2010 ubo/ubu conference health budgets & financial policy 111 briefing: common coding pitfalls...
TRANSCRIPT

2010 UBO/UBU Conference
Health Budgets & Financial Policy
111
Briefing: Common CodingPitfalls Impacting MS-DRGs
Date: 24 March 2010
Time: 1300–1350

2010 UBO/UBU ConferenceTurning Knowledge Into Action
22
Objectives
Foster greater understanding about MS-DRGs– Background– Weighted value (TRICARE)
Identify Common Coding Pitfalls Discuss Rescue Attempts Summation
2010 UBO/UBU ConferenceTurning Knowledge Into Action
3
MS-DRGs Background
Military Health System (MHS) adopted the Medicare Severity-DRGs effective 1 October 2008 (FY09).
TRICARE/CHAMPUS DRG uses– MS-DRG logic– MS-DRG assignment for SIDR
DoD assigned weightshttp://www.tricare.mil/drgrates/
– TRICARE MS-DRG
2010 UBO/UBU ConferenceTurning Knowledge Into Action
44
MS-DRGs Background (cont’d)
Evolution brought change and new terminology.– Increased number of DRGs– Revised CC listing– Created MCCs– Hospital-Acquired Conditions (HACs)– Present on Admission (POA) indicator
Under the MS-DRGs, the severity of a patient’s illness must be more accurately documented in order for the hospital to be reimbursed appropriately for the care provided.
4

2010 UBO/UBU ConferenceTurning Knowledge Into Action
55
MS-DRG Terminology
MS-DRG: Medicare Severity-Based Diagnosis Related Groups Complexity: Differences in resource needs that are not
diagnosis-related – Heart assist devices– Organ transplants– Bone marrow transplants– Tracheostomy
CC: A secondary diagnosis determined to be a complication or co-morbidity in relationship to the principal diagnosis
MCC: A secondary diagnosis determined to be a complication or co-morbidity which exceeds the resource use of the standard CC
2010 UBO/UBU ConferenceTurning Knowledge Into Action
66
DRGs vs. MS-DRGs
DRGs split – Age– With CC– Without CC
MS-DRGs split – Tiers– Presence or absence of CC– If present, is CC “major” (MCC) or not? – Could result in up to three tiers of payment
Absence of CC Presence of CC Presence of MCC
6

2010 UBO/UBU ConferenceTurning Knowledge Into Action
77
MS-DRGs – Assignment to Severity Tiers
Severity and weight increase with each tier Severity tier depends on secondary diagnosis
MS-DRG Description Weight (FY10)291 Heart Failure and shock w/MCC 1.4872292 Heart Failure and shock w/CC 0.9164 293 Heart Failure and shock w/o CC/MCC 0.7176
If none of the secondary diagnoses codes are MCCs or CCs, the MS-DRG w/o CC/MCC is assigned.
MCCs take precedence over CCs.
Only one CC or MCC code is needed for assignment to a specific MS-DRG. BUT, DON’T STOP there!

2010 UBO/UBU ConferenceTurning Knowledge Into Action
8
Initial Split: TRICARE MS-DRG in 2009
014 Intracranial Hemorrhage or Cerebral Infarction
1.3807
064 Intracranial Hemorrhage or Cerebral Infarction w/MCC
2.4223
065 Intracranial Hemorrhage or Cerebral Infarction w/CC
1.3422
066 Intracranial Hemorrhage or Cerebral Infarction w/o CC/MCC
1.0291
8
FY09
Note: Comparison is FY08 DRG w/ FY09 MS-DRG.
FY08
2010 UBO/UBU ConferenceTurning Knowledge Into Action
9
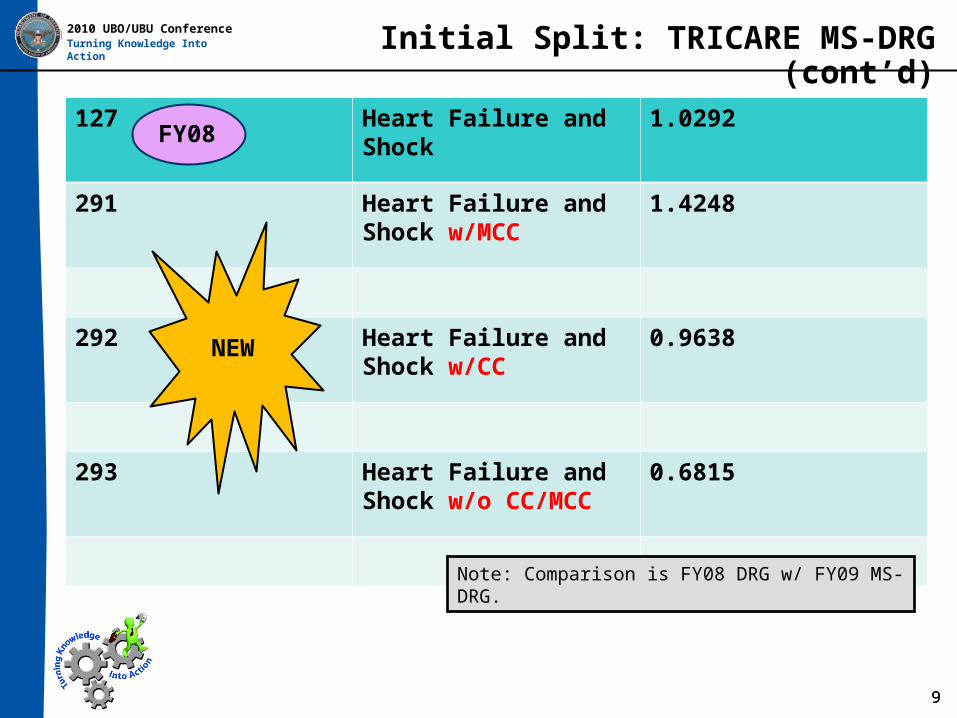
Initial Split: TRICARE MS-DRG (cont’d)
127 Heart Failure and Shock
1.0292
291 Heart Failure and Shock w/MCC
1.4248
292 Heart Failure and Shock w/CC
0.9638
293 Heart Failure and Shock w/o CC/MCC
0.6815
9
NEW
Note: Comparison is FY08 DRG w/ FY09 MS-DRG.
FY08

2010 UBO/UBU ConferenceTurning Knowledge Into Action
10
TRICARE MS-DRG 2008 / 2009 / 2010
078 PulmonaryEmbolism
1.1580
175 PulmonaryEmbolismw/ MCC
1.5659 1.3731
176 PulmonaryEmbolismw/o MCC
1.0013 0.9910
10
NEW
Notice adjustment from FY09 to FY10
FY08 FY09 FY10
2010 UBO/UBU ConferenceTurning Knowledge Into Action
11
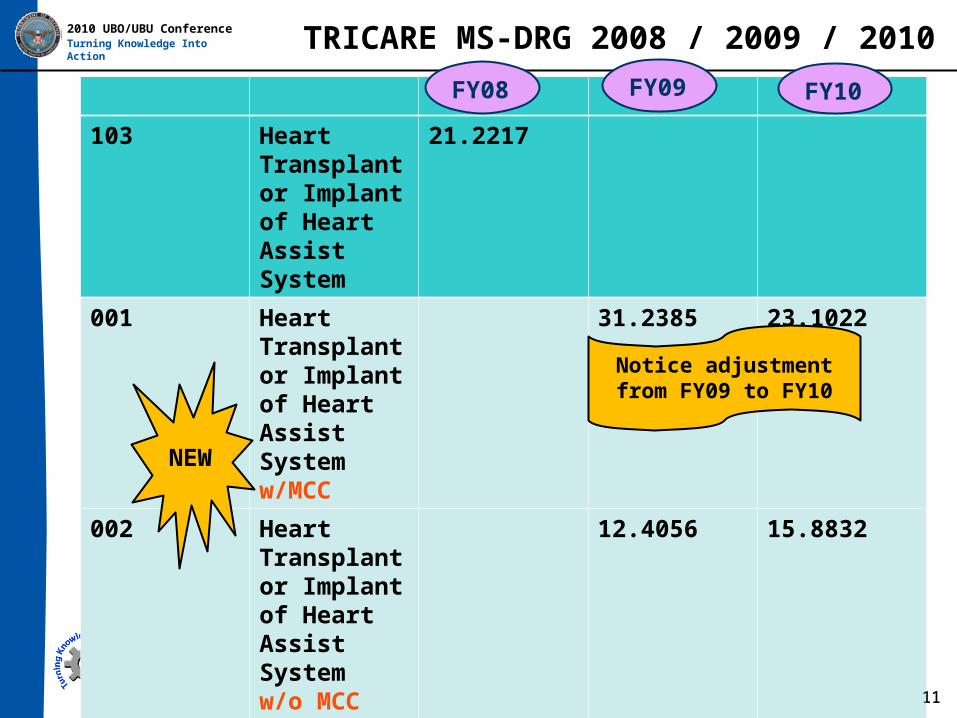
TRICARE MS-DRG 2008 / 2009 / 2010
103 Heart Transplant or Implant of Heart Assist System
21.2217
001 Heart Transplant or Implant of Heart Assist System w/MCC
31.2385 23.1022
002 Heart Transplant or Implant of Heart Assist System w/o MCC
12.4056 15.8832
11
NEW
Notice adjustment from FY09 to FY10
FY08 FY09 FY10

2010 UBO/UBU ConferenceTurning Knowledge Into Action
12
How DRGs 079, 080, & 081 Changed
177 Respiratory infections and inflammations w/MCC
2.4099 2.3302
178 Respiratory infections and inflammations w/CC
1.7119 1.8230
179 Respiratory infections and inflammations w/o CC/MCC
1.1799 1.0813
12
MS-DRGs
FY09
FY10

2010 UBO/UBU ConferenceTurning Knowledge Into Action
13
Common Coding Pitfalls
Lack of Documentation Lack of Granularity (in data) Decrease in Case Mix Index (severity) Wrong POA Indicator Loss of Revenue
2010 UBO/UBU ConferenceTurning Knowledge Into Action
1414
Pitfall – Lack of Documentation
Scenario: Patient admitted with abdominal pain and melena. Repeat lab shows precipitous drop in Hct.
Discussion:– Melena (578.1 or 562.xx [GI tract, unsp/diverticulosis/
diverticulitis]) – could be CC/MCC
– No documentation re: precipitous drop in Hct– Is CC/MCC missing? – Could it be anemia?
Chronic blood loss (unspecified) – No CC or MCC Acute post-hemorrhagic anemia – CC
Diagnostic Findings– Lab and other ancillary tests– Biopsies
Only one CC or MCC needed …BUT, DON’T STOP there!

2010 UBO/UBU ConferenceTurning Knowledge Into Action
15
Rescue
Fact: precipitous drop in Hct
Was there blood loss? Was there an impact due to blood loss? Was there treatment for possible blood loss? Is it associated w/the melena? Is drop in Hct indicative of another condition?
– Is it anemia? – Other blood dyscrasia?
15
Rescue: Query the physician
2010 UBO/UBU ConferenceTurning Knowledge Into Action
16
Pitfall – Documentation of Neonatal Codes
Scenarios: Physician uses both Transient Tachypnea of the
Newborn (TTN) and Respiratory Distress Syndrome (RDS) in the baby’s chart, AND
Physician does not clearly explain (at discharge) which is correct, OR
Continuous Positive Airway Pressure (CPAP) or high nasal cannula (HFNC) used for > 24 hours

2010 UBO/UBU ConferenceTurning Knowledge Into Action
17
Neonatal Codes (cont’d)
“The American Hospital Association’s Coding Clinic from November-December 1986 initially separated RDS into type 1 (coded to 769) and type 2 or TTN (code 770.6). It further stated that the type 2 version was also referred to as mild and commented that recovery was generally made by the third day of life.
Confusion continued, however, and the first quarter 1989 issue of Coding Clinic added that the two conditions were mutually exclusive: The coder was allowed to apply only one of the diagnoses. The explanation continued that the tabular instructions with each code excluded the other, and RDS includes clinical symptoms of tachypnea. It further added that the milder diagnosis of TTN ‘by definition resolves within 6 to 24 hours of birth.’ …
Even physicians themselves have trouble reaching a consensus about when the problem constitutes RDS and when the symptoms are representative of the less severe diagnosis of TTN…If neither the payers nor the doctors can agree on what constitutes a valid RDS diagnosis, how are coders supposed to figure it out?”
Reference: “Dealing With Fussy Neonatal Codes” For the Record, October 13, 2008.
17
Excerpt…

2010 UBO/UBU ConferenceTurning Knowledge Into Action
18
Rescue
Discussion: If documentation in chart is TTN, there are no significant CXR findings, the
baby makes a speedy recovery, there was no O2 or face mask was used for a few hours only – TTN code is appropriate. OR,
If baby is preterm, CXR shows significant findings and requires Rx for resolution, gets CPAP or other mechanical ventilation for > 24 hrs, and documentation = hyaline membrane disease or RDS, the code 769 would be appropriate. BUT,
If discharge note shows mild RDS or hyaline membrane disease, or the physician uses both RDS & TTN in the note, or not in the note but in the same chart, and never clearly states which was correct …
18
RESCUE: Query the provider• Do Not Guess• Risk and Reimbur$ement at stake• Coder not clinically qualified re: final diagnosis.
2010 UBO/UBU ConferenceTurning Knowledge Into Action
19
Pitfall and Rescue
Pitfall: Not staying abreast of coding changes
Pitfall: Not establishing a working relationship with providers
Pitfall: Not optimizing reimbursement opportunities
New Major Complications and Comorbidities (MCC) for current fiscal year. 277.88 Tumor lysis syndrome 670.22 Puerperal sepsis (delivered w/postpartum complication) 670.24 Puerperal sepsis (postpartum condition/complication) 670.32 Puerperal septic thrombophlebitis (delivered w/postpartum complication) 670.34 Puerperal septic thrombophlebitis (postpartum condition/complication) 670.80 Other major puerperal infection (unspecified episode or N/A) 670.82 Other major puerperal infection (delivered w/postpartum complication) 670.84 Other major puerperal infection (postpartum condition/complication) 756.72 Omphalocele 756.73 Gastroschisis 768.73 Severe hypoxic-ischemic encephalopathy 779.32 Bilious vomiting in newborn
19
Rescue: Read! Read! Read! Could the CC be a MCC? Capitalize on educational
opportunities!
2010 UBO/UBU ConferenceTurning Knowledge Into Action
2020
Pitfalls and Rescue
Pitfall: Inadequate Physician Documentation
Pitfall: Lack of Specificity
Pitfall: Lack of granularity● In general
● 4th and 5th level of the ICD-9-CM code
● Did you read through all pertinent documents when coding the record?
● Discharge Summary/Note● History/Physical (H/P) Examination● Operation/Pathology Report
● Did you look for “details” in the ancillary notes/reports?● Did you follow up on problems?
● Focused audits● Educating the providers
•
20
Rescue: More Adjectives!
2010 UBO/UBU ConferenceTurning Knowledge Into Action
21
Pitfall – Decrease in Case Mix Index (CMI)
Pitfall: Not knowing coding trends
Pitfall: Not knowing case mix
Pitfall: Not capturing appropriate level of severity
Pitfall: Not using appropriate secondary diagnoses
Pitfall: Not getting appropriate reimbur$ement
Pitfall: Not getting accurate record of patient care
21
2010 UBO/UBU ConferenceTurning Knowledge Into Action
22
Rescue
Rescue:● Monitor coding pattern changes● Don’t ignore the “specifics” in the documentation (including
ancillary notes/reports)● Code all significant conditions (CC/MCC)/surgery● Results
● Increase in hospital resources for● Treatment of acute disease● Treatment of chronic diseases (advanced, exacerbated,
or associated with extensive disability)
● Accurate reimbursement
22
A true picture of how sick your patients are…
2010 UBO/UBU ConferenceTurning Knowledge Into Action
23
Rescue (cont’d)
Rescue:● Implement Clinical Documentation Improvement (CDI)
plan● Education (coders/providers)● All rescue plans activated…
● Accurate record of patient care● Appropriate reimbur$ement● Accurate CMI and severity● It’s your MTF’s report card!
23

2010 UBO/UBU ConferenceTurning Knowledge Into Action Rescue (cont’d)
Compute CMI for your MTF for specified time frame CMI = average cost weight for all discharges
Example:
- Total RWPs = 12,450
- 9,575 discharges
- CMI = (12,450/9575) = 1.3003 Many factors
– Classification system used– Statistical methodologies, etc.– +/- “outliers”
Baseline and Trend Severity (CMI)
24
Sum of RWPs of all patients discharged
Divided by number of discharges (patients)

2010 UBO/UBU ConferenceTurning Knowledge Into Action
25
Rescue (cont’d)
25
To run CM reports in CHCS:
1. After logging into CHCS, select ORM = Output Reports Menu
2. Select EOUT = Encoder-Grouper Output Menu
3. Select one of the reports below:
1 (460) No of Dispositions and Days Data by DRG 2 (461) Inputs Who Exceed DRG LOS 3 (462) No of Dispositions and Days Data by Category 4 (463) Records with DRGs 468, 469 or 470 5 (464) Case Mix Deviation from Expected Wt 6 (469) Patient Summary 7 (204) Clinical Records with Forced (Override) Flag 8 Batched Records Without DRGs 9 Final Diagnoses, Procedures, & DRG Report

2010 UBO/UBU ConferenceTurning Knowledge Into Action
26
Rescue (cont’d)
26
DRG Analysis Report
RWP
DRG
# of patients by DRG

2010 UBO/UBU ConferenceTurning Knowledge Into Action
2727
POA Indicators
There are five POA indicators. Y = Yes
N = No
U = Unknown (documentation insufficient)
W = Unable to determine if diagnosis was present at the time of admission
1 = Exempt, indicates specific code is on the exempt list

2010 UBO/UBU ConferenceTurning Knowledge Into Action
28
Assessing POA Status
Scenario: Patient develops “acute cystitis” 3 days into the hospitalization.
Question: What is the POA indicator?
Discussion: Although the MS-DRG assignment flags the cystitis as a “CC,” when it comes to reimbursement, payment will be re-calculated as if the cystitis were not present (no CC) and the case will be re-grouped to a different (lower paying) MS-DRG by the payer.
28
Is a query necessary? Perhaps the cystitis was present but not documented.
2010 UBO/UBU ConferenceTurning Knowledge Into Action Assessing POA Status (cont’d)
Scenario: Patient with Diabetes Mellitus developed uncontrolled diabetes on day 3 of the hospitalization.
Question: What is the POA indicator?
Discussion: Assign “Y” if all parts of the combination code were present on admission with diabetic nephropathy is admitted with uncontrolled diabetes).
Assign “N” if any part of the combination code was not present on admission (e.g., obstructive chronic bronchitis w/acute exacerbation and the exacerbation was not present on admission; asthma patient develops status asthmaticus after admission).
29

2010 UBO/UBU ConferenceTurning Knowledge Into Action
30
Analyzing a Diagnosis for POA Status
30

2010 UBO/UBU ConferenceTurning Knowledge Into Action
31
Coding Guidelines for POA
Distinguishes between pre-existing conditions and hospital-incurred complications on inpatient claims
Conditions which develop during an outpatient encounter, including Emergency Room (ER) encounters, or ambulatory surgery are considered present on admission.
Note: For the POA Reporting Guidelines and POA exempt list, see page 100 of the Official Coding Guidelines for ICD-9-CM. http://www.cdc.gov/nchs/data/icd9/icdguide09.pdf

2010 UBO/UBU ConferenceTurning Knowledge Into Action
32
Pitfall – Loss of Revenue
PDX 428.31 PDX 428.31
2°DX 427.31 2°DX 427.31
486 * 491.21 *
DRG 291 DRG 292
Heart Failure & Shock Heart Failure & Shock
w/MCC w/CC
RWP 1.4872 RWP 0.9164 PPS $12,904 PPS $7,951
FY09
2010 UBO/UBU ConferenceTurning Knowledge Into Action
33
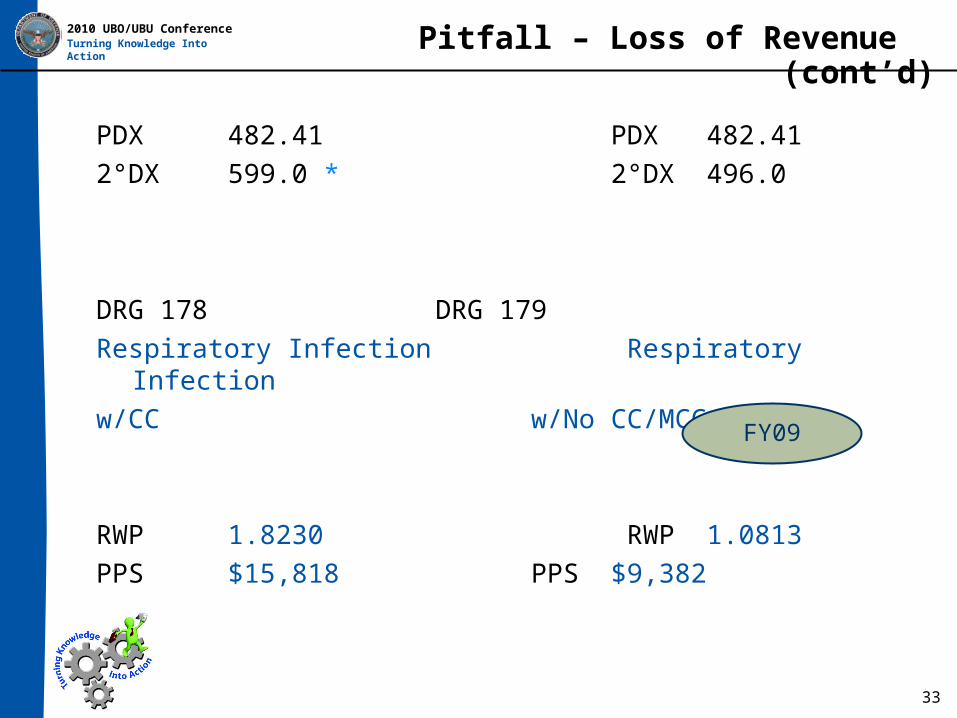
Pitfall – Loss of Revenue (cont’d)
PDX 482.41 PDX 482.41
2°DX 599.0 * 2°DX 496.0
DRG 178 DRG 179
Respiratory Infection Respiratory Infection
w/CC w/No CC/MCC
RWP 1.8230 RWP 1.0813
PPS $15,818 PPS $9,382
FY09
2010 UBO/UBU ConferenceTurning Knowledge Into Action
3434
Review of Rescue Attempts
Clinical Documentation Improvement (CDI)Accurate POA selectionMaster the Physician Query Process

2010 UBO/UBU ConferenceTurning Knowledge Into Action
35
Rescue Attempt – CDI
Clarify discrepancies found between the Discharge Summary and doctor notes during admission.
Coders should utilize ancillary reports as clues to initiate physician queries for clarification.
Common Documentation Documentation (specificity)
Chest Pain GERD, non-cardiac pain, type of angina
Nursing notes state redness and/or breakdown at pressure points
Decubitus Ulcer: site and stage
Infiltrates on CXR, Increased MBC, +sputum cultures, fever, dyspnea
Pneumonia: possible/probable organism and/or bacterial, viral or aspiration

2010 UBO/UBU ConferenceTurning Knowledge Into Action Rescue Attempt – POA accuracy
Coders must Perform detailed review and analysis of the record Assign POA accurately
– Differentiate between Conditions/complications developed during the
hospitalization Conditions/complications prior to the admission order
(review ER encounter and H/P exam)– If documentation “conflicting, inconsistent or unclear”
Query physician Issue must be resolved by the provider
Don’t forget ramifications of CC/MCC
36

2010 UBO/UBU ConferenceTurning Knowledge Into Action Rescue Attempt – Physician Query
Clarify clinical relationship between– Clinical findings and – Diagnosis implied by the clinical management
(of the patient) Common Query Topics Requiring Clarification
– Bacteremia versus Septicemia– Blood loss anemia– Diabetes Mellitus, type and manifestation– Septicemia, Sepsis, and Urosepsis
37
2010 UBO/UBU ConferenceTurning Knowledge Into Action Summation
Documentation is critical to assigning the appropriate diagnoses and procedure codes.– Coding secondary diagnoses is very important!– Don’t forget the “adjectives”!
Don’t forget– Official Coding Guidelines (civilian sector) – Military Health System Guidelines for Inpatient Coding
Granularity you need (patient care, research, etc.) The $$$ your MTF deserves!
38

2010 UBO/UBU ConferenceTurning Knowledge Into Action
39
Questions