2011 center for fetal diagnosis and treatment
DESCRIPTION
2011 Center for Fetal Diagnosis and Treatment, the Children's Hospital of PhiladelphiaTRANSCRIPT
D I V I S I O N O F G E N E R A L ,T H O R A C I C & F E T A L S U R G E R Y
Cause for HOPEHealing before birth and beyond
Giftof Childhood.org
Dear Friends,
While much of the work we do in the Division of General, Thoracic and Fetal Surgery takes place in the operating room, that’s just the beginning of the story. The real measure of our success takes place at soccer practice and ballet recitals, birthday parties and school plays; it’s the kids, once gravely ill, now experiencing the normal joys of childhood.
You’ll read in the coming pages about 3-year-old Jake. Born with a rare digestive disorder, Jake was given a poor prognosis at the hospital near his home. Thanks to a referral to CHOP, where we have expertise in complex cases like his, Jake is getting the chance to be a normal little boy.
You’ll also read about Sean, a year-round athlete who plays baseball, soccer, basketball and tennis, and swims in the summertime. To meet this bright, active 10-year-old, you would never guess he had surgery for spina bifi da at CHOP before he was born — and that without it, he would have likely been in a wheelchair.
There is nothing more fulfi lling to a surgeon than to watch children like Sean and Jake grow up. You should be proud that your donations to CHOP play a big role in making that happen.
Donors like you have funded the groundbreaking research to develop new lifesaving surgical techniques. You have helped us educate the next generation of physician-scientists. You have helped us recruit talented medical staff whose combined expertise offers an unparalleled level of patient care and gives children the best chance at life. And you have supported a fund for families who need our services but cannot afford to travel to Philadelphia.
As you read about our recent achievements, please know that we could not have accomplished them without your generosity. Thank you for all you have done to give hope to children and their families. If you would like to fi nd out how you can help further, please contact Becky Rohtbart, director of development, at 267-426-6529 or [email protected].
Sincerely,
N. Scott Adzick, M.D., M.M.M.Surgeon-in-ChiefChief, General, Thoracic and Fetal SurgeryDirector, Center for Fetal Diagnosis and TreatmentC. Everett Koop Endowed Chair in Pediatric Surgery
Max, fetal CCAM patient, pictured on cover and here with his twin brother, Alex. Read his story of lifesaving care on page 10.
N. Scott Adzick, M.D., M.M.M.Surgeon-in-ChiefChief, General, Thoracic and Fetal SurgeryDirector, Center for Fetal Diagnosis and Treatment
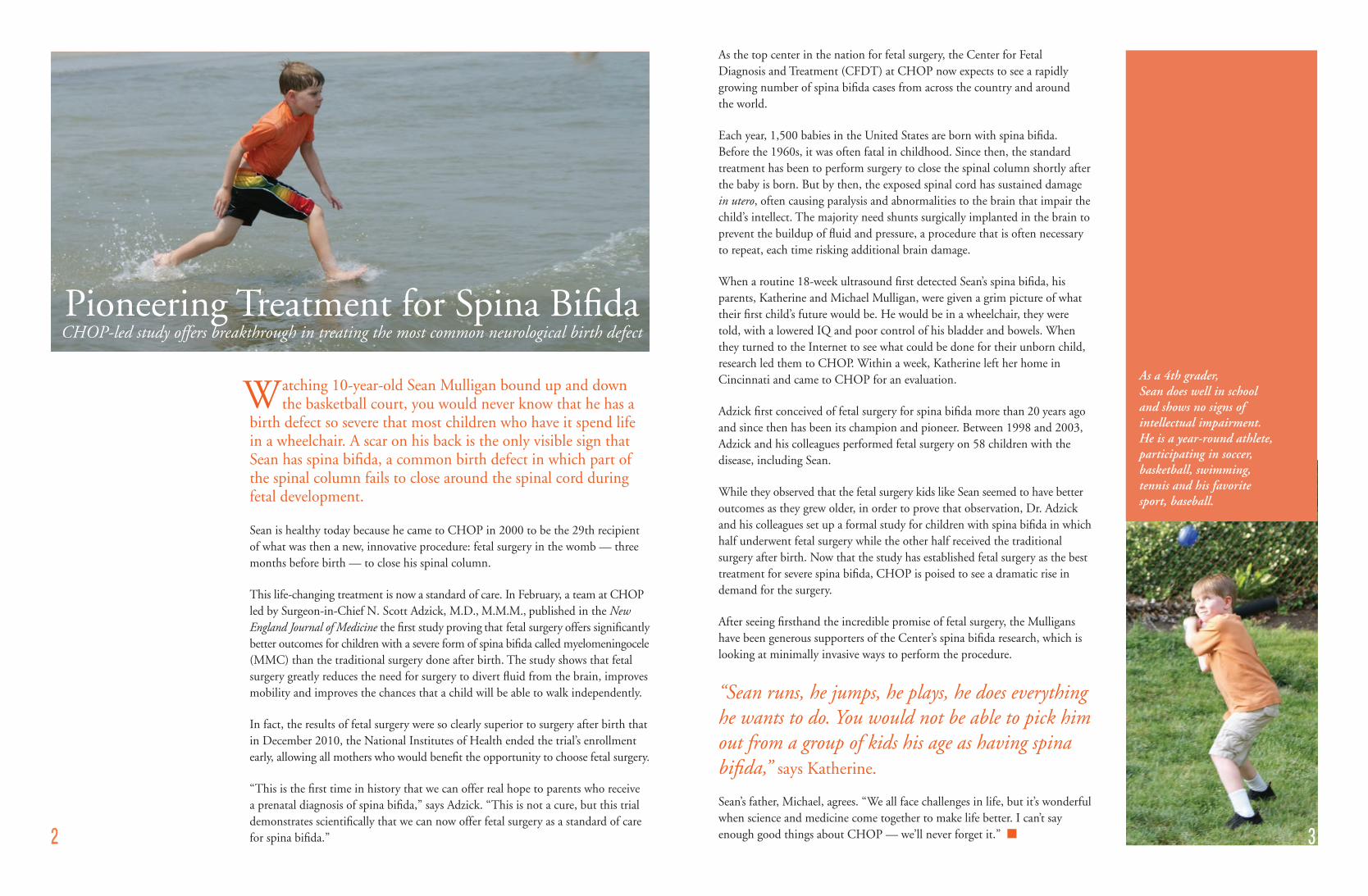
atching 10-year-old Sean Mulligan bound up and down the basketball court, you would never know that he has a
birth defect so severe that most children who have it spend life in a wheelchair. A scar on his back is the only visible sign that Sean has spina bifida, a common birth defect in which part of the spinal column fails to close around the spinal cord during fetal development.
Sean is healthy today because he came to CHOP in 2000 to be the 29th recipient of what was then a new, innovative procedure: fetal surgery in the womb — three months before birth — to close his spinal column.
This life-changing treatment is now a standard of care. In February, a team at CHOP led by Surgeon-in-Chief N. Scott Adzick, M.D., M.M.M., published in the New England Journal of Medicine the first study proving that fetal surgery offers significantly better outcomes for children with a severe form of spina bifida called myelomeningocele (MMC) than the traditional surgery done after birth. The study shows that fetal surgery greatly reduces the need for surgery to divert fluid from the brain, improves mobility and improves the chances that a child will be able to walk independently.
In fact, the results of fetal surgery were so clearly superior to surgery after birth that in December 2010, the National Institutes of Health ended the trial’s enrollment early, allowing all mothers who would benefit the opportunity to choose fetal surgery.
“This is the first time in history that we can offer real hope to parents who receive a prenatal diagnosis of spina bifida,” says Adzick. “This is not a cure, but this trial demonstrates scientifically that we can now offer fetal surgery as a standard of care for spina bifida.”
Pioneering Treatment for Spina BifidaCHOP-led study offers breakthrough in treating the most common neurological birth defect
2
As the top center in the nation for fetal surgery, the Center for Fetal Diagnosis and Treatment (CFDT) at CHOP now expects to see a rapidly growing number of spina bifida cases from across the country and around the world.
Each year, 1,500 babies in the United States are born with spina bifida. Before the 1960s, it was often fatal in childhood. Since then, the standard treatment has been to perform surgery to close the spinal column shortly after the baby is born. But by then, the exposed spinal cord has sustained damage in utero, often causing paralysis and abnormalities to the brain that impair the child’s intellect. The majority need shunts surgically implanted in the brain to prevent the buildup of fluid and pressure, a procedure that is often necessary to repeat, each time risking additional brain damage.
When a routine 18-week ultrasound first detected Sean’s spina bifida, his parents, Katherine and Michael Mulligan, were given a grim picture of what their first child’s future would be. He would be in a wheelchair, they were told, with a lowered IQ and poor control of his bladder and bowels. When they turned to the Internet to see what could be done for their unborn child, research led them to CHOP. Within a week, Katherine left her home in Cincinnati and came to CHOP for an evaluation.
Adzick first conceived of fetal surgery for spina bifida more than 20 years ago and since then has been its champion and pioneer. Between 1998 and 2003, Adzick and his colleagues performed fetal surgery on 58 children with the disease, including Sean.
While they observed that the fetal surgery kids like Sean seemed to have better outcomes as they grew older, in order to prove that observation, Dr. Adzick and his colleagues set up a formal study for children with spina bifida in which half underwent fetal surgery while the other half received the traditional surgery after birth. Now that the study has established fetal surgery as the best treatment for severe spina bifida, CHOP is poised to see a dramatic rise in demand for the surgery.
After seeing firsthand the incredible promise of fetal surgery, the Mulligans have been generous supporters of the Center’s spina bifida research, which is looking at minimally invasive ways to perform the procedure.
“Sean runs, he jumps, he plays, he does everything he wants to do. You would not be able to pick him out from a group of kids his age as having spina bifida,” says Katherine.
Sean’s father, Michael, agrees. “We all face challenges in life, but it’s wonderful when science and medicine come together to make life better. I can’t say enough good things about CHOP — we’ll never forget it.” n 3
WAs a 4th grader, Sean does well in school and shows no signs of intellectual impairment. He is a year-round athlete, participating in soccer, basketball, swimming, tennis and his favorite sport, baseball.

magine if a child with a devastating genetic disease could be born completely symptom-free.
Instead of a childhood spent shuttling from one doctor to the next, she is
dashing from ballet class to soccer practice. A child who today lives with the
grim knowledge that his disease is fatal could instead look forward to carefree
summer vacations and birthday parties with ice-cream cake.
This is the promise of prenatal gene therapy, and thanks to research led by
Alan Flake, M.D., at The Children’s Hospital of Philadelphia, this exciting
future of medicine is getting ever closer.
Just as fetal surgery can repair certain defects while the child is still in the
womb, prenatal gene therapy could “correct” DNA errors in utero by replacing
an abnormal gene with a healthy one.
Along with his team, Dr. Flake, director of the Center for Fetal Research
at CHOP and the Ruth M. and Tristram C. Colket, Jr. Endowed Chair
in Pediatric Surgery, is studying this approach with several single gene
disorders, a group of more than 6,000 diseases which, combined, affect one
in every 200 births. Unlike diseases caused by a combination of genes and
environmental factors, single gene disorders are caused by defects in one
gene, giving researchers a precise target for therapy.
Generous support from an anonymous donor is advancing CHOP’s
research into prenatal gene therapy for cystic fibrosis (CF), a single gene
disorder which affects approximately 30,000 children and adults in the
U.S., making it the nation’s most common fatal genetic disease.
CF causes the body to produce a thick, sticky mucus that clogs the lungs,
destroying lung tissue and leading to chronic infection. This mucus also
causes serious problems in the digestive system. The average lifespan of a
person with CF is roughly 35 years. If gene therapy is successful in treating
the disease, people with CF would not only have the hope of longer lives,
but would be free from the breathing and digestive problems that impact
their quality of life.
“With gene therapy, this condition could be diagnosed in utero and genes could be added to the amniotic fluid while the baby is still developing to correct the defect,” Flake says.
“There’s a lot of work to be done to prove the safety of fetal gene therapy,”
says Flake, who is currently working in animal models, “but there’s so
much promise and such clear progress being made. Charitable giving is
essential to further our efforts. It allows our team the freedom to find the
best ways to progress in a particular treatment strategy.”
Though there are a number of technical hurdles investigators need to
overcome before attempting prenatal gene therapy in humans, these
treatments, once thought to be the stuff of science fiction, are now truly
on the horizon. If proven effective, in utero gene therapy could offer so
many children born with single gene disorders like CF something never
thought possible: a completely normal life. n
The Ultimate Preventative CareResearchers aim to heal life-threatening genetic diseases before birth
4
IAlan Flake, M.D., right, and his team are working to ensure that one day, children with life-threatening single gene disorders could be cured before birth.
Dr. Flake is also researching in utero
transplantation of stem cells as a
possible cure for sickle cell disease.
The Albert M. Greenfield Foundation
more than doubled its already
generous commitment to the work
this past year, which will help
Dr. Flake move his groundbreaking
treatment through the last stages
before clinical trials.
For more information,
please call 267-426-6477 or e-mail
On the Cusp of a Cure
for Sickle Cell
To become involved in advancing
this promising research and bringing
the best treatment to sickle cell
patients, consider attending the
Blue Tag Gala & Silent Auction
on Saturday, Sept. 10, 2011.
Dr. Flake will be the
keynote speaker for
an evening of cocktails,
dinner and dancing at the Hyatt
at the Bellevue.
very year, injuries kill more children between ages 1 and 14 than all other causes combined. “Some people think it’s
unfixable,” says Michael Nance, M.D., surgeon and director of CHOP’s Pediatric Trauma Program. “Few people realize that by studying trauma, we can find new ways to prevent injuries.”
Although the lack of awareness can make it hard for Nance to get the funding he needs from traditional sources, he is being supported by two other CHOP visionaries: John M. Templeton Jr., M.D., a pediatric surgeon who established the trauma program Nance now directs, and Josephine J. Templeton, M.D., who served CHOP as a pediatric anesthesiologist.
Nance’s current research receives invaluable funding from the Josephine J. and John M. Templeton Jr. Endowed Chair in Pediatric Trauma, created by a generous gift from Drs. Templeton.
One arm of Nance’s research deals with a hot topic today: concussions. Currently, there is no consistent process for diagnosing and evaluating kids with concussions or for making recommendations for their recovery. The neurocognitive tests that have shown promise with older athletes haven’t been thoroughly tested with younger children, who take longer to recover from concussions. Nance and his team have tested certain neurocognitive evaluations with some inpatients at CHOP; now they are expanding the study into the emergency department, where many children with concussions first seek treatment.
John M. TeMpleTon Jr., M.D. ——————— and ——————
Josephine J. TeMpleTon, M.D.
have been two of the most
important supporters of The
Children’s Hospital of Philadelphia
for decades, beginning when they
both served as physicians here
and continuing to the present day.
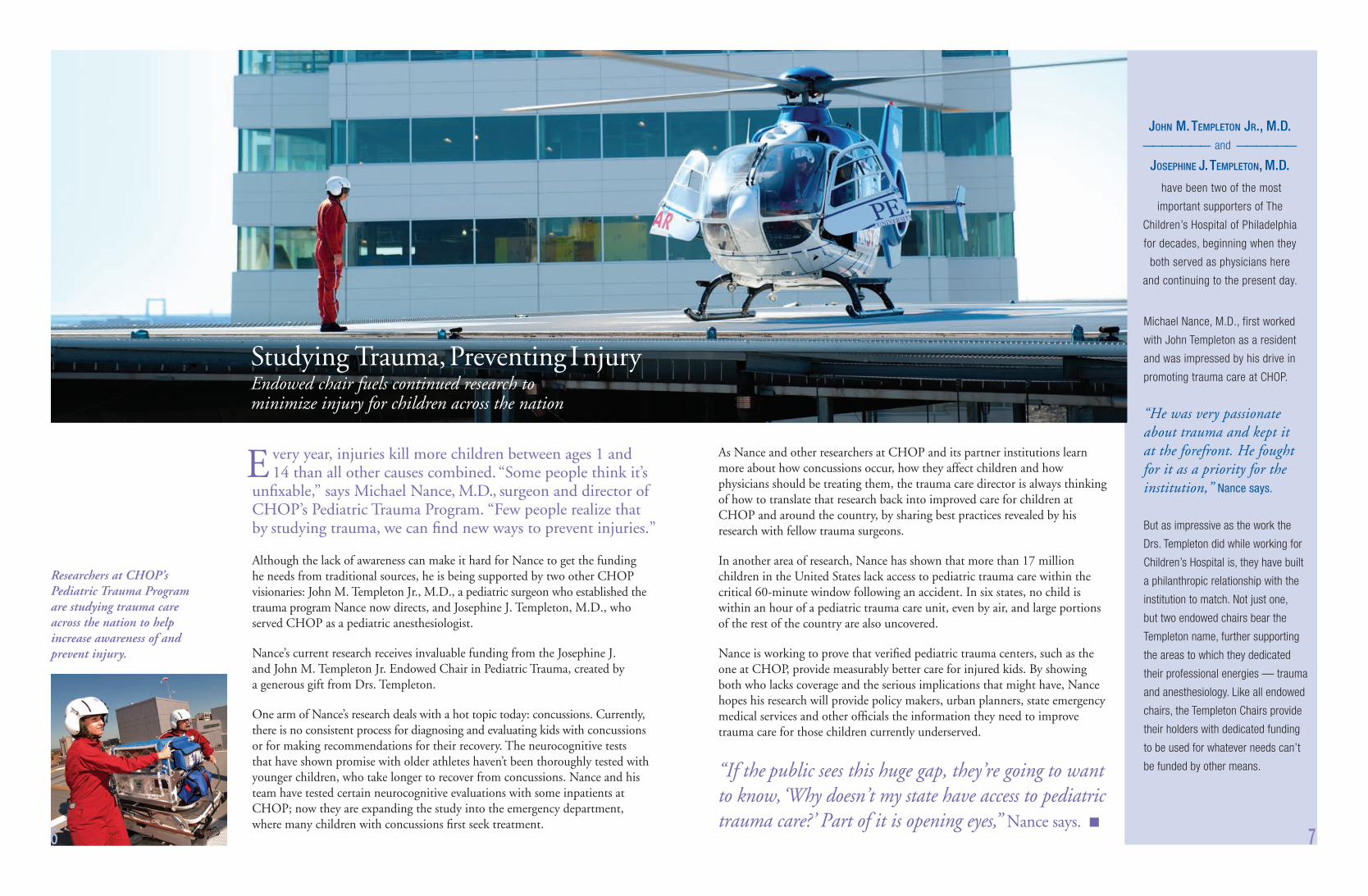
Studying Trauma, Preventing InjuryEndowed chair fuels continued research tominimize injury for children across the nation
As Nance and other researchers at CHOP and its partner institutions learn more about how concussions occur, how they affect children and how physicians should be treating them, the trauma care director is always thinking of how to translate that research back into improved care for children at CHOP and around the country, by sharing best practices revealed by his research with fellow trauma surgeons.
In another area of research, Nance has shown that more than 17 million children in the United States lack access to pediatric trauma care within the critical 60-minute window following an accident. In six states, no child is within an hour of a pediatric trauma care unit, even by air, and large portions of the rest of the country are also uncovered.
Nance is working to prove that verified pediatric trauma centers, such as the one at CHOP, provide measurably better care for injured kids. By showing both who lacks coverage and the serious implications that might have, Nance hopes his research will provide policy makers, urban planners, state emergency medical services and other officials the information they need to improve trauma care for those children currently underserved.
“If the public sees this huge gap, they’re going to want to know, ‘Why doesn’t my state have access to pediatric trauma care?’ Part of it is opening eyes,” Nance says. n
6 7
E
Michael Nance, M.D., first worked
with John Templeton as a resident
and was impressed by his drive in
promoting trauma care at CHOP.
“He was very passionate about trauma and kept it at the forefront. He fought for it as a priority for the institution,” Nance says.
But as impressive as the work the
Drs. Templeton did while working for
Children’s Hospital is, they have built
a philanthropic relationship with the
institution to match. Not just one,
but two endowed chairs bear the
Templeton name, further supporting
the areas to which they dedicated
their professional energies — trauma
and anesthesiology. Like all endowed
chairs, the Templeton Chairs provide
their holders with dedicated funding
to be used for whatever needs can’t
be funded by other means.
Researchers at CHOP’s Pediatric Trauma Program are studying trauma care across the nation to help increase awareness of and prevent injury.

t’s not easy being a modern pediatric surgeon. Cutting-edge robotic tools are allowing more and more procedures
to be done in a minimally-invasive way — terrific for the patient, but technically rigorous for the surgeon, who is both learning new techniques and working in ever smaller spaces.
“We used to do a few hundred minimally invasive-type procedures in kids every year, and now we do more than 1,000,” says Thane Blinman, M.D., director of Minimally Invasive Surgery and attending surgeon in the Division of General, Thoracic and Fetal Surgery at The Children’s Hospital of Philadelphia (CHOP). “We’re operating from a foot and a half away by remote control in these infants in spaces about the size of a large strawberry. The question is how do you take our novices and make them experts?”
In an effort to tackle this dilemma, Blinman and Pat Casale, M.D., attending urologist and director of Minimally Invasive Surgery for the Division of Urology, have developed Surgical Training Advancement, Competency and Knowledge (STACK), the nation’s most advanced pediatric surgical practice laboratory that uses simulation and training to make experts of surgical trainees and operating room staff. Launched in late 2010, STACK is founded on the belief that surgeons with more expertise are faster, more precise, more confident, more communicative and make fewer errors, resulting in improved patient safety.
“If you were learning to play an instrument or fly a plane, you wouldn’t simply read a book about it,” says Blinman. “You would want to practice on the real instrument or sit in the cockpit. It’s the same with surgery. It’s so important to work with the actual tools and get the feel for a procedure.”
In STACK, surgeons can practice minimally invasive procedures, both supervised and independently, using the actual tools of laparoscopic surgery. The program also gives them the space to tinker with equipment and new devices, taking them apart to fully understand how they work.
“I am as excited about this as I was for fetal surgery 15 years ago,” says N. Scott Adzick, M.D., M.M.M., CHOP’s surgeon-in-chief and a fetal surgery pioneer who founded the Hospital’s Center for Fetal Diagnosis and Treatment in 1995. “Our goal is to be the very best we can be at all times so we can provide the safest, most efficient, most state-of-the-art treatment to every child entrusted to our care. This initiative makes that vision a reality.”
While currently in a temporary space, STACK will soon move to a larger space with an operating room (OR) mockup that simulates real-life OR, emergency room and intensive care unit scenarios using infant and child models. Each training area has video recording capability to evaluate trainee performance. Surgical fellows and residents in the Division of Urology and the Division of General, Thoracic and Fetal Surgery, along with surgical nurses and technicians, will attend supervised classes in the space and will be required to log a certain number of hours in unsupervised practice time between classes.
The program will also allow CHOP researchers to study the design of surgical tools, which are often created “one size fits all,” and how those tools can best be adapted for use in children. Ultimately they hope to help develop better surgical instruments customized for babies and small children.
STACK relies on private donations for equipment and personnel. The program is a beneficiary of this year’s Carousel Ball, Children’s Hospital’s signature biennial black-tie dinner dance and one of the region’s most prestigious social fundraising events, with more than 650 attendees.
“It’s been shown that if you can get people physically better at using equipment, the side effect is that they become cognitively better problem solvers. And you can imagine what that would mean in terms of our efficiency and safety,” Blinman says. n
2011 Carousel BallSaturday, Nov. 5, 2011 • 7 p.m.
Hyatt Regency Philadelphia
at Penn’s Landing
201 South Columbus Boulevard
Philadelphia, Pa.
Contact Lori Busch at
267-426-6465
for more information.
Benefitting STACK and the Center for Simulation, Advanced
Education and Innovation.
8 9
I
Giftof Childhood.org/carouselball
Creating ExpertsCHOP leads the way in simulation and training
Above, Thane Blinman, M.D., who leads the nation’s most advanced pediatric surgical practice laboratory, instructs a resident.
At right, a resident practices minimally invasive techniques on simulated tissue.
Five weeks after she and Jeff temporarily relocated to Philadelphia, Max and his twin brother, Alex, were born. Less than 24 hours after delivery, N. Scott Adzick, M.D., M.M.M., director of the Center for Fetal Diagnosis and Treatment, removed Max’s CCAM.
After surgery, Max’s growth and recovery in the Harriet and Ronald Lassin Newborn/Infant Intensive Care Unit (N/IICU) was so impressive that N/IICU staff nicknamed him “Mighty Max.” Five weeks later, he went home. Now 3 years old, Max is a little dynamo. By the time he is 8, his lungs will have grown to fi ll the space the CCAM once occupied. By that point, his CHOP doctors say his lungs will be so strong he could run a marathon if he wanted to.
“When we think of the range of outcomes we were told at fi rst, he’s not even on the scale,” Jeff says. “We credit everybody at CHOP who helped us before, during and after surgery. There’s no question that without them he wouldn’t be here. They saved his life.”
“When we look back at this diffi cult time we could not have gotten through it without the help of our faith and our family support, as well as the help from those at CHOP,” Nora adds.
CHOP’s commitment to Max’s well-being continues through the Pulmonary Hypoplasia Program (PHP), a comprehensive, interdisciplinary program that provides care and long-term follow-up for children born with conditions that can restrict lung development. The PHP is the fi rst program of its kind to follow patients with the full range of conditions that cause small lungs.
The PHP’s multidisciplinary team of specialists collaborates with the Nazzaros to improve Max’s pulmonary health, evaluate his neurodevelopmental growth, monitor and treat any surgical issues that may arise throughout childhood, meet nutritional needs, and help locate resources and support services near their home.
“The idea is to optimize each child’s outcome. The program makes it easier to track outcomes because patients are followed by the same specialists. By working together, we deliver a unifi ed plan to the families,” says Holly Hedrick,
M.D., director of the PHP.
The Nazzaros channeled their appreciation for the care they received at CHOP into a donation to support the PHP. Over time, Hedrick believes the work will yield insights that will improve therapies and follow-up.
“It was really important for us to give a gift that was relevant to Max’s experience,” Nora says. “We think his case provides hope to people, and we feel really comfortable knowing he’s being watched by the best people in the world. Hopefully, by contributing to this program, we’ll help the team to analyze data and make it just a little bit easier for the next person who goes through what we went through.” n
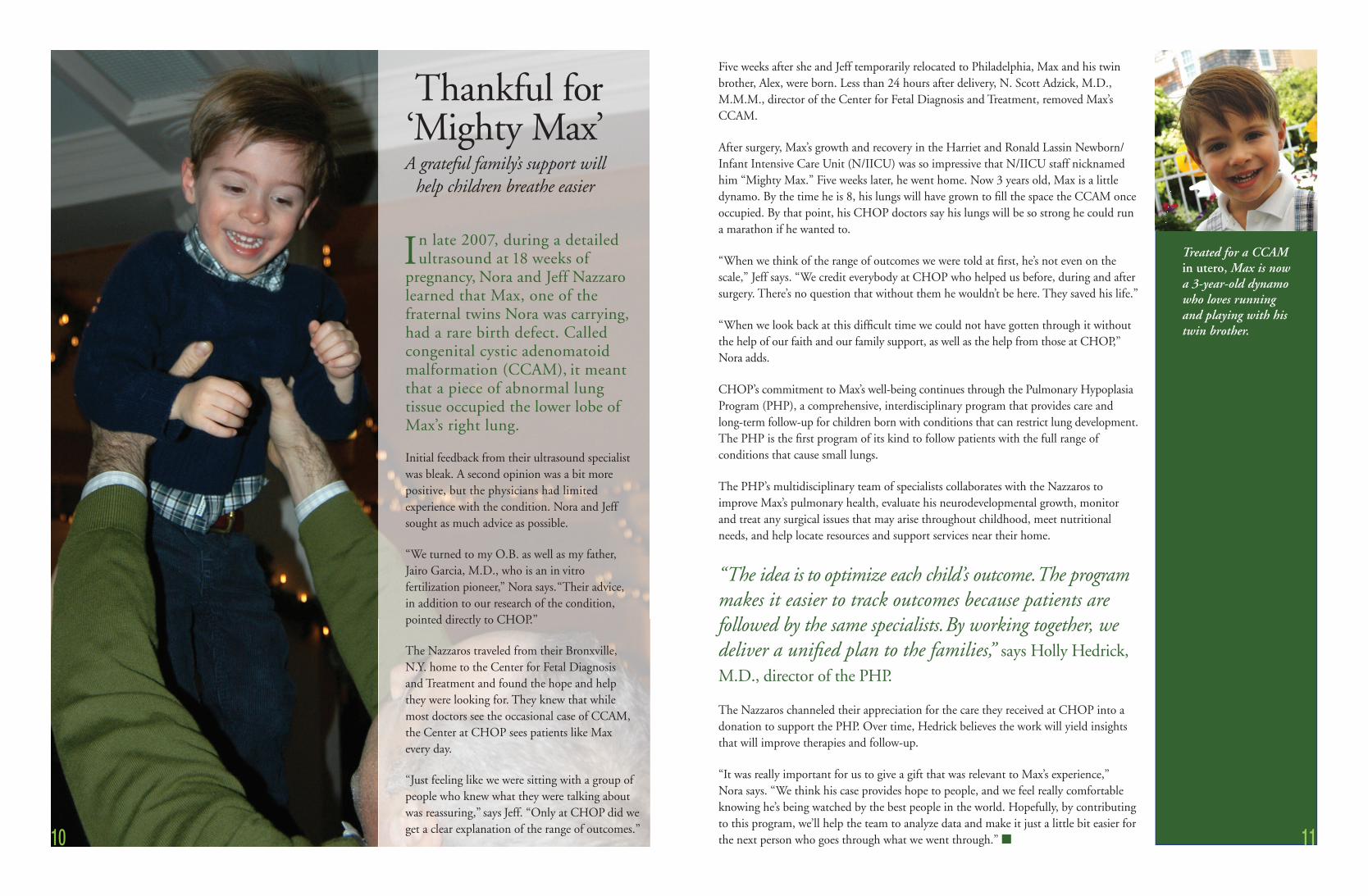
Thankful for ‘Mighty Max’A grateful family’s support will
help children breathe easier
10 11
n late 2007, during a detailed ultrasound at 18 weeks of
pregnancy, Nora and Jeff Nazzaro learned that Max, one of the fraternal twins Nora was carrying, had a rare birth defect. Called congenital cystic adenomatoid malformation (CCAM), it meant that a piece of abnormal lung tissue occupied the lower lobe of Max’s right lung.
Initial feedback from their ultrasound specialist was bleak. A second opinion was a bit more positive, but the physicians had limited experience with the condition. Nora and Jeff sought as much advice as possible.
“We turned to my O.B. as well as my father,Jairo Garcia, M.D., who is an in vitro fertilization pioneer,” Nora says. “Their advice, in addition to our research of the condition, pointed directly to CHOP.”
The Nazzaros traveled from their Bronxville, N.Y. home to the Center for Fetal Diagnosis and Treatment and found the hope and help they were looking for. They knew that while most doctors see the occasional case of CCAM, the Center at CHOP sees patients like Max every day.
“Just feeling like we were sitting with a group of people who knew what they were talking about was reassuring,” says Jeff. “Only at CHOP did we get a clear explanation of the range of outcomes.”
I Treated for a CCAM in utero, Max is now a 3-year-old dynamo who loves running and playing with his twin brother.

osted by 11-time World Series of Poker Bracelet Winner Phil Hellmuth
and with support from actor and comedian Steve Martin and book author
Amy Tan, the third annual “All In” for Kids Poker Tournament raised more than
$900,000 in October 2010 to benefi t the Center for Fetal Diagnosis and Treatment
at The Children’s Hospital of Philadelphia. The event, held at New York City’s
Mandarin Oriental Hotel, was sponsored by grateful family and Honorary Chairs
Jami and Joel Friedman and attended by more than 200 guests, including Royal
Flush Sponsors Mary and Jed Kelly and Nora and Jeffrey Nazzaro. To view a
video of the event, please visit allinforkids.org.
Honorary Chairs and Presenting Sponsors Jami and Joel Friedman with son, Skylar, a patient of the Center for Fetal Diagnosis and Treatment
2010 “All In” for Kids Poker Tournament
1. N. Scott Adzick, M.D., M.M.M., with Royal Flush Sponsors Mary and Jed Kelly
2. Players, including tournament co-founder Dan Shak (seated center), celebrate a winning hand
3. Amy Tan (center, in hat) cheers on Steve Martin and the other players
4. Center for Fetal Diagnosis and Treatment Executive Director Lori Howell, R.N., M.S., (center right) with Jed Kelly (far right) and friends at the tables
5. CHOP CEO Steven Altschuler, M.D., with comedian Steve Martin and poker legend and event host, Phil Hellmuth
6. Dr. Adzick with Royal Flush Sponsors Nora and Jeffrey Nazzaro
12
3
1 2
4 5 6
H
13
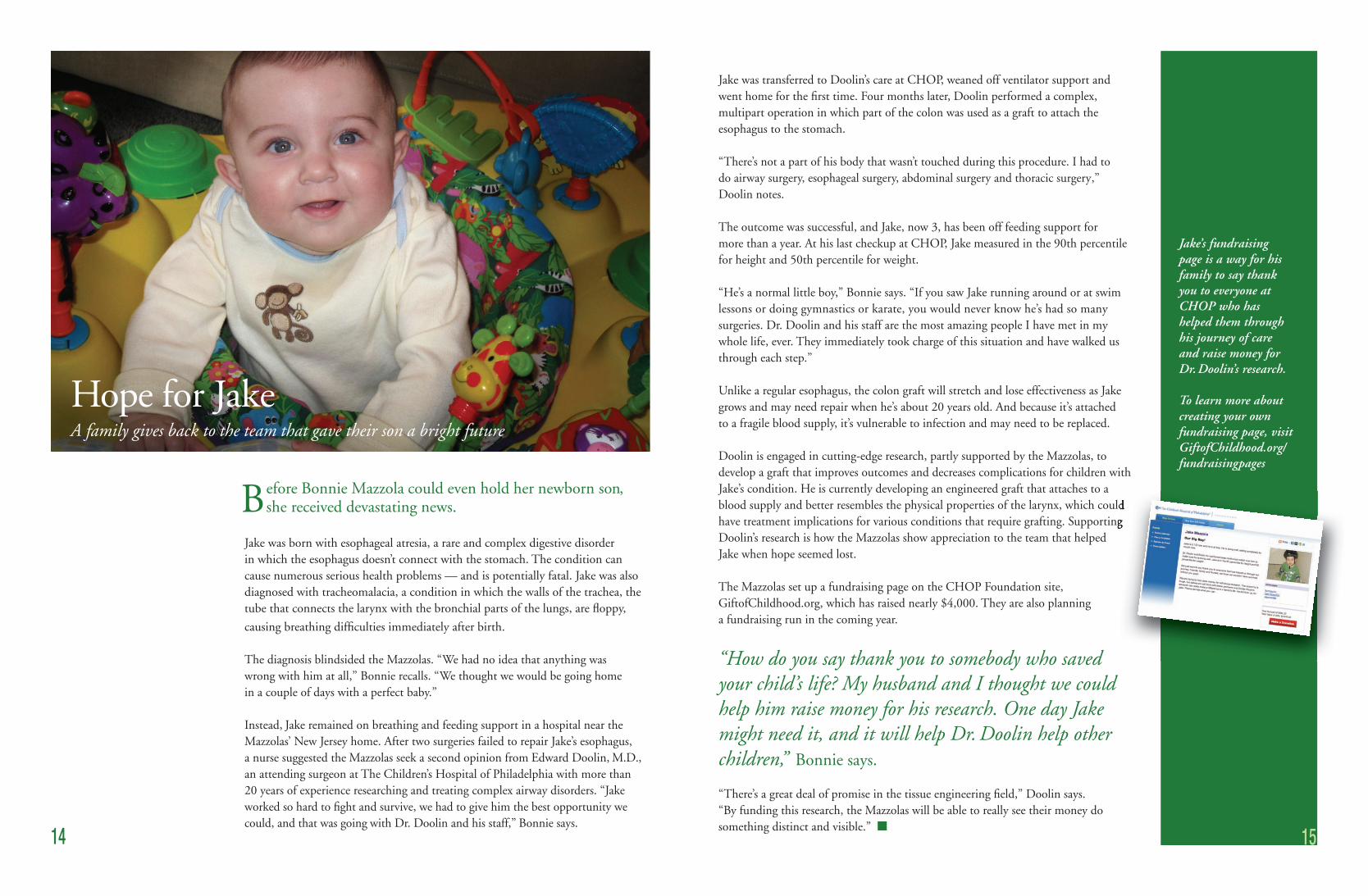
efore Bonnie Mazzola could even hold her newborn son, she received devastating news.
Jake was born with esophageal atresia, a rare and complex digestive disorder in which the esophagus doesn’t connect with the stomach. The condition can cause numerous serious health problems — and is potentially fatal. Jake was also diagnosed with tracheomalacia, a condition in which the walls of the trachea, the tube that connects the larynx with the bronchial parts of the lungs, are fl oppy,
causing breathing diffi culties immediately after birth.
The diagnosis blindsided the Mazzolas. “We had no idea that anything was wrong with him at all,” Bonnie recalls. “We thought we would be going home in a couple of days with a perfect baby.”
Instead, Jake remained on breathing and feeding support in a hospital near the Mazzolas’ New Jersey home. After two surgeries failed to repair Jake’s esophagus, a nurse suggested the Mazzolas seek a second opinion from Edward Doolin, M.D., an attending surgeon at The Children’s Hospital of Philadelphia with more than 20 years of experience researching and treating complex airway disorders. “Jake worked so hard to fi ght and survive, we had to give him the best opportunity we could, and that was going with Dr. Doolin and his staff,” Bonnie says.
Jake was transferred to Doolin’s care at CHOP, weaned off ventilator support and went home for the fi rst time. Four months later, Doolin performed a complex, multipart operation in which part of the colon was used as a graft to attach the esophagus to the stomach.
“There’s not a part of his body that wasn’t touched during this procedure. I had to do airway surgery, esophageal surgery, abdominal surgery and thoracic surgery,” Doolin notes.
The outcome was successful, and Jake, now 3, has been off feeding support for more than a year. At his last checkup at CHOP, Jake measured in the 90th percentile for height and 50th percentile for weight.
“He’s a normal little boy,” Bonnie says. “If you saw Jake running around or at swim lessons or doing gymnastics or karate, you would never know he’s had so many surgeries. Dr. Doolin and his staff are the most amazing people I have met in my whole life, ever. They immediately took charge of this situation and have walked us through each step.”
Unlike a regular esophagus, the colon graft will stretch and lose effectiveness as Jake grows and may need repair when he’s about 20 years old. And because it’s attached to a fragile blood supply, it’s vulnerable to infection and may need to be replaced.
Doolin is engaged in cutting-edge research, partly supported by the Mazzolas, to develop a graft that improves outcomes and decreases complications for children with Jake’s condition. He is currently developing an engineered graft that attaches to a blood supply and better resembles the physical properties of the larynx, which could have treatment implications for various conditions that require grafting. Supporting Doolin’s research is how the Mazzolas show appreciation to the team that helped Jake when hope seemed lost.
The Mazzolas set up a fundraising page on the CHOP Foundation site, GiftofChildhood.org, which has raised nearly $4,000. They are also planning a fundraising run in the coming year.
“How do you say thank you to somebody who saved your child’s life? My husband and I thought we could help him raise money for his research. One day Jake might need it, and it will help Dr. Doolin help other children,” Bonnie says.
“There’s a great deal of promise in the tissue engineering fi eld,” Doolin says. “By funding this research, the Mazzolas will be able to really see their money do something distinct and visible.” n
Hope for JakeA family gives back to the team that gave their son a bright future
14 15
Here’s the Mazzola’s contact info for the story about Dr. Doolin’s research and their fundraising efforts: Bonnie Mazzola – cell 609-332-0802, home [email protected]
B
Jake’s fundraising page is a way for his family to say thank you to everyone at CHOP who has helped them through his journey of care and raise money for Dr. Doolin’s research.
To learn more about creating your own fundraising page, visit GiftofChildhood.org/fundraisingpages
blood supply and better resembles the physical properties of the larynx, which could have treatment implications for various conditions that require grafting. Supporting

16
The stories of hope, innovation and progress within this report are possible
thanks to the support of generous families. Your assistance is vital to the
pioneering work of the Division of General, Thoracic and Fetal Surgery at
The Children’s Hospital of Philadelphia. To learn more about how you can help,
please contact Becky Rohtbart, director of development, at 267-426-6529
or [email protected], or visit GiftofChildhood.org.
The Center for Fetal Diagnosis and Treatment’s 14th Annual Family Reunion in 2010 brought together more than 700 people.
17

D I V I S I O N O F G E N E R A L ,T H O R A C I C & F E T A L S U R G E R Y
Hope lives here.
The Children’s Hospital of Philadelphia is one of only eight pediatric hospitals in the nation named
to the prestigious U.S.News & World Report Best Children’s Hospitals Honor Roll for 2010-11.
34th Street and Civic Center Boulevard, Philadelphia, PA 19104-4399 • 267-426-6500 • GiftofChildhood.org
The Division of General, Thoracic and Fetal Surgery
at The Children’s Hospital of Philadelphia was
established by C. Everett Koop, M.D., in 1946 as the
fi rst pediatric surgical program in the city of Philadelphia,
and the second in North America. Throughout its long
history, the Division has provided some of the fi nest,
most compassionate multidisciplinary care in the nation,
and has continued to pioneer advancements to improve
the lives of children for generations to come. The Center
for Fetal Diagnosis and Treatment, founded in 1995
by N. Scott Adzick, M.D., M.M.M., allows us to
dedicate these unparalleled resources to the care of
babies even before birth.
© 2
011
The
Chi
ldre
n’s
Hos
pita
l of P
hila
delp
hia.
All
Rig
hts
Res
erve
d.
435
2/2.
5M/0
3-20
11