20130517214119-lumbarspineapproachesbraydatelietal
DESCRIPTION
http://www.marcoteli.it/public/file/20130517214119-LumbarspineapproachesBraydaTelietal.pdfTRANSCRIPT

Lumbar Surgical Approachesfor Nonfusion TechniquesMarco Brayda-Bruno, Franco Gobetti, Alessio Lovi,
and Marco Teli
A nonfusion option in low back pain (LBP) surgery has become more and morepopular as an aLternative strategy to fusion in the treatment of patients with disc-
related pain unresponsive to nonoperative care. Although still in the early phases ofdevelopment after some pioneer devices, the future in this field is promising and themotion-preservation techniques will become part of the spine surgeon's armamen-tarium, especially with the introduction of new materials and new implants designs.Lumbar disc or nucleus prosthesis and posterior lumbar "dynamic" instrumentationswere introduced in the last 10 to 15 years, showing promising results in short- andmidterm outcomes, which must be confirmed in long-term follow-up studies.
One of the most important aspects in this "functional" surgery is to preserve
as much of the anatomic structures as possible (muscles, fascia, ligaments, and joints)during the surgical exposure.
Using less invasive surgical approaches to the spine, it is possible to adequately
expose the desired anatomic structures while minirnizing the disadvantages of excessive
soft tissue stripping, dissection, and prolonged retraction. Several srudies have demon-strated that prolonged soft tissue refraction generates a greater force per unit area on theretracted tissues, resulting in an increased regional ischemia, leading to paraspinalelectromyogram abnormalities and decreased muscle densiry. Muscle weakness anddenervation could be critical consequences resulting in potentially long-term adverse
side effects, such as chronic pain and muscular dysfunction.Ttris can then be prevented by minimizing the traditional approaches (anterior
or posterior) to the lumbar spine using new refactors, video-assisted techniques,
and/or navigation. On the other side, one of the most important drawbacks tominimally invasive surgery entails the long learning curve necessary to master the
various techniques (1).
POSTERIOR APPROACHES
Posterior approaches to the lumbar spine for nonfusion techniques are used for inter-spinous devices (2) and for dynamic pedicular screws implants (3).
Interspinous systems are designed to provide dynamic stabilization to the lumbarspine, creating a tension-bend in the posterior column. These implants control the
101
t02NONFUSION TECHNOLOGIES IN SPINE SURGERY
CHAPTER 1 1 Lun
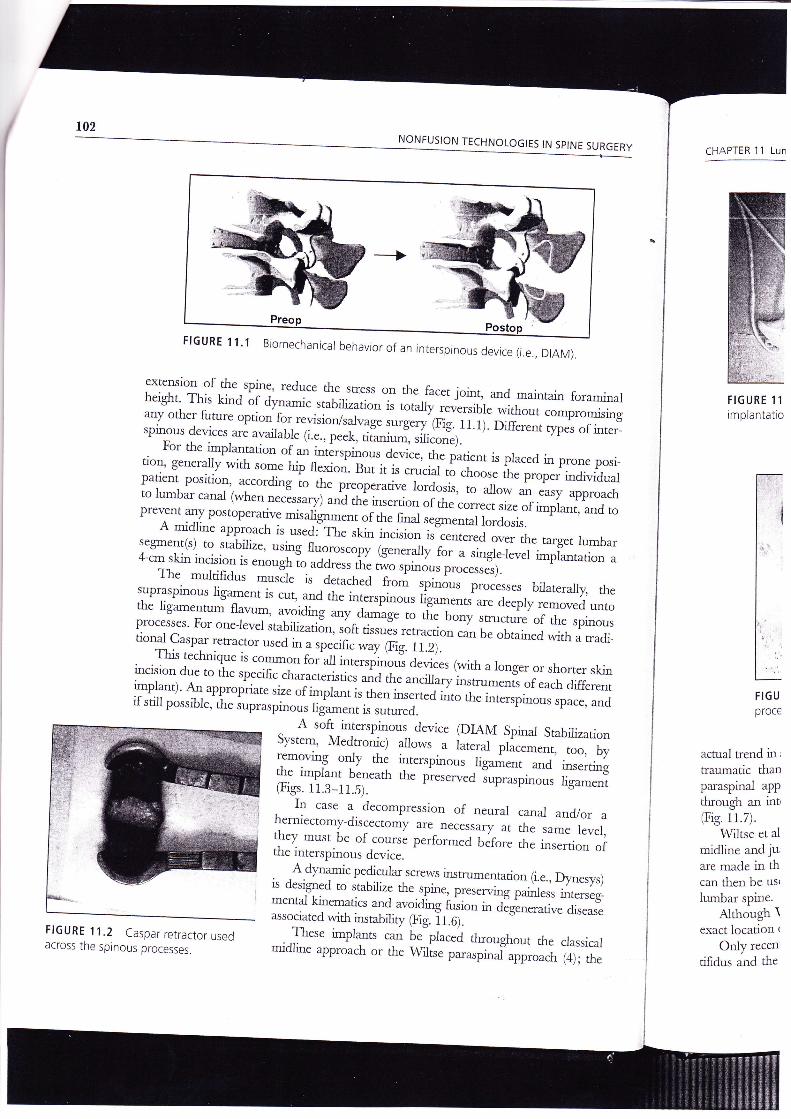
FTGURE 11'1 Biomechanical behavior of an interspinous device (i.e., ornrv]
extension of the soine' reduce the sftess on the-facet joint, and maintain foraminalheight' This kind àr ay,'"*i. rr"t,rr;ri"""is totary .J.;;iú;rhour compromisingany other furure option for revision/su.lrug; :urgery (Fig. 1l.i). Ofi....rt q,pes of inter_spinous devices are availab.le 1i..., p..t-, JiJ""i, ,íri.""".1r^'rl.
u,r,
. For the implantadon of * _-,àrtfi".ir ì.ti.", ,rr. íuri.r,, is praced in prone posihon, genera-lly with some hip flexion. But it is .*uJ ,i-.rr"iri,i. oroo.r individualpatient position, according il ,fr. p.*pirative lordosis, to allowto lumbar canal (whennecessary) and thà inserrion orrh..orr.i;;.:;ffi|u;i[T.,1prevenr any posroperative misarignment of the fi"rl.gr";;;Jì"ra*rr.A midline approach ir "r.aiTrr.-rd ir,.irio., ir"..",.;";;;; the targer rumbar;:.iltr*,':lTî#ilri::1x::"fl $."::grr"';.;iJ,,.ri,,,piu',,u,io,'ìThe muldfiJ* i,rr.r. ;, detached f.t"^T-t-T
processes)'
s upraspino u s tisu-.,,i i, . u,,. *a À J;;;r;,T;, ;?il::,rTJ.i: !i,i,lH#í, "*;the iigamentum flar''m, lydhs uty a*'ug. to tÈe bony ,;;;;r. of the spinousprocesses' For one-rever stabilizatiàn, rlr, ,ir*o rerracdon can be orio-.a with a rradi_tional Caspar rerractor used in " ,úid ;"y Fi g. 11.2).This technique is common for a-il rrrt..rpi'o'.-r, devices (wirh a longer or shorter skinincision due to rhe soecific.rturu.,.rirri.ì;;;.
"".ii,;,i,.,;;.'i, or.u.t differentimplanr)' Att uppropiiut. rir. of i*pil;r*rh"; inserted ú,",rr.l,'r.*pinous space, andtl.stillpossible,thesupraspinousrig;;"ii'';'*a.
FIGURE 11
implantatio
FIGUproce
acual rrend in r
lraumatic thanparaspinal app
through an int'(Fis. 11.7).
Wiltse et al
midline and jur
are made in thcan then be usr
lumbar spine.Although \
exact location r
Only recen'
tifidu.s and the
^ A soft
_interspinous device pIAM Spinal StabiiizationSystem, Medrronic) *:*r.u iu,.rut-ji..*.",, too, byremoving only the inrerspinous [Sa-ri.;;-*d insertingthe implant beneath th. preservet:;;r"qp_"us ligament(Figs. 11.3-11.S).
I1 :*" a. decompression of neural canal and/or a
il:r,_T"., oe of course p..for-.JiJf; ;. '#H':?the interspinous device.
FIGURE 11.2 Caspar retractor usedacross the spinous processes.
A dynamic pedicular screws irun_umentadon (i.e., Dynesy$is designed ro stabitize g:,1lt.l p.J;;;;-;r".tess inrerseg_mental kinematics and avoiding fixion in dlgi.r.rutirre diseaseassociated with irutabiliry 69. ír.O;" --ù'^'
. .Lh... implants can be"placed tluoughout the classicalmidline approach or the \Ahtise p-*p;i;;;roach (4); the

dL]rAM).
SPINE SURGERY
ain foraminal:ompromising
lpes of inter-
n prone posi-rer individualrsy approachrplant, and to
arg€t lumbarrplantation a
aterally, the:moved untothe spinouswith a tradi-
shorter skinach differentrs space, and
Srabilizarionnt, too, byLd insertingus ligament
I and/or asame level,insertion of
:., D;'nesys)ess interseg-
Ltive disease
he classicalrch (4); the
I
CHAPTER I1 Lumbar Surgical Approaches for Nonfusion Techniques 103
FIGURE 11.3 lnterspinous retractor for DIAM
implantation.
FIGURE 1 1.5 DIAM fixed between spinal
processes.
FIGURE 11.6 Dynamic pedicular screws
implants (Dynesys).
actual trend in spinal surgery is favorable to the latteq whenever possible, because it is less
rraumatic than the former in muscular detachment and in blood loss. The Wiltse
paraspina-l approach allows to expose the posterolateral part of the lumbar pedicles
tlnough an intermuscular splitting between the multifidus and the longissimus muscles
(Fis. 11.7).
Wiltse et al. proposed to make the skin incision approximately 2 crnlateral from the
midtine and just medial to the posterior-superior iJìac spine bilaterally. Similar incisions
are made in the fascia at the same distance from the spinal processes. The index finger
can then be used as a dissector inside the sacrospinalis above the L4-5 level to reach the
lumbar spine.Although Wiltse et al. described the technical details of this approach in 1968, the
exact location of trans-sacrospinalis splitting is still unclear.
Only recently, Vialle et al. (5) described the natural fibrous cleavage berween the mul-
tifidus and the longissimus muscles (Fig. 11.8), which can be located by the perforating
FIGURE 11.4 lnsertion of DIAM.

104 NONFUSION TECHNOLOGIES IN SPf NE SURGERY
vessels that leave thl, inr.rrnlrscular space and arevisible at the surface of sacrospina_lis muscle. The meandistance berween the perforating vessels and the midlineís 4.04 crn (2.4-7 cm).
Vialle -et
al. proposed then to operì rhe superficialmuscular fascia near the midÌine u.rd to retract it later_ally to expose the posterior aspect of the sacrospinalismuscle as much as necessary to locate this vascularlandmark. The intermuscular dissection through thefibrous cleavage (after vessels cauterization) piermitsthe surgeon to easily reach the posterolateral aspect ofthe pedicles from L3 to the sacrum (a more carefuldissection must be done at the cranial level to avoid
lamage of the posterior rarnus of the LB root).Foraminotomy or discectomy can be performedthrough this approach; if a central decompression withlaminectomy or laminotomy is necessaryi th.r, a mid_line traditional approach is preferable.
FIGURE 1 1.7 The natural cleavage planebetween the multifidus and the longissimusmuscies (arrows).
FIGURE I 1.8 The natural fibrous cleavage between the multifidusand the longissimus muscles (dotted lind.
Complications of Posterior Approaches
The minimally invasive spinal access for posterior lumbar procedures is becoming moreand more coqunon, but long-term follow-up is required tó determine the relativ"e risksandùenefits of this approach compared with more traditional open procedures.
. Complications specifically related to the surgical exposure are rare, because theseminimal approaches need much less soft rissue dissecrion arrd then morbidiry. The majordifficulty is the lack o1 visgalization for safe neural decompression and implant place-ment: This could risk potential stretch neurapraxia or durJ vioiation, whici are much
more difficulr to repair through aminimal access.
ANTERIORAPPROACHES
These approaches are used fortotal disc replacement. The newgeneration of implants has beendeveloped to be implantedthrough minimally invasive ante-rior retroperitoneal approachesto the lumbar levels L2-8, LS-4,L4-5, and L5-S1.
The patient is posirionedsupine with abducted and semi_flexed hips. With the assistance ofthe C-arm, an accurate identifica-tion of the midline is made (it is

Éurryry
I
cHAPTER 11 Lumbar Surgical Approaches for Nonfusion Techniques
' space and areruscle. The means and the midline
:n the superficialto retract it later-the sacrospinalisate this vascularion through therization) permitsrlateral aspect of(a more carefulil level to avoid' the L3 root).be performed
ompression withary then a mid-
; becoming morethe relative riskscedures.
e, because theseridiry. The majord implant place-which are much:epair through a
; are used fornent. The newrlants has beenbe implantedr invasive ante-:al approachesels L2-3, L3-4,
is positioned:ted and semi-he assistance of:rate idendfica-: is made (it is
cnrcial to carefully conffol the patient's position in a true neutral supine position without
any lateral tilt). Once rhe centerline has been found, it is usually helpful to mark the
cenrerline on the skin, as well as to mark the skin for the lateral projection of the target
vertebral bodies by lateral fluoroscopic check (6).
Anterior minimally invasive retroperitoneal approach to L5-S1 (Fig. 11.94):
. 5 to 6 cm horizontal skin incision, fascia, and rectus abdominis sheath op.ri.O(Fig.11.10).
. Retroperitoneum, approached through Douglas' space (Fig. 11.11).
FIGURE 11.9 Anterior retroperitoneal approach to L5-S1 (A) and L4-15 (B) relative to the bifurcation
of the great vessels.
FIGURE 11.10 Opening of the rectus sheath FIGURE 11.1 1 Douglas' space opening.

106NONFUSION TECHNOLOGIES IN SPINE SURGERY
FIG URE
ligated.11.12 Middle sacral artery and vein
. Left cornmon iliac/aortic bifurcation mobilized(690/o located at IA-S).
. Middle sacral artery and vein mobilized
ia ligalga (they are betow the,bifurcation)(Fig. 11.12).
. Blunt dissection and mobilizarion ro the rightof the left cornmon iÌiac artery also sweeping
T.l bf, to right the preverteba Jlrr.(including the superior hypogastric plexus) offthe lumbosacral disc Fig.1f .f ey.
. Disc approached in the rnidline (Fig. 11.14).
Anterior_minimally invasive refoperitonealapproach toL4-LS (Fig. 11.98):
FIGURE l l.l4 Midline disc approach, discectomycompleted.
. 5 to 6 cm vertical skin incision, fascia, and
' Retroperitoneum, approached ",""r,
;Trî:,l:ffi'**. fl ?T."" (Fig' 1 1' 1 0)'
' Left ileoìumbar ascending.vein ligated (atL4-Ls),because this vein is a horizontaltether, which crosses the body oi rs i.o,,' right to left urrJ ascends in the leftparavertebral space. It acts as a direct tether to prevent rerraction ofthe iliac vein offthe spine and is very vulnerable to avulsion.' Left cornmon iliac vein mobilization from left to dghr (Fig. 11.12) and self-retractorsin place.
' Disc approached in the midtine (Fig. 11.14).
currentrv some Tf)A implaats (i.e., o-MAV, M"dtronic) may be correctly praced atI-zt-S level by an oblique diiection, th.r, .lJrr.irg the retraction srress on the vessersbecause their complete dislocation ,. ,fr. afr, i, no longer necessary.
FIGURE ll.l3 Mobilization of left commoniilac vein.

NE SURGERY
mobilizedbifurcation)
to the right;o sweeping
:bral tissue: plexus) off
ig. 11.la).
roperitoneal
fascia, andFig.11.10).
a horizontals in the leftiliac vein off
elf-retractors
:tly placed atr the vessels
, discectomy
CHAPTER 1 1 Lumbar Surgical Approaches for Nonfusion Techniques
Complications of Anterior Approaches
Most of the data available from the literature about the complication rate of anterior
approaches to tt. t,-,*# tfi;;;t ;" ALIF techniques' but Èt-tu13t this access is the
same as that used tor total disc replacement, the duia cun be similarly considered in
anterior lumbar spine nonfusion surgery' ,
The most ."**""- "pprr".rr-i.r^r.a inrraoperative complications are vascular \
injuries, ureteral-tears' ilT;;;t"* t'i()],"'l"n' whereas the postoperative complica-
dons are sympathetrc dyrfu;;il (.rp*iully rerrograde ejaculation in males), urinary
retention, and Prolonged ileus'
Toexposetheanteriorlumbarspine,atransperitonealapproachcanalsobeused,either open or laparoscopic' However, :nTy
co;Pu'utit'9 lunttt were published in the
iast few years, showing a clear superionry of the mini-ópén retroperitoneal anterior
"oo;""* homogeneous consecutive series of patients *irl * oqen tradftlolrll
retroperitoneal access J* pr.r.rr, a22olo to 3g0/o total rate of intra- and postoperatrve
complicarionr, u..oraii!',:'èù; ,ì "r tzl and Rajaraman et al. (8), whereas with
a minimally invasive rètroperitoneal exposure in a large cohort of patients (684)'
Xf..*-., uf. (g) showed i"ry low complication rate of 2'5010'
Among ,fr. .orrrp*ui* "íait', ZlJUU"tt et al' (10) evidenced significant lower
complication, ir "úri;;." erry (4%) versus laparoscopic ALIF (200/0) without any
technical difference. nr.àb* et al. (11) compared fou, difietettt approaches (two video-
assisted and two "p.";;;;pLi."rJ' Their conclusion is that endoscopic approaches
alenotconvenientwhencomparedtoopenarrdthatthebestaccessisthemini.openreffoperitoneal with u io*., .o*pti.ution rate: rerrograde ejaculation (RE) was P esent
in 80/o of mal., in ,o,u1"*ti.r;--il,h. mini-open cohlort it was 20lo' The latter complica-
tion is one of the most dangerous po"opt'ui"t unpredictable'problems *t*::tt-l-t:
rhe anrerior access ro"lu;;r^.rut lrr.r.tion: sasso et al. (12) showed in a prospectrve
srudy on 146 male p";i; that thÉ incidence of RE, due to th.-e superior hypogasrric
syTnpatheticplexusdaml$e,wasl0Úl!'S'eate'inthetransperitoneallaparoscopicíppti^.ft tftrt i. the mini-open retroperitoneal one'
The advantage of mini-ìpen versus laparoscopic tectrnique tl uguitt confrrmed by
other papers (13-15i .rp..iu11y if we .consider
tie difficulry of endoscopic biplanar
surgery with a to.rg r.;r;;-;*í. .*a the possibfiry of at least 100/o of open conversion
toà ";.
errdos.olic s'"gt; also in very experienced operative teams'
CONCLUSION
Theminimat-accessexposureofposrcriorandanteriorlumbarspinehasbecomemore popular u, .r.*..t"ul.lrr .o"ri rt"* been developed and reiined' minimizing the
;;tàtó and shortenittf tnt learning curve of previous. endoscopic surgery'
This minimally i.rrruii.r. technique ,.q,rir., adjustable blade retractor systems for
anterior and posterior ;r;;;iis prwing to bÉ a valuable alternative to ffaditional
ooen procedur.r. Ho*."#;, ;r;;;J.. *lí1. siower in spinal surgery than in other
rítgt.Í tp..irrJ.lì"" 'o
iht titkt àf tteural or vascular ittj"ry'
Gradual conversion to minimal-access procedures is proceeding' and then.more
outcomes data will u.*rrr. available to determine the value of these mini approaches'
/t108 NONFUSION TECHNOLOGIE5 IN SPINE SURGERY
REFERENCES
1. Lehman RAJr, Vaccaro AR, Bertagnoli R, KukloTR. Staadard arrd minimally invasive approachesto the spine. Orthop Ctin North Am 2005; J6:281-292.
2. Christie SD, SongJK, Fessler RG. Dynamic inter-spinous process technology. Spine 2005; 30:s73-78.
3. Grob D, Benini A,Junge A. Clinical experiencewith the Dy'nesys semirigid frxation system forthe lumbar spine: surgica-l and patient-orientedoutcome in 50 cases after an average of 2 years.Spine 2005; 30: 324-331.
4. Wiltse LL, Bateman JB, Hutchinson RH, er ai.The paraspinal sacrospinalis-splitting approach tothe lumbar spine.J BoneJoint Surg 1968; 50-A:919-926.
5. Vialle R, !\tcart R Drain O, et al. The Wiltseparaspinal approach to the lumbar spine revis-ited. Clin Orthop Relat Res 2006; 445 175-180.
6. Le HuecJ, Basso ! Mathews H, et ai. The effectof single{evel, total disc arthroplasry on sagittalbalarce parameters: a prospecrive study. EurSpineJ 2005; 14: 480-486.
7. Gumbs AA, Shah R! Yue J], et al. The openalterior paramedian reuoperitonea.l approach forspine procedures. Arch Surg 2005; 140: 33g-343.
8. Rajaramaa V, Vingan R, Rorh P, et aJ. Visceraland vascular complicacions resulting from ante-rior lumbar interbody fusion.J Neurosurg 1999;91:60-64.
9. Kleeman TJ, Michael Ahn U, Cluuerbuck \AlB,et al. Laparoscopic alterior lumbar interbody
fusion at L4-L5: at alatomic eva_luation andapproach classification. Spine )OOZ; 2Z:1390-1395.
10. Zdeblick TA, David SM. A prospecrive com-parison of surgical approach for anterior L4-L5fusion: laparoscopic versus mini anterior lumbarinterbody fusion. Spine 2000 ; 25 : 2G82-2687.
11. Escobar E, tansfeldt E, Garvey T, et al. \4deo-assisted versus open anterior lumbar spine fusionsurgery: a comparison of four techniques andcomplications in 135 patients. Spine 2003; 28:729-732.
12. Sasso RC, Kenneth BurnusJ, LeHuecJC. Rerro-grade ejaculation after anterior lumbar interbodyfusion: transperitoneal versus retroperitonea_l
exposure. Spine 2003; 28: 1023-1026.
13. Dewald CJ, Millikan KW, Hammerberg KW,Doolas A, Dewa-ld RL. An open, minimaJlyinvasive approach to the lumbar spine. Am Surg1999; 65(1): 61-68.
14. Chung SK, Lee SH, Lim SR, et aI. Comparativestudy of laparoscopic L5-S1 fusion versus openmini-Aun with a minimum 2-year follow-up.Eur SpineJ 2003; 12:613-617.
15. Regan JJ, Yuan H, McAfee PC. Laparoscopicfusion of the lumbar spine: minimally invasivespine surgery. A prosiective multicenter studyevaluating open and laparoscopic lumbar fusion.Spine 1999; 24: 402-411.