2010 aha changes - cabell huntington...
TRANSCRIPT

2010 AHA BLS, 2010 AHA BLS, ,,ACLS & PALS ACLS & PALS
Changes: Changes: Changes: Changes: What’s New?What’s New?What s New?What s New?
Jennifer Murray MSN, RNJennifer Murray MSN, RNCritical Care Educator Critical Care Educator
AHA T i i C t C di tAHA T i i C t C di tAHA Training Center CoordinatorAHA Training Center CoordinatorPALS Regional FacultyPALS Regional Faculty
ACLS Training Center FacultyACLS Training Center Faculty

ObjectivesObjectivesObjectivesObjectives• This module will only cover the • This module will only cover the
changes in BLS, ACLS & PALS from the 2005 to 2010 guidelinesthe 2005 to 2010 guidelines.
• By the end of this program, the learner should:learner should:–Be able to state the changes made in
emergency cardiovascular care emergency cardiovascular care algorithms

2010 Highlights of 2010 Highlights of BLSBLS2010 Highlights of 2010 Highlights of BLSBLS• Look, listen and feel removed from the Look, listen and feel removed from the
algorithm due to delays in CPR• Early activation of EMSa y act at o o S• High quality CPR• Minimize compression interruptionsMinimize compression interruptions• De-emphasis on pulse checks during CPR
due to interrupting CPRdue to interrupting CPR• Cricoid pressure no longer recommended
for use with ventilation

BLSBLSBLSBLS• CAB not ABC• CAB not ABC• Chest compressions, Airway,
Breathing (CAB)Breathing (CAB)• Most arrests are adults and most
i VF/VTsurvivors are VF/VT• Emphasis on performing high quality
CPR and early defibrillation• Delay in ‘C’ when attempting ‘A’y p g


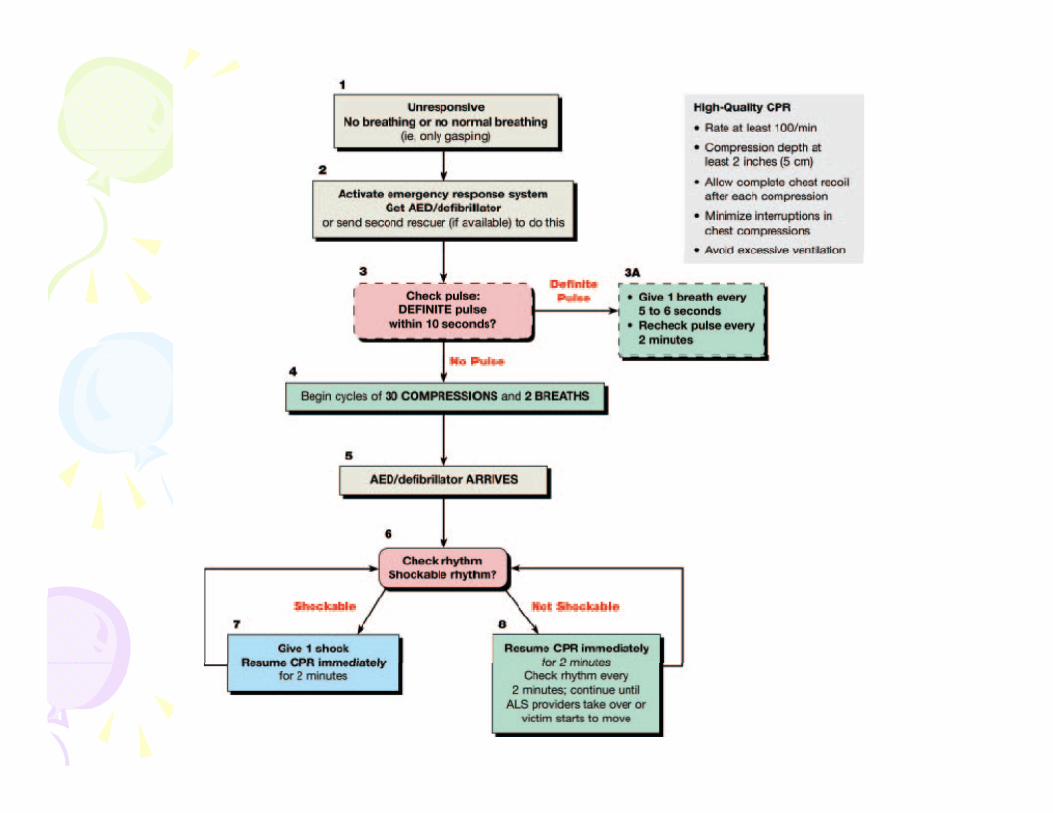
BLSBLSBLSBLS• New science indicates the following order New science indicates the following order
for Healthcare providers:– Check the pt. for responsiveness &
presence/absence of breathing or gasping– Call for help
Ch k th l f th 10 d– Check the pulse for no more than 10 seconds– Give 30 compressions– Open airway and give 2 breaths/ventilations– Open airway and give 2 breaths/ventilations– Resume compressions

BLSBLSBLSBLS• Take no longer than 10 seconds• Take no longer than 10 seconds
to check for a pulse. If no pulse detected within 10 seconds begin detected within 10 seconds, begin chest compressions!!!
• Compression rate at least • Compression rate at least 100/minute, so each set of 30 compressions should take ~18 compressions should take ~18 seconds or less.

BLSBLSBLSBLS• 30 compressions : 2 breaths• 30 compressions : 2 breaths• Compression depth:
Ad lt At l t 2 i h (5 )–Adults: At least 2 inches (5cm)–Children: At least 1/3 depth of the
chest 2 inches (5 cm)chest, ~2 inches (5 cm)– Infants: At least 1/3 depth of the
chest ~1 5 inches (4 cm)chest, ~1.5 inches (4 cm)

BLSBLSBLSBLS


2010 Highlights of 2010 Highlights of ACLSACLSChangesChangesChangesChanges
• Successful ACLS is predicated on good Successful ACLS is predicated on good BLS– High quality CPR with minimal interruptionsg– Early defibrillation
• Fifth link in “Chain of Survival”: Post Cardiac Arrest Care– Multidisciplinary care from BLS to discharge for
good neurologic outcomegood neurologic outcome• Qualitative waveform Capnography

ACLS: Airway & BreathingACLS: Airway & BreathingACLS: Airway & BreathingACLS: Airway & Breathing• Continuous quantitative capnography Continuous quantitative capnography
is now recommended for intubated patients throughout the peri-arrest p g pperiod.
• Capnography is also recommended p g p yfor confirmation of ETT placement & for monitoring CPR– If PETCO2 is <10 mmHg, then attempt
to improve CPR quality

ACLS: Airway & BreathingACLS: Airway & BreathingACLS: Airway & BreathingACLS: Airway & Breathing• ETCO2 Capnography:• ETCO2 Capnography:
–Persistently low PETCO2 values <10 mmHg during CPR in the intubated mmHg during CPR, in the intubated patient, suggest that Return of Spontaneous Circulation (ROSC) is p ( )unlikely
– If PETCO2 abruptly increases to normal value of 35-40 mmHg, it is reasonable to consider this an indicator of ROSC

ACLS: Airway & BreathingACLS: Airway & BreathingACLS: Airway & BreathingACLS: Airway & Breathing• Once ROSC occurs arterial • Once ROSC occurs, arterial
oxyhemoglobin saturation should be monitored and titrate O2 to monitored, and titrate O2 to maintain this to >94%
• Supplementary O2 is not needed for • Supplementary O2 is not needed for pts. without evidence of respiratory distress or when oxyhemoglobin distress or when oxyhemoglobin saturation is >94%

ACLS: PharmacologyACLS: PharmacologyACLS: PharmacologyACLS: Pharmacology• Atropine is NOT recommended for Atropine is NOT recommended for
routine use in PEA/asystole and has been removed from the algorithm!!!g
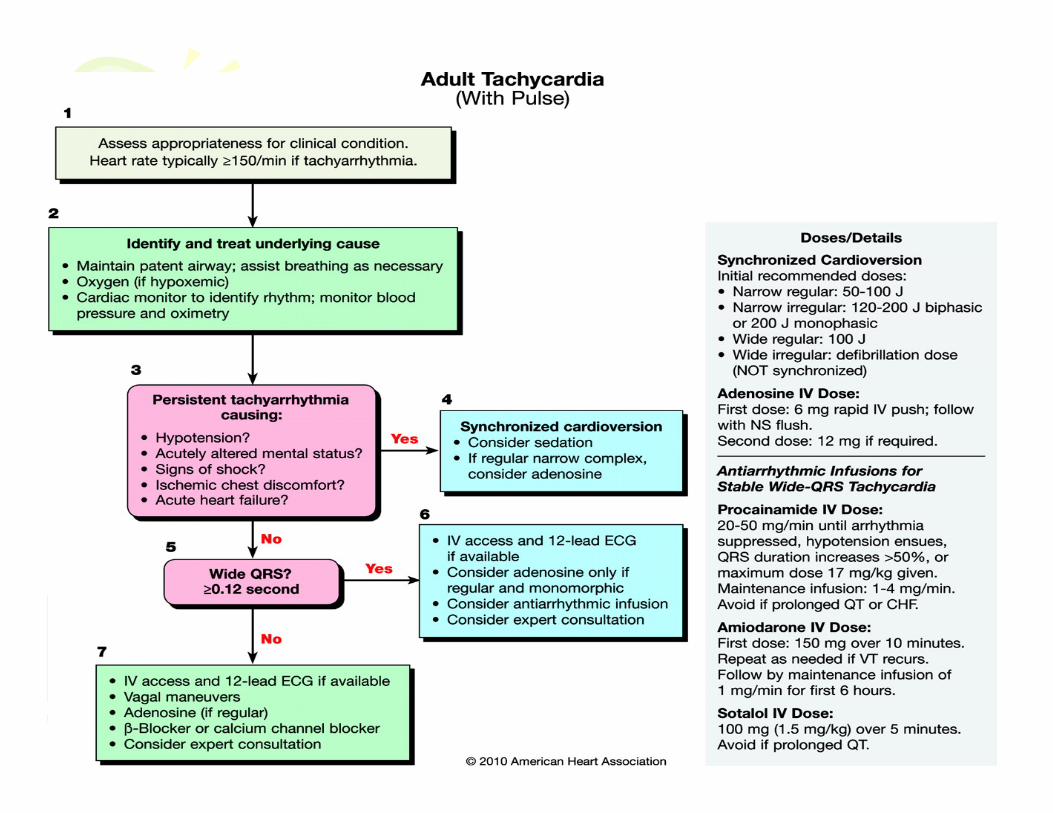
• Adenosine may be considered in the initial diagnosis of stable, g ,unidifferentiated, regular, monomorphic, wide-complex t h di tachycardia –Do not use if pattern is irregular

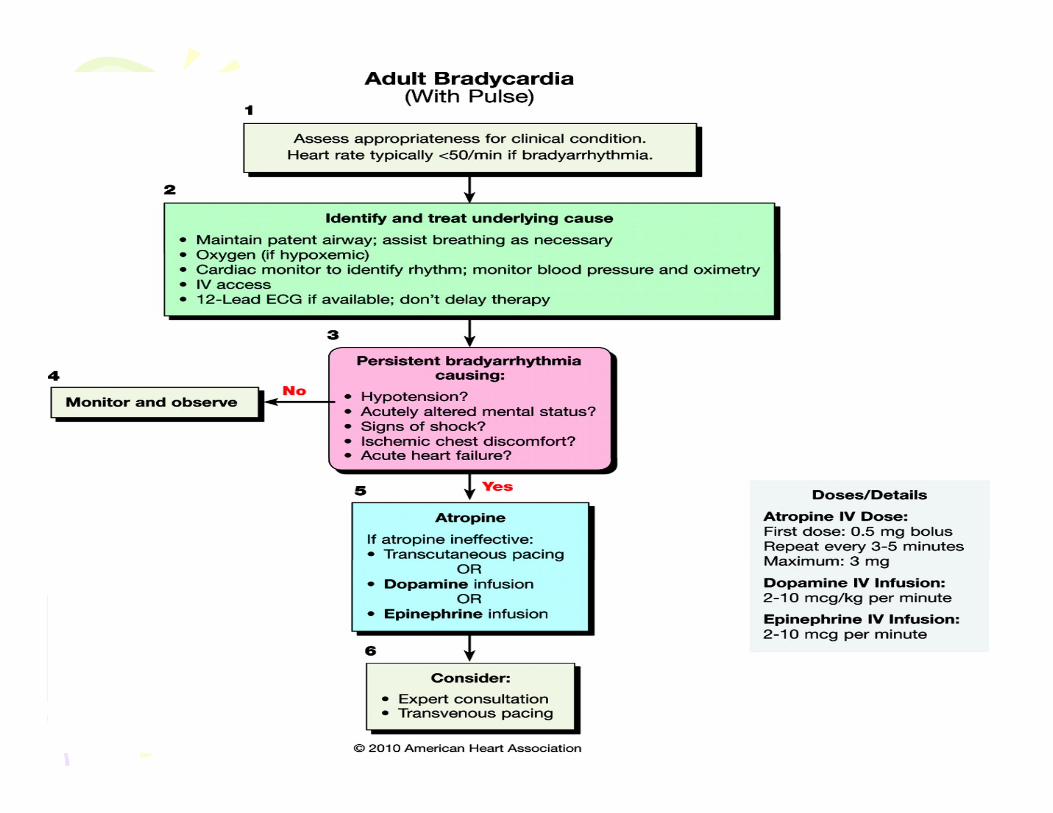
ACLS: PharmacologyACLS: PharmacologyACLS: PharmacologyACLS: Pharmacology• For treatment of symptomatic & • For treatment of symptomatic &
unstable bradycardia, chronotropic drug infusions are recommended as drug infusions are recommended as an alternative to pacing (dopamine or epinephrine drip)or epinephrine drip)
• Morphine should be given with caution to patients with unstable caution to patients with unstable angina

ACLS: ACLS: Defibrillation/CardioversionDefibrillation/CardioversionDefibrillation/CardioversionDefibrillation/Cardioversion
• Cardioversion• Cardioversion–A. fib…120-200J biphasic and 200J
monophasicmonophasic–A flutter & other supraventricular…50-
100J biphasic and monophasic (requires 100J biphasic and monophasic (requires less energy than a fib)
**If the initial cardioversion shock fails, ,providers should increase the dose in a stepwise fashion
ACLS: ACLS: Defibrillation/CardioversionDefibrillation/CardioversionDefibrillation/CardioversionDefibrillation/Cardioversion
• Monomorphic V tach• Monomorphic V tach–Cardioversion…Initial energy of 100J in
biphasic and monophasicbiphasic and monophasic– If no response to initial shock, then
increase dose in a stepwise fashionincrease dose in a stepwise fashion



ACLS: Post Resuscitation ACLS: Post Resuscitation CareCareCareCare
• New Section aimed @ improving survival New Section aimed @ improving survival after ROSC returns include:– Optimizing cardiopulmonary function & vital g
organ (brain and heart) perfusion– Transporting out of hospital arrest to facility
with acute coronary interventions neurologic with acute coronary interventions, neurologic care, goal directed critical care & hypothermia
– Transporting in hospital arrest to the critical p g pcare unit capable of providing comprehensive post cardiac arrest care

CONTCONTCONT.CONT.– IDing and treating the causes of the arrest and g g
preventing recurrence– Considering therapeutic hypothermia to
optimize survival and neurological recovery in optimize survival and neurological recovery in comatose patients
– IDing and treating acute coronary syndromesO ti i i h i l til ti t i i i – Optimizing mechanical ventilation to minimize lung injury
– Gathering data for prognosisg p g– Assisting patients & families with rehabilitation
services if needed

ACLS: Post Cardiac Arrest ACLS: Post Cardiac Arrest CareCareCareCare
• Critical actions for post-cardiac arrest Critical actions for post cardiac arrest care:– Hemodynamic optimization, including a focus g
on treating hypotension– Acquisition of 12 lead ECG
I d ti f th ti h th i– Induction of therapeutic hypothermia– Monitoring advanced airway placement &
ventilation status with quantitative waveform ventilation status with quantitative waveform capnography in intubated patients
– Optimizing arterial oxygen saturation


ACLS:BradycardiaACLS:BradycardiaACLS:BradycardiaACLS:Bradycardia• Heart rate parameter is now <50 • Heart rate parameter is now <50
bpm• Always assess clinical condition• Always assess clinical condition• Atropine is 1st line treatment• Chronotropic drug IV infusion is
equally as effective to external transcutaneous pacing when atropine is ineffective
ACLS: Tachycardia with a ACLS: Tachycardia with a PulsePulsePulsePulse
• Adenosine:• Adenosine:–1st dose = 6 mg IVP; 2nd dose = 12 mg
IVPIVP–Reduce initial dose to 3mg if pt. has CVL–Does NOT convert a fib a flutter or –Does NOT convert a fib, a flutter or
Vtach

2010 Highlights of 2010 Highlights of PALS PALS ChangesChangesChangesChanges

PALS: Airway and BreathingPALS: Airway and BreathingPALS: Airway and BreathingPALS: Airway and Breathing• Once circulation is restored, monitor ,
oxyhemoglobin saturation. Titrate O2 to maintain >94%. **An oxyhemoglobin saturation of 100% is generally an indication to wean the FiO2.g y
• Exhaled CO2 detection is recommended in addition to clinical assessment to confirm ETT placement in neonates infants & children with a placement in neonates, infants & children with a perfusing cardiac rhythm in all settings (prehospital, ED, ICU, ward, OR)
• Cricoid pressure is not routinely recommended • Cricoid pressure is not routinely recommended during Intubation.

PALS: DefibrillationPALS: DefibrillationPALS: DefibrillationPALS: Defibrillation• Initial dose for defibrillation is now 2-• Initial dose for defibrillation is now 2
4 J/kg, instead of starting at 2 J/kg• For refractory vfib it is reasonable to • For refractory vfib, it is reasonable to
increase the dose to 4 J/kgS b t l l h ld b t –Subsequent energy levels should be at least 4 J/kgHigh levels (not to exceed 10 J/kg or –High levels (not to exceed 10 J/kg or adult max dose) may be considered

PALS: ECGPALS: ECGPALS: ECGPALS: ECG
• Wide complex tachycardia is present if the QRS width is >0 09 secondif the QRS width is >0.09 second
PALS: PharmacologyPALS: PharmacologyPALS: PharmacologyPALS: Pharmacology• Routine calcium administration is NOTout e ca c u ad st at o s O
recommended for pediatric cardiopulmonary arrest in the absence of documented hypocalcemia calcium documented hypocalcemia, calcium channel blocker OD, hypermagnesemia or hyperkalemiayp
• Etomidate has been shown to facilitate ETT intubation in infants/children with
i i l h d i ff t b t it i minimal hemodynamic effect, but it is NOT recommended for use in ped patients with evidence of septic shockwith evidence of septic shock

PALS: Post Cardiac Arrest PALS: Post Cardiac Arrest CareCareCareCare
• Although there have been no published g presults of prospective randomized pediatric trials of therapeutic hypothermia, based on adult evidence, therapeutic based o adu t e de ce, t e apeut chypothermia (32 degrees C – 34 degrees C) may be beneficial for adolescents who remain comatose after resuscitation from remain comatose after resuscitation from sudden witnessed out of hospital vfib
• Therapeutic hypothermia may also be considered for infants and children who considered for infants and children who remain comatose after resuscitation from cardiac arrest




WHY?????WHY?????WHY?????WHY?????

2010 AHA Changes FAQs2010 AHA Changes FAQs2010 AHA Changes FAQs2010 AHA Changes FAQs• Why did the CPR sequence change from A-B-y q g
C to C-A-B?– 1st, this change allows rescuers to begin chest
compressions right away. As we know, most victims of sudden cardiac arrest (SCAs) receive no bystander CPR. Opening the airway is the most difficult and daunting task for the rescuer. The change attempts to decrease the barriers to performing CPR by allowing the rescuer the barriers to performing CPR by allowing the rescuer to start with chest compressions.
– 2nd, the vast majority of SCAs occur in adults who suffer a witnessed arrest & vfib or pulseless vtach. In these pts, the critical elements of CPR are chest compressions and early defibrillation.

FAQsFAQsFAQsFAQs• Why do the 2010 Guidelines put so much y p
emphasis on chest compressions?– Compressions provide vital blood flow to the heart &
brain during SCA, and research shows that delays or interruptions to compressions reduced survival rates.
– Ventilations are not as critical, as victims have O2 remaining in their lungs & bloodstream for the 1st few minutes of an SCA Starting CPR with chest minutes of an SCA. Starting CPR with chest compressions can pump that blood to the victim’s brain & heart sooner.
– Compressions should be started ASAP, and interruptions Compressions should be started ASAP, and interruptions in chest compressions should be minimized throughout the entire resuscitation period.
FAQsFAQsFAQsFAQs• What are the key recommendations for y
healthcare professionals?– Effective teamwork techniques should be learned &
practiced regularly– Professional rescuers should use quantitative waveform
capnography – the monitoring of CO2 output – to confirm intubation & monitor CPR qualityTh ti h th i li h ld b t f – Therapeutic hypothermia, or cooling, should be part of an overall interdisciplinary system of care after resuscitation from cardiac arrest.
– Atropine is no longer recommended for routine use in Atropine is no longer recommended for routine use in managing & treating pulseless electrical activity (PEA) or asystole

ReferencesReferencesReferencesReferences• 2010 comparison charts American • 2010 comparison charts. American
Heart Association.• AHA Advanced cardiovascular life • AHA. Advanced cardiovascular life
support: Provider manual. 2011.