©2014 mfmer | slide-1 tb class arrivals: targeted testing and treatment of foreign-born persons...
TRANSCRIPT

©2014 MFMER | slide-1
TB Class Arrivals:Targeted testing and treatment of foreign-born persons
Alicia Earnest, MPHSeptember 18, 2014

Disclosures
Relevant Financial Relationships
None
Off-Label/Investigational Uses
None

Learning Objectives
After this presentation, participants will be able to:
1. Name two types of U.S. visas that do not require that the person undergo TB testing prior to arriving in the U.S.
2. Describe the differences in TB Class designations by overseas screening results.
3. Describe the purpose of the domestic TB medical evaluation recommended after an individual with a TB Class condition identified overseas arrives in the U.S.

Learning Objectives
After this presentation, participants will be able to:
4. Describe the different roles of state TB control, local public health agencies, private providers, community clinics, and refugee resettlement agencies in ensuring that immigrants and refugees with TB Class conditions are evaluated after arriving in the U.S.
5. Name two barriers to successful TB follow-up evaluation and describe how they may be overcome.

Abbreviations• CXR = chest X-ray
• DTBE = Division of TB Elimination (CDC)
• DGMQ = Division of Global Migration and Quarantine (CDC)
• IGRA = Interferon Gamma Release Assay
• MTB = Mycobacterium tuberculosis
• Q-station/QS = Quarantine Station (CDC)
• TB TIs = TB Technical Instructions (guidelines) issued by CDC
• TST = tuberculin skin test

Outline1. TB Control in the U.S. and the global reality2. Background on TB Class designations
• Who? What? Why? When?3. Domestic TB Class Follow-up Evaluation
• Purpose• Recommended protocol
4. Roles of different players in North Dakota• Refugees vs. immigrants• Data collection tool• Barriers
5. Resources

TB Prevention and Control Strategies
1. Active TB disease
2. Contact investigation
3. Targeted testing and treatment of LTBI
4. Infection control measures in high-risk settings

TB Worldwide“TB is a social disease with medical implications.”
• It is estimated that 1/3 of the world’s population is infected with Mycobacterium tuberculosis.
• In 2010, a total of 8.8 million people worldwide became sick with TB disease, most of whom (82%) live in one of the 22 high burden countries for TB.*
• While the U.S. is a low-burden country for TB, this disease remains an urgent public health problem in many other parts of the world.
• TB in the U.S. reflects the global nature of this disease.
*CDC. (2012) CDC’s Role in Global TB Control. http://www.cdc.gov/tb/topic/globaltb/role.htm. Accessed 4 Sept 2014.
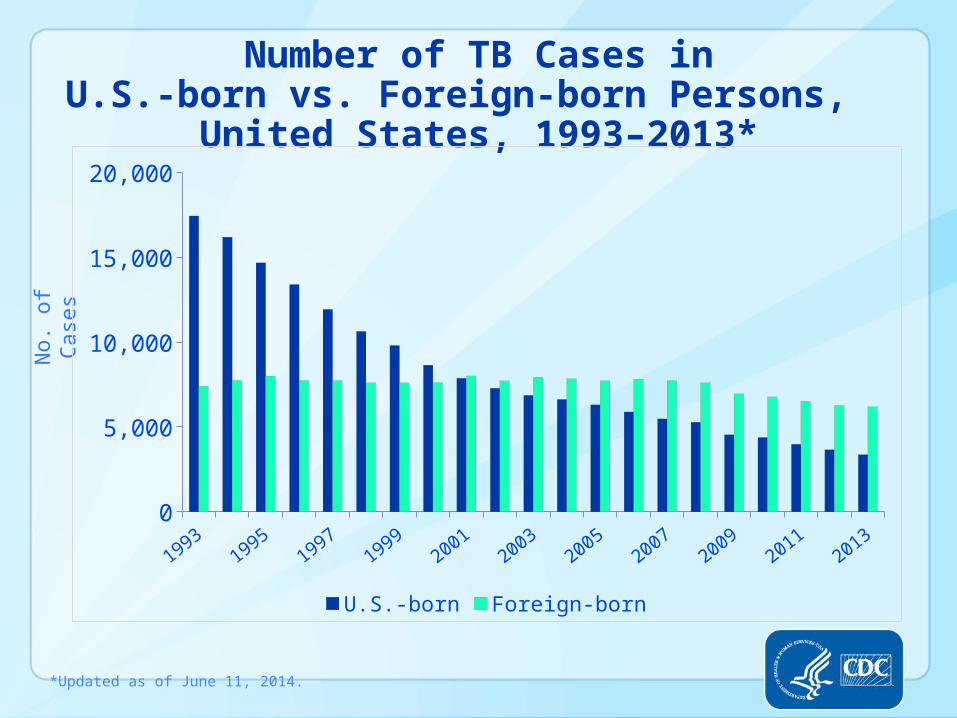
Number of TB Cases inU.S.-born vs. Foreign-born Persons,
United States, 1993–2013*
*Updated as of June 11, 2014.
No. of
Case
s
19931995
19971999
20012003
20052007
20092011
20130
5,000
10,000
15,000
20,000
U.S.-born Foreign-born

Trends in TB Cases in Foreign-born Persons,
United States, 1993 – 2013*
*Updated as of June 11, 2014.
No. of Cases Percentage
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
0%
10%
20%
30%
40%
50%
60%
70%
Number of Cases Percent of Total Cases

2003 2013
DC
*Updated as of June 11, 2014.
Percentage of TB Cases Among Foreign-born Persons, United States*
DC
>50%25%–49%<25%No cases

Data source: North Dakota Department of Health
80%
75%
100%
15%
33%
63%
North Dakota

Opportunities for TB Screening
• Overseas Exam
- TB Class determination• Domestic Refugee Health Assessment• Domestic TB Class Follow-up • Adjustment of Status• Primary care

Refugee Health Program, Minnesota Department of Health
U.S.A.
U.S. Citizen Non-Citizen (Foreign-born)
Persons fleeing from persecution
LPR
Immigrant*
LTR authorized employment
Non-Immigrant
student tourist
refugee asylee parolee
undocumented individual
Dept. of Homeland Security DefinitionsDept. of Homeland Security Definitions
visitor on business
*Immigrants have O/S exam (Non-Immigrants do not)
Background

Background
1. Lawful permanent residents (LPR) “green card”:
• Relatives of U.S. citizens or LPRs • Fiancées • Adoptees• Employees and investors• Special immigrant visas• Diversity program
All persons applying for immigrant visas MUST have a medical exam done overseas as part of their application process. This includes:

Background
2. Lawful temporary residents (LTR) – Must adjust their status to LPR after one year.
• Refugees• Asylees• Parolees
All persons applying for immigrant visas MUST have a medical exam done overseas as part of their application process. This includes:

Background
• Students• Tourists• Temporary employment• Business visitors• Diplomats, athletes, entertainers
Persons who wish to enter the U.S. temporarily apply for non-immigrant visas and do not need a medical exam. This includes:

Medical Examination for Entry into the U.S.Pre-immigration or Overseas Exam
Purpose: To screen for certain medical conditions relevant to U.S. law• Required for entry into the U.S. as an immigrant
• Administered by Panel Physicians (training and guidelines provided by CDC)
• NOT a comprehensive medical exam; expires in 3-6 months
Screening for “excludable conditions”:• Communicable diseases of public health significance (including TB)
• Physical and mental disorders with associated harmful behaviors
• Psychoactive substance abuse and dependence
• Other physical or mental abnormalities, disorders, or disabilities
Background

BackgroundTuberculosis Screening and Treatment Technical Instructions (TIs) using Cultures and Directly Observed Therapy (DOT) for
Panel Physicians (‘07 TB TIs)• Revised in 2007 from 1991 TB TIs
• Global implementation – all countries as of October 1, 2013• DTBE & DGMQ involvement• Small update in 2009
Examining chest x-rays, National TB Institute, Kabul, Afghanistan (WHO/TDR/Perkins)
Woman receiving TB drugs at a clinic in Cotonou, Benin (CDC)

‘07 TB TIs Components• Medical history• Physical examination• TST (for ages 2-14) or IGRA*• CXR (for ages >15 and those younger with + TST/IGRA)• If abnormal CXR:
• Sputum smears & cultures • Drug susceptibility testing on positive cultures • Treatment for active disease• Identify contacts to cases of TB disease
Background
*Does not apply in countries where TB incidence rate is <20 cases per 100,000 population.

TB Classifications – 2007 TIsClass A TB – active TB disease, sputum smear and/or culture positive; requires a waiver (i.e., on treatment and smear negative prior to travel).
Class B1 TB, Pulmonary – CXR abnormal suggestive of TB with negative sputum smears and cultures; includes previously treated TB.
Class B2 TB – LTBI (TST > 10 mm or IGRA +) and normal CXR
Class B3 TB – recent contact of a known infectious TB case
Class B1 TB, Extrapulmonary – evidence of extrapulmonary TB
Background

Electronic Disease Notification (EDN)• Electronic notification system for all refugee and TB Class
arrivals• Provides overseas exam information for arrivals• Database for outcomes of TB Class arrivals• Enables states to transfer records to other states• ALL states and Q-stations participating• Housed at CDC – DGMQ
Background

BackgroundFlow of information:
Overseas exam
DGMQ Quarantine
StationEDN
LPHND
Dept of Health
Provider

Opportunities for TB Screening
• Overseas Exam
- TB Class determination• Domestic Refugee Health Assessment• Domestic TB Class Follow-up • Adjustment of Status• Primary care

Domestic TB Class Follow-up Evaluation
Why is this follow-up evaluation important?
The overseas exam only clears the person for travel to the U.S. It rules out active, pulmonary, infectious TB at time of exam. It is not meant to be diagnostic of other TB conditions.
What is the purpose of the follow-up evaluation?
To evaluate the person for active pulmonary TB, extrapulmonary TB, and LTBI, and to treat these conditions, if found.

Domestic TB Class Follow-up EvaluationCDC indicators for TB Class Follow-up:
For immigrants and refugees with CXRs read overseas as consistent with active TB (Class B1):
• % Evaluation initiated within 30 days of notification
• % Evaluation completed within 90 days of notification
• % LTBI treatment initiated (if LTBI diagnosed in the U.S.)
• % LTBI treatment completed (if LTBI treatment initiated)

Domestic TB Class Follow-up EvaluationTB Screening Recommendations:
• Varies slightly by TB Class
• Evaluate all for signs and symptoms of TB disease.
• Screen all with a TST or IGRA, unless they have:
• Reliable documentation of a previous positive result or
• Reliable history of TB disease

Domestic TB Class Follow-up Evaluation
TB Screening Recommendations:
• CXR for those with positive TST or IGRA.
• Class B1: should always have a CXR –regardless of TST or IGRA result or treatment history.
• Ideally the arrival should have a CD of their overseas CXR with them for comparison.

Domestic TB Class Follow-up Evaluation
TB Screening Recommendations:
• Detailed recommendations by TB Class available on the MDH TB Program website: http://www.health.state.mn.us/divs/ idepc/diseases/tb/hcp/classrecs.pdf
• If active TB cannot be ruled out, further testing is needed (i.e., sputum smear and culture).
• Come to a diagnosis.
• If LTBI or active disease, initiate treatment as appropriate.

Domestic TB Class Follow-up EvaluationIGRA use in foreign-born persons:
Preferred due to better specificity than the TST• Specific to Mycobacterium tuberculosis• Does not detect BCG
Important for foreign-born persons in the U.S.• May have been exposed to non-TB mycobacteria• Many come from countries where BCG vaccination is
common
Not recommended for children under 5 years old.

Domestic TB Class Follow-up EvaluationIGRA use in foreign-born persons:
Recently issued MDH recommendations specific to this population:
Use of IGRAs to Detect LTBI in Foreign-Born Persons – Recommendations from the Minnesota Department of Health:http://www.health.state.mn.us/divs/idepc/diseases/tb/igrarecs.pdf

Refugee Admissions Ceilings for FY2013
Ceiling: 70,000
Source: US Department of State
Actual No. of Arrivals: 69,930

The Numbers for North Dakota
Year* 2014** 2013 2012 2011 2010 2009
Refugees (all) 564 449 555 354 470 438
Immigrants with TB Class conditions
18 33 17 6 10 5
*Federal fiscal year **Through August 21, 2014
Top countries of origin for refugees:Bhutan, Iraq, Somalia, Congo, Sudan
Top cities of resettlement for refugees:Fargo/West Fargo (~75%), Grand Forks, Bismarck
Data source: Lutheran Social Services of North Dakota and EDN

State TB Control Role
1. Receive notifications of new arrivals from EDN. Print records, EDN TB Follow-up Worksheet, and forward to the appropriate local health department.
2. Provide consultation as needed.
3. Ensure the results of the evaluation are returned.
4. Enter results into the EDN system.

Refugee Resettlement Agency Role
Lutheran Social Services of North Dakota
• Arrange for screening appointment for the new arrival.
• Provide or arrange for transportation to the screening appointment.
• Provide health and safety orientation and introduction to U.S. healthcare system.

Local Public Health Role
1. Contact the arrival, explain the importance of the follow-up exam, and help the arrival obtain a TB evaluation with a local provider (immigrants only).
2. Ensure the results of the evaluation are submitted to the North Dakota Department of Health and that data is accurate and complete.
3. Facilitate medical treatment for any TB-related condition that is identified.

Private Provider and Community Clinic Role
1. Screen arrival for TB according to recommendations.
2. Report all positive TSTs, QFTs, and suspected or confirmed cases of TB disease to the North Dakota Department of Health.
3. Encourage uptake and refer for treatment for LTBI, if found, through the local health department.
4. Fill out the EDN TB Follow-up Worksheet and return to the local health department. Instructions available: http://www.health.state.mn.us/divs/idepc/diseases/tb/hcp/classwkshtguid.pdf

EDN TB Follow-up Worksheet

Barriers to Evaluation• Invalid contact information• Lack of insurance or payment source• Traveling back to home country• Stigma of TB• One of many health issues• Culture• Trust of the health care system• Transportation• Language barrier

OutcomesWhy is this worth the effort?
For public health:
• Identify and treat cases of TB• Prevent future cases of TB• Greater understanding of TB trends in mobile populations• Targeted resources to those most at risk• Development of systems and tools to serve diverse populations
For the patient:
• Access to health care system• Greater empowerment and understanding of health care system• Treatment for their condition• Improved health and wellbeing

ResourcesNorth Dakota Department of Health TB page:http://www.ndhealth.gov/Disease/TB/default.htm
MDH TB Class Arrival Website: http://www.health.state.mn.us/divs/idepc/diseases/tb/hcp/classarrival.htmlIncludes links to:• Recommended Medical Follow-up for TB Class Arrivals• Instructions for Completion of TB Class Follow-up Worksheet
CDC’s Tuberculosis Screening and Treatment Technical Instructions (TB TIs) Using Cultures and Directly Observed Therapy (DOT) for Panel Physicians: http://www.cdc.gov/immigrantrefugeehealth/exams/ti/panel/tuberculosis-panel-technical-instructions.html

ResourcesTB Technical Instructions for Panel Physicians: Implications for U.S. Practitioners• 2012 webinar by the New Jersey Medical School/Rutgers
Global TB Institutehttp://globaltb.njms.rutgers.edu/educationalmaterials/ audioarchives.html
CDC Division of Global Migration and Quarantine (DGMQ):http://www.cdc.gov/ncezid/dgmq/
CDC’s Updated Guidelines for Using IGRAs to Detect MTB infection – United States, 2010: http://www.cdc.gov/mmwr/PDF/rr/rr5905.pdf

Acknowledgements
• Mayo Clinic Center for Tuberculosis
• Dee Pritschet, ND TB Controller
• Laetitia Mizero, MS, State Refugee Coordinator, Lutheran Social Services of North Dakota
• Linda Schell, MSW, Assistant State Refugee Coordinator, Lutheran Social Services of North Dakota
• Marlene Espejo, RN, Family HealthCare Center - Fargo

language that you will never be so smart or funny in as in your true language. It takes years to start to feel semi-normal. And yet people still come from Russia, Vietnam and Cambodia and Laos, Ethiopia, Iran, Haiti, Korea, Cuba, Chile, and they come on behalf of their children, and they come for freedom. Not for our land (Russia is as beautiful), not for our culture (they have their own, thank you), not for our system of government (they don't even know about it, maybe not even agree with it), but for freedom. They are heroes who make an adventure on our behalf, showing by their struggle how precious beyond words freedom is, and if we knew their stories, we could not keep back the tears."
Final Quote"Heroes, all of them, at least they're my heroes, especially the new immigrants, especially the refugees. Everyone makes fun of the New York cab drivers who can't speak English: they're heroes. To give up your country is the hardest thing a person can do: to leave the old familiar places and ship out over the edge of the world to America and learn everything over again different than you learned as a child, learn the new
- Garrison Keillor

Contact Information:
Alicia Earnest, MPH TB Follow-up Data Coordinator
Minnesota Department of Health651-201-5523 (office)651-201-5500 (fax)
Thank you!