20071025 understanding the ub04 clean claim process program i.pdf · 1 hfma october 25,2007...
TRANSCRIPT

1
HFMAHFMAOctober 25,2007October 25,2007
Understanding the Understanding the UB04 Clean Claim UB04 Clean Claim
ProcessProcess
UB04UB04Presented byPresented byCarol D. EatonCarol D. Eaton
Citrus Valley Health PartnersCitrus Valley Health Partners
2
Hospital Billing 101+UB04Hospital Billing 101+UB04AgendaAgenda
RegistrationCharge Description Master(CDM)Coding/Claim CreationHIPAA Electronic Transaction ProcessUB04 Billing PreparationUB04 CMS-1450 Billing ProcessBilling InformationWebsitesQuality Improvements
3
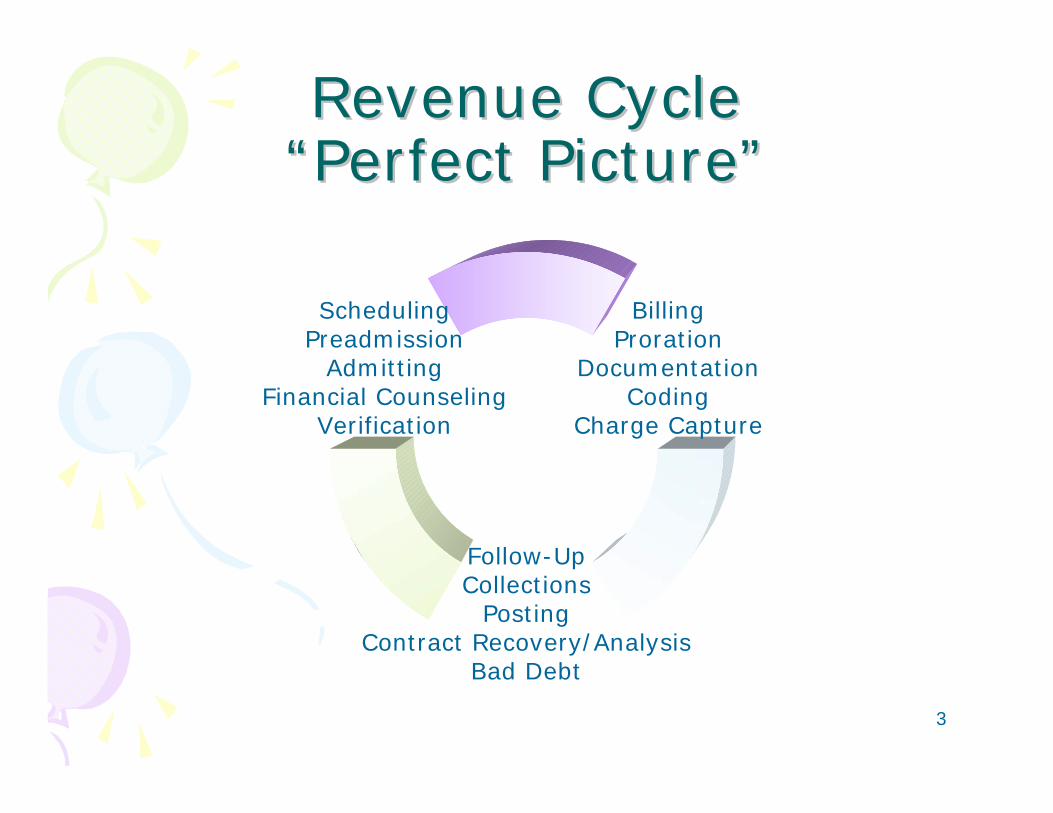
Revenue Cycle Revenue Cycle ““Perfect PicturePerfect Picture””
BillingProration
DocumentationCoding
Charge Capture
Follow-UpCollections
PostingContract Recovery/Analysis
Bad Debt
SchedulingPreadmission
AdmittingFinancial Counseling
Verification
4
Section:Section:Registration ProcessRegistration Process
Scheduling: Target for improvement. Look at the number of departments and patients that can be scheduled or prescheduled.Pre-registration & registration: Improve your pre-registration to improve the time needed to create a clean registrations. Eligibility & Authorization/Certification: Use electronic sources to obtain. Work with your area IPAs to communicate authorizations ahead of time. Assure services match certification / authorizationCollecting Co-payments & deductibles: The more you collect and notify upfront, the better chance you have at collecting at all. Payment arrangements also can be made. Published messages or pre-registration & verification.Screening for Medical Necessity & Covered Services: Create the best system for obtaining LMRP/NCD information for Medicare patients. ABNs. Work with Utilization Review or Nursing departments to assure appropriate admissions
5
Section:Section:Registration ProcessRegistration Process
Training must include:
Corporate Compliance: Reporting, accuracy of admit/dischg coding, charity and discount guidelinesInsurance eligibility, certification, authorization, matrix payer informationMedicare: (ABN) Advanced beneficiary notice, (MSP) Medicare Secondary Payer, 3 day window rules, 1 day stay & re-admission rules, Observation requirements, Important Message for Medicare (letter), Condition of Admissions formsHIPAA:(Health Insurance Portability Accountability Act of 1996, Privacy vs Security. (Electronic/Passwords, verbal info, paper shredding). Never breach patient confidentiality.EMTALA: Emergency Medical Treatment Labor Act 1986Clear “patient friendly billing” communication with patients. Smile and maintain eye contact. Sit & stand tall. Voice toneJob Description, manuals, departmental tour (timecard, vacation, attendance, dress code, name tag, HIPAA waste disposal, overtime, tardiness, switching, holidays)
6
Section:Section:Registration ProcessRegistration Process
HEALTH PLAN ADDRESSES(Use for NPI news)Sign up for Passwords and ID#s, make lists available to the staff involved:
AETNA www.aetna.comBLUECROSS http://provideraccess.bluecrossca.comBLUE SHIELD www.mylifepath.comCIGNA www.cignaforhcp.comCBCA ADMINISTRATOR www.cbca.com/login.pageFIRST HEALTH www.firsthealth.comHEALTHNET www.healthnet.comINTER VALLEY www.ivhp.comMEDPOINT MGMT-HLA www.medpointmanagement.comPHYSICIANS ASSOC www.physicianassoc.comPACIFICARE/SECURE HORIZONS www.pacificare.comUNITED HEALTHCARE www.unitedhealthcareonline.comUNIVERSAL CARE www.universalcare.com
7
Section:Section:Registration ProcessRegistration Process
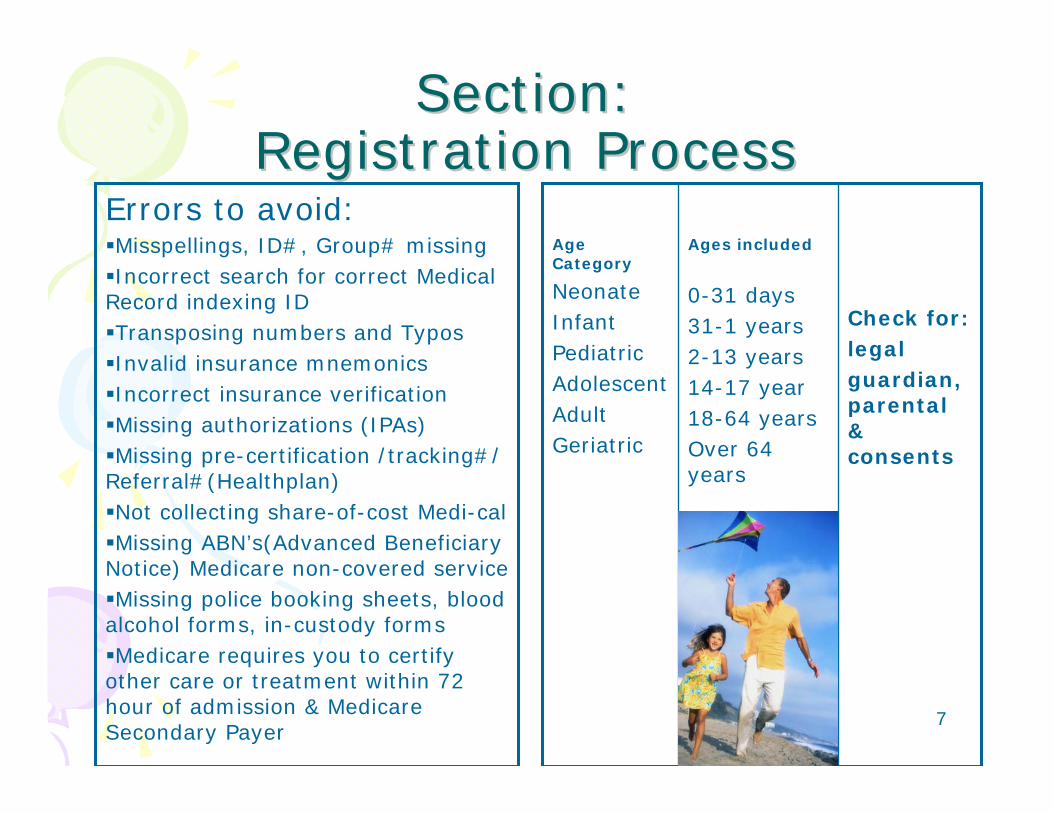
Errors to avoid:Misspellings, ID#, Group# missingIncorrect search for correct Medical
Record indexing IDTransposing numbers and TyposInvalid insurance mnemonicsIncorrect insurance verificationMissing authorizations (IPAs)Missing pre-certification /tracking#/
Referral#(Healthplan)Not collecting share-of-cost Medi-calMissing ABN’s(Advanced Beneficiary
Notice) Medicare non-covered serviceMissing police booking sheets, blood
alcohol forms, in-custody formsMedicare requires you to certify
other care or treatment within 72 hour of admission & Medicare Secondary Payer
Check for:legalguardian, parental & consents
Ages included
0-31 days31-1 years2-13 years14-17 year18-64 yearsOver 64 years
Age Category
NeonateInfantPediatricAdolescentAdultGeriatric
8
Section:Section:Charge Master ProcessCharge Master Process
Conduct annual charge master reviewsUpdates should be quarterly or as often as changes are receivedAssure that computer order entry is connected to each charge in the specific departments matches the CDM. Review charging tickets frequentlyDepartmental involvement with charge protocols created includingCCI editsDevelop departmental daily revenue master logs to review for accuracy and assure quality of systemsTeam approach to charge master changes should include accounting, HIM,IS, PFS, specific department managementPeriodic review of all coding on claims by third party to check your internal review processingReview ordering practices and assure documentation is present and accurate to match billing claimsEducation to all staff of changes, charge protocols, Federal payer documents as they arrive. System capture of requests, changes, audits and educationMake sure the claim editor, billing staff or claim vendors are not changing your claim without you know exactly what’s changed!
9
Section:Section:Charge Master ProcessCharge Master Process
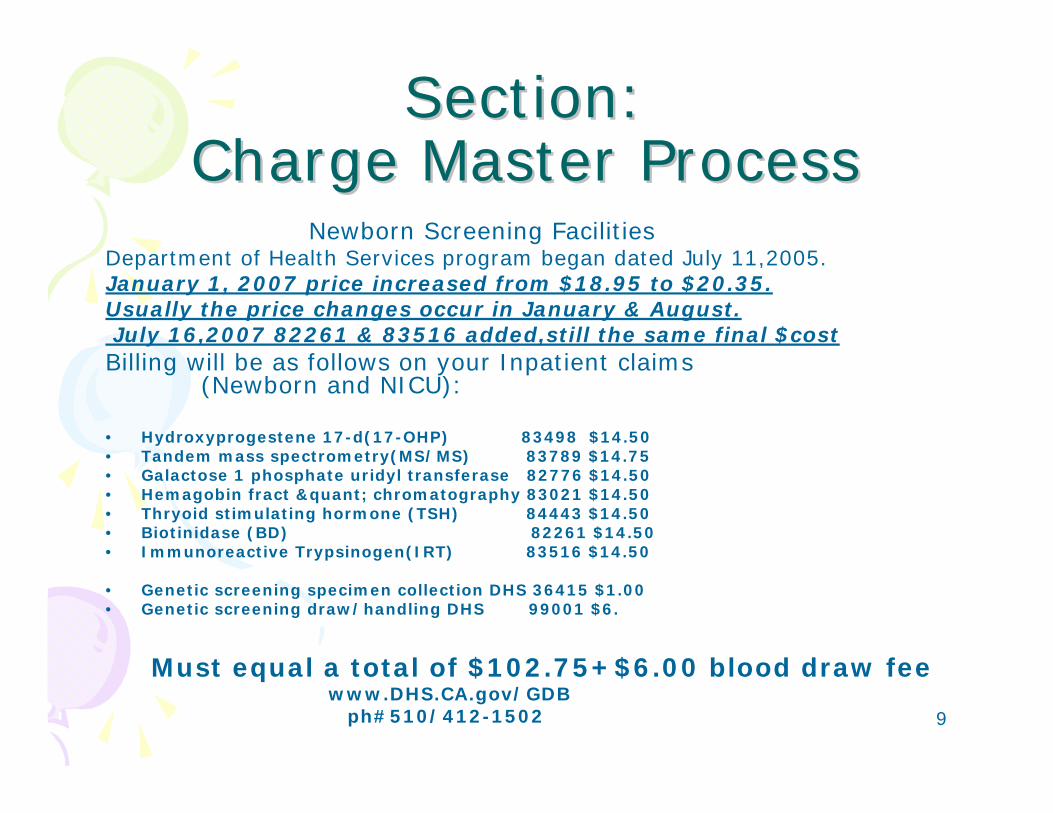
Newborn Screening Facilities Department of Health Services program began dated July 11,2005.January 1, 2007 price increased from $18.95 to $20.35.Usually the price changes occur in January & August.July 16,2007 82261 & 83516 added,still the same final $costBilling will be as follows on your Inpatient claims
(Newborn and NICU):
• Hydroxyprogestene 17-d(17-OHP) 83498 $14.50• Tandem mass spectrometry(MS/MS) 83789 $14.75• Galactose 1 phosphate uridyl transferase 82776 $14.50• Hemagobin fract &quant; chromatography 83021 $14.50• Thryoid stimulating hormone (TSH) 84443 $14.50• Biotinidase (BD) 82261 $14.50• Immunoreactive Trypsinogen(IRT) 83516 $14.50
• Genetic screening specimen collection DHS 36415 $1.00• Genetic screening draw/handling DHS 99001 $6.
Must equal a total of $102.75+$6.00 blood draw feewww.DHS.CA.gov/GDB
ph#510/412-1502
10
Section:Charge Master Process
Revenue Code Assignment Reminder• CMS recommends the use of revenue codes that closely
define where the procedures are performed. Revenue codes involved:
036x Surgical,045x Emergency Room, 051x Clinic,075x GI• Surgical Procedures
10021-69990, 0008T, 0016T-0024T, 0027T 0033T-0040T, 0046T-0048T, 0050T-0056T, 0061T-0063T, 0071T, 0075T-0081T,
0084T, 0088T, 0090T-0100T, 0120T-0126T, 0133T, 0138T, 0141T-0143T
• Cardiovascular 92950-92961(Resp.& ER can’t both charge for the same encounter)
• Photodynamic therapy 96567, 96570-96571• Other services & procedures 99170, 99185-99186, G0127• Critical Care 99291-99292 Therapeutic 90782-90799
Device Coding• Effective April 1, 2005 OPPS require providers to code
device HCPCS even if many of the are status indicator “N”.• Devices are reported under RC 272,275,276,278,279.
11
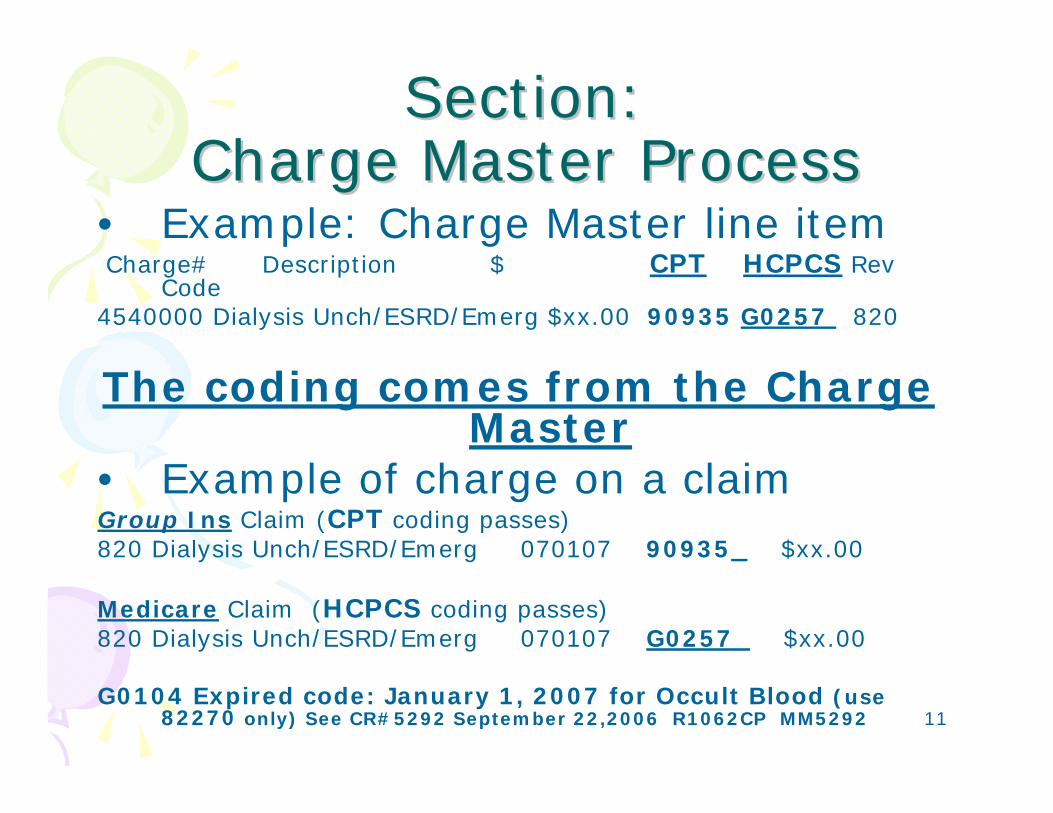
Section:Section:Charge Master ProcessCharge Master Process
• Example: Charge Master line itemCharge# Description $ CPT HCPCS Rev
Code4540000 Dialysis Unch/ESRD/Emerg $xx.00 90935 G0257 820
The coding comes from the Charge Master
• Example of charge on a claimGroup Ins Claim (CPT coding passes)820 Dialysis Unch/ESRD/Emerg 070107 90935 $xx.00
Medicare Claim (HCPCS coding passes)820 Dialysis Unch/ESRD/Emerg 070107 G0257 $xx.00
G0104 Expired code: January 1, 2007 for Occult Blood (use 82270 only) See CR#5292 September 22,2006 R1062CP MM5292
12
Section:Section:Coding/Claim CreationCoding/Claim Creation
ICD-9-CM – International Classification of Diseases 9th
Revision Clinical Modification
Volume 1 – Contains five appendices & Tabular list of codes including V codes (i.e.,426.6 Other heart block):
Appendix A: Morphology of Neoplasm'sAppendix B: Deleted effective October 1 of each yearAppendix C: Classification of Drugs by AMA and their ICD9CM equivalentsAppendix D: Classification of Industrial Accidents according to agency (i.e., external
causes: E828 Animal,riden)Appendix E: List of Three-Digit categories
Volume 2 – Diagnostic terms that are not in volume 1. Index to diseases includes most diagnostic terms in use.
Volume 3 – Operations and procedures. 2 digits with one or two digits following the decimal point. (i.e.,01.31 Incision. cerebral meninges)
For information on ICD-9-CM and POA information:MM5499 CR5499http://www.cms.hhs.gov/Transmittals/downloads/R1240CP.pdfhttp://www.cdc.gov/nchs/datawh/ftpserv/ftpicd9/icdguide06.pdfICD-10-CM is scheduled for October 2008
13
Section:Section:Coding/Claim CreationCoding/Claim Creation
CPT Level I- AMA’s physicians’ Current Procedural Terminology Often referred to as HCPCS by the federal government
payersEvaluation and Management (99201-99499)Anesthesiology (00100-01999, 99100-99140)Surgery (10021-69990)Radiology (including nuc.medicine, radiation onc., diagnostic ultrasound)(70010-79999)Pathology & Laboratory (80048-89356)Medicine (90281-99602)HCPCS Level II-National-Healthcare Common Procedure Coding
System. Broad spectrum of services and supplies from patient transport to ostomy supplies, from
chemotherapy drugs to durable medical equipment, and new technologies.(i.e.,G0103,J7030,Q3001)
Local Codes Level III-Specific State codes for Medicaid programs.
CPT & HCPCS level II Modifiers -Provides communication with payers to indicate altered by some special circumstance(s) but the code description itself has not changed.
**The existence of a procedure code does not imply coverage under any given insurance plan.**
14
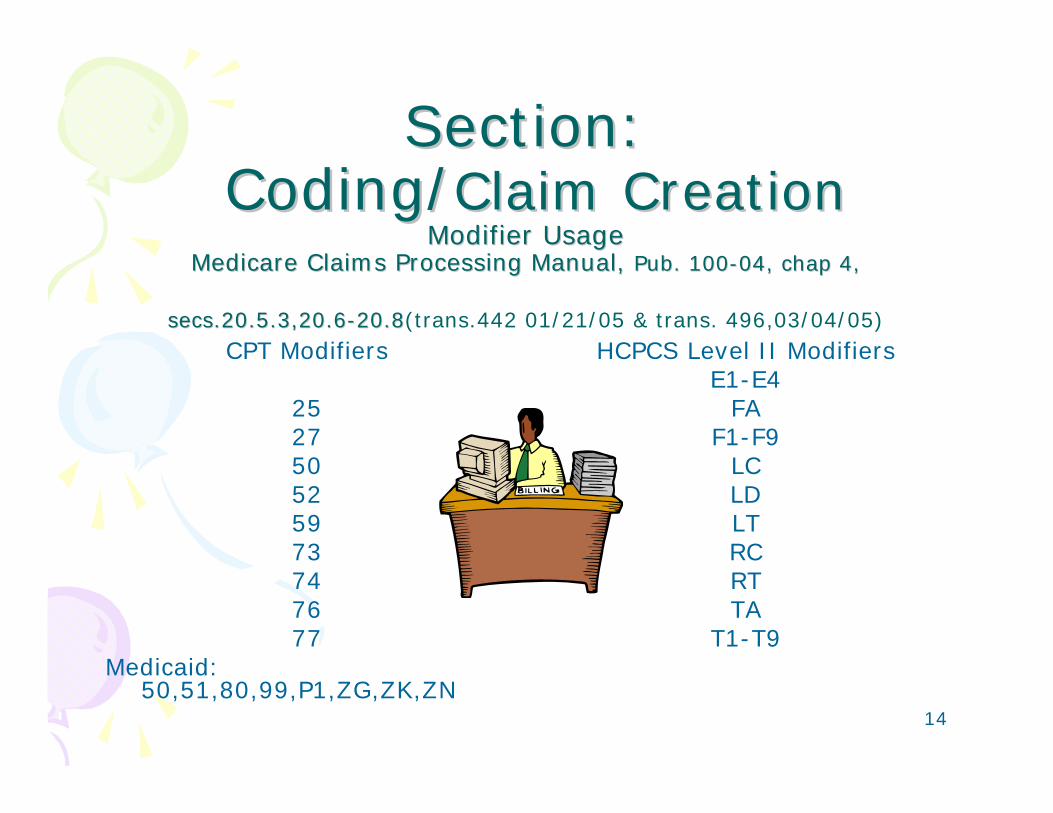
Section:Section:Coding/Coding/Claim CreationClaim Creation
Modifier UsageModifier UsageMedicare Claims Processing Manual, Medicare Claims Processing Manual, Pub. 100Pub. 100--04, chap 4, 04, chap 4,
secs.20.5.3,20.6secs.20.5.3,20.6--20.820.8(trans.442 01/21/05 & trans. 496,03/04/05)CPT Modifiers
252750 525973747677
Medicaid: 50,51,80,99,P1,ZG,ZK,ZN
HCPCS Level II ModifiersE1-E4
FAF1-F9
LCLDLTRCRTTA
T1-T9
15
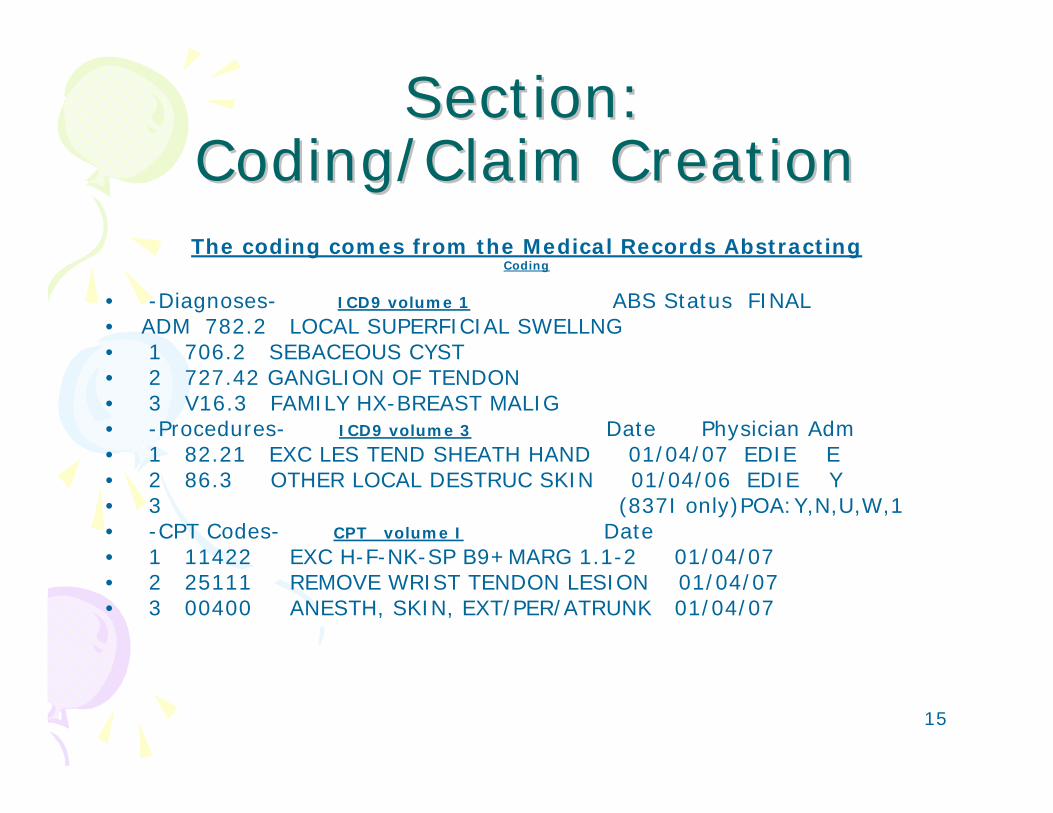
Section:Section:Coding/Claim CreationCoding/Claim CreationThe coding comes from the Medical Records Abstracting
Coding
• -Diagnoses- ICD9 volume 1 ABS Status FINAL• ADM 782.2 LOCAL SUPERFICIAL SWELLNG• 1 706.2 SEBACEOUS CYST• 2 727.42 GANGLION OF TENDON• 3 V16.3 FAMILY HX-BREAST MALIG• -Procedures- ICD9 volume 3 Date Physician Adm• 1 82.21 EXC LES TEND SHEATH HAND 01/04/07 EDIE E• 2 86.3 OTHER LOCAL DESTRUC SKIN 01/04/06 EDIE Y• 3 (837I only)POA:Y,N,U,W,1 • -CPT Codes- CPT volume I Date • 1 11422 EXC H-F-NK-SP B9+MARG 1.1-2 01/04/07• 2 25111 REMOVE WRIST TENDON LESION 01/04/07• 3 00400 ANESTH, SKIN, EXT/PER/ATRUNK 01/04/07
16
Section:Section:Coding/Claim CreationCoding/Claim Creation
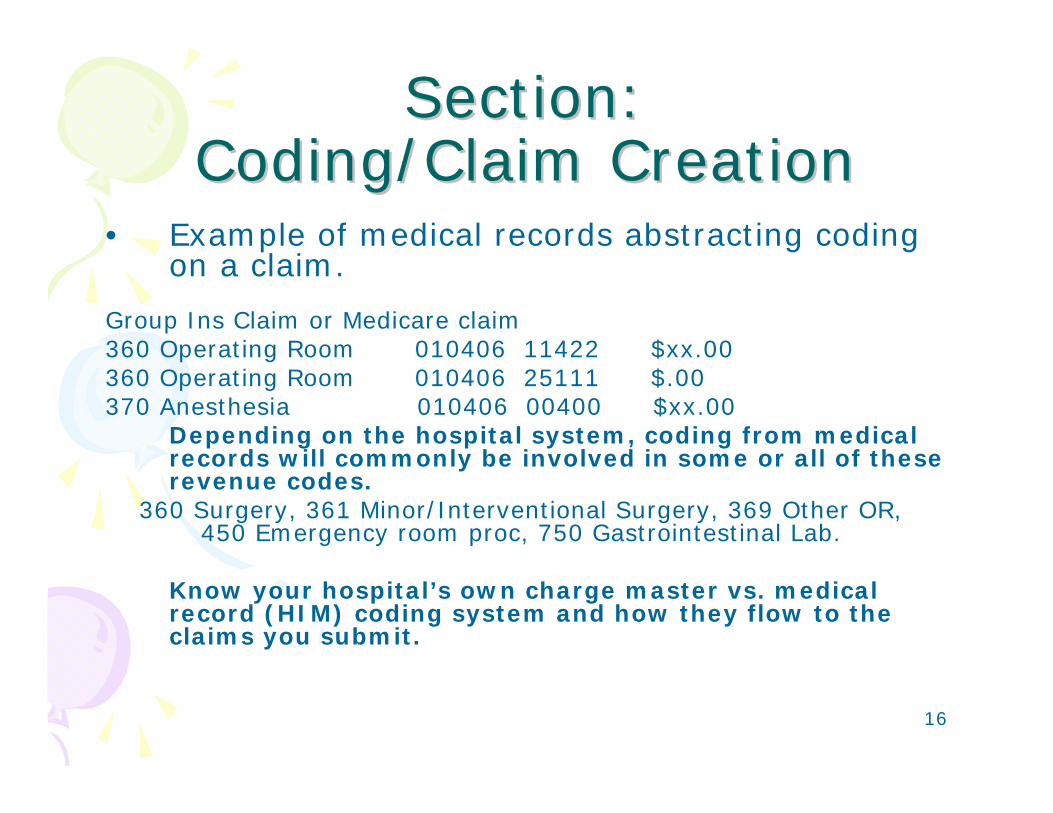
• Example of medical records abstracting coding on a claim.
Group Ins Claim or Medicare claim360 Operating Room 010406 11422 $xx.00 360 Operating Room 010406 25111 $.00370 Anesthesia 010406 00400 $xx.00
Depending on the hospital system, coding from medical records will commonly be involved in some or all of these revenue codes.
360 Surgery, 361 Minor/Interventional Surgery, 369 Other OR,450 Emergency room proc, 750 Gastrointestinal Lab.
Know your hospital’s own charge master vs. medical record (HIM) coding system and how they flow to the claims you submit.
17
Section:Section:Coding/Claim CreationCoding/Claim Creation
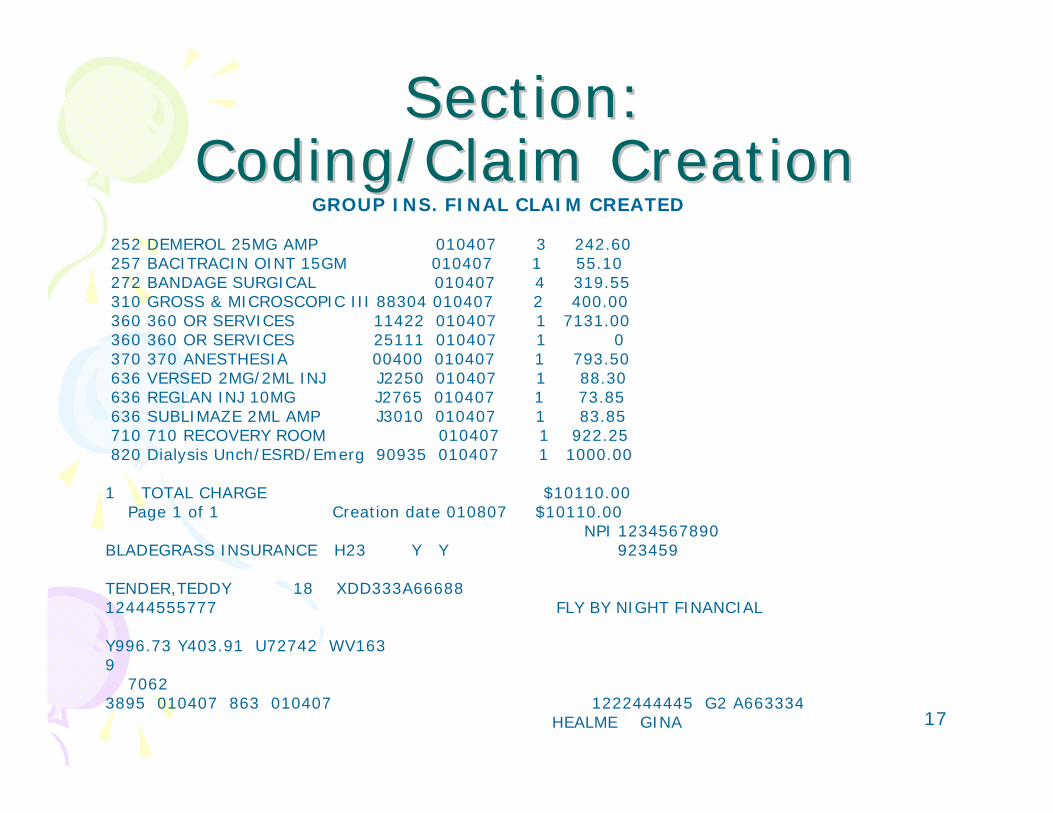
GROUP INS. FINAL CLAIM CREATED
252 DEMEROL 25MG AMP 010407 3 242.60257 BACITRACIN OINT 15GM 010407 1 55.10272 BANDAGE SURGICAL 010407 4 319.55310 GROSS & MICROSCOPIC III 88304 010407 2 400.00360 360 OR SERVICES 11422 010407 1 7131.00360 360 OR SERVICES 25111 010407 1 0 370 370 ANESTHESIA 00400 010407 1 793.50636 VERSED 2MG/2ML INJ J2250 010407 1 88.30636 REGLAN INJ 10MG J2765 010407 1 73.85636 SUBLIMAZE 2ML AMP J3010 010407 1 83.85710 710 RECOVERY ROOM 010407 1 922.25820 Dialysis Unch/ESRD/Emerg 90935 010407 1 1000.00
1 TOTAL CHARGE $10110.00Page 1 of 1 Creation date 010807 $10110.00
NPI 1234567890BLADEGRASS INSURANCE H23 Y Y 923459
TENDER,TEDDY 18 XDD333A66688 12444555777 FLY BY NIGHT FINANCIAL
Y996.73 Y403.91 U72742 WV163 9
70623895 010407 863 010407 1222444445 G2 A663334
HEALME GINA

18
HIPAAHIPAAElectronic Transaction ProcessElectronic Transaction Process
Claim/Encounter (837)Status Inquiry (276)
Status Response (277)Payment/Remittance (835)
Eligibility Inquiry (270)Eligibility Response (271)
UR Certification Request (278)UR Certification Response (278)
19
HIPAAHIPAAElectronic Transaction ProcessElectronic Transaction Process
270/271 Inquire and Receive Response providing health care eligibility or benefit information associated with a subscriber or dependent. 278 Inquire and Receive a response for the following from Utilization Review units:
Admission certification reviewReferral reviewHealth care services certificationExtend certification review
837 Institutional, Professional, Dental claim276/277 Claim Status Request/Response to obtain payer status (accepted/rejected, denied, approved and pending835 Claim Payment/Advice, Explanation of Benefits (EOB) submission to providers or other payers
20
Section:Section:Billing PreparationBilling PreparationUB04 CMSUB04 CMS--14501450
This section was developed to train you on specific FL-fields of the UB04 CMS-1450
Not all of the FLNot all of the FL--fields are in this text, only the fields that have heavy fields are in this text, only the fields that have heavy usage and need knowledge based trainingusage and need knowledge based training
For more information on the new forms UB04 CMS-1450
May 23,2007 Implementation(Transitional 3/1/07-5/22/07 CMS trans#1018 July 28, 2006)
National Standars Insti X12N 837 I Health care claim companion documenthttp://www.cms.hhs.gov/transmittals/downloads/R1116CP.pdf
Go to: http://www.nubc.org
New 1500 HICF X12N 837 (08/05)July 2, 2007 Implementation (Updated R1247CP)
http://www.cms.hhs.gov/transmittals/downloads/R899CP.pdfhttp://www.cms.hhs.gov/transmittals/downloads/R1247CP.pdf
Go to : http://www.nucc.org
21
Section:Section:Billing PreparationBilling PreparationUB04 CMSUB04 CMS--14501450
Transitional Evolution changes fromUB-92 to UB-04
• Pay-to-name and address (New FL02)• Patient name – ID (Update FL08)• Accident State (New F29)• Page_of_Creation date (New F43-F44)• Creation date (New FL45)• Identifiers – NPI National Provider Identifier (FL56,FL76-
FL79)• Principal diagnosis code required. (FL67 & other FL67A-Q)• Diagnosis indicator Field – Report if the diagnosis was
present on admission (FL69)• Patient’s Reason for Visit Code (FL 70A 70C)• PPS Code Field (New FL71)• External Cause of Injury Code (New FL72 1-E code only)• Code-Code Qual/Code/Value (New FL81)
22
Section:Section:Billing PreparationBilling PreparationUB04 CMSUB04 CMS--14501450
ModificationsUB-92 to UB-04
• Increase Type of Bill to 4 digits• Increase filed size for HCPCS/Rate/HIPPS Rate
codes-2 added modifier positions• Additional 3 Condition Code fields• Expanded diagnosis code field to prepare for ICD-
10-CM• Additional Occurrence Span Code field• Usage matrix created for Type of Bill• Current regulations and industry standards
restated on the back of the form
23
Section:Section:Billing PreparationBilling PreparationUB04 CMSUB04 CMS--14501450
CMS Related Publications/Articles
SE0608 – CMS Subpart Policy:http://www.cms.hhs.gov/MLNMattersArticles/Downloads/SE0608.pdfSE0659 - Guidance for Reporting NPI In Medicare claimshttp://www.cms.hhs.gov/MLNMattersArticles/downloads/SE0659.pdfMM4023- CMS policy for NPI-stage 2 implementation:http://www.cms.hhs.gov/MLNMattersArticles/downloads/MM4023.pdfMM5229 – Modification of NPI editing requirements of CR4023/MM4023http://www.cms.hhs.gov/MLNMattersArticles/downloads/MM5229.pdfMM5243 - R1024CP-Reporting Taxonomy Codes for Subpart NPI’shttp://www.cms.hhs.gov/MLNMattersArticles/downloads/MM5243.pdfCR5436 –Trans#1154 Healthcare Provider Taxonomy Codes Update
24
Section:Section:Billing PreparationBilling PreparationUB04 CMSUB04 CMS--14501450
CMS Related Publications/Articles continued
MM5072 – UB-04 Implementation:http://www.cms.hhs.gov/MLNMattersArticles/downloads/MM5072.pdfMM5081 revised – Stage 2 NPI Changes for 835 transactions:http://www.cms.hhs.gov/MLNMattersArticles/downloads/MM5081.pdfCR5318 Trans#183 Jan 24,2007- Update the MCS System to Validate NPI
in place of UPINCR4191 Trans#141 Feb 24,2006-Modification to the UPIN processCR5072 Trans#1104 Nov 3,2006-Uniform Billing (UB-04)
ImplementationSE0659-Important Guidance regarding NPI usage in Medicare claimsMM5499 / CR5499 – Present on Admission Indicator POAMM5378 Revised-Claims submitted with only a NPI during the Stage 2NPI
Transition PeriodMM5452 Trans#R1241CP Stage 3 NPI changes for transactions 835 & RA

25
Section:Section:Billing PreparationBilling PreparationUB04 CMSUB04 CMS--14501450
CMS Related Publications/Articles continued
MM5072 Revised-Uniform Billing (UB-04)Implementation-UB92 ReplacementMM5584-Discontinuance of the UPIN RegistryMM5411-Institutional Value Code ChangesFederal Register Vol.72 #103,Wed. May 30,2007 –HIPAA National Plan and
Provider Enumeration System Data DisseminationMLN SE0725 NPI Errors, using NPI on claims and 835 Remittance advices
changes http://www.cms.hhs.gov/MLNMattersArticles/downloads/SE0725.pdf
http://www.cms.hhs.gov/NationalProvIdentStand/06a_DataDissemination.asp
NPI REGISTRY SEARCH!!! Look up all your Individual or Organizational Providerhttps://nppes.cms.hhs.gov CLICK on REGISTRY SEARCH
CMS Related Publications/Articles CMS1500 08-05MM5060 - CMS1500 08-05 Implementationhttp://www.cms.hhs.gov/MLNMattersArticles/downloads/MM5060.pdfMedi-Cal website to Register NPI(s) MEDI-CAL will still require Provider#!!!!!!!! http://files.medical.ca.gov/pubsdoco/npi/articles/npi_8806.asp
26
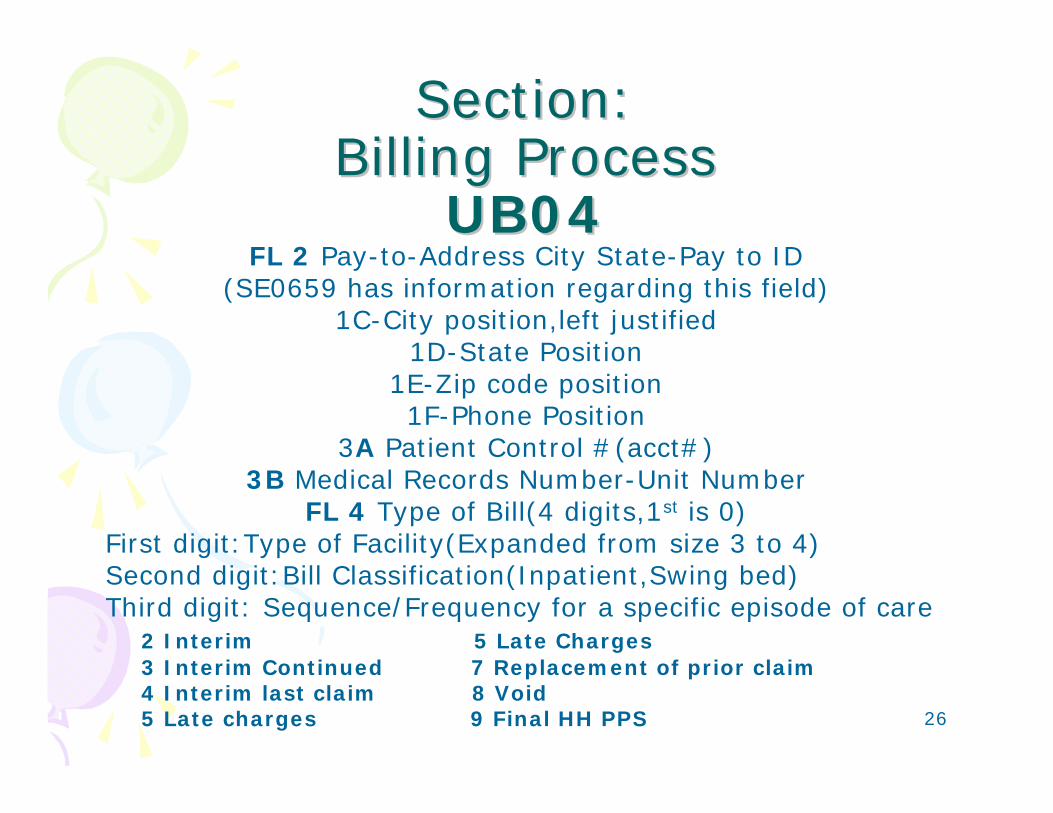
Section:Section:Billing ProcessBilling Process
UB04UB04FL 2 Pay-to-Address City State-Pay to ID
(SE0659 has information regarding this field)1C-City position,left justified
1D-State Position1E-Zip code position1F-Phone Position
3A Patient Control #(acct#)3B Medical Records Number-Unit Number
FL 4 Type of Bill(4 digits,1st is 0)First digit:Type of Facility(Expanded from size 3 to 4)Second digit:Bill Classification(Inpatient,Swing bed)Third digit: Sequence/Frequency for a specific episode of care
2 Interim 5 Late Charges3 Interim Continued 7 Replacement of prior claim4 Interim last claim 8 Void5 Late charges 9 Final HH PPS
27
Section:Section:Billing ProcessBilling Process
UB04UB04FL 4 ContinuedCommon Examples:11x Hospital Inpatient 12x Hospital Inpatient (Medicare Part B
Only)13x Hospital Outpatient21x Skilled Nursing Inpatient (Including
Medicare Part A)DISCONTINUED Medicare 10/01/05: 17x.
24x, 27x, and 5xx
28
Section:Section:Billing ProcessBilling Process
FL 6 Statement Covers Period• Report the beginning and ending dates of
service for the entire period reflected on the bill.
• Outpatient hospital claims where the from and through dates are equal and a HCPCS
code is reported, a line-item date of service must be reported also in FL45.
• SNF inpatient claims must equal the total units reported in FL46 for accommodation.
29
Section:Section:Billing ProcessBilling Process
FL7 Unlabeled(UB92 FL7 Replace w/ Value code 80)
”Medicare Covered Days”FL8 Patient Name & ID(8a) UB92 FL 8
Replace w/Value code 81)FL8(a)=Patient Identifier-Patients
insurance policy numberFL9 Street, City, State, Zip &
Country(outside USA)Code (UB92 FL 9 Replace w/Value code 81)
FL10 Patient Birthdate(UB92 FL10 Replace w/Value code 83)
30
Section:Section:Billing ProcessBilling Process
FL11 Patient SexOld: FL08,09,10 replaced=value codes
Marital status has been eliminatedFL12 Admission DateFL13 Admission Hour
FL14 Type of Admission /Visit (old FL19)1 Emergency2 Urgent3 Elective4 Newborn5 Trauma9 Info not available
Note: Date of death can not be changed by Medicare Intermediaries/Carriers. Death certificates must be sent with a
request directly to the Social Security Administration office.
31
Section:Section:Billing ProcessBilling Process
FL15 Source of Admission(Reorganized to focus on patients’ place or point of origin rather than source of physician order or referral)
1 Physician Referral2 Clinic Referral3 HMO Referral (Discontinued 10/01/07)4 Transfer from a hospital (Different facility)5 Transfer from a SNF-Skilled Nursing or ICF-Intermediary Care Facility6 Transfer from Another Health Care Facility7 Emergency Room8 Court/law enforcementA Transfer from a Critical Access Hospital (Discontinued 10/1/07)B Transfer from Another HHAC Readmission to same HHAD Transfer from one Dist.Unit of the Hospital to Another Distinct unit,
(resulting in a separate claim to the payer)E Transfer from Ambulatory Surgery CenterF Transfer from Hospice under Plan of Care or enrolled in Hospice ProgramADDITIONAL FL Coding Structure: NEWBORN1 Normal Delivery (Normal) (Discontinued 10/01/07)2 Premature Delivery (Premie) (Discontinued 10/01/07)3 Sick baby (Sick) (Discontinued 10/01/07)4 Extramural Birth (Born in non-sterile envirn.)(Discont.10/01/07)5 Born inside the Hospital (NEW 10/01/07)6 Born outside the Hospital (NEW 10/01/07)9 Unknown
32
Section:Section:Billing ProcessBilling Process
FL 17 Patient StatusHospitals are responsible for ensuring that patient status codes are
accurate. This is an OIG audit target for PPS reimbursement
01 Discharged to Home or Self-Care02 Discharged/Transferred to a Short-Term General Hospital for
Inpatient Care03 Discharged/Transferred to SNF w/Medicare Certification (TCU)04 Discharged/Transferred to an Intermediate Care Facility (ICF)05 Discharged/Transferred to a Non-Medicare PPS Children’s hospital or
PPS Cancer Hospital for Inpatient Care06 Discharged/Transferred to Home under Care of organized Home
Health Service Organization in anticipation of covered skilled careCode when patient is disch/transf to home with a written plan of care for home care services. Not used for HHA provided by a DME supplier or from a home IV provider for Home IV services. See also condition 42 or 43
07 Left against Medical Advice or Discontinued Care08 (Discontinued 10/1/05)09 Admitted as an Inpatient to this hospital
33
Section:Section:Billing ProcessBilling Process
FL17 Patient Status- Continued20 Expired (*accepted by Medi-Cal)30 Still a Patient40 Expired at home41 Expired in a Medical Facility such as a hospital, SNF,ICF or Free
standing hospice (TOB 81x,82x)42 Expired, Place Unknown (TOB 81x, 82x)43 Discharged/Transferred to a Federal Health Care Facility (VA,
Dept Of Defense Hospital)61 Discharged/Transferred within this institution to a Hospital-Based
Medicare Approved Swing Bed62 Discharge/Transferred to an Inpatient Rehabilitation Facility (IRF)
Including Rehab. Distinct part units of a hospital63 Discharged/Transferred to a Medicare Certified Long Term Care
Hospital (LTCH)64 Discharged/Transferred to a Nursing Facility Certified Under
Medicaid but not certified under Medicare65 Discharged/Transferred to a Psychiatric Hospital or Psychiatric
Distinct Part Unit of a Hospital
34
Section:Section:Billing ProcessBilling Process
FL18-28 Conditions (FL 26,27,28 New condition codes):
The codes communicate to the payer employment and eligibility conditions that affect the claims processing
Examples:01 Military service related02 Condition is employment related06 ESRD patient in first 18 months of entitlement
covered by employer group health insuranceSpecial Conditions:09 Neither patient nor spouse is employed (MSP)17 Homeless18 Maiden Name Retained19 Child Retains Mother’s Name20 Beneficiary requested billing ”Demand”44 Inpatient Admission Changed to Outpatient
(documentation & physician agreement is required before before billing)
35
Section:Section:Billing ProcessBilling Process
FL18-28 Conditions:49 Product replacement within product lifecycle
(Nov 4, 2005 MM4058 CR 4058) *CMS to track costs
50 Product replacement for know recall of product (Nov 4, 2005 MM4058 CR 4058) *CMS to track costs
GO Multiple ER visits occur on the same day (see modifiers 25,27)
Claims reviewed by QIO or QIC with denial or preauthorization see codes: C3-C7
in Transmittal 632 July 29,2005 Effective 01/03/06,after service dates 07/01/05
Medicaid claims:81 Emergency certification A1 EPSDT/CHDPA4 Family Planning AI
Sterilization/Consent Form(PM330)• There are many codes under this section, refer to the
UB92-UB04 manual
36
Section:Section:Billing ProcessBilling Process
FL 29 Accident State FL31-36
31A= A1-Ins 1 subscriber birth date32A= B1 Ins 2 subscriber birth date33A= C1 Ins 3 subscriber birth date
Occurrence & Dates: The codes & dates communicate to the payer specific events to determine
liability and coordinate benefits that will affect the claims processing
Examples:01 Accident/Medical coverage w/date of accident06 Crime Victim10 Last Menstrual Period (Maternity related condition claims)11 Onset of symptoms or exacerbation/illness w/date treatment started(Rev
codes: 041x,042x,043x,044x,0943)27 Date of Hospice certification or recertification35 Date Treatment Started for Physical Therapy44 Date Treatment Started for Occupational Therapy45 Date Treatment Started for Speech Therapy46 Date Treatment Started for Cardiac Rehab
37
Section:Section:Billing ProcessBilling Process
FL35-36Occurrence Span codes & Dates:
(2 new Occurrence Span codes)The codes & dates communicate to the payer specific events
that SPAN over time to coordinate benefits that will affect the claims processing
Examples:70 Qualifying stay dates for SNF(3 day hospital that qualifies
the patient for Medicare SNF)72 Actual dates of the first and last outpatient services visit (if
dates in FL6 are different)FL38
Responsible Party (for the bill) Name and Address
38
Section:Section:Billing ProcessBilling Process
FL39-41Value codes & Amounts:
The codes & amounts communicate specific codes and related monetary amounts that will affect the claims processing
Examples:01 Most common semi-private room rate,$$$02 Hospital has no semi-private rooms (0.00)12 Working aged beneficiary/spouse with EGHP, $$$13 ESRD Beneficiary in Medicare Coordination Period w/EGHP14 No-Fault, Including auth/other15 Work Compensation,$$$41 Black Lung (BL)42 Veterans Affairs (VA)43 Disabled Beneficiary Under Age 65 w/LGHP45 Accident Hour(non Medicare) 2pm=14 00 in cents
39
Section:Section:Billing ProcessBilling Process
FL39-41Value codes & Amounts:
50 Physical Therapy Visits (# from onset from billing provider through this billing period)
51 Occupation Therapy Visits “52 Speech Therapy Visits “53 Cardiac Rehabilitation Visits “54 Newborn birth weight in grams55 Eligibility Threshold for Charity Care68 EPO Drug-Amount reflect the #EPO units admin or supplied69 State Charity Care Percent - Amount reflect the % of
charity care eligibility for the patient75-79 These codes are set aside for payer use ONLY80 Covered Days 81-Noncov.Days 82-Co-ins Days 83-LTRA4-A6 Self-Administrable Drug codes to support revenue 0637July 1,2007 A1,A2,A7,B1,B2,B7,C1,C2,C7 now restricted to
paper claims only,no longer X12N 837 Insti.claims MM5411
40
Section:Section:Billing ProcessBilling Process
FL42Revenue Codes
There are 22 lines available on a single UB-04 claim form to list revenue codes and charges. The codes consist of 4 digits. Many systems drop the first digit from paper claims. Each facility must decide to program these codes with either a “General” revenue code (ending in 0) OR “Detail” revenue code (ending in 1-9 as appropriate).
Example:250 “General” Pharmacy
251-259 “Detail” PharmacyIn most cases it is to your advantage to code detail for Medicare and
Payer requirements. Accuracy is important to your facilities cost reporting. Avoid manual changes to your claims.
Under Home Health PPS one revenue code line is used for the request for anticipated payment (RAP) The line is used to report the Health
Insurance Prospective Payment System (HIPPS) code(FL44)
Certain revenue codes are contracted with payer to pay with invoice or requisition forms. 278 Implants, 636 Specifically coded drugs
This requires some step by step review by your facility to ease the process for the billing staff to deal with the carve-out contract
requirements
41
Section:Section:Billing ProcessBilling Process
FL42 FL42 Revenue CodesRevenue Codes
CommonCommon
0001 Total Charges002X HIPPS PPS codes-Subcategory2 Skilled Nursing Facility (TCU) SNF PPS(RUG)3 Home Health PPS HHS PPS (HRG)4 Inpatient Rehabilitation PPS IRF PPS (CMG)
01XX&02xx Room & Board charges
025x Pharmacy027x Supplies03xx Lab032x Radiology Diagnostic033x Radiology Therapeutic034x Nuclear Medicine0343 Diagnostic Radiopharm.0344 Therapeutic Radiopharm.035x CT Scan036x Surgery037x Anesthesia
041x Respiratory042x Physical Therapy043x Occupational Therapy044x Speech-LanguagePathology045x Emergency Room046x Pulmonary Function048x Cardiology049 Ambulatory Surgical Care061x MRI063x Pharmacy(HCPCS required)072x Labor Room/Delivery073x EKG/ECG075x Gastro-Intestinal Services076x Treatment or Observation080x Inpatient Renal Dialysis092x Other Diagnostic Services
42
Section:Section:Billing ProcessBilling Process
FL43 - 44 Page__of __Creation Date *NEW*
FL44 Rates/HIPPS/HCPCS-CPT Codes(Expanded to 4 modifiers =14 digits)
Almost all revenue codes require a HCPCS/CPT code. This field is to report appropriate codes for the service performed. Some payers have edits that will require a specific “detail” revenue code for a specific HCPCS/CPT
• This field is also for reporting Room and Board Rates
• RC 0022=Skilled Nursing Facility HIPPS Rate/RUG code• RC 0023=Home Health HHPPS Rate/HRG code• RC 0024=Inpatient Rehab.Facility IRF HIPPS Rate/CMG code
• NDC-National Drug Code #s(11 digits) for specific drugs (See Federal Register Feb 20,2003 Vol.68,number 34 Page 8381-8399) No standard code set at this time for non-retail. Trading partners must carefully make agreements. Medicare requires NDC# with the use of C9399 newly approved FDA drugs/ biologicals. CDHS (Calif.Dept.Health Services) is in the process of discussions with providers regarding the implementation of NDC’s on Medi-cal claims. CalHospitalAssociation-Sherreta Lane is working on a provider communication panel.
43
Section:Section:Billing ProcessBilling Process
FL 45 Service Date – Creation DateRequired Outpatient
Report line item dates of service on all bills containing revenue codes, procedure codes or drug codes. This includes claims where the “from” and “through” dates are equal. This was due to HIPAA
requirements
This line is also used for transmitting:• SNF MDS assessment reference date RC 0022• HHPPS date of first billable services provided RC
0023• IRF must enter the date the final assessment was
transmitted to CMS national assessment collection database RC 0024
Late assessment policy will affect your Rehabilitation payments eff.01/01/06 (28 days or more from Dischg):
http://www.cms.hhs.gov/medlearn/matters/mmarticles/2005/MM3885.pdf

44
Section:Section:Billing ProcessBilling Process
FL46 Units of Service • Number of services that relate to the HCPCS/CPT
codes reported• Rehabilitation Therapy Services modalities that have
time increments are to report each 15min in unit measurements. Example: 1 unit = 8mins. To <23 mins.
• OPPS Emergency Room exceeds 24 hour, see Trans#881 CR4252 March 3,2006,eff April 3,2006
• Maximum allowable unit OCE edits will require system programming to avoid rejected claims
• Drugs- Facility CDM description vs. HCPCS/CPT description. Many drugs need to be multiplied to equal the HCPCS description on the claim.
Example: CDM Description rev.636 : Insulin inj.100 unitsCDM HCPCS/CPT:J1815 Inj. Insulin per 5 units MULTIPLY 20 to get paid for the 100 units
45
Section:Section:Billing ProcessBilling Process
FL46 Units of Service Continued:
• Observation: Service units will equal the number hours rounded to the nearest hour and counted from the time the physician wrote the order to admit and discharge. PM Transmittal A-02-129 January 3,2003
• Infusion Therapy and Chemo Therapy: Make sure to charge & count units appropriately by rules made in Pub 100-04 Medicare claim processing December 16,2005 Trans#785 CR4258 & April 7, 2006 Trans#902 CR4388
• Outpatient Therapy Visits-0410, 0420, 0430,044, 0480, 0910, and 0943 (Units=number of times the proc/service is performed)Trans#805 CR4226 Jan.06,2006
46
Section:Section:Billing ProcessBilling Process
FL48 Non-covered Charges• Non-covered days (FL8) must have Non-covered charges placed in this
field• Modifiers that pertain to reporting ABN signed items, must have reported
non-covered charges (report occurrence code & date in FL32-35)
(modifiers EY,GA,GL,GY,GZ,KB or TS along w/ HCPCS in FL44)
FL49 Unlabeled
FL50 Payer Identification• Payer must be placed in position 50A,50B,50C. A being the primary and B
secondary, C tertiary• Proof of MSP screening to support Medicare placement position is critical
(GHP working aged,ESRD,LGHP disabled beneficiary,auto or liability ins.,workers’ compensation,black lung, VA)
• Medicaid utilizes “Type of Claim” in this field. See manuals
47
Section:Section:Billing ProcessBilling Process
FL50 Provider Number• This field has 13 alphanumeric characters in each of the three lines • Yearly checks of your claim forms and facilities to assure correct provider
numbers are used. • CMS is now processing new applications for the national provider identifier
(NPI) to each provider. This will replace the current provider numbering system by May 23, 2007 for most health care providers. Small plans May 23, 2008
• Make sure no hyphens • Medicaid utilizes nine characters in their assigned number system
FL51 A-C Health Plan IDWill be used after the National Plan ID rule is published. NPPES will also issue
these numbers. Electronic vendors may already submit using these payer tables currently.
FL54 Prior payments-Payers / Patients• Prior payments should be entered up to 10 digits• Amounts should be entered is titled “due from patient” (deductibles,co-ins,
prior payments from primary payers)
48
Section:Section:Billing ProcessBilling Process
FL56 NATIONAL PROVIDER IDENTIFIEREffective 5/23/2007 NPI rule is mandatory in all electronic &
paper healthcare transactions for all but small health plansMany payers have different implementation dates for the NPI.
Beginning May 1, 2006 CMS announces the capability for health industry organizations to submit health care providers’applications for NPIs o the National Plan and Provider
Enumeration System (NPPES) via Electronic File Interchange (EFI).
Hospitals should have received NPI information from most of the Physicians (Attending/Rendering;Operating;Referring)
Apply for NPI:https://nppes.cms.hhs.gov 1-800-465-3203
CMS NPI Page http://www.cms.hhs.gov/NationalProvIdentStand/
Useful sites of information:http://www.cms.hhs.gov/NationalProvIdentStand/Downloads/NPI_Tr
aining_Package.pdfhttp://www.cms.hhs.gov/EducationMaterials/Downloads/NationalProv
iderIdentifierRoundtable.pdf
FAQ NPI- htt;://questions.cms.hhs.gov (search NPI term/phrase)

49
Section:Section:Billing ProcessBilling Process
NATIONAL PROVIDER IDENTIFIER• NPI will be permanent for a Health Care Provider.
One NPI for a lifetime• A new NPI will NOT be required for change of
ownership, change to corporation, or change name, tax id#, address, Taxonomy classification, state of licensure, or state license number.
• Entity type codes for NPI: (2 types)– Type Code 1 = HCP that are humans-doctor, ARNP, PA,
PT– Type Code 2 + HCP that is organization-non-human such
as physician group, hospital, HHA, pharmacies, nursing homes
• Subparts:– You only obtain a NPI for a “subpart” IF the subpart
currently is required for identification in processing of electronic transactions such as claims processing (this isn’t for group practice satellite offices)
50
Section:Section:Billing ProcessBilling ProcessNATIONAL PROVIDER IDENTIFIER
Listing Existing Legacy Numbers:It is important for you to list in the NPI application all current legacy numbers
NPI: WILL “replace” all “legacy/OSCAR” numbers such as Medicare, Medicaid, UPIN, Blue-Cross, Blue Shield, etc.
NPI: Does NOT replace tax identification or “Pay to address”.Health Plans are NOT required to have NPI. The health plan IS required to use your NPI in
electronic transactions, one of which is claims processing.
FL57 A-C Other Provider IDMay include Legacy#s
FL58 Insured’s Name• Last name, Middle name and middle initial• The name entered must be exactly what is on the health insurance card or eligibility
websites• 25 alphanumeric characters are allowed for the three lines• No spaces, hyphens or titles (Mr.,Sir, Dr.)• Medicaid uses the recipient’s name (mother’s ID for infants)
51
Section:Section:Billing ProcessBilling Process
FL59 Patient’s Relationship to InsuredThis field is for the relationship to the insured (make sure billing staff do not use their memory of prior
coding, these have been updated)01 Spouse02 Grandfather or Grandmother05 Grandson or Granddaughter07 Nephew or Niece10 Foster Child15 Ward (due to court order)17 Stepson or Stepdaughter18 Self19 Child20 employee 21 Unknown22 Handicapped Dependent23 Sponsored Dependent24 Dependent of a Minor Dependent29 Significant other32 Mother33 Father36 Emancipated Minor39 Organ door40 Cadaver Donor41 Injured Plaintiff43 Child Where Insured Has No Financial Responsibility53 Life PartnerG8 Other Relationship
52
Section:Section:Billing ProcessBilling Process
FL60 Insured’s Unique ID
This field allows for 20 alphanumeric characters on the three lines• Id#s must include alpha prefixes, no spaces, dashes, no blanks, no 99999• Medicare uses HIC numbers and prefix & suffix to indicate eligibility status• Medicaid utilizes the 10-character recipient ID number as it appears on the
BIC card
A Retired worker over 65 B Wife over 65C Child or GrandchildD WidowerE Widowed motherF Parent categoryJ Special beneficiary due w/quarters of employment under
SSIK Beneficiary entitled due to quarters of employmentM Individual enrolled in Part B,no elig. for Part A, but may
have purchased Part A benefitsT Individual entitled to Part A or entitled to Medicare based
on Chronic renal diseaseW Disabled Widow

53
Section:Section:Billing ProcessBilling Process
FL60 Insured’s Unique ID# *Continued*
Railroad Retirement Board PrefixesA Retired railroad workerMA Spouse WA Widow or widowerWCA Widow w/child or child alonePA Parent of deceasedJA SurvivorWD Widow or widower of an employee who is 60+WCD Widow w/ child in her care or child alone(of
employee)PD Parent of deceased employeeH Retired workerMH Spouse of retired workerWH Widow or widower of retired workerWCCH Widow w/child of retired workerPH Parent of deceased retired worker
54
Section:Section:Billing ProcessBilling Process
FL61 Insurance Group NameGroup name that relates to the health insurance coverageFL62 Insurance Group NumberInsurance companies assign group policy codes• Champus-enter military status and pay grade• Champva, enter veteran’s military status• BlueCard-enter 999999 in Grp field,NO MORE: “ITSPPO”• Check cards and internet eligibility for group#sFL63 Treatment Authorization Code
• IPA authorization• Medi-cal TAR#FL64 Document Control Number(Employer Location deleted from the UB04)FL66 DX Version Qualifier (9=ICD-9-CM or 10 = ICD-10-CM)
55
Section:Section:Billing ProcessBilling Process
*All of this coding comes from Medical Records Department*
FL67A-C Principal & FL67I-Q Other Diagnosis Code• Use the highest level of ICD-9-CM DIAGNOSIS code specificity to avoid claim errors. No
decimals (i.e.,47870 not 478.70)• Screen for medical necessity edits and utilize the Advanced Beneficiary Notice for
Medicare patients. • The sign/symptoms that prompt the ordering of diagnostic tests should be used in the
absence of a diagnosis. • Medicare will ignore data sumitted in 67I-67Q, 17 secondary allowed however CMS will
only identify 8.• POA(Present on Admission) Indicator applies to inpatient admissions to general
acute-care hospitals or other facilities, as required by law or regulation for public health reporting.Health plans should not reject the claim if they have no use for the POA info. Medicare began to accept POA October 1,2007 indicator for every diagnosis on IP claims.(MM5499 May 11,2007)(837I claims only!!)
• Reporting Options:Y-Yes(present at the time of inpatient admissionN-No (not present at the time of inpatient admissionU-Unknown(documentation is insufficient to determine if present upon IP admissionW-Clinically undetermined(provider unable to determine if present on admission or not1- Unreported/not used-Exempt from POA reporting(1 is equal to blank for 4010A1 data)
FL68 UnlabeledFL70 Admitting Diagnosis/Patient’s Reason for Visit• Required for Inpatient Hospital swing-bed & Skilled Nursing Facility claims• April 1, 2005, OPPS reimbursed observation must be reported in FL76 or
FL67 to be reimbursed appropriately• Global Release 08/03/05 California Blue Shield(G94036), required on all
Outpatient claims. Check with your EDI department.
56
Section:Section:Billing ProcessBilling Process
*All of this coding comes from Medical Records Department*
FL71 PPS Code – Required for inpatient claims when contracted to provide MS-DRG(4 digit leading w/zeros, all zeros if no DRG defined)
Can be used for MS-DRG,RUG,IRF,APC,HHRG PPS identification
FL72 External Cause of Injury (E codes=ECI)• Not required by all payers, but worth adapting to. Diagnosis related to
injury, poisoning, or adverse effect. CMS will ignore.FL73 UnlabeledFL74 Principal Procedure Code & Date• Principal ICD-9-CM PROCEDURE and date required during inpatient stays. Date must fall
within 3 days prior to the date of admission and/or within the statement period (FL6)• Denials may occur if these are placed on Outpatient Medicare claims. Check with your
specific payer guidance's. See FL 44 for TOB(FL4)13x claims (HIPAA electronic compliant claim)
FL74 a-e Other Procedure Codes & Dates• Do not repeat codes unless bilateral procedures are performed OR payer specific
instructions require repeats
FL75 Unlabeled
57
Section:Section:Billing ProcessBilling Process
FL76 Attending NPI/QUAL/ID,Last/First Name
Qualifiers: OB= State License numer
1G=Provider UPING2=Provider commercial number
The licensed physician entered is the one that certifies and recertifies the medical necessity of services
NPI-National provider identifier is currently being processed by CMS for implementation.
No apostrophe or hyphens. Only alphabetic characters.Medicare: UPIN and name of the attending physicianSelf-referred use SLF000 (self referred clinic or
mammography)Medicaid-Check with your state requirements (CA Medi-
cal provider number or State license number i.e.,00A987654)
Others-Check with specific contract & bill requirements
58
Section:Section:Billing ProcessBilling Process
FL77 Operating Provider/NPI (Qualifier)FL78 Other Provider/NPI (Qualifier)
FL79 Other ID Qual/NPI/Qual/IDFL81A-E Code overflow fields
B3(Qualifier)=Billing Provider Taxonomy & #(i.e.,B3282N00000X)
(Other procedures and dates) Do not repeat codes unless they arebilateral procedures
TAXONOMY CODES (Facility)MM5243, CR# 5243 Sept 8,2006 Eff. 1/1/07
59
Section:Section:Billing ProcessBilling Process
Values-Qualifiers (UB04 vs. 837I/NM108)BQ – HCPCS procedure Code
BQ – ICD-9-CMOB – State License number (UB04)1A – Blue Cross Provider number1B – Blue Shield Provider number1C – Medicare provider number1D – Medicaid Provider number
1G – Provider UPIN number (UB04)1H – TRICARE identification number
EI – Employer’s identification numberG2 – Provider commercial number(UB04)
LU – Location numberN5 – Provider plan network identification number
SY – Social Security number (not for Medicare)X5 – State industrial accident provider number
60
Section:Section:Billing ProcessBilling Process
CMS website Q&A (9/12/06)• Feedback Should all institutional providers submit a taxonomy code
on their claims after the implementation of the National Provider Identifier (NPI)?
• Answer Only institutional providers that currently bill Medicare using more than one legacy identifier in order to identify sub-parts of their facility are required to submit a taxonomy code on all of the claims they submit to Medicare. Medicare legacy identifiers are six digit Medicare provider numbers, also called OSCAR numbers. A table of legacy identifiers that were used to identify sub-parts is included as an attachment to CMS Change Request 5243. Taxonomy codes shall be reported by these facilities whether or not the facility has applied for individual NPI for each of their subparts. Institutional providers that do not currently bill Medicare for sub-parts are not required to use taxonomy codes on their claims to Medicare.
Taxonomies for physicians will be obtained by electronic claim vendors to submit when payer-specific requirements apply.

61
Section:Section:Billing InformationBilling Information
Common Reasons for RejectionCommon Reasons for Rejection
Commercial/HMO/PPO:
Member ID number & Group is incorrectICD-9-CM Codes missing or invalidDate of injury missingUntimely filingAlpha prefix of the ID number missingInappropriate Utilization Mgmt. infoHCPCS/CPT codes missing/invalid/unlistedServices were not medically necessaryRequest for medical recordsDuplicate billings (overlap DOS, within 30 days last billed)
Medicaid:
Local billing limit exception codes-condition codes (FL19-28)Missing value codes and amounts (FL39-41)Missing payer info. “I/P” indicator (FL50)Missing/incorrect Health Plan ID (FL51)ID number incorrectly (verify using POS or AEVS) (FL60)EVC# entered instead of TAR (FL63)Incorrect attending physician 9 digit (FL76-79)Reducing font size or abbreviating terminology to fit in field when attachments should be created instead (FL80)
62
Section:Section:Billing InformationBilling Information
Basics to KnowCMS Manual Pub 100-04 Medicare claims processing Transmittal #407 CR3633 Dec.17,2004 Eff.1/1/05
“Hospital Billing for Repetitive Services”Know your admit and discharge status’ and how they impact your claims (transfer rules for PPS) DRG Payment Window Requirements(3 day window & 1 day pre-admission diagnostic services) must be included in the inpatient DRG stay claim. Medicare Billing Manual 40.3 Rev#714 implementation 4/3/06NCCI (National Correct Coding Initiatives)& Outpatient Code Editor (OCEs)Revenue codes, Value Codes, Condition/Occurrence codes, HCPCS, CPT, Bill types, modifiers.Medicare Secondary Payer (MSP)Observation rules and regulationsConsolidated billing for Skilled Nursing Facilities Make sure families have enrolled babies within 30 days with health plans
63
Section:Section:Billing InformationBilling Information
Basics to KnowMost companies are now using scanning equipment, this means that we should not use Highlighters.Check for COB-Coordination of Benefits-secondary insuranceInjury coding and principal diagnosisDo not use photocopies of claims, use laser forms or “red drop out ink” formsNo stamps should be used unless you are sending the claim to a specified unit for “Carve-outs”, “Appeal” or “Stop-loss” processingDischarge date must be consistent w/DOS-for Inpatient & OutpatientGroup plans-CA license number-not UPIN Auth. number for all scheduled, elective admissions-available on admission-precert would have been doneSplit bill if the baby stays after the mother is discharged (Unless contract requires other action)
64
Section:Section:Billing InformationBilling Information
• Transmittal 515Subject: Update to 100-04 and Therapy Code Lists
– CMS identifies specific CPT codes as therapy services• Physical Therapy – Modifier -GP• Occupational Therapy – Modifier -GO• Speech Therapy – Modifier –GN
– Paragraph B identifies specific CPT codes which are:• Not priced from fee schedule, priced by carrier. FI contacts the carrier to
obtain the appropriate fee schedule amount• Codes that are bundled• Paid by Outpatient Prospective Payment System (OPPS)• Always therapy codes regardless who performs them (PT/OT/ST)• Codes that sometimes represent therapy services
– All codes on this table always represent therapy services when performed by therapists
• Revisions to benefit policy for therapy services: http://www.cms.hhs.gov/medlearn/matters/mmarticles/2005/MM3648.pdf
• Physical & Occupational Therapy Billing Guide Oct. 2006: http://www.medicarenhic.com/providers/pubs/ptotguide_oct06.pdf
65
WebsitesWebsitesBeneficiary Notice Initiative:http://www.cms.hhs.gov/MLNProducts/10_BeneficiaryRelated.aspCMS Claims processing Manual:
http://www.cms.hhs.gov/Manuals/IOM/itemdetail.asp?filterType=none&filterByDID=-99&sortByDID=1&sortOrder=ascending&itemID=CMS018912
Clinical Lab Information: http://www.cms.hhs.gov/suppliers/clinlab/default.asp
Federal Register:http://www.access.gpo.gov/su_docs/fedreg/frcont06.htmlHIPAA EDI:www.hipaadocs.com ,http://nchica.org, http://www.wpc-
edi.com/codesHMO Help: http://www.hmohelp.ca.gov/Intermediaries/Carriers: California (Regional Office: San Francisco)
http://www.cms.hhs.gov/contacts/incardir.asp#1Part A - United Government Services, LLC; Mutual of Omaha Insurance
CompanyPart B - National Heritage Insurance CompanyRHHI - United Government Services, LLCDMERC - Connecticut General Life Insurance CompanyIntermediaries/Carriers/DMERC’s may change in the near future
Inmate Info by County Sheriff Inmate Info (booking#search):LA: http://app1.lasd.org/iic/ajis_search.cfmOC:http://app1.ocsd.org/SB: http://app1.sbsd.org
66
WebsitesWebsitesLifetime Reserve Days:
http://www.cms.hhs.gov/MLNMattersArticles/downloads/SE0663.pdfMedicare/Medicaid Manuals:http://www.cms.hhs.gov/Manuals/PBM/list.asphttp://www.cms.hhs.gov/Manuals/IOM/list.aspMedicare Hospital Payment System,Policies,NPI & More:http://www.cms.hhs.gov/center/hospital.aspMedlearn: http://www.cms.hhs.gov/medlearn/pubs.aspMedi-Cal: http://www.medi-cal.ca.gov/Medical Review Strategy:http://www.medicarenhic.com/cal_prov/med_review.shtmlNUCC & NUBC:1500: www.nucc.org , UB04: www.nubc.org837I 5010: www.wps-edi.com2007
Transmittals:http://www.cms.hhs.gov/Transmittals/2007Trans/list.aspNCD/LCD & Basic Coverage Issues:
http://www.cms.hhs.gov/center/coverage.asphttp://www.medicarenhic.com/cal_prov/policies.shtlNPI: https://nppes.cms.hhs.gov/NPPES/Welcome.do &
http://www.cms.hhs.gov/NationalProvIdentStand/01_overview.aspLab NCD coverage manuals (Great for physician offices)
http://www.cms.hhs.gov/CoverageGenInfo/04_LabNCDs.asp#TopOfPageTransmittals: http://www.cms.hhs.gov/Transmittals/

67
Quality Improvement Quality Improvement Organizations are watching!Organizations are watching!
• March 2005, CMS began 3 year pilot DRG revenue recovery demonstration project in the 3 states with highest Medicare expenditures- CA, FL, and NY. Common DRG findings 416, 217, 397, 188.2010 CMS plans to phase in the RACs among all states.
• One-day stays for: DRG 127 (heart failure and shock), DRG 143 (chest pain), DRGs 182/183 (esophagitis, gastroenteritis and other digestive disorders with and without complications or co morbidities, respectively), DRGs 296/297 (nutritional and metabolic dis-orders with and without complications or co morbidities) and other one-day stays excluding transfers. Because one-day stays are so short, CMS is concerned that they may be medically unnecessary or that the patient could have been treated in a less costly setting.
• DRG 217 (Wound Debridement & Skin Graft) Need physician documentation ie.e.,sharp, excisional as well as the depth and site of all excisional wound debridement procedures.
• DRG 188 (Other digestive system disorders with cc) 578,.x Target:Only CC• DRG 397 (Coagulation Disorders) Coding clinic 2004 Qtr 3 provides explicit
guidelines regarding the specific bleeding disorders resulting from Coumadin therapy. Watch use of 599.7,784.7,578.x
• DRG 416 (septicemia). This is often confused with kidney and urinary tract infections with or without complica-tions or co morbidities. Watch use of 790.7, 599.0, 996.62
• Higher-weighted DRGs in a complications or co-morbidity pair. If you always bill for the higher paying DRG with complications or co morbidity after discharge, it may raise fraud suspicions.
• Three-day qualifying skilled nursing facility admissions. OIG revealed hundreds of overpayments to SNFs nationwide that occurred because there was no three-day stay at an inpatient hospital prior to admission.
• Readmissions for the same health problem within seven days of discharge. If a patient is readmitted for the same problem soon after discharge, it suggests that the original treatment did not work and therefore Medicare should not pay for it.
68
Quality ImprovementQuality ImprovementQuality data captured in your hospital system upfront will determine much of your success in your hospital revenue cycle.Formal employee training, auditing, policies & procedures for functional productivity and goal setting.Fine-tune your hospital system so it’s user friendly, incorporates internet access and good communication for the flow of informationCreating a committee that reviews and reports all findings and accomplishes solutions to reimbursement and workflow issues.

69
What can we offer in future What can we offer in future seminars to help you?seminars to help you?
QUESTION?AND
ANSWER!SESSION
Disclaimer: This document was designed to provide accurate information as a tool for your use. HFMA, AAHAM , agents and staff, make no representation, guarantee or warranty, express or implied, that this is error-free, and will bear no
responsibility or liability for the results of it’s use. However, the ultimate responsibility for accuracy lies with the user.
70
GlossaryGlossary• Ambulatory Payment Classification Groups (APCs):A classification
system that groups outpatient visits and procedures into paymentcategories for payment under the Medicare Outpatient PerspectivePayment System (OPPS)
• CDM: Charge Description Master AKA Chargemaster• Clearinghouse: Processes information for health care providers and
sends batches of claims to multiple payers• Diagnosis-related Groups (DRGs):A classification system that groups
patient according to diagnosis, type of treatment, age, and other relevant criteria. MS-DRG Medicare Severity DRG’s eff 10/01/07
• EDI: Electronic Data Interchange is the computer-to-computer transfer of business-to-business document transactions and information between trading partners
• EGHP: Employer Group Health Plan • Final Claim: Final itemized bill form from an institutional provider
detailing all the charges for which the institutional provider is seeking payment
• HIM: Health Information Management/Medical Records• HIPAA: Health Insurance Portability & Accountability Act• HIPPS: Health Insurance Perspective Payment System rate codes-Home
Health HHPPS• HIS: Hospital Information Systems/Information Services• HRG code: HealthCare Resource Groups-Rehab Medicare PPS• LGHP: Large Group Health Plan • Medically Necessary: Services or supplies that: are proper and needed
for diagnosis or treatment of your medical condition, are provided for the diagnosis, direct care, and treatment of your medical condition, meet the standards of good medical practice in the local area, and aren’t mainly for the convenience of you or your doctor.
71
GlossaryGlossary• Medicare Contractor: A Medicare Part A fiscal intermediary (institutional),
a Medicare Part B Carrier (professional), or a Medicare Durable Medical Equipment Regional Carrier (DMERC)
• MSP: Medicare Secondary Payer• NCD: National Coverage Determinations (previously LMRP-Local Medical
Review Policies=LCD)• National Provider Identifier (NPI): Beginning May 23, 2005, health care
providers may apply for an NPI. May 23, 2007 all covered health care providers and clearinghouses must use NPI. Small plans May 23, 2008
• OCE edits: Outpatient Code Editor• PFS: Patient Financial Services AKA Business Services• RC: Revenue Code• RUG code: Resource Utilization Groups, SNF/TCU-PPS• Unbilled charges: Charges or services provided for and not billed.• UPIN-Unique Physician Identification Number• Unbundling: Submitting bills using separate billing codes for multiple
treatments or services that were billed separately, or fragmenting one treatment or service into its component parts and coding each component part as if it were a separate treatment or service. A common example of unbundling is when a provider performs surgery and then bills for the pre-and post-operative visits that are included in the billing of the surgery
• Up-coding: Using a diagnosis or billing code that does not best represent the patient's actual condition or the treatment or service actually performed. A common example of up-coding is billing for a higher code than justified by the complexity of the case
• Vendor: Develops software application to enable claims to be submitted electronically
72
Corporate ComplianceCorporate ComplianceOIG OIG WorkPlanWorkPlan 20082008
• Hospital Capital Payments are appropriate levels• Adjustment for Graduate Medical Education payments• Inpatient Prospective Payment System wage indices, analyze data and
assure accurate reporting• Payments for Organ Procurement Organizations• Inpatient Hospital Payment for New Technologies• Special payment provisions for patient who are transferred to onsite
providers and readmitted to LTC hospitals (Long Term Care)• Special Payment Provisions for LTC hospitals discharging beneficiaries to
collocated or satellite providers• Critical Access Hospitals-review payments• Medicare Disproportionate Share Payments review, eligibility, States use
and distribution• Inpt Psychiatric Facility ER dept adjustments• Provider Bad Debts• Compliance with Medicare’s Transfer Policy.• Payments for diagnostic x-rays in hospital emergency departments• Patient care and safety in physician-owned specialty hospitals• Oversight of the Joint Commission Hospital Accreditation Process• Medicare Secondary Payer
73
Corporate ComplianceCorporate ComplianceOIG OIG WorkPlanWorkPlan 20082008
• Cyclical Noncompliance in Medicare Home Health Agencies• Accuracy of Home Health Data & coding/claims resource groups (HHRG)• Medicare Hospice Care for nursing home residents, appropriate services and payments• Physicians: Place of Service errors, E&M during global surgery periods• Medicare payments for selected physician services• Medicare “Incident to” Services• Medicare payment of Polysomnography• Business Relationships with use of MRI under Physician fee schedule• Accept assignment rules for physician providers• Geographic areas: high utilization of Ultrasound • Physician Reassignment of Benefits• Medicare Part B drug reimbursement & Part D • Medicare payments for Observation vs. Inpatient for dialysis services• Laboratory Rendered during an Inpatient stay• Therapy Services provided by Comprehensive Outpatient Rehabilitation facilities• Emergency Services for Undocumented Aliens• Separately billable Lab under End Stage Renal Disease Program• Pricing of Clinical Laboratory tests• Medicare Advantage: Stabilization fund, rates, bids, encounter data• Recovery Audit Contractors• Medicaid-much of the same issues as Medicare• Credit balances for Medi-Medi beneficiaries• Public Health, oversight, Lab preparedness, vaccines
Disclaimer: This document was designed to provide accurate information as a tool for your use. HFMA, AAHAM , agents and staff, make no representation, guarantee or warranty, express or implied, that this is error-free, and will bear no
responsibility or liability for the results of it’s use. However, the ultimate responsibility for accuracy lies with the user.