has also conducted research and published in the long-term care field. She is recognized as an expert in geriatric clinical management and nursing administration of long-term care services. She is a licensed nursing home administrator. She is currently a board member for the Arkansas Board of Nursing.
Area IvMember: deborah churchey, rn Director of Nurses
Arc of Washington County
Board: Maryland Board of Nursing
Setting: Community, Home Health
Churchey has a total of 32 years of nursing experience with 22 years as an LPN and 10 years as an RN in the fields of geriatrics, long-term care and developmental disabilities. She is currently the director of nurses at Arc of Washington County. She has worked as a residential director, assistant director of nurses, community health nurse, home manager, LPN and a nurse aide; volunteered as an in-structor for the American Red Cross CPR and First Aid courses. She has also served as a training program and refresher course instructor for the American Heart Association. She assisted nurses from the regional developmental disabilities administration with the development of English comprehension and mathematics pretests and final exams for the medication technicians training program. She assisted regional nurses with final revisions of the medication technicians training pro-gram. Additionally, Churchey is a member of the LPN Practice Issues Committee of the Maryland Board of Nurses. She received awards for Outstanding Employee of the Year for Residential Program in 2002, a Special Recognition Award from Arc of Washington County in 1999, and a First Place award from the Washington County Medical Society in 1996.
Member: Josephine seinkiewicz, Msn, rn Director of Education and Clinical Practice
Home Care Association of New Jersey
Board: New Jersey Board of Nursing
Setting: Home Care/Assisted Living
Seinkiewicz has 36 years of nursing experience with special ex-pertise in community/home health care, educational program development and delivery, staff development and training. She is the emergency preparedness coordinator for the Home Care Association of New Jersey. She authored several articles for publication and spent several years managing health care professionals and paraprofession-als. Seinkiewicz is a well-established speaker on a variety of topics. She has received a certificate in nursing administration advanced through the American Nurses Association. She is a member of the American Nurses Association, the New Jersey State Nursing Association and Sigma Theta Tau. She has also been nominated for and received nu-merous nursing awards.
Member: Margaret walker, MA, rn Associate Dean of Academics
SUNY Brockport/REOC
Board: New York Board of Nursing
Setting: Nursing Education
Walker has 38 years in nursing and is currently the associate dean of academics at SUNY Brockport/REOC. She has expertise in nurs-ing education at multiple levels and in curriculum development. She co-authored the New York State LPN to RN transition program. She is a member of New York State Board for Nursing and chairperson of the Licensure and Education Committee.
APPendix b

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�2 APPendix c
APPENDIx C: 2006 mEDICATIoN ASSISTANT SuRvEy INSTRumENT

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
��APPendix c
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�4 APPendix c

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�5APPendix c

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�6 APPendix c

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�7APPendix c

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�� APPendix c
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
�9
March 2006
Dear Colleague:
You have an invitation and unique opportunity to participate in a nationwide research study on the prac-tice characteristics and activities of Medication Assistants (MA). The study is being conducted by the National Council of State Boards of Nursing (NCSBN™). Your name was selected by a process designed to obtain a representative sample of Medication Assistants from all parts of the country and from all types of educational programs. Your feedback is essential to this process, as it will ensure that the practices of a wide range of Medication Aides are truly represented.
In about a week, you will be receiving a questionnaire in the mail. It consists of questions regarding the activities you perform at work. Because there are so many different types of practice and employment settings, it is extremely important that those selected decide to participate by returning a completed questionnaire. Your decision to participate is voluntary. Responses are completely confidential, and only information that describes groups of participants will be reported.
Please take this opportunity to make a difference and contribute to the nursing profession. In appreciation for your participation, you will receive:
• an opportunity to win one (1) of forty (40) $100 cash prizes
• a 10% discount on all internet courses offered by NCSBN (access learningext.com to see available courses)
• an opportunity to enter a drawing to win a free internet course
• a letter of recognition that you can submit to your supervisor
• an opportunity to receive a summary of the findings
If you have any questions, please contact NCLEX® information at 866-293-9600 (toll free) or email [email protected]. Thank you in advance for your participation!
Sincerely,
Testing Services Department
National Council of State Boards of Nursing
Cover Letter 1
APPendix d
APPENDIx D: mAIlINg CoRRESPoNDENCES

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
40
April 2006
Dear Colleague:
About one month ago, the National Council of State Boards of Nursing, Inc. (NCSBN™) sent a ques-tionnaire to you as part of a national study on Medication Assistant (MA) practice. This study will assist NCSBN to describe Medication Assistant practice.
Your name was selected by a process designed to obtain a representative sample of Medication Assis-tants from all parts of the United States and its territories. Your participation is critical to the outcome of this study. It is vital that we receive surveys describing the practices of MAs from all areas of the country and working in all types of health care agencies and settings.
You recently requested a replacement copy of the questionnaire, which is enclosed. Please complete it as soon as possible — preferably this week — and return it in the enclosed envelope. If you are not currently working in nursing or are not working as a Medication Assistant, please indicate this on question #3 on the questionnaire. All responses will be completely confidential, and only data summarizing groups of participants will be reported.
We hope you take advantage of this unique opportunity to contribute to the nursing profession by completing the questionnaire. Please take the time to make a difference. In appreciation for your par-ticipation, you will receive:
• an opportunity to win one (1) of forty (40) $100 cash prizes
• a 10% discount on all internet courses offered by NCSBN (access learningext.com to see available courses)
• an opportunity to enter a drawing to win a free internet course
• a letter of recognition that you can submit to your supervisor
• an opportunity to receive a summary of the findings
If you have any questions about the study or the questionnaire, please contact NCLEX® information at 866-293-9600 (toll free number) or email [email protected]. We look forward to receiving your com-pleted questionnaire. Please accept our thanks and appreciation for your participation in the study.
Sincerely,
Testing Services Department
National Council of State Boards of Nursing
APPendix d
Cover Letter 2

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
41
Dear Colleague:
Several weeks ago the National Council of State Boards of Nursing (NCSBN™) sent you a survey about your work as a Medication Assistant. If you have already completed and returned the questionnaire, please accept our sincere thanks and disregard this and any future reminders. If you haven’t had a chance to complete it, please try to do so in the next day or two.
You are one of a small group selected to represent many Medication Assistant similar to yourself. There-fore, your participation is crucial to an accurate description of medication aide practice. The information you provide will make a very important contribution to this significant national research study. If you have any questions about the study, please contact NCLEX information at 866-293-9600 (toll free number) or email [email protected].
Testing Services Department
National Council of State Boards of Nursing
Dear Colleague:
Last week the National Council of State Boards of Nursing (NCSBN™) sent you a questionnaire asking for information about your work experiences as a experienced Medication Assistant. If you have already completed and returned the questionnaire, please accept our sincere thanks and disregard this and any future reminders.
If you haven’t had a chance to complete it yet, please try to do so in the next few days. Only a small, representative sample of practicing Medication Assistants was selected for participation in this study. Therefore, your input is especially important if NCSBN is to accurately describe the practice of Medica-tion Assistant. If you did not receive the questionnaire or have misplaced it, please contact NCLEX® information at 866-293-9600 (toll free number) or email [email protected], and you will be sent a replacement.
Testing Services Department
National Council of State Boards of Nursing
APPendix d
Postcard Reminder 1
Postcard Reminder 2

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
42
(Date)
Dear Colleague,
The National Council of State Boards of Nursing, Inc. (NCSBN™) thank you for your participation in this significant national survey of Medication Assistants (MA). Your participation is essential to ensure a com-plete and accurate description of the practice patterns of Medication Assistants.
You have made an important contribution to the nursing profession by returning your completed survey on the MA practice analysis. Please share the attached letter of recognition for your participation with your supervisor and employer.
In appreciation of your participation, your name has been entered into a drawing to win a free Internet course offered by NCSBN’s Learning Extension. To find out the winners of the drawing, please access the following Internet site, www.ncsbn.org/testing/surveys.asp
As a special “thank you” for your participation we are offering you a coupon for 10% off any online con-tinuing education (CE) course at NCSBN Learning Extension. To redeem this special offer, go to www.learningext.com to register for the course of your choice. Please use coupon code ______ at checkout. The coupon expires on _____________________.
Once again, thank you for your contribution to the nursing profession.
Sincerely,
Testing Services Department
National Council of State Boards of Nursing, Inc.
APPendix d
Thank You

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
4�
APPENDIx E: ACTIvITIES SoRTED By PERCENT NoT APPlICABlE
APPendix e
Appendix E. Activities Sorted by Percent Not Applicable
ID# Activity Statement % NA
t62 Administer medications by nasogastric (NG) tube 89.10
t84 Mix insulin from two different vials for client 88.09
t68 Administer a medication by intradermal route (e.g., PPD test) 87.78
t63 Administer medications by jejunostomy (j-tube) 84.83
t32 Take telephone orders for medication 81.96
t65 Administer an emergency medication (e.g., glucagon, epinephrine (Epi-pen™) 77.55
t31 Take verbal orders for medication 74.68
t64 Administer a subcutaneous medication 72.97
t34 Transcribe orders 70.79
t61 Administer medications by gastric tube (g-tube) 68.35
t33 Take (receive) written orders for medication 59.41
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
58.64
t20 Participate in interdisciplinary client care conferences 56.55
t11 Use restraints according to agency policy 55.74
t67 Administer a medication by vaginal route 50.08
t85 Administer medication to coincide with lab tests 49.96
t5 Provide non-invasive treatments (e.g., basic first aid and continuous passive motion (CPM) machine) 44.70
t4 Perform capillary blood glucose testing 43.15
t9 Assist with admission, transfer, and/or discharge of client 37.76
t15 Check oxygen saturation percentage using pulse oximetry 34.77
t7 Perform Cardiopulmonary Resuscitation (CPR) 34.26
t100 Access poison control agency when necessary 34.12
t72 Administer medication by nebulizer 33.52
t22 Communicate effectively with family, parent, or guardian regarding health care status of client 33.39
t39 Act/serve as an advocate for the client 33.11
t40 Promote client self-advocacy 31.75
t19 Reinforce client teaching using an established plan of care 29.98
t66 Administer a medication by rectal route 29.86
t14 Administer oxygen as ordered 29.60
t10 Use cost effective measures when providing client care (e.g., supplies) 29.52
t69 Administer medication by sublingual route 28.97
t27 Send medication orders to pharmacy 26.36
t45 Identify ethical issues affecting staff or client 24.56
t3 Assist client with self-administration of medication 24.11
t90 Dispose of client’s unused or expired medications according to facility/agency policy 23.88
t71 Administer medication by a metered dose inhaler 23.18
t41 Provide culturally sensitive care 22.90
t35 Review medication record for order changes 22.44
t8 Initiate emergency care for a client who is choking 20.18
t70 Administer medication by transdermal route (e.g., patch) 19.74

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
44 APPendix e
Appendix E. Activities Sorted by Percent Not Applicable
ID# Activity Statement % NA
t44 Complete incident/accident report according to facility/agency policy 17.82
t73 Administer ear medications 16.61
t38 Report violation of client rights within required time frame 16.51
t26 Documents adverse effects/ side effects of client’s medication 15.31
t2 Assist client with activities of daily living (ADLs) (e.g., bathing, feeding, hygiene, toileting) 15.19
t18 Respond to signs and/or symptoms of high or low blood sugar 15.04
t42 Report unsafe practice by a health care worker (e.g., improper care, substance abuse, medication theft) 14.95
t17 Take client’s apical pulse 14.82
t43 Report client abuse, neglect, injury 13.14
t102 Maintain equipment for client care 12.89
t75 Administer nasal medication 12.48
t51 Count controlled substances 12.37
t24 Document client information in accordance with agency policy and procedure 12.25
t12 Identify signs and/or symptoms of high or low blood sugar 12.23
t29 Document medication errors according to facility/agency policy 12.22
t77 Administer topical medication 12.17
t16 Maintain the supply of medication 11.74
t104 Date appropriate medication when first used (e.g., insulin, eye drops) 11.02
t23 Give or receive report (e.g., communication log, shift report) 10.66
t59 Withhold medication if necessary 10.45
t13 Report signs and/or symptoms of high or low blood sugar 10.22
t53 Recognize limitations within scope of practice 10.01
t99 Follow facility/agency procedures to verify client identity (e.g., client’s name bands, allergy bands) 9.44
t82 Administer medications prepared by self, not others 9.39
t60 Administer PRN medications 9.33
t36Use knowledge of medical terminology to interpret symbols, common abbreviations, and terminology used in administration of medications
9.18
t86 Prepare medication for administration (e.g., crushing, mixing with food or water) 9.07
t54 Position a client for medication administration 8.71
t93 Maintain security of controlled substances according to legal statutes and facility/agency policy 8.33
t58 Respond to client’s adverse reaction to medication according to facility/agency policy 8.06
t74 Administer eye medications 7.78
t30 Use resources to review medication information (e.g., drug book, pharmacist, nurse, information technology) 7.60
t97 Check for client allergies (e.g., latex, food/medications/vaccines/environmental factors) 7.51
t52 Report medication errors according to facility/agency policy 7.42
t21 Notify appropriate personnel of change in client’s condition 7.08
t28 Document client’s medication administration according to facility/agency policy 6.64
t101 Recognize life threatening emergencies 6.55
t1 Use effective time management skills 6.49
t49 Identify if a medication or route is appropriate to administer 6.41
t6 Measure client vital signs (e.g., temperature, pulse, respiration, and blood pressure) 5.99
t96 Monitor for and report client care safety hazards 5.76
t83 Identify expiration date prior to administration of medication 5.16
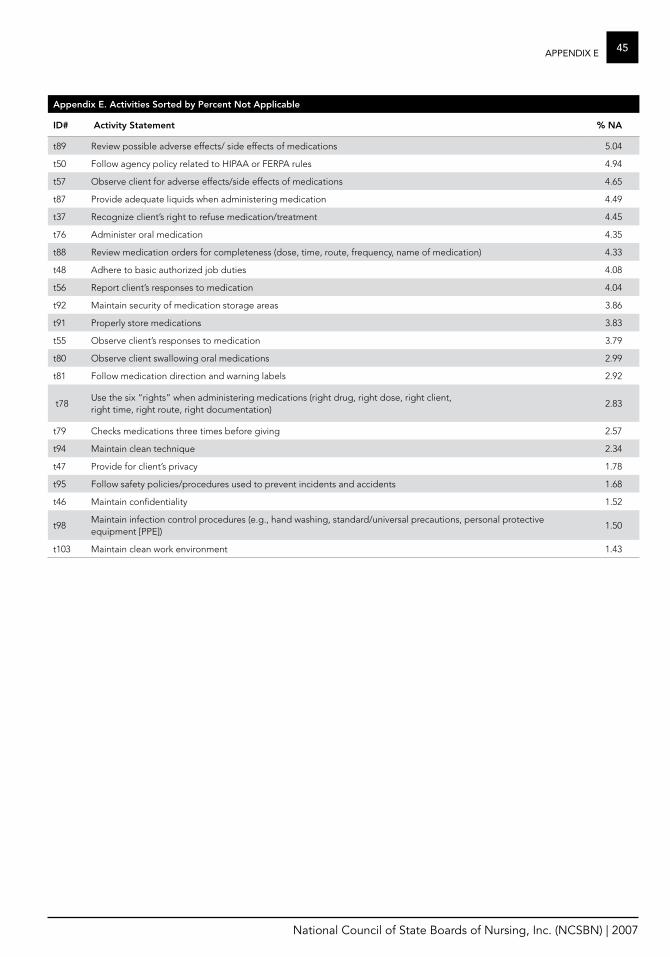
National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
45APPendix e
Appendix E. Activities Sorted by Percent Not Applicable
ID# Activity Statement % NA
t89 Review possible adverse effects/ side effects of medications 5.04
t50 Follow agency policy related to HIPAA or FERPA rules 4.94
t57 Observe client for adverse effects/side effects of medications 4.65
t87 Provide adequate liquids when administering medication 4.49
t37 Recognize client’s right to refuse medication/treatment 4.45
t76 Administer oral medication 4.35
t88 Review medication orders for completeness (dose, time, route, frequency, name of medication) 4.33
t48 Adhere to basic authorized job duties 4.08
t56 Report client’s responses to medication 4.04
t92 Maintain security of medication storage areas 3.86
t91 Properly store medications 3.83
t55 Observe client’s responses to medication 3.79
t80 Observe client swallowing oral medications 2.99
t81 Follow medication direction and warning labels 2.92
t78Use the six “rights” when administering medications (right drug, right dose, right client, right time, right route, right documentation)
2.83
t79 Checks medications three times before giving 2.57
t94 Maintain clean technique 2.34
t47 Provide for client’s privacy 1.78
t95 Follow safety policies/procedures used to prevent incidents and accidents 1.68
t46 Maintain confidentiality 1.52
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
1.50
t103 Maintain clean work environment 1.43

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
46 APPendix f
Appendix F. Activities Sorted by mean Frequency
ID# Activity Statement mean Frequency
t7 Perform Cardiopulmonary Resuscitation (CPR) 0.26
t8 Initiate emergency care for a client who is choking 0.45
t65 Administer an emergency medication (e.g., glucagon, epinephrine (Epi-pen™) 0.68
t42 Report unsafe practice by a health care worker (e.g., improper care, substance abuse, medication theft) 0.80
t43 Report client abuse, neglect, injury 0.81
t62 Administer medications by nasogastric (NG) tube 0.85
t100 Access poison control agency when necessary 0.90
t67 Administer a medication by vaginal route 0.90
t68 Administer a medication by intradermal route (e.g., PPD test) 0.97
t52 Report medication errors according to facility/agency policy 1.04
t29 Document medication errors according to facility/agency policy 1.05
t45 Identify ethical issues affecting staff or client 1.08
t44 Complete incident/accident report according to facility/agency policy 1.09
t38 Report violation of client rights within required time frame 1.10
t32 Take telephone orders for medication 1.13
t66 Administer a medication by rectal route 1.27
t63 Administer medications by jejunostomy (j-tube) 1.28
t84 Mix insulin from two different vials for client 1.29
t31 Take verbal orders for medication 1.42
t69 Administer medication by sublingual route 1.43
t73 Administer ear medications 1.58
t9 Assist with admission, transfer, and/or discharge of client 1.64
t101 Recognize life threatening emergencies 1.68
t11 Use restraints according to agency policy 1.70
t20 Participate in interdisciplinary client care conferences 1.71
t59 Withhold medication if necessary 1.75
t5 Provide non-invasive treatments (e.g., basic first aid and continuous passive motion (CPM) machine) 1.78
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
1.81
t61 Administer medications by gastric tube (g-tube) 1.88
t58 Respond to client’s adverse reaction to medication according to facility/agency policy 1.91
t64 Administer a subcutaneous medication 1.96
t34 Transcribe orders 2.01
t85 Administer medication to coincide with lab tests 2.07
t40 Promote client self-advocacy 2.09
t18 Respond to signs and/or symptoms of high or low blood sugar 2.09
t70 Administer medication by transdermal route (e.g., patch) 2.14
t39 Act/serve as an advocate for the client 2.16
t13 Report signs and/or symptoms of high or low blood sugar 2.18
t33 Take (receive) written orders for medication 2.21
APPENDIx F: ACTIvITIES SoRTED By mEAN FREQuENCy

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
47APPendix f
Appendix F. Activities Sorted by mean Frequency
ID# Activity Statement mean Frequency
t12 Identify signs and/or symptoms of high or low blood sugar 2.22
t26 Documents adverse effects/ side effects of client’s medication 2.24
t75 Administer nasal medication 2.26
t14 Administer oxygen as ordered 2.26
t22 Communicate effectively with family, parent, or guardian regarding health care status of client 2.29
t72 Administer medication by nebulizer 2.3
t41 Provide culturally sensitive care 2.34
t90 Dispose of client’s unused or expired medications according to facility/agency policy 2.35
t15 Check oxygen saturation percentage using pulse oximetry 2.43
t27 Send medication orders to pharmacy 2.46
t30 Use resources to review medication information (e.g., drug book, pharmacist, nurse, information technology) 2.49
t37 Recognize client’s right to refuse medication/treatment 2.49
t19 Reinforce client teaching using an established plan of care 2.53
t71 Administer medication by a metered dose inhaler 2.53
t4 Perform capillary blood glucose testing 2.54
t23 Give or receive report (e.g., communication log, shift report) 2.56
t17 Take client’s apical pulse 2.56
t53 Recognize limitations within scope of practice 2.63
T77 Administer topical medication 2.63
t10 Use cost effective measures when providing client care (e.g., supplies) 2.68
t21 Notify appropriate personnel of change in client’s condition 2.68
t51 Count controlled substances 2.73
t3 Assist client with self-administration of medication 2.78
t74 Administer eye medications 2.85
t102 Maintain equipment for client care 2.87
t35 Review medication record for order changes 2.88
t56 Report client’s responses to medication 2.88
t104 Date appropriate medication when first used (e.g., insulin, eye drops) 2.89
t96 Monitor for and report client care safety hazards 2.92
t2 Assist client with activities of daily living (ADLs) (e.g., bathing, feeding, hygiene, toileting) 2.97
t6 Measure client vital signs (e.g., temperature, pulse, respiration, and blood pressure) 3.04
t57 Observe client for adverse effects/side effects of medications 3.05
t16 Maintain the supply of medication 3.06
t60 Administer PRN medications 3.07
t89 Review possible adverse effects/ side effects of medications 3.08
t97 Check for client allergies (e.g., latex, food/medications/vaccines/environmental factors) 3.17
t24 Document client information in accordance with agency policy and procedure 3.22
t54 Position a client for medication administration 3.25
t49 Identify if a medication or route is appropriate to administer 3.25
t36Use knowledge of medical terminology to interpret symbols, common abbreviations, and terminology used in administration of medications
3.29
t86 Prepare medication for administration (e.g., crushing, mixing with food or water) 3.35

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
4� APPendix f
Appendix F. Activities Sorted by mean Frequency
ID# Activity Statement mean Frequency
t55 Observe client’s responses to medication 3.38
t28 Document client’s medication administration according to facility/agency policy 3.44
t83 Identify expiration date prior to administration of medication 3.47
t99 Follow facility/agency procedures to verify client identity (e.g., client’s name bands, allergy bands) 3.55
t91 Properly store medications 3.56
t50 Follow agency policy related to HIPAA or FERPA rules 3.56
t46 Maintain confidentiality 3.56
t76 Administer oral medication 3.60
t48 Adhere to basic authorized job duties 3.60
t95 Follow safety policies/procedures used to prevent incidents and accidents 3.62
t93 Maintain security of controlled substances according to legal statutes and facility/agency policy 3.62
t103 Maintain clean work environment 3.62
t82 Administer medications prepared by self, not others 3.63
t47 Provide for client’s privacy 3.63
t92 Maintain security of medication storage areas 3.64
t1 Use effective time management skills 3.64
t88 Review medication orders for completeness (dose, time, route, frequency, name of medication) 3.65
t87 Provide adequate liquids when administering medication 3.68
t79 Checks medications three times before giving 3.71
t80 Observe client swallowing oral medications 3.72
t81 Follow medication direction and warning labels 3.73
t94 Maintain clean technique 3.74
t78Use the six “rights” when administering medications (right drug, right dose, right client, right time, right route, right documentation)
3.78
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
3.87

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
49APPendix g
Appendix g. Activities Sorted by mean Importance
ID# Activity Statement mean Importance
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
2.96
t11 Use restraints according to agency policy 2.97
t32 Take telephone orders for medication 2.97
t9 Assist with admission, transfer, and/or discharge of client 2.98
t20 Participate in interdisciplinary client care conferences 2.99
t68 Administer a medication by intradermal route (e.g., PPD test) 3.00
t5 Provide non-invasive treatments (e.g., basic first aid and continuous passive motion (CPM) machine) 3.02
t31 Take verbal orders for medication 3.03
t62 Administer medications by nasogastric (NG) tube 3.05
t10 Use cost effective measures when providing client care (e.g., supplies) 3.09
t63 Administer medications by jejunostomy (j-tube) 3.12
t84 Mix insulin from two different vials for client 3.17
t34 Transcribe orders 3.18
t65 Administer an emergency medication (e.g., glucagon, epinephrine (Epi-pen™) 3.22
t67 Administer a medication by vaginal route 3.26
t64 Administer a subcutaneous medication 3.26
t19 Reinforce client teaching using an established plan of care 3.29
t61 Administer medications by gastric tube (g-tube) 3.31
t33 Take (receive) written orders for medication 3.38
t66 Administer a medication by rectal route 3.38
t45 Identify ethical issues affecting staff or client 3.42
t40 Promote client self-advocacy 3.43
t3 Assist client with self-administration of medication 3.43
t2 Assist client with activities of daily living (ADLs) (e.g., bathing, feeding, hygiene, toileting) 3.44
t4 Perform capillary blood glucose testing 3.45
t22 Communicate effectively with family, parent, or guardian regarding health care status of client 3.46
t39 Act/serve as an advocate for the client 3.48
t41 Provide culturally sensitive care 3.49
t15 Check oxygen saturation percentage using pulse oximetry 3.51
t69 Administer medication by sublingual route 3.53
t85 Administer medication to coincide with lab tests 3.53
t73 Administer ear medications 3.54
t72 Administer medication by nebulizer 3.55
t17 Take client’s apical pulse 3.57
t27 Send medication orders to pharmacy 3.57
t75 Administer nasal medication 3.58
t71 Administer medication by a metered dose inhaler 3.59
t77 Administer topical medication 3.60
t7 Perform Cardiopulmonary Resuscitation (CPR) 3.60
APPENDIx g: ACTIvITIES SoRTED By mEAN ImPoRTANCE

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
50
Appendix g. Activities Sorted by mean Importance
ID# Activity Statement mean Importance
t70 Administer medication by transdermal route (e.g., patch) 3.61
t14 Administer oxygen as ordered 3.61
t1 Use effective time management skills 3.62
t74 Administer eye medications 3.64
t23 Give or receive report (e.g., communication log, shift report) 3.66
t60 Administer PRN medications 3.66
t6Measure client vital signs (e.g., temperature, pulse, respiration, and blood pressure)
3.67
t53 Recognize limitations within scope of practice 3.68
t44 Complete incident/accident report according to facility/agency policy 3.69
t100 Access poison control agency when necessary 3.69
t90Dispose of client’s unused or expired medications according to facility/agency policy
3.69
t30 Use resources to review medication information (e.g., drug book, pharmacist, nurse, information technology) 3.70
t37 Recognize client’s right to refuse medication/treatment 3.70
t24 Document client information in accordance with agency policy and procedure 3.70
t59 Withhold medication if necessary 3.71
t102 Maintain equipment for client care 3.71
t38 Report violation of client rights within required time frame 3.72
t8 Initiate emergency care for a client who is choking 3.72
t54 Position a client for medication administration 3.73
t35 Review medication record for order changes 3.73
t48 Adhere to basic authorized job duties 3.73
t18 Respond to signs and/or symptoms of high or low blood sugar 3.74
t16 Maintain the supply of medication 3.75
t26 Documents adverse effects/ side effects of client’s medication 3.76
t36Use knowledge of medical terminology to interpret symbols, common abbreviations, and terminology used in administration of medications
3.76
t86 Prepare medication for administration (e.g., crushing, mixing with food or water) 3.77
t96 Monitor for and report client care safety hazards 3.77
t21 Notify appropriate personnel of change in client’s condition 3.77
t12 Identify signs and/or symptoms of high or low blood sugar 3.78
t56 Report client’s responses to medication 3.78
t89 Review possible adverse effects/ side effects of medications 3.79
t103 Maintain clean work environment 3.80
t76 Administer oral medication 3.80
t104 Date appropriate medication when first used (e.g., insulin, eye drops) 3.80
t58 Respond to client’s adverse reaction to medication according to facility/agency policy 3.80
t55 Observe client’s responses to medication 3.81
t29 Document medication errors according to facility/agency policy 3.81
t13 Report signs and/or symptoms of high or low blood sugar 3.81
t97 Check for client allergies (e.g., latex, food/medications/vaccines/environmental factors) 3.83
t87 Provide adequate liquids when administering medication 3.83
APPendix g

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
51APPendix g
Appendix g. Activities Sorted by mean Importance
ID# Activity Statement mean Importance
t42 Report unsafe practice by a health care worker (e.g., improper care, substance abuse, medication theft) 3.84
t57 Observe client for adverse effects/side effects of medications 3.84
t91 Properly store medications 3.85
t50 Follow agency policy related to HIPAA or FERPA rules 3.85
t83 Identify expiration date prior to administration of medication 3.85
t52 Report medication errors according to facility/agency policy 3.85
t28 Document client’s medication administration according to facility/agency policy 3.87
t95 Follow safety policies/procedures used to prevent incidents and accidents 3.87
t99 Follow facility/agency procedures to verify client identity (e.g., client’s name bands, allergy bands) 3.87
t94 Maintain clean technique 3.87
t49 Identify if a medication or route is appropriate to administer 3.87
t47 Provide for client’s privacy 3.87
t43 Report client abuse, neglect, injury 3.88
t51 Count controlled substances 3.89
t82 Administer medications prepared by self, not others 3.89
t92 Maintain security of medication storage areas 3.89
t101 Recognize life threatening emergencies 3.89
t88 Review medication orders for completeness (dose, time, route, frequency, name of medication) 3.90
t93 Maintain security of controlled substances according to legal statutes and facility/agency policy 3.91
t46 Maintain confidentiality 3.93
t80 Observe client swallowing oral medications 3.93
t79 Checks medications three times before giving 3.93
t81 Follow medication direction and warning labels 3.93
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
3.94
t78Use the six “rights” when administering medications (right drug, right dose, right client, right time, right route, right documentation)
3.96

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
52
Appendix h. Subgroup Analysis: mean Importance by years of Experience
ID#
Activity Statement
1 year or less
mean
2 to 5 yearsmean
6 to 10 yearsmean
11 to 15 yearsmean
more than 15 years
mean
t1 Use effective time management skills 3.62 3.64 3.61 3.67 3.54
t2Assist client with activities of daily living (ADLs) (e.g., bath-ing, feeding, hygiene, toileting)
3.47 3.39 3.45 3.41 3.48
t3 Assist client with self-administration of medication 3.43 3.42 3.48 3.50 3.35
t4 Perform capillary blood glucose testing 3.43 3.44 3.39 3.50 3.50
t5Provide non-invasive treatments (e.g., basic first aid and continuous passive motion (CPM) machine)
2.97 2.98 3.10 3.10 3.03
t6Measure client vital signs (e.g., temperature, pulse, respiration, and blood pressure)
3.60 3.68 3.70 3.67 3.70
t7 Perform Cardiopulmonary Resuscitation (CPR) 3.62 3.58 3.57 3.67 3.51
t8 Initiate emergency care for a client who is choking 3.72 3.74 3.64 3.71 3.77
t9 Assist with admission, transfer, and/or discharge of client 2.92 2.93 2.93 3.07 3.14
t10Use cost effective measures when providing client care (e.g., supplies)
2.99 3.12 3.04 3.27 3.05
t11 Use restraints according to agency policy 2.86 2.92 2.95 3.19 3.11
t12Identify signs and/or symptoms of high or low blood sugar
3.73 3.77 3.78 3.81 3.83
t13 Report signs and/or symptoms of high or low blood sugar 3.77 3.80 3.83 3.85 3.83
t14 Administer oxygen as ordered 3.52 3.59 3.63 3.66 3.67
t15Check oxygen saturation percentage using pulse oximetry
3.46 3.51 3.50 3.54 3.60
t16 Maintain the supply of medication 3.70 3.74 3.76 3.75 3.79
t17 Take client’s apical pulse 3.50 3.60 3.53 3.64 3.60
t18Respond to signs and/or symptoms of high or low blood sugar
3.66 3.73 3.78 3.84 3.76
t19 Reinforce client teaching using an established plan of care 3.24 3.26 3.34 3.39 3.29
t20 Participate in interdisciplinary client care conferences 2.93 2.91 3.03 3.28 2.99
t21Notify appropriate personnel of change in client’s condition
3.80 3.77 3.73 3.82 3.76
t22Communicate effectively with family, parent, or guard-ian regarding health care status of client
3.45 3.49 3.47 3.46 3.38
t23Give or receive report (e.g., communication log, shift report)
3.66 3.66 3.61 3.65 3.65
t24Document client information in accordance with agency policy and procedure
3.74 3.69 3.69 3.72 3.66
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
2.87 3.01 2.93 3.10 2.94
t26Documents adverse effects/ side effects of client’s medication
3.69 3.75 3.77 3.81 3.78
t27 Send medication orders to pharmacy 3.48 3.58 3.54 3.66 3.63
t28Document client’s medication administration according to facility/agency policy
3.83 3.88 3.87 3.86 3.89
APPENDIx h. SuBgRouP ANAlySIS: mEAN ImPoRTANCE By yEARS oF ExPERIENCE
APPendix h

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
5�APPendix h
Appendix h. Subgroup Analysis: mean Importance by years of Experience
ID#
Activity Statement
1 year or less
mean
2 to 5 yearsmean
6 to 10 yearsmean
11 to 15 yearsmean
more than 15 years
mean
t29Document medication errors according to facility/agency policy
3.76 3.80 3.84 3.85 3.76
t30Use resources to review medication information (e.g., drug book, pharmacist, nurse, information technology)
3.69 3.68 3.72 3.75 3.71
t31 Take verbal orders for medication 2.87 3.02 3.03 3.22 3.10
t32 Take telephone orders for medication 2.86 2.94 2.94 3.13 3.07
t33 Take (receive) written orders for medication 3.32 3.39 3.35 3.47 3.36
t34 Transcribe orders 3.06 3.15 3.14 3.32 3.28
t35 Review medication record for order changes 3.72 3.74 3.74 3.73 3.73
t36Use knowledge of medical terminology to interpret symbols, common abbreviations, and terminology used in administration of medications
3.75 3.74 3.79 3.82 3.77
t37 Recognize client’s right to refuse medication/treatment 3.71 3.69 3.69 3.85 3.64
t38Report violation of client rights within required time frame
3.67 3.71 3.73 3.77 3.68
t39 Act/serve as an advocate for the client 3.54 3.44 3.48 3.52 3.41
t40 Promote client self-advocacy 3.54 3.39 3.39 3.41 3.35
t41 Provide culturally sensitive care 3.54 3.46 3.46 3.57 3.49
t42Report unsafe practice by a health care worker (e.g. improper care, substance abuse, medication theft)
3.83 3.82 3.82 3.90 3.87
t43 Report client abuse, neglect, injury 3.87 3.88 3.87 3.95 3.91
t44Complete incident/accident report according to facil-ity/agency policy
3.62 3.68 3.68 3.79 3.67
t45 Identify ethical issues affecting staff or client 3.35 3.40 3.44 3.57 3.37
t46 Maintain confidentiality 3.9 3.92 3.95 3.94 3.95
t47 Provide for client’s privacy 3.84 3.86 3.90 3.92 3.90
t48 Adhere to basic authorized job duties 3.71 3.71 3.77 3.87 3.69
t49Identify if a medication or route is appropriate to administer
3.85 3.85 3.87 3.94 3.91
t50 Follow agency policy related to HIPAA or FERPA rules 3.86 3.83 3.84 3.89 3.87
t51 Count controlled substances 3.86 3.87 3.88 3.94 3.91
t52Report medication errors according to facility/agency policy
3.84 3.85 3.85 3.89 3.86
t53 Recognize limitations within scope of practice 3.67 3.65 3.69 3.74 3.64
t54 Position a client for medication administration 3.68 3.73 3.71 3.81 3.77
t55 Observe client’s responses to medication 3.79 3.80 3.76 3.91 3.83
t56 Report client’s responses to medication 3.75 3.78 3.77 3.86 3.80
t57Observe client for adverse effects/side effects of medications
3.81 3.84 3.84 3.84 3.87
t58Respond to client’s adverse reaction to medication according to facility/agency policy
3.77 3.81 3.82 3.77 3.83
t59 Withhold medication if necessary 3.67 3.70 3.73 3.74 3.70
t60 Administer PRN medications 3.63 3.67 3.64 3.72 3.64
t61 Administer medications by gastric tube (g-tube) 3.31 3.24 3.24 3.27 3.48
t62 Administer medications by nasogastric (NG) tube 3.04 2.97 2.96 3.02 3.19

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
54 APPendix h
Appendix h. Subgroup Analysis: mean Importance by years of Experience
ID#
Activity Statement
1 year or less
mean
2 to 5 yearsmean
6 to 10 yearsmean
11 to 15 yearsmean
more than 15 years
mean
t63 Administer medications by jejunostomy (j-tube) 3.04 3.02 3.08 3.21 3.29
t64 Administer a subcutaneous medication 3.23 3.19 3.23 3.37 3.23
t65Administer an emergency medication (e.g., glucagon, epinephrine (Epi-pen™)
3.18 3.18 3.20 3.24 3.24
t66 Administer a medication by rectal route 3.32 3.37 3.43 3.41 3.43
t67 Administer a medication by vaginal route 3.18 3.22 3.27 3.34 3.31
t68Administer a medication by intradermal route (e.g., PPD test)
2.98 2.93 3.00 3.04 2.99
t69 Administer medication by sublingual route 3.43 3.50 3.57 3.67 3.51
t70Administer medication by transdermal route (e.g., patch)
3.48 3.63 3.62 3.69 3.62
t71 Administer medication by a metered dose inhaler 3.5 3.59 3.62 3.73 3.54
t72 Administer medication by nebulizer 3.49 3.59 3.51 3.57 3.46
t73 Administer ear medications 3.49 3.54 3.56 3.55 3.50
t74 Administer eye medications 3.57 3.64 3.65 3.73 3.65
t75 Administer nasal medication 3.51 3.59 3.59 3.66 3.52
t76 Administer oral medication 3.73 3.80 3.83 3.84 3.83
t77 Administer topical medication 3.57 3.57 3.62 3.70 3.57
t78Use the six “rights” when administering medications (right drug, right dose, right client, right time, right route, right documentation)
3.92 3.96 3.98 3.97 3.96
t79 Checks medications three times before giving 3.90 3.93 3.94 3.96 3.94
t80 Observe client swallowing oral medications 3.89 3.94 3.92 3.95 3.96
t81 Follow medication direction and warning labels 3.91 3.94 3.92 3.93 3.96
t82 Administer medications prepared by self, not others 3.87 3.88 3.90 3.93 3.93
t83Identify expiration date prior to administration of medication
3.80 3.87 3.88 3.89 3.84
t84 Mix insulin from two different vials for client 3.13 3.15 3.11 3.16 3.09
t85 Administer medication to coincide with lab tests 3.37 3.51 3.60 3.60 3.61
t86Prepare medication for administration (e.g., crushing, mixing with food or water)
3.72 3.78 3.74 3.81 3.81
t87Provide adequate liquids when administering medica-tion
3.74 3.84 3.85 3.88 3.86
t88Review medication orders for completeness (dose, time, route, frequency, name of medication)
3.85 3.90 3.90 3.94 3.92
t89Review possible adverse effects/ side effects of medications
3.74 3.79 3.82 3.80 3.80
t90Dispose of client’s unused or expired medications according to facility/agency policy
3.68 3.70 3.69 3.68 3.67
t91 Properly store medications 3.81 3.86 3.87 3.87 3.82
t92 Maintain security of medication storage areas 3.85 3.90 3.88 3.93 3.89
t93Maintain security of controlled substances according to legal statutes and facility/agency policy
3.87 3.91 3.91 3.96 3.94
t94 Maintain clean technique 3.84 3.86 3.86 3.93 3.90
t95Follow safety policies/procedures used to prevent incidents and accidents
3.84 3.86 3.87 3.91 3.89

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
55
Appendix h. Subgroup Analysis: mean Importance by years of Experience
ID#
Activity Statement
1 year or less
mean
2 to 5 yearsmean
6 to 10 yearsmean
11 to 15 yearsmean
more than 15 years
mean
t96 Monitor for and report client care safety hazards 3.76 3.77 3.76 3.80 3.81
t97Check for client allergies (e.g., latex, food/medications/vaccines/environmental factors)
3.82 3.80 3.88 3.83 3.83
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
3.94 3.94 3.95 3.94 3.97
t99Follow facility/agency procedures to verify client iden-tity (e.g., client’s name bands, allergy bands)
3.81 3.88 3.88 3.85 3.89
t100 Access poison control agency when necessary 3.68 3.67 3.74 3.68 3.64
t101 Recognize life threatening emergencies 3.86 3.89 3.89 3.90 3.91
t102 Maintain equipment for client care 3.69 3.70 3.71 3.77 3.70
t103 Maintain clean work environment 3.77 3.79 3.81 3.85 3.78
t104Date appropriate medication when first used (e.g., insulin, eye drops)
3.78 3.81 3.80 3.84 3.77
APPendix h

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
56
Appendix I. Subgroup Analysis: mean Importance by Work Setting
ID#
Ast liv Fac
Com-Amb Care
Corr Fac
Day Care
Dev Dis Fac
grp hme
hme hlth
hspc hsptl ltC Psych hlth Fac
Rehab Resd Fac
Sch
oth
mean mean mean mean mean mean mean mean mean mean mean mean mean mean mean
t1 3.64 3.63 3.63 3.67 3.49 3.52 3.59 3.76 3.64 3.70 3.45 3.77 3.63 3.32 3.67
t2 3.54 3.46 2.69 3.89 3.60 3.64 3.62 3.39 3.50 3.45 3.51 3.34 3.49 3.00 3.63
t3 3.45 3.52 3.26 3.56 3.48 3.51 3.59 3.52 3.46 3.48 3.37 3.50 3.52 3.56 3.49
t4 3.65 3.32 2.80 3.33 3.41 3.10 3.54 3.67 3.44 3.49 3.31 3.29 3.39 3.08 3.45
t5 3.06 3.33 2.79 3.00 3.06 2.94 2.92 3.00 2.86 3.02 2.93 2.91 3.01 3.43 3.02
t6 3.69 3.59 3.45 3.83 3.54 3.57 3.53 3.81 3.63 3.75 3.67 3.75 3.68 3.57 3.72
t7 3.58 3.78 3.48 3.56 3.73 3.49 3.42 3.64 3.66 3.63 3.71 3.61 3.67 3.52 3.69
t8 3.71 3.90 3.59 3.61 3.77 3.74 3.60 3.84 3.65 3.76 3.76 3.82 3.76 3.76 3.84
t9 3.02 3.14 3.11 3.08 2.76 2.81 2.80 3.02 3.28 3.04 3.01 2.92 2.96 2.38 3.12
t10 3.10 3.38 3.25 3.14 2.93 3.02 3.06 3.20 3.13 3.13 2.80 3.21 3.25 2.73 3.29
t11 2.68 2.63 3.29 2.85 2.93 2.52 2.74 3.00 3.29 3.11 3.28 2.99 2.75 2.48 2.95
t12 3.81 3.90 3.52 3.94 3.72 3.62 3.59 3.85 3.61 3.84 3.76 3.83 3.78 3.59 3.69
t13 3.82 3.87 3.74 3.88 3.72 3.62 3.58 3.85 3.58 3.87 3.72 3.84 3.84 3.62 3.69
t14 3.61 3.62 3.38 3.82 3.51 3.29 3.44 3.61 3.55 3.71 3.55 3.58 3.64 3.13 3.57
t15 3.46 3.30 3.00 3.77 3.45 3.13 3.37 3.68 3.39 3.67 3.58 3.64 3.40 3.05 3.28
t16 3.79 3.65 3.66 3.76 3.73 3.68 3.76 3.83 3.61 3.80 3.80 3.81 3.76 3.48 3.63
t17 3.57 3.39 3.29 3.58 3.36 3.31 3.41 3.70 3.48 3.69 3.55 3.73 3.44 3.09 3.51
t18 3.78 3.60 3.80 3.82 3.61 3.61 3.62 3.82 3.53 3.78 3.75 3.73 3.73 3.57 3.65
t19 3.22 3.26 3.44 3.45 3.42 3.47 3.42 3.45 3.18 3.31 3.41 3.32 3.37 3.17 3.52
t20 3.04 3.04 3.05 3.10 3.15 3.19 3.10 2.86 3.08 2.99 3.33 2.89 3.05 2.57 2.88
t21 3.78 3.72 3.82 3.84 3.74 3.67 3.69 3.83 3.79 3.82 3.78 3.90 3.83 3.54 3.77
t22 3.55 3.52 3.27 3.69 3.57 3.45 3.62 3.57 3.55 3.49 3.28 3.43 3.46 3.54 3.55
t23 3.73 3.69 3.89 3.67 3.61 3.69 3.52 3.70 3.68 3.68 3.70 3.68 3.78 3.39 3.59
t24 3.72 3.82 3.83 3.89 3.72 3.69 3.60 3.79 3.59 3.72 3.75 3.76 3.75 3.58 3.69
t25 2.92 3.08 2.95 3.21 3.23 3.09 3.02 2.89 2.90 3.00 3.06 2.95 2.86 2.84 2.76
t26 3.76 3.63 3.78 3.88 3.76 3.69 3.77 3.85 3.76 3.80 3.73 3.81 3.79 3.39 3.85
t27 3.63 3.68 3.48 3.58 3.37 3.39 3.55 3.72 3.56 3.66 3.51 3.70 3.61 2.62 3.67
t28 3.88 3.76 3.97 3.94 3.90 3.83 3.64 3.97 3.72 3.91 3.85 3.91 3.88 3.81 3.90
APPENDIx I. SuBgRouP ANAlySIS: mEAN ImPoRTANCE By WoRk SETTINg
APPendix i

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
57APPendix i
Appendix I. Subgroup Analysis: mean Importance by Work Setting
ID#
Ast liv Fac
Com-Amb Care
Corr Fac
Day Care
Dev Dis Fac
grp hme
hme hlth
hspc hsptl ltC Psych hlth Fac
Rehab Resd Fac
Sch
oth
mean mean mean mean mean mean mean mean mean mean mean mean mean mean mean
t29 3.83 3.69 3.79 4.00 3.87 3.84 3.60 3.87 3.67 3.85 3.79 3.89 3.79 3.70 3.79
t30 3.69 3.55 3.78 3.78 3.57 3.59 3.69 3.76 3.60 3.77 3.67 3.82 3.65 3.66 3.66
t31 3.16 3.27 2.89 3.31 2.94 2.77 2.93 3.13 3.09 3.12 3.12 2.98 3.18 2.58 3.32
t32 3.09 3.33 2.61 3.33 2.93 2.66 2.96 2.97 3.05 3.07 2.81 2.83 3.10 2.52 3.31
t33 3.45 3.54 3.32 3.54 3.36 3.36 3.35 3.49 3.29 3.41 3.60 3.30 3.35 3.46 3.53
t34 3.29 3.50 2.80 3.33 3.06 2.98 3.20 3.35 3.36 3.27 3.46 2.98 3.07 2.77 3.32
t35 3.77 3.80 3.52 3.63 3.72 3.65 3.61 3.89 3.48 3.80 3.72 3.83 3.67 3.31 3.73
t36 3.76 3.71 3.77 3.81 3.71 3.66 3.62 3.90 3.65 3.85 3.78 3.84 3.72 3.68 3.78
t37 3.71 3.58 3.75 3.76 3.68 3.58 3.62 3.73 3.50 3.72 3.67 3.77 3.62 3.55 3.77
t38 3.72 3.68 3.70 3.88 3.80 3.73 3.63 3.76 3.56 3.77 3.71 3.83 3.72 3.39 3.71
t39 3.43 3.34 3.08 3.75 3.62 3.56 3.48 3.59 3.50 3.54 3.50 3.49 3.42 3.33 3.52
t40 3.37 3.74 2.76 3.57 3.66 3.50 3.45 3.37 3.23 3.47 3.47 3.44 3.50 3.44 3.52
t41 3.43 3.69 3.50 3.63 3.55 3.35 3.48 3.48 3.30 3.55 3.52 3.62 3.34 3.15 3.60
t42 3.84 3.73 3.80 3.94 3.88 3.82 3.73 3.96 3.74 3.89 3.82 3.92 3.84 3.48 3.93
t43 3.86 3.76 3.93 3.94 3.92 3.87 3.79 3.99 3.77 3.93 3.87 3.95 3.90 3.60 3.95
t44 3.75 3.73 3.80 3.82 3.76 3.81 3.56 3.69 3.60 3.66 3.74 3.63 3.76 3.53 3.72
t45 3.44 3.45 3.46 3.38 3.41 3.37 3.34 3.52 3.41 3.45 3.58 3.43 3.41 3.37 3.48
t46 3.91 3.97 3.91 4.00 3.94 3.86 3.88 3.94 3.80 3.95 3.91 3.93 3.91 3.94 3.95
t47 3.87 3.86 3.87 3.94 3.83 3.79 3.86 3.94 3.82 3.91 3.88 3.91 3.82 3.83 3.92
t48 3.70 3.77 3.87 3.76 3.71 3.66 3.63 3.76 3.67 3.78 3.79 3.79 3.76 3.75 3.67
t49 3.86 3.87 3.90 3.94 3.86 3.76 3.81 3.93 3.88 3.91 3.85 3.94 3.76 3.84 3.89
t50 3.80 3.86 3.85 3.94 3.88 3.83 3.72 3.90 3.80 3.89 3.83 3.88 3.85 3.84 3.86
t51 3.87 3.71 3.85 3.94 3.82 3.79 3.85 3.99 3.75 3.94 3.88 3.95 3.86 3.73 3.86
t52 3.86 3.80 3.90 3.89 3.88 3.85 3.76 3.91 3.73 3.88 3.88 3.93 3.85 3.83 3.84
t53 3.65 3.77 3.73 3.81 3.63 3.51 3.61 3.75 3.67 3.71 3.74 3.72 3.65 3.61 3.77
t54 3.68 3.59 3.48 3.87 3.72 3.60 3.62 3.78 3.39 3.83 3.65 3.88 3.65 3.40 3.53
t55 3.78 3.64 3.86 3.94 3.77 3.76 3.73 3.83 3.69 3.85 3.81 3.87 3.83 3.66 3.81
t56 3.77 3.72 3.86 3.89 3.77 3.71 3.74 3.82 3.77 3.84 3.78 3.87 3.83 3.60 3.75
t57 3.82 3.72 3.86 3.94 3.81 3.75 3.85 3.87 3.75 3.90 3.84 3.88 3.83 3.69 3.81

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
5�
Appendix I. Subgroup Analysis: mean Importance by Work Setting
ID#
Ast liv Fac
Com-Amb Care
Corr Fac
Day Care
Dev Dis Fac
grp hme
hme hlth
hspc hsptl ltC Psych hlth Fac
Rehab Resd Fac
Sch
oth
mean mean mean mean mean mean mean mean mean mean mean mean mean mean mean
t58 3.78 3.74 3.94 4.00 3.84 3.76 3.74 3.86 3.79 3.85 3.85 3.85 3.82 3.52 3.85
t59 3.69 3.58 3.54 3.80 3.60 3.65 3.66 3.79 3.63 3.78 3.76 3.79 3.68 3.59 3.74
t60 3.63 3.55 3.59 3.65 3.51 3.49 3.45 3.65 3.58 3.72 3.77 3.72 3.62 3.55 3.67
t61 3.08 3.32 2.88 3.55 3.54 3.07 3.29 3.55 3.24 3.50 3.18 3.44 3.13 3.00 3.03
t62 2.95 3.23 2.71 3.36 3.20 2.95 3.06 3.30 3.17 3.19 3.07 2.93 2.86 2.85 2.85
t63 2.95 3.23 2.71 3.55 3.17 2.92 3.15 3.40 3.13 3.29 3.07 3.08 2.91 2.74 2.97
t64 3.35 3.36 3.00 3.42 3.11 2.95 3.19 3.39 3.30 3.31 3.19 2.95 2.96 2.91 3.49
t65 3.12 3.27 3.33 3.45 3.22 3.08 3.36 3.37 3.35 3.31 3.12 3.06 3.02 3.54 3.22
t66 3.34 3.44 3.30 3.53 3.34 3.15 3.19 3.44 3.30 3.48 3.38 3.45 3.36 3.17 3.24
t67 3.24 3.22 3.1 3.46 3.29 3.09 3.09 3.42 3.22 3.35 3.23 3.12 3.10 3.00 3.23
t68 2.96 3.52 2.88 3.17 3.05 2.85 3.08 2.96 3.13 3.14 3.06 2.83 2.88 2.85 2.97
t69 3.51 3.61 3.32 3.56 3.40 3.24 3.35 3.62 3.31 3.63 3.52 3.59 3.45 3.08 3.60
t70 3.63 3.48 3.31 3.50 3.46 3.32 3.46 3.66 3.40 3.71 3.51 3.64 3.49 3.00 3.70
t71 3.60 3.62 3.36 3.60 3.45 3.41 3.61 3.68 3.43 3.66 3.74 3.66 3.46 3.46 3.67
t72 3.59 3.62 3.44 3.60 3.49 3.36 3.54 3.64 3.23 3.60 3.56 3.49 3.44 3.34 3.60
t73 3.59 3.52 3.57 3.50 3.59 3.56 3.32 3.56 3.50 3.57 3.59 3.52 3.53 3.37 3.54
t74 3.69 3.54 3.61 3.53 3.63 3.58 3.41 3.69 3.55 3.69 3.69 3.66 3.60 3.41 3.64
t75 3.62 3.52 3.56 3.50 3.55 3.51 3.38 3.62 3.48 3.62 3.66 3.63 3.56 3.36 3.60
t76 3.80 3.69 3.93 3.76 3.78 3.72 3.73 3.81 3.78 3.82 3.85 3.83 3.79 3.73 3.87
t77 3.60 3.55 3.56 3.47 3.55 3.48 3.56 3.57 3.75 3.62 3.68 3.59 3.53 3.69 3.43
t78 3.97 3.91 4.00 4.00 3.96 3.99 3.92 3.99 3.88 3.98 3.96 3.99 3.95 3.91 3.98
t79 3.93 3.82 3.90 3.94 3.93 3.96 3.88 3.99 3.88 3.96 3.90 3.96 3.93 3.88 3.95
t80 3.93 3.78 4.00 4.00 3.94 3.97 3.82 3.97 3.85 3.95 3.94 3.95 3.90 3.84 3.93
t81 3.91 3.81 3.97 4.00 3.95 3.96 3.86 3.97 3.82 3.96 3.91 3.96 3.90 3.81 3.93
t82 3.87 3.83 3.72 4.00 3.85 3.92 3.75 3.96 3.59 3.92 3.91 3.88 3.83 3.80 3.96
t83 3.87 3.76 3.76 3.94 3.83 3.93 3.81 3.87 3.68 3.88 3.86 3.94 3.86 3.60 3.87
t84 3.20 3.27 2.83 3.54 3.25 2.71 3.02 3.30 3.10 3.26 3.02 2.80 2.97 2.90 3.28
t85 3.52 3.55 3.29 3.87 3.57 3.33 3.44 3.70 3.50 3.63 3.74 3.52 3.36 3.15 3.57
t86 3.73 3.67 3.67 3.82 3.80 3.69 3.58 3.82 3.59 3.84 3.80 3.86 3.72 3.62 3.71
APPendix i

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
59APPendix i
Appendix I. Subgroup Analysis: mean Importance by Work Setting
ID#
Ast liv Fac
Com-Amb Care
Corr Fac
Day Care
Dev Dis Fac
grp hme
hme hlth
hspc hsptl ltC Psych hlth Fac
Rehab Resd Fac
Sch
oth
mean mean mean mean mean mean mean mean mean mean mean mean mean mean mean
t87 3.82 3.76 3.81 3.76 3.85 3.79 3.87 3.91 3.69 3.87 3.83 3.88 3.78 3.63 3.77
t88 3.89 3.81 3.87 3.89 3.90 3.90 3.83 3.91 3.75 3.92 3.86 3.90 3.83 3.81 3.95
t89 3.78 3.66 3.87 3.67 3.78 3.74 3.69 3.84 3.79 3.82 3.81 3.82 3.81 3.71 3.83
t90 3.68 3.67 3.63 3.75 3.76 3.57 3.58 3.75 3.60 3.74 3.76 3.75 3.65 3.47 3.60
t91 3.87 3.74 3.97 3.89 3.90 3.88 3.80 3.85 3.76 3.85 3.83 3.87 3.83 3.91 3.90
t92 3.87 3.73 3.87 3.89 3.91 3.90 3.74 3.90 3.66 3.91 3.83 3.88 3.86 3.84 3.97
t93 3.91 3.77 3.97 3.94 3.86 3.94 3.76 4.00 3.76 3.94 3.85 3.93 3.89 3.90 3.93
t94 3.85 3.86 3.91 3.79 3.86 3.81 3.84 3.92 3.77 3.89 3.83 3.88 3.83 3.88 3.89
t95 3.87 3.88 3.88 3.94 3.89 3.79 3.85 3.91 3.80 3.88 3.83 3.90 3.86 3.78 3.95
t96 3.75 3.82 3.86 3.78 3.76 3.72 3.77 3.83 3.69 3.79 3.81 3.80 3.80 3.65 3.85
t97 3.81 3.88 3.82 3.87 3.82 3.82 3.73 3.87 3.94 3.87 3.88 3.92 3.82 3.68 3.87
t98 3.94 3.97 3.97 4.00 3.90 3.92 3.96 3.99 3.89 3.95 3.89 3.93 3.91 3.91 3.97
t99 3.85 3.87 3.97 3.94 3.82 3.80 3.62 3.96 3.76 3.92 3.87 3.93 3.86 3.66 3.83
t100 3.66 3.70 3.83 3.69 3.75 3.72 3.70 3.69 3.68 3.73 3.74 3.69 3.68 3.75 3.74
t101 3.87 3.91 3.88 3.83 3.94 3.90 3.92 3.91 3.85 3.91 3.88 3.95 3.91 3.81 3.98
t102 3.66 3.64 3.92 3.78 3.66 3.61 3.75 3.73 3.74 3.75 3.75 3.72 3.71 3.62 3.68
t103 3.79 3.85 3.87 3.74 3.8 3.72 3.81 3.79 3.67 3.81 3.74 3.80 3.80 3.81 3.86
t104 3.83 3.75 3.93 3.81 3.77 3.67 3.75 3.84 3.68 3.84 3.79 3.85 3.76 3.67 3.81

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
60
Appendix J. Subgroup Analysis by NCSBN geographic Area
ID# Activity StatementArea Imean
Area IImean
Area IIImean
Area Ivmean
t1 Use effective time management skills 3.63 3.63 3.70 3.52
t2Assist client with activities of daily living (ADLs) (e.g., bathing, feeding, hygiene, toileting)
3.27 3.56 3.41 3.42
t3 Assist client with self-administration of medication 3.47 3.42 3.48 3.35
t4 Perform capillary blood glucose testing 3.36 3.62 3.07 3.48
t5Provide non-invasive treatments (e.g., basic first aid and continuous passive motion (CPM) machine)
2.90 3.17 2.75 3.08
t6Measure client vital signs (e.g., temperature, pulse, respiration, and blood pressure)
3.64 3.64 3.77 3.67
t7 Perform Cardiopulmonary Resuscitation (CPR) 3.55 3.68 3.56 3.53
t8 Initiate emergency care for a client who is choking 3.67 3.77 3.75 3.70
t9 Assist with admission, transfer, and/or discharge of client 2.93 3.03 3.02 2.88
t10 Use cost effective measures when providing client care (e.g., supplies) 2.92 3.16 3.20 3.02
t11 Use restraints according to agency policy 2.85 3.07 3.15 2.70
t12 Identify signs and/or symptoms of high or low blood sugar 3.73 3.82 3.78 3.76
t13 Report signs and/or symptoms of high or low blood sugar 3.74 3.86 3.79 3.80
t14 Administer oxygen as ordered 3.61 3.74 3.40 3.48
t15 Check oxygen saturation percentage using pulse oximetry 3.54 3.61 3.42 3.30
t16 Maintain the supply of medication 3.73 3.70 3.80 3.81
t17 Take client’s apical pulse 3.60 3.55 3.62 3.48
t18 Respond to signs and/or symptoms of high or low blood sugar 3.68 3.79 3.71 3.77
t19 Reinforce client teaching using an established plan of care 3.28 3.30 3.31 3.26
t20 Participate in interdisciplinary client care conferences 2.89 3.00 3.03 3.08
t21 Notify appropriate personnel of change in client’s condition 3.77 3.76 3.83 3.79
t22Communicate effectively with family, parent, or guardian regarding health care status of client
3.40 3.49 3.44 3.51
t23 Give or receive report (e.g., communication log, shift report) 3.55 3.69 3.64 3.73
t24 Document client information in accordance with agency policy and procedure 3.61 3.75 3.77 3.71
t25Participate in performance improvement/quality assurance activity (e.g., collecting data, serving on performance improvement committee)
2.79 2.98 3.13 2.98
t26 Documents adverse effects/ side effects of client’s medication 3.74 3.76 3.82 3.72
t27 Send medication orders to pharmacy 3.60 3.53 3.59 3.61
t28Document client’s medication administration according to facility/agency policy
3.85 3.86 3.89 3.87
t29 Document medication errors according to facility/agency policy 3.79 3.82 3.81 3.80
t30Use resources to review medication information (e.g., drug book, pharmacist, nurse, information technology)
3.74 3.67 3.81 3.59
t31 Take verbal orders for medication 2.96 3.15 3.10 2.81
t32 Take telephone orders for medication 2.76 3.11 3.01 2.92
t33 Take (receive) written orders for medication 3.32 3.41 3.31 3.45
t34 Transcribe orders 3.09 3.23 3.12 3.22
t35 Review medication record for order changes 3.72 3.72 3.82 3.73
APPENDIx J. SuBgRouP ANAlySIS: mEAN ImPoRTANCE By NCSBN gEogRAPhIC AREA
APPendix J

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
61APPendix J
Appendix J. Subgroup Analysis by NCSBN geographic Area
ID# Activity StatementArea Imean
Area IImean
Area IIImean
Area Ivmean
t36Use knowledge of medical terminology to interpret symbols, common abbre-viations, and terminology used in administration of medications
3.75 3.80 3.82 3.66
t37 Recognize client’s right to refuse medication/treatment 3.70 3.68 3.76 3.70
t38 Report violation of client rights within required time frame 3.76 3.70 3.78 3.64
t39 Act/serve as an advocate for the client 3.59 3.49 3.40 3.38
t40 Promote client self-advocacy 3.47 3.46 3.41 3.34
t41 Provide culturally sensitive care 3.52 3.52 3.51 3.41
t42Report unsafe practice by a health care worker (e.g., improper care, substance abuse, medication theft)
3.84 3.85 3.85 3.79
t43 Report client abuse, neglect, injury 3.87 3.90 3.90 3.84
t44 Complete incident/accident report according to facility/agency policy 3.58 3.71 3.69 3.75
t45 Identify ethical issues affecting staff or client 3.37 3.49 3.42 3.36
t46 Maintain confidentiality 3.88 3.95 3.95 3.90
t47 Provide for client’s privacy 3.83 3.91 3.92 3.82
t48 Adhere to basic authorized job duties 3.75 3.73 3.76 3.68
t49 Identify if a medication or route is appropriate to administer 3.86 3.88 3.90 3.83
t50 Follow agency policy related to HIPAA or FERPA rules 3.79 3.90 3.88 3.82
t51 Count controlled substance 3.90 3.88 3.94 3.82
t52 Report medication errors according to facility/agency policy 3.84 3.85 3.90 3.85
t53 Recognize limitations within scope of practice 3.70 3.69 3.68 3.62
t54 Position a client for medication administration 3.77 3.71 3.81 3.65
t55 Observe client’s responses to medication 3.84 3.78 3.83 3.78
t56 Report client’s responses to medication 3.81 3.76 3.80 3.77
t57 Observe client for adverse effects/side effects of medications 3.87 3.83 3.86 3.80
t58Respond to client’s adverse reaction to medication according to facility/agency policy
3.83 3.81 3.83 3.75
t59 Withhold medication if necessary 3.72 3.70 3.76 3.66
t60 Administer PRN medications 3.69 3.66 3.70 3.59
t61 Administer medications by gastric tube (g-tube) 3.47 3.42 3.06 2.87
t62 Administer medications by nasogastric (NG) tube 3.02 3.18 2.97 2.83
t63 Administer medications by jejunostomy (j-tube) 3.09 3.28 3.01 2.77
t64 Administer a subcutaneous medication 3.04 3.40 3.16 3.32
t65Administer an emergency medication (e.g., glucagon, epinephrine (Epi-pen™)
3.12 3.38 3.17 3.03
t66 Administer a medication by rectal route 3.36 3.46 3.40 3.24
t67 Administer a medication by vaginal route 3.10 3.41 3.31 3.06
t68 Administer a medication by intradermal route (e.g., PPD test) 2.74 3.19 3.10 2.82
t69 Administer medication by sublingual route 3.54 3.61 3.55 3.31
t70 Administer medication by transdermal route (e.g., patch) 3.60 3.65 3.63 3.52
t71 Administer medication by a metered dose inhaler 3.64 3.65 3.46 3.52
t72 Administer medication by nebulizer 3.56 3.58 3.35 3.63
t73 Administer ear medications 3.47 3.55 3.53 3.58
t74 Administer eye medications 3.59 3.67 3.66 3.65

National Council of State Boards of Nursing, Inc. (NCSBN) | 2007
62 APPendix J
Appendix J. Subgroup Analysis by NCSBN geographic Area
ID# Activity StatementArea Imean
Area IImean
Area IIImean
Area Ivmean
t75 Administer nasal medication 3.53 3.61 3.61 3.56
t76 Administer oral medication 3.78 3.82 3.83 3.78
t77 Administer topical medication 3.55 3.64 3.59 3.59
t78Use the six “rights” when administering medications (right drug, right dose, right client, right time, right route, right documentation)
3.95 3.96 3.95 3.97
t79 Checks medications three times before giving 3.90 3.93 3.93 3.96
t80 Observe client swallowing oral medications 3.91 3.93 3.95 3.92
t81 Follow medication direction and warning labels 3.92 3.94 3.94 3.91
t82 Administer medications prepared by self, not others 3.82 3.90 3.91 3.90
t83 Identify expiration date prior to administration of medication 3.85 3.83 3.88 3.89
t84 Mix insulin from two different vials for client 3.02 3.35 3.12 2.97
t85 Administer medication to coincide with lab tests 3.54 3.60 3.54 3.34
t86Prepare medication for administration (e.g., crushing, mixing with food or water)
3.78 3.78 3.81 3.68
t87 Provide adequate liquids when administering medication 3.83 3.84 3.86 3.79
t88Review medication orders for completeness (dose, time, route, frequency, name of medication)
3.88 3.90 3.90 3.90
t89 Review possible adverse effects/ side effects of medications 3.82 3.79 3.76 3.77
t90Dispose of client’s unused or expired medications according to facility/agency policy
3.71 3.65 3.77 3.67
t91 Properly store medications 3.84 3.86 3.84 3.85
t92 Maintain security of medication storage areas 3.87 3.91 3.88 3.86
t93Maintain security of controlled substances according to legal statutes and facility/agency policy
3.88 3.93 3.92 3.88
t94 Maintain clean technique 3.85 3.89 3.88 3.85
t95 Follow safety policies/procedures used to prevent incidents and accidents 3.85 3.88 3.88 3.85
t96 Monitor for and report client care safety hazards 3.76 3.78 3.78 3.76
t97Check for client allergies (e.g., latex, food/medications/vaccines/environmental factors)
3.84 3.83 3.86 3.78
t98Maintain infection control procedures (e.g., hand washing, standard/universal precautions, personal protective equipment [PPE])
3.94 3.94 3.95 3.93
t99Follow facility/agency procedures to verify client identity (e.g., client’s name bands, allergy bands)
3.86 3.86 3.92 3.83
t100 Access poison control agency when necessary 3.67 3.73 3.71 3.63
t101 Recognize life threatening emergencies 3.92 3.91 3.87 3.85
t102 Maintain equipment for client care 3.70 3.73 3.71 3.67
t103 Maintain clean work environment 3.79 3.79 3.86 3.78
t104 Date appropriate medication when first used (e.g., insulin, eye drops) 3.78 3.80 3.83 3.83