2006 protocol update central new york ems 50 presidential plaza jefferson tower, suite ll1 syracuse,...
TRANSCRIPT
2006 Protocol Update2006 Protocol Update
Central New York EMS50 Presidential Plaza
Jefferson Tower, Suite LL1Syracuse, New York 13202
Click mouse anywhere on slide to continue….

OverviewOverview
• Format Readjustments• Adult Protocol Changes• Pediatric Protocol Changes• Special Protocols and Charts• Review

Format ChangesFormat Changes
• Index– Easier to read and quickly locate protocols
• Pages – Laminated for durability and longevity
• Section tabs– Indicate the protocol section on the side of
the page– Sections are no longer designated at the top
of the page

Format ChangesFormat Changes
• Fonts– Though it may still seem small, font
size has been maximized without compromising the size of the book
• Clinical judgment boxes– Protocol sections that require clinical
judgment are:
black with white letters

Format ChangesFormat Changes
• Cardiac Protocol Titles– Titles are based on subject and the word
“cardiac” has been removed from the titles
– Asystole– Bradycardia, Symptomatic– Cardiogenic Shock– Chest Pain– PEA– Tachycardia, Unstable– Tachycardia, Stable– V-Fib / Pulseless V-Tach

Adult Protocol ChangesAdult Protocol Changes
• Pain – Non-Cardiac (page 29)Routine Medical or Trauma Care
Nubain 10 mg IVOR
Morphine up to 5 mg IV
May repeat every 5 min.
up to 20 mg
Major Pain
Acetaminophen PO 15 mg/kg (maximum dose 1000mg) if patient can tolerate oral
medication
Assess with Visual Analog Pain Scale (page 71) or
equivalent
Minor Pain
EMT-CC/EMT-P
* For pain of 6 and below via the Visual Analog Pain Scale (page 71) consider treatment via the Minor Pain pathway only, and care may be transferred to BLS.

Adult Protocol ChangesAdult Protocol Changes
• Pain – Non-Cardiac– Agencies will carry 325 mg and/or 500 mg
tablets of acetaminophen and potable water. – While available under standing order and not
technically a controlled substance, the storage, use, distribution and record-keeping shall be the same for nalbuphine (Nubain) as is currently utilized for ALL controlled substances.

Adult Protocol ChangesAdult Protocol Changes
• Facilitated Intubation (page 5)– Etomidate 0.3 mg/kg
Etomidate 20 mg IV over 30 to 60 seconds
Repeat Etomidate dose after 1-2 minutes if desired effect is not achieved
After successful intubationConsider Diazepam 5.0 mg or Versed 2.0 mg for continued
sedation*
To reverse effects of diazepam (Valium ) or midazolam (Versed ) due to complications arising from unsuccessful intubation (for
example: hypotension or inability to maintain an airway) flumazenil (Romazicon ) 0.2 mg IV may be given.

Adult Protocol ChangesAdult Protocol Changes• Allergic Reaction/Anaphylaxis (page 10)
Systolic BP <90 mmHg or severe respiratory
compromise
Epi 1:1000 0.3 mg SC
Benadryl 50 mg slow IV/IM
If patient does not improve
Fluid Challenge (page 7)
Transport
If patient does not improve
Epi 1:1000 0.3 mg SC
Epi 1:10,000 0.5 –1.0 mg IV or 2 mg ET
Epi 1:10,000 0.3mg IV slow over 5 minutes or 2 mg ET
Adult Protocol ChangesAdult Protocol Changes
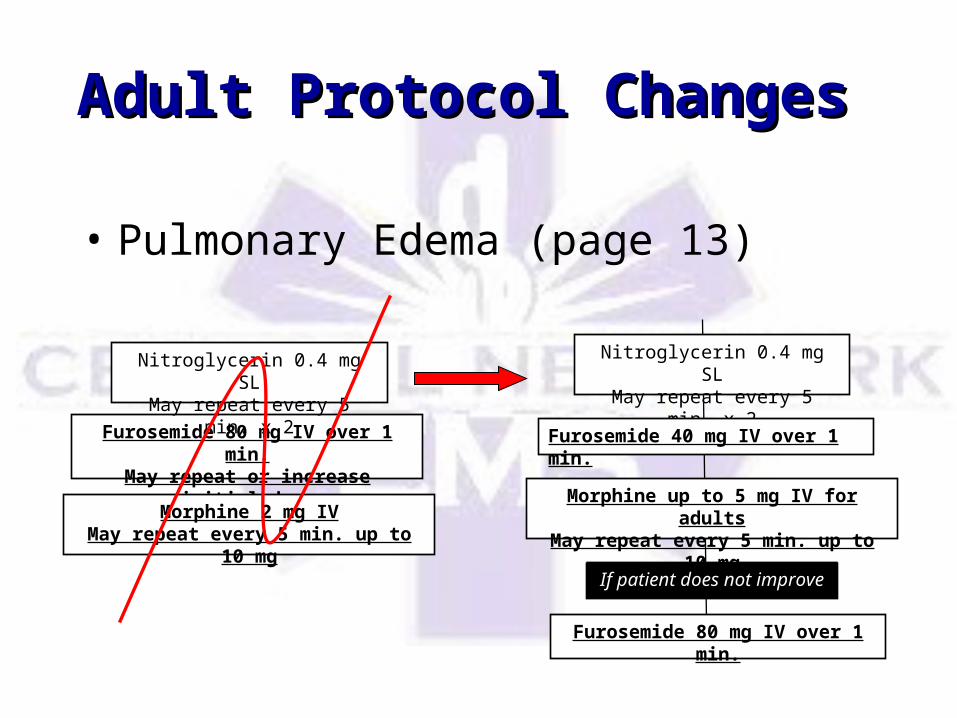
• Pulmonary Edema (page 13)
Furosemide 80 mg IV over 1 min.
May repeat or increase initial dose
Nitroglycerin 0.4 mg SLMay repeat every 5 min. x
2
Morphine 2 mg IVMay repeat every 5 min. up to 10
mg
Nitroglycerin 0.4 mg SLMay repeat every 5 min. x
2
Furosemide 40 mg IV over 1 min.
Morphine up to 5 mg IV for adults
May repeat every 5 min. up to 10 mg
Furosemide 80 mg IV over 1 min.
If patient does not improve

Adult Protocol ChangesAdult Protocol Changes
• Morphine initial dose change to range, still requires orders for all providers– “Up to 5 mg” for adults
• Pulmonary Edema (page 13)• Chest Pain (page 17)

Pediatric Protocol Pediatric Protocol ChangesChanges
• All pediatric protocols:– Use of Broselow Tape for adjunct
sizes and drug dosages is required.

Pediatric Protocol Pediatric Protocol ChangesChanges
• Acute Respiratory Distress– Atrovent 500 mcg in 2.5 milliliters
normal saline
Albuterol (2.5 mg in 3 ml NS) andAtrovent (500 micrograms in 2.5ml
NS)Administer via nebulizer*
Wheezing or history ofAsthma or Bronchiolitis
Albuterol 2.5 mg in 3 ml via nebulizer
orEpi 1:1000 0.01 mg/kg SC
to a total of 0.3 mgMay repeat in 20 min.
Pediatric Protocol Pediatric Protocol ChangesChanges
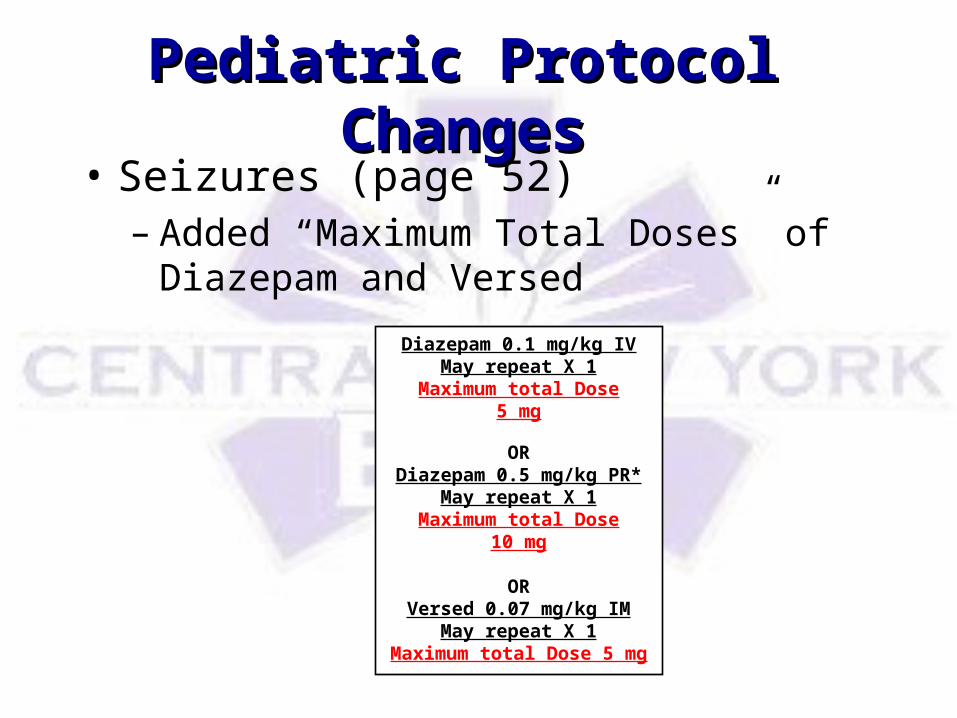
• Seizures (page 52)– Added “Maximum Total Doses” of
Diazepam and Versed
Diazepam 0.1 mg/kg IVMay repeat X 1
Maximum total Dose5 mg
ORDiazepam 0.5 mg/kg PR*
May repeat X 1Maximum total Dose
10 mg
ORVersed 0.07 mg/kg IM
May repeat X 1Maximum total Dose 5
mg

Special ProtocolsSpecial Protocols
• Trauma Triage Criteria added (page 64)
Major trauma is present if the mechanism of injury or patient’s physical findings meet any one of the following criteria:
Mechanism of Injury
- Death in the same passenger compartment- Fall >20 feet- Vehicle-pedestrian collision- Patient ejected from the vehicle- Vehicle collision >20 mph resulting in 12 inches of deformity to the vehicle- Vehicle rollover- Motorcycle crash- Vehicle vs. bicycle collision >5 mph
Physical Findings
- Pulse <50/min or >120/min- Systolic blood pressure of 90 mmHg or less- Respiratory rate <10/min or >28/min- Glasgow Coma Scale <14- Penetrating injuries of the trunk, head, neck, chest, abdomen or groin- Two or more proximal long bone fractures- Flail chest- Burns that involve 15% or more of the body surface or facial/airway burns- Combined system trauma that involves two or more body systems- Spinal cord injury or limb paralysis- Amputation (except digits)

Special ProtocolsSpecial Protocols
• 12 Lead EKG (page 65)
– Criteria– Frequency– Considerations for suspected MI– Reminders
ILateral
aVR V1Septal
V4Anterio
rIIInferior
AVLLateral
V2Septal
V5Lateral
IIIInferior
AVFInferior
V3Anterio
r
V6Lateral
V1 4th intercostal space @ R sternum edge
V2 4th intercostal space @ L sternum edge
V3 Between V2 & V4
V4 5th intercostal space, midclavicular line
V5 Level with V4, L anterior axillary line
V6 Level with V5, L mid axillary line

ChartsCharts
• Visual Analog Pain Scale (page 71)• This scale is designed to be used as a tool to
subjectively determine pain level. • Refer to the Pain — Non-Cardiac protocol (page
29)

ReviewReview
• Provider-friendlier format• Adult protocol changes to:
– Pain – Non-Cardiac – Facilitated Intubation– Allergic Reaction/Anaphylaxis– Pulmonary Edema– Chest Pain

ReviewReview
• Pediatric Protocol changes to:– Acute Respiratory Distress
• Special Protocol Additions:– Trauma Triage Criteria– 12 Lead EKG
• Charts Additions:– Visual Analog Pain Scale
EvaluationEvaluation• All ALS providers must successfully
complete the quiz in order to maintain ALS practicing privileges in Central New York. You will be directed from the next slide to take the test.
• Please evaluate this update. Login www.cnyems.org, and take the “evaluation questionnaire”.

Protocol Update TestsProtocol Update TestsClick appropriate link below to take test – you will be directed to login to your cnyems account in
an Internet browser. Login and proceed from there with the test. (You may have to close the
presentation).
Paramedic Protocol Update Test
Critical Care Protocol Update Test
Intermediate Protocol Update Test