2007 venezia, congresso mondiale, ablazione delle tachicardie ventricolari
TRANSCRIPT

Stefano Nardi MD, PhD
“ “SANTA MARIA” GENERAL HOSPITAL - TERNISANTA MARIA” GENERAL HOSPITAL - TERNI THORACIC SURGERY AND THORACIC SURGERY AND
CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOGIC CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOGIC CENTER AND CARDIAC PACING UNIT CENTER AND CARDIAC PACING UNIT
Venice Arrhythmias ‘07Venice Arrhythmias ‘07
Mapping and Ablation of Mapping and Ablation of late post-ischemic late post-ischemic sustained Ventricular sustained Ventricular Tachycardias, guided by Tachycardias, guided by EnSite System.EnSite System.

Post-ischemic sustained VTsPost-ischemic sustained VTsHow does it work?

Methodology • Identification of protected isthmuses of conducting tissue related to slow conduction zone
• electrically (entrainment with concealed fusion)• anatomically (computer-assisted,3D-mapping)
RF lesion bridges between constraining barriers
Interventional TherapyPost-ischemic sustained VTsPost-ischemic sustained VTs

How can we approach ?How can we approach ?
MappingMapping• Point by pointPoint by point
• EP EP criteriacriteria
TrackingTracking• XrayXray
• CARTOCARTO• LocaLisaLocaLisa• NavXNavX• RPMRPM
• ICEICE
AblationAblation• ConventionalConventional
• 8 mm tip8 mm tip• Irrigated tipIrrigated tip• InvestigationalInvestigational(balloon, cryo...)(balloon, cryo...)- Framework for ablationFramework for ablation
- Mapping guidanceMapping guidance
- Anatomic localizationAnatomic localization
- Tagging of ablation sites- Tagging of ablation sites- Determine Determine catheter contactcatheter contact
- Improved Improved efficiency of efficiency of power deliverypower delivery
Post-ischemic sustained VTsPost-ischemic sustained VTs

EP drawbacks• High complex SUBSTRATE • Non-uniform distribution of MYOCARDIAL SCAR• Imprecise fluoro guidance in ISCHEMIC BORDER ZONE• Imprecise creation of contiguous lesions
Post-ischemic sustained VTsPost-ischemic sustained VTs
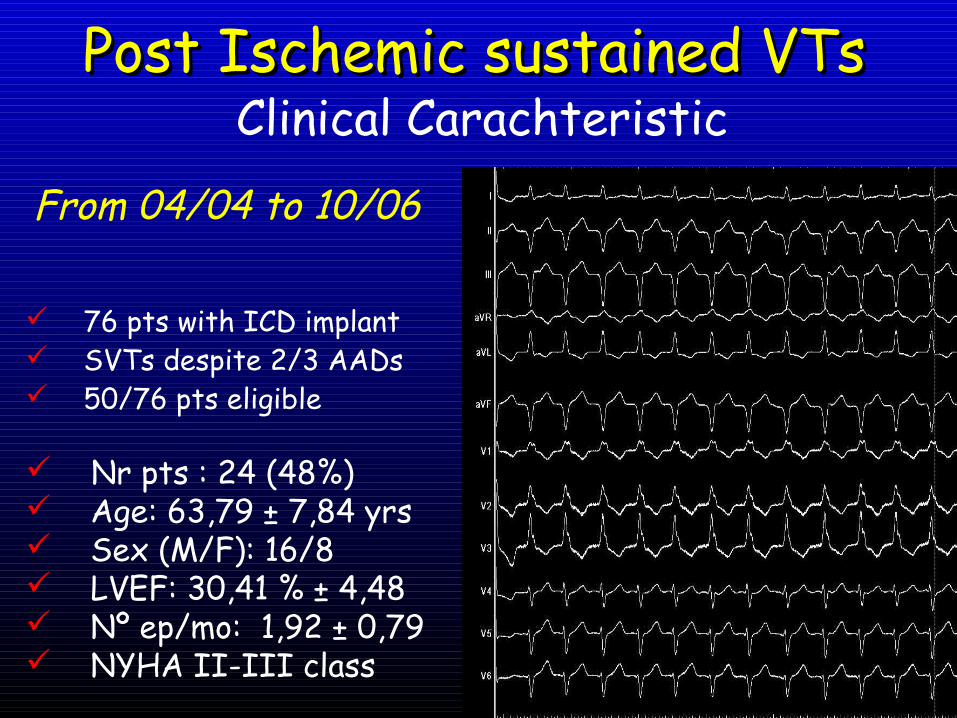
Clinical Carachteristic
Nr pts : 24 (48%) Age: 63,79 ± 7,84 yrs Sex (M/F): 16/8 LVEF: 30,41 % ± 4,48 Nº ep/mo: 1,92 ± 0,79 NYHA II-III class
Post Ischemic sustained VTsPost Ischemic sustained VTs
76 pts with ICD implant SVTs despite 2/3 AADs 50/76 pts eligible
From 04/04 to 10/06

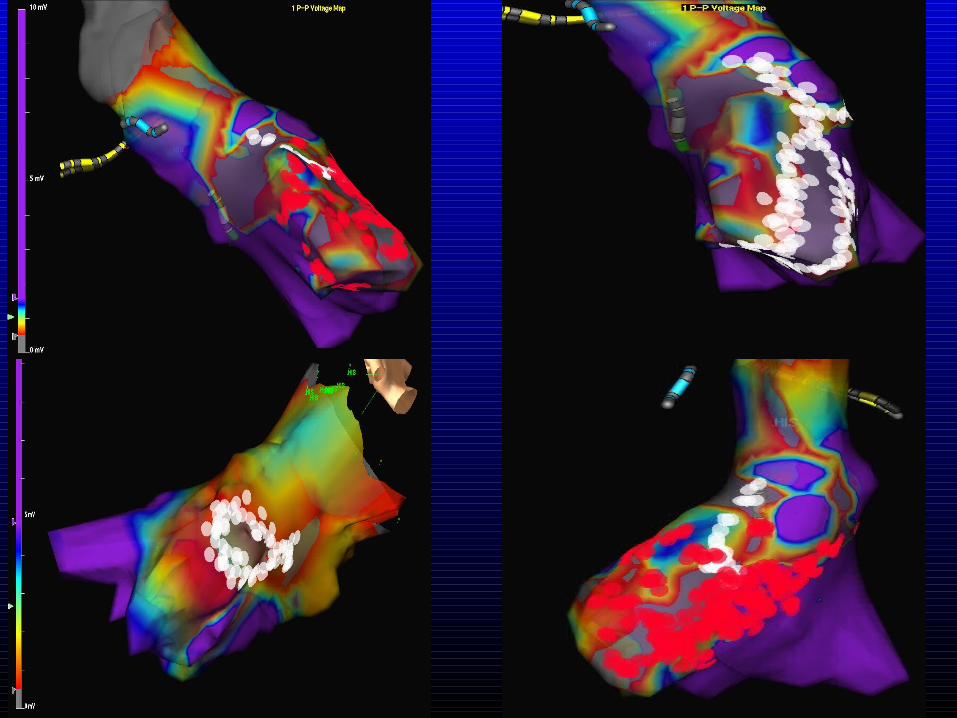
- CREATE a virtual geometry of LV chamber- IDENTIFY the target zone of each SVT (low-voltage zone, diastolic potentials, scar)- DESCRIBING the EA and EP characteristics of the
substrate- EVALUATE the efficacy of RF lesions at the identified critical isthmus- DEMONSTRATE with post-RF EP study the non-inducibility of SVTs.
operative end pointsoperative end pointsPost-ischemic sustained VTsPost-ischemic sustained VTs

Post Ischemic sustained VTsPost Ischemic sustained VTsResults

Post-ischemic sustained VTsPost-ischemic sustained VTsResults

RFCA consisted in a series of contiguous CTR RF guided by EA activation map and EP criteria of atrial potentials
Post Ischemic sustained VTsPost Ischemic sustained VTs

• Procedure (min): 148±26 144±24 151± 29
Global SR VT
• Fluoroscopy (min): 59±17 58±16 66±19
• Mapping (min): 35±8 33±9 38±4
• Pulses of RF: 34±16 28±17 41±19
Post Ischemic sustained VTsPost Ischemic sustained VTsResults

Procedure (min): 148±26
Fluoroscopy (min): 59±17
Mapping (min):
35±8 Nr. Pulses
of RF: 37±1624/27 SVTs operative mechanism (88%)
Acute EfficacyAcute Efficacy
24/27 SVTs (85%)24/27 SVTs (85%)
InefficacyInefficacy
4/27 SVTs (15%)4/27 SVTs (15%)
Post Ischemic sustained VTsPost Ischemic sustained VTsResults
After mean FU of 13,4±6,7 18/20 pts free SVTs

Post Ischemic sustained VTsPost Ischemic sustained VTsAblation

Post Ischemic sustained VTsPost Ischemic sustained VTsAblation
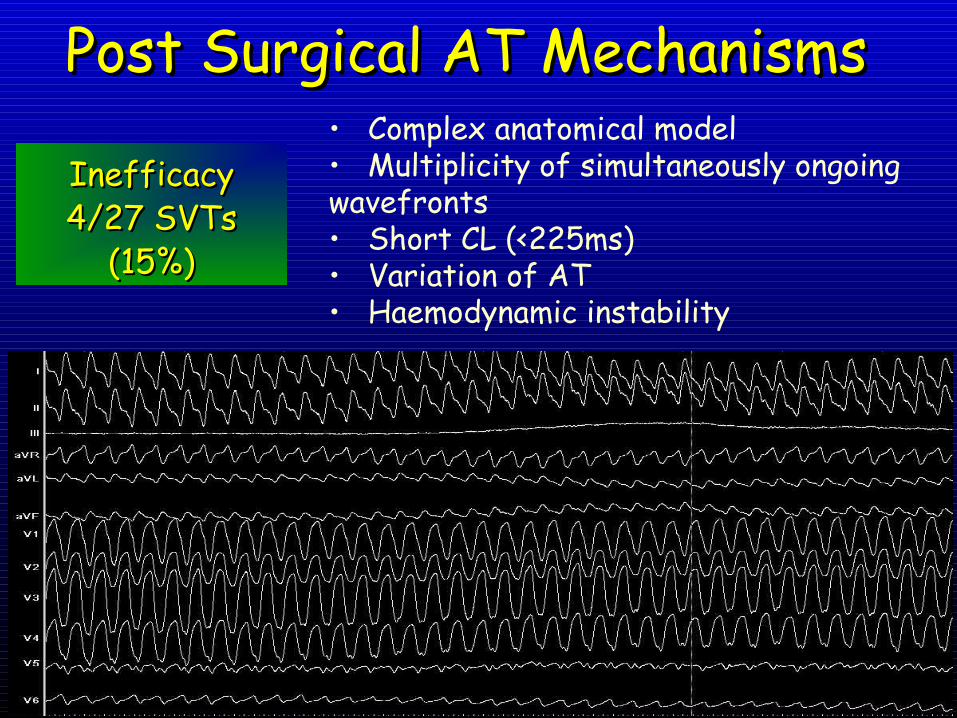
Post Surgical AT MechanismsPost Surgical AT Mechanisms• Complex anatomical model• Multiplicity of simultaneously ongoing wavefronts• Short CL (<225ms)• Variation of AT• Haemodynamic instability
Inefficacy Inefficacy 4/27 SVTs 4/27 SVTs
(15%)(15%)

POTENTIAL SUBSTRATES
How does it work?Post-ischemic sustained VTsPost-ischemic sustained VTs

Conclusions (1)Conclusions (1)• Conventional EP mapping
it’s not always appropriate strategies for SVTs
ablation because it provides very limited understanding of these complex arrhythmias which
are highly variable from one pt to the other.
• The main drawback of a pure EP approach is that the identification of all putative “endpoint” could be extremely difficult to achieve.

Post-ischemic sustained VTsPost-ischemic sustained VTs
• The implemented use of virtual geometry and a combined approach of EP with EA criteria is able to allow us a realistic 3D reconstruction of LV
• An individually tailored approach is needed
• A combined approach may be useful in the treatment of pts where RFCA is
primarily both EP and EAbased.

What is success?
• Complete freedom of VF, off drug RX?• No symptoms, but drug Rx required?• Dramatic decrease in symptoms, but AADs
still required?• QoL• How do we detect asymptomatic episodes?• Anticoagulation ………………...?
QUESTIONSQUESTIONS

Post Ischemic sustained VTsPost Ischemic sustained VTs

Post Ischemic sustained VTsPost Ischemic sustained VTs

- Related to the slow conductionregions located in the MI region or at the border zone
Post-ischemic sustained VTsPost-ischemic sustained VTs
- Macro-reentry is the most frequent mechanism
- Larger is the area of tissue infarted larger is the probability of potential reentrant circuits
How does it work?







