2009 acerra, congresso regionale sicoa, la terapia elettrica dello scompenso cardiaco nel paziente...
TRANSCRIPT

La CRT in pts with standard PM La CRT in pts with standard PM indication and in pts with DCM indication and in pts with DCM
and short QRS and short QRS
Stefano Nardi MD, PhDStefano Nardi MD, PhDRESPONSABILERESPONSABILE
Centro di ARITMOLOGIA CLINICA ed ELETTROFISIOLOGIA CARDIACACentro di ARITMOLOGIA CLINICA ed ELETTROFISIOLOGIA CARDIACADiaprtimento CardiotoracovascolareDiaprtimento Cardiotoracovascolare
AO S.Maria TerniAO S.Maria Terni

VOO
VVI
RR
AAIR <-> DDDR
Cardiac pacing evolution …
DDD
Rate…
AV synchrony…
What does it mean
Physiological pacing ?
Since 30-ies .......

What Does it mean Physiologic Pacing ?
DDD can reduce PCWP and improve COIshikawa, Eur J Card Pacing Electr ‘96
DDD improves prognosis in CHF compared to VVILinde-Edelstam PACE ‚92
• 1 and 2 year mortality significantly lower with DDD compared to VVI(R) pacing
MEDICAREn = 36,312
VVI(R)
DDD(R)
Lamas, Circulation `95
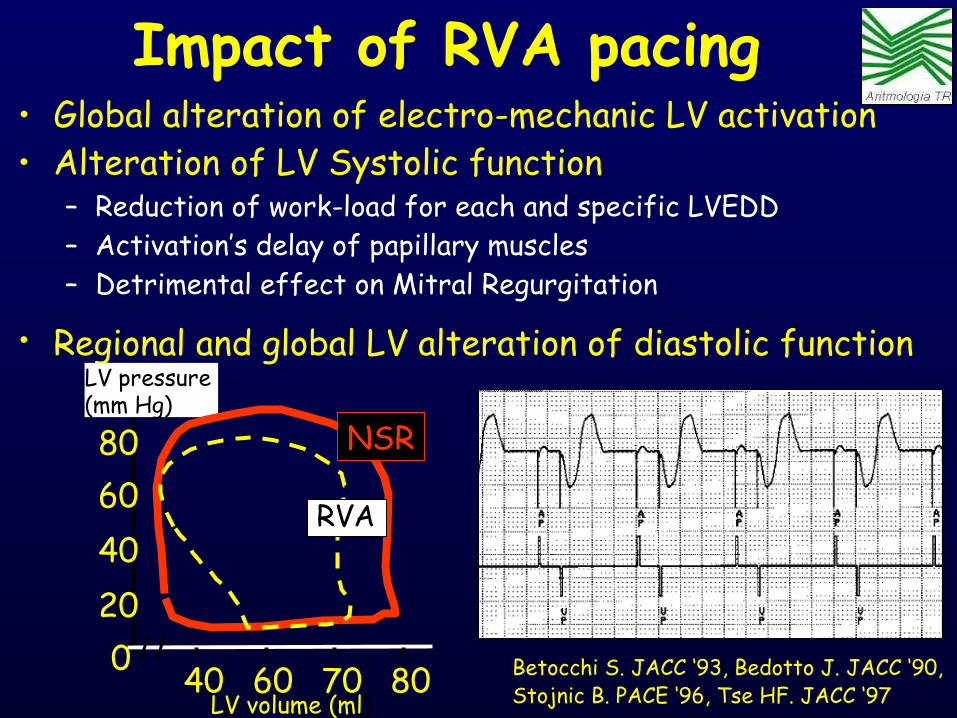
Impact of RVA pacing• Global alteration of electro-mechanic LV activation
Betocchi S. JACC ‘93, Bedotto J. JACC ‘90, Stojnic B. PACE ‘96, Tse HF. JACC ‘97
• Alteration of LV Systolic function– Reduction of work-load for each and specific LVEDD– Activation’s delay of papillary muscles – Detrimental effect on Mitral Regurgitation
• Regional and global LV alteration of diastolic function
020406080
40 60 70 80LV volume (ml)
LV pressure (mm Hg)
NSR
RVA

Delayed Delayed conductionconduction
SinusSinusnodenode
AVAVnodenode
Mimic LBBBMimic LBBB
• Abnormal RV-LV sequence• Abnormal LV activation sequence• Segmentary dyskinesia• Disynchrony of RV and LV filling flows
24 pts (19.5±8.1) with normal Segmental Anatomy paced from the RV apex (median 10 yrs (0.7–18.9) and compared with 33 CTR
Tantengco MVT. JACC ‘01
Impact of RVA pacing

Ansalone G. It H J ‘99
Altered Left Ventricular Performance

Altered Left Ventricular Performance
• Lister (‘64)– Greater reduction in CO when pacing
from ventricular sites associated with longest total activation time → muscle conduction
• Conduction velocity differences (Purkinje = 2-4 m/s; Muscle = 0.2-1 m/s)
• Wiggers (‘25)– “The initial slower rise of intraventricular pressure is prolonged, IVCT phase is
lengthened, the gradient is not so steep, the pressure maximum is lower, and the duration of systole is increased.”
Artificial stimuli induce local fractionate contractions → Slow
Sweeney MO. JACC ‘06
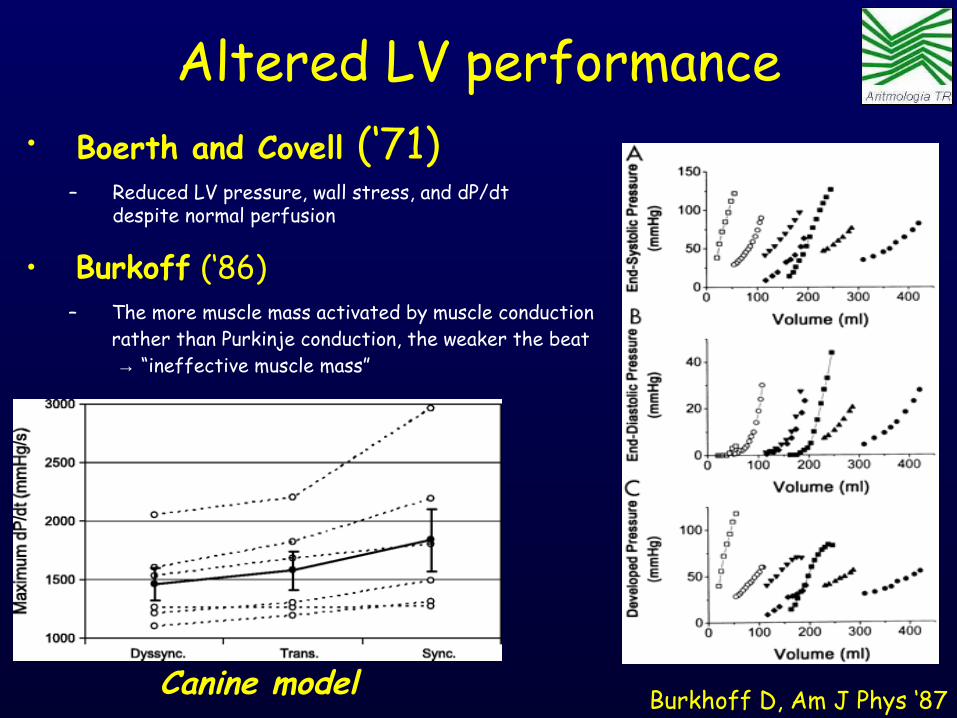
Altered LV performance• Boerth and Covell (‘71)
– Reduced LV pressure, wall stress, and dP/dt despite normal perfusion
• Burkoff (‘86)– The more muscle mass activated by muscle conduction
rather than Purkinje conduction, the weaker the beat → “ineffective muscle mass”
Canine model Burkhoff D, Am J Phys ‘87

Altered Myocardial Perfusion
• Heyndrickx (1985)– Coronary blood flow was higher despite
decreased cardiac output
• Prinzen (1990)– Similarity in behavior of electrical
activation, fiber strain and blood flow • Redistribution of strain and blood flow
with RV pacing• Early activated regions ~ 60% blood flow of
late activated regions
– The regions of the heart activated via the Purkinje system (simultaneous activation) have greater fiber strain and blood flow
Sweeney MO. JACC ‘06

Karpawich PP. PACE ‘99, Tse HF. JACC ‘02, Thambo JB. Circulation ‘04
• Detrimental effects on ventricular remodeling – Regional alteration of flow
“patterns” – Improvement of O2
consumption without increment of flow
– Abnormal and asymmetric ipertrofy of LV wall
Altered Myocardial perfusion
VO2
(ml/
min
/mVO
2 (m
l/m
in/m
22 ))DODO22 (ml/min/m (ml/min/m22))
Critical DOCritical DO2 2
DISOXIADISOXIA
Critical VOCritical VO22
NormalNormal
• Rosenqvist (‘88)– Increased incidence of CHF in
RV paced pts

Right ventricular pacing HISTOPATHOLOGY
• Karpawich (‘90) – Pediatric Canine Model– LV myofibril disarray was found after 4
months of pacing from RV apex• 90° misalignment of adjacent fibers (stress related?)
– Also noted appearance of prominent Purkinje cells in subendocardium, variable-sized mitochondria, and dystrophic calcification
• Adomain (‘86)– Myofibril disarray was found in 75% of canine hearts
after 3 months of pacing from RV apex• Greatest at base of left ventricular free wall
RV septal pacing: no disarray
Karpawich PP. Am Heart J 1991.
RV apical pacing: disarray
Karpawich PP. Am Heart J 1990.
• Karpawich (‘99) – Pediatric Pts– Myofibril hypertrophy, intracellular vacuolation,
degenerative fibrosis, and fatty deposits in the LV after more than 3 years RV apical pacing
– Independent of paced time, patient age, epi- or endocardial electrode placement, and mode

Spragg DD, Circulation ’03
Regional Alterations of Protein Expression in RVP dogs
TNF-alpha expressionApoptosis and Fibrosis

Delayed Delayed conductionconduction
SinusSinusnodenode
AVAVnodenode
Mimic LBBBMimic LBBB
• Abnormal RV-LV sequence• Abnormal LV activation sequence• Segmentary dyskinesia• Disynchrony of RV and LV filling flows
24 pts (19.5±8.1) with normal Segmental Anatomy paced from the RV apex (median 10 yrs (0.7–18.9) and compared with 33 CTR
Tantengco MVT. JACC ‘01
Impact of RVA pacing

Ansalone G. It H J ‘99
Altered Left Ventricular Performance

SinusSinusnodenode
AVAVnodenode
BundleBundlebranch orbranch or
diffuse blockdiffuse block
Delayed conductionDelayed conduction
• Abnormal RV-LV sequence• Abnormal LV activation
sequence• Segmentary dyskinesia• Aggravation of mitral
regurgitation• Disynchrony of RV and LV
filling flows
Dyssynchrony Ventricular ContractionDyssynchrony Ventricular Contraction
What is abnormal in the RVP pts?What is abnormal in the RVP pts?Cardiac Resynchronization TherapyCardiac Resynchronization Therapy
• Delayed AV sequence• Mitral regurgitation• Decreased filling time

Sinusnode
AVnode
Bundlebranch or
diffuse block
Delayed conduction
• Delayed AV sequence
• Mitral regurgitation
• Decreased filling time
Delayed Ventricular ActivationDelayed Ventricular Activation
What is abnormal in the HF pts?What is abnormal in the HF pts?Cardiac Resynchronization TherapyCardiac Resynchronization Therapy

• As the LV becomes more spherical this twisting ability of LV reduced (apical
counter-clockwise /basal clockwise) with reduction both of LVEF and filling.
• As CHF progresses, the associated dilation of the LV will often change both SIZE and SHAPE of LV
Left Ventricular Remodelling Size, Shape and MV apparatus
• As CHF progresses, the associated dilation of LV will often pull the MV
apparatus out of proper anatomical alignment (MR)
• The misalignment reduces the ability of MV apparatus to assist LV in the contraction (additional work-load)
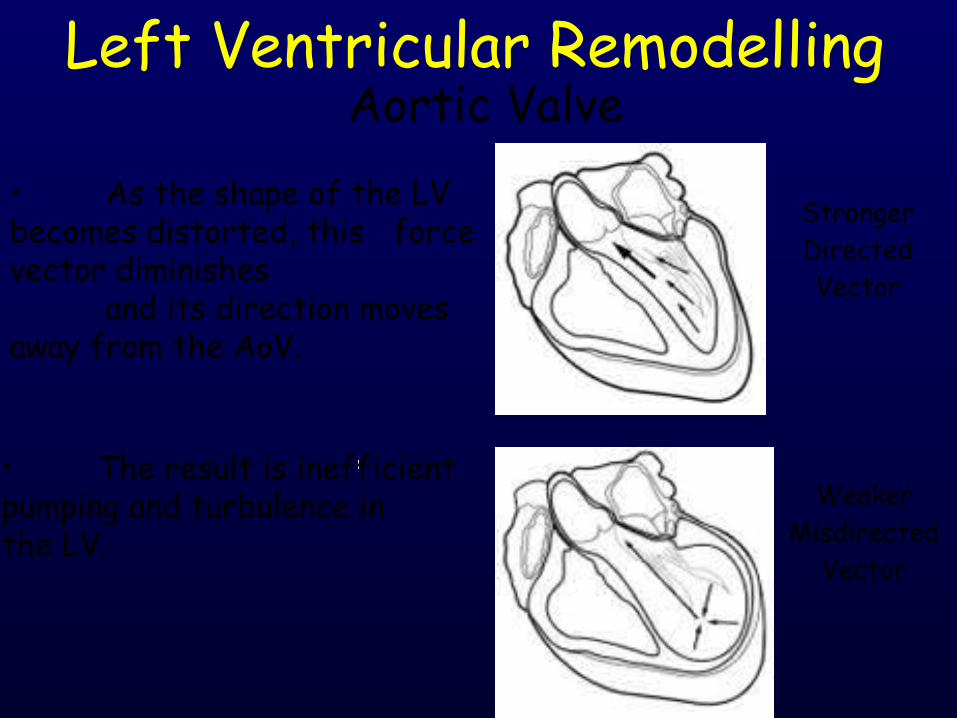
Stronger Directed Vector
Weaker
Misdirected Vector
• As the shape of the LV becomes distorted, this force vector diminishes
and its direction moves away from the AoV.
• The result is inefficient pumping and turbulence in the LV.
Left Ventricular Remodelling Aortic Valve
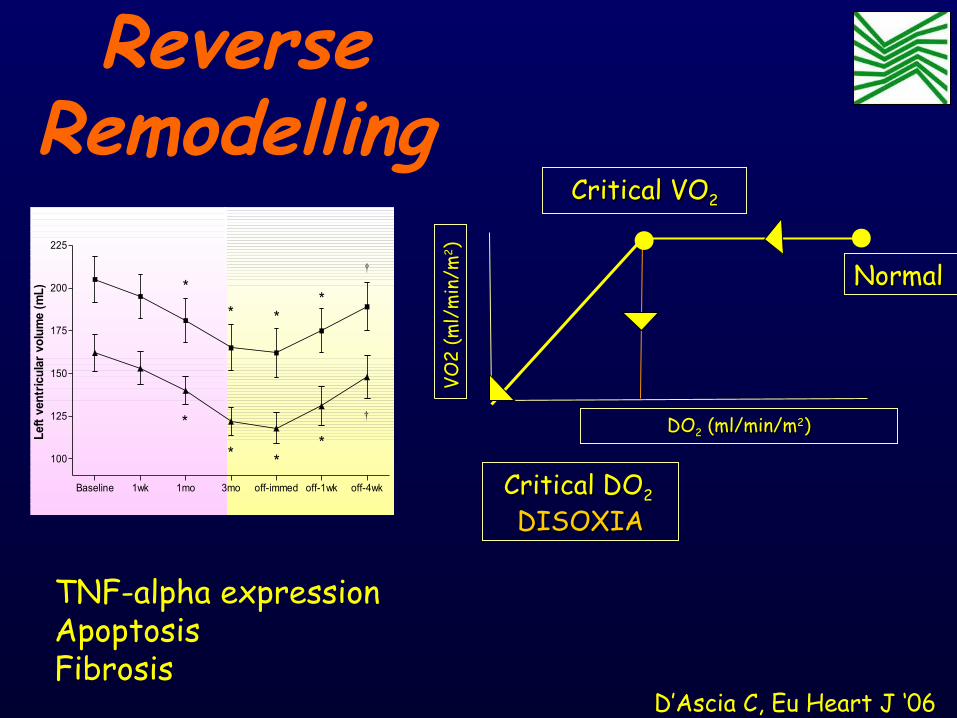
D’Ascia C, Eu Heart J ‘06
Baseline 1wk 1mo 3mo off-immed off-1wk off-4wk
100
125
150
175
200
225
**
*
*
†
* *
*
†
Left
ven
tric
ular
vol
ume
(mL) *
VO2
(ml/
min
/mVO
2 (m
l/m
in/m
22 ))DODO22 (ml/min/m (ml/min/m22))
Critical DOCritical DO2 2
DISOXIADISOXIA
Critical VOCritical VO22
NormalNormal
ReverseRemodelling
TNF-alpha expressionApoptosisFibrosis

Prolate Spheroidal Coordinates
Costa, Biomech Eng. ‘96 www.continuity.ucsd.edu
Ventricular Muscle Fiber Orientation
Walker et al, J Thorac CV Surg. ‘05
CHF PATHOLOGY

Definition of Stress
Fung, A 1° Course in Continuum Mechanics, ‘94
LV PV loops
McCulloch, Theory of Heart, ‘91
CHF PATHOLOGY

Model of Shortening
Deactivation
Guccione and McCulloch, J Biomech Eng. ‘93 Feb;115(1):72-90
Muscle Contraction Model Comparison

D’Ascia C, Eu Heart J ‘06
Baseline 1wk 1mo 3mo off-immed off-1wk off-4wk
100
125
150
175
200
225
**
*
*
†
* *
*
†
Left
ven
tric
ular
vol
ume
(mL) *
VO2
(ml/
min
/mVO
2 (m
l/m
in/m
22 ))DODO22 (ml/min/m (ml/min/m22))
Critical DOCritical DO2 2
DISOXIADISOXIA
Critical VOCritical VO22
NormalNormal
ReverseRemodelling
TNF-alpha expressionApoptosisFibrosis

DAVIDMOSTMOST
DANISHDANISH
CTOPPCTOPP
UKPACEUKPACEPASEPASE
C. W. Israel CW, Cardiostim `06
DAVID TrialJAMA ‘02
RV stimulation may be more deleterious in patients with advanced LV dysfunction (ICD candidates); DDDR-70
was worse than VVI-40; more pacing (60%) was seen in DDDR-70; however, only 30.8% of the patients had a
QRS>130ms
MOST Trial Sweeney M, et al. PACE ‘02
(mode selection trial in sinus-node dysfunction)Hospitalization was not associated with mode but with
prevalence of more then 40% RV pacing
Danish Pacemaker StudyAndersen HR, et al. Lancet ‘97
AAI vs. VVI for SSSDanish pacemaker study: AAI had slightly better
survival and was associated with lower occurrence of CHF (native AV conduction is better)
Pacemaker Selection in the ElderlyLamas GA, et al. NEJM ‘98
VVI vs. DDD for Sinus Node Dysfunction or AV block; no difference in quality of life or outcome (CV or death)
Different Pacing Modalities in Randomized Clinical Trials

Why was DDD not better than AAI/VVI in several Trials ?
(DAVID, DANISH, PASE, CTOPP, MOST, UKPACE ?)
A: Because DDD doesn‘t workB: Because DDD was programmed badlyC: Because leads were not implanted optimallyD: Because all these studies had severe limitationsE: B, C + D

• Cumulative percentage of RVP is an INDIPENDENT PREDICTOR of AF development
0
1
2
3
4
0 20 40 60 80 100Cum % VP
Ris
k of
AF
rela
tive
to
DD
DR
pat
ient
wit
h Cu
m%
VP=
0
• RR of AF INCREASE LINEARLY with the RVP until about 80-85%, both in the DDDR group and VVIR group
• AF risk is REDUCE of 1% for each 1% of reduction of Cumulative % of VP in the DDD(R) group.
Sweeney MO, Circulation ‘03
0
1
2
3
4
0 20 40 60 80 100Cum % VP
Ris
k of
AF
rela
tive
to
VVIR
pat
ient
wit
h Cu
m%
VP=
0
MOST Sub-Study (1339pts (67%) with Know Cum%VP)
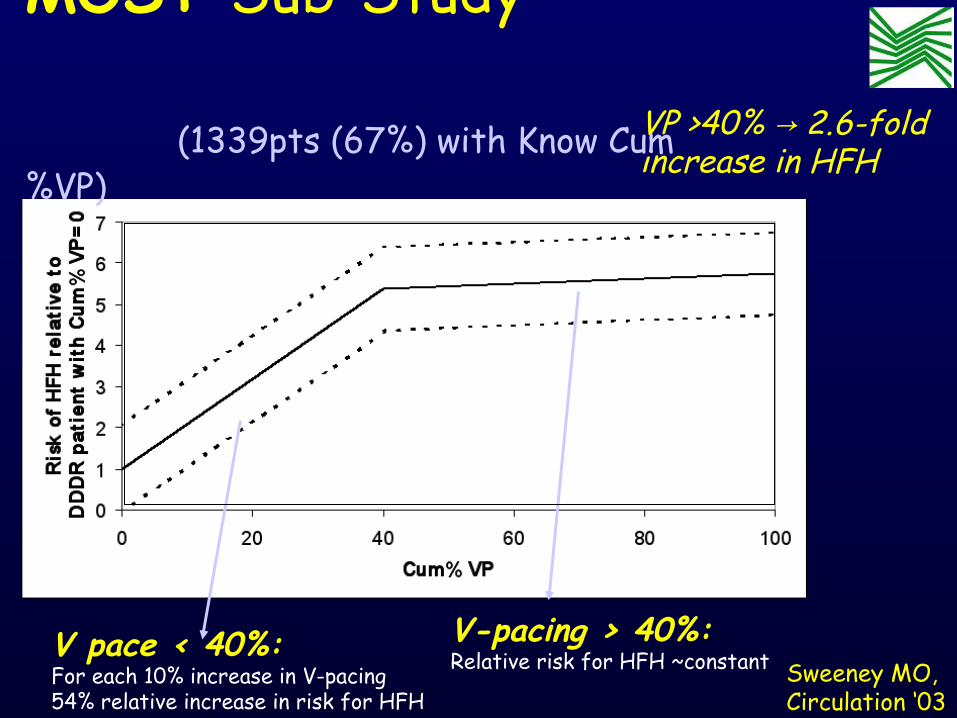
V pace < 40%:For each 10% increase in V-pacing 54% relative increase in risk for HFH
V-pacing > 40%:Relative risk for HFH ~constant
VP >40% 2.6-fold →increase in HFH
Sweeney MO, Circulation ‘03
MOST Sub-Study (1339pts (67%) with Know Cum%VP)

0
2
4
6
0 20 40 60 80 100Cum % VP
RR of 1st CHF-H • RR INCREASE between 0% and 40% of Cum% VP, but doesen’t change for >40% (45% and 65% have the same RR)
• The RR is REDUCED at ≈2% if RV pacing is minimised
When Cum% VP<40% for each 10% of reduction of Cum %VP, there is a relative reduction of 54% of RR for 1st CHF-H
0
2
4
6
8
10
12
0-20 20-30 30-40 > 40Cum% VP
Ris
k of
HFH
DDDRVVI R
RR of CHF-H: VVIR > DDDR, regardless of %VPRR is max for VVIR vs DDDR, INDIPENDENTELY for % of VP
MOST Sub-Study (1339pts (67%) with Know Cum%VP)

• Normal ventricular activation requires a synchronized participation of the distal components of the specialized conduction system
• Conventional RV pacing results in “forced” ventricular desynchronization, which mimics LBBB and has adverse effects on structure and function.
Sweeney, JACC `06
Executive Summary
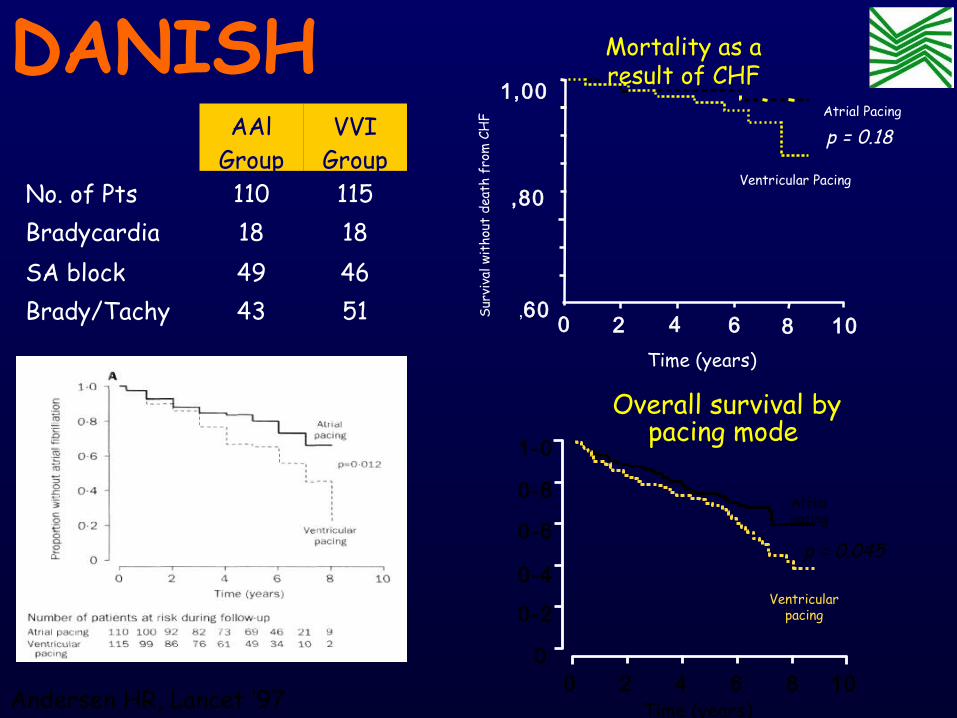
Andersen HR, Lancet ‘97
DANISHAAl
GroupVVI
GroupNo. of Pts 110 115Bradycardia 18 18SA block 49 46Brady/Tachy 43 51
1,00
,80
,600 2 4 6 8 10
Atrial Pacing
Ventricular Pacing
p = 0.18
Surv
ival
wit
hout
dea
th f
rom
CH
F
Time (years)
p = 0.045
Atrialpacing
Ventricularpacing
Time (years)0 2 4 6 8 10
0
0-2
0-4
0-6
0-8
1-0
Mortality as a result of CHF
Overall survival by pacing mode

Study Mean FU Time
Incidence of CHB
Annualized Incidence
Rosenqvist ‘89(review of 28 stud)
3 yrs Median 2.1%Range: 0-11.9%
Median: 0.6%Range: 0-4.5%
Andersen ’97 8 yrs 3.6% 0.6%
Brandt ’92 5 yrs 8.5% 1.8%
Sutton ’86 3 yrs 8.4% 2.8%
Rosenqvist ‘86 2 yrs 4.0% 2.0%
Rosenqvist ’85 5 yrs 3.3% 0.7%
Hayes ’84 3 yrs 3.4% 1.1%
Incidence of persistent AVB in pts paced for SND
Back
grou
nd

StudyPacing Mode
Mean FU
Time
Incidence of AF
Annualized
IncidenceAndersen ’97 AAI 5 years 8.8% 1.8%Sutton ’86 AAI 3 years 4.5% 1.5%Brandt ’92 AAI 5 years 7.0% 1.4%PASE ’98 DDDR
only18
months19.0% 12.7%
CTOPP ’00 DDDRVVIR
3 years 16.6% 5.5% (DDDR)
Incidence of Chronic AFib in pts paced for SND
Back
grou
nd

Is VVI better then DDD ?
Is AAI better then VVI ?

What kills the Patients: the DDD Mode or Inadequate Implantation/
Programming?
Seeking answers, Seeking answers, but what about some but what about some unanswerable questions? unanswerable questions?

Nardi S, AIAC ’08 Poster Abstract
Clinical implication of different pacing modalities Clinical implication of different pacing modalities for reducing unnecessary ventricular pacingfor reducing unnecessary ventricular pacing
METHODSMETHODS • Jan ’04 - Sept ‘07, 910 patients (71+18, M=67%) underwent at DC
PM implant for SND (33%), Parox AVB (39%) or BTS (28%)
Patients (n=910)
Frequency (%)
Sinus node dysfunction
300 33
Persistent or parox. AV block
355 39
Bradycardia-tachycardia syndrome
255 28
Pts (n=910)
(%)
Group 1 - Short AVD (≤150msec)
231 (86%)
25
Group 2 – Long AVD (300msec)
225 (84%)
25
Group 3 – AV hysteresis
212 (88%)
23
Group 4 – AAISafeR
242 (84%)
27

Group 1 Short AVD
Group 2 Long AVD
Group 3 AV hysteresis
Group 4 AAISafeR
P
CP/VP (%)
92.4* 38* 24.6* 4.6 <0.0001
*4 vs(1+2+3)
AF (%)
24.2* 19.4* 16.8* 6.8 <0.001
*4 vs(1+2+3)
HFH (%)
17.6* 14.3* 13.3* 4.7 <0.001
*4 vs(1+2+3)
Nardi S, AIAC ’08 Poster Abstract
Clinical implication of different pacing modalities Clinical implication of different pacing modalities for reducing unnecessary ventricular pacingfor reducing unnecessary ventricular pacing
Close relationship between Cum%VP and AF incidence and HF-H AAIsafeR represent the best pacing modality respect other.
METHODS:METHODS: No statistically differences were observed between these four groups in term of age, sex, NYHA functional class, LVEF and drugs therapy (p=NS)

• Conventional DDD systems often result in a higher level of RVA pacing due to:
– AVD programmed shorter than intrinsic AV conduction
– Lower rate settings higher than necessary
– Rate-responsive algorithms which increase VP in response to stress
• Higher level of Cum %VP in DDDR has adverse long-term effects that mitigate the benefit of AV synchrony.
Sharma AD, HRS `05
DAVID post-hoc analysis
Mean Cum%VP VVI: 3%Mean Cum%VP DDD: 56%

Potential Flaws in RCTs on DDD versus VVI
• PASE: - High cross-over due to pacemaker syndrome in VVIR (intention-to-treat analysis)
• CTOPP: - Patients with low unpaced heart rates benefit from DDD
• MOST: - very high cross-over due to pacemaker syndrome in VVIR
• UKPACE: (inappropriately) short programmed AV delay (75-150 ms)
Ellenbogen AJC 2000;86:59-63
Tang, Circulation 2001;103:3081-5
Toff, NEJM 2005;353:145-55
Link, J Am Coll Cardiol 2004;43:2066-71

Sweeney, Circulation `06
Relationship between mechanical asynchrony and HF development, as derived from various
RANDOMIZED clinical trials
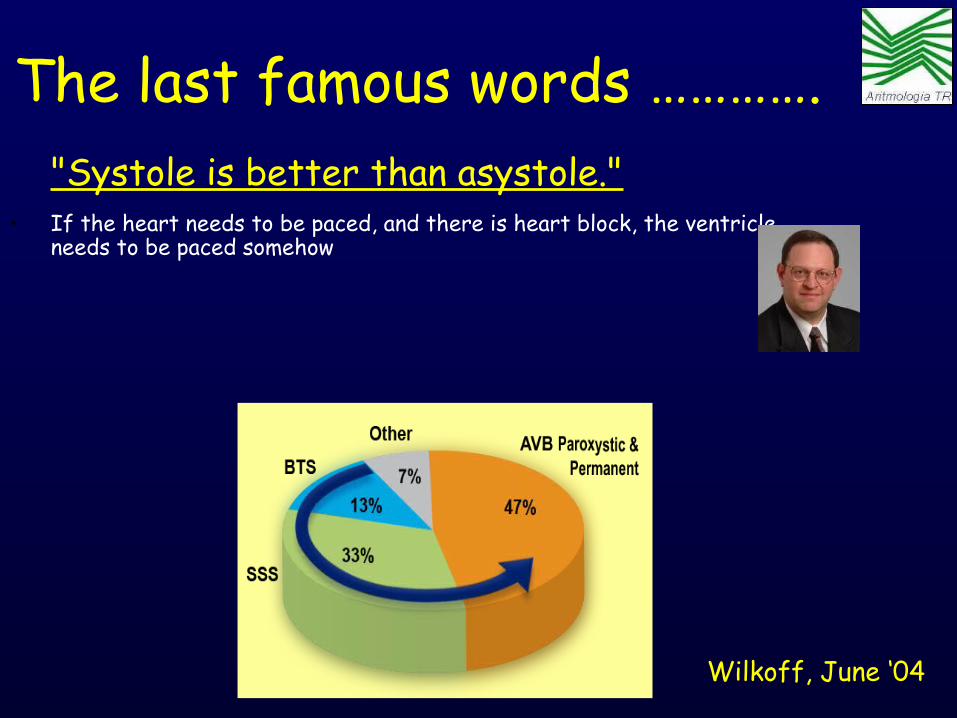
"Systole is better than asystole."• If the heart needs to be paced, and there is heart block, the ventricle
needs to be paced somehow
Wilkoff, June ‘04
The last famous words ………….

Seeking answers, but what about Seeking answers, but what about some unanswerable questions?some unanswerable questions?
Who is the ideal candidate for a pure
RV pacing ?
Are we able to identify pts that will develop a iatrogenic CHF “pace-
mediated”?
None
ON

Why we pace RV apex? – Because the primary objective
was cure symptomatic bradi- cardya due to syncope
– Because this is the common way of treating
– Because actually, standard electro-catheters are projected for an easy and stable positioning in RV apex – Because there were no convincing reasons for stimulate another site

Standard PM indicationStandard PM indication

• Optimizes AV contraction sequence• Reduces pre-systolic mitral regurgitation• Improves atrial preloading of the ventricle• Increases filling time
Mechanism IMechanism IAtrio-Ventricular SynchronyAtrio-Ventricular Synchrony
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy Rationale for CRTRationale for CRT What does pacing changeWhat does pacing change??

• Optimizes ventricular activation• Increases pumping effectiveness• Reduces regional wall stress (WMSI)• Decreases mitral regurgitation• Resynchronizes ventricular filling flows• Decreases filling pressures
Mechanism IIMechanism IIVentricular CoordinationVentricular Coordination
Rationale for CRTRationale for CRT What does pacing changeWhat does pacing change??
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy

LV Conduction Delay: Fusion of E- and A- Waves
Surface ECG
Spectral Doppler Fused E & A waves
Aortic Flow
Fused E & A waves
PR
LVFTLVFT
Aortic Flow
PR
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy
Karloff, PACE ‘87

Synchronizing the Ventricles: Separation of E- and A- Waves
Surface ECG
IVRT IVRT
A-waveA-wave
Aortic Flow
E-waveE-waveSpectral Doppler
PR PR
LVFTLVFT
Aortic Flow
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy
Karloff, PACE ‘87
A New Paradigm for Physiologic Ventricular
Pacing
Sweeney MO, JACC ‘06
Ventricular pacing, not a lack of AV synchrony, is a Ventricular pacing, not a lack of AV synchrony, is a more important predictor of LV dysfunctionmore important predictor of LV dysfunction
The New Goals of Pacing Therapy Maintain normal ventricular activation sequence Maintain normal ventricular activation sequence
whenever possible or pacing in a BV manner whenever possible or pacing in a BV manner

What we can do ?• Try to identifie an “optimal” or a “better” region of VP
where stimulation is able to provide an “hemodinamic effect” or a “mechanical dyssinchrony” that is not so much different from “spontaneous synchronism”
Sweeney MO. JACC ‘06
1– Alternative sites for RV pacing (RVOT, RVS, His)– Bifocal RV pacing – Isolate LV pacing– BV pacing
Pacing at alternative ventricular site(s) to attenuate the adverse effects imposed by ventricular desynchronization when VP can not be avoided and/or abnormal ventricular conduction is already present.
2

What we can do ?Identifie a “better” region where stimulation
is able to provide an “hemodinamic effect” that is not so much different from
“spontaneous synchronism” – Alternative sites for RV pacing (RVOT, RVS, His)– Bifocal RV pacing – Isolate LV pacing– BV pacing

Kass et al, Kass et al, Circulation 99Circulation 99
IntrinsicIntrinsicPacedPaced
00 100100 200200 30030000
4040
8080
120120RV SeptumRV Septum
00 100100 200200 30030000
4040
8080
120120BiventricularBiventricular
00 100100 200200 30030000
4040
8080
120120RV ApexRV Apex
00 100100 200200 30030000
4040
8080
120120LV FreewallLV Freewall
LV Volume LV Volume (mL)(mL)
LV P
ress
ure
LV P
ress
ure
(mm
Hg)
(mm
Hg)
LV P
ress
ure
LV P
ress
ure
(mm
Hg)
(mm
Hg)
LV Volume LV Volume (mL)(mL)
Acute studiesCardiac Resynchronization TherapyCardiac Resynchronization Therapy

RV Bifocal pacing - How it worksRV Bifocal pacing - How it works
RV LV RVRV LV LV
IVS IVS
RV Apical Biventricular RV Bifocal
In accordance with Matsushita and Coll. – Europace 2005; 7, Suppl.; 229 (abs)
Propagation of DEPOLARIZATION
IVS

What we can do ?Identifie a “better” region where stimulation
is able to provide an “hemodinamic effect” that is not so much different from
“spontaneous synchronism” – Alternative sites for RV pacing (RVOT, RVS, His)– Bifocal RV pacing – Isolate LV pacing– BV pacing

‘ALTERNATIVE’ sites of
right Ventricular pacing septal Stimulation (RVS) RVOT stimulation bi-focal stimulation (RVOT + RVA) para-hisian pacing
PARA-HISIAN
Rev Esp Cardiol ‘01
RVS
Lieberman, PACE ‘04
RVOT
Bourke JP, Europace ‘02
BI-SITE

Intrinsic LBBBHis Bundle Pacing
Bifocal RV Pacing
Unipolar RVA Safety Pace (80 ms)
Morina Vazquez, PACE ‘05
Gold MR. JACC ‘99
Rev Esp Cardiol ‘01
Lieberman, PACE ‘04Bourke JP, Europace ‘02

Intrinsic LBBBHis Bundle Pacing
Bifocal RV Pacing
Unipolar RVA Safety Pace (80 ms)
Morina Vazquez, PACE ‘05
‘ALTERNATIVE’ sites of right Ventricular pacing
Gold MR. JACC ‘99

Victor F. JACC ‘99
“No statistical differences (16 pts, 3 mo FU) between two sites of pacing (RVOT vs RVA) for all parameter considered. These results are valid bothg in pts with LVEF >40% that in pts with LVEF <40%.”
Randomized Crossover ROVA Trial (RVA vs RVOT
vs Dual site pacing)
‘’ RVOT and Dual–site pacing reduce QRS duration whereas not improve all other parameters (QOL, LVEF, NYHA, 6-MWT) ‘’
Stambler BS, JCE ‘0380 pts completed RVOT/RVA crossover and 50 pts completed dual site (SUB-STUDY)

Comparison of LV performance (12 pts) during high RVS pacing and RVA pacing after His bundle ablation for refractory Chronic AFib, in pts with mild LV dysfunction
Mera F, PACE ‘99
RVS activation increased the resting first pass LV ejection fraction (0.51 ±0.14vs 0.43 ± 0.10, P <0.01)
APEX
SEPTUM
LV fractional shortening improved during RVS pacing (0.31 ± 0.05 vs 0.26 ± 0.07, P <0.01).
How Right Ventricular How Right Ventricular Septal (RVS) Pacing work ? Septal (RVS) Pacing work ?
High RVOTLow RVOT
High FWLow FW

CARDIAC FUNCTION - Reduction LVEDD - Reduction of LVESD- Improvement FS (fractional shortening) - Improvement of LVEF
18 AF ptsCHF (LVEF<40)
P Deshmukh, Circulation ‘00
PREimpianto
FUP
P.Deshmukh, PACE ‘04
39 AF ptsCHF (LVEF<40)NYHA III IV
FU 42 mo
CARDIAC FUNCTION - Improvement LVEF - Reduction of NYHA- Improvement of DP/dt- Prolonged excercise time- Superior Treppe effect- Improvement Cardio-Pulmon riserve
How para-hisian How para-hisian pacing work ? pacing work ?
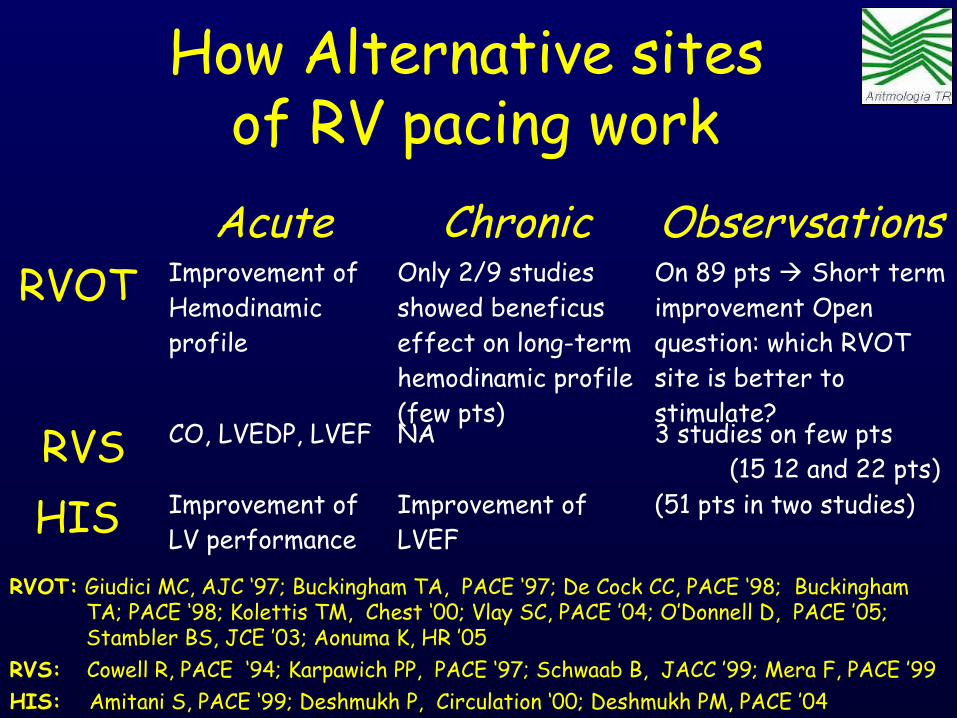
How Alternative sites of RV pacing work
Acute Chronic ObservsationsRVOT Improvement of
Hemodinamic profile
Only 2/9 studies showed beneficus effect on long-term hemodinamic profile (few pts)
On 89 pts Short term improvement Open question: which RVOT site is better to stimulate?
RVS CO, LVEDP, LVEF NA 3 studies on few pts (15 12 and 22 pts)
HIS Improvement of LV performance
Improvement of LVEF
(51 pts in two studies)
RVOT: Giudici MC, AJC ‘97; Buckingham TA, PACE ‘97; De Cock CC, PACE ‘98; Buckingham TA; PACE ‘98; Kolettis TM, Chest ‘00; Vlay SC, PACE ’04; O’Donnell D, PACE ’05; Stambler BS, JCE ’03; Aonuma K, HR ’05 RVS: Cowell R, PACE ‘94; Karpawich PP, PACE ‘97; Schwaab B, JACC ’99; Mera F, PACE ’99 HIS: Amitani S, PACE ‘99; Deshmukh P, Circulation ‘00; Deshmukh PM, PACE ’04


Cumulative Enrollment in C.R. Cumulative Enrollment in C.R. Randomized TrialsRandomized Trials
0
1000
2000
3000
4000
1999 2001 2003 2005Result s Present ed
Cum
ulat
ive
Patie
nts
PATH CHF
MUSTIC SR
MUSTIC AFMIRACLE
CONTAK CD
MIRACLE ICD
PATH CHF II
COMPANION
MIRACLE ICD II
CARE HF
• • Actual � ProjectedActual � ProjectedDOUG SMITHDOUG SMITH
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy

Weight of Evidence: CRT• More than 7000 patients evaluated in
randomized controlled trials• Consistent improvement in QOL, functional
status, and exercise capacity• Strong evidence for reverse remodeling
– ↓ LV volumes and dimensions� ↑ LV ejection fraction– ↓ Mitral regurgitation
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy

2002 Classe IIa: Symptomatic pts, Class NYHA III or IV, DCM (hydiopatic or ischemic) prolonged QRS interval (≥ 130 ms), LVEDD≥ 55 mm, LVEF ≤ 35%.
News 2005Classe I:Symptomatic pts, Class NYHAIII, Synus Rhythm, OMT forCHF, Dyssynchrony
(Level of Evidence A)
Aggiornamento delle linee guida ACC/AHA (2002 2005) →
Terapia CRT
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy

ESC 2005 Classe IIa: Symptomatic pts in NYHA Class III or IV in OMT for CHF, Dyssinchrony and reduced LVEF
ACC/AHA 2005Classe I:Symptomatic pts, Class NYHAIII, Synus Rhythm, OMT forCHF, Dyssynchrony
(Level of Evidence A)
Confronto tra LINEE GUIDA ESC e ACC/AHA (2005)
Terapia CRT
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy
CRT for improve symptoms and CHF-H (Level of Evidence A)
CRT for improve risk of death (Level of Evidence B)

CLASS I SR, LVEF ≤ 35%, QRS > 120ms, NYHA III-IV, OMT
CLASS II
Atiral Fibrillation LVEF ≤ 35%, QRS > 120ms, NYHA III-IV in OMT LVEF ≤ 35%, QRS ≤ 120 ms, NYHA III-IV, OMT Dysshynchronism (Echo), SR, LVEF ≤ 35%, QRS > 120msSymptomatic NYHA class II, PM or ICD indication (in primary prevention) Chronic RVA pacing, LVEF ≤ 35%, NYHA III-IV, OMT, Severe Dyssynchronism (Up-grading),
Cardiac Resynchronization TherapyCardiac Resynchronization Therapy
LINEE GUIDA AIAC 2006CRT

Background: Linee Guida
A seguito della pubblicazione degli studi Companion e Care-HF, le linee guida Europee (ESC) ed Americane (ACC/AHA) hanno introdotto la
CRT come Terapia di classe I per pazienti con:• Scompenso Cronico in classe III NYHA o IV stabile,
nonostante terapia medica ottimale• FE ≤ 35%• QRS ≥ 120 ms• Ritmo sinusale solo per ACC/AHA
Swedberg K et al, European Heart Journal (2005) 26, 1115–1140Hunt S A et al, Circulation. 2005;112

Background: Linee GuidaCRT come Terapia di classe II per pazienti con:
• FA, scompenso cronico in classe III o IV NYHA stabile, nonostante terapia medica ottimale, FE ≤ 35% e dissincronia ventricolare (QRS > 120 msec) ;
• FE ≤ 35%, QRS ≤ 120 msec e dissincronia ventricolare ECO documentata, scompenso cronico in classe III o IV NYHA stabile, nonostante terapia medica ottimale;
• Classe NYHA II con indicazione alla stimolazione ventricolare e/o ad ICD profilattico, in RS, QRS ≥ 120 ms, FE ≤ 35%;
• Stimolazione ventricolare destra, scompenso cronico in classe III o IV NYHA stabile, nonostante terapia medica ottimale, FE ≤ 35% e dissincronia ventricolare (upgrade)
Swedberg K et al, European Heart Journal (2005) 26, 1115–1140 Hunt S A et al, Circulation. 2005;112

Terapia Resincronizzante CardiacaLa CRT utilizzando un BVP, può essere considerata in pts
con ridotta FE e dissincronia ventrioulare (QRS width>120 ms), che rimangono simtomatici (NYHA III–IV) malgrado
una terapia farmacologica ottimale, per migliorare:
i sintomi(Classe di raccomandazione I, livello di evidenza A)
le ospedalizzazioni(Classe di raccomandazione I, livello di evidenza A)
e la mortalità (Classe di raccomandazione I, livello di evidenza B)

New section: Gaps in evidence• 'In pts with HF and a wide QRS complex, which pt
characteristics should lead to a CRT-D being preferred over a CRT-P?'
• 'Is there any role for ECHO assessment of dyssynchrony in the selection of pts for CRT?'
• 'Does CRT improve clinical outcomes in pts with a low LVEF, wide QRS but mild symptoms (NYHA class II)?'
• 'Does CRT improve clinical outcomes in pts with a low LVEF, severe symptoms (NYHA class III/IV) and a QRS width <120 ms?'
• 'Does an ICD improve clinical outcomes in HF with an EF >35%?'
• 'What aspects of remote monitoring might best detect early decompensation?'
REVERSE not published
in time!
RethinQ
Good question...
PROSPECT
SENSE-HF?
ICD e CRT
L’impianto di un ICD in combinazione con pacing bi-ventricolare, può essere considerato in pazienti che rimangono sintomatici, con HF grave (classe NYHA
III–IV), con FE ≤ 35% e durata del QRS >120 ms, per migliorare morbidità e/o mortalità
(Classe di raccomandazione IIa, livello di evidenza B)

New ESC HF Guidelines 08

New guidelines launched 30/8
• Great hush-hush before launch– ESC members
embargoed• Major launch event at
ESC– Dickstein– Priori– Focus sessions on
different aspects of the guidelines

Positive aspects of new guidelines
• One set of HF guidelines to use for all international MDT materials– Same citations for CRT and ICD recommendations
• Clearer language used this time• Clearer cut-off points• More diagrams• More focus on collaboration

New: Standardised wordingsClass of
recommendationRecommended wording
IIs recommendedIs indicated
IIa Should be considered
IIb May be considered
III Is not recommended

• 'CRT-P is recommended to reduce morbidity and mortality in pts in NYHA III-IV class who are symptomatic despite OMT, and who have a reduced EF (LVEF <35%) and QRS prolongation (QRS width >120 ms)'Class 1 level A
New guidelines: CRT v CRTD• 'CRT with ICD function is
recommended to reduce morbidity and mortality in pts in NYHA III-IV class who are symptomatic despite OMT, and who have a reduced EF (LVEF <35%) and QRS prolongation (QRS width >120 ms)'Class 1 level A
Dickstein et al. Eur Heart J. 2008. DOI:10.1093/eurheartj/ehn309
New guidelines: CRT v CRTD
'The survival advantage of CRT-D vs CRT-P has not been adequately addressed. Due to the documented effectiveness of ICD therapy in the prevention of SCD, the use of a CRT-D device is commonly preferred in clinical practice in pts satisfying CRT criteria including an expectation of survival with good functional status for >1 year'Class of recommendation I, level of evidence A
Dickstein et al. Eur Heart J. 2008. DOI:10.1093/eurheartj/ehn309
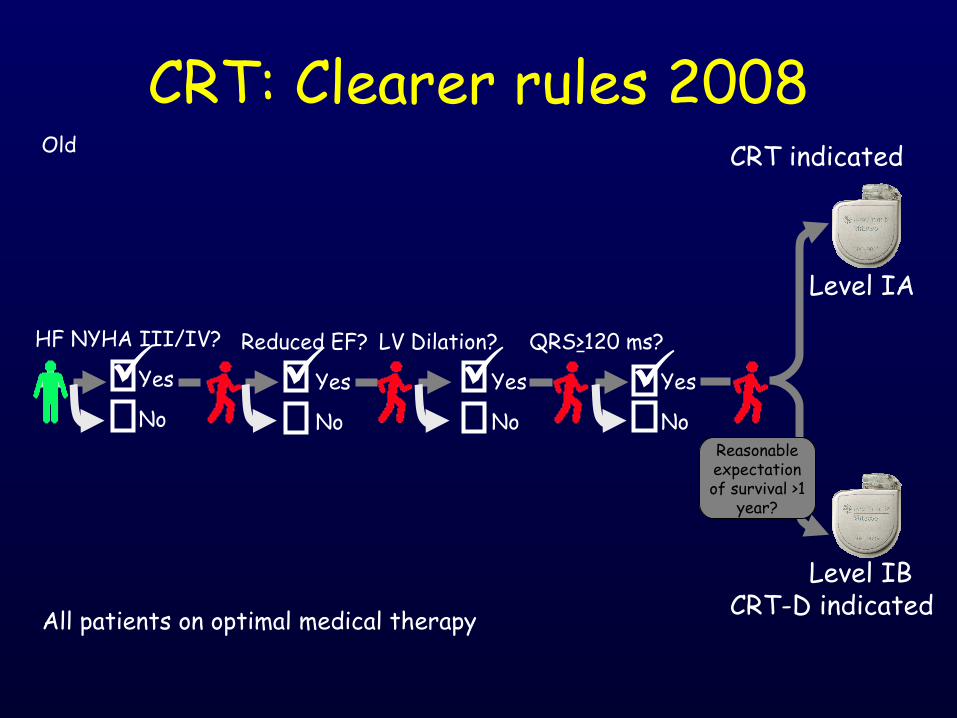
CRT indicated
HF NYHA III/IV?
Yes
No
Level IA
QRS>120 ms?
Yes
No
Reduced EF?
Yes
No
Level IBCRT-D indicatedAll patients on optimal medical therapy
LV Dilation?
Yes
No
Reasonable expectation of survival >1
year?
CRT: Clearer rules 2008Old

CRT indicated
HF NYHA III/IV?
Yes
No
Level IA
QRS>120 ms?
Yes
No
EF <35%?
Yes
No
Level IACRT-D indicatedAll patients on optimal medical therapy
Reasonable expectation of survival >1
year?
CRT: Clearer rules 2008New
Dickstein et al. Eur Heart J. 2008. DOI:10.1093/eurheartj/ehn309

CRT: role of echo
Dickstein et al. Eur Heart J. 2008. DOI:10.1093/eurheartj/ehn309

Reduced LV function?
Yes
No
Sustained ventricular tachycardia?
Yes
No
Experienced a cardiac arrest
Yes
No
ICD indicated
Level IA
Level IA
All patients on optimal medical therapy with life expectancy >1 year
ICD: Clearer rules 2008Old

LV EF <40%?
Yes
No
Documented haemodynamically unstable VT and/or VT with syncope?
Yes
No
Survivor of ventricular fibrillation?
Yes
No
ICD indicated
Level IA
All patients on optimal medical therapy with life expectancy >1 year
ICD: Clearer rules 2008
Level IA
New

ICD: Clearer rules 2008
>40 days past MI?
Yes
No
Nonischaemic heart disease?
Yes
No
EF ≤30-35%?
Yes
No
EF ≤30-40%?
Yes
No
Level IA
NYHA II/III
Yes
No
ICD indicated
Level IA
All patients on optimal medical therapy with life expectancy >1 year
Old
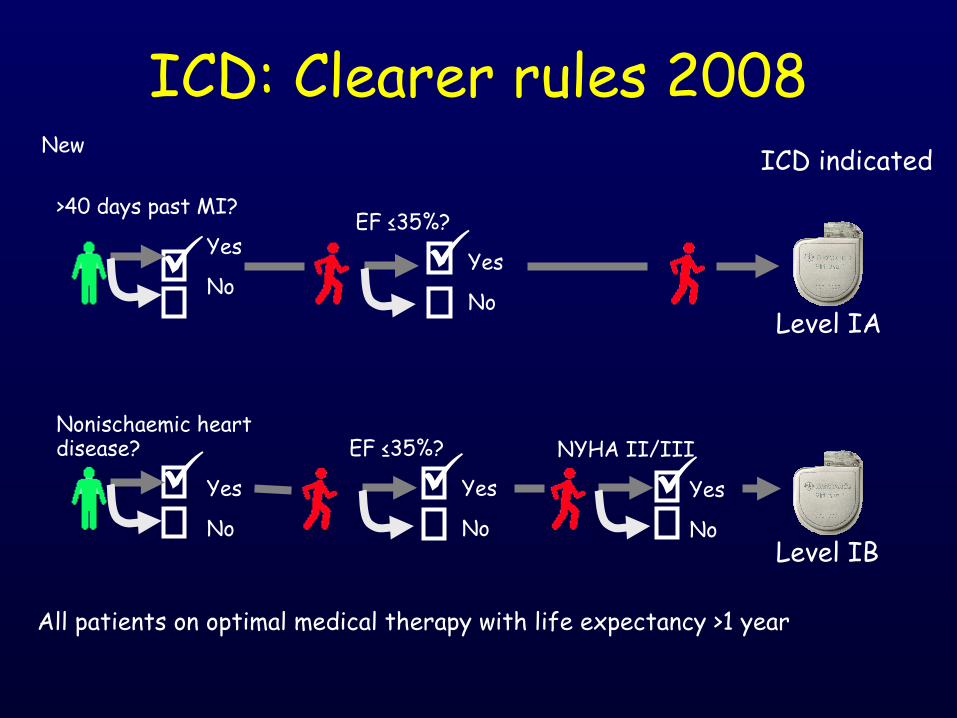
ICD: Clearer rules 2008
>40 days past MI?
Yes
No
Nonischaemic heart disease?
Yes
No
EF ≤35%?
Yes
No
EF ≤35%?
Yes
No
Level IA
NYHA II/III
Yes
No
ICD indicated
Level IB
All patients on optimal medical therapy with life expectancy >1 year
New

ICD in primary prevention'Data on the role of ICD in pts with non-ischaemic DCM are limited. The SCD-HeFT trial enrolled pts with both DCM and ischaemic LV dysfunction and showed a 23% reduction in mortality. A meta-analysis* of trials enrolling only non-ischaemic DCM pts showed a 25% reduction in mortality in the group of pts receiving an ICD (p=0.003). These data suggest that the aetiology of HF may not justify a different approach for the primary prevention of SCD.
* Desai 2004. JAMA 292:2874Dickstein et al. Eur Heart J. 2008. DOI:10.1093/eurheartj/ehn309
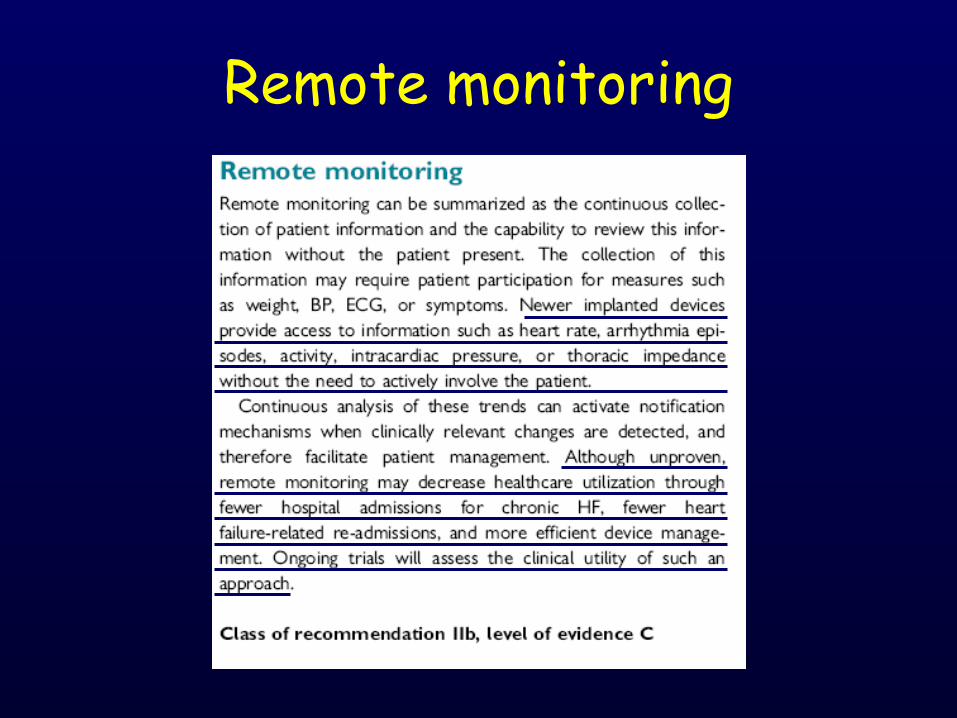
Remote monitoring

Notable in the new guidelines
• No range of EF; all <35%• SCD-HeFT patients recommendations now 1B• Devices for NYHA I not in guidelines
– Post MI– NICM EF <30%
• CRTP and CRTD both have Class IA
Dickstein et al. Eur Heart J. 2008. DOI:10.1093/eurheartj/ehn309
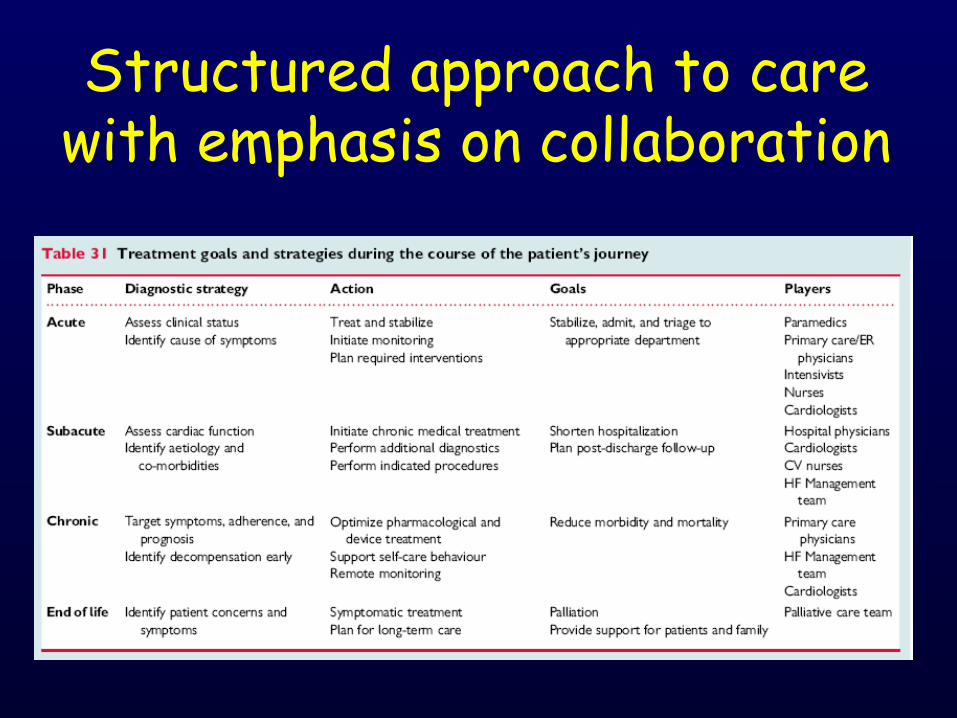
Structured approach to care with emphasis on collaboration

TerapiaTerapia
Publicazioni scientifiche
• I risultati I risultati possono essere possono essere confrontati con confrontati con dati storicidati storici
Registry
Risultati “real life”
Clinical PracticeValutazione del grado di
accettazione degli studi randomizzati nella pratica clinica
Collezione prospettica di dati clinici in pts che hanno già un PM impiantato
Valutazione dei benefici dell’utilizzo di funzioni specifiche del PM (es impatto di alcuni algoritmi funzionali su specifici “end-point”)
Ipotesi, gruppi di CTR,
valutazioni economiche
CLINICAL Practice VS Registries

TerapiaTerapia
• Obbligatorietà criteri di selezione pazienti
• Uniformità procedure
• Follow-up ed esami di controllo definiti
• Predeterminazione e condivisione dei criteri
di valutazione
Randomized Trials
Pubblicazioni scientifiche
Risultati “real life”
Ipotesi, gruppi di CTR,
valutazioni economiche
CLINICAL Practice VS RANDOMIZED Trials
Courtesy of Dr. Botto
Clincal Practice• Criteri di selezione dei
pts non obbligatori
• Procedure, Follow-up ed esami secondo le
abitudini dei centri
• Criteri di valutazione più soggettivi (giudizio del
medico e/o del pts)

Scientific Paper
• Results coud be Results coud be matched with matched with hystorical hystorical clinical data clinical data
Registry
“Real life” results
Clinical PracticeAcceptance degree of
randomized studies in clinical practice
Prospectic data retrived of clinical aspects in pts already implanted with a PM
Evaluation of clinical benefits due to specific PM functions (ex. Impact of special modality on several specific “end-point”)
Hp, Control groups, economic evaluation
CLINICAL Practice VS Registries
Courtesy of Dr. Botto
TherapyTherapy

Collezione prospettica di dati clinici in pazienti che hanno un pacemaker già impiantato
Ruolo dei Registri nella Pratica Clinica
Courtesy of Dr. Botto
Valutazione dei benefici dell’utilizzo di funzioni specifiche del pace-maker (ad es.:impatto di un determinato algoritmo su alcuni “end point” con CHF, HF-H, AFib …)
Fotografia “Real life” della nostra routine clinica

TherapyTherapy
• Specific pts selection criteria
• Uniformity of clinical procedure
• Well defined Follow-up and clinical exams
• Pre-determined and sharing of evaluation
criteria
Randomized Trials
Scientifc Papers
“Real life” results
Hp, Control group,
economic evaluation
CLINICAL Practice VS RANDOMIZED Trials
Courtesy of Dr. Botto
Clinical Practice• Pts selection criteria
not mandatory
• Procedure, Follow-up and exams according to centre clinical practice
• Evaluation criteria according to physician
and/or pts point of view