2018 pharmacy benefit summary book - fep blue · 2018 pharmacy benefit summary book fepblue.org. 2...
TRANSCRIPT

2018 PHARMACY BENEFIT SUMMARY BOOK
fepblue.org

2
Review this summary booklet to learn how to get the most from your pharmacy benefit such as:
n Your pharmacy benefits and highlights
n Your formulary and cost share
n Ways to save moneyn Filing a claim
Your pharmacy benefitThe Blue Cross and Blue Shield Service Benefit Plan works with Pharmacy Benefit Managers (PBMs) to administer your pharmacy benefit.
n Retail Pharmacy Program - CVS Caremark®
n Mail Service Pharmacy Program - CVS Caremark
n Specialty Pharmacy Program - AllianceRx Walgreens Prime
General questions n See the Blue Cross and Blue Shield Service
Benefit Plan brochure (RI 71-005)
n Visit fepblue.org
n Call CVS Caremark Customer Service for Retail and Mail Service Pharmacy Programs toll-free at 1-800-624-5060
n Call AllianceRx Walgreens Prime for Specialty Pharmacy Program toll-free at 1-888-346-3731
NEW FOR 2018 n Expanded “Managed Not Covered” drug list See p. 2
n Cost share increases for certain Tier 3 drugs See pgs. 6-12
n Preventive benefit for cholesterol-lowering drugs See p. 22
n Lower cost share for certain asthma drugs See p. 22
n Lower cost share for certain high blood pressure drugs See p. 23
n Dispense as Written cost share change See p. 23
n Medical Foods Benefit See p. 23

1
TABLE OF CONTENTS
Your Pharmacy Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 n Pharmacy Benefit Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 n Formulary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 n Quantity Limits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 n Prior Approval . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Your Cost Share . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 n How Tiers Relate to Costs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 n Basic Option Cost Share Tiers . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 n Standard Option Cost Share Tiers . . . . . . . . . . . . . . . . . . . . . . . . 8 n Basic Option Medicare Part B Cost Share Tiers. . . . . . . . . . . . . 10 n Standard Option Medicare Part B Cost Share Tiers . . . . . . . . . . 12
Ways to Save . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 n Be a Smart Consumer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 n Use Preferred Brand Name Drugs . . . . . . . . . . . . . . . . . . . . . . . 15 n Use Generics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15 n Use Preferred Specialty Drugs If You Have a Specialty Prescription. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 n Use the Mail Service Pharmacy for Long-term Drugs . . . . . . . . 18 n Use a Preferred Retail Pharmacy . . . . . . . . . . . . . . . . . . . . . . . . 19
Filing a Claim . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 n Retail Pharmacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 n Overseas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 n Drugs from Supplementary Providers . . . . . . . . . . . . . . . . . . . . 21 n Hospital Outpatient Departments. . . . . . . . . . . . . . . . . . . . . . . . 21
Pharmacy Benefit Highlights . . . . . . . . . . . . . . . . . . . . . . . . 22 n Cholesterol-lowering Drug Benefit . . . . . . . . . . . . . . . . . . . . . . . 22 n Asthma Drug Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22 n High Blood Pressure Drug Benefit . . . . . . . . . . . . . . . . . . . . . . . 23 n Dispense as Written Cost Share Change . . . . . . . . . . . . . . . . . . 23n Medical Foods Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23n Contraceptive Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 n Diabetic Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 n Wellness Incentives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 n Other Programs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Fepblue.org . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Find it Fast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Find a Form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29How to Contact Us . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32

2
Pharmacy Benefit Options
Understanding your pharmacy benefit will save you time and money. Your Basic or Standard Option benefits will cover many of your prescription costs.
You have four ways to get the prescription drugs you need:
1. Preferred Retail Pharmacies: for all Service Benefit Plan members
See p. 19
2. Mail Service Pharmacy Program: for all Standard Option members and Basic Option members with Medicare Part B
See p. 18
3. Specialty Pharmacy Program: for all Service Benefit Plan members
See p. 16-17
4. Non-preferred Retail Pharmacies: for Standard Option members
See p. 19
Formulary, Exclusions and “Managed Not Covered” Drugs
The formulary is a complete list of your covered prescription drugs. It includes generic, brand name, and specialty drugs, as well as Preferred drugs that will lower your out-of-pocket costs. The formulary has 5 tiers of drugs.
See p. 5
The Pharmacy and Medical Policy Committee (PMPC) is an independent group of doctors and pharmacists. This group recommends drugs for each tier based on their:
n Effectiveness
n Safety
n How they compare to other drugs in the same class
The PMPC meets every quarter to review new drugs and other changes to the formulary.
YOUR PHARMACY BENEFIT
For the formularies including covered drugs, exclusions and list of “Managed Not Covered” drugs:
- visit fepblue.org/pharmacy - call CVS Caremark for Retail or Mail Order drugs: 1-800-624-5060 - call AllianceRx Walgreens Prime for Specialty drugs: 1-888-346-3731
3
Drugs may change tiers or prior approval status. Check your formulary often to be aware of any changes.
STANDARD OPTION FORMULARY
A few drugs are not covered on the Standard Option drug formulary. These excluded drugs have available covered options in the same class.
BASIC OPTION FORMULARY
Some drugs are not covered on the Basic Option drug formulary. These “Managed Not Covered” drugs have Preferred alternative options in the same class.
Standard and Basic Option members taking an excluded or a “Managed Not Covered” drug should expect to pay the full cost of the prescription.
QUANTITY LIMITS
Certain drugs on the formulary have quantity limits (for example, number of pills). This means your pharmacy benefit will only cover up to a specific amount per prescription or a limited amount per year. Quantity limits help ensure drugs are used safely and appropriately. Drug quantities are approved based on accepted standards of health care practice in the United States.
PRIOR APPROVAL
Some prescription drugs and supplies need approval in advance, or “prior approval” before we provide coverage for them. We need to confirm two things:
n Your use of the drug is related to a service or condition covered under the Service Benefit Plan.
n Your doctor prescribes it in a way that matches generally accepted medical practices.
YOUR PHARMACY BENEFIT

4
FACTS TO KNOW ABOUT PRIOR APPROVAL
n You will need to renew your prior approval periodically.
n Drugs and supplies on the prior approval list may change throughout the year.
n Mail Service and Specialty Programs will not fill prescriptions that need prior approval until you receive prior approval.
n Preferred retail pharmacies will fill your prescriptions, but you will pay the full cost until you get prior approval. Once you have received prior approval, you may file a claim for reimbursement of out-of-pocket costs paid while awaiting approval.
See p. 19
YOUR PHARMACY BENEFIT
Visit fepblue.org/priorapproval. Or call CVS Caremark toll-free any time at 1-800-624-5060. You will be able to:n See a list of drugs that need prior approvaln Get a prior approval request form
Your doctor can submit requests for prior approval by:n Submitting an ePA (electronic prior approval)n Calling toll-free 1-877-727-3784n Filling out the Prior Approval Form found at
fepblue.org/priorapproval
Help with Prior Approval

5
HOW TIERS RELATE TO COSTS
The costs of drugs vary. How much you pay is your cost share. Look for your drug in the 5-tier formulary for your Plan option. The tier level where your drug type is listed determines your cost.
Generally, the lower the drug tier, the lower the cost. Generic drugs (Tier 1) and Preferred brand name drugs (Tier 2) provide you with high-quality, cost-effective options.
YOUR COST SHARE
TIER DRUG TYPE
Tier 1 Generic Drugs: typically the most affordable, and are equal to their brand name counterparts in quality, performance and intended use.
Tier 2 Preferred Brand Name Drugs: proven to be safe, effective, and cost less than Non-preferred brands.
Tier 3 Non-preferred Brand Name Drugs: typically higher cost share since there is a generic or Preferred brand available.
Tier 4 Preferred Specialty Drugs: proven to be safe, effective, and favorably priced compared to Non-preferred specialty drugs.
Tier 5 Non-preferred Specialty Drugs: typically higher cost share since there is a Preferred specialty drug available.
Basic and Standard Options
To see your cost share for a prescription drug:
- visit fepblue.org/pharmacy - call CVS Caremark for Retail or Mail Order drugs: 1-800-624-5060 - call AllianceRx Walgreens Prime for Specialty drugs: 1-888-346-3731

6
BASIC OPTION COST SHARE TIERS
Basic Option members must use a Preferred retail pharmacy and will save by choosing generic drugs and Preferred brand name drugs when possible. Use the charts below to find your cost share.
YOUR COST SHARE
* Basic Option members with Medicare Part B coverage have Mail Service Pharmacy benefits and some lower cost shares.
See p. 10-11
BASIC OPTION: Cost Share Based on Where You Fill Your Prescription
TIER PREFERRED RETAIL PHARMACY
NON-PREFERRED RETAIL & MAIL SERVICE PHARMACY
Tier 1: Generic Drugs
- Up to $10 - You can get up to a 30-day supply for 1 copayment or up to a 90-day supply for 3 copayments
Not covered*
Tier 2: Preferred Brand Name Drugs
- Up to $50 - You can get up to a 30-day supply for 1 copayment or up to a 90-day supply for 3 copayments
Tier 3: Non-preferred Brand Name Drugs
- 60% of the drug price when the price is $110 or greater
- $75 copayment or the drug price when the price is less than $125
- You can get up to a 30-day supply for 1 copayment or up to a 90-day supply for 3 copayments

7
YOUR COST SHARE
BASIC OPTION: Specialty Drugs - Cost Share Based on Where You Fill Your Prescription
TIER SPECIALTY PHARMACY PREFERRED RETAIL PHARMACY
Tier 4: Preferred Specialty Drugs
- Up to $55 for a 30-day supply or $165 for a 31 to 90-day supply
- You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill
- Up to $65 for up to a 30-day supply only
- When you buy specialty drugs at a Preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
Tier 5: Non-preferred Specialty Drugs
- Up to $80 for a 30-day supply or $240 for a 31 to 90-day supply
- You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill
- Up to $90 for up to a 30-day supply only
- When you buy specialty drugs at a Preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy

8
STANDARD OPTION COST SHARE TIERS
Standard Option members save by using the Mail Service Pharmacy and Preferred retail pharmacies for filling prescription drugs. Members can also save by asking for generic drugs and Preferred brand name drugs when possible. Use the charts below to find your cost share.
YOUR COST SHARE
* Lower cost shares are available to Standard Option members with Medicare Part B.
See p. 12-13
STANDARD OPTION: Cost Share Based on Where You Fill Your Prescription
TIER MAIL SERVICE PHARMACY
PREFERRED RETAIL PHARMACY
NON-PREFERRED RETAIL PHARMACY
Tier 1: Generic Drugs
- Up to $15* - 20% of our allowance*
- 45% of the average wholesale price plus any difference between our allowance and the billed amount
- If you use a Non-preferred retail pharmacy, you need to file a paper claim for reimbursement
Tier 2: Preferred Brand Name Drugs
- Up to $80 - 30% of our allowance
Tier 3: Non-preferred Brand Name Drugs
- Up to $125 - 50% of our allowance

9
STANDARD OPTION: Specialty Drugs - Cost Share Based on Where You Fill Your Prescription
TIER SPECIALTY PHARMACY
PREFERRED RETAIL PHARMACY
NON-PREFERRED RETAIL PHARMACY
Tier 4: Preferred Specialty Drugs
- $35 for up to a 30-day supply
- $95 for a 31 to 90-day supply
- You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill
- 30% of our allowance - up to 30-day supply
- When you buy specialty drugs at a Preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
- 45% of the average wholesale price plus any difference between our allowance and the billed amount
- When you buy specialty drugs at a Non-preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
Tier 5: Non-preferred Specialty Drugs
- Up to $55 for a 30-day supply
- $155 for a 31 to 90-day supply
- You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill

10
BASIC OPTION MEDICARE PART B COST SHARE TIERS
If you have Medicare Part B as your primary payer you can lower your cost share on your prescription drugs. Use the charts below to find your cost share.
YOUR COST SHARE
BASIC OPTION MEDICARE B: Your Cost Share Based on Where You Fill Your Prescription
TIER MAIL SERVICE PHARMACY
PREFERRED RETAIL PHARMACY
NON-PREFERRED RETAIL PHARMACY
Tier 1: Generic Drugs
- Up to $20 - Up to $10 - You can get up to a 30-day supply for 1 copayment or up to a 90-day supply for 3 copayments
Not Covered
Tier 2: Preferred Brand Name Drugs
- Up to $90 - Up to $45 - You can get up to a 30-day supply for 1 copayment or up to a 90-day supply for 3 copayments
Tier 3: Non-preferred Brand Name Drugs
- Up to $125 - 50% of the drug price when the price is $120 or greater
- $60 copayment or the drug price when the price is less than $120
- You can get up to a 30-day supply for 1 copayment or up to a 90-day supply for 3 copayments

11
Members who have Basic Option with Medicare Part B can also use the Mail Service Pharmacy in addition to Preferred retail pharmacies for more savings and the added convenience of having your drugs delivered to your door.
YOUR COST SHARE
TIER SPECIALTY PHARMACY PREFERRED
RETAIL PHARMACY
Tier 4: Preferred Specialty Drugs
Tier 5: Non-preferred Specialty Drugs
- Up to $50 for a 30-day supply or $140 for a 31 to 90-day supply - You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill
- Up to $70 for a 30-day supply or $195 for a 31 to 90-day supply - You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill
- Up to $60 for up to a 30-day supply only - When you buy specialty drugs at a Preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
- Up to $80 for up to a 30-day supply only - When you buy specialty drugs at a Preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
BASIC OPTION MEDICARE PART B: Specialty Drugs - Your Cost Share Based on Where You Fill Your Prescription

12
STANDARD OPTION MEDICARE PART B COST SHARE TIERS
If you have Standard Option with Medicare Part B as your primary payer, you can enjoy lower cost share at the pharmacy and through the Mail Service Pharmacy. Use the charts below to find your cost share.
YOUR COST SHARE
TIER MAIL SERVICE PHARMACY
PREFERRED RETAIL PHARMACY
NON-PREFERRED RETAIL PHARMACY
Tier 1: Generic Drugs
Tier 2: Preferred Brand Name Drugs
Tier 3: Non-preferred Brand Name Drugs
-Up to $10
-Up to $80
-Up to $125
- 15% of our allowance
- 30% of our allowance
- 50% of our allowance
- 45% of the average wholesale price plus any difference between our allowance and the billed amount
- If you use a Non-preferred retail pharmacy, you need to file a paper claim for reimbursement
STANDARD OPTION MEDICARE PART B: Your Cost Share Based on Where You Fill Your Prescription

13
YOUR COST SHARE
STANDARD OPTION MEDICARE PART B: Specialty Drugs - Your Cost Share Based on Where You Fill Your Prescription
TIER SPECIALTY PHARMACY
PREFERRED RETAIL PHARMACY
NON-PREFERRED RETAIL PHARMACY
Tier 4: Preferred Specialty Drugs
- $35 for up to a 30-day supply
- $95 for a 31 to 90-day supply
- You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill
- 30% of our allowance - up to a 30-day supply
- When you buy specialty drugs at a Preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
- 45% of the average wholesale price plus any difference between our allowance and the billed amount
- When you buy specialty drugs at a Non-preferred retail pharmacy, you are limited to one 30-day supply for each prescription. You must get all refills through the Specialty Pharmacy
Tier 5: Non-preferred Specialty Drugs
- Up to $55 for a 30-day supply
- $155 for a 31 to 90-day supply
- You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get up to a 90-day supply after the 3rd fill

14
Be a Smart Consumer
Use Preferred Brand Name Drugs
Use Generics
Use Preferred Specialty Drugs If You Have a Specialty Prescription
Use Mail Service for Long-term Prescription Drugs
Use a Preferred Retail Pharmacy
Read on to learn more about how each of these ways can help you save.
Understanding your pharmacy benefit will save you time and money. Here are even more ways to save:
WAYS TO SAVE
BRAND

15
BRAND
Be a Smart Consumer
Drug makers spend a lot of money on research and development. Bringing their new, brand name drug to market has huge costs. Those costs are passed along to you. So it’s important to choose a drug based on how well it works, not its advertising slogan.
Work with your doctor and pharmacist to choose drugs that are right for you. They are the experts on health conditions and the prescription drugs used to treat them. Ask questions. The more you know, the better you will feel about your drug therapy choices.
Use Preferred Brand Name Drugs
Preferred brand name drugs have been proven to be safe, effective, and lower in cost. Your cost share for a Preferred brand name drug is always lower than the cost of a Non-preferred brand name drug.
Use Generics
The FDA requires that generic drugs are equal in quality to their brand name counterparts, and you almost always pay less for generics. Ask your doctor to approve a generic substitution when possible.
STANDARD OPTION
Standard Option members have the option of using the Generic Incentive Program (GIP). When using the GIP, your cost share for the first 4 prescriptions filled (and/or refills ordered) per generic drug each calendar year are waived when you do 2 things:
n You switch from a brand name drug on the GIP list to a generic drug replacement (not from one generic to another generic).
n You buy both the brand name drug and the corresponding generic drug replacement during the same calendar year.
WAYS TO SAVE

16
Use Preferred Specialty Drugs If You Have a Specialty Prescription
A specialty prescription drug is used to treat complex health conditions, such as multiple sclerosis and hemophilia. Specialty drugs are usually high in cost and have one or more of these elements:
n Are injectable n Are infused n Are products of
biotechnology n Have special requirements
for handling, shipping, and storage
n Need specialized patient training and coordination of care
The Specialty Pharmacy Program provides more than just your specialty drugs. You can also count on services tailored to your needs, such as:
n Access to an on-call pharmacist, any time day or night
n Options to have your specialty drugs mailed to your home, doctor’s office or location of your choice
n Advice and information about managing your health and medicine
n Online support through fepblue.org, including information about your condition and drug cost.
WAYS TO SAVE

17
FACTS TO KNOW ABOUT SPECIALTY DRUGS
n Specialty drugs in Tier 4 are Preferred.
n Specialty drugs in Tier 5 are Non-preferred.
n You can get your first 30-day specialty fill through the Specialty Pharmacy Program, which may save you money, or through a Preferred retail pharmacy. You must get all refills through the Specialty Pharmacy Program.
n You are limited to a 30-day supply for the first 3 fills of each specialty drug. You can get a 90-day supply after the third fill.
TO FILL YOUR SPECIALTY DRUGS
1. Make sure your drug is on the Specialty Drug List. To see the list:
n Visit fepblue.org/specialtypharmacy.
n Call the Specialty Pharmacy toll-free at 1-888-346-3731.
2. Ask your doctor to get prior approval, if required.
3. Be sure to have your prescription information and member ID card with you. Then choose an option:
n Ask your doctor to send an electronic prescription to AllianceRx Walgreens Prime.
n Call, or ask your doctor to call, toll-free at 1-888-346-3731 Monday-Friday, 7:00 a.m. to 9:00 p.m. or Saturday-Sunday 8:00 a.m. to 6:30 p.m. Eastern time.
n Ask your doctor to fill out the Specialty Medicine Order Form and send it to:
AllianceRx Walgreens Prime P.O. Box 692169 Orlando, FL 32869
WAYS TO SAVE

18
Use Mail Service Pharmacy for Long-term Drugs
STANDARD OPTION AND BASIC OPTION WITH MEDICARE PART B
The Mail Service Pharmacy Program is a convenient way to get your maintenance or long-term drugs:
n Those you take regularly and need to take long-term
n Examples include drugs for high blood pressure, arthritis, or other chronic conditions
You can get up to a 90-day supply (minimum 22-day supply) of long-term drugs for one copayment. Choose to have these drugs sent to your home, office, or a location of your choice with free standard shipping. Using Mail Service saves you time by avoiding trips to the pharmacy.
TO FILL YOUR DRUGS WITH MAIL SERVICE PHARMACY
It’s easy to request your Mail Order prescription:
n Log in to fepblue.org/myblue and follow the Mail Order prescription links
n Ask your doctor to electronically prescribe or call the Mail Service Customer Care line toll-free at 1-877-727-3784
n Complete the Mail Service Order Form. Mail the form, your prescription, and your copayment to: CVS Caremark P.O. Box 1590 Pittsburgh, PA 15230-9607
The Mail Service Order Form is available at fepblue.org/forms or by calling the Mail Service Customer Care line toll-free at 1-800-262-7890.
BASIC OPTION WITHOUT MEDICARE PART B
Mail Service is not a covered benefit. You can save money by using a Preferred retail pharmacy to fill your generic and Preferred drugs (no benefit coverage at Non-preferred retail pharmacies).
WAYS TO SAVE
19
WAYS TO SAVE
Use a Preferred Retail Pharmacy
Standard and Basic Option members have access to more than 65,000 Preferred retail pharmacies across the country. You only pay the cost share under your Plan for each prescription or refill. It’s that easy.
TO FIND A PREFERRED RETAIL PHARMACY NEAR YOU
n Visit fepblue.org/pharmacy.
n Call CVS Caremark any time toll-free at 1-800-624-5060.
TO FILL YOUR PRESCRIPTION AT A PREFERRED RETAIL PHARMACY
Simply show your member ID card when submitting your prescription.
If You Use a Non-preferred Retail Pharmacy
BASIC OPTION
You must use a Preferred retail pharmacy. If you get your drug from a Non-preferred retail pharmacy, you will pay 100% of the prescription cost.
It’s easy to switch to a Preferred retail pharmacy. Just tell the pharmacist where your prescription is on file. The pharmacist will contact the Non-preferred retail pharmacy and transfer your prescription.
STANDARD OPTION
You may buy your prescription drugs and supplies from Non-preferred retail pharmacies. You will need to pay the full cost for these items. Then file a Retail Prescription Drug Claim for reimbursement. For claim forms:
n Visit fepblue.org/forms.
n Call 1-800-624-5060.

20
RETAIL PHARMACY
1. Pay the full price for the prescription.
2. Get an itemized bill. It should include the pharmacy’s name and address, patient’s name, prescription number, date filled, name of drug or supply, strength, quantity, dosage and charge for each drug or supply.
3. Ask your pharmacist to help you fill out the pharmacy and prescription information sections of the claim form:
n Visit fepblue.org/forms. Choose the Retail Prescription Drug Claim Form.
n Call 1-800-624-5060.
4. Complete the enrollee information and patient information sections of the claim form and sign the bottom. Your claim will not be accepted after one year from payment date.
5. Send the completed claim form and any related pharmacy receipt(s) to:
Blue Cross and Blue Shield Service Benefit Plan Retail Pharmacy Program P.O. Box 52057 Phoenix, AZ 85072-2057
OVERSEAS
Drugs you buy overseas must be equivalent to drugs that need a prescription in the United States. This is a U.S. federal law. File a claim for covered drugs and supplies you buy from pharmacies outside the United States and Puerto Rico. Please note that claims are not accepted after one year from payment date.
Use the address above in red to send both your:n Completed Retail Prescription
Drug Overseas Claim Formn Itemized pharmacy receipts
or billsOr fax the information to:001-480-614-7674We provide translation and conversion services for your overseas claims. To get a claim form for your overseas prescription drug purchases:n Visit fepblue.org/forms.n Call 1-800-624-5060.
FILING A CLAIM

21
SAVE TIME WITH OVERSEAS CLAIMS BY FILING ONLINE
For faster processing and payment, you can also submit overseas pharmacy claims online. It’s easy. Just follow these simple steps:
1. Log in to MyBlue at fepblue.org/myblue.
2. On the homepage, hover over the Health Tools tab and click Submit Overseas Claim.
3. Follow the instructions to submit the claim and upload your itemized bills.
DRUGS FROM SUPPLEMENTARY PROVIDERS
You may get prescription drugs and supplies from providers other than retail or mail pharmacies, like:n Your doctorn Your hospitaln A government health centerIn these cases, you need to pay for your items and file a claim form for reimbursement:
1. Be sure to get an itemized receipt.
2. Then, fill out the Health Benefits Claim Form.
3. Send your form, along with your itemized receipt, to your local Blue Cross and Blue Shield company.
For drugs and supplies you get from these providers, your medical cost share amounts apply to covered charges. Check the 2018 Service Benefit Plan brochure (RI 71-005) for details.
HOSPITAL OUTPATIENT DEPARTMENTS
Most hospital outpatient pharmacies are Non-preferred retail pharmacies.
FILING A CLAIM

22
PHARMACY BENEFIT HIGHLIGHTS
NEW: High Cholesterol-lowering Drug Benefit
BASIC OPTION AND STANDARD OPTION
Members of all ages can receive generic cholesterol-lowering drugs (known as statins) at no cost. This benefit applies when you use a Preferred retail pharmacy.
NEW: Asthma Drug Benefit
BASIC OPTION AND STANDARD OPTION
Your cost share is reduced for generic and Preferred non-specialty asthma drugs. This benefit applies when you use a Preferred retail pharmacy or through the Mail Service Pharmacy Program for all Standard Option members or Basic Option members with Medicare Part B.
STANDARD OPTION
BASIC OPTION
BASIC OPTIONMEDICARE PART B
PREFERREDRETAIL
Tier 1: up to $5 copayment
Tier 2: 20% of our allowance
Tier 1: $5 copayment
Tier 2: $35 copayment (for each 30-day supply)
Tier 1: $5 copayment
Tier 2: $30 copayment (for each 30-day supply)
MAIL Tier 1: $5 copayment
Tier 2: $65 copayment
No Benefit Tier 1: $5 copayment
Tier 2: $75 copayment
All cost shares are for up to a 90-day supply unless otherwise noted.
23
PHARMACY BENEFIT HIGHLIGHTS
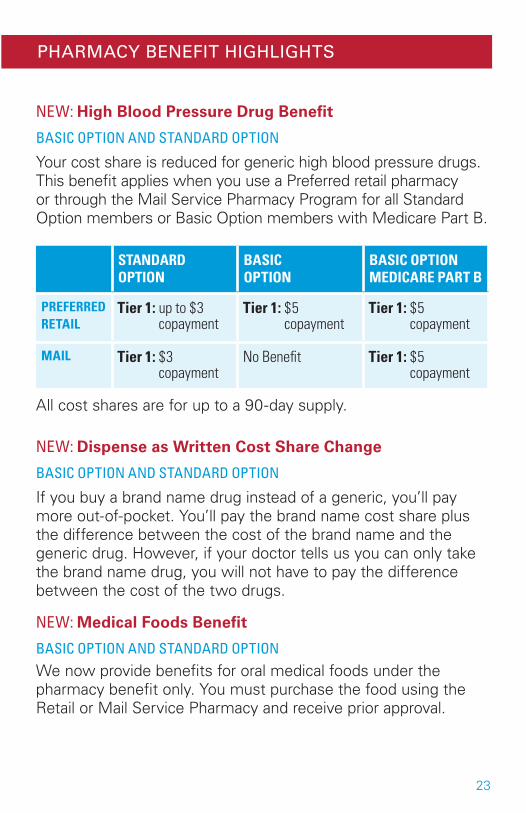
NEW: High Blood Pressure Drug Benefit
BASIC OPTION AND STANDARD OPTION
Your cost share is reduced for generic high blood pressure drugs. This benefit applies when you use a Preferred retail pharmacy or through the Mail Service Pharmacy Program for all Standard Option members or Basic Option members with Medicare Part B.
NEW: Dispense as Written Cost Share Change
BASIC OPTION AND STANDARD OPTION
If you buy a brand name drug instead of a generic, you’ll pay more out-of-pocket. You’ll pay the brand name cost share plus the difference between the cost of the brand name and the generic drug. However, if your doctor tells us you can only take the brand name drug, you will not have to pay the difference between the cost of the two drugs.
NEW: Medical Foods Benefit
BASIC OPTION AND STANDARD OPTIONWe now provide benefits for oral medical foods under the pharmacy benefit only. You must purchase the food using the Retail or Mail Service Pharmacy and receive prior approval.
STANDARD OPTION
BASIC OPTION
BASIC OPTIONMEDICARE PART B
PREFERRED RETAIL
Tier 1: up to $3 copayment
Tier 1: $5 copayment
Tier 1: $5 copayment
MAIL Tier 1: $3 copayment
No Benefit Tier 1: $5 copayment
All cost shares are for up to a 90-day supply.

24
Contraceptive Benefit
BASIC OPTION AND STANDARD OPTIONYour cost share is waived for generic and brand name contraceptives that have no generic equivalent or alternative. This benefit applies when you use a Preferred retail pharmacy or through Mail Service Pharmacy Program for all Standard Option members and Basic Option members with Medicare Part B.
Diabetic Benefit
BASIC OPTION
Members may get insulin and diabetic supplies from a Preferred retail pharmacy.
STANDARD OPTION
Members may get insulin and diabetic supplies from a Preferred or Non-preferred retail pharmacy or the Mail Service Pharmacy Program.
PRIMARY COVERAGE WITH MEDICARE PART B
You may also receive insulin and diabetic supplies from doctors or other healthcare providers.
PHARMACY BENEFIT HIGHLIGHTS

25
Preventive Benefit
Standard Option and Basic Option members who meet age and gender range guidelines will have their cost share amount waived for the following generic, brand and over-the-counter (OTC) prescriptions:n Iron supplements for children
from age 6 months through 12 months
n Oral fluoride supplements for children from age 6 months through 5 years
n Folic acid supplements, 0.4 mg to 0.8 mg, for women capable of pregnancy
n Vitamin D supplements for adults, age 65 and over, limited to a recommended daily allowance of 600-800 international units (I.U.s) per day
n Low-dose aspirin (81 mg per day) for pregnant women at risk for preeclampsia
n Aspirin for men age 45 through 79 and women age 50 through 79 for the primary prevention of cardiovascular disease and colorectal cancer
n Cholesterol-lowering generic statin drugs
Eligible members must meet the following criteria:n Medicine must be filled at a
Preferred retail pharmacyn Obtain a written prescription
from their physician for all products, including OTC products which do not require a prescription by law
Other Programs
These are just a few of your pharmacy benefit highlights. Your Service Benefit Plan includes so much more. For other programs such as the breast pump benefit and more, see:n The Service Benefit Plan
brochure (RI 71-005)n Our website at fepblue.org
PHARMACY BENEFIT HIGHLIGHTS

26
Through our easy-to-use website, you can discover everything the Blue Cross and Blue Shield Service Benefit Plan has to offer. Easily compare benefit plans, learn about our wellness resources and Health Tools, register for a MyBlue® account, and much more.
By visiting fepblue.org/pharmacy you’ll be able to: n Find a pharmacyn Check drug costsn View formulariesn Review Prior Approval drugsn And more
Register and log in to MyBlue®
MyBlue is our exclusive member’s only website. It’s your personal health website designed to help you get the most out of your healthcare coverage.
With your MyBlue account, you’ll be able to:n Keep track of your out-of-pocket costsn View your claims historyn Check drug costsn Access health and wellness toolsn Request additional member ID cards or view your digital versionn And more
Create your account today at fepblue.org/signup. After you register for the first time, you’ll be able to access MyBlue 24/7 at fepblue.org/myblue.
Take the Blue Health Assessment
The Blue Health Assessment (BHA) is an online questionnaire that helps address health risks before they become issues. It takes 10 minutes or less to complete. All you need to do is answer a few questions related to your health. Then, you’ll receive a personalized wellness plan. You can print a copy of the wellness plan to take to your next doctor’s visit.
FEPBLUE.ORG

27
Take advantage of additional BCBS programs
DIABETES MANAGEMENT INCENTIVE PROGRAMIf you have diabetes, earn up to $100 on your MyBlue Wellness Card for taking steps to keep your A1c levels under control. Learn more at fepblue.org/diabetes.
TOBACCO CESSATION INCENTIVE PROGRAMIf you’re ready to quit smoking, you can receive free over-the-counter and prescription tobacco cessation products. Learn more at fepblue.org/tobacco.
HYPERTENSION MANAGEMENT PROGRAMIf you have high blood pressure, you may be eligible to receive a free in-home blood pressure monitor every two years. Learn more at fepblue.org/highbloodpressure.
DISCOUNT DRUG PROGRAMThis program gives you a discount on specific drugs, such as weight loss drugs, that are not covered under your prescription drug benefit. You can see a full list of eligible drugs and participating pharmacies at fepblue.org/pharmacy.
FINANCIAL DASHBOARDThe Financial Dashboard is a tool on MyBlue that lets you see a complete picture of your annual healthcare spending to date, including:n How much you have left to pay out of pocket until you meet
your out-of-pocket maximumn Your medical and pharmacy claims historyn Your MyBlue Wellness Card balance
FEPBLUE.ORG

28
Fill a Prescription1. Preferred Retail Pharmacies: for all Service Benefit Plan members
See p. 19
2. Mail Service Pharmacy Program: for Standard Option members and Basic Option with Medicare Part B members See p. 18
3. Specialty Pharmacy Program: for all Service Benefit Plan members See p. 16-17
4. Non-preferred Retail Pharmacies: for Standard Option members See p. 19
Get Information about Cost Share Tiersn Basic Option Cost Share Tiers See p. 6-7
n Standard Option Cost Share Tiers See p. 8-9
n Basic Option Medicare Part B Cost Share Tiers See p. 10-11
n Standard Option Medicare Part B Cost Share Tiers See p. 12-13
Learn More about Your Pharmacy Benefitn Visit fepblue.org/pharmacy
n Call CVS Caremark for Retail and Mail Order Programs any time toll-free at 1-800-624-5060
n Call AllianceRx Walgreens Prime for Specialty Pharmacy Program any time at 1-888-346-3731
FIND IT FAST

29
FIND A FORM
Find a Form n Visit fepblue.org/forms. Then click Forms to find:
- Retail Prescription Drug Claim Form
- Mail Service Prescription Drug Form
- Retail Prescription Drug Overseas Claim Form
- Specialty Medicine Order Form
- Prior Approval Pharmacy Forms
- Managed Formulary Exception Form (for “Managed Not Covered” Drugs)
- Standard Option Exclusion Form n Call CVS Caremark at 1-800-624-5060 for most formsn Call AllianceRx Walgreens Prime at 1-888-346-3731 for specialty
drug forms

30
NOTICE OF NONDISCRIMINATION
The Blue Cross and Blue Shield Service Benefit Plan complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. This Plan does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
The Blue Cross and Blue Shield Service Benefit Plan:
Provides free aids and services to people with disabilities to communicate effectively with us, such as:n Qualified sign language
interpretersn Written information in
other formats (large print, audio, accessible electronic formats, other formats)
Provides free language services to people whose primary language is not English, such as:n Qualified interpretersn Information written in other
languages
If you need these services, contact the Civil Rights Coordinator of your local Blue Cross and Blue Shield company by calling the customer service number on the back of your member ID card.
If you believe that this Plan has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with the Civil Rights Coordinator of your local BCBS company. You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, your local BCBS company’s Civil Rights Coordinator is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office of Civil Rights, electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:

31
U.S. Department of Health and Human Services 200 Independence Ave, SW Room 509F, HHH Building Washington, D.C. 20201 1-800-368-1019, 800-537-7697 (TDD)
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
Language Assistance Para obtener asistencia en español, llame al servicio de atención al cliente al número que aparece en su tarjeta de identificación.
請撥打您 ID 卡上的客服號碼以尋求中文協助。
Gọi số dịch vụ khách hàng trên thẻ ID của quý vị để được hỗ trợ bằng Tiếng Việt.한국어로 도움을 받고 싶으시면 ID 카드에 있는 고객 서비스 전화번호로 문의해 주십시오.
Para sa tulong sa Tagalog, tumawag sa numero ng serbisyo sa customer na nasa inyong ID card.
Обратитесь по номеру телефона обслуживания клиентов, указанному на Вашей идентификационной карточке, для помощи на русском языке.
دوجوملا ءالمعلا ةمدخ مقرب لصتا ىلع لوصحلل كتيوُه ةقاطب ىلع.ةيبرعلا ةغللاب ةدعاسملاRele nimewo sèvis kliyantèl ki nan kat ID ou pou jwenn èd nan Kreyòl Ayisyen.
Pour une assistance en français du Canada, composez le numéro de téléphone du service à la clientèle figurant sur votre carte d’identification.
Ligue para o número de telefone de atendimento ao cliente exibido no seu cartão de identificação para obter ajuda em português.
Aby uzyskać pomoc w języku polskim, należy zadzwonić do działu obsługi klienta pod numer podany na identyfikatorze.日本語でのサポートは、IDカードに記載のカスタマーサービス番号までお電話でお問い合わせください。
Per assistenza in italiano chiamate il numero del servizio clienti riportato nella vostra scheda identificativa.
Rufen Sie den Kundendienst unter der Nummer auf Ihrer ID-Karte an, um Hilfestellung in deutscher Sprache zu erhalten.
نابز هب ییامنهار تفایرد یارب هک یرتشم تامدخ هرامش اب ، یسراف جرد امش ییاسانش تراک یور رب..دیریگب سامت تسا هدش

32
HOW TO CONTACT US
Call these numbers for prescription drug information:
RETAIL PHARMACY PROGRAM CVS Caremark (Basic and Standard Option) Toll-free any time at 1-800-624-5060
MAIL SERVICE PHARMACY PROGRAM CVS Caremark (All Standard Option and Basic Option with Medicare Part B) Toll-free any time at 1-800-262-7890
SPECIALTY PHARMACY PROGRAM AllianceRx Walgreens Prime (Basic and Standard Option) Toll-free at 1-888-346-3731
Monday-Friday: 7 a.m. to 9 p.m. Eastern time
Saturday-Sunday: 8 a.m. to 6:30 p.m. Eastern time
OTHER BENEFIT OR CLAIMS INFORMATIONCall your local Blue Cross and Blue Shield company. The customer service number is on the back of your member ID card.
This is a summary of the features of the Blue Cross and Blue Shield Service Benefit Plan. Before making a final decision, please read the Plan’s Federal brochure, RI 71-005. All benefits are subject to the definitions, limitations and exclusions set forth in the Federal brochure.