2014 employee benefits guide -...
TRANSCRIPT

2014 Employee Benefits Guide


WELCOME
Welcome to the 2014 WESCO Employee Benefits Guide. We are committed to providing you an excellent benefits package. This guide provides a quick overview of your benefits options.
WESCO offers a total rewards package that goes far beyond your pay to help you get the most out of your career and personal life. These benefits include:
Company Paid Holidays Company Paid Vacation Company Paid Sick Time Employee Assistance Program (EAP) Tobacco Cessation Program Medical Insurance Pharmacy Benefits Dental Plans Vision Plans Flexible Spending Account (FSA)
Health Savings Account (HSA) Company Paid Life Insurance Company Paid AD&D Insurance Voluntary Supplemental Life Insurance
Voluntary AD&D Insurance Voluntary Accident Insurance Voluntary Critical Illness Insurance Long-Term Disability Insurance Education Assistance 401(k) Plan with Employer Match
Most of these benefits are outlined in this guide. Additional information is available on the enrollment website.
ELIGIBILITY
You are eligible to enroll in benefits if you are a full-time employee working 30 or more hours per week. Your dependent children are eligible for medical, dental, and vision coverage if less than 26 years of age. Dependents will lose coverage the day they reach age 26. You will receive a COBRA Election Notice by mail after their coverage ends. Disabled children older than 26 may be eligible after necessary application. For Life Insurance, dependent children are covered up to age 19, or age 23 if a full time student.
Domestic Partnerships consisting of the employee and one other person of the same or opposite sex are eligible if specific requirements are met. If you elect coverage for a Domestic Partner, you must complete the Affidavit of Domestic Partnership at the time of enrollment.
ENROLLMENT
Open enrollment is once a year and all elections will take effect January 1, 2014. Elections stay in effect through December 31, 2014 unless a change is allowed by a qualifying event. Qualifying events are marriage, divorce, legal separation, birth, adoption, death, loss of coverage, spouse open enrollment, or a change in employment or residence that affects eligibility. Qualifying events must be reported to Human Resources within 30 days from the event date or changes are not permitted until the next open enrollment.
DEADLINE TO ENROLL
The deadline to enroll is November 24, 2013. Enrollment is available now. Please see enclosed instructions. All full-time employees must enroll or decline coverage every year, even if the same benefits are desired. Failure to re-enroll each year will result in no coverage for the entire year.
QUESTIONS
For benefits or enrollment questions, please e-mail [email protected]

CHANGES FOR 2014
The following changes are effective beginning January 1, 2014.
CONSULT A DOCTOR
WESCO now offers Consult A Doctor for employees enrolled in Medical. This benefit provides you and your dependents access to licensed physicians via phone, video and secure messaging. Physicians are able to provide you information, advice, and treatment, including prescription medications as needed. Highlights include:
Quality medical care for conditions such as colds, flu, sinus infections, allergies, headaches, eye/ear infections, rash/skin irritations, stomach aches/diarrhea
24 / 7 access to US qualified board certified physicians – no limits on usage Saves you time – no waiting rooms; no insurance forms Saves you money -- helps avoid unnecessary trips to the doctor and ER
DENTAL PLAN
WESCO now offers two dental plans:
Dental: This plan is the same plan as 2013 except as follows: No orthodontia coverage Annual benefit maximum per person is $1000 Lower premium Dental Plus: This plan is new for 2014 and differs from Dental as follows: Orthodontia coverage Annual benefit maximum per person is $1500 Higher premium for the additional coverage
HEALTH SAVINGS ACCOUNT
You may pair your Medical plan with a Health Savings Account (HSA) and make tax-free contributions to HSA via payroll deduction. WESCO will also contribute to active HSA accounts as follows:
$1000 annually for single coverage
$2000 annually for family coverage
WESCO will contribute the full amount via single deposit as follows:
Current employees: full contribution with the first payroll in January
New employees hired January - June: full contribution with the first payroll in July
New employees hired July - December: no employer contribution
Federal contribution limits for 2014 are $3300 annually (for single medical coverage) and $6550 annually (for other medical coverage). This contribution limit includes both employee and employer contributions so include WESCO contributions in calculating your own contribution to your HSA, and stay within the limit. Age 55 or older may be eligible to make an additional catch-up contribution of $1000 annually.
401(k) PLAN
Employer match to 401(k) is now 100% of the first 3%, 50% of the next 2%, with a maximum match of 4%.

FLEXIBLE SPENDING ACCOUNT
WESCO has a new provider for Flexible Spending Accounts (FSA). You should only consider an FSA if you are not eligible for an HSA account, or if you have significant dental and vision expenses and you are already contributing the maximum amount to an HSA. New reimbursement and claim processing will become available in January.
QUIT TOBACCO
Tobacco users will contribute a greater portion to total medical premiums. During enrollment, you will be asked if you or your spouse / domestic partner have used tobacco, in any form, within the last six months. If the answer is no, non-tobacco users receive a reduced medical premium rate.
Falsely denying tobacco use is fraudulent and subject to disciplinary action, including, but not limited to, termination of employment, termination of health coverage, and/or required repayment of any employer paid health insurance premiums.
Employees and spouses who use tobacco and are enrolled in Medical, may enroll in a Tobacco Cessation Program to receive a reduced Medical premium. The program is now administered by Delta TeamCare and led by health coaches certified in Live to Breathe, a highly successful curriculum sponsored by the American Lung Association. Delta TeamCare will develop a customized plan of action for you, your spouse/domestic partner, and/or your dependent children to help you quit tobacco permanently.
IMPORTANT NOTICES
If you are newly enrolled or have changed benefits plans, you may be receiving new materials by mail such as medical and dental ID cards, HSA debit cards, and FSA debit cards. Be sure your enrollment includes your current mailing address. You are responsible to keep your mailing address current throughout the year.
If enrolling in Supplemental Life Insurance through the Hartford, you may be required to complete a Personal Health Application before your coverage is confirmed. Failure to complete the Application will result in no supplemental coverage.
If enrolling in a Health Savings Account for the first time, you may be required to verify your account before your account is activated. Failure to comply with verification requests from OptumHealth Bank will delay your account activation and make you ineligible for an employer contribution in 2014.
To confirm your benefits premiums are properly being deducted, check your first paystub in the month of effective coverage to verify that the correct insurance premiums and other contributions have been withheld. You are responsible to verify the accuracy of all deductions for employee benefits.

ONLINE ENROLLMENT INSTRUCTIONS
THE DEADLINE TO ENROLL IS NOVEMBER 24, 2013
STEP 1
Before you enroll, gather information that you may need to enroll, such as: Dependant Information, Social Security Numbers, Dates of Birth, Address for Dependents, and Beneficiary Information.
STEP 2
Log on to https://benefits.plansource.com
Username is: the first two letters of your legal first name plus the first two letters of your last name and the last five digits of your social security number.
For example, John Smith with SSN XXX-X1-2345, Username = josm12345
Password is: your birth date in this format YYYYMMDD
For example, John Smith’s date of birth 02/07/1978, Password = 19780207
Your username and password can be changed once you have logged in.
STEP 3
From the home screen, click on “Benefit Elections” located on the upper toolbar
On the left side of the screen click on “Enroll in Benefits – Open”
Follow the enrollment wizard through each step. Be sure to:
Verify and update your Personal Profile and add your current e-mail address
Add all your dependents and their information, including Social Security numbers
Click on each available option to elect or decline coverage
STEP 4
Once you have made your elections, the system will bring you to a “Benefits Confirmation” screen. Your enrollment is not complete until you select the “Confirm” button and see a confirmation screen. If you provided an e-mail address in your profile, confirmation of enrollment will be e-mailed to you.
Please review your elections for accuracy and print a copy for your records.
To print a copy, click on “Future Benefits Confirm” on the main menu.
QUESTIONS ABOUT ENROLLMENT WEBSITE
Please call (800) 835-4559 or send an e-mail to [email protected].

COSTS OF INSURANCE
MEDICAL: UNITEDHEALTHCARE CONSUMER DRIVEN HEALTH PLAN (CDHP)
NON-TOBACCO USER
Employee Premium
Twice Monthly Employee Premium
Monthly WESCO Contribution
Monthly
Single
$38.00
$76.00
$325.00
Employee & Spouse/ Domestic Partner
$88.00
$176.00
$756.00
Employee & Child(ren)
$83.00
$166.00
$711.00
Family $119.00 $238.00 $1018.00
TOBACCO USER
Employee Premium
Twice Monthly Employee Premium
Monthly WESCO Contribution
Monthly
Single
$57.00
$114.00
$287.00
Employee & Spouse/ Domestic Partner $132.00 $264.00 $668.00
Employee & Child(ren)
$124.50
$249.00
$628.00
Family $178.50 $357.00 $899.00
DENTAL: DELTA DENTAL PLAN
DENTAL
Employee Premium
Twice Monthly Employee Premium
Monthly WESCO Contribution
Monthly
Employee
$2.75
$5.50
$22.50
Employee & Spouse/ Domestic Partner
$5.25
$10.50
$44.50
Employee & Child(ren)
$5.50
$11.00
$47.00
Family $9.50 $19.00 $83.00
DENTAL PLUS
Employee Premium
Twice Monthly Employee Premium
Monthly WESCO Contribution
Monthly
Employee
$5.00
$10.00
$23.00
Employee & Spouse/ Domestic Partner
$9.50
$19.00
$44.00
Employee & Child(ren)
$10.00
$20.00
$46.00
Family $17.50 $35.00 $82.00

VISION: UNITEDHEALTHCARE VISION PLAN
VISION
Employee Premium
Twice Monthly Employee Premium
Monthly WESCO Contribution
Monthly
Employee
$3.22
$6.44
$0.00
Employee & Spouse/ Domestic Partner
$5.85
$11.70
$0.00
Employee & Child(ren)
$5.85
$11.70
$0.00
Family $9.93 $19.86 $0.00

CONTACT INFORMATION
COVERAGE
CARRIER
CONTACT
Medical UnitedHealthcare Group ID: 706610
Customer Service: (866) 844-4868
Web: www.myuhc.com
Pharmacy UnitedHealthcare Group ID: 706610
Customer Service: (877) 844-4868
Web: www.myuhc.com
Health Savings Account (HSA)
OptumHealth Bank Customer Service: (800) 791-9361
Web: www.myuhc.com (portal access)
Flexible Spending Account (FSA)
National Benefit Services
Customer Service: (800) 274-0503 x 502
Web: www.nbsbenefits.com
Telemedicine Consult A Doctor Customer Service: (800) 362-2667
Web: www.mydrconsult.com
Dental Delta Dental Group ID: 11068
Customer Service: (800) 510-9915
Web: www.deltadentalins.com
Vision UnitedHealthcare
Vision
Customer Service: (800) 638-3120
Web: www.myuhcvision.com
Employee Assistance Program (EAP)
Care 24 Confidential Service: (888) 887-4114
Life Insurance and AD&D Insurance
The Hartford Group ID: GL-673707
Customer Service: (800) 563-1124
Web: www.thehartford.com
Long Term Disability The Hartford Group ID: 072175
Customer Service: (866) 945-7801
Web: www.thehartfordatwork.com
AFLAC Programs Aflac Company Representative, Natalie Price
(800) 427-6586 x7731
E-mail: [email protected]
401(k) Prudential Customer Service: (877) 778-2100
Web: www.prudential.com/online/retirement

MEDICAL AND PHARMACY PLAN
UNITEDHEALTHCARE CONSUMER DRIVEN HEALTH PLAN (CDHP)
When it comes to managing your health and money, you are in control. You have the freedom to manage your own care and associated costs. Our Consumer Driven Health Plan is built on the belief that your health care should be managed the same way – this plan gives you:
- In-network preventive care covered at 100% with no copays, coinsurance, or deductibles
- A nation-wide network allowing you to choose any Choice Plus providers, facilities and/or hospitals
- No lifetime maximums - No pre-existing condition limitations - Preventive Drug List providing an expanded list of preventive medications on a copayment basis (not subject to your annual deductible)
Once you meet your in-network annual deductible, you are responsible for 20% of the cost of care and WESCO will pay 80% of the cost. You’ll continue to pay your cost share until you reach the annual out-of-pocket maximum. YOUR OUT-OF-POCKET COSTS:
BENEFIT
CHOICE PLUS PROVIDERS
OUT-OF-NETWORK PROVIDERS
Deductible Employee only coverage
2-party or more coverage
$1500
$3000
$3000
$6000
Out-of-Pocket Maximum Employee only coverage
2-party or more coverage
$4500
$9000
$9000
$18000
Preventive Care Covered at 100%
Not subject to deductible
40% after deductible
Office Visits 20% after deductible 40% after deductible
Urgent Care 20% after deductible 40% after deductible
Emergency Room 20% after deductible 20% after deductible
Hospital Services 20% after deductible 40% after deductible
Prescriptions Retail Pharmacy
Home Delivery
Tier 1 – Generic $10 after deductible $25 after deductible
Tier 2 – Formulary $40 after deductible $100 after deductible
Tier 3 – Non-Formulary $60 after deductible $150 after deductible
Tier 4 – Specialty $10 after deductible $25 after deductible
Preventive medications listed on the 2014 Preventive Drug List are NOT subject to the annual deductible.
For these prescriptions, you will pay the associated co-payment based upon the coverage tier listed above.
CONSULT A DOCTOR TELEMEDICINE: CONSULT A DOCTOR WESCO now provides an exciting new healthcare benefit for you and your family members enrolled in Medical. We have partnered with Consult A Doctor, the leading provider of cloud-based telemedicine solutions, to provide 24/7, on-demand access to qualified, U.S. board-certified doctors via phone, video and secure messaging for non-emergency consultations. This great service will be offered as part of your healthcare benefits package. HOW TO ENROLL To get started with Consult A Doctor, activate your account at www.MyDrConsult.com. If you have any questions, please do not hesitate to contact Consult A Doctor Member Services at 1-800-DOC-CONSULT (1-800-362-2667). Once you activate your account, you will be able to instantly connect with a doctor to get advice. You may even request a prescription, if appropriate, for pickup at the pharmacy of your choice*. The benefit allows a doctor to call you back in as little as 30 minutes to obtain a diagnosis or make an appointment for a more in depth consultation. ADVANTAGES Consult A Doctor is a fast, convenient alternative to waiting days for an appointment or spending hours sitting in the doctor's office, urgent care or ER. Consult A Doctor provides numerous benefits: Save time: Consult with a qualified doctor without leaving your home or office. Save on drive time and
avoid waiting hours for an appointment. Save money: Save hundreds or even thousands of dollars – compared to costly doctor’s office, urgent
care or ER visits. Enjoy peace of mind: Enjoy the peace of mind that comes from having on-demand, 24/7 access to state-
licensed, U.S. board certified doctors that have undergone rigorous credentialing. Get healthier faster: Don’t avoid care because you cannot make it to the doctor. With Consult A Doctor,
you can call, video chat with or message a doctor at anytime, from anywhere. Stay well-informed: Use My Personal Health Manager (MyPHM), a one-stop web portal that combines
24/7 physician access with cutting-edge health applications, like Symptom Checker, to research the latest health topics and better manage your health.
Cover your entire family: Everyone is welcome – there are no denials based on pre-existing conditions.
*Consult A Doctor makes no warranty as to the content of any treatment response. You and your physician are solely responsible for all information and/or communication sent during a consultation. Consult A Doctor is not health insurance, and does not replace your primary care physician. You agree to contact your Primary Care Physician should your condition change or your symptoms worsen. Priority and By Appointment consultations do not guarantee prescription s as requested. Consult A Doctor is not a prescription fulfillment center. It is not guaranteed that the doctor will issue a script for prescription medication. Consult A Doctor's physicians do not prescribe DEA-controlled medications or lifestyle drugs. If you have an emergency medical condition, please dial 911. All services are HIPAA-compliant.

PREVENTIVE CARE UNITEDHEALTHCARE PREVENTIVE CARE Remember to take advantage of preventive care benefits when enrolled in the UHC Consumer Driven Health Plan (CDHP). Your 2014 in-network preventive care is covered at 100% with no copays, coinsurance, or deductibles. This allows you to receive age appropriate preventive screenings. Our plan follows the preventive care services based upon the recommendations determined by the U.S. Preventive Services Task Force (USPSTF) and other health organizations. Visit http://www.uspreventiveservicestaskforce.org/uspstf/uspsabrecs.htm to find information on the list of covered preventive services based on the USPSTF recommendations rated “A” or “B,” including any new items that may not have been previously covered under our preventive care benefit, but are now mandated for inclusion by the Patient Protection and Affordable Care Act.
The USPSTF was convened to rigorously evaluate clinical research in order to assess the merits of preventive measures, including screening tests, counseling, immunizations, and preventive medications. The topics in the above mentioned lists include all recommendations: active, inactive, and in progress. Visit http://www.uspreventiveservicestaskforce.org/uspstopics.htm to read these topics. You may also visit http://www.healthcare.gov/law/features/rights/preventive-care/index.html for more detailed information regarding preventive care services. LEARN MORE
There are several tools available to you and your family at www.uhcpreventivecare.com to determine if a service is considered preventive. We also encourage you to consult with your physician and discuss preventive care recommendations based on factors, such as a ge, gender, personal health h i s to ry , and other health concerns. WHAT IS NOT CONSIDERED PREVENTIVE?
If you visit your provider for any underlying cause then that will not be considered preventive. Neither will any service in connection with the treatment or diagnosis of a medical condition, which includes any condition discovered during a preventive exam. Keep in mind that if you go in for a preventive visit and discuss an existing condition with your physician, you may be charged for that portion of the exam. To limit confusion, be upfront with your provider and staff regarding the reason for the visit, exam, or test. Providers can always contact UHC directly at (800) 599-4301 to review preventive coding before any procedure or test is completed. Here are examples of what is not considered a preventive visit: Any procedure, lab work, test or consultation that is the result of an underlying medical condition Example: Sending blood work to a lab to determine insulin levels for a known diabetic Services that diagnose or treat and existing condition or newly discovered condition as a result of a preventive test Example: Lab tests on a polyp removed during a colonoscopy Services rendered during a preventive visit that are in connection to an existing health condition or illness Example: During a preventive office visit a strep test was performed because of a sore throat

MYUHC WEBSITE UNITEDHEALTHCARE MYUHC.COM WEBSITE
UnitedHealthcare offers a variety of tools available to you upon completion of your registration at myuhc.com. Your personalized website provides you quick access to:
Print an ID Card Claims & Accounts: - Review Claims - Health Statements and Explanation of Benefits (EOB) Physicians & Facilities: - Find an in-network physician that’s right for you and has been recognized by UHC’s two-star rating for providing quality and cost-efficient care Pharmacies & Prescriptions: - Locate an in-network retail pharmacy and price your medication for possible lower cost options Health & Wellness: - Access to hundreds of Health and Wellness Articles - Listen in on Recorded and Live Seminars - Check your health condition with Symptom Checker - Health Improvement Tools and much more
HAVE A SMARTPHONE? It’s myuhc.com in your pocket so you can look up doctors and benefit information anywhere. It also allows you to view, fax and email an electronic image of your ID Card. Just type myuhc.com into a browser window and you’re there. A full feature app, Health4Me, is also available in the App Store.

TOBACCO CESSATION PROGRAM QUIT TOBACCO Employees and spouses who use tobacco and are enrolled in Medical, may enroll in a Tobacco Cessation Program to receive a reduced Medical premium. The program is now administered by Delta TeamCare and led by health coaches certified in Live to Breathe, a highly successful curriculum sponsored by the American Lung Association. Delta TeamCare will develop a customized plan of action for you, your spouse/domestic partner, and/or your dependent children to help you quit tobacco permanently.
WHO IS ELIGIBLE?
Anyone who is: - Covered by WESCO’s qualified Consumer Driven Health Plan (CDHP) with UnitedHealthcare - Includes spouses and dependents (age 18-25) covered by a WESCO Medical Plan
HOW CAN I ENROLL?
Call a Delta TeamCare Health Coach at 1-866-724-0032 or e-mail [email protected] to join.
HOW MUCH DOES IT COST?
There is no employee cost to enroll in the program.
REQUIREMENTS
Participants are required to be actively engaged in the coaching process. Free health coaching available after you quit.
TOPICS COVERED
Health risks associated with tobacco use
The health benefits of quitting
Identifying your triggers
Techniques to help you quit
Medicines that help
Preparing for Quit Day
Ongoing support
Relaxation techniques
Weight management tips
Handling slips and relapses
Living as a non-tobacco user
Techniques to handle cravings and stress
Affirmations – what they are and how they help
HEALTH SAVINGS ACCOUNT (HSA)
HEALTH SAVINGS ACCOUNT A Health Savings Account (HSA) paired with a Consumer Driven Health Plan (CDHP) helps individuals and families to plan, save, and pay for their health care expenses. An HSA is an employee-owned savings account that is funded with your tax exempt dollars and company contributions to help pay for eligible medical, dental, and vision expenses. WHO IS ELIGIBLE?
Anyone who is: - Covered by WESCO’s qualified Consumer Driven Health Plan (CDHP) with UnitedHealthcare - Not enrolled in Medicare, Medicaid, TRICARE or TRICARE for Life, or another plan that is not
a qualified Consumer Driven Health Plan*
- Not eligible to be claimed as a dependent on someone else’s tax return - Not covered by a Traditional Flexible Spending Account (Traditional FSA) HOW MUCH CAN I CONTRIBUTE?
Federal contribution limits for 2014 are $3300 annually (for single medical coverage) and $6550 annually (for other medical coverage). This contribution limit includes both employee and employer contributions so include WESCO contributions in calculating your own contribution to your HSA, and stay within the limit. Those ages 55 or older may be eligible to make a catch-up contribution of $1,000 annually.
WILL WESCO CONTRIBUTE?
In prior years, WESCO has been generous in making employer contributions to individual HSA accounts. For 2014, WESCO will contribute to active HSA accounts as follows:
$1000 annually for single coverage
$2000 annually for family coverage
WESCO will contribute the full amount via single deposit as follows:
Current employees: full contribution with the first payroll in January
New employees hired January - June: full contribution with the first payroll in July
New employees hired July - December: no employer contribution
ELECTION CHANGES
You may change the amount that your contribute to your HSA once per month. Provide written notice to Human Resources before the first day of the month in which a change is desired.
CARRY OVER
Funds contributed to an HSA account carry over from year to year. Additionally, HSA accounts are portable, so if you leave WESCO, your HSA goes with you.
REMINDER
Even if you were enrolled in the HSA in the prior plan year, you must re-enroll each year. Elections will NOT rollover; however, you may continue to use your same debit card.

FLEXIBLE SPENDING ACCOUNT (FSA)
LIMITED PURPOSE FSA
If you are contributing to a Health Savings Account (HSA), the Limited Purpose Flexible Spending Account (Limited FSA) allows you to set aside up to $2,500 with your tax exempt dollars to pay for dental and vision expenses only. You may not be reimbursed for medical and Rx services that fall under the Consumer Driven Health Plan (CDHP). Your Limited Purpose FSA debit card may be used at certain dental and vision provider offices only.
TRADITIONAL FSA
If you are NOT enrolled in a Health Savings Account (HSA), the Traditional Flexible Spending Account (Traditional FSA) allows you to set aside up to $2,500 with your tax exempt dollars to pay for medical, dental and vision expenses. You may not enroll in the Traditional FSA if you enroll in an HSA.
DEPENDANT CARE FSA
With a Dependent Care FSA you can set aside tax exempt dollars to pay for qualified dependent care expenses, such as day care, that you normally pay with after-tax dollars. Qualified dependents include children under 13 and/or dependents who are physically or mentally disabled. If your spouse is unemployed or doing volunteer work, you cannot set up a dependent care account. You must meet the following criteria in order to set up this account:
- You and your spouse both work
- You are the single head of household
- Your spouse is disabled or a full-time student Each calendar year the IRS allows you to contribute the following amounts, depending on your family status:
- If you are single you may contribute up to $5,000 - If you are married and filing jointly, you may contribute up to $5,000 - If you are married and filing separately, you may contribute up to $2,500
NO ELECTION CHANGES Once you have designated how much you want to contribute on an annual basis to one or both of your FSA accounts, you cannot stop or change your contributions unless you have a qualified change in family status. USE IT OR LOSE IT Remaining funds at the end of the year do NOT carry over. You will forfeit any balance remaining. You have 90 days after the plan year ends to submit claims for expenses incurred during that plan year. REMINDER
Even if you were enrolled in the FSA in the prior plan year, you must re-enroll each year. Elections will NOT rollover to the new plan year.
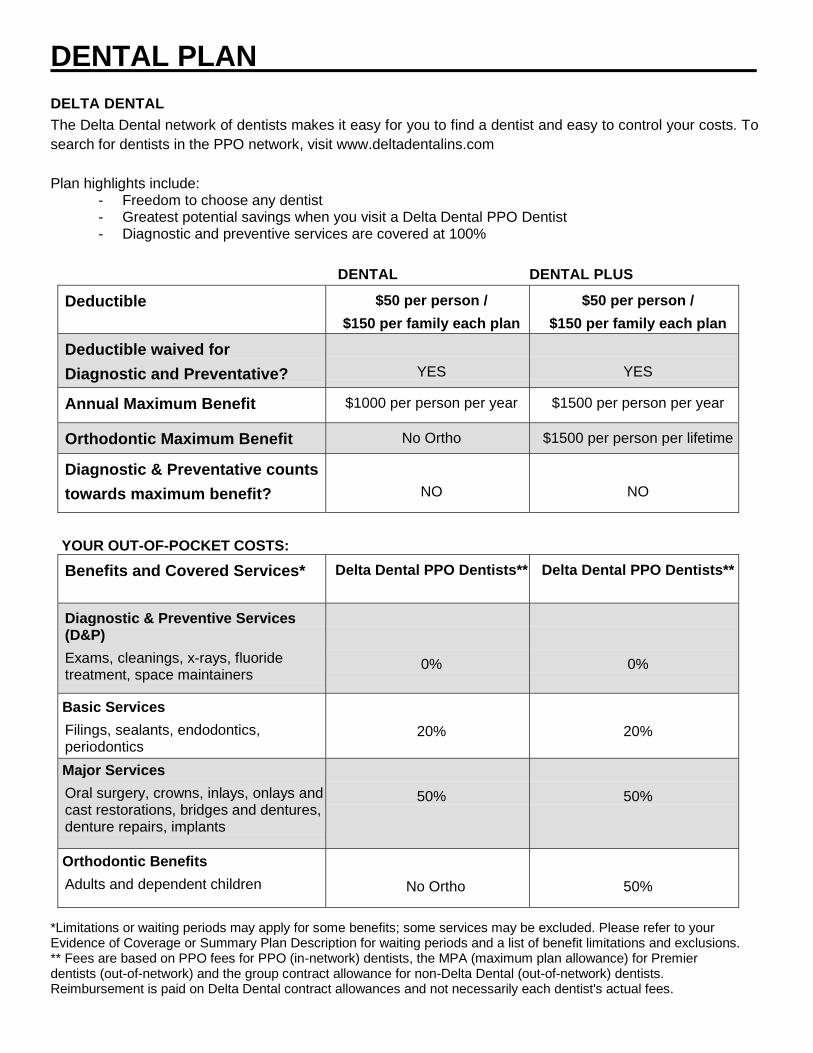
DENTAL PLAN
DELTA DENTAL
The Delta Dental network of dentists makes it easy for you to find a dentist and easy to control your costs. To search for dentists in the PPO network, visit www.deltadentalins.com
Plan highlights include: - Freedom to choose any dentist - Greatest potential savings when you visit a Delta Dental PPO Dentist - Diagnostic and preventive services are covered at 100%
DENTAL DENTAL PLUS
Deductible
$50 per person /
$150 per family each plan
$50 per person /
$150 per family each plan
Deductible waived for
Diagnostic and Preventative?
YES
YES
Annual Maximum Benefit $1000 per person per year $1500 per person per year
Orthodontic Maximum Benefit No Ortho $1500 per person per lifetime
Diagnostic & Preventative counts
towards maximum benefit?
NO
NO
YOUR OUT-OF-POCKET COSTS:
Benefits and Covered Services*
Delta Dental PPO Dentists**
Delta Dental PPO Dentists**
Diagnostic & Preventive Services (D&P)
Exams, cleanings, x-rays, fluoride treatment, space maintainers
0%
0%
Basic Services
Filings, sealants, endodontics, periodontics
20%
20%
Major Services
Oral surgery, crowns, inlays, onlays and cast restorations, bridges and dentures, denture repairs, implants
50%
50%
Orthodontic Benefits
Adults and dependent children
No Ortho
50%
*Limitations or waiting periods may apply for some benefits; some services may be excluded. Please refer to your Evidence of Coverage or Summary Plan Description for waiting periods and a list of benefit limitations and exclusions. ** Fees are based on PPO fees for PPO (in-network) dentists, the MPA (maximum plan allowance) for Premier dentists (out-of-network) and the group contract allowance for non-Delta Dental (out-of-network) dentists. Reimbursement is paid on Delta Dental contract allowances and not necessarily each dentist's actual fees.

VISION PLAN
UNITEDHEALTHCARE VISION
In-network, covered-in-full benefits (after applicable copay) include a comprehensive exam, eye glasses with standard single vision, lined bifocal, or lined trifocal lenses, standard scratch-resistant coating and the frame, or contact lenses in lieu of eye glasses. To find in-network providers visit www.myuhcvision.com
Plan highlights include:
- Competitive premiums - Freedom to choose any provider - Best level of coverage when selecting a UHC Vision provider
Benefit In-Network Providers
Copayments Exam Materials
$10 $25
Benefit Frequency Comprehensive Exam Spectacle Lenses Frames Contact Lenses in Lieu of Eye Glasses
Every 12 Months Every 12 Months Every 24 Months Every 12 Months
Frame Benefit Private Practice Provider Retail Chain Provider
$130 retail frame allowance $130 retail frame allowance
Prescription & Contact Lenses
Covered in full (after copay)
Laser Vision Benefit UnitedHealthcare Vision has partnered with the Laser Vision Network of America (LVNA) to provide members with access to discounted laser vision correction providers. Members receive 15% off usual and customary pricing, or 5% off promotional pricing at over 500 network provider locations and even greater discounts through set pricing at LasikPlus locations. For more information, call 1-888-563-4497 or visit www.uhclasik.com.

LIFE AND AD&D INSURANCE EMPLOYER PAID GROUP LIFE BENEFIT WESCO is pleased to provide all full-time active employees with group basic life and accidental death and dismemberment policy. The employer paid benefit amount for:
- Employee Life is equal to 2x your annual salary - Employee Spouse Life is $5,000 - Employee Child Life is $2,000 or $500 if child is less than 6 months of age - Employee Accidental Death & Dismemberment is equal to 2x your annual salary
EMPLOYEE PAID SUPPLEMENTAL LIFE INSURANCE During initial enrollment, you may elect supplemental life coverage up to a maximum of $300,000. If you elect supplemental coverage for yourself, you may also elect spouse coverage up to a maximum of $200,000 (not to exceed 50% of your total basic and supplemental life coverage). Dependent children may be covered up to age 19 or 23 if a full time student. If you declined coverage during your initial enrollment period for you and/or your spouse and decide to enroll at a later open enrollment, you will be subject to underwriting approval. A Personal Health Application will need to be completed and returned to The Hartford. Please refer to the chart below to find the monthly premium rate per $1,000 for your own and your spouse’s coverage.
EMPLOYEE or SPOUSE EMPLOYEE or SPOUSE
Age Non-Tobacco User Tobacco User Under 30 0.050 0.083
30-34 0.080 0.121 35-39 0.090 0.148 40-44 0.120 0.250 45-49 0.195 0.436 50-54 0.315 0.714 55-59 0.510 1.080 60-64 0.660 1.160 65-69 1.270 2.150 70-74 2.540 3.840 75-79 4.640 6.500 80+ 8.310 10.920
The monthly rate for dependent child(ren) coverage is: $1.25 per family for the $5,000 benefit $2.50 per family for the $10,000 benefit
EMPLOYEE PAID AD&D INSURANCE You may elect employee only coverage or family coverage in increments of $10,000 up to $500,000.
Employee only: $0.24 per $10,000 per month of Employee’s selected Principal Sum Amount. Employee & Family: $0.40 per $10,000 per month of Employee’s selected Principal Sum Amount.

AFLAC VOLUNTARY PROGRAMS ACCIDENT INSURANCE Accidents are unexpected. How you care for them shouldn’t be. Accident insurance from Aflac can help prepare you for what happens next.
Benefits include:
- Cash paid to you for the care and treatment of a covered accidental injury
- Benefits are paid regardless of any other insurance you have with other insurance companies
The following is an example of the premium rates per week for off-the-job Accident coverage:
Individual Couple One-Parent Family Two-Parent Family
$2.91 $4.26 $5.97 $7.32
CRITICAL ILLNESS INSURANCE No one plans on it, but statistics show you or someone you love may suffer from a heart attack, stroke, cancer or some form of critical illness in your lifetime. In fact, according to the American Cancer Society, one in every two men now living and one in every three women now living will develop some form of cancer. Critical Illness insurance from Aflac can help provide the protection you need when you need it most.
Benefits include: - Guaranteed Issue: Employees currently participating in Critical Illness will be given the opportunity
to increase coverage up to $20,000 with no questions asked. Employees not currently participating will be given the opportunity to participate in the $10,000 benefit level with no questions asked.
- Cash paid to you to assist with direct or indirect costs related to diagnosis and treatment - Dependent children are covered at no additional cost - Your coverage is portable; you can take the coverage with you if you change jobs or retire
New applicant Critical Illness rates per week: $10,000 employee and $5,000 spouse benefit
Non-Tobacco Rates Tobacco Rates
Age Employee Spouse Employee Spouse
18-29 $1.25 $0.83 $1.83 $1.12 30-39 $1.97 $1.18 $3.10 $1.75
40-49 $3.58 $1.99 $7.09 $3.75
50-59 $6.15 $3.28 $11.94 $6.17
60-69 $9.63 $5.02 $18.86 $9.63
Existing policyholder Critical Illness buy-up rates per week: $20,000 employee and $10,000 spouse benefit (these rates are in addition to current rates)
Non-Tobacco Rates Tobacco Rates Age Employee Spouse Employee Spouse
18-29 $1.71 $0.85 $2.86 $1.43 30-39 $3.14 $1.57 $5.40 $2.70
40-49 $6.37 $3.18 $13.38 $6.69
50-59 $11.51 $5.75 $23.08 $11.54
60-69 $18.46 $9.23 $36.92 $18.46
American Family Life Assurance Company of Columbus (Aflac)
IMPORTANT NOTICES

Qualified Medical Child Support Orders (QMCSOs) A Qualified Medical Child Support Order (QMCSO) is a judgment, decree or order issued by a court or appropriate state agency that requires a child to be covered for medical benefits.
Generally, a QMCSO is issued as part of a paternity, divorce, or other child support settlement. If the Health Plan receives a medical child support order for your child that instructs the Plan to cover the child, the Plan Administrator will review it to determine if it meets the requirements for a QMCSO. If it determines that it does, your child will be enrolled in the Plan as your Dependent, you will be required to pay any additional cost for such coverage, and the Plan will be required to pay Benefits as directed by the Order.
You may obtain, without charge, a copy of the procedures governing QMCSOs from the Plan Administrator. Note: A National Medical Support Notice will be recognized as a QMCSO if it meets the requirements of a QMCSO.
General Notice of Special Enrollment Rights Under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Your group health plan is required to provide you this notice explaining your group health plan’s procedures for your special enrollment rights. Your Special Enrollment Rights – If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance coverage, you may in the future be able to enroll yourself or your dependents in this plan, provided that you request enrollment within 31 days after your other coverage ends. In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents, provided that you request enrollment within 31days after the marriage, birth, adoption, or placement for adoption. If you have a special enrollment event and want to enroll yourself or your dependent(s) in the WESCO group health plan, please go online to PlanSource at https://benefits.plansource.com.
Mandatory Insurer Reporting Law Employees are required to provide Social Security numbers for all dependents enrolled in the medical plan. You will be asked to enter Social Security numbers for all dependents you enroll on your medical plan.
The reason for this requirement is the Medicare, Medicaid and SCHIP Extension Act of 2007 (MMESA). This law requires that providers of group health plans must report certain information (Social Security numbers of plan participants) to the Secretary of Health and Human Services (HHS) to determine Medicare entitlement. The reporting party will be the insurer or third-party administrator if the plan is fully insured or plan administrator or fiduciary if the plan is self-insured and self-administered. The law also provides penalties for noncompliance. This law became effective on January 1, 2009.
Newborns’ and Mothers’ Health Protection Act & Maternity Minimum Stay Provisions Under Federal law, group health plans and health insurance issuers offering group health insurance coverage generally may not restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a delivery by cesarean section. However, the plan or issuer may pay for a shorter stay if the attending provider (e.g. your physician, nurse midwife, or physician assistant), after consultation with the mother, discharges the mother or newborn earlier.

Also, under Federal law, plans and issuers may not set the level of benefits or out-of-pocket costs so that any later portion of the 48-hour (or 96-hour) stay is treated in a manner less favorable to the mother or newborn than any earlier portion of the stay. In addition, a plan or issuer may not, under Federal law, require that a physician or other health care provider obtain authorization for prescribing a length of stay of up to 48 hours (or 96 hours). However, to use certain providers or facilities, or to reduce your out-of-pocket costs, you may be required to obtain precertification. For information on precertification, call the member phone number on your health plan ID card. If the hospital stay is less than 48 hours after a normal vaginal delivery or less than 96 hours after a cesarean delivery, this plan will cover a follow-up visit for the mother and newborn within 48 hours of discharge, when prescribed by the treating physician. This visit shall be provided by a licensed health care provider whose scope of practice includes postpartum and newborn care. The treating physician, in consultation with the mother, shall determine whether this visit shall occur at home, in a medical facility, or at the physician’s office.
Women’s Health and Cancer Rights Act (WHCRA) As required by the Women’s Health and Cancer Rights Act of 1998, our medical plan provides benefits for mastectomy, including reconstruction and surgery to achieve symmetry between the breasts, prostheses, and complications resulting from a mastectomy (including lymphedema). If you are receiving benefits in connection with a mastectomy, benefits are also provided for the following covered health services, as you determine appropriate with your attending physician: o All stages of reconstruction of the breast on which the mastectomy was performed; o Surgery and reconstruction of the other breast to produce a symmetrical appearance; and o Prostheses; and o Treatment of physical complications of the mastectomy, including lymphedema. The amount you must pay for such covered health services (including copayments, coinsurance and any annual deductible) and the benefit coverage limitations are the same as are required for any other covered health service as described in your Summary Plan Description.
Genetic Information Non-Discrimination Act (GINA) In accordance with GINA, this Plan does not deny coverage or benefits, or charge a higher rate or premium, to an otherwise healthy individual found to have a potential genetic condition or genetic predisposition towards a disease or disorder. GINA defines genetic information as that obtained from an individual’s genetic test results, as well as genetic test results of family members and the occurrence of a disease or disorder in family members.

Notice of Privacy Practices for the Use and Disclosure of Private Health Information
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Effective Date: September 1, 2013
The Dyno Nobel Inc. Employee Benefits Plan (“the Plan”) is required by law to maintain the privacy of Protected Health Information (PHI) and to provide individuals with notice of our legal duties and privacy practices with respect to PHI. PHI is information that may identify you and that relates to your past, present or future physical or mental health or condition and related health care services. This Notice of Privacy Practices (Notice) describes how we may use and disclose PHI to carry out treatment, payment or health care operations and for other specified purposes that are permitted or required by law. This Notice also describes your rights with respect to PHI about you.
The Plan is required to follow the terms of this Notice. We will not use or disclose PHI about you without your written au thorization, except as describe in this Notice. We reserve the right to change our practices and this Notice, and to make the new Notice effective for all PHI we maintain. Upon request, we will provide any revised Notice to you.
SECTION 1 – NOTICE OF PHI USES AND DISCLOSURES
Required PHI Uses and Disclosures.
Upon your request, the Plan is required to give you access to certain PHI in order to inspect and copy it.
Use and disclosure of your PHI may be required by the Secretary of the Department of Health and Human Services to investigate or determine the Plan’s compliance with the privacy regulations.
Uses and disclosures to carry out treatment, payment, and health care operations.
The Plan and its business associates will use PHI without your consent, authorization or opportunity to agree or object to carry out treatment, payment and health care operations. The Plan also will disclose PHI to the Plan Sponsor Dyno Nobel Inc. for purposes related to treatment, payment and health care operations. The Plan Sponsor has amended its plan documents to protect your PHI as required by federal law.
Treatment is the provision, coordination or management of health care and related services. It also includes but is not limited to consultations and referrals between one or more of your providers. For example, the Plan may disclose to a treating orthodontist the name of your treating dentist so that the orthodontist may ask for your dental X-rays from the treating dentist.
Payment includes but is not limited to actions to make coverage determinations and payment (including billing, claims management, subrogation, plan reimbursement, reviews for medical necessity and appropriateness of care and utilization review and preauthorizations). For example, the Plan may tell a doctor whether you are eligible for coverage or what percentage of the bill will be paid by the Plan.
Health care operations include but are not limited to quality assessment and improvement, reviewing competence or qualifications of health care professionals, underwriting, premium rating and other insurance activities relating to creating or renewing insurance contracts. It also includes disease management, case management, conducting or arranging for medical review, legal services and auditing functions including fraud and abuse compliance programs, business planning and development, business management and general administrative activities. For example, the Plan may use information about your claims to refer you to a disease management program, project future benefit costs or audi t the accuracy of its claims processing functions.
If PHI is used or disclosed for underwriting purposes, the Plan is prohibited from using or disclosing any of your PHI that is genetic information for such purposes.
Uses and disclosures that require your written authorization.
Your written authorization generally will be obtained before the Plan will use or disclose psychotherapy notes about you from your psychotherapist. Psychotherapy notes are separately filed notes about your conversations with your mental health professional during a counsel ing session. They do not include summary information about your mental health treatment. The Plan may use and disclose such notes when needed by the Plan to defend against litigation filed by you.
Uses and disclosures that require that you be given an opportunity to agree or disagree prior to the use or release.
Disclosure of your PHI to family members, other relatives and your close personal friends is allowed if:
• the information is directly relevant to the family or friend’s involvement with your care or payment for that care; and, you have either agreed to the disclosure or have been given an opportunity to object and have not objected.

26
Uses and disclosures for which consent, authorization or opportunity to object is not required.
Use and disclosure of your PHI is allowed without your consent, authorization or request under the following circumstances:
1. When required by law. 2. When permitted for purposes of public health activities, including when necessary to report product defects, to permit product recalls and to
conduct post-marketing surveillance. PHI may also be used or disclosed if you have been exposed to a communicable disease or are at risk o f spreading a disease or condition, if authorized by law.
3. When authorized by law to report information about abuse, neglect, or domestic violence to public authorities if there exists a reasonable belief that you may be a victim of abuse, neglect or domestic violence. In such case, the Plan will promptly inform you that such a disclosure has been or will be made unless that notice would cause a risk of serious harm. For the purpose or reporting child abuse or neglect, i t is not necessary to inform the minor that such a disclosure has been or will be made. Disclosure may generally be made to the minor’s parents or other representatives although there may be circumstances under federal or state law when the parents or other representatives may not be given access to the minor’s PHI.
4. The Plan may disclose your PHI to a public health oversight agency for oversight activities authorized by law. This includes uses or disclosures in civil, administrative or criminal investigations; inspections; licensure or disciplinary actions (for example, to investigate complaints against providers); and other activities necessary for appropriate oversight of government benefit programs (for example, to investigate Medicare or Medicaid fraud).
5. The Plan may disclose your PHI when required for judicial or administrative proceedings. For example, your PHI may be disclosed in response to a subpoena or discovery request provided certain conditions are met. One of those conditions is that satisfactory assurances must be given to the Plan that the requesting party has made a good faith attempt to provide written notice to you, and the notice provided sufficient information about the proceeding to permit you to raise an objection and no objections were raised or were resolved in favor of disclosure by the court or tribunal.
6. When required for law enforcement purposes (for example, to report certain types of wounds). 7. For law enforcement purposes, including for the purpose of identifying or locating a suspect, fugitive, material witness or missing person. Also,
when disclosing information about an individual who is or is suspected to be a victim of a crime but only if the individual agrees to the disclosure or the Covered Entity is unable to obtain the individual’s agreement because of emergency circumstances. Furthermore, the law enforcement official must represent that the information is not intended to be used against the individual, the immediate law enforcement activity would be materially and adversely affected by waiting to obtain the individual’s agreement and disclosure is in the best interest of the individual as determined by the exercise of the Plan’s best judgment.
8. When required to be given to a coroner or medical examiner for the purpose of identifying a deceased person, determining a ca use of death or other duties as authorized by law. Also, disclosure is permitted to funeral directors, consistent with applicable law, as necessary to carry out their duties with respect to the decedent.
9. The Plan may use or disclose PHI for research, subject to conditions. 10. When consistent with applicable law and standards of ethical conduct if the Plan, in good faith, believes the use or disclosure is necessary to
prevent or lessen a serious and imminent threat to the health or safety of a person or the public and the disclosure is to a person reasonably able to prevent or lessen the threat, including the target of the threat.
11. When authorized by and to the extent necessary to comply with workers’ compensation or other similar programs established by law.
Except as otherwise indicated in this notice, uses and disclosures will be made only with your written authorization subject to your right to revoke such authorization.
SECTION II – RIGHTS OF INDIVIDUALS
Right to Request Restrictions on PHI Uses and Disclosures
You may request the Plan to restrict uses and disclosures of your PHI to carry out treatment, payment or health care operatio n, or to restrict uses and disclosures to family members, relatives, friends or other persons identified by you who are involved in your care or payment for your care. However, the Plan is not required to agree to your request.
The Plan will accommodate reasonable requests to receive communications of PHI by alternative means or at alternative locations.
You or your personal representative will be required to complete a form to request restrictions on uses and disclosures of your PHI.
Such requests should be made to the following officer:
Privacy Official/Contact: Benefits Manager Human Resources Department 2795 East Cottonwood Parkway, Suite 500 Salt Lake City, Utah 84121 Phone: (801) 364-4800 For Dyno Nobel Inc. Employee Benefits Plan

Right to Inspect and Copy PHI
You have a right to inspect and obtain a copy of your PHI contained in a “designated record set”, for as long as the plan maintains the PHI.
Protected Health Information (PHI) includes all individually identifiable health information transmitted or maintained by the Plan, regardless of form.
Designated Records Set includes the medical records and billing records about individuals maintained by or for a covered health care provider; enrollment, payment, billing, claims adjudication and case or medical management record systems maintained by or for a health plan; or other information used in whole or in part by or for the Covered Entity to make decisions about individuals. Information used for q uality control or peer review analyses and not used to make decisions about individuals is not in the designated record set.
The requested information will be provided within 30 days if the information is maintained on site or within 60 days if the information is maintained offsite. A single 30-day extension is allowed if the Plan is unable to comply with the deadline. You or your personal representative will be required to complete a form to request access to the PHI in your designated recor d set. Requests for access to PHI should be made to the following officer:
Privacy Official/Contact: Benefits Manager Human Resources Department 2795 East Cottonwood Parkway, Suite 500 Salt Lake City, Utah 84121 Phone: (801) 364-4800 For Dyno Nobel Inc. Employee Benefits Plan
If access is denied, you or your personal representative will be provided with a written denial setting forth the basis for the denial, a description of how you may exercise those review rights and a description of how you may complain to the Secretary of U.S. Department of Health and Human Services.
Right to Amend PHI
You have the right to request the plan to amend your PHI or a record about you in a designated record set for as long as the PHI is maintained in the designated record set.
The Plan has 60 days after the request is made to act on the request. A single 30-day extension is allowed if the Plan is unable to comply with the deadline. If the request is denied in whole or part, the Plan must provide you with a written denial that explains the basis for the denial. You or your personal representative may then submit a written statement disagreeing with the denial and have that statement included with any future disclosures of your PHI.
Requests for amendment of PHI in a designated record set should be made to the following officer:
Privacy Official/Contact: Benefits Manager Human Resources Department 2795 East Cottonwood Parkway, Suite 500 Salt Lake City, Utah 84121 Phone: (801) 364-4800 For Dyno Nobel Inc. Employee Benefits Plan
You or your personal representative will be required to complete a form to request amendment of the PHI in your designated record set.
The Right to Receive an Accounting of PHI Disclosures
At your request, the Plan will also provide you with an accounting of disclosures by the Plan of your PHI during the six years prior to the date of your request. However, such accounting need not include PHI disclosures made:
1. to carry out treatment, payment or health care operations; 2. to individuals about their own PHI; 3. prior to the compliance date; or, 4. based on your written authorization.
If the accounting cannot be provided within 60 days, an additional 30 days is allowed if the individual is given a written statement of the reasons for the delay and the date by which the accounting will be provided.
If you request more than one accounting within a 12-month period, the Plan will charge a reasonable, cost-based fee for each subsequent accounting.
The Right to Receive a Paper Copy of This Notice Upon Request

To obtain a paper copy of this Notice contact the following officer: Privacy Official/Contact: Benefits Manager Human Resources Department 2795 East Cottonwood Parkway, Suite 500 Salt Lake City, Utah 84121 Phone: (801) 364-4800 For Dyno Nobel Inc. Employee Benefits Plan
The Right to Be Notified of a Breach of Unsecured PHI The Plan is required by law to notify you following a breach of any Unsecured PHI.
A Note about Personal Representatives
You may exercise your rights through a personal representative. Your personal representative will be required to produce evidence of his/her authority to act on your behalf before that person will be given access to your PHI or allowed to take any action for you. Pr oof of such authority may take one of the following forms:
• a power of attorney for health care purposes, notarized by a notary public; • a court order of appointment of the person as the conservator or guardian of the individual; or, • an individual who is the parent of a minor child.
The Plan retains discretion to deny access to your PHI to a personal representative to provide protection to those vulnerable people who depend on others to exercise their rights under these rules and who may be subject to abuse or neglect. This also applies to personal representatives of minors.
SECTION III – THE PLAN’S DUTIES
The Plan is required by law to maintain the privacy of PHI and to provide individuals (participants and beneficiaries) with notice of its legal duties and privacy practices.
This notice is effective beginning September 1, 2013 and the Plan is required to comply with the terms of this notice. However, the Plan reserves the right to change its privacy practices and to apply the changes to any PHI received or maintained by the Plan prior to that date. If a privacy practice is changed, a revised version of this notice will be provided (to all past and present participants and beneficiaries) for whom the Plan still maintains PHI. Revised notices will be provided via electronic mail and posted on the company intranet within 60 day of the material revision to the notice.
Any revised version of this notice will be distributed within 60 days of the effective date of any material change to the use s or disclosures, the individual’s rights, the duties of the Plan or other privacy practices stated in this notice.
Minimum Necessary Standard
When using or disclosing PHI or when requesting PHI from another Covered Entity, the plan will make reasonable efforts not to use, disclose or request more than the minimum amount of PHI necessary to accomplish the intended purpose of the use, disclosure or request, taking into consideration practical and technological limitations.
However, the minimum necessary standard will not apply in the following situations:
• disclosures to or requests by a health care provider for treatment; • uses or disclosures made to the individual; • disclosures made to the Secretary of the U.S. Department of Health and Human Services; • uses or disclosures that are required by law; and, • uses or disclosures that are required for the Plan’s compliance with legal regulations.
This notice does not apply to information that has been de-identified. De-identified information is information that does not identify an individual and with respect to which there is to reasonable basis to believe that the information can be used to identify an individual is not individually identifiable health information.
In addition, the Plan may use or disclose “summary health information” to the plan sponsor for obtaining premium bids or modi fying, amending or terminating the Group Health Plan, which summarizes the claims history, claims expenses or type of claims experienced by individuals for whom a plan sponsor has provided health benefits under a Group Health Plan; and from which identifying information has been deleted in accordance with HIPAA.
If the plan sponsor creates, receives, maintains, or transmits any electronic PHI (other than enrollment/disenrollment information and Summary Health Information, which are not subject to these restrictions) on behalf of the covered entity, it will implement administrative, physical,

and technical safeguards that reasonably and appropriately protect the confidentiality, integrity, and availability of the electronic protected health information, and it will ensure that any agents (including subcontractors) to whom it provides such electronic PHI agrees to implement reasonable and appropriate security measures to protect the information. The plan sponsor will report to the Plan any security incident of which it becomes aware.
The plan sponsor will ensure that the provisions of this Section are supported by reasonable and appropriate security measures to the extent that the designees have access to electronic PHI.
SECTION IV – YOUR RIGHT TO FILE A COMPLAINT WITH THE PLAN OR THE HHS SECRETARY
If you believe that your privacy rights have been violated, you may complain to the Plan in care of the following officer:
Privacy Official/Contact: Benefits Manager Human Resources Department 2795 East Cottonwood Parkway, Suite 500 Salt Lake City, Utah 84121 Phone: (801) 364-4800 For Dyno Nobel Inc. Employee Benefits Plan
You may file a complaint with the Secretary of the U.S. Department of Health and Human Services, Hubert H. Humphrey Building, 200 Independence Avenue S.W., Washington, D.C. 20201.
The Plan will not retaliate against you for filing a complaint.
SECTION V – WHOM TO CONTACT AT THE PLAN FOR MORE INFORMATION
If you have any questions regarding this notice or the subjects addressed in it, you may contact the Human Resources Department.

Medicaid and the Children’s Health Insurance Program (CHIP) Offer Free Or Low-Cost Health Coverage To Children And Families
If you are eligible for health coverage from your employer, but are unable to afford the premiums, some States have premium assistance programs that can help pay for coverage. These States use funds from their Medicaid or CHIP programs to help people who are eligible for employer-sponsored health coverage, but need assistance in paying their health premiums.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, you can contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, you can contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, you can ask the State if it has a program that might help you pay the premiums for an employer-sponsored plan.
Once it is determined that you or your dependents are eligible for premium assistance under Medicaid or CHIP, your employer’s health plan is required to permit you and your dependents to enroll in the plan – as long as you and your dependents are eligible, but not already enrolled in the employer’s plan. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance.
If you live in one of the following States, you may be eligible for assistance paying your employer health plan premiums. The following list of States is current as of January 31, 2011. You should contact your State for further information on eligibility –
ALABAMA – Medicaid
CALIFORNIA – Medicaid
Website: http://www.medicaid.alabama.gov Phone: 1-800-362-1504
Website: http://www.dhcs.ca.gov/services/Pages/ TPLRD_CAU_cont.aspx Phone: 1-866-298-8443
ALASKA – Medicaid COLORADO – Medicaid and CHIP
Website: http://health.hss.state.ak.us/dpa/programs/medicaid/ Phone (Outside of Anchorage): 1-888-318-8890 Phone (Anchorage): 907-269-6529
Medicaid Website: http://www.colorado.gov/ Medicaid Phone (In state): 1-800-866-3513 Medicaid Phone (Out of state): 1-800-221-3943 CHIP Website: http:// www.CHPplus.org CHIP Phone: 303-866-3243
ARIZONA – CHIP FLORIDA – Medicaid Website: http://www.azahcccs.gov/applicants/default.aspx Phone (Outside of Maricopa County): 1-877-764-5437 Phone (Maricopa County): 602-417-5437
Website: http://www.fdhc.state.fl.us/Medicaid/index.shtml Phone: 1-877-357-3268
ARKANSAS – CHIP MISSOURI – Medicaid
Website: http://www.arkidsfirst.com/ Phone: 1-888-474-8275
Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
GEORGIA – Medicaid MONTANA – Medicaid Website: http://dch.georgia.gov/
Click on Programs, then Medicaid Phone: 1-800-869-1150
Website: http://medicaidprovider.hhs.mt.gov/clientpages/ clientindex.shtml Phone: 1-800-694-3084
IDAHO – Medicaid and CHIP NEBRASKA – Medicaid Medicaid Website: www.accesstohealthinsurance.idaho.gov Medicaid Phone: 1-800-926-2588 CHIP Website: www.medicaid.idaho.gov CHIP Phone: 1-800-926-2588
Website: http://www.dhhs.ne.gov/med/medindex.htm Phone: 1-877-255-3092
INDIANA – Medicaid NEVADA – Medicaid and CHIP Website: http://www.in.gov/fssa Phone: 1-800-889-9948 IOWA – Medicaid
Website: www.dhs.state.ia.us/hipp/ Phone: 1-888-346-9562
Medicaid Website: http://dwss.nv.gov/ Medicaid Phone: 1-800-992-0900 CHIP Website: http://www.nevadacheckup.nv.org/ CHIP Phone: 1-877-543-766

KANSAS – Medicaid NEW HAMPSHIRE – Medicaid Website: https://www.khpa.ks.gov Phone: 1-800-792-4884
Website: www.dhhs.nh.gov/ombp/index.htm Phone: 603-271-4238
KENTUCKY – Medicaid NEW JERSEY – Medicaid and CHIP Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570 LOUISIANA – Medicaid Website: http://www.lahipp.dhh.louisiana.gov Phone: 1-888-342-6207
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 1-800-356-1561 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
MAINE – Medicaid NEW MEXICO – Medicaid and CHIP Website: http://www.maine.gov/dhhs/OIAS/public- assistance/index.html Phone: 1-800-321-5557 MASSACHUSETTS – Medicaid and CHIP Medicaid & CHIP Website: http://www.mass.gov/MassHealth Medicaid & CHIP Phone: 1-800-462-1120
Medicaid Website: http://www.hsd.state.nm.us/mad/index.html Medicaid Phone: 1-888-997-2583 CHIP Website: http://www.hsd.state.nm.us/mad/index.html
Click on Insure New Mexico CHIP Phone: 1-888-997-2583
MINNESOTA – Medicaid TEXAS – Medicaid Website: http://www.dhs.state.mn.us/
Click on Health Care, then Medical Assistance Phone (Outside of Twin City area): 800-657-3739 Phone (Twin City area): 651 -431-2670
Website: https://www.gethipptexas.com/ Phone: 1-800-440-0493
NEW YORK – Medicaid UTAH – Medicaid Website: http://www.nyhealth.gov/health_care/medicaid/ Phone: 1-800-541-2831
Website: http://health.utah.gov/upp Phone: 1-866-435-7414
NORTH CAROLINA – Medicaid VERMONT– Medicaid Website: http://www.nc.gov Phone: 919-855-4100
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
NORTH DAKOTA – Medicaid VIRGINIA – Medicaid and CHIP Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-800-755-2604 OKLAHOMA – Medicaid Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
Medicaid Website: http://www.dmas.virginia.gov/rcp- HIPP.htm Medicaid Phone: 1-800-432-5924 CHIP Website: http://www.famis.org/ CHIP Phone: 1-866-873-2647
OREGON – Medicaid and CHIP WASHINGTON – Medicaid Medicaid & CHIP Website: http://www.oregonhealthykids.gov Medicaid & CHIP Phone: 1-877-314-5678
Website: http://hrsa.dshs.wa.gov/premiumpymt/Apply.shtm Phone: 1-800-562-3022 ext. 15473
PENNSYLVANIA – Medicaid WEST VIRGINIA – Medicaid Website: http://www.dpw.state.pa.us/partnersproviders/medicalassis tance/doingbusiness/003670053.htm Phone: 1-800-644-7730
Website: http://www.wvrecovery.com/hipp.htm Phone: 304-342-1604
RHODE ISLAND – Medicaid WISCONSIN – Medicaid Website: www.dhs.ri.gov Phone: 401-462-5300
Website: http://www.badgercareplus.org/pubs/p-10095.htm Phone: 1-800-362-3002
SOUTH CAROLINA – Medicaid WYOMING – Medicaid Website: http://www.scdhhs.gov Phone: 1-888-549-0820
Website: ttp://www.health.wyo.gov/healthcarefin/index.html Phone: 307-777-7531
To see if any more States have added a premium assistance program since January 31, 2012, or for more information on special enrollment rights, you can contact either:
U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Ext. 61565


GBS BENEFITS , INC.
465 South 400 East, Suite 300 Salt Lake City, UT 84111
Phone (801) 364-7233